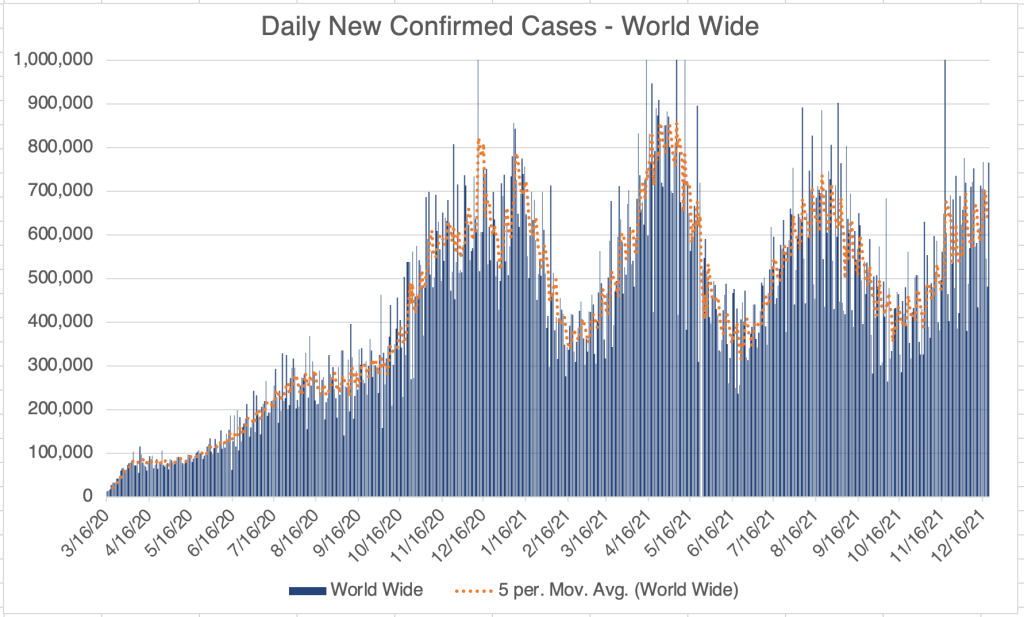
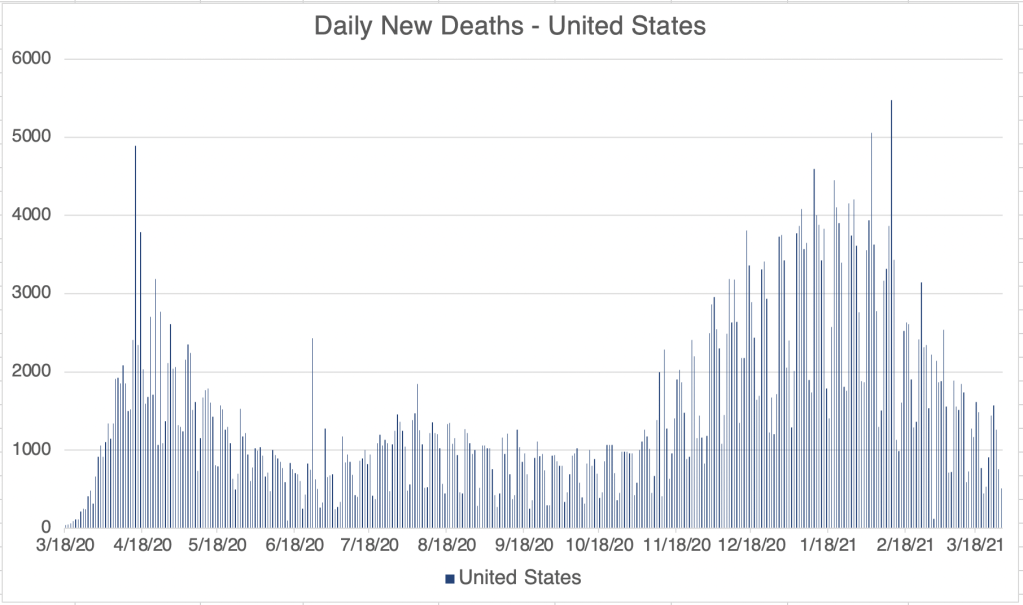
This is a case update. I’ll also discuss the new Omicron numbers in the United States, and reevaluate if Omicron will represent our way out of the pandemic.
In terms of whole numbers, cases are still increasing in the US, mostly in the Northeast. In some amazing news, most of the cases in the Northeast are now from Omicron and not Delta (more detail on this below).
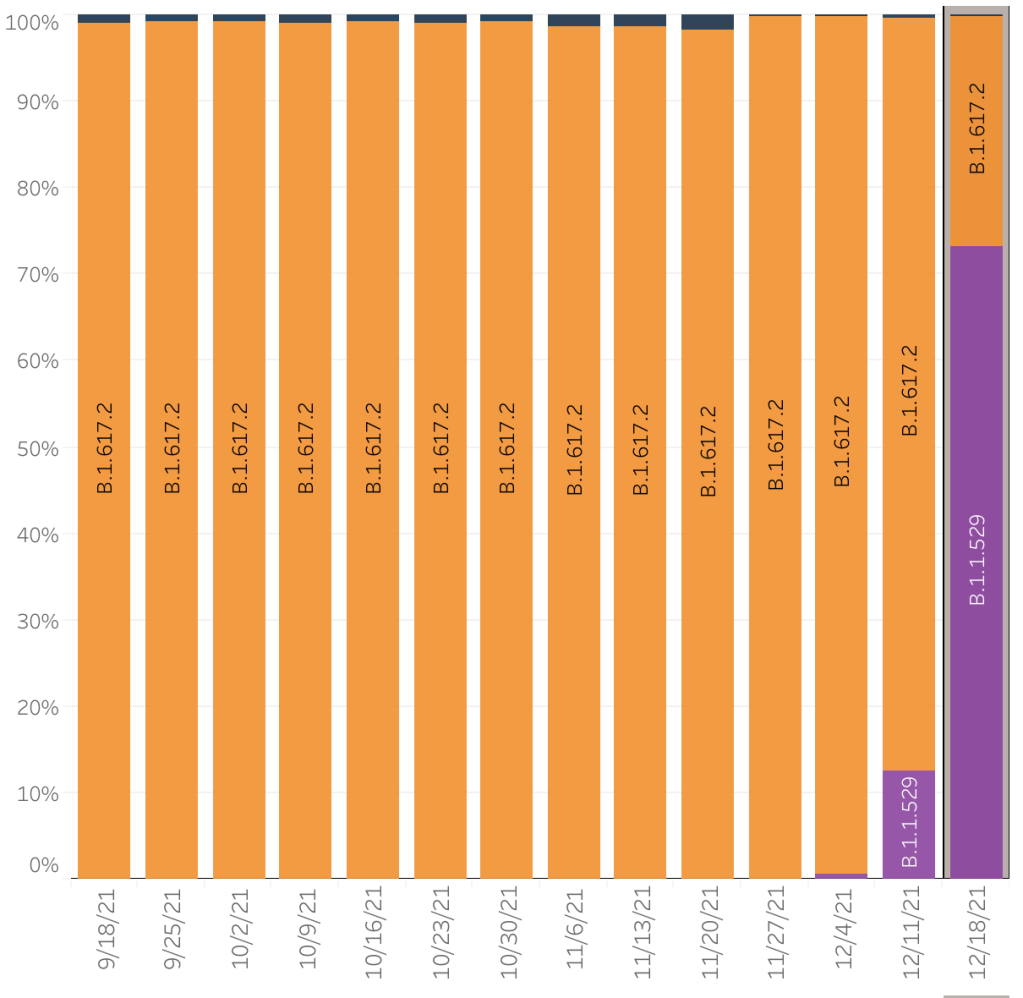
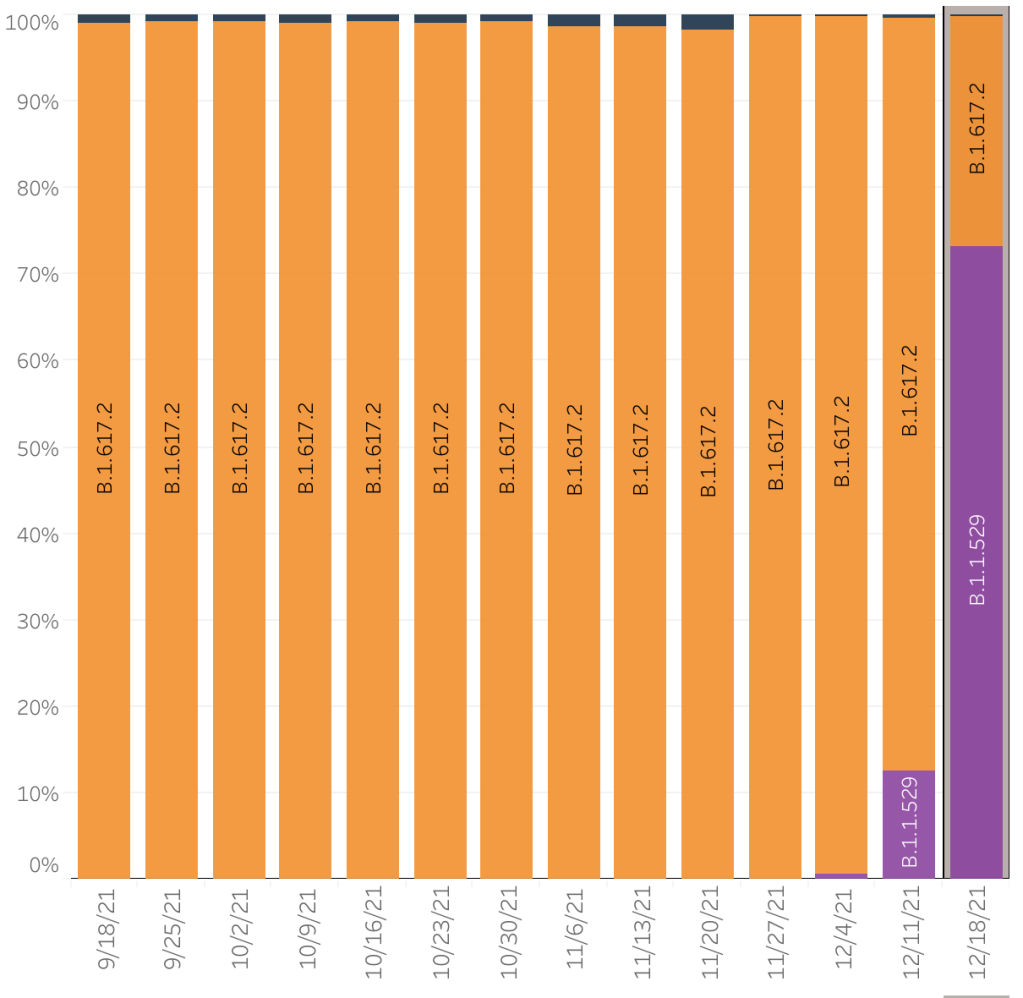
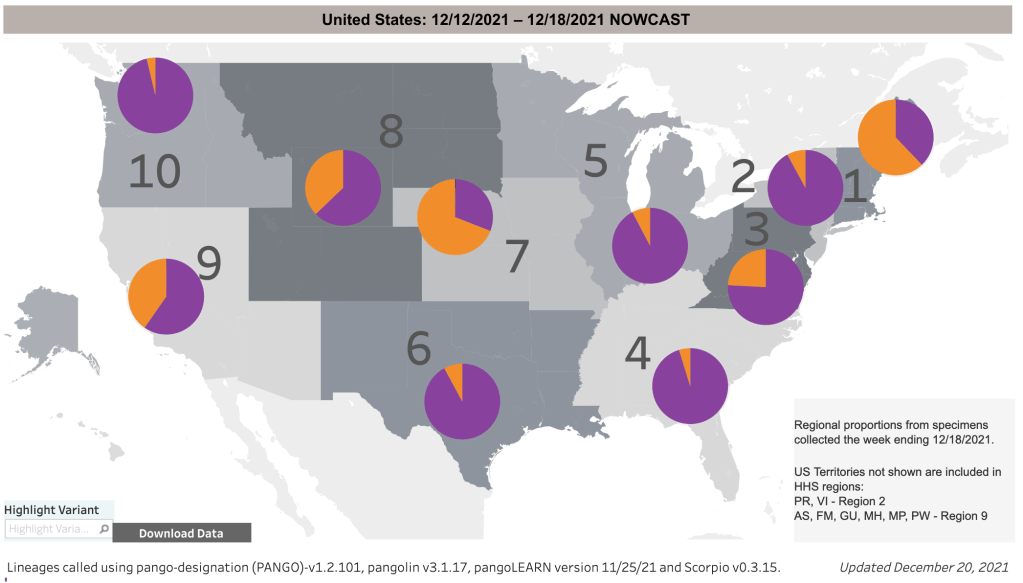
Omicron rapidly overtakes Delta!:In amazing news, cases from Omicron already outnumbers cases due to Delta in the US, and are 90% of new cases in some regions. Last week, the CDC was reporting that 3% of US cases were from Omicron. This week, they revised that number upward to 12%, but also reported that for 12/18, 73% of COVID cases in the US were caused by Omicron, 60% in the Southwest. I expect 95% of cases in the US to be Omicron by next week, and virtually 100% by New Years. This is potentially great news!
