This is a cancer update. In response to a recent PET scan, I started my second set of chemo rounds on July 10th. This time, I plan to have 6 rounds instead of just 4. While my new rib tumor is much smaller than the first time, we want to give it more rounds this time, so we make sure we get everything.
NGS: We reanalyzed my tumor using Next Generation Sequencing. This amazing new technology allow scientists to sequencing many different pieces of DNA in the same sample. In this case, instead of a biopsy, they took a blood sample and looked for their targets, a particular set of gene, in the sample. Even though my tumor cells would be a tiny minority of the total cells in my blood, NGS can still find them and sequence them individually. Happily, analysis shows that my new tumor is genetically the same as my old one, so it should respond to chemotherapy in the same way, just as we hoped.
I also took a monitoring test that finds and counts the number of tumor cells in my blood, which will help us track progress in the future. This is a different technology called real-time PCR. I have worked extensively with both of these technologies at my job at Quest Diagnostics, and in my current consulting business.
Chemotherapy: The July 10th chemo itself went well. Usually, the week after is the worst part. I take some medications in the few days surrounding the actual infusion. They counter act many of the side effects I might normally feel like nausea and fatigue. I stop taking some of these medications on Monday, so Tuesday and Wednesday of the following week are usually the worst. This time, since I’m so much healthier in general than last time, my “bad week” was much better, just a little sleepiness and a little skin irritation, both very manageable. I actually started my second new round yesterday with another infusion.
Kathy and I enjoy a celebratory bag of Doritos during yesterday’s infusion. Don’t mind my pasty complexion. I pretty much always look like that. Photo credit: Kathy Johnson
Radiation: As it turns out, my radiation oncologist says they can treat the rib tumor again, since I didn’t get too much radiation the first time. I’ve already had my mapping session, and I start radiation next week. This will greatly accelerate rib tumor healing. It will likely make me even sleepier next week. So if you call or text next week, you may not hear from me for a while! But weeks 2 and 3 will be better, because of my better overall health. Outdoor meetings are definitely possible!
Thank you so much for your continued prayers! It’s definitely helping!
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
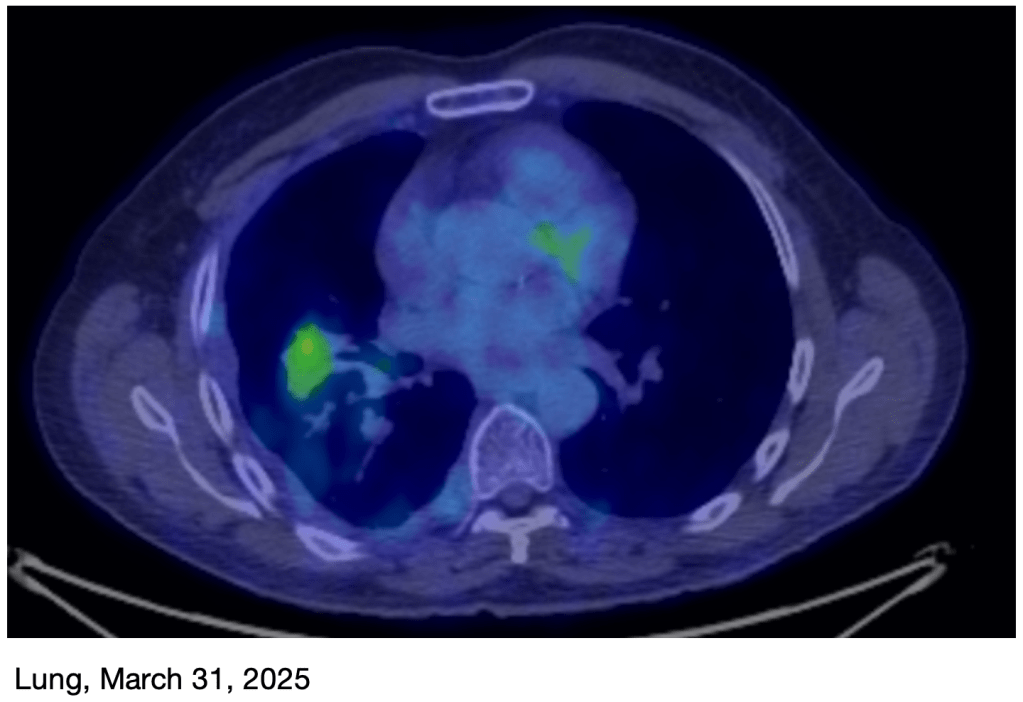
I have some sobering news. I had a PET scan on Tuesday and it appears that the rib tumor is trying to make a comeback. My original treatment plan had just 4 rounds of chemo, and then immunotherapy after that. While the chemotherapy worked well, it appears that the immunotherapy has not been as effective as was hoped.
