This post is about a new California law seeking to limit misinformation.
California’s Governor Gavin Newsom signed AB 2098 into law on Friday. The new law allows the Medical Board of California to punish health care providers for spreading misinformation. The law does this by adding the act of spreading misinformation to the definition of “unprofessional conduct” used by the Medical Board of California. Unprofessional conduct is punishable in California by up to the suspension or loss of a license to perform medicine.
The law defines “misinformation” as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.”
There are many, many examples of ideas in science and medicine that were opposed by the scientific consensus and later accepted as true. There are so many examples of this, that it should be considered as a normal part of the scientific process. Examples include:
- The Earth revolves around the Sun
- Not cleaning surgical tools between operations can lead to increased mortality in patients
- Ulcers are caused by the bacteria H. pylori, not by spicy food
- Viruses can cause cancer
- Cells produce energy by passing electrons through a membrane
- The universe began at a discrete moment, and then expanded to its current form, creating both space and time in the process
- The SARS-2 virus was created in a laboratory in Wuhan*
The idea that misinformation can reasonably be defined as an idea that is contradicted by scientific consensus is itself contradicted by centuries of scientific practice.
Scientific ideas come to be seen as true not merely by achieving consensus, but also by surviving challenge by new ideas. No scientific idea is immune to this process. Science is not a set of facts set in stone, but a constantly changing set of ideas guided by the scientific process, a process which includes debate among scientists. Requiring that new ideas achieve consensus immediately would freeze the advance of science in place, the current, and often wrong, ideas remaining dominant forever.
Of course, I have not yet addressed the obvious First Amendment violation this new law creates. The First Amendment clearly allows freedom of speech, a cornerstone of American life. This law will quickly be challenged by First Amendment advocates and will almost certainly be struck down.
As I’ve stated before, freedom of speech is not the cause of misinformation. It is the antidote. Only if we allow the free flow of ideas can these 3 things happen:
All ideas to be aired
Good ideas to be confirmed and adopted
Bad ideas to be discredited
The correct way to battle misinformation is clear and persuasive communication, not censorship.
Dr. Mobeen Syed points out several other negative impacts this law will have:
- Doctors will be suspicious of their patients, compromising the doctor/patient relationship.
- Doctors will only give consensus advice, making going to the doctor more like going to a call center.
- Laws will expand to include other kinds of “misinformation” further compromising the exchange of ideas.
- Law will be used unequally to silence only certain kinds of speech.
- Doctors may choose not to practice in California.
If I’m being too subtle, I’ll just say that this is a bad, unconstitutional law and should simply be ignored.
Don’t fear, but be smart,
Erik
* I’m taking a little liberty on this one. This idea was rejected totally early in the pandemic. It is not yet universally recognized as true, but many scientists, including me, see it as most likely to be true.
Another excellent video by Dr. Christy Risinger.
_____________________________________________
Update: January 13, 2023
California Physician Misinformation Act: On October 4th, 2022, I wrote about California AB 2098. This new law went into effect on January 1st and adds “the dissemination of misinformation or disinformation related to the SARS-CoV-2 coronavirus” to the definition of unprofessional conduct for physicians in California. Unprofessional conduct can result in the suspension or loss of license for physicians in California.
Just yesterday, I had lunch with a friend of mine who is a doctor in California. I asked him how he is dealing with this new law. He said most of the doctors at his hospital follow the official guidance promoting vaccination, and the few who don’t have become very quiet about vaccines. Doctors can’t say anything negative about the vaccine, for the risk of their medical license.
In 2021, this same doctor was coerced into getting the vaccine to retain his position at the hospital. He got a booster later in the year. A month after receiving his booster, despite being very physically fit for his age, he had a heart attack. His cardiologist said he had none of the arterial plaques that typically cause heart attacks. My friend cannot prove this, but he strongly suspects that clotting due to the vaccine contributed to his heart attack. Despite all this, he does not feel at liberty in California to give information to patients that would reflect negatively on the vaccines.
Because this law is so new, I don’t yet know how it will be handled by the Medical Board of California. If they choose to ignore it, then doctors won’t be under threat. However, doctors and pharmacists have lost their licenses in the last few years for violating CDC guidelines, so the threat is a real one.
If you live in California, you cannot expect your doctor to give you their honest opinion about vaccines. This is literally illegal now. Consider writing your state senator or assemblymember and ask them to support the repeal of AB 2098.
________________________________________
Update: October 10th, 2023:
The Repeal of the California Physician Misinformation Act: Last October, I wrote about a new California law which made “misinformation” a cause for physicians in California to lose their medical license. Misinformation was defined as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.” As I argued, it is common for new scientific ideas to be opposed by the majority of scientists before gaining acceptance.