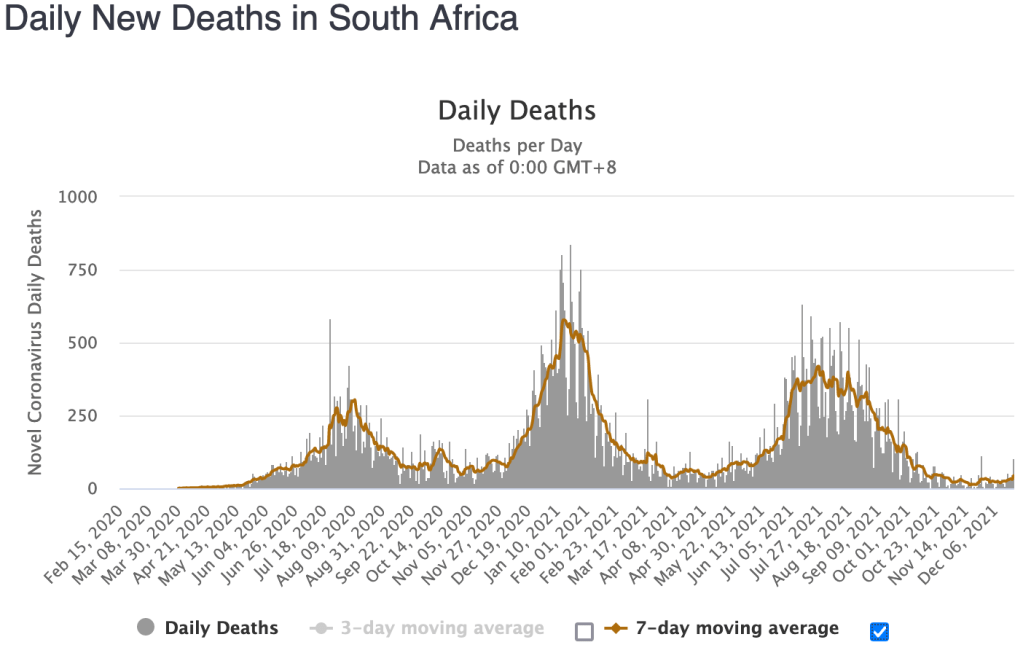
While still very early, a few other countries have started to produce data that can tell us what we might expect. In South Africa, the peak of new cases is already coming down. In previous waves there, peak deaths have trailed peak case by about 10 days. But for the Omicron wave, there is only a modest increase in deaths 10 days after peak new cases. This seems to confirm reports that Omicron produces very mild disease.
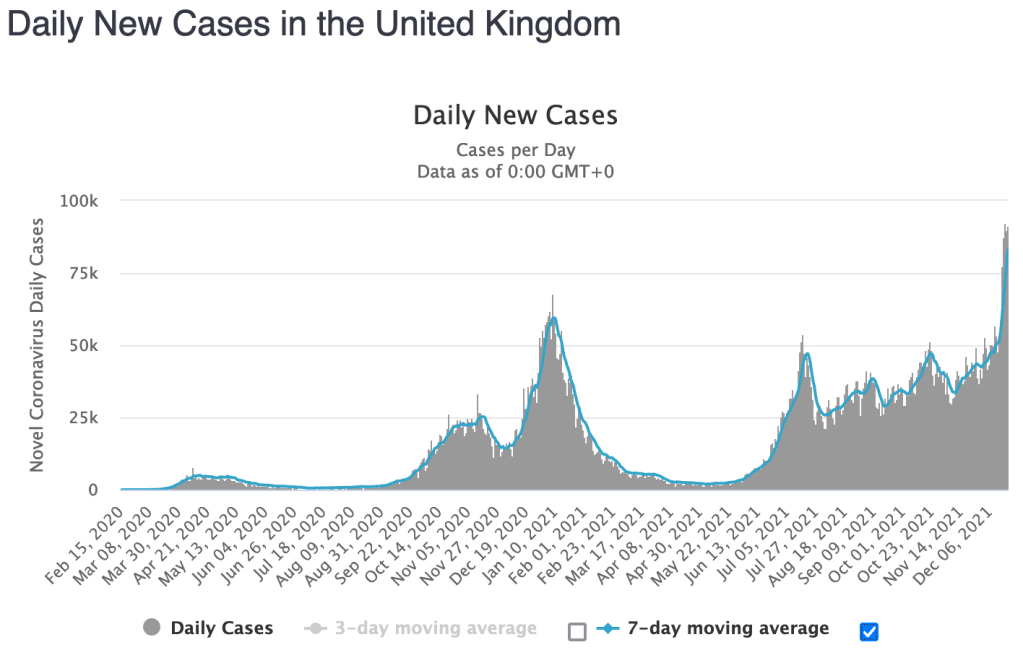
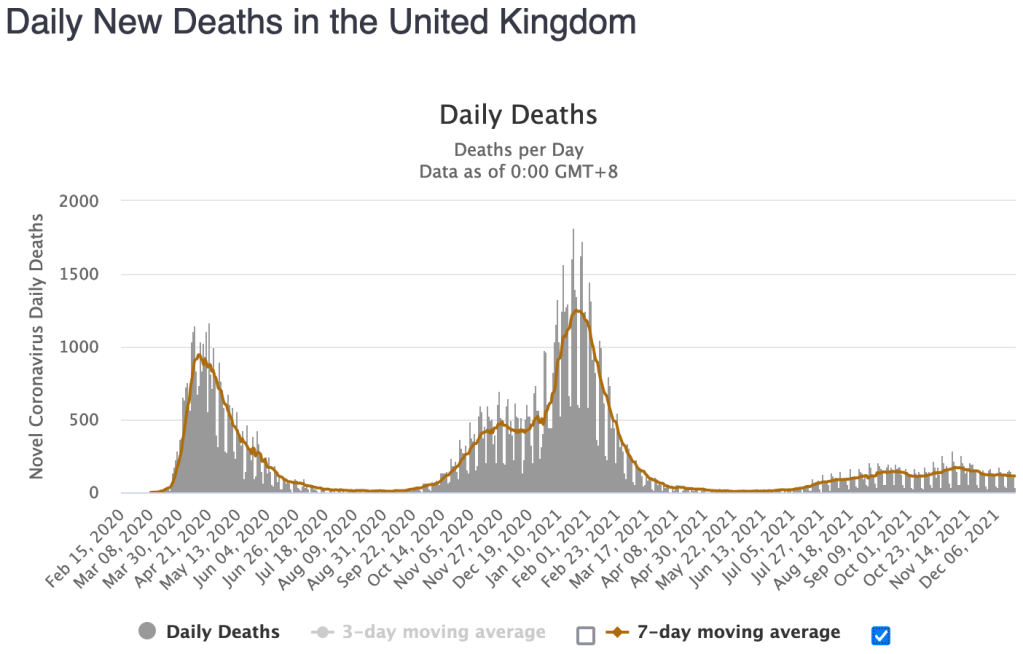
In the UK, Omicron cases are surging dramatically, with cases doubling every few days. In spite of this, there were 909 COVID deaths last week. In total, only 14 people have died from an Omicron infection this far. As Omicron spreads in the UK, we will likely see hospitalizations and deaths go down dramatically. I will caution that in the UK, deaths trail cases by about 12-20 days, and we are still early in the Omicron wave in the UK.
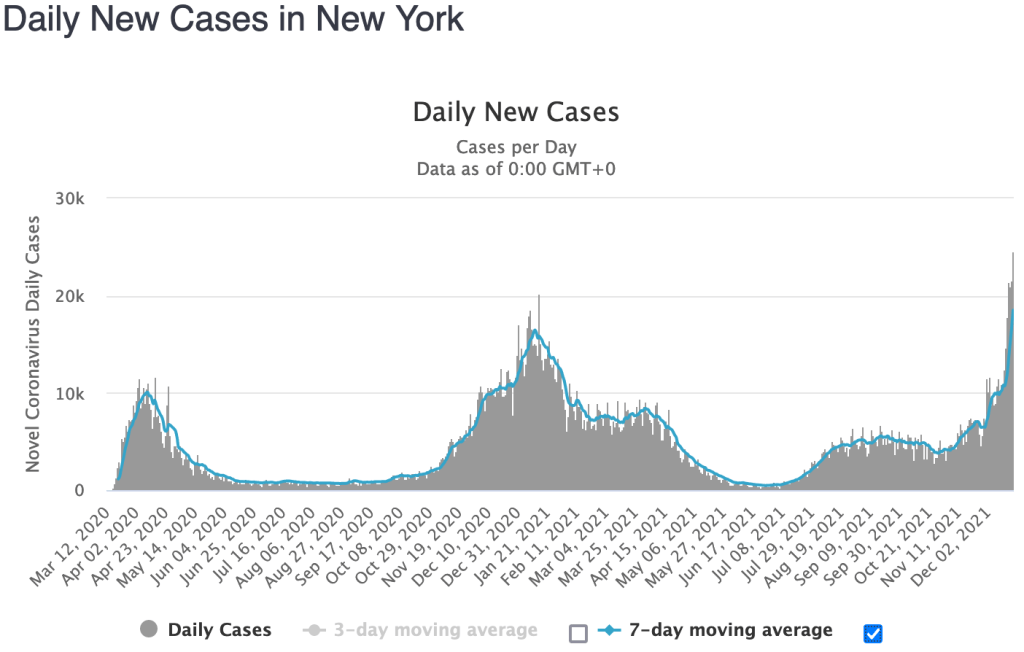
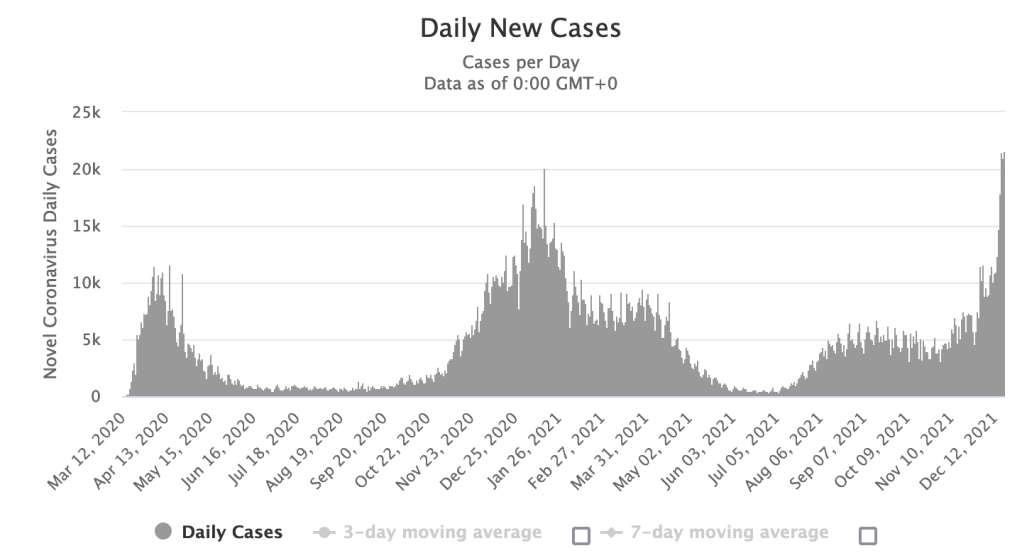
Back in the US, 90% of new cases in the Northeast are due to Omicron right now. In spite of this, total case numbers in New York are roughly double what they were a week ago. This means that of the 20,000 new cases daily in New York State, only 1600 are from Delta, the rest are from Omicron. So Delta cases in New York have gone down by 80%! Indeed, Omicron appears to be displacing Delta!