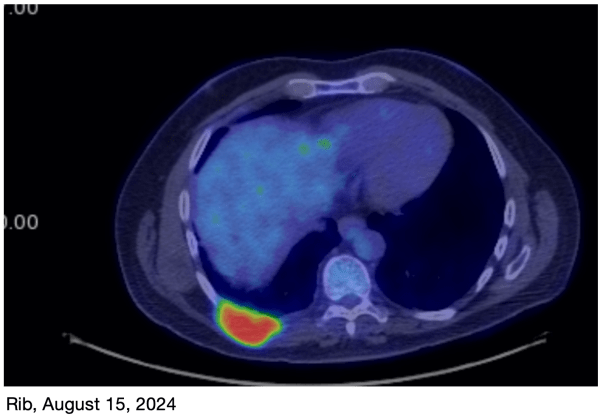
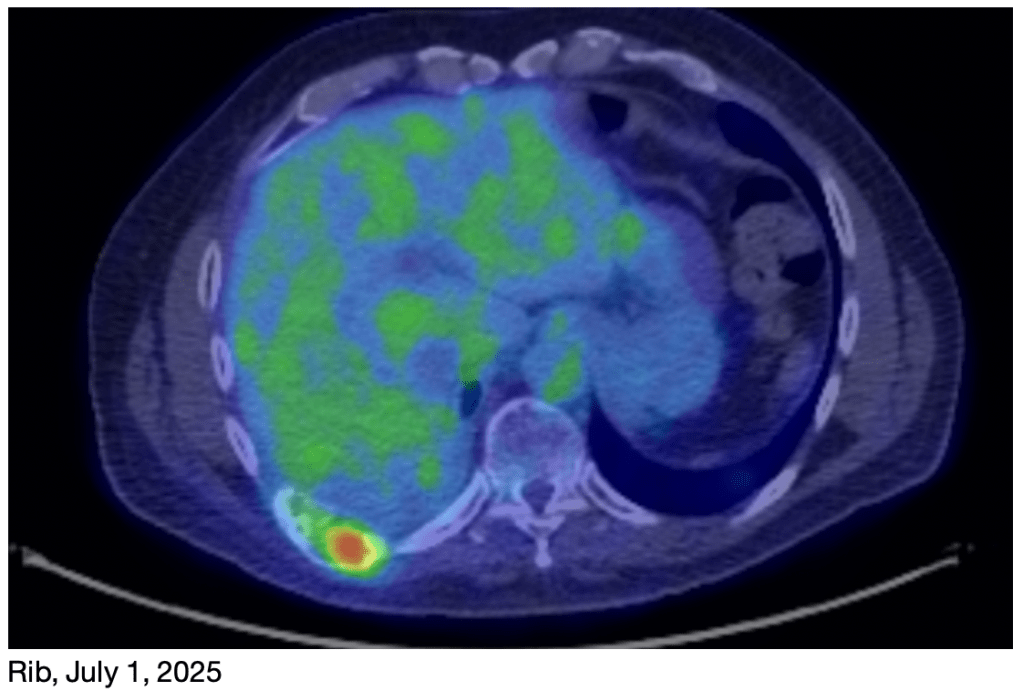
As you can see in the images, the rib tumor was basically absent in the March 30th image, but has reappeared in the image from this week (July 1st).
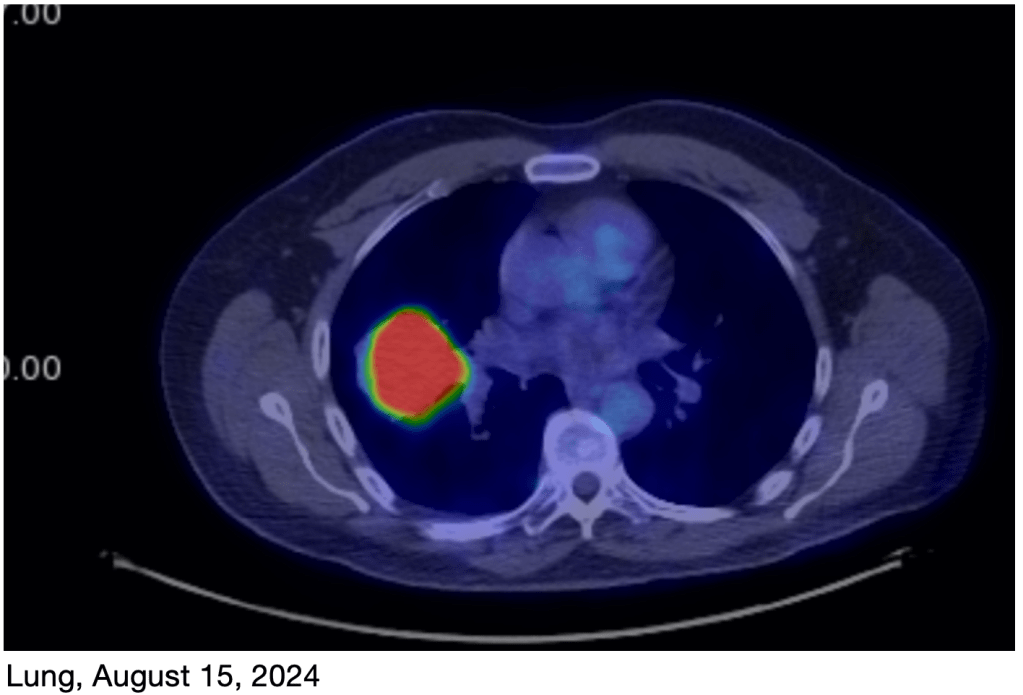
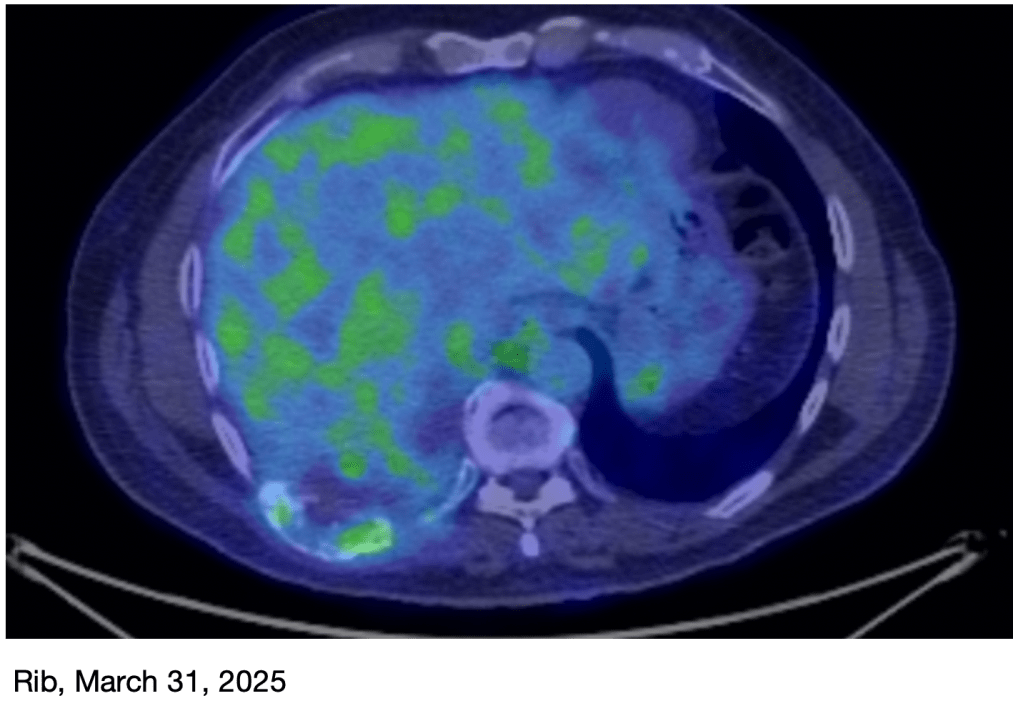
The rib tumor is essentially gone. You can see the “expansile” nature of the damaged rib in the March image. The extra green you see is background activity in the liver.As you can see, the rib tumor has reappeared, although still much smaller than the original size.The primary lung tumor is very faint in this image, and the rib tumor is gone.The rib tumor is still smaller and less hypermetabolic (Cancer cells use lots of sugar, which makes them light up in a PET scan. This is called hypermetabolism) than it was before.
We met with my oncologist this morning. Since the chemo was effective last Fall, and the tumor is now much smaller than it was back then, he is very hopeful that it will be effective again. While we will do another Next Generation Sequencing test to determine the genetics of the tumor, he expects that it will not have changed significantly since the first time. So the same chemo treatment should still be effective. Tentatively, we plan 6 rounds this time, instead of the 4 we had before. We will likely start next Thursday.
I’m in much better shape this time than I was last time. Last time, I was still struggling with serious complications from my pleural effusion, and the big infection I had. This time, I’m in generally good health, much stronger, and doing well except for the remaining rib pain. The lung tumor has not returned.
All this to say, there is a lot of reason for hope.
But my hope is not just in technology. Our God is the Maker of heaven and earth (a Hebrew idiom for everything!) and He does whatever He wants. Man does not live by bread alone, but by every Word that proceeds from the mouth of God (Deuteronomy 8:3, Matthew 4:4). This means that if God says I will live, then I will live. We have already experienced legitimate miracles during our journey, and I am confident that we will experience more. God isn’t finished with me yet!
Once I start my new treatment, I expect to be tired and somewhat immunocompromised, so I’ll need to stay close to home again. My energy permitting, I’d love to hang out with you in the warm sun in my backyard.
If you are a praying person, I would of course love to have your continued prayers.
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
As I said in my last update, March was a difficult month. Despite some great test results, my nerves were growing back and causing some extra pain in my torso.
