This post is about the over the counter Antigen tests that a lot of us have used in the last few months, and whether they really work.
As we’ve discussed, BA.5 is re-infecting lots of people, even those who’ve had Omicron just a few months ago. Those with recent cases generally have a mild case the second time around, even with BA.5
I just got back from summer camp with a bunch of high school students. I knew I could get COVID again, but since I had Omicron in January, I figured I’d be OK, even if I got BA.5. One of our counselors got sick while we were there, and tested negative for COVID, with an antigen test. I got sick on Sunday morning, after we were back, and also tested negative for COVID using an antigen test. On Sunday I just had a sore throat, Monday and Tuesday morning I had fatigue, sore throat, and just a little coughing. My sore throat felt very similar to the one I had in January, kind of like a weird heart burn, so I tested myself again on Monday. Still negative.
Meanwhile, the other counselor tested negative again when he got home, but then tested positive after that. His wife too. So he had 2 negative tests before testing positive.
So did I have COVID again? I still don’t know. I’m at the “just getting over a cold” stage right now and am feeling pretty normal. I had 2 negative tests and I’m not going to test myself again.
Doing a good scientific study is a slow process, and we’re probably unlikely to get good scientific articles on how well the antigen tests work for every new variant. The only articles I could find on BA.5 and antigen tests were from Slate and CNET. I usually don’t bother to read popular level articles on COVID since journalists often get things wrong, but that’s all we have. Both basically say that yes, they work, but you may need to take several tests. Well, that’s kind of like saying they don’t work very well.
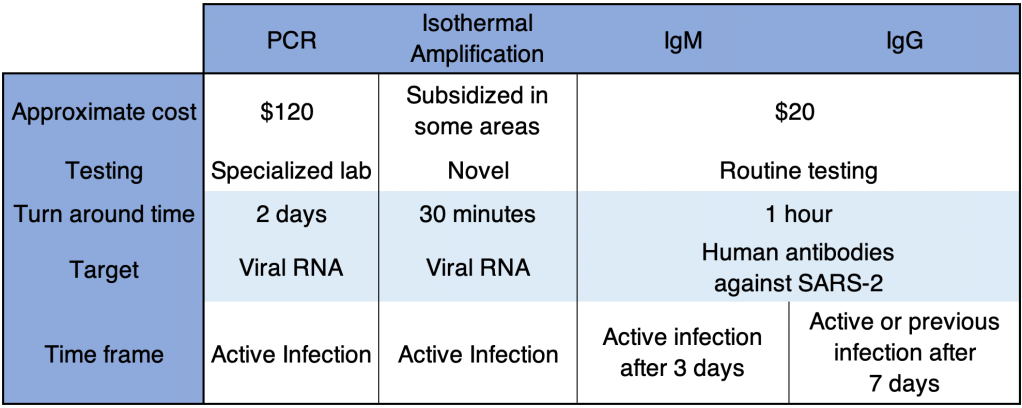
How Antigen tests work: There are 2 kinds of tests that use antibodies for testing. One is an Antibody test. This kind of test looks for human antibodies against SARS-2 proteins. It actually determines whether you’ve been infected at some point in the past. IgM antibodies appear after a few days and persist for about a week. IgG antibodies appear after about a week and persist for weeks or months. So a positive SARS IgM tests says you basically have COVID right now, while a positive IgG test you have it now, or had it weeks or months ago. An IgG test is not useful if you want to know if you have COVID now.
An Antigen test detects actual SARS-2 proteins. They usually detect the Nucleocapsid protein (N), a protein on the inside of the virus which does not mutate rapidly. In theory, these tests should work well even if the Spike protein changes, which is by far the most common changes in new variants. They are not usually thoroughly tested with each new variant.
The Slate article suggests the tests may not be working as well because the BA.5 variant may not be as present in the nostrils as previous variants. Scientists know that a Nasopharyngeal (back of the nose/throat) site is better, but patients far prefer a nostril test. So this may be why the tests are not working as well for BA.5.
Antigen tests are less sensitive than a PCR test, but they are far cheaper, faster, and easier to use, which is why they are so common now. If you really need to know if you have COVID, a PCR test is the way to go. I frankly am pretty disappointed that a clearly symptomatic person can test negative for COVID right now with an Antigen test.
All this to say, if you have cold-like symptoms in the next few weeks, you’re better off staying at home and laying low for a few days, even if you have a negative Antigen test. You may actually have COVID.
Happily, if I indeed have COVID now, it’s a very mild case.
In yesterday’s post, I outlined some of the factors that resulted in the very high COVID case rate in the US. Today I will discuss how we can prepare for the next pandemic.
I have a PhD in molecular biology, and I specialize in infectious disease testing. I am not a physician or epidemiologist. I have an informed but not expert opinion.
Identifying the threat:
First, most new infectious diseases do not pose a global threat. SARS-2 was so dangerous because of its high infectivity, long incubation time, and asymptomatic spread. Most diseases do not have these parameters. Whenever a new disease comes around, and they will, we should soberly and cautiously assess the real threat. Coming to the wrong conclusions about the threat will lead to the wrong conclusions about combating it.
There have been several important new infectious disease outbreaks in the last few years, including Hantavirus (1993), SARS (2003), Avian Influenza (2004), H1N1 Swine Flu (2009), Ebola (2013), Zika (2015), and of course HIV in the 80s. They all have different disease parameters which make them behave very differently. Most of these diseases did not have global impact. The first SARS for example was much less infectious than SARS-2, but much deadlier, so it was contained quickly and didn’t spread much beyond Asia. HIV can be spread by asymptomatic victims for a full 8-10 years, avoids the immune system, and evades vaccination efforts, so it has become endemic in much of the world.
The following parameters determine how a new disease will behave:
Mechanism of spread
Infectivity
Asymptomatic/ambulatory spread – can the victim walk around and spread disease?
Incubation period
Fatality rate
Vector – what carries the virus to a new host
Non-human reservoir – diseases that come from non-humans are harder to control and cannot be eradicated.
Obviously, we cannot respond to different diseases in the same way. Part of the reason we failed to contain the virus was that we used measures that were designed for viruses that spread by droplet transmission against a virus that spreads through aerosol transmission. Using the wrong measures was less effective.
Much of my concern with the SARS-2 virus was the Antibody Dependent Enhancement issue, which is very uncommon among viruses, so is not usually a concern.
Be cautious. Whenever a new threat arises, it is wise to be extra cautious until information can be gathered. Although many of our precautions turned out to be unnecessary, I still support taking extra precautions early on. Remember that early estimates were that the fatality rate for COVID was 3.68%. With the 82 million confirmed cases in the US, this would have been over 3 million deaths if the fatality rate had really been this high. As it stands, we have had almost 1 million COVID related deaths, a death rate of approximately 1.2%. Yes, I know we can debate how many of these are deaths really resulted from COVID and how many infections there really were. But we cannot discount that COVID had an enormous impact.
What if COVID were deadlier? Or what if it had selectively killed children, or caused more long-term symptoms like polio did? Things would have been much different.
All this to say, I think caution was warranted in the beginning of COVID, and we should continue to be cautious in future pandemics. On the other hand, we should also learn to abandon precautions that are not effective. Maintaining ineffective precautions wastes resources, causes extra economic and social suffering, and causes people to lose confidence in government agencies. It started to become clear to me by May of 2020 that lockdowns were ineffective, and that transmission was happening mostly indoors, but I still see people wearing masks outside to this very day.
Persuasion, not coercion: From the beginning of the pandemic, public communication was terrible. Official guidelines were confusing and often contradictory. Far worse, explanation or evidence was rarely given for policies. Instead, disagreement was met with accusations of being anti-science, rather than persuasion. This approach contributed to the loss in confidence in official channels.
Going forward, officials need far better communication skills when dealing with emergencies. Give evidence rather name-calling, and respect the population enough to tell the whole truth.
Then came the vaccine mandates. Many people I know were coerced into getting vaccinated against their will, and many others were fired. All at a time when information about the vaccines was being hidden from the public. This is unacceptable, and no way to run an emergency.
Restoring Trust: Both the CDC and FDA hid information from the public. In order to restore confidence, senior leadership needs to be replaced and new leadership should explain how things will be better in the future. Is likely to happen? No, it is not.
Government agencies need to be far more transparent. Lack of transparency forces people to wonder what is going on, and create their own theories. Government agencies often decry conspiracy theories, but they had a big role in creating them.
Misinformation: Freedom of speech, censorship, and misinformation had a major role in the public discussion over the pandemic. Doctors and scientists were frequently censored, shunned, or fired for sharing ideas that went against WHO or CDC guidelines. This includes ideas like the lab leak hypothesis that later turned out to be likely.
Freedom of speech is a foundational principle of American life. It’s in our DNA, as some would say. We are not America without it. Some will say that too much freedom of speech leads to misinformation and conspiracy theories. While it’s true that this freedom allows the spread of falsehoods, it also allows all ideas to be debated, true ideas to be raised up, and false ideas to be discredited. Freedom of speech is the solution to misinformation, not the cause. Most of the leaders in world history that wanted to control freedom of speech had something to hide. It is essential that we maintain this basic right.
State emergency powers: As discussed in yesterday’s post, the US federal government has surprisingly little power to deal with a public health crisis. The CDC can develop guidelines, but most of the real work is done at the state and local level. State officials need to step up and realize it’s their responsibility to respond well. Citizens need to hold state and local officials accountable.
Manufacturing: The US needs to maintain manufacturing capacity for certain essential items like personal protective equipment, testing kits and equipment, and medications. Tax incentives need to exist to encourage companies not to send these functions overseas.