The new law immediately became a target of legal action, one case being Høeg vs Newsom. On September 29th, 2023, Høeg’s attorney filed a request that the law be permanently barred from enforcement. Just a few days later, on October 1st, California Governor Gavin Newsom signed a repeal of the law. This is great news for California physicians and patients. California physicians are again free to communicate to their patients without fear of losing their license. This is also great news for the cause of freedom of speech in the US.
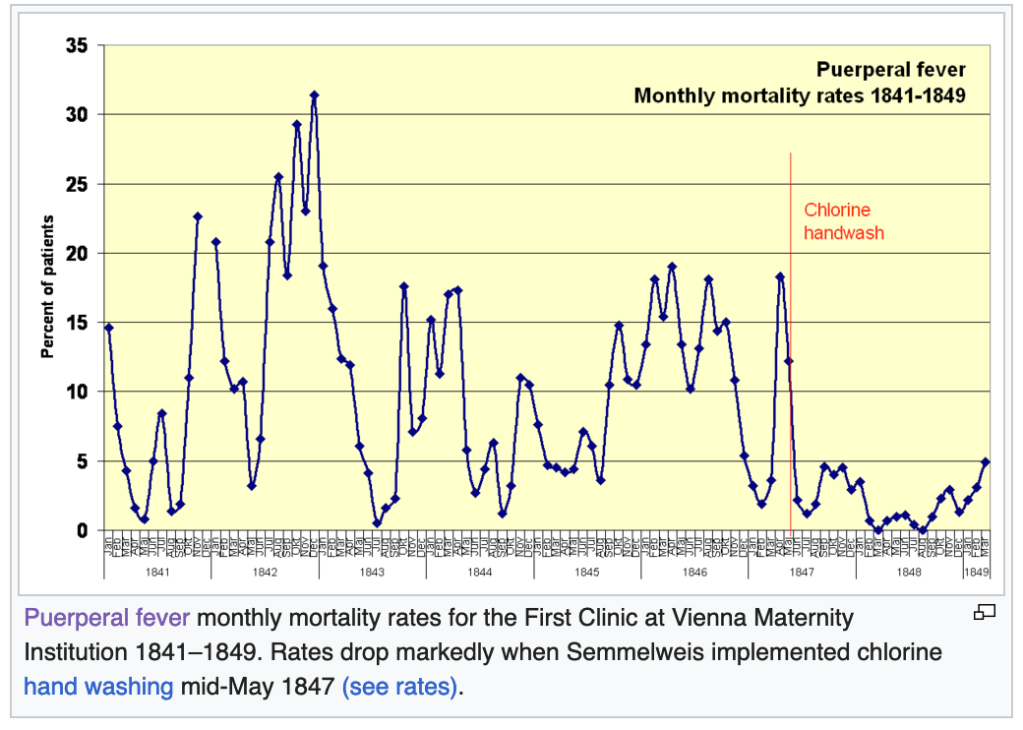
The fascinating yet tragic case of Dr. Ignaz Semmelweis: Ignaz Semmelweis was a physician at Vienna General Hospital in 1847. One of his jobs was to deliver babies in the maternity ward. Unfortunately, in his ward, the rate of fatality for new mothers was high, an average of 18.3%. Women were afraid to deliver in his hospital, and begged to deliver somewhere else!

Then one day, a colleague of Dr. Semmelweis died of Puerperal Fever, with symptoms very similar to the women in the maternity ward. His colleague had nicked himself with a scalpel while performing an autopsy on a cadaver. Dr. Semmelweis thought that maybe the fatalities in the maternity ward had something to do with the fact that Doctors where going straight from performing autopsies to delivering babies!
At this point, you’re probably holding your head and saying “What!?”, perhaps with some other colorful words added in. It’s obvious to us now that this was a terrible idea, but the Germ Theory of Disease had not yet been accepted in medicine. The field at that time had no idea that microscopic organisms could transmit disease.
Dr. Semmelweis started having physicians wash their hands in a chlorine solution after performing autopsies. The maternal death rate fell immediately to below 5%, some months having zero deaths. Dr. Semmelweis tried to tell others of his findings, but no one believed him. After increasingly passionate and ultimately embarrassing behavior, his friends and family had him committed to a mental institution. He was abused by guards and died in 1865.
That same decade, Louis Pasteur and Robert Koch were producing evidence supporting the Germ Theory, and Joseph Lister began popularizing the use of anti-septic procedures in surgery, greatly improving outcomes for surgical patients. Semmelweis’ ideas would be vindicated, but not until after his tragic death.
Semmelweis is now considered a hero of modern medicine, having a university, several hospitals, and even a minor planet named after him.
Why did I tell this story? Under a law similar to the California Physician Misinformation Act, people like Semmelweis would have lost their licenses. Semmelweis’ story underscores the need for strict adherence to the Scientific Method, not the suppression of “misinformation.” We suppress unpopular ideas at our peril.