April and May were much better! I had steady progress in my nerve and muscle pain in my torso every week! I also started doing exercises in the pool, under the instruction of my physical therapist. The climax of this was a bunch of traveling that I would not have dared to attempt a few months ago!
A week few weeks ago, I went to Virginia to visit my parents. My sister lives there too, and my brother came out from Montana as well. It was great seeing everyone, and they were happy to see that I was doing well! I was a little concerned about walking through the airports and lifting my bag into the overhead, but all of that stuff went well! I was very pleased!
Kathy and I on the plane waiting for takeoff.Broose, Gretchen, and I in Virginia. So great to be together!
Then, just last week, we took a road trip to Oregon! I was even more nervous about this trip, because it involved a lot of driving, which has been difficult for me in the last few months. Thanks to the good lumbar support in my wife’s Highlander, the trip went well! This was a milestone in my recovery, and demonstrates that I am ready to do more than I have been doing so far!
Driving back from Oregon, between Klamath Falls and Weed. Yes, that’s the magnificent Mount Shasta in the background. Before this trip, I hadn’t driven any farther than Orange County!
I’m very thankful that everything went well!
My next PET scan is at the end of June, and I will let you know the results!
I actually plan to go back to work part-time this month! I’m looking forward to getting back to normal life!
Thank you so much for your continued prayers!
Don’t fear, but be smart! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
This a cancer update. I’ll talk about continuing challenges with recovery, a great PET scan result, and I’ll revisit my post on suffering.
Overdoing it: In my last update, I wrote about my triumphant climb up a local peak, using my newly added lung capacity after a cold. The next day, however, I was surprised to discover that my sore torso muscles were even more sore. As an aside, my physical therapist said this should be no surprise that after walking only on sidewalks for months, a lot more muscles are needed to walk on a rugged trail!.
It’s been a month since then, and my abs, back and side muscles on the right side continue to be very grumpy, keeping me from going on my longer walks, and occasionally even preventing me from sleeping. I’ve sometimes been discouraged by the regression of some of my capabilities, and I’m even trying to re-dial in my pain meds.