In addition, we should have national and state stockpiles of certain equipment. I know many hospitals and labs are now creating stockpiles of their own.
Testing: Most countries that did well produced lots of COVID testing early. In the US, the CDC tried to manage all the testing themselves, and quickly became overwhelmed. By the time private labs were allowed to develop their own tests, it was way too late. Testing capacity didn’t become nearly adequate until at least July of 2020. Next time, the CDC needs to allow testing by private labs right away. Ideally, anyone who wants a test and anyone potentially exposed to an agent should be tested.
Quarantine, not Lockdown: Countries that did well did not quarantine healthy individuals, although some of these countries had more restrictions during the big Winter waves. Instead, only COVID positive people should be quarantined. This is only effective when tests are readily available.
Later in the pandemic, some outlets acknowledged that most infections were happening in private settings. Basically, people would get infected outside, then bring COVID home to infect everyone in the household.
Here is a very interesting video using computer models to show why our model of lockdown was not effective. Computer models are only as good as they are programmed to be, so this is only for demonstration purposes, and is not data.
Contact tracing: Contact tracing was very successful in some countries, but the long incubation time of COVID made this difficult. Successful programs involved tracking of individuals by cell phone and credit card data, practices that would probably not be tolerated in the US. Such programs would need to be voluntary to not trigger the creepiness factor and violate constitutional rights.