Keep in mind that we are only a few weeks into the Omicron wave, and things are still early. I will also caution that there are still a few people dying due to Omicron, so it’s not all over. Cases may be extremely high in the next few weeks. That being said, Omicron definitely has the potential to essentially end the pandemic, maybe in just a few weeks! If you’re one of my colleagues in the medical industry, start polishing up your post-COVID business models now!
I am NOT saying you should run out right now and get a nice case of Omicron. It’s still to early to say if that will be a good idea. For now, keep it together and stay cautious for just a few more weeks until we know more. I will also caution that I have a track record of being overly optimistic on my expectations of when the pandemic will end!
Given that the vaccines have some inherent risks of their own, and that Omicron appears to have very mild symptoms and completely ignores previous immunization, I do not recommend a booster to prevent Omicron infection at this time. Instead, those with risk factors should simply take precautions until the Omicron wave is over, or until more is known. As always, consult with your medical provider when making health care decisions. I am a molecular biologist, not a physician.
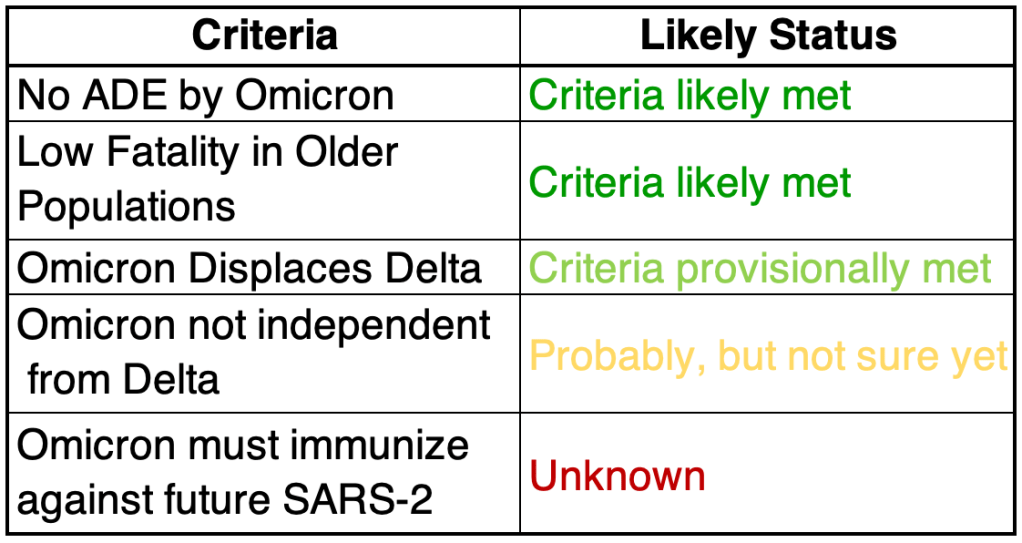
Omicron scorecard: Here’s my revised “scorecard” from last week. As a reminder, I am not an epidemiologist, I’m a molecular biologist. This is my informed but not expert opinion.
1) Omicron must not use the ADE pathway to produce more severe cases: Looking at the available data so far, while Omicron may preferentially infect those who have been previously infected, cases are still mild, and fatality rates very low. So for now, this criteria is met.
2) Low fatality in older populations: South Africa has a relatively young population, so reports of mild symptoms may not carry over to countries with older populations. The UK data from this week suggests that Omicron deaths will be low, even in older populations.
3) Displace Delta: Delta has a much higher case fatality rate in the US than Omicron appears to have. For Omicron to end the pandemic, it must displace Delta from the COVID population of strains. With the super high infectiousness of Omicron, it might just do that. Total Delta cases are currently down 80% since the start of the Omicron wave in New York State. This is very encouraging. This criteria is provisionally met.
4) Omicron must not circulate independently from Delta: Related to the above, if Omicron is very different from Delta, it may act as a completely different virus. There’s a chance that Omicron may displace Delta on the short term but still allow Delta to persist. Since Omicron is displacing Delta, it looks like this criteria may be met, but we won’t know for sure until we can see if Delta pops back up after the Omicron wave is over.
5) Omicron infection must immunize against future SARS-2: Since Omicron appears to infect those with immunity to Delta, it may be that it is different enough that it will not provide immunity to Delta or other SARS-2 strains. This criteria is not strictly necessary if Omicron completely displaces other SARS-2 strains (see 3 above), but it would be really nice to have some protection against future strains. We won’t know for sure about this one until a new version of COVID arises.
“Omicron” may sound like a killer robot, but it turns out, it’s OUR killer robot!
You’ll have to forgive my imprecise language this evening, but we have some potentially VERY good news, and I’m a little giddy. Last week I reported that 3% of the COVID cases in the US were because of the super infectious but mild disease causing Omicron variant. On Monday afternoon, the CDC updated their numbers from last week stating that 12% of the COVID was from Omicron. Today, they are reporting that for this week ending Sunday, a full 73% percent of COVID cases were from the Omicron variant! With only a doubling of cases in the last few days, that means at least 50% of Delta variant cases have been displaced by Omicron cases. This means that Omicron is displacing Delta. At the current rate of expansion, by Christmas, at least 95% of COVID in the US will be from Omicron, and nearly 100% by New Years! If we can keep Delta suppressed for at least 2 weeks, it will be eradicated from the US. This is so great!
From the CDC page on Variant Proportions. Currently, 73% of COVID cases are from Omicron.From the CDC page on Variant Proportions. Currently, 60% of COVID cases in the Southwest are from Omicron.Daily new cases in New York State. Note the doubling of cases in the few days. But 90% of these cases are from Omicron, so Delta cases are roughly 25% of what they were a week ago, having been displaced by Omicron.
I have often been overly optimistic, but literally, if things go they way they’re going now, the Pandemic could virtually be over by New Years!
You know that cop at the beginning of all those movies who is about to retire and then gets killed in the first 10 minutes? Don’t be that guy. We’re almost out of the woods. Don’t go crazy and get COVID now. Keep it together for another few weeks, for crying out loud.
After I’ve settled down a but, I’ll be adding more information, links to my blog post, and a more sober assessment on this topic tomorrow, so check again then. For now, crack open a Diet Coke, in the seclusion of your own home or sensible outdoor gathering and celebrate!
This post is detailed, but adds an important new set of facts regarding the Delta Variant, the current vaccines, and prospects for a new booster shot.
You may have heard commentators in the last few days talking about the reduced efficacy of the current set of vaccines. There has also been a lot of discussion about a study from Israel about relatively high numbers of Delta COVID cases among vaccinated individuals.
First a little background on antibodies. Your immune system is making a random set of new antibodies all the time. In an ingenious mechanism, your immune cells “mix and match” pieces of a gene in your immune cells, producing the ability to make a zillion (scientific language for a whole lot) of different antibodies. Your body is basically making different “keys” that can fit into the “lock” of some new protein.
When you get an infection, several different antibodies may bind to the invading agent, on different regions, so you may be protected by several different “keys”. When this happens, a bunch of different things happen, including the manufacture of Memory B cells which makes just the antibody that binds to a particular protein. These cells get activated if you get re-invaded by something with that protein. All this to say, if you’ve had COVID, or been vaccinated, your body will have B cells with antibodies on them that bind to different parts of the Spike protein.
Before I say anything else, I want to repeat that I have not been vaccinated, but have recommended that high risk individuals get vaccinated! I’ve also pointed out many times in the past few weeks that countries with large vaccination programs have lower death rates due to Delta than other countries!
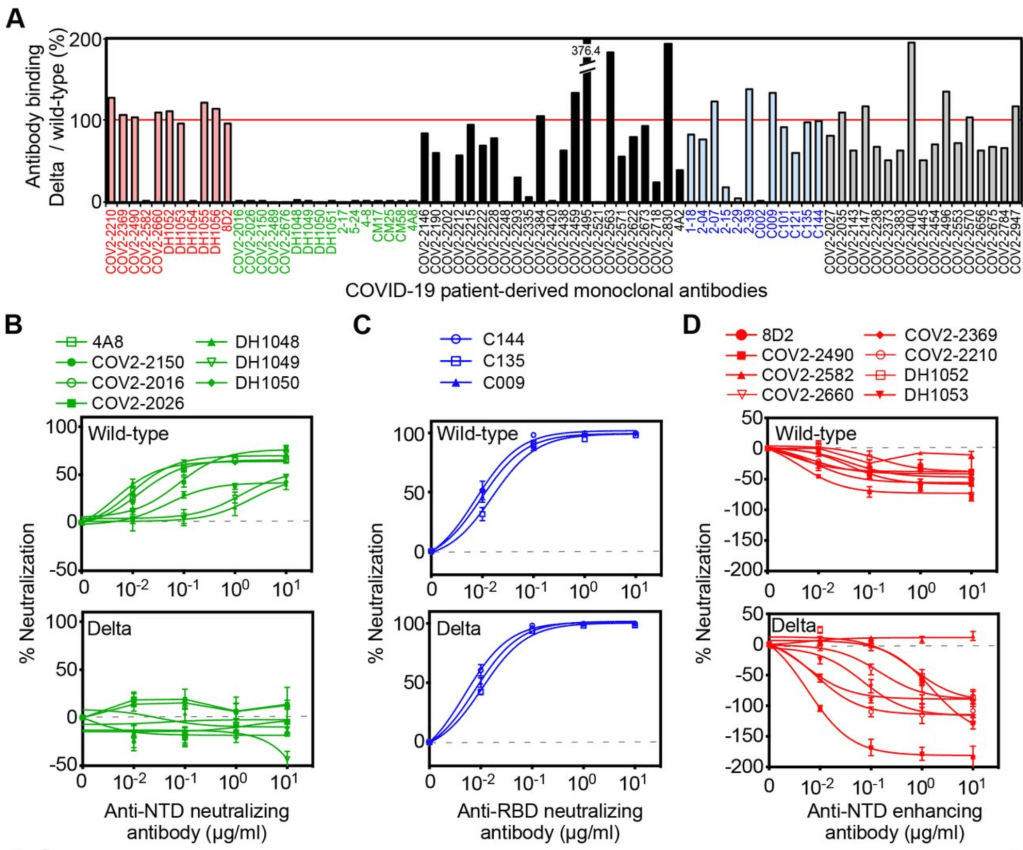
Literally 30 minutes after Thursday’s post on vaccine myths, a doctor friend of mine sent me a pre-print paper from a lab in Japan. Please note, this is a pre-print paper and has not yet finished peer review! The paper describes experiments using antibodies derived from patients infected with the Wuhan strain, as well as with the Delta Variant. They then studied binding of these antibodies to artificial viruses. The paper argues that Delta variant viruses are less neutralized by vaccines against “wild-type” or Wuhan strain vaccines. While the “wild-type” antibodies against Wuhan can neutralize a region of the Delta Spike protein called the Receptor Binding Domain (RBD) (Figure 1C), other antibodies binding to another region of Delta Spike protein actually enhance infectivity. Figure 1D from the paper shows negative levels of “neutralization” for antibodies that bind the N-terminal domain of the Spike protein. The paper calls this “enhanced”. Yes, this is the ADE I’ve been talking about.
They suggest that with rapid changes in COVID variants, a new version of Delta is going to be able to use the ADE pathway in the near future, when Wuhan era antibodies will no longer be able to neutralize a mutated Delta strain.
To sum that all up in simpler language, it basically says that Delta is more infectious because it is partially using the ADE method of infection. Future versions may be less prone to be neutralized by Wuhan antibodies, making them fully enhanced. If this happens, we may have more severe disease in those who get infected with this new enhanced Delta.
They conclude by saying a booster against the Wuhan strain will not be effective in improving protection from Delta, and that a new vaccine against Delta will be required.
The material in the paper may help to explain why we have been seeing lowering levels of vaccine effectiveness in some countries.
Just to be very clear, they are not saying that this new enhanced Delta exists now, just that it may exist in the future.
I will pay close attention to this issue. If you have already been vaccinated or had COVID, a new Delta vaccine will be your best defense against possible ADE arising from a possible enhanced Delta.
If an enhanced Delta arises, and you have had Wuhan COVID or a Wuhan vaccine, and you haven’t had Delta, then you may be at greater risk for severe disease.
If you have had COVID since July 2021, you are likely already immune to the Delta variant, and this will not be an issue for you.
I am fully aware this complicated. Also, the CDC has rarely if ever discussed this possibility, so unfortunately, most of the people you talk to about this will not believe it. I am sharing this with you so you can make wise decisions for you and your family.