Kathy suggested that maybe my nerves near my broken rib are healing, and maybe this is causing some extra pain, kind of like how a cut may become more sensitive a week or so after it starts healing, as the nerves in the area start working again. This seems to be true. I have some patches of skin that used to be numb that are no longer numb, and others that now feel normal! So my nerves are recovering!
March PET Scan: I just had a new PET scan on Monday, and the results are great! The tumor on my rib is basically gone, and the primary tumor in my lung is now very small, just a faint reminder of what it was! This is obviously great news! I’ll have another scan in June.
The lung tumor is much reduced, now with low levels of increased sugar uptake.The rib tumor is essentially gone. You can see the “expansile” nature of the damaged rib in the March image. The extra green you see is background activity in the liver.The primary lung tumor is very faint in this image, and the rib tumor is gone. I had to guess where the rib tumor was!
Suffering, Part 2: This section contains significant Christian content. Way back in October, I wrote a piece on suffering. The slow recovery of my torso muscles has caused me to reconsider this topic, and I’ve realized recently that the piece had a few key missing parts. A video I saw recently offered a commentary on those missing parts. The below video is humorous and charming but is also required watching for what I write next:
The little English girl is complaining about her great suffering to her mother. She implies that she wants her mother to relieve her of the great burden of carrying her backpack.
As adults, we know that her life will face many more challenges in her future than just the carrying of a 4 pound pack. In fact, we know that in order for the little girl to learn to face these challenges, she may as well learn to carry her burdensome load to school. In order to build her character, the little girl must, in fact, carry her backpack to school.
Kathy and I have felt strongly for some time that the challenge we are going through right now is training for what will come later. But I won’t always have cancer, and Kathy won’t always need to cook and clean for me, manage my medications, run all the errands, and do the extra paperwork necessary to get us reimbursed for our medical expenses. We probably won’t have to carry a burden like this again in the near future, but we will probably need to help others carry their burdens. In fact, we have a friend who was diagnosed with cancer just a few weeks ago. We have encouraged him and prayed for him often in the last few weeks, with an authority that we wouldn’t have had without our recent challenges. Your suffering will give you extra authority to help others.
Suffering changes us. As a general rule, people who suffer either start to degrade and become worse and more miserable, or they become wiser, more seasoned, and more useful to those around them. They become bitter or better. How you respond to suffering will determine which way you go.
If you’re suffering, don’t do the following:
Fixate on your problems: Focusing on the negative is depressing and self-defeating. While facing reality often requires us to face negative aspects of our situation, fixating on them is not healthy, and can keep us from progressing. Wishing things were different is a waste of time.
Blame others for your situation: Yes, others may have contributed to your situation. But you can’t control their behavior, and they may not be willing or able to help you get out of it. Focus on what you can do instead, and what support you may be able to get from those who may be more helpful.
Plot revenge: It’s a big waste of mental effort ruminating on how to get revenge on those that harmed you. Your effort is far better spent considering how you can help yourself. Plus, we can’t all be Edmond Dantès. Most of us are not clever enough to pull off the perfect crime. You’ll probably end up in jail.
Hide from God. It’s actually OK to be angry, even at God. Read the Psalms to see how open David is with God. It’s actually much better to be honest and open with God than to hide from Him and not pray.
Instead, do the following:
Continue to be grateful for the good things in your life. Gratitude is the super weapon of a balanced life. Remembering the good things in your life helps you stay positive and have the proper perspective. Thanksgiving is not a preview for Christmas. Use it to remember the good things in your life, even if you have cancer.
Learn to accept help. Type-A people like me like to get stuff done. But you may find yourself in a position where you have no choice but to accept help from others. It’s ok. We all need help sometimes, and accepting help from others will also make you more gracious when others need your help.
On the other hand, don’t complain if your loved ones can’t help you. Remember that your caregivers carry a special burden during this time. They deeply want to help you, but they often feel helpless to do so. Try and reserve your complaints to things they can help with. Telling them everything may add extra burdens that they don’t need to bear.
Ask, what can I learn from this? I know a lot of people that have prayed for patience. What they don’t realize is that God doesn’t usually give us patience by magically bestowing patience on us. Instead, He puts us in a situation in which patience is required, then gives us the perseverance to endure it. After the challenge is over, we find that we can endure a lot more than we could before. Your suffering is probably like this, slowly and secretly teaching you new ways to face life’s challenges and making you a stronger person.
Ask, how will my experience help others? Am I learning things that others may benefit from knowing? Who in my life may be willing to accept this information? Who can I help right now? Helping others is a wonderful and productive distraction from your suffering.
Ask, did I contribute to my suffering? Can I undo some of the things I did?
What can I do to change my situation? Take responsibility for your situation and do what you can to change it.
What can God do to change my situation? This is a trick question. He can do anything He wants to, but we tend to forget that. He may not take away your suffering, but He can bring people around to support you, give you great ideas to fix things, give you perseverance, give wisdom to your doctors, and yes, even heal you.
Pray. Prayer is not a last resort. It’s a first resort. God can do a lot of things that you can’t. Prayer is also the primary way that God transforms you into a better person. When you are suffering, prayer is essential.
Forgive whoever may have wronged you. Sometimes we have been wronged, even deeply wronged, by others who have caused us suffering. But being angry at them and saying “if only they hadn’t done this to me” is of very little value. In fact, it’s very likely to do much more harm than good. Someone once said, “being bitter against someone is like drinking poison and expecting them to die”. Even if they’ve harmed you greatly, and even if you have a right to be angry, you have to let go of your anger for your sake. This is very difficult. So difficult that often we can’t do it without God’s help. Start by praying for them (Matthew chapter 5). It becomes very difficult to hate those you are praying for!