Masking: I was a big proponent of wearing a medical grade respirator (N95, KN95, or KN94) indoors during the pandemic. Because COVID spread as an aerosol as well as droplet form, cloth and blue surgical masks were ineffective. Simpler masks can be effective against colds and flu, however. So the choice of mask depends on the agent in question. CDC guidelines need to reflect the method of spread of the agent in question.
So what should Dr. Fauci have said early on? Something like this:
“N95 masks offer the best protection against infection by the SARS-2 virus. However, our current supply is very low, and we desperately need to save these masks for our medical professionals. Please do not purchase N95 masks at this time. In the mean time, there are some options that will help reduce the risk…”
In actuality, of course, I didn’t see an N95 in a store from March 2020 until at least February of 2021, so I couldn’t have bought one if I’d wanted to!
Treatment: Most medical facilities in the US didn’t treat COVID until a patient was experiencing respiratory distress. By then, treatment options were limited. To their credit, intubation was largely abandoned by the medical community when it was learned that this treatment was largely ineffective.
However, controversy swirled over potential treatments that became disfavored by the medical community. Doctors are usually granted the right to prescribe “off label” medications, meaning they can use medications for treatments outside the guidelines of the manufacturer. But drugs like Hydroxychloroquine, Ivermectin, and others quickly become forbidden, and some doctors even got fired for prescribing them. Research on these drugs were minimal.
I am not arguing here that these drugs are effective against COVID. I’m simply saying that forbidding doctors from working with or publishing papers about these drugs was a big mistake. While it is of course wise for a doctor to consider guidelines, treating a novel virus may require some “outside the box” thinking.
Let me know in the comments if I missed something important!
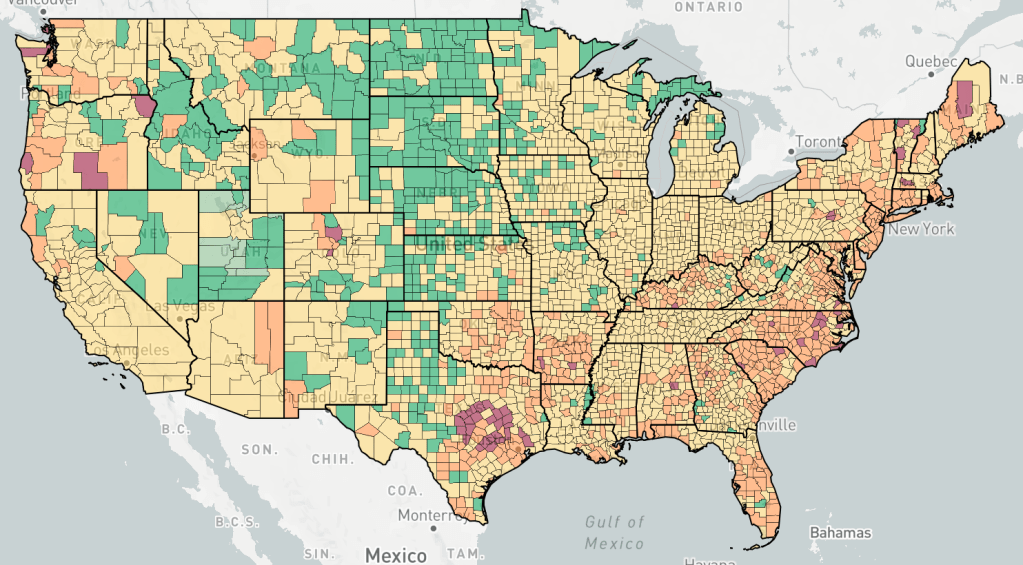
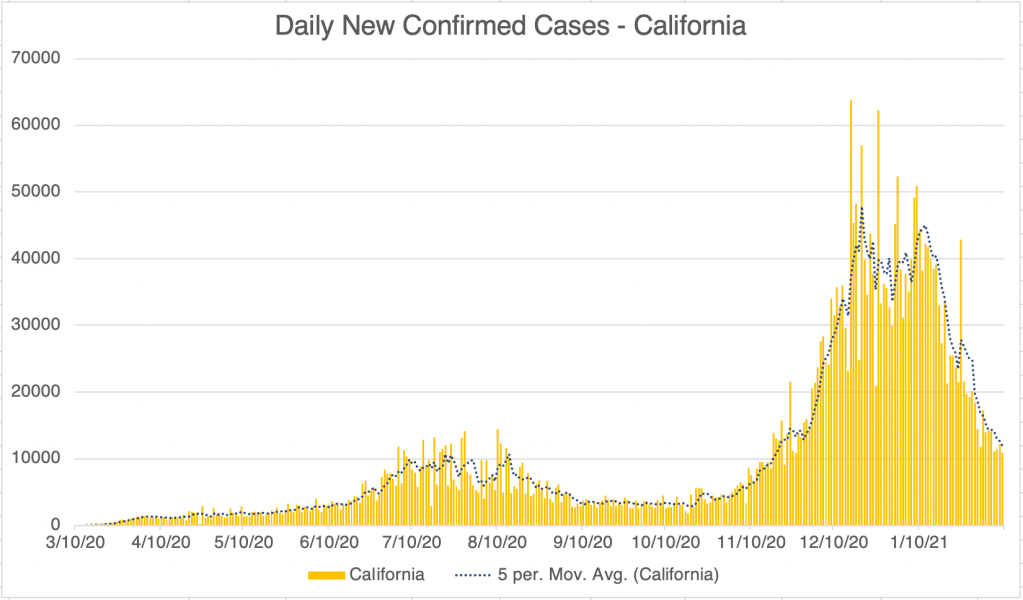