Some companies are already working on Delta versions of the vaccine. If you have had the current vaccines, or had COVID, you should get the Delta vaccines as soon as they are available.
Of course, discuss your medical history with your doctor before making medical decisions.
Another note on misinformation:My post from last Thursday generated a lot of discussion regarding censorship and misinformation. I argued strongly that the dangers of misinformation do not outweigh the benefits of free speech. Many of you are pro-vaccine and others are suspicious of the vaccine. I would simply urge this:
1) If you use the words “misinformation” and “disinformation” in a post or in a discussion, please come ready with evidence to support whatever claim your making! Don’t just throw out this word, support it!
I recently saw a video with a pro-vaccine medical person saying “we just need to keep pounding this information into people”. That is the wrong approach. With someone who is not yet convinced to get a vaccine, “pounding” away on them is just going to raise their defenses and exasperate you. Instead, gently show them your reasons for believing what you do! Explain to them what the data means. You may not convince them, but you may move them toward being more open to your view.
2) If someone makes a claim that sounds unfounded or that you don’t trust, don’t just tell them they’re wrong or make a counter claim, ask them to provide evidence, or where they got their information. You don’t have to do their homework for them! If they can’t produce any evidence, you are under no obligation to counter it. I’ve saved myself A LOT of work with this approach. It’s OK that they just heard it somewhere IF their source is reliable and has evidence themselves. You can still ask them to provide you with a link or something to that person’s statement. However, “I just heard it somewhere” is not evidence.
Part of the reason I’m not so worried about “misinformation” for myself is because of my regular use of suggestion #2.
In the interest of openness and full disclosure, I need to share a video with you that I just watched. Dr. Zubin Damania is a Youtube commentator that I actually listen to a lot, and I find him more reliable than many. He just posted a video “Top 3 COVID Vaccine Myths“. Two of his myths are:
2) The Spike protein is toxic. 3) Antibody Dependent Enhancement may cause vaccinated individuals to experience more severe disease if infected with SARS-2.
If you have been reading my posts, then you know I have been concerned about both these issues. So am I spreading myths?
2). My concerns about Spike protein toxicity are based on persistent rumors of people having moderate severe reactions to the vaccines. For awhile, I dismissed these as just the standard reaction that some have had to any vaccine, including those for flu. But more and more rumors piled up and made me wonder if something else was going on. Then I saw the video by Bret Weinstein and Robert Malone. Dr. Malone is the inventor of the mRNA vaccine technology. The video argues that the Spike protein itself is toxic. Dr. Malone’s credentials are at least as good as Dr. Damania’s on this matter, likely better, so I can’t dismiss his view.
Unfortunately, I haven’t yet been able to find enough reliable information on adverse events to form my own opinions based on the data, so I’ve been relying on others to inform me. Frankly, because of the politicized nature of the vaccine issue, I don’t feel at all confident that I can get reliable information. So I may never be able to develop an informed opinion on this matter.
Dr. Damamia claims that convincing evidence exists that demonstrates that Spike protein is not toxic, but he doesn’t give it in this video. This of course is very common.
3) I’ve talked a lot about the ADE issue. In this video, Dr. Damania claims that ADE has not been an issue in the vaccine roll out, and the new variants have not caused more severe symptoms. I agree with both of these points. I point these out in my November 2020, December 2020, and April 2021 updates to my ADE post. I am still concerned about that new variants may someday arise that can use the ADE pathway, or that a new SARS strain, a hypothetical “SARS-3” will arise that will be different enough to trigger ADE. So while I agree with Dr. Damania’s point on ADE, it’s not quite the point that I’m still concerned with.
As I’ve stated many times, the vaccines are likely to help you if you have a risk factor and I have several friends and family members that I have recommended get the vaccine. So I am not anti-vax per se. But I don’t think it’s the obvious choice for everyone, and I’m staunchly for personal medical freedom in regards to COVID vaccines.
So what do I do now? What should a thinking person do when confronted with new information from a trusted source that you’re not sure about? These things are all true when dealing with complicated issues:
People you generally agree with may say something you don’t agree with. People you generally disagree with may say something you agree with or makes you think about an issue in a new way.
Both of these are normal. When dealing with a complicated issue like COVID, race relations, worldview, politics in general, it is critical to keep an open but critical mind. You have to read widely from both your side and others to hope to get a clear view of the issues involved.
I respect Dr. Damamia. He might be right! I’ll have to think about his points, do some more homework, and reassess my opinion. There are 3 possibilities.
I will abandon my position and accept his. I will learn new things that will reinforce my position. I will do a bunch of research, but will not find conclusive information that will allow me to form a new opinion either way.
If I can arrive at a place closer to the truth, then the exercise will be a good one. If I decide I think Dr. Damania is wrong on these points I’ll likely still watch his videos, since I think he is right more often than he is wrong, and he’s more open minded than most, so I think he is at least being honest about what he believes, which is a very valuable trait! Dr. Damania is both for COVID vaccination and against vaccine mandates.
I started out posting on COVID because as a scientist I felt a responsibility to help my non-scientific friends and family members make some sense of the pandemic, especially when scientific communication is so often poor. I hope I have done that. I can’t claim to always be right, and have changed by view several times. But I have given you the truth as best as I can find it, and supported it with evidence.
A word on tech censorship: The WHO said 2 false things early on:
SARS-2 is not human to human transmissible SARS-2 is not transmissible as an aerosol.
Both of these things were demonstrably false, and perhaps politically motivated, even at time the WHO stated them. In in spite of this, the social media platforms came to hold the WHO as the gold standard for the truth on COVID matters. To this day, F@¢3b00k may place a tag on the end of this post claiming the WHO as the authority on COVID matters. Most platforms would delete or restrict anything that ran against the WHO. Yes, computer programmers in Silicon Valley are still pulling down information posted by medical doctors and scientists. Even Dr. Damania has had videos censored!
One of the worst results of the pandemic in the US is censorship of divergent opinions. Freedom of speech allows 3 things:
All opinions to be held up to public scrutiny. True things to rise to the surface. False things to be discredited.
When freedom of speech is restricted, none of these can happen. If a wrong thing becomes the “orthodox” view, and no other views are permitted, then the orthodox view will always be wrong, and we will end up solving all of the wrong problems. If there is a hole in your gas tank, it doesn’t matter how many times you put gas in it. It will always be empty. Fix the real problem first.
This is why all the claims of misinformation, from all sides, are so insidious. When you claim misinformation, you are claiming to have the whole truth on an issue. Sure, we can and should argue against views we think are false. But we must also protect the right to air all views! Or we are doomed only to have the first view that becomes dominant, and we are less likely to find the truth!
I also found an article on why some are still vaccine hesitant. For those of you who are wondering, you should read it.
This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Origin: Controversy over the origins of the SARS-2 virus began very early in the pandemic. The most common theories were that the virus arose naturally at a live animal market in Wuhan China, where animals from a wide variety of species are sold. The predominant theory is that the SARS-2 virus arose in bats, then transferred to another animal, perhaps a pangolin, before moving to humans. This has been the most accepted theory for the majority of the pandemic, promoted by the WHO, the CDC, and American media.
The lab leak theory, the idea that the virus arose from the Wuhan Institute of Virology, was present from the beginning, but was heavily disfavored by official channels for most of the pandemic. On May 23, 2021, the Wall Street Journal published an article that gave evidence for idea, followed closely by an article from Vanity Fair. The articles normalized discussion of the theory and as of this writing, polls show that a majority of Americans believe that the virus came from the WIV.
Emails between several virologists, public health officials and Dr. Fauci strongly suggest that this group believed that the virus may have come from the laboratory as early as January 31, 2020. However, this same group published a scientific article on February 9th supporting the natural origin theory. The paper was at odds with discussion in the email correspondence. If investigations show that the group published claims they knew to be false, this would represent a significant case of scientific fraud.
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, outdoor transmission of SARS-2 appears to be extremely rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable viral can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include:
age asthma or COPD heart conditions kidney conditions liver disease high blood pressure diabetes obesity auto-immune disease use of NSAID anti-inflammatory medications being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant) vitamin-D deficiency type A blood (Type O appears to be protective) inadequate sleep
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms. Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection or lowers the viral load of exposure. N95, KN95, and KF94 respirators are effective at filtering close to 95% of virus. A good mask is well fitting and filters the air moving in an out of your mouth and nose. The commonly used surgical masks and other loosely fitting masks do not filter air and I don’t recommend using them.
Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection. Social distancing may be more important for droplet transmission, like the flu, than for aerosol transmission in which microdroplets can stay suspended for much longer and travel much further.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US. Supplementing Vitamin C and Zinc is also recommended.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
I’ve been traveling all over the country, and have been in dozens of airports, gas stations, and stores. I get tested regularly and have always been negative. Here are the precautions I use:
1) Wear a mask or face covering indoors in public. Now that vaccines are available, I no longer avoid unmasked people indoors, but as an unvaccinated person, I still wear mine. 2) Keep 6 ft away from others. (I basically ignore this one if other precautions are in place, especially on an airplane!) 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. This is now voluntary now that we have vaccines, as an unvaccinated person, I still follow this rule. 4) Outdoor gatherings are fine, even without masks, if everyone maintains a distance. I have hosted several outdoor gatherings. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however. 6) Wear an N95 or KN95 mask when going to more high risk areas like airports or public areas where people may gather. These masks are rated to filter out 95% of viral particles. In my opinion, surgical masks and especially neck gators are nearly worthless in these settings. 7) I never take my mask off on the plane, and find an isolate spot in the airport to eat or drink on layovers.
Vaccinated people can relax many of these rules! Vaccines are 90-95% effective, so you still have a small chance of infection.
Testing: There are several kinds of tests, and they tell you different things.
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test. They can take longer to process because they need specialized equipment that most small labs don’t have, so most of the wait time is just for shipping to a specialized facility.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody. These tests are cheap and fast, but are more prone to false positives and false negatives than PCR tests.
Antigen: These tests use a very similar technology to Antibody tests, but instead of detecting a patients antibodies against virus, they use antibodies to detect viral proteins in a sample. An “antigen” in immunology lingo is just a protein that can induce an immune response. So in this context, an “antigen” is a SARS-2 protein that can be bound by an antibody. Like PCR tests, these tests detect an active infection, because they detect viral proteins currently in the body.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR but more prone to false negatives.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Antibody Dependent Enhancement:I’ve written about this a lot and I won’t describe it in depth here. In short, this pathway allows some viruses to create more severe disease on the 2nd time infecting a person than the first. It is theoretically possible, perhaps even likely with SARS viruses, which is why I have been careful to avoid infection and why I’m not going to get the vaccine unless perhaps my work requires it.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Supportive care: Most treatment is supportive care, treating symptoms while the patient recovers naturally. Anti-inflammatory medications are often used to prevent the immune system from over-reacting to the virus.
Ventilators/nasal cannula: While widely used early on, some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor oxygen therapy using a nasal cannula, using ventilators only as a last resort breathing if labored.
Remdesivir: This antiviral was used widely for much of the pandemic, but many sources now claim it has limited effectiveness.
Dexamethasone: Steroid used to treat patients with low oxygen levels.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. Treatment with Ivermectin is likely more beneficial in a wider range of disease state than HCQ.
Ivermectin: A anti-parasitic medication used since 1981, Ivermectin has reportedly been used by doctors around the world, notably India and Mexico, to reduce COVID fatalities. Reports claim that Ivermectin is beneficial in a wide range of disease state, from pre-disease prevention to late stage disease. Like Hydroxycholoroquine, promising data was often labeled “misinformation” by outlets in Western countries, and western doctors were strongly discouraged from prescribing it. Thus, experimentation with Ivermectin was hindered and the drug’s potential is still unknown.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Several vaccines against SARS-2 were finally released to the public in December of 2020. The vaccines released to the public are in 2 types:
Attenuated vaccine: This type has been commonly used for decades for a variety of viruses. The technique makes a severely weakened form of the virus that still makes viral proteins that provoke an immune response. With this type of vaccine, the patient is infected by a weak form of the virus that they quickly recover from, usually with no symptoms other than occasionally the flu like symptoms that are your body’s natural response to invasion.
mRNA vaccine: This is a brand new technology that has been worked on for years. The SARS-2 vaccines are the first ones that have been introduced to the public using this technology. The vaccine includes a piece of mRNA inside a lipid bilayer that mimics the cell wall. The mRNA is inserted into the cell where it is translated into a copy of the viral Spike protein. These vaccines are 90-95% effective against infection, and even those infected have less severe symptoms. However, they are not 100% effective, so some infections of vaccinated individuals has occurred.