Believe me when I tell you that I haven’t mastered the above list. I write this as much to remind myself as to tell you. I have had to remind myself of the above many times in the last few months.
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
As you know, I’m done with chemo and radiation treatments, but I’m still recovering from complications stemming from my cancer. I have some medium news and some great news to share today!
Rib progress: First the medium news. I wanted to find out how close my broken rib was to being intact, so I asked my chiropractor to take an X-ray of the area and send it her radiologist. The results were different than I expected. First, there is some confusion about what ribs were affected. Some radiologists say the 8th rib, some the 9th, and some both. This radiologist says both. The great news is, the 8th rib seems to be intact, and is pretty much healed. The 9th rib however is a much more complicated story. The next paragraph and photos may be TMI for some. If you’re easily grossed out, you might want to skip them.
I always thought the rib was merely broken and the cancer had damaged the bones on either side, creating a space in between them. This may have been true for the 8th rib, but the 9th is another story. Instead of breaking the rib, the tumor got inside the rib and pushed material outward, creating a kind of bubble of material, see attached photos. My bone cells may remodel this rib back to looking normal, or they may just leave it be. Only time will tell.
Figure A shows a hot dog shaped area of “expansile” bone around the 9th rib, clarified in Figure B.
The continuing damage to my 9th rib may explain why I have persistent tenderness in several of my torso muscles, making things like bending over and sitting in an office chair for long periods difficult. Physical therapy is definitely helping, but it will take a while for my muscles to adapt.
Lung capacity: Now for the great news! Until last week, I hadn’t had a cold in years. On the few occasions that I coughed or sneezed, it was extremely painful. My ribs have been much better for the past few months, and I finally caught a cold last week. I did A LOT of coughing and sneezing, but it wasn’t nearly as bad as it might have been earlier. As it turns out, all that coughing helped break up material in my lungs and helped them dry out. After my cold, my lung capacity had improved a lot! My cold was a blessing in disguise!
I have a device called a spirometer that kind of measures my lung capacity. After my cold, I could max out the spirometer easily! So on Sunday, Kathy and I decided to see if I could climb a local small peak, Mount Calavera, on a hike I often do with a neighbor. We went up slowly and methodically, but I only needed to stop twice and we made it to the top! I actually see this as a big milestone!
Climbing the steep east slope of Mount Calavera. Brought my trekking poles so I didn’t lose my footing!The view of the ocean from the top was particularly gratifying! On September 13th, I could barely get out of my hospital bed without passing out!My wife Kathy is always by my side!
It’s been more than a month since my last update! To recap, a PET scan showed that the primary tumor in my lung has shrunk a lot and the secondary tumor on my rib is essentially gone. While it seems to me like progress since then is more gradual than I’d like, I definitely see some nice milestones as I look back on the month. While I’m done with radiation and chemo, I’m still getting immunotherapy infusions.
First, I was able to quit taking my last opioid medications a few weeks ago! This granted me the wonderful freedom of being able to drive again! My first solo trip was to grab a carne asada burrito with some friends. I’ve really enjoyed being able to drive myself around again (not too far!), and Kathy has enjoyed a little time to herself at home!
I’m continuing with my physical therapy. My posture is much better, and I’m not so hunchy anymore. A lingering issue is that the muscles of my right lower torso are still quite grumpy. My PT thinks it’s because they are trying to stabilize my rib cage because of the broken rib. While my muscles are loosening up and I’m making progress, I won’t be totally back to normal until my rib completely heals. My oncologist thinks the remaining pieces are about a centimeter or 2 from each other now, so it will still be a while before they come together completely. It’s still a challenge to pick up something off the floor, or to pick up something heavy.
My lung capacity is not back to normal, but I have made big progress. We go for a walk in our neighborhood almost every day. When we first started, I could only make it about 25 yards before I had to come back. Just yesterday, we walked our pre-cancer route, which is 2 miles, with 2 uphill sections. I have to take it slow sometimes, but it’s very nice to know I can go that far. When I return to work, I’ll need to be able to walk quickly around airports to travel again!
That’s all for now. I may not send out another update until after my next PET scan, which will be late March.
Keep praying for better lung capacity, that my rib would heal quickly, and that my torso muscles would settle down.
Don’t fear, but be smart! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
On Monday, I went in for my PET scan. In this procedure, radioactively labeled sugars are injected and allowed to be taken up by cells in the body. Because cancer cells particularly love sugar, the radioactivity mostly ends up in the cancer cells. Scanning for radioactivity highlights the location of tumor tissue.