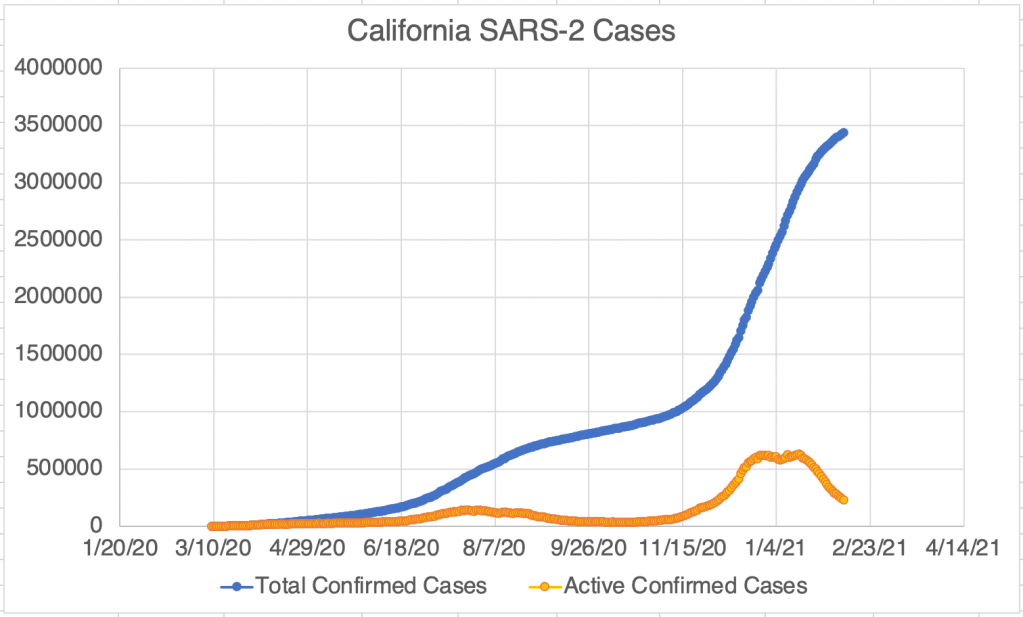
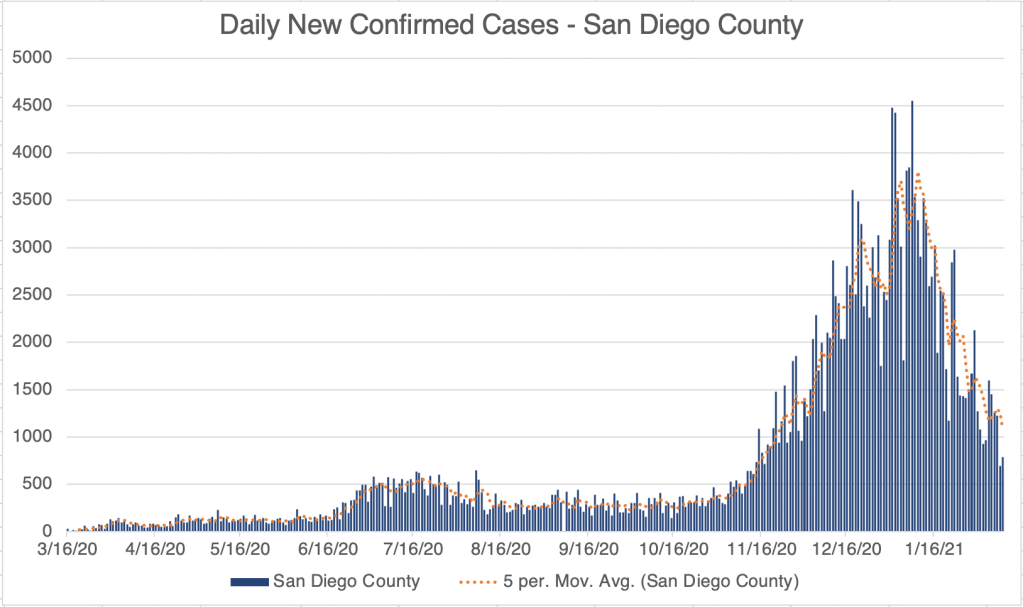
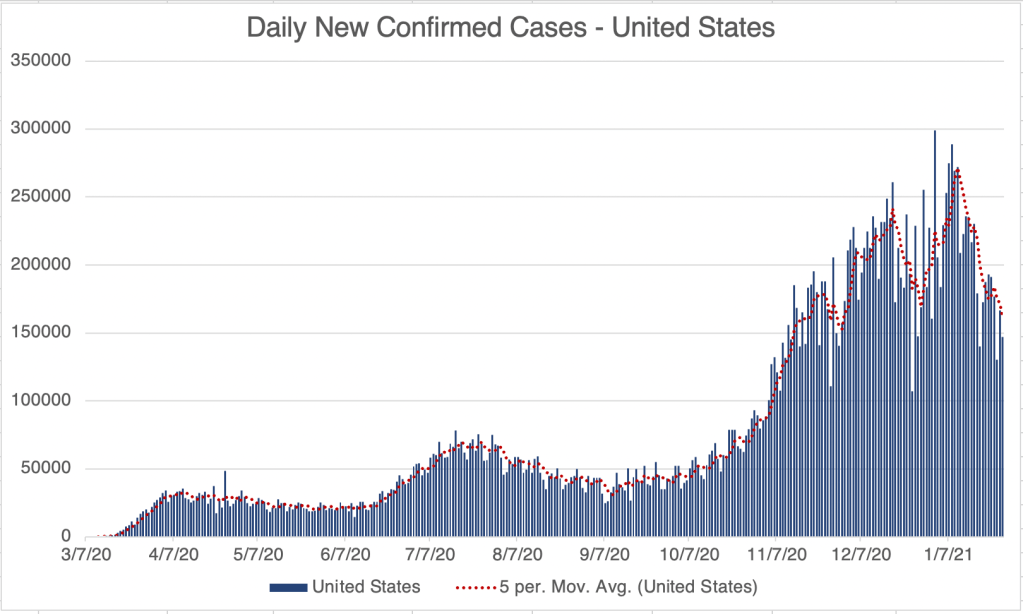
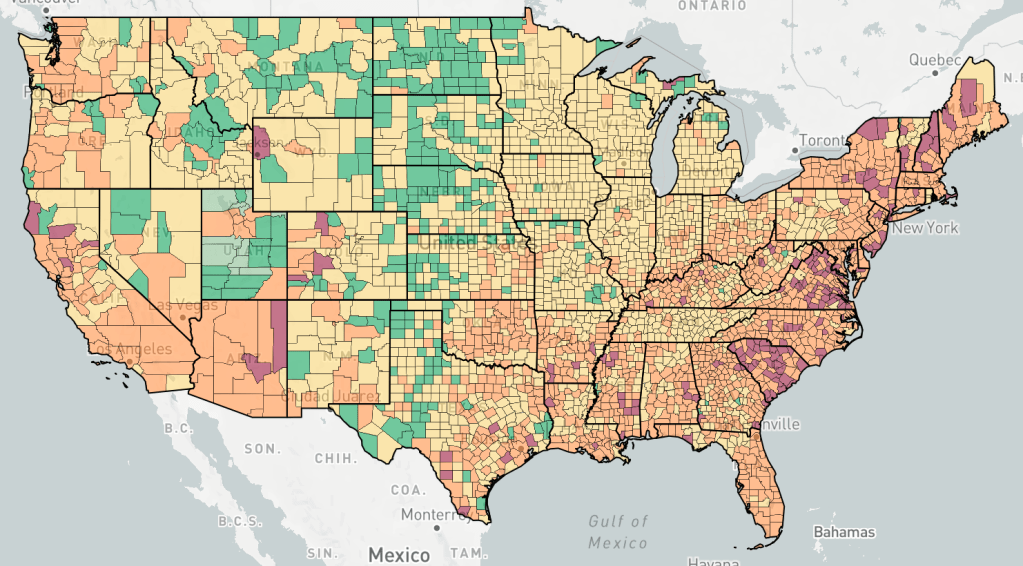
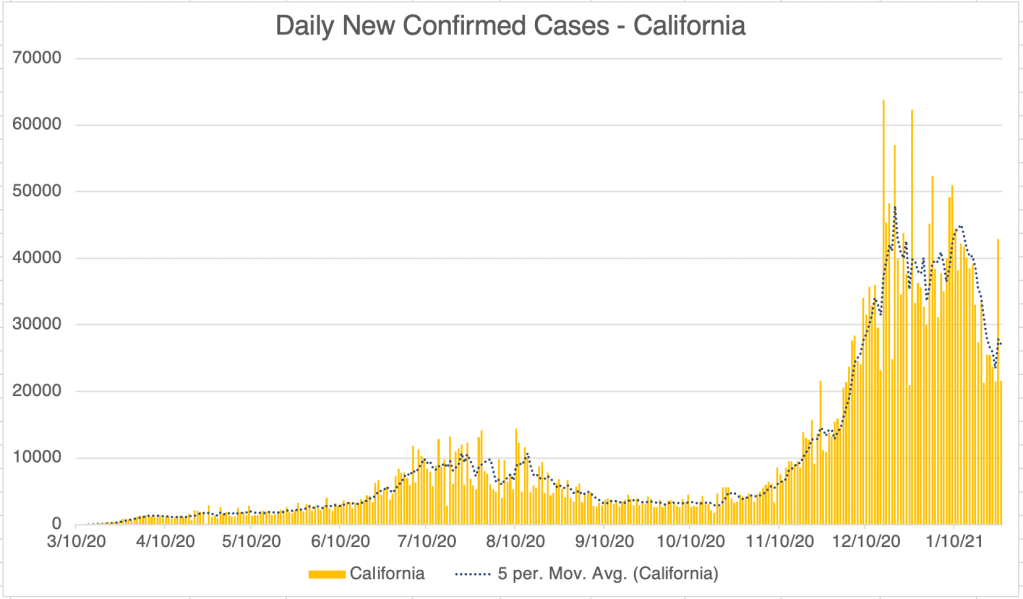
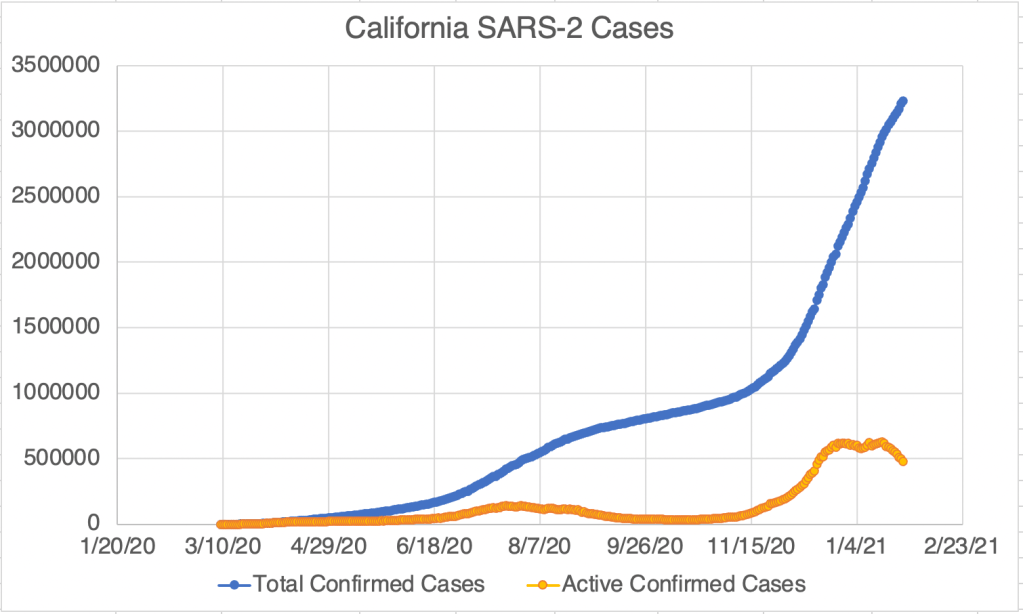
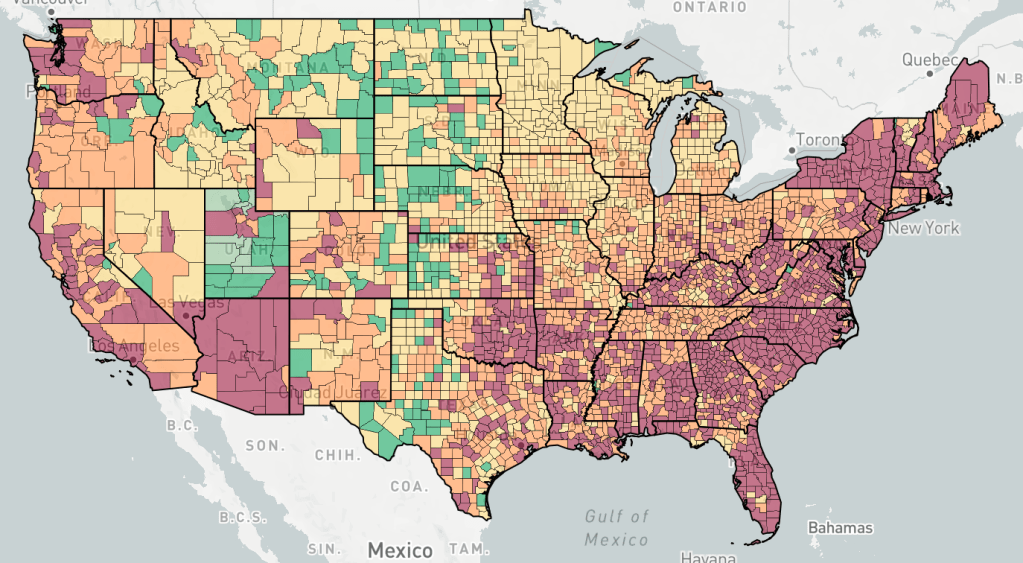
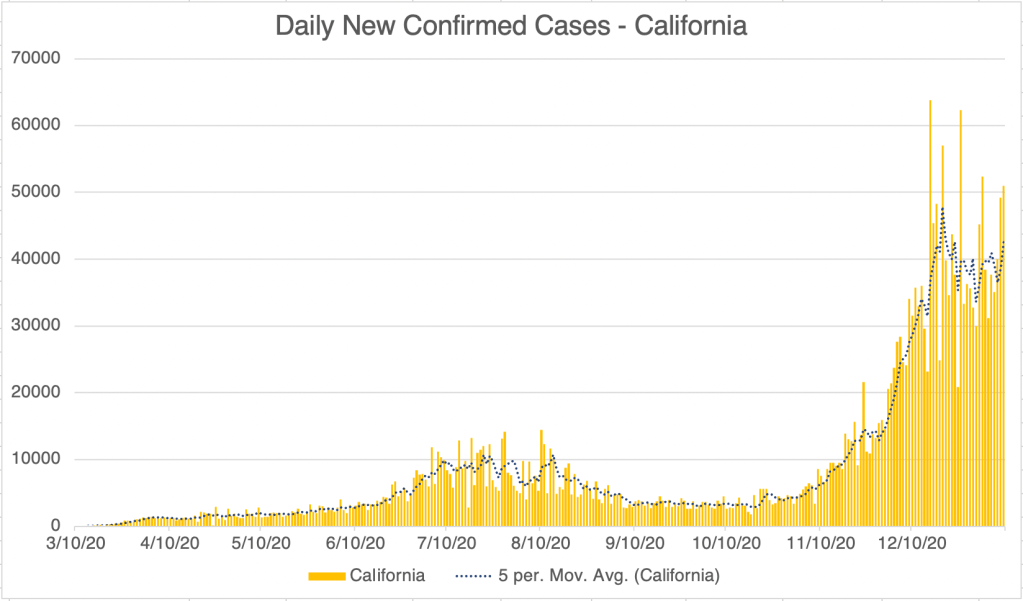
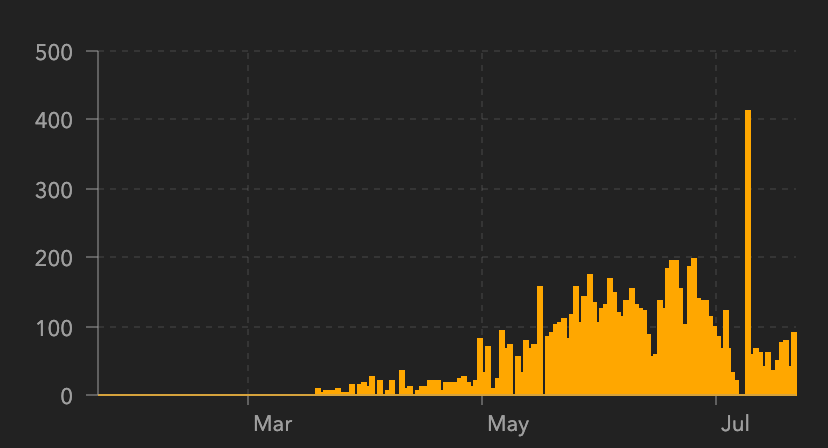
This is a case update. New case numbers continue to plummet for the US, California, and San Diego County. New case numbers are now similar to those in early November. Obviously, the number are still not zero, so we still have work to do, but we have good news. As an interesting side note, the endcoronavirus map of new cases reveals a little pocket of new cases spreading out from Austin, Texas! Other parts of the country are generally improving, and the central part of the country is doing particularly well.
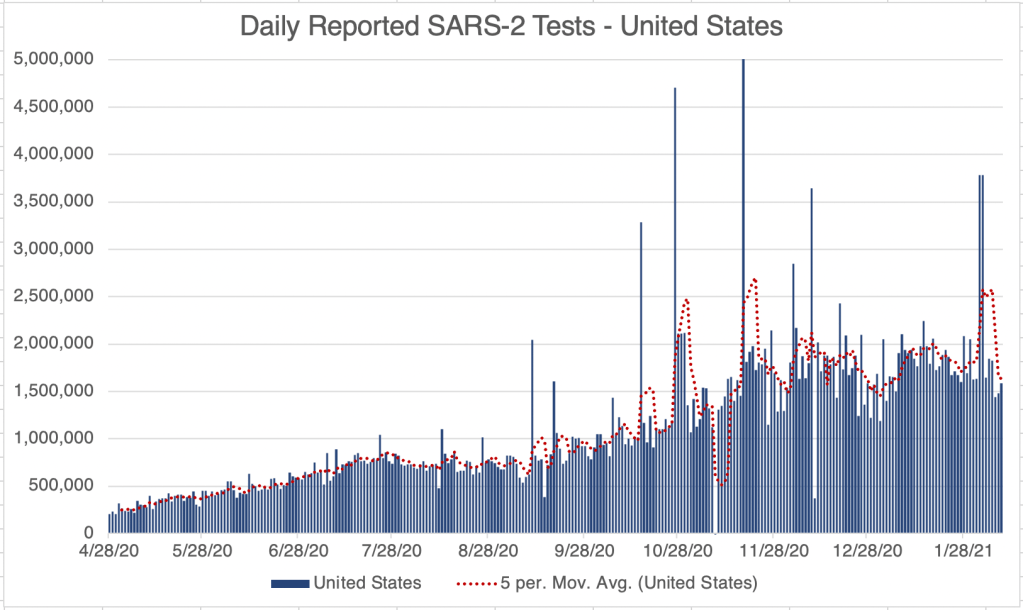
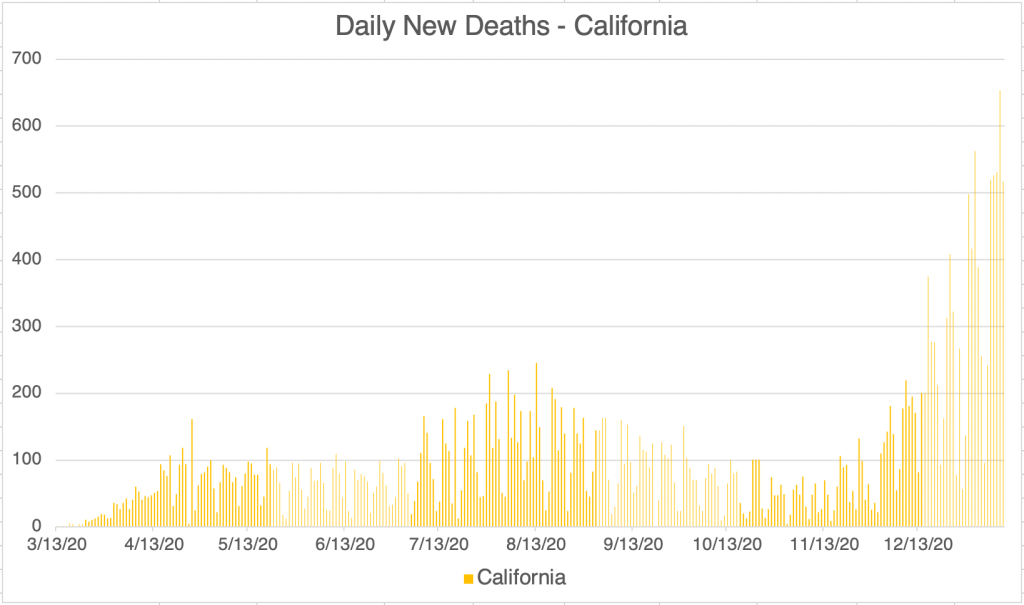
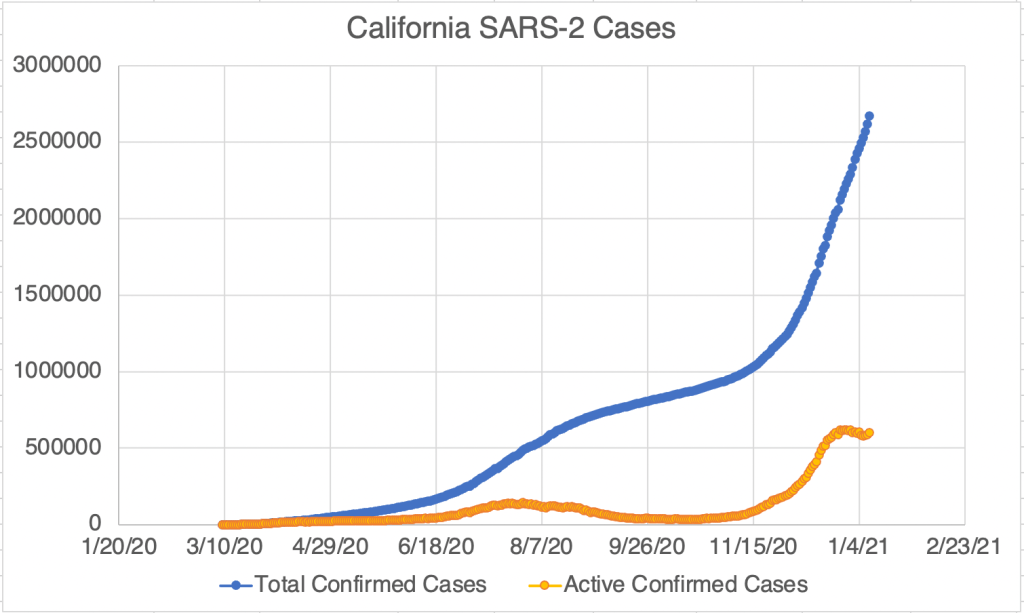
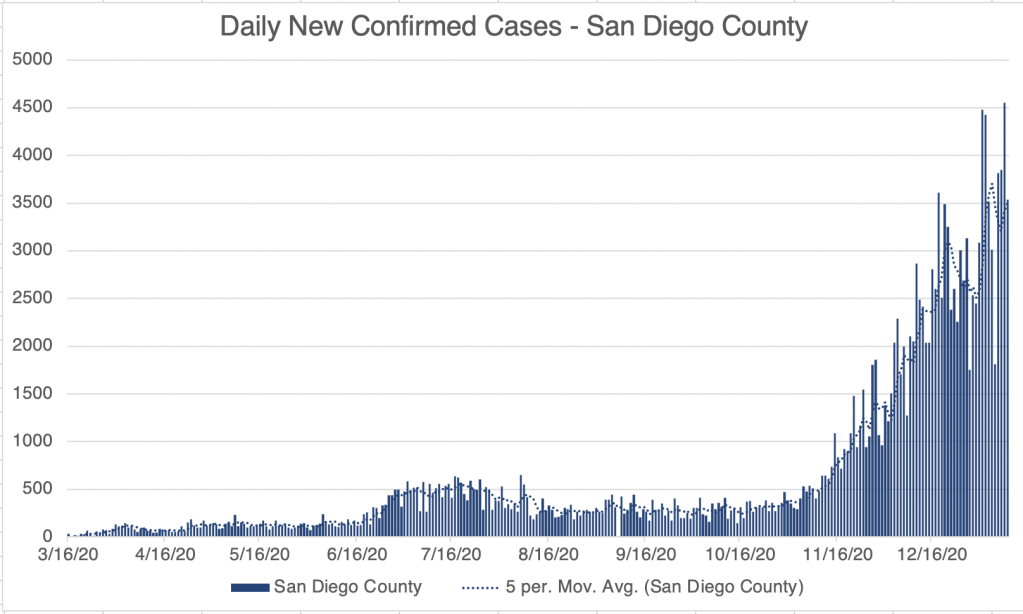
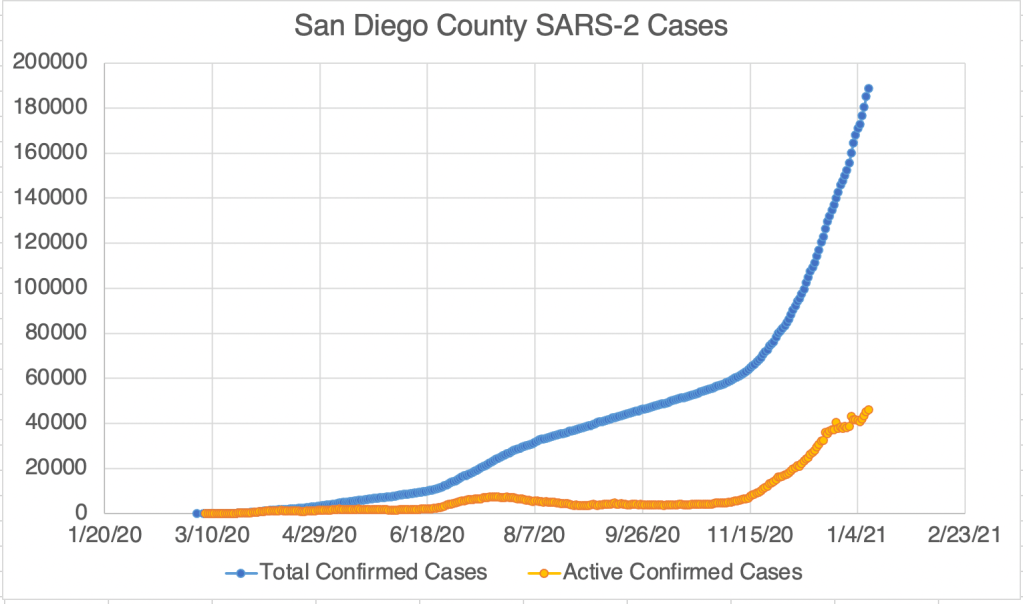
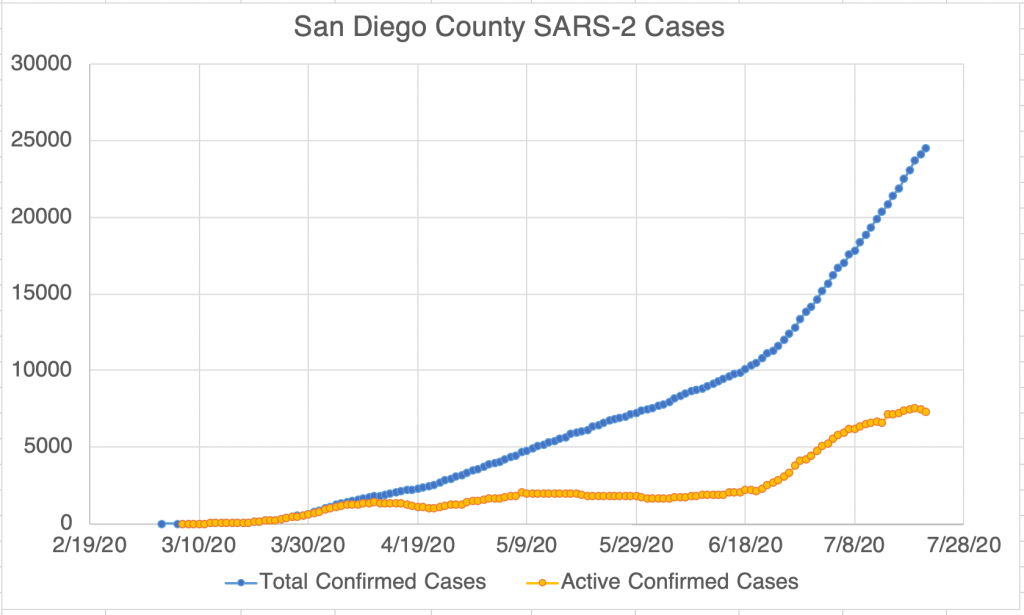
Graph is by me, from data collected from Johns Hopkins University COVID site.Endcoronavirus County Level Map, February 10th, 2021Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from Johns Hopkins University COVID site. “Active Confirmed Cases” numbers are calculated based on the assumption that patients confirmed to have SARS-2 virus at least 17 days ago have recovered.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. “Active Confirmed Cases” numbers are calculated based on the assumption that patients confirmed to have SARS-2 virus at least 17 days ago have recovered.Graph is by me, from data collected from Johns Hopkins University COVID site. This graph shows reported tests. Laboratories are currently required to report both to the ordering physicians and also report positives (without identifying information) to the CDC as well as county and state public health. Some labs have been late reporting to public health, which is why you see some days which have either a very high or very low number of tests.