As has often happened, the vaccines have generated significant controversy. As you know, I have been careful to avoid being infected and also getting the vaccine because of the potential of ADE. My concern with the vaccine actually has nothing to do with the new mRNA technology, I actually have no reservations about the mRNA vaccines. From an ADE perspective both the attenuated vaccines (Johnson & Johnson) and the mRNA vaccines (Pfizer and Moderna) produce Spike protein that may trigger an ADE response should a new strain of SARS virus appear, not a variant, a new SARS strain, like a “SARS-3”.
When the vaccines were released, rumors of side effects, sometimes severe, arose immediately. For some time, I minimized these as a risk of any vaccine. All vaccines carry the risk of side effects and even death. However, a video podcast featuring Robert Malone, the inventor of mRNA vaccine technology, convinced me that the Spike protein itself has toxic properties of its own, separate from the vaccine technology used. This is because the Spike protein can bind to cells all over the body and may have wide ranging effects.
Despite ADE and issues with side effects, I actually still believe some will benefit from the vaccine. These include the following groups:
Anyone over 60 Anyone with 1 or more risk factors:
obesity certain auto-immune diseases use of NSAID medications heart, lung or kidney condition immunocompromised patients (HIV, cancer and transplant patients) respiratory condition such as asthma or COPD.
Frequently working with the public Musicians who sing in indoor settings Medical personnel
Again, I am not a physician, so check with your healthcare provider while making decisions about getting the vaccine or changing your medication.
If you’ve had the vaccine or had COVID and are concerned about ADE, remember that it will only become a factor if a significantly new strain arises (“SARS-3”). If this happens, then the procedure for you would be to be very careful initially, then get the “SARS-3” vaccine as soon as possible. The new vaccine will protect you from the new virus. In the future, vaccines against Coronaviruses will be produced even more quickly than this time.
The vaccines have pros and cons. I’m in support of vaccines for some but not necessarily for others. Each person needs to weigh the risks for themselves. I am not for companies or government agencies coercing individuals to get the vaccine.
Herd Immunity: The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. The idea is useful, but in my opinion, efforts to push people into getting vaccinated to achieve herd immunity are misplaced. Before a vaccine is available, the only way to reach herd immunity is to expose large numbers of people to the virus, which is counter productive. Now that the vaccine is available, those who are concerned should just get the vaccine themselves and not harangue others about getting it. Gentle persuasion may be convincing, but haranguing rarely is. Given even the pre-pandemic resistance to vaccines, a forceful effort to vaccinate is likely to back-fire.
Variants: During the course of the pandemic, several variants have arisen that have a slightly different Spike protein sequence from the original Wuhan strain. Confusingly, naming conventions have changed several times, making it difficult to keep them all straight. As a general rule, the variants have all been more infectious than the Wuhan strain, but have not been more pathogenic. Fortunately, the vaccines have been effective against all of the variants, although are not as effective against some variants.