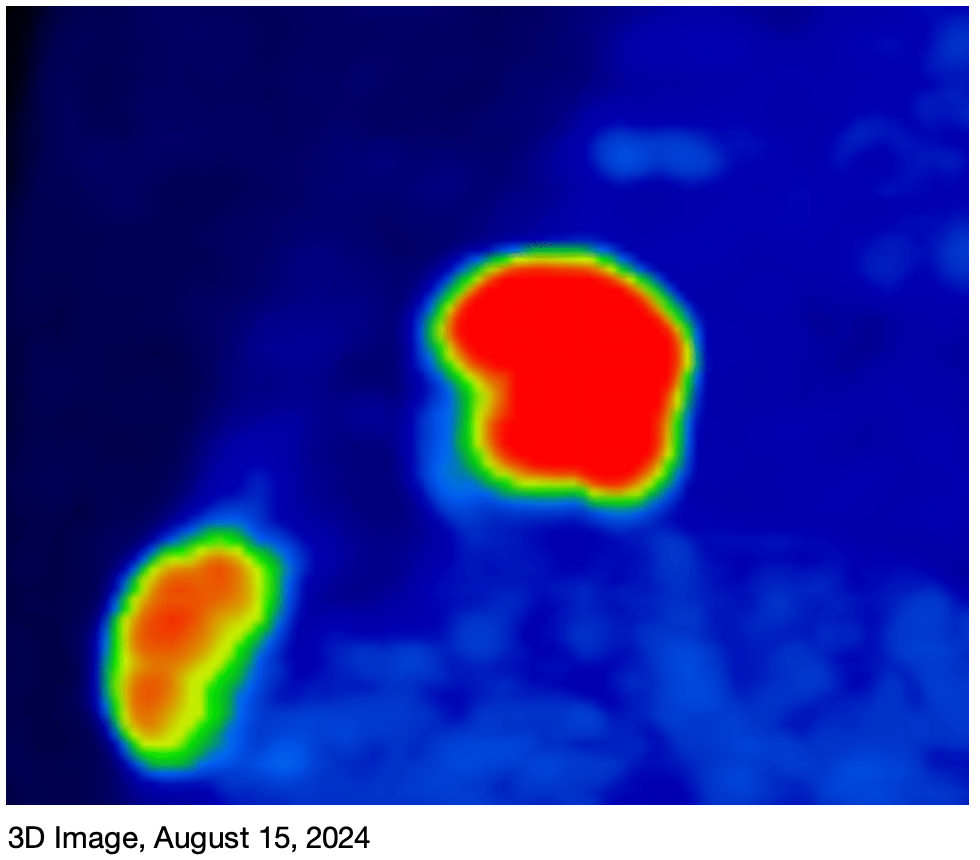
While not gone, the size of the lung tumor is much reduced. The chemo agents will continue to work for a few more weeks, and the immunotherapy will take care of the rest. Prognosis remains good!While some concentration of sugars is apparent at the rib site, my oncologist said the rib tumor is essentially gone.A 3D image, before and after for both tumors. The rib tumor is essentially gone. Technically, the dimensions of the lung tumor is a little smaller, but you can see that the tumor is much narrower and smaller by mass.
Earlier this morning, we met with our oncologist, and he was very happy with the results! There is some of the lung tumor left, but the rib tumor is essentially gone. He said we won’t need to do any more chemo, but we will continue with the immunotherapy. Even though we’re all done with chemo, it will actually continue to work for a few more weeks.
Since immunotherapy is so new, it’s not really known how long it we will use it. The initial studies were done for 2 years, so he’s saying we’ll potentially go for 2 years, but he also said there’s a good chance we’ll stop early, depending on how things go. I’ll get another PET scan in March to see how things are going.
So the news is good! I still have limited lung capacity, which I’m looking forward to getting over, but I’m steadily improving if slowly. My visits to physical therapy are producing improvements to my posture and strength too.
Thanks for your continued prayers! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
This is a note about the current Avian Flu epidemic spreading among poultry and dairy farms in the US, and which has been in the news in the last few days.
In the last few years, an H5N1 strain of the flu has been spreading among commercial poultry and even dairy farms, causing a lot of trouble for farmers, including the culling of animals. According to the CDC, 66 humans have been infected in the US during this same time period. So far, all of these people were infected because of close contact with birds or cattle. There is still no human to human transmission.
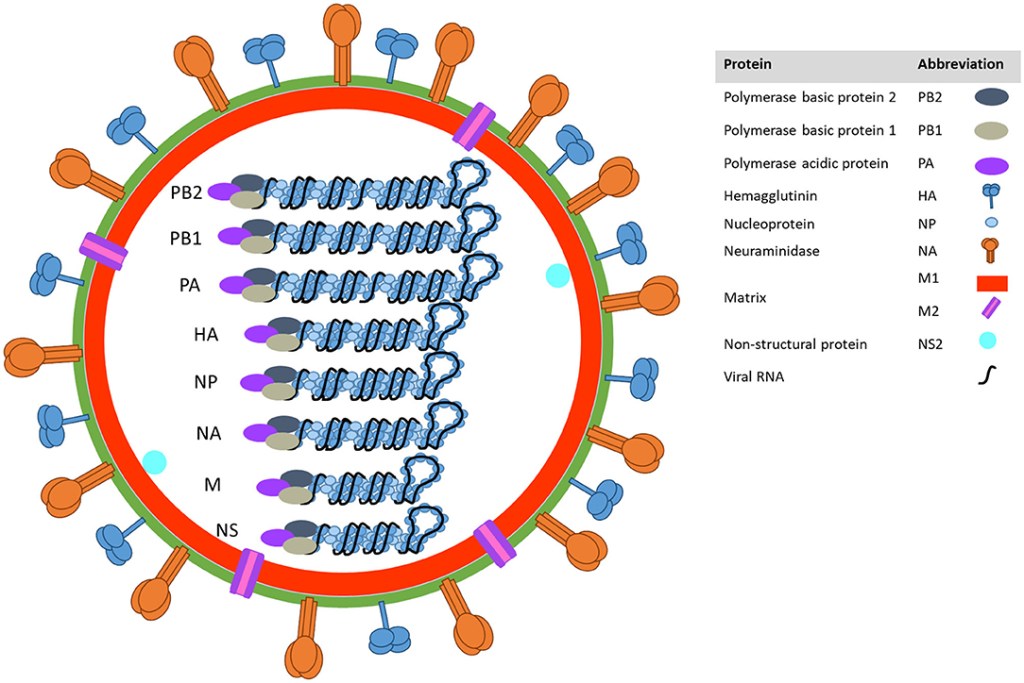
The reason avian influenza is in the news right now is that there is a case of severe disease in a human in Louisiana. DNA sequencing has been done on the strain in this case, and it appears that there was significant mutation that occurred in the infected individual. Mutation in a human host makes it more likely that the new strain may be able to infect other humans directly. The mutations were in the Hemagglutinin protein, the protein from which the H in H5N1 is derived.