Of course, we just had the Superbowl, which I count as an American cultural holiday. We may have had some new infections associated with gathering in peoples homes. If so, we may start to see numbers coming up starting on Friday or Saturday. After Thanksgiving and Christmas, new cases started to increase a little less than a week afterward.
During the year, we’ve seen testing capacity come up slowly but steadily from just a few hundred a day when the CDC was trying to do all the testing themselves in March, to around 1.5 to 2 million per day in December ’20 and January ’21. Now that new cases are starting to come down, testing is just starting to head down as well. If you are a medical professional, especially in testing, you may begin to find it easier to buy pipette tips in the next month! We can only hope!
This is a case update. I’ll also briefly discuss some cases of anaphylactic shock in some vaccine recipients. The US, California, and San Diego County are all experiencing a continuing decrease in new confirmed cases! The center of the country seems to mostly have recovered from the 3rd wave according to endcoronavirus, and the coasts are improving as well.
Anaphylactic shock in some patients: According to Paul Offit, in a YouTube interview (at 2:30 in the linked video), a number of vaccine recipients have experienced anaphylactic shock after being vaccinated. All vaccines carry some risk of this phenomena, but the COVID vaccines appear to produce this at about 11x the rate of the flu vaccines. This is about 11 patients per 1 million vaccinations, about 0.0011%. Dr. Offit thinks this allergic reaction is likely caused by Poly Ethylene Glycol (PEG), a component of many vaccines, also used in many other products, including Dr. Pepper!