The Delta Variant: The UK/Alpha variant caused waves of new infections in some countries and was more infectious than the original Wuhan strain. In late 2020, a new variant arose in India, the India/Delta variant. This variant was significantly more infectious than other strains and has caused huge peaks in cases in several countries. As of this writing, several countries are still experiencing waves of new cases most likely due to the Delta Variant, including the United States.
While the Delta Variant has caused large numbers of new cases and an increase in hospitalizations, data suggests it may be less pathogenic than the Wuhan or UK variants.
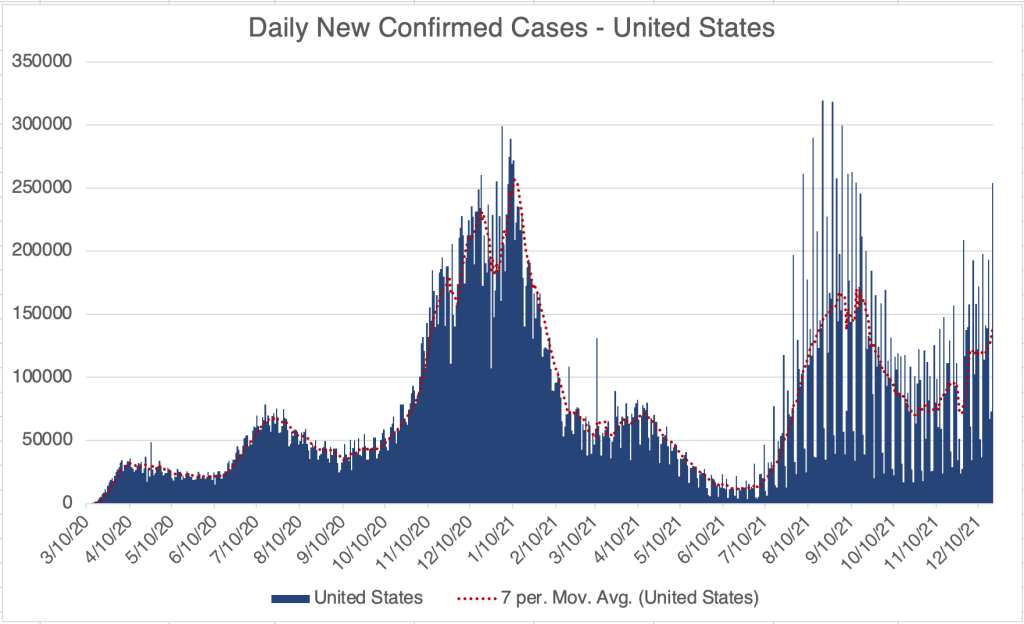
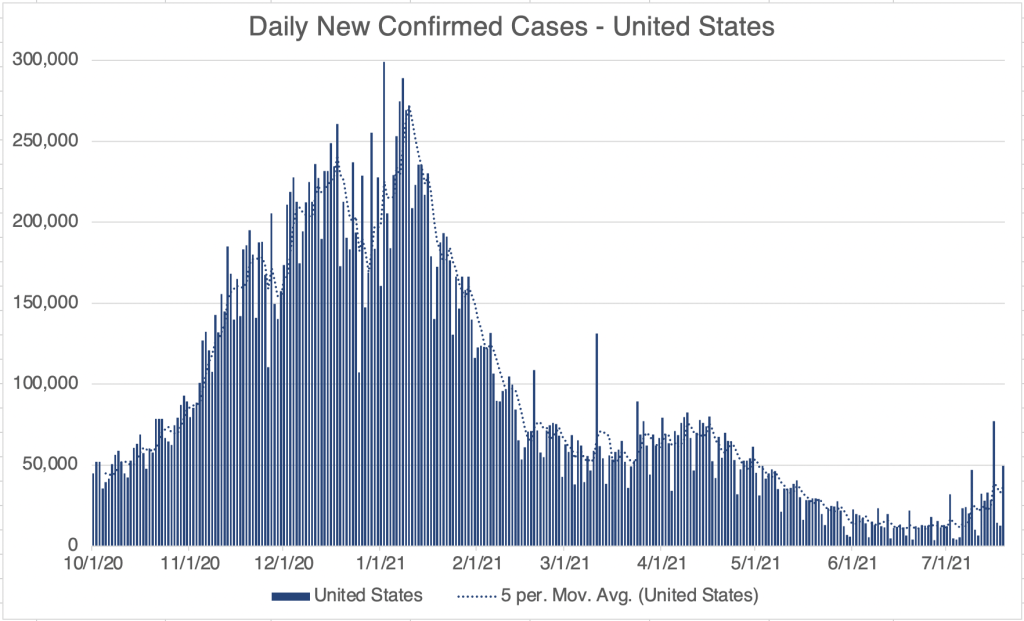
Current Status: In late Spring, at least in the US, life began to get back to normal, with approximately 50% of the US population vaccinated, much lower new case numbers, and reduced restrictions. Currently however (July 21, 2021) a wave of infections, likely caused by the Delta variant, is causing concern and some calls for new restrictions. Several other countries scattered across the globe are also currently experiencing peaks in cases.
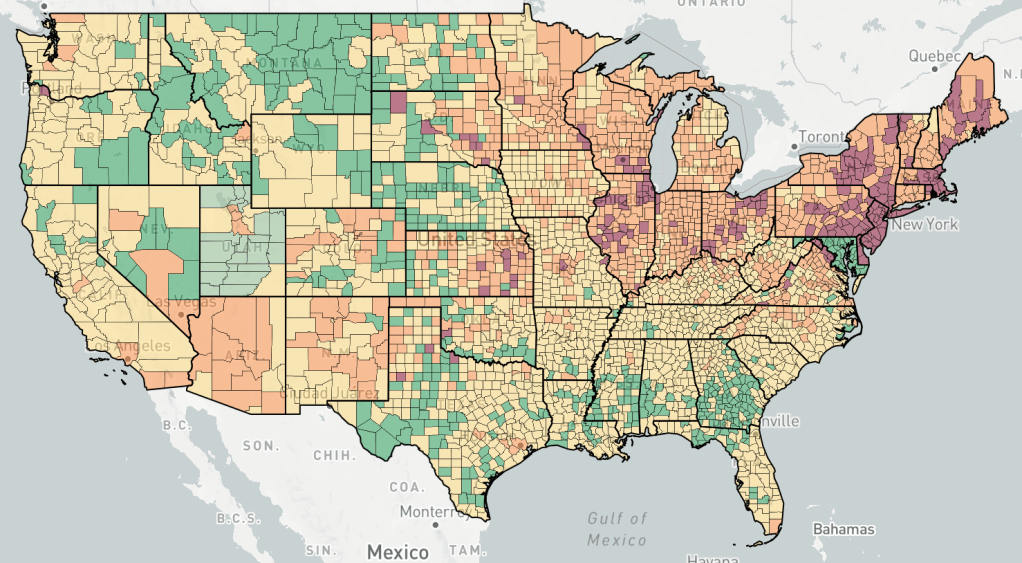
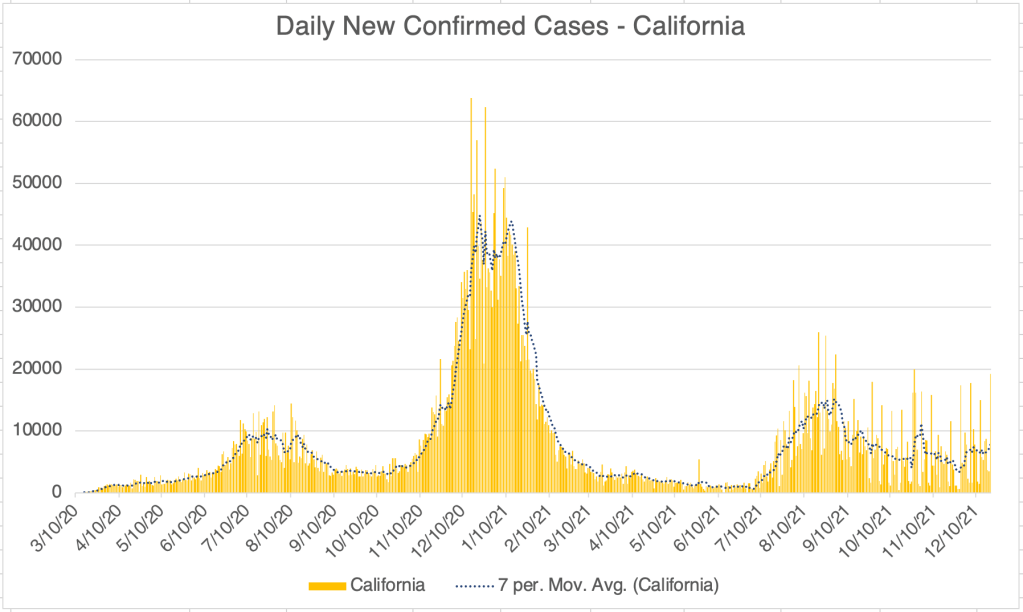
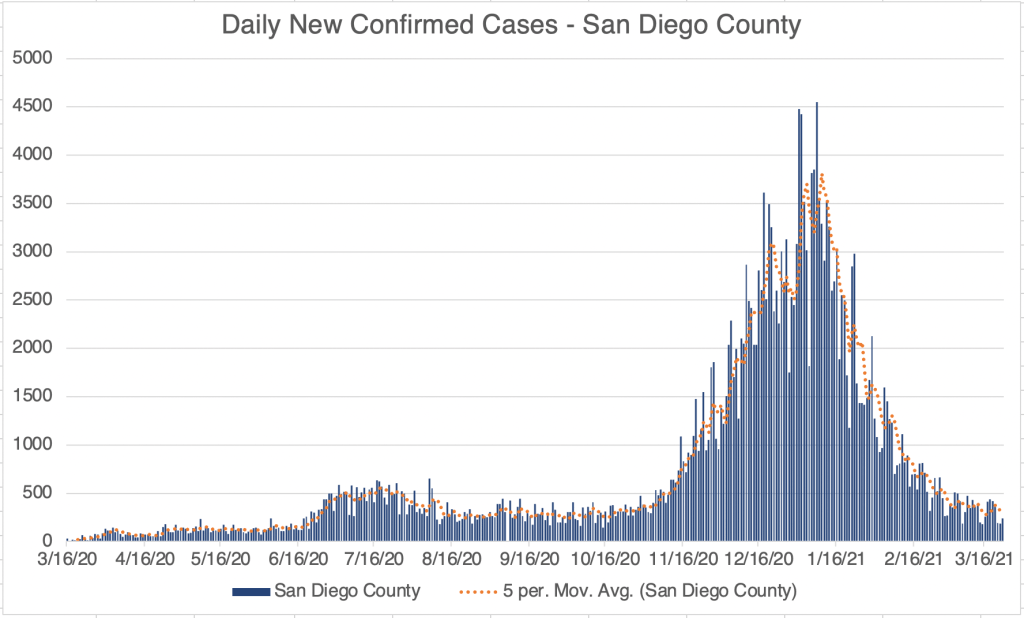
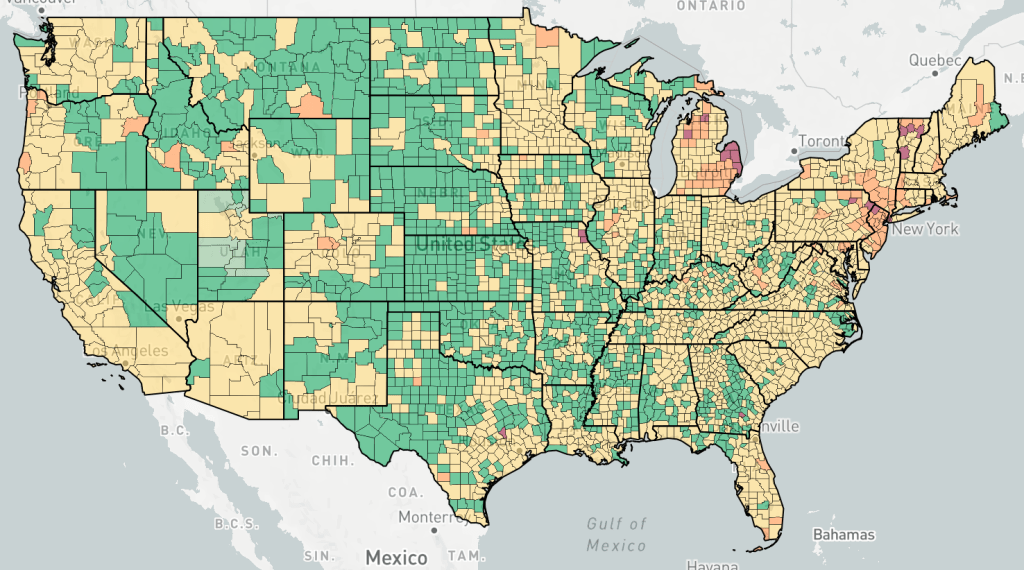
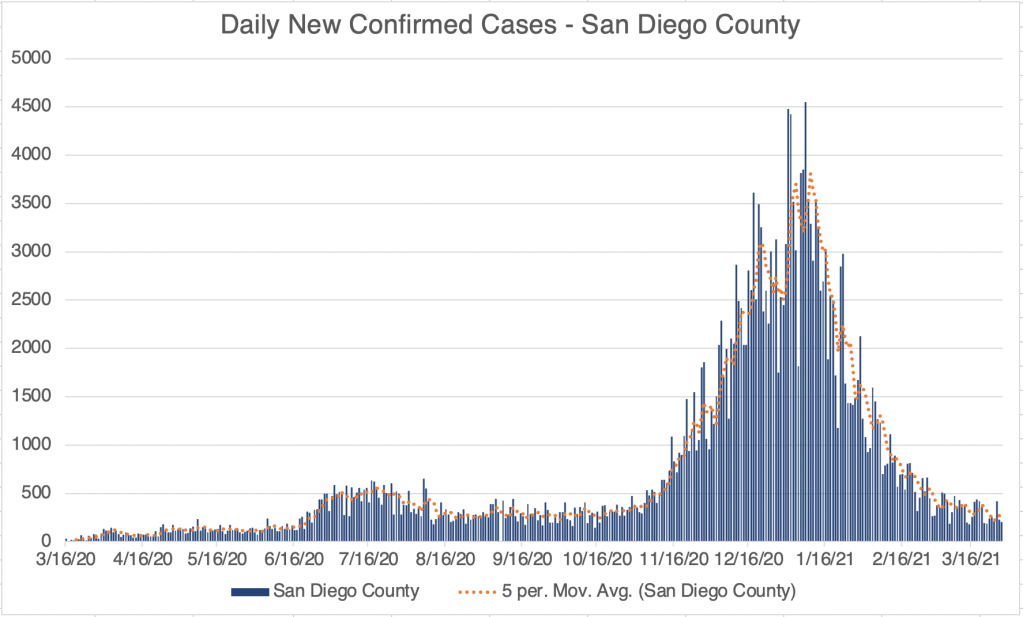
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format and includes only the Fall/Winter 2020, Spring ’21, and Delta Variant peaks.Endcoronavirus County Level Map, July 20th, 2021Daily new confirmed cases in India, from data collected from Johns Hopkins University COVID site. The Delta Variant peak is the large one on the right. Notice the sharp upward and downward trends. The new persistent daily case numbers are higher than before the Delta peak began.
The Future: Since vaccination started in the US, there have been many fewer new cases. This has led many to basically go back to behaving normally. The Delta Variant is rightly causing concern, but I’m still hopeful that the current peak in new cases will be short lived. In other countries with Delta related waves, the peak has been very sharp, with quickly increasing, then quickly decreasing case numbers. However, I’ve started to be a little more cautious in public again, while we wait for the increase in cases to slow.
Several other countries are still experiencing an elevated case load. The pandemic won’t be truly over until cases are low in all countries. I’m hopeful that this will happen this year, but it’s certainly too early to know for sure. So far, all new variants have been susceptible to the vaccines and natural immunity. There is a small chance however, that we may see new versions that are not. If this happens, SARS may become endemic, circulating seasonally like the flu does. So far, I don’t see evidence that this will happen.
In the future, we may have a “SARS-3” a new virus from the SARS family that will be similar, but different enough to trigger the ADE pathway. If this happens, those of you that have had COVID or been vaccinated should be very careful to avoid infection initially, then get the “SARS-3” vaccine as soon as it is available.
In a future post, I’ll give my recommendations for what should be done differently if a new pandemic should arise.
This is a COVID update. I also have a short note on the Delta Variant and sobering new information on vaccines.
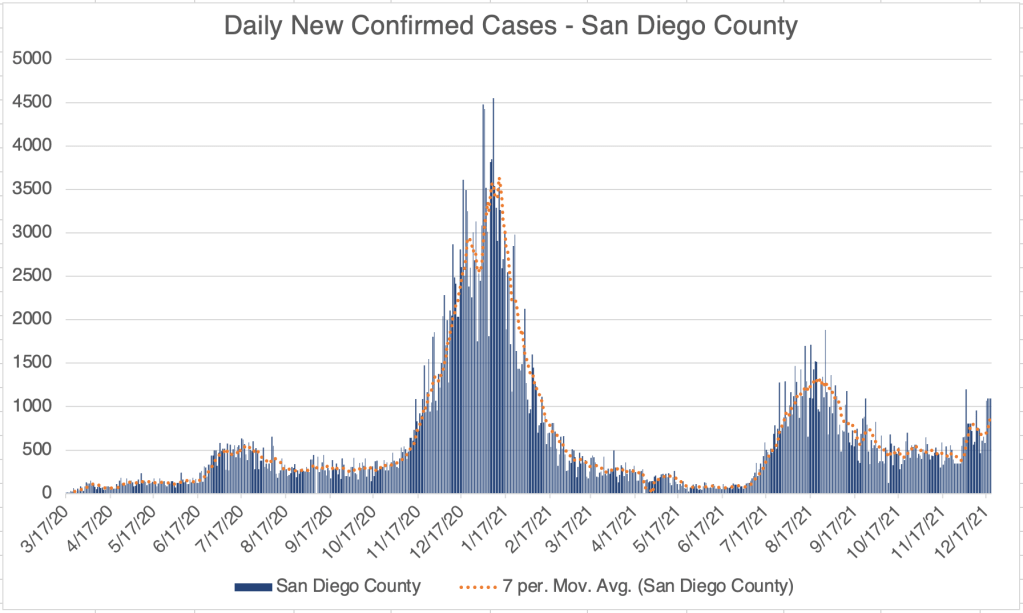
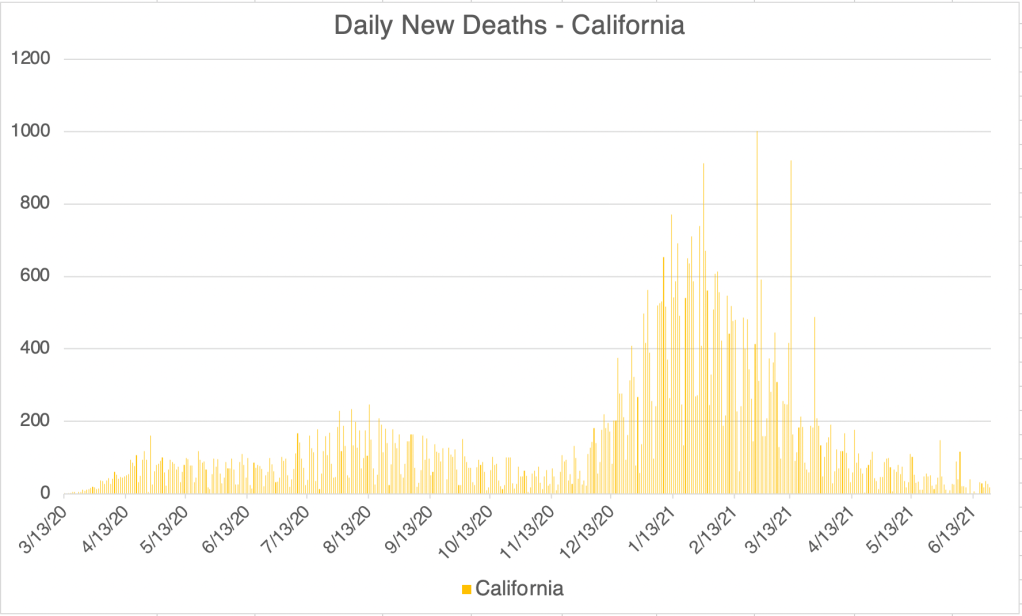
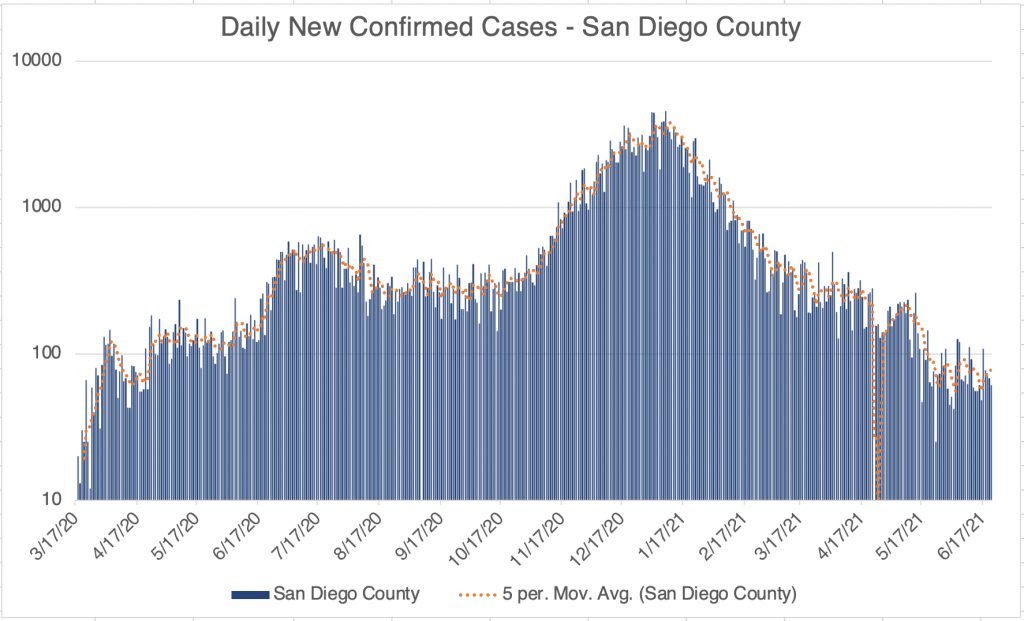
New case numbers continue to trickle down in the US, California, and San Diego County. New cases in San Diego County have been less than 100 a day for most of last week. Unfortunately, new cases aren’t really plummeting, just trickling down, but we are still making progress.