Structure of the Influenza Virus. Hemagglutinin and Neuraminidase are surface proteins that mediate infection in animal cells. These proteins are when the H and N designations come from in H5N1.
Again I want to be clear that no human to human transmission has been detected as of yet, so there is not yet any need to go into COVID mode! However, if you work with poultry or cattle, you should be more cautious. Wash your hands regularly, and make sure fluids from your animals stay out of your mouth, nose or eyes. This includes milk! If you drink raw milk, make sure you are getting your milk from a source that performs regular testing for flu. Also, if you have back yard chickens, you should limit your birds’ contact with wild birds by keeping them in a coup with a roof, even one made of wire is fine.
As usual, make sure chicken products are cooked thoroughly before consumption.
There has also been a significant number of cases in house cats. If you can keep your house cat indoors, it might be a good idea to do that until things die down.
The State of California has declared a state of emergency regarding this flu outbreak. My opinion is that this is premature, since we still don’t have human to human transmission. I will continue to monitor the situation, and will let you know if more concern is warranted.
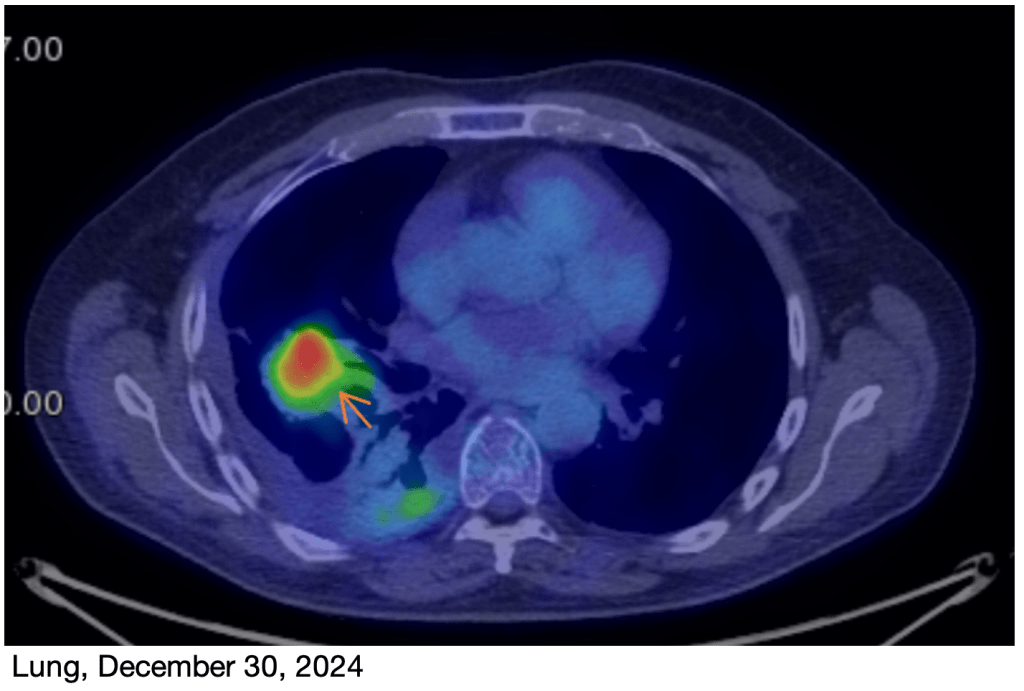
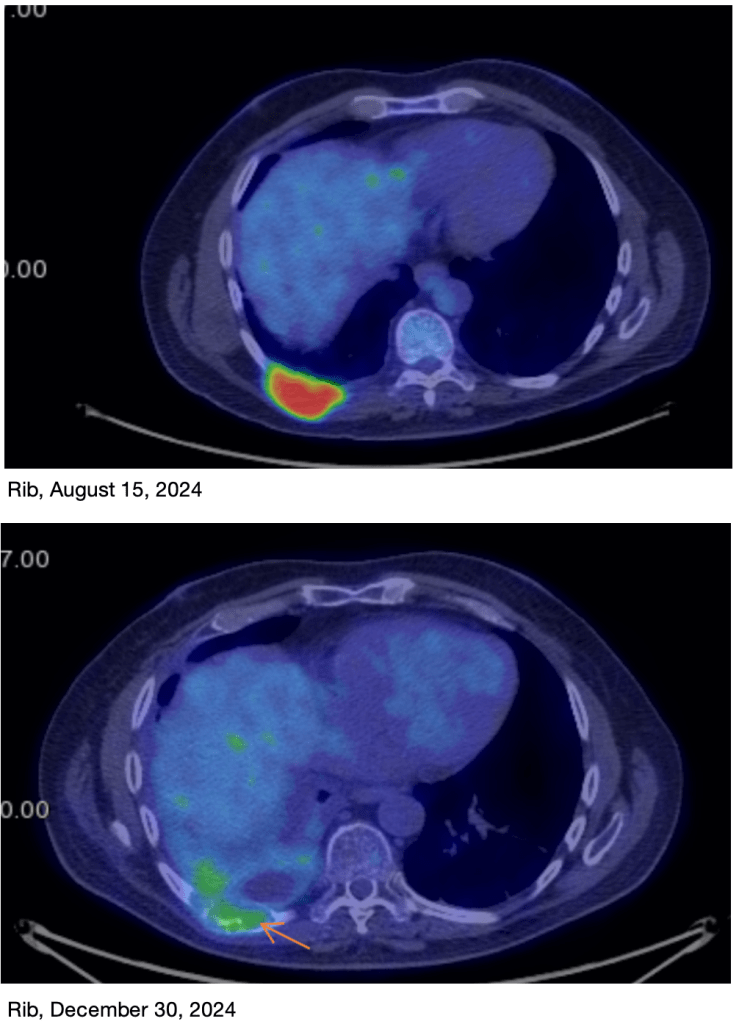
Last week was probably my last hard week after an infusion, as I probably won’t have another chemo infusion! So to extend my analogy from my “Wednesday” post, it’s now “Friday”! I should be feeling better from here on out. My chemo oncologist also said no more immunotherapy until they see the results from my PET scan on December 30th, so I get a nice little Christmas vacation from my immunotherapy too! My next update will probably be after the 30th, letting you know my PET scan results.