The good news is that anaphylaxis is easily treatable using an epi-pen. If you are prone to allergic reactions, let your provider know before getting the vaccine.
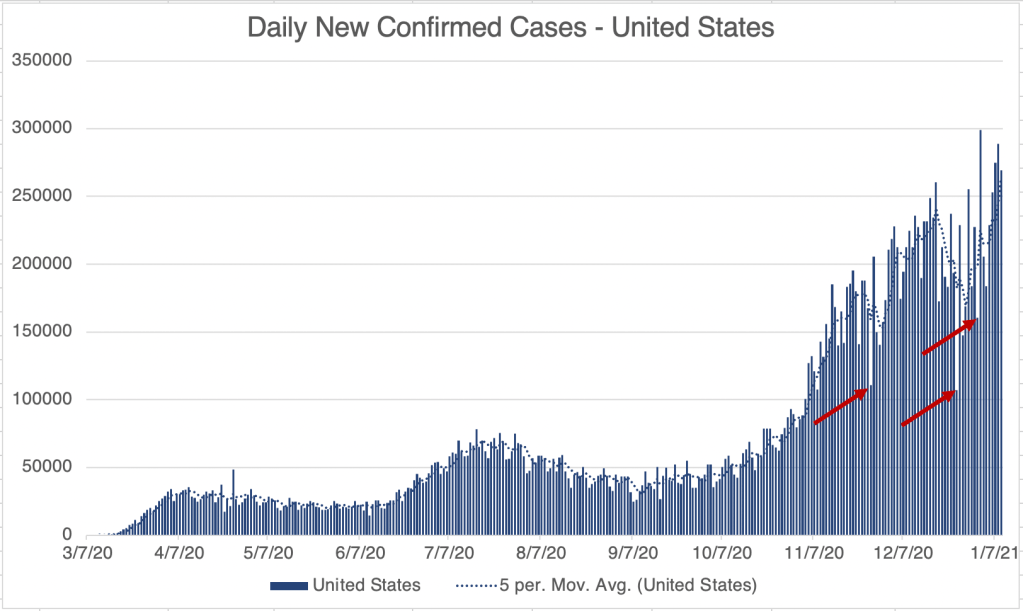
This is a case update. I’ll also briefly discuss some more new variants, and a testing equipment shortage. For the US, cases continue to increase. Day to day case rates have been very erratic for the past several weeks. This is partially because many testing facilities don’t report on holidays, so that there is an artificially low case number on holidays, and an artificially high case number the day after. The arrows in the case number graph for the US show Thanksgiving, Christmas, and New Years Day. Wave 3c, the wave starting after Christmas day, is still increasing in confirmed case numbers.
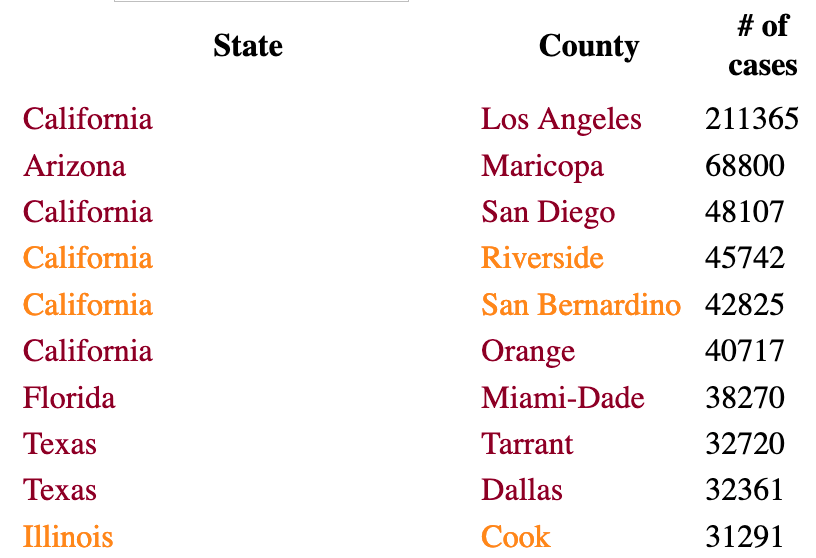
New cases continue to be focused in the East and Southwest. In particular, new case numbers have plateaued in California, but numbers are still quite high, with 4 of the top 5 counties being in California.
More new variants? I mentioned the new UK variant a few weeks ago. Since then, I’ve heard reports of new variants also arising in South Africa and Colorado. I don’t have much information on those yet, but the more people who are infected, the more likely a new strain will arise.
Equipment shortage. For those outside the medical community, just a little inside knowledge. The crisis has revealed many of the items that are limiting in our efforts to combat the virus. For the medical testing industry, many common materials have been very difficult to obtain, leading to long wait times for testing. There is a short supply of testing instruments, detection kits, RNA extraction machines, extraction kits, plastic plates used to contain testing reactions, and even plastic tips used to move small volumes of liquid in the lab. If you place an order of tips today, they may not arrive until April or May! This is part of the reason testing has been so slow and new labs difficult to start. I’m told that part of the issue is that there are only a few factories in the world that make medical plastics, and they are all overwhelmed. As a country, we’ll have to rethink our supply chain now and in the future.
Happily, there is some good news about the virus this week. For the US and California, the number of daily new cases suggests that for both regions, we may have hit a peak in new cases. Sunday or Monday is always the low number for the week, but the number of new cases on those days usually predicts the peak for the rest of the week. For both, this week’s low is near or below last week’s low, suggesting that the high for the week will be near or lower than the high for last week.
San Diego has been flat since early July. New cases aren’t going down yet, but they aren’t going up anymore either. In addition, the number of active cases in San Diego is probably going down, after a peak of almost 8000 active cases. Unfortunately, California overtook New York for the number of confirmed cases in the country this week, and LA County has the most new cases in the entire country, and has 40% of confirmed cases in California.
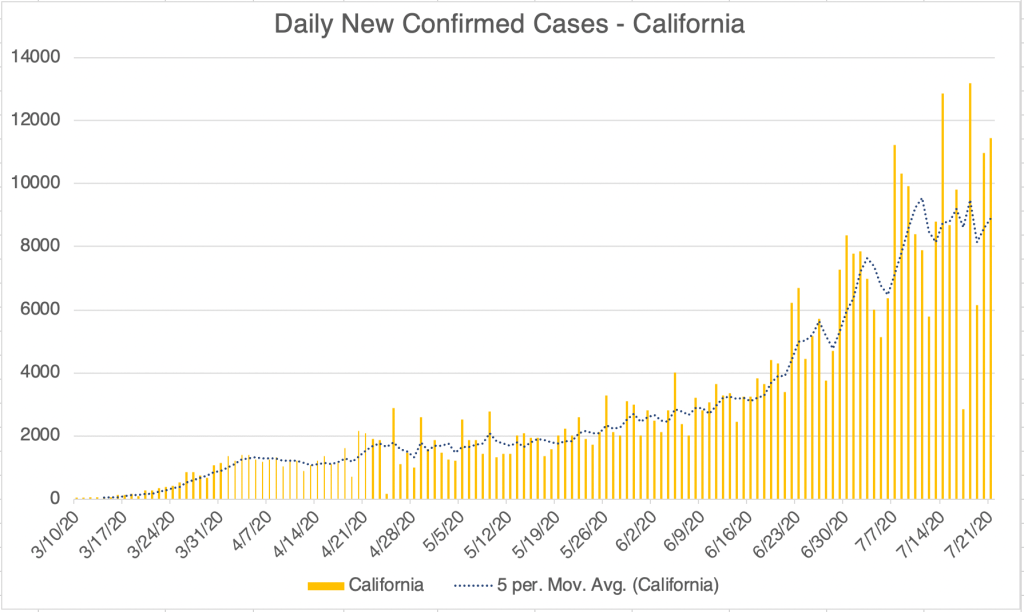
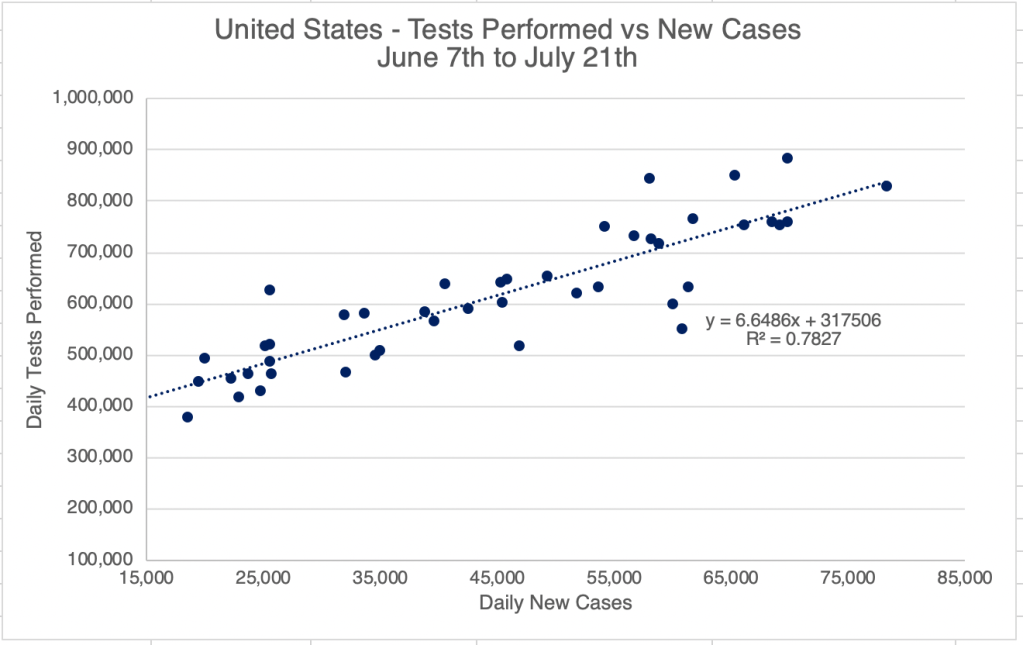
As we discussed in May 12thpost on new cases, comparing the number of tests and new cases can tell us if all the new cases are just related to new testing. An R2 number between 0.95 and 1.00 shows strong correlation, “proof” that two things are related. The tests vs cases for the US since early July give an R2 of 0.78. This suggests that though many of the cases are real, at least some are because of new testing. In California the R2 is 0.44, a much weaker relationship, meaning more of the new cases are not just due to more testing.