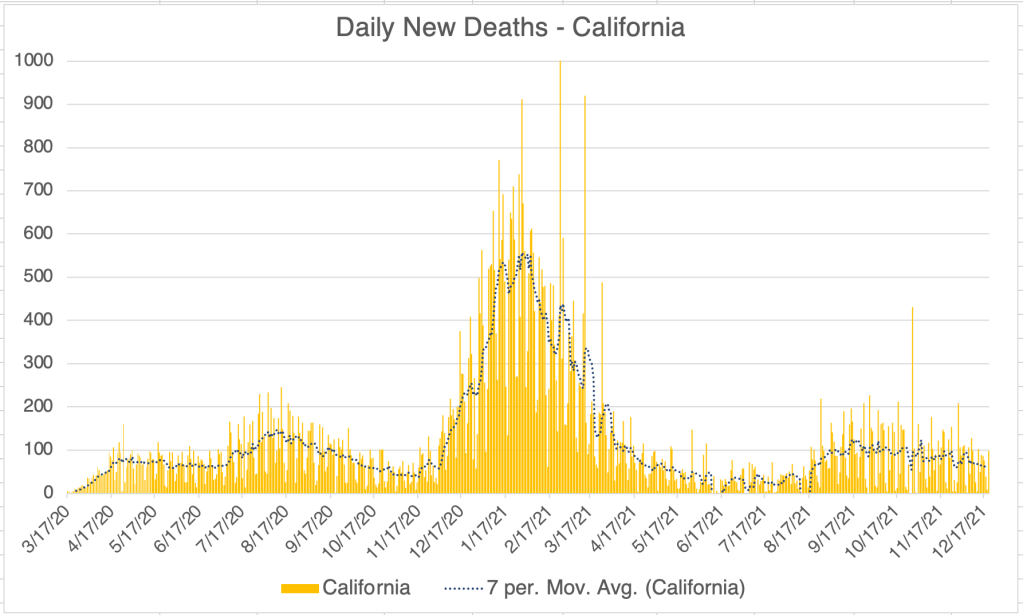
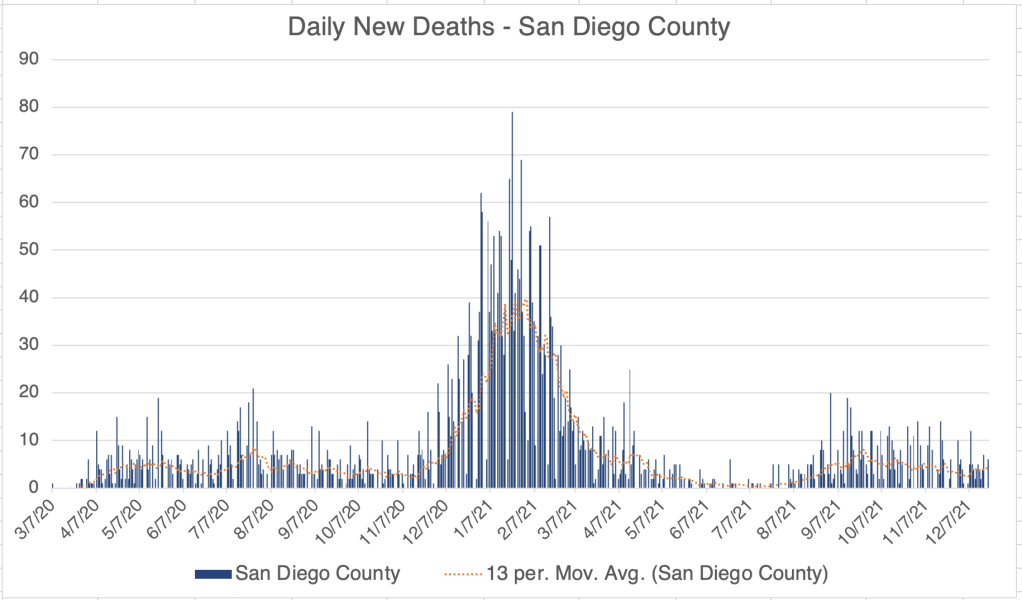
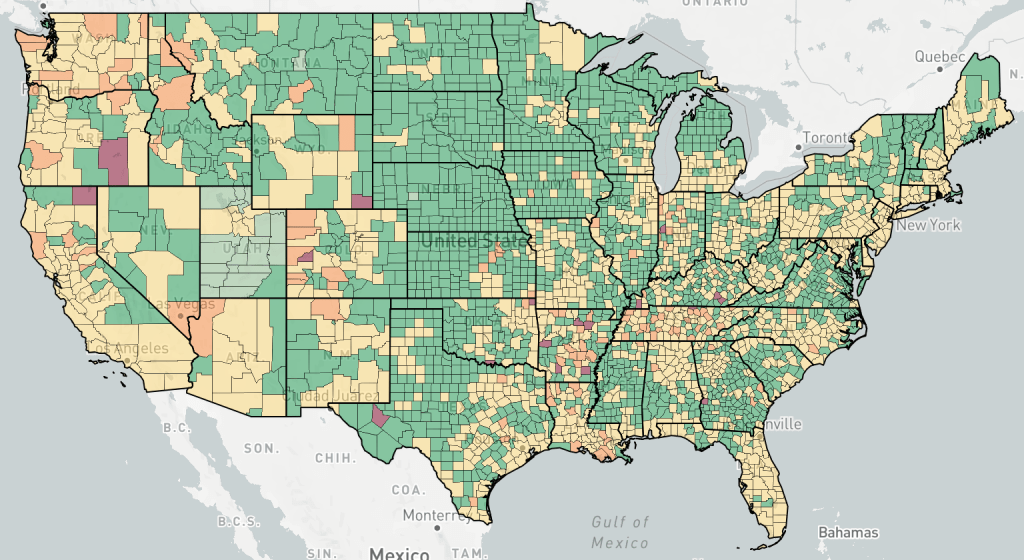
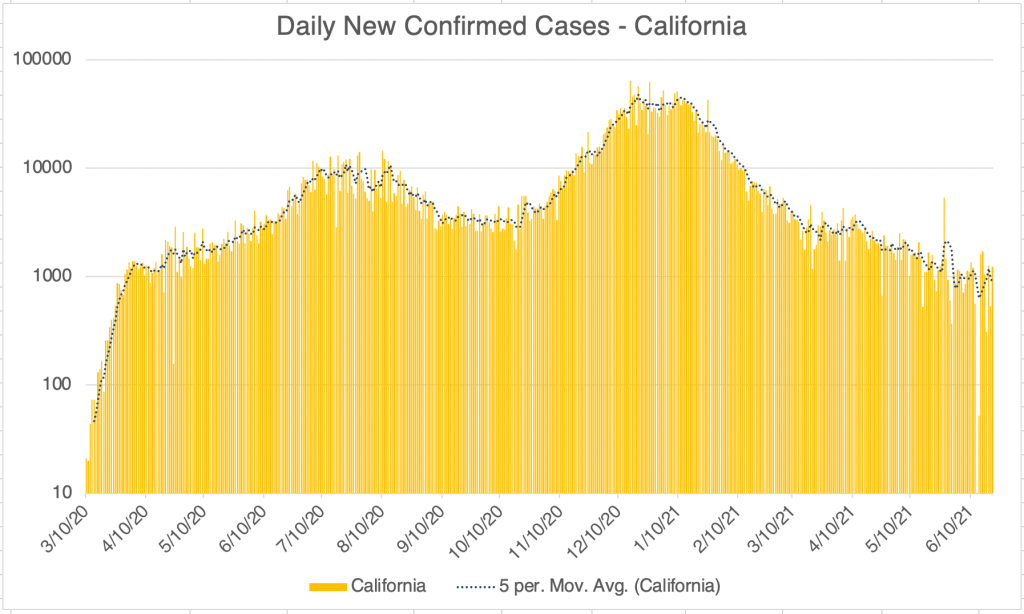
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site.Endcoronavirus County Level Map, June 18, 2021Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. The County is often making adjustments to various numbers and sometimes they do not update numbers for several days. As a result, this graph is becoming less reliable. This is likely impacted by the low number of cases, so that anomalies have a greater impact on overall trends. I may not post this graph for much longer.Graph is by me, from data collected from Johns Hopkins University COVID site.
I did some traveling this week, and in several places, including airports, about half of the people there did not have masks on. I was OK with this, since I know most people are now vaccinated, but this is reflective of our ongoing transition back into normality.
The Delta Variant: Way back in October of 2020, a new variant arose in India. First called the India Variant, the naming of variants has changed again in the last few weeks, and it’s now being called the Delta Variant (B.1.617.2). As with other variants, it’s much more infectious than the original Wuhan strain, but it doesn’t appear to cause more severe disease. The current vaccines appear to be effective against the Delta variant, so if you’re vaccinated, you are likely protected against this variant.
___________________________________ Updated from June 29th, 2021 post: As I’ve stated before, the Delta Variant is significantly more infectious than the original Wuhan strain, as well as more infectious than the UK Variant. I said last week that it is not more pathogenic. I have to adjust that assessment. While it hasn’t so far produced more deaths than other versions, it does seem to produce more hospitalizations, so it does appear to be more pathogenic at least by that measure.
I’m going to way out on a limb and suggest that the Delta Variant will not cause large numbers of new cases in the US because of our natural immunity and our large number of vaccinations. That being said, there have been reports of fully vaccinated individuals contracting the Delta Variant. None of their symptoms were severe. I may of course end up being wrong about this and I will keep you posted on new confirmed case numbers.
Some municipalities are considering new lockdown measures. I have not supported “lockdowns” since last Spring, but as an unvaccinated person, I still wear a mask in indoor spaces in public. ____________________________________
Vaccines and Spike protein toxicity: Now for a topic that is even more likely to get me cancelled than last time. I ran into a video with Bret Weinstein, Dr. Robert Malone, and Steve Kirsch. Robert Malone is the scientist that was instrumental in the development of the mRNA vaccines, like the Pfizer and Moderna vaccines. He speaks very authoritatively on the vaccine issue.
Dr. Malone is very pro-vaccine in general, and certainly believes that the mRNA vaccine is effective in principle. However, he also has come to believe that while mRNA vaccines in general are safe, the SARS-2 vaccine in particular does have a big liability. This is that the Spike protein made by the SARS-2 vaccine has a toxic effect on multiple cell types. This explains the higher than normal rate of complications related to the SARS-2 vaccines.
Part of the reason SARS-2 is such a difficult virus is that the Spike protein attaches to a cellular receptor called ACE2. The ACE2 receptor is present on many cells types in the body. This is why the SARS-2 virus can infect so many different cell types, including immune cells.
In response to the vaccine, cells make Spike protein so that the immune system can develop a response to the virus. This is true of all vaccines. However, since the Spike protein can attach to so many different cell types, there is a wide range of symptoms a person may experience in response to the vaccine. Of course, most experience no symptoms at all.
So what if you got the vaccine? Should you be concerned? It’s too early to tell how prolonged an impact Spike protein in the vaccine will have on an individual person. My guess is the impact will subside after a few days, when the Spike protein in cells is degraded. However, since the Spike protein interacts will cells and impacts their functioning, some reactions may take longer to resolve. If you had no reaction to the vaccine, you probably won’t ever have one.
If you haven’t had the vaccine, should you still get it? There is no denying that the vaccine has had a positive impact on the re-opening process and has likely saved many lives. On the other hand, it obviously carries risk. If you are in a high risk group or work with the public, you are still very likely to benefit. As you know, I haven’t gotten the vaccine because of the ADE issue and also because I’m reasonably certain I can avoid getting the virus, especially now since cases are so low. I will be less likely to get the vaccine now.