I was pretty sleepy this time, and my fatigue from chemo my have been compounded by the immunotherapy. There are other potential side effects from immunotherapy, but happily, I didn’t really experience any of those. The sleepiness just lasted a few extra days.
I had an appointment with my physical therapist for the first time in many months. I had a laundry list of things to work on, and it will take us a while to work through them all. I lost significant strength and muscle mass while in the hospital, so I worked on a bunch of exercises primarily designed to improve my leg and core strength, and to improve my posture, which has gone funky since my hospital stay. I’ve gotten started on doing my exercises at home and I’m looking forward to improvement.
Strengthening my upper back musclesThis looks like a wall sit, but it’s mostly for working on my posture.
Please continue to pray for improved lung capacity. I’m still short of breath, meaning that my Vital Capacity, the volume of air that I can breathe if I exhale as much as I can, then inhale as much as I can, is still lower than it should be, and I have to take more breaths when I go for a walk.
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
This is a cancer update. Yesterday I had my last of 4 expected chemo infusions, and my first of many immunotherapy infusions. I mentioned before that I take an anti-side effect medication for the first weekend, but I’ll be fatigued for some of next week. There may also be some additional side effects from the immunotherapy, Keytruda.
I’ve been very cautious about getting sick up until now, since I didn’t want to have to postpone treatments. But after next week, I’ll probably start being more free to “move about the cabin” as it were.
Writing this very blog, earlier today! Broose and his wife Penny bought me this sweet chair, which practically dumps me out of the chair if I want. Super comfy!
This last round has not been without drama. On the Sunday right after my last infusion, I passed out twice within a few minutes of each other. I was probably only out for a few seconds both times. I ended up going to the ER but my visit there was actually pretty uneventful. They couldn’t really find anything, and said it was pretty much just the chemo. So Kathy took me home after a few hours, and I’ll just need to remember to get low right away if I get lightheaded again. We’re always thankful when they don’t admit me!
My chemo side effects have been quite mild, which I’ve been very happy about. I threw up a lot after the first infusion, but not the others, which is great. I have another kind of amusing side effect of chemo that I’ve never been aware of. My skin is shedding a lot, kind of like full body dandruff! Kathy jokes that it’s like having her own personal snow globe! Every time I change my clothes, there’s a flurry of “snow” as I fold them! Kathy even says that I look younger with reduced age spots! And no, I don’t recommend this method of exfoliation! Anyone else have this side effect?
After a low weight of 165 lbs, I’m back up to 180, which is great. I’m going to take a little pause from the weight gain until I can start meeting with my physical therapist on the 16th. My target weight is 190 to 195, and I want to put on some muscle instead of fat! So I’m cutting back from 2 bowls of ice cream a day to just one!! Favorites are Mint Chip, Mocha, and Cherry from Tillamook. This is just an interesting detail. Please don’t leave a bunch of ice cream on my porch!
A little detail about my daily life is that we love Gospel music and I’ve have fallen into the habit of waking up to “You are the Living Word” and “Give Me a Clean Heart” by Fred Hammond. They’re great songs, with great bass lines, of course. I try and get out of bed before the first one is over!
Back to the medical side, my prognosis remains good and my tumors are shrinking faster than anticipated. I’ll get a PET-scan on the 30th. For this test, I have radioactive sugar injected, then wait 45 minutes for the cancer cells to suck it up. Cancer cells love sugar, and quickly absorb the radiolabeled glucose. Then I get scanned in a specialized scanner and see how the tumors look. PET scans are the most sensitive way to detect tumors and allow doctors to see even small tumors wherever they are. My chemo oncologist expects that my rib tumor will already be completely gone, and that my primary lung tumor will be much reduced. The chemo will continue working for awhile, and the immunotherapy will continue for to up to 2 years!
A word on immunotherapy. As mentioned in Update 7, immunotherapy agents cause T and B cells to attack tumor cells. Some tumor cells express a surface protein called PD-L1. This protein causes the immune system to see the tumor as “self” by binding to the PD-1 protein on T and B cells. Keytruda stops these proteins from binding to each other, causing the T and B cells to see the tumor as alien. Unfortunately, this can cause some normal cells to appear alien as well, leading to some side effects. My autoimmune disease is not expected to be impacted by all this, but I’ll need to be monitored to make sure. My oncologist says that since my tumors have a lot of PD-L1, this therapy may work especially well on my tumors. Depending on how I respond, I may end up being on Keytruda for up to 2 years!!
Please continue to pray that my tumors will become normal lung tissue and not scar tissue. I’ve also had some shortness of breath for the last 2 weeks, but I’ve seen some improvement over the last few days. Pray that my lung capacity improves!
Merry Christmas and Happy Hanukkah, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.