An R2 number of above 0.95 suggests good correlation, a number of 0.78 suggests that while there is a contribution from increased testing, some of the increase is real new cases. Graph is by me, from data collected from Johns Hopkins University COVID site.An R2 number of above 0.95 suggests good correlation, a number of 0.44 suggests that while there may be some contribution from increased testing, much of the increase is real new cases. Graph is by me, from data collected from Johns Hopkins University COVID site.
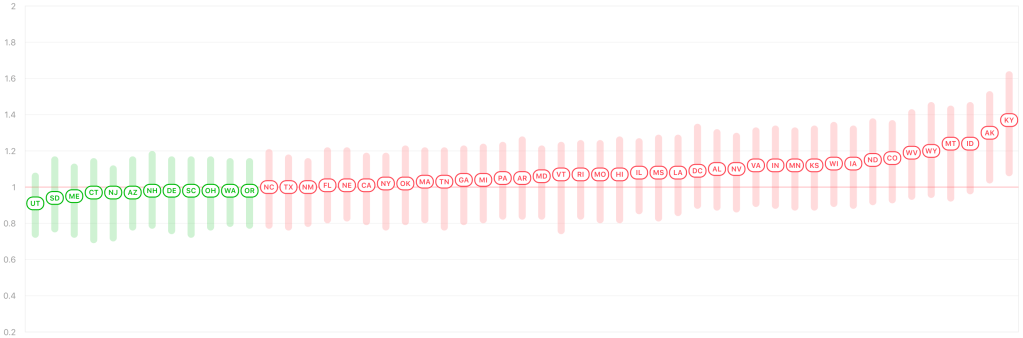
Rt Live shows that more states have an Rt number of less than 1.0, indicating that the virus is slowly going away in that state.
I have some African readers, so I’ll point out that the number of new cases appears to have peaked in Nigeria, DR Congo, Malawi, and South Africa, as well as in Brazil, a country which now has the 2nd highest number of confirmed cases, behind the US. Let’s hope we can keep this progress going!
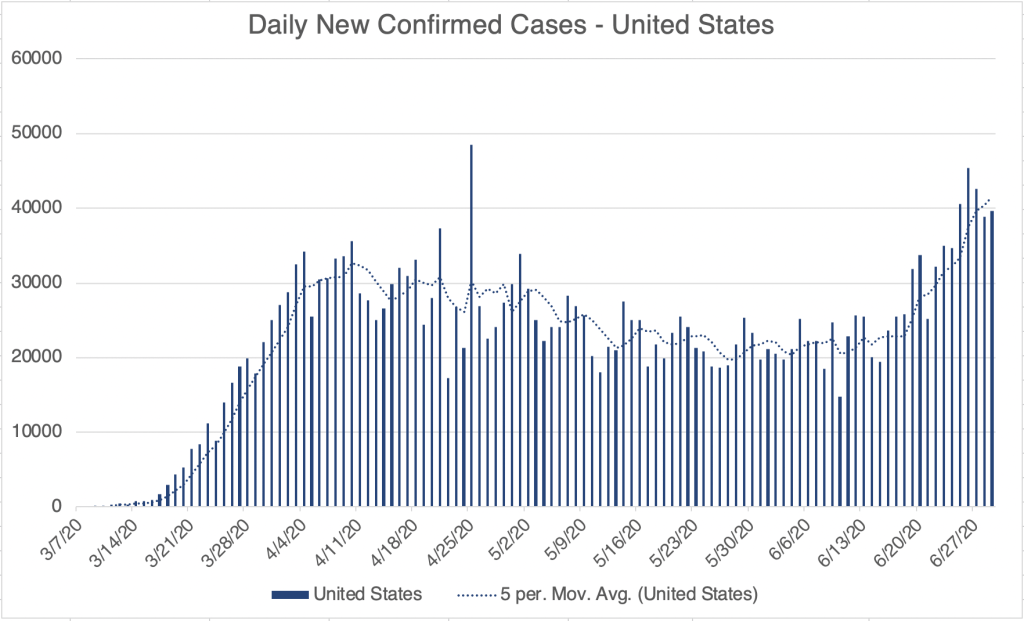
This is a case update. Unfortunately, we are experiencing an explosion of new cases in the US, California, and San Diego County this week, continuing the trend that started a few weeks ago. For all of these regions, this week brought record highs for all three regions. California reached approximately 66k active cases, and San Diego County has doubled it’s active caseload to 4,222 in just the past week.
Why is this happening? Probably for multiple reasons. First, as things re-open, some businesses and individuals are not following guidelines for safe reopening. San Diego County had 7 super-spreader events in the last week, 4 at restaurants, and 1 at a private residence. You may have seen a story in the news this week about a bar in Michigan in which 85 college aged people were infected in a single evening. As you might imagine, they were not wearing masks, and were not practicing social distancing. The recent protests and riots almost certainly have had an impact as well.
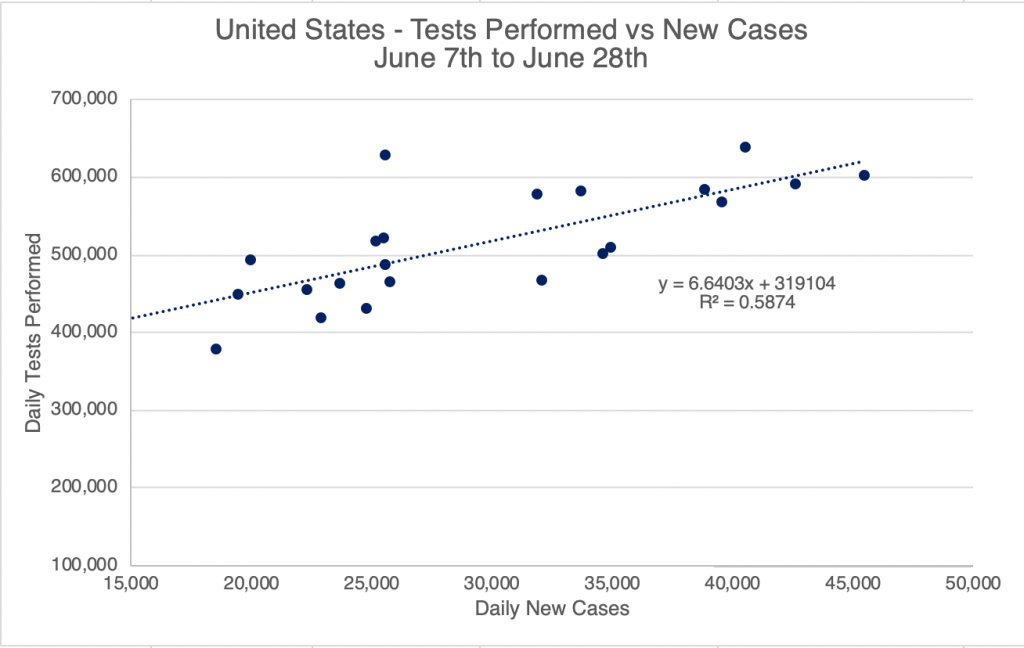
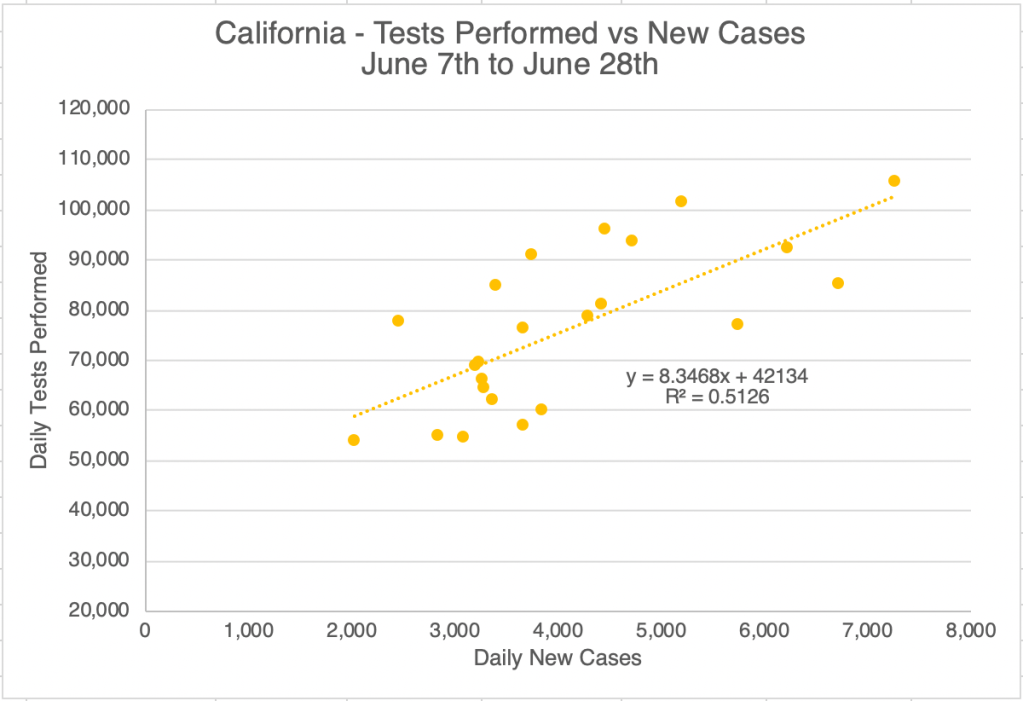
In my May 12 post, I explained how you can tell if testing is having an impact on confirmed cases by graphing daily tests against daily new confirmed cases. In the last few weeks, the R2 number has risen into the 0.5 range for the US and California. An R2 number of 0.95 “proves” correlation, but a number in the 0.5 range suggests some contribution by increased testing. These graphs suggest that increased testing has contributed some of the new cases numbers, but some of the new cases are simply new infections as well.
An R2 number of above 0.95 suggests good correlation, a number of 0.59 suggests that while there may be some contribution from increased testing, much of the increase is real new cases.An R2 number of above 0.95 suggests good correlation, a number of 0.51 suggests that while there may be some contribution from increased testing, much of the increase is real new cases.
There is some good news. That is that if you are careful and follow the below guidelines, you can be reasonably certain you won’t catch COVID:
1) Wear a mask or face covering in public. Avoid places with unmasked people. 2) Keep 6 ft away from others. 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. 4) Small outdoor gatherings are fine, even without masks, if everyone maintains a distance. Have guests bring their own food. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors, however.there may be some contribution from increased testing, much of the increase is real new cases.
An epidemic is like a brush fire. When it dies down, we can start to be complacent, but diligence is still required. We are experiencing this new burst of cases because we have let our guard down. Hopefully, we can get things back under control soon.
Maybe take a break. After all the troubling news of the past month, a friend of mine complained that he is feeling depressed and not doing well. While I encourage everyone to follow the news and to be engaged with public life, studies show that over consumption of social media can lead to depression and anxiety. If you feel depressed, or your blood pressure is high, or you’ve been ranted to your wife more than she would like (I know someone like that), you may benefit from a news and/or social media fast. Consider taking a day or more off a week to let yourself calm down and get back to normal. In our information age, we can receive all the bad news of the world at all times, and we aren’t designed to carry that burden.
This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, they are much more rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable virus can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim recently that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include respiratory conditions like asthma or COPD, heart conditions, kidney conditions, liver disease, diabetes, obesity, auto-immune disease, use of NSAID anti-inflammatory medications, being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant), vitamin-D deficiency, type A blood (Type O appears to be protective), inadequate sleep.
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms.
Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection, or lowers the viral load of exposure. Some, but not all, also prevent the wearer from inhaling airborne virus. N95 style masks without a valve are best if you can obtain one.
Best option: An N95 mask with no valve.
Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
Testing: There are several kinds of tests, and they tell you different things.
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR and are both sensitive and very fast.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Ventilators: Some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor a nasal cannula, using ventilators only as a last resort if breathing is labored.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. I’m still holding a “wait and see” posture with this treatment.
MATH+: This regimen uses Methylprednisolone (an anti-inflammatory), Vitamin C, Thymine, and Heparin, as well as optional other treatments including Vitamin D and Zinc. Early reports suggest success with this treatment.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Early estimates for a Coronavirus vaccine were around 18 months. My guess is that this is too optimistic. Personally, I wouldn’t count on a vaccine for at least a few years. In addition, some studies have suggested that Coronavirus vaccines in particular may cause side effects that may make vaccine development challenging. My standard practice for my family is to wait on new drugs for a few years before using them myself. While I pro-vaccine in general, I would personally recommend waiting for a few years before getting a Coronavirus vaccine.
Herd Immunity: Some are promoting herd immunity as a way to move through the crisis faster. The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. This is a good idea when a vaccine is available, but not when there is no vaccine. Putting many people in harm’s way to protect fewer others is not wise and is not standard medical practice.
The Future: Of course, it’s impossible to know what will happen next. My initial prediction was that the first wave would be over by July, and at this point, this doesn’t look likely. New confirmed cases have started to rise or rise faster in the 3 areas I monitor most closely, the US, California, and San Diego County, and cases are rising fast in some countries previously unaffected, especially Brazil, Russia, and India. So I’m starting to think we may not be out of the first wave before the Fall season.
In addition, RNA viruses, such as Coronavirus, can mutate very quickly because the proteins used to copy their genomes are very error prone. This means that a virus may change to a new form that can re-infect a person who has already had a previous version. Some reports suggest that this may already be happening with SARS-2. Some good news is that on the very long term (years), novel viruses tend to evolve to be less virulent, because it’s not in the “interest” of the virus to make the host very sick. The message is, we may need to adapt to a new reality for the next few months or years. We can’t really afford to be “locked down” anymore, but mask wearing and elbow bumps may be a part of the landscape for some time.
My friend who works for San Diego County Health, Brit Colanter, just posted that all San Diego County residents are encouraged to get tested for COVID-19. Check with your health care provider first to see if they will give you a free test. If not, check the below website, or call 2-1-1 for an appointment at a County Site. State run testing sites are located in Escondido, El Cajon, Chula Vista, San Ysidro and Southeastern San Diego. Check the website for a phone number or link to get an appointment at a state site.
These are likely the Abbott, ID Now rapid COVID test.
Getting a test gives you peace of mind, but also helps scientists understand the real rate of infection in the County!
Yesterday right after I posted, Mark Rasmussen sent me an article that ran in Science Magazine, one of the 2 most highly regarded science journals in the world. It’s a news article, not a peer-reviewed journal article, but it attempts to pull together information from different sources, and I think clarifies the picture regarding SARS-2 viral spread. The take-away message of the article is that while the R0 appears to be between 2.5 and 3 (more on that later), it’s not true that the average individual will pass the virus on to 2 or 3 others. Rather, most infected people don’t pass the virus on to anyone at all, rather a few infected people are “super-spreaders”, infecting a large number of people at once. There are many documented cases of super-spreading, from choir practices, funerals, concerts, fitness classes, and meat packing plants. The commonality appears to be indoor locations with lots of people in a small space, with some of them shouting or singing. While the risk in outdoor venues isn’t zero, indoor venues account for 19 times the number of super-spreading events, according to a Japanese study.
According to the article, SARS-2 has a tendency to cluster in this way more than other respiratory diseases such as the flu or colds. This may be partially because of the “viral load” effect mentioned in the Erin Bromage article I posted on May 12th. In that article, it appears that the initial number of viruses an individual is exposed to partially determined if they will be infected, and how sick they will get. This also explains why so many medical workers in Italy got very sick or died in the early stages of the pandemic. Many medical procedures such as intubation create a bloom of floating virus from a sick patient, exposing unprotected workers to high viral loads.
The science article suggests that while the virus is still dangerous and outdoor venues are not completely without risk, it may be appropriate to relax restrictions on some outdoor activities. So here’s my informed but not expert advice on how to adapt to life with COVID:
Staying at home all the time may no longer be the best approach, although it was probably very helpful in the early stages of the pandemic. Going outside to get some fresh air and exercise is probably a good thing, although still not without risk.
When doing outdoor activities, it’s probably OK to not wear a mask, but maintain at least 6-10 ft from others you don’t live with. Locations with a gentle breeze will help move virus away from you!
At work or shopping, wear a mask when around others to reduce the viral load that you are wafting into air should you be infected without your knowledge. Any reduction in viral load will help.
If you suspect you may have been exposed, contact your physician and see if you can get a test.
If you have a yard, invite a few friends over for lunch or dinner at a safe distance. Since Summer is starting, an evening outdoor dinner will be a welcome break from the isolation. You may want to have your guests bring their own food and utensils. Don’t invite a large number of friends, and sorry to say, don’t invite those friends who can’t resist hugging everyone! Young children may require supervision to be safe.
Now that restaurants are open in California, I would personally only be comfortable with outdoor seating at the moment. If you’re comfortable, visit your favorite local restaurants to give them some business, sit outside, and leave your server a big tip if you’re able!
I am a church goer, and I want to see my peeps again, but singing in a congregation is still a high-risk activity. Churches will need to be creative to open up again safely. Consider lower density services without singing, and/or hold services outdoors.
Regarding the R0 value for SARS-2. I saw a CDC website last week that gave the R0 value as 2.5. After 10 minutes of looking, I couldn’t find this site again. The Sanche paper I’ve referenced before (High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2, EID, July 2020), published in the official CDC journal, Emerging Infectious Disease, gave the R0 as 5.7. So the CDC itself seems confused about what the R0 number is. My guess is, it’s somewhere between 2.5 and 5.7. That was a joke. Obviously, this range is far too large to be useful, and 2.5 and 5.7 are very different as applied to an R0 number. 2.5 is a very infectious disease, 5.7 is a super-infectious disease.
I’ve mentioned this before, but I want to remind everyone. Herd immunity is only a goal when a vaccine is available. Seeking herd immunity when there is no vaccine is not a good idea, because it will put large numbers of people at risk. Additionally, I am generally very pro-vaccine, but because of the risks of side-effects with this particular virus, a vaccine may not be available for several years. We will need to adapt to this reality. My hope is that we will start seeing daily cases come down this Summer.