I believe that the censorship of ideas present in our current culture has had a profound and negative impact on the progress of the pandemic, and on our culture in general. As I’ve said repeatedly, politics and science are a terrible mix. We’ve seen many examples this year. I deeply hope we can find our way out of this mess as soon as possible.
This is a COVID new case update. I’ll also discuss new cases world wide, and discuss a new video from immunologist Shane Crotty with lots of important information on vaccines and variants.
In the US, we’re starting to see an increase in new case numbers in several states, Michigan and New York in particular. This may be because of the relaxing of requirements by many municipalities, but may also be because of some of the new variants arriving in the US. More on the new variants below.
New case numbers have stabilized in California and San Diego County with around 2000 new cases a day in California and 300 in San Diego. We have yet to see a clear uptick in cases in those 2 regions, but we may see this soon.
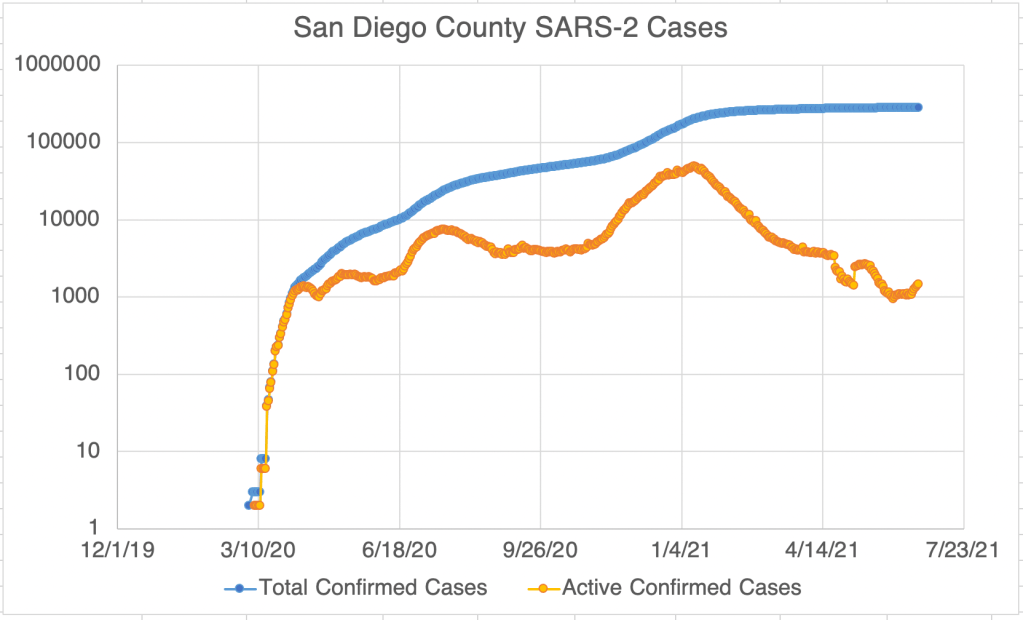
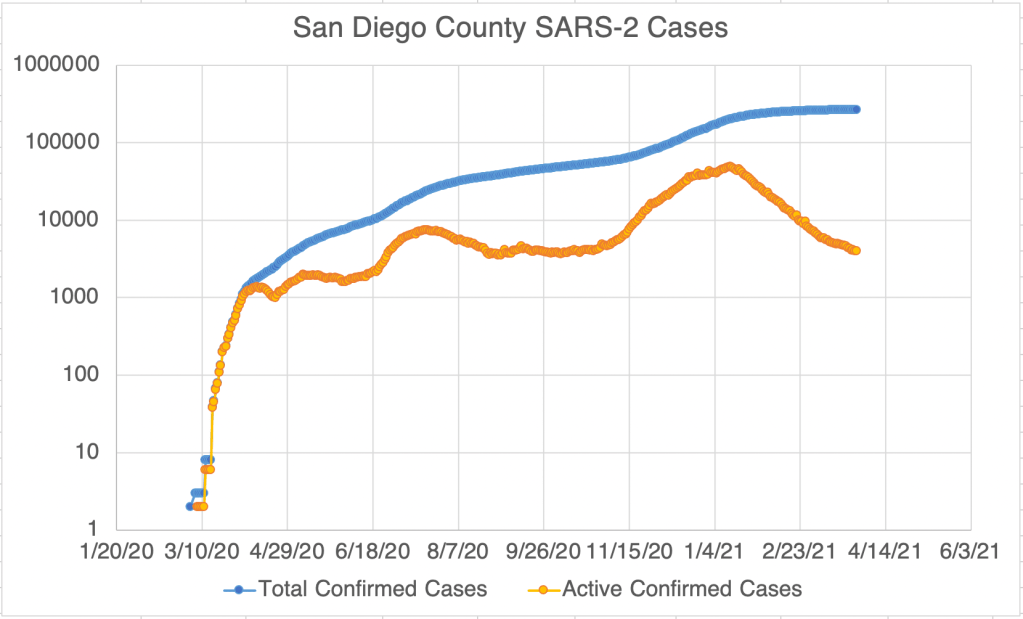
Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from Johns Hopkins University COVID site. “Active Confirmed Cases” numbers have been calculated based on the assumption that patients confirmed to have SARS-2 virus at least 17 days ago have recovered. Recently, however, this would produce an active case number that is too low to make sense in comparison to San Diego. This graph estimates 17 to days to recover in January, but gradually moves to 22 days for mid-March. I’ve lost confidence that I can make an Active Case plot that is accurate, so this will probably be the last time I post this for California. Let me know if you think it’s still useful.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. “Active Confirmed Cases” numbers are reported by San Diego County. Because our new active case numbers are getting low, I’ve switched to a logarithmic view. This emphasizes small values and makes them easier to see. Notice that the case number on the left now go up 10 fold with each higher line on the graph.
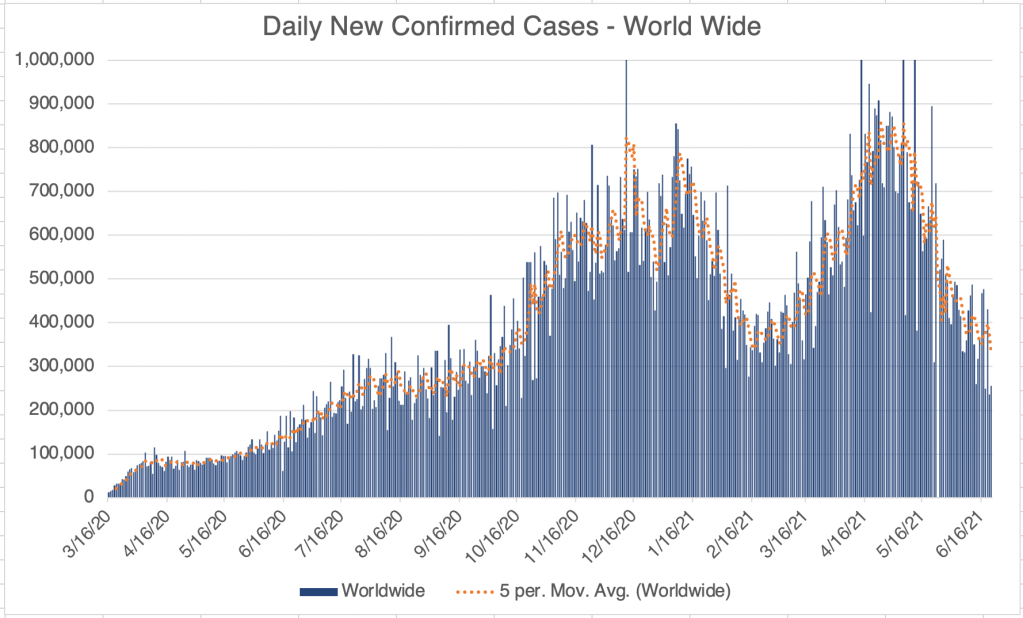
Internationally, the US and UK are doing better than average at the moment, but many countries scattered all over the world, with concentrations in Eastern Europe and South America, are seeing new surges in cases. The US and UK are both vaccinating heavily right now, with vaccine rollouts moving slowly in continental Europe, so vaccination may play heavily in this pattern. Also several new variants of the SARS-2 virus are more infectious than the original strain and likely factor in these new surges.
Important new video with Dr. Shane Crotty: MedCram has posted a new video interview with Dr. Shane Crotty, an immunologist in San Diego. His work looks into immune system responses to vaccination as well as native infection. He has several very interesting points to make about SARS-2 immunity and vaccines. First, he says that those infected with SARS-2 do have significant lasting immunity for many months, although it does go down a bit over time. Different people can respond very differently, however, and reinfection is possible in some.
Regarding vaccines, he said that those who have been infected have a good but not great immune response, but it is significantly boosted by a single vaccine dose, gaining an immune response higher than those vaccinated alone. So there is a good reason to be vaccinated if you have already been infected. Of course, if you’ve been infected, you may choose to wait until at-risk people have been vaccinated before you get a vaccine booster.
As for variants, he says there are 2 broad categories of variants, those similar to the UK variant (now commonly called B.1.1.7), and those similar to the South Africa variant (B.1.351). Both new strains are more infectious than the original Wuhan strain. The big difference between them is that those who have had SAR-2 are immunized against the UK strain, but not the South Africa strain. Also, the Astra-Zeneca vaccine does not protect well against the South African strain, and the Pfizer and Moderna vaccines appear to be less effective as well. The good news is, the Johnson and Johnson and Novavax vaccines do appear to protect against the South Africa strain. This suggests that although the South Africa strain is different, it isn’t so radically different that we have nothing to fight it with.
_____________________________ Update, April 6th A new small study from Pfizer suggests that their vaccine does work on the South Africa variant. The patient number in this trial is small, so they still don’t know exactly how effective it is. _____________________________
Soberingly, the South Africa strain has reached the US, so if we see a surge in the next few weeks, this strain may be at least partially responsible.
Impact on ADE? If you’ve read my posts on ADE, then you know that the danger from ADE may come when a different strain arises. With the South Africa strain arriving in the US, we may be able to see if ADE will have an impact with SARS-2 in the next few weeks and months. So far, new death numbers have come down with Wave 3, and there is no apparent impact from ADE on case severity. I will certainly be watching to see if this changes.
This is a long post about the philosophy of science. I probably should have written this one a long time ago, but here it is.
During the pandemic, we’ve often heard scientists and commentators say “I’m just following the science.” Confusingly, we’ve heard people on all sides of the issues say this, pro-maskers, anti-maskers, vaccine fans, vaccine detractors, people who love Hydroxychloroquine, and those who think it kills people. Very often, when people have used the word “science” in the last year, they’ve used it in a way that you DIDN’T learn in high school biology class (thanks, Mr. Walker!). So what do people mean when they say this, and how can you evaluate what they are saying?
When you hear the word “science” on the news or in discussions on the pandemic, other definitions are often smuggled in. I’ll give you a few different ways people use the word “science”, and then I’ll talk about how you can evaluate science related discussions.
1) In actuality, science is a method for measuring things in the natural world, and using reasoning and the scientific method to make, falsify, and confirm hypotheses about natural things. Science has been phenomenally successful at describing aspects of the natural world, as well as producing useful applications for communication, travel, health, manufacturing, the arts, and nearly every conceivable human endeavor. The incredible success of science has given it enormous cultural power as well, and many ascribe to it powers that it does not have. By definition, science measures and describes the natural world, but cannot describe many common aspects of reality, questions like “what is justice?” or “what is the meaning of life?”.
While many contributed to the Scientific Method, the steps were formalized by Francis Bacon. The steps include 1) the formulation of a question, 2) the development of a hypothesis, or a guess about what actually happening, 3) a prediction about what impact the hypothesis may have on a system, 4) doing experiments to test the hypothesis, and last 5) analyzing results, to include falsifying or confirming the hypothesis and forming a new question.
The scientific process is not a slow gradual accumulation of truth. It’s often ugly, with long searches down the wrong path before finding the right one. Fields can experience sudden, jerky changes in direction.
2) The collection of facts currently believed by the majority of scientists. When many in our current culture use the word “science”, this is what they mean. The phrase “settled science” often refers to this. But scientific truth is not decided by a vote. Yes, if a “fact” is believed by most scientists, it’s more likely to be true, but science history is full of people who had “weird” ideas that later turned out to be right. By definition, topics under current study are not well understood, and there can be widely varying opinions about what’s going on.
It’s always OK for a scientist to question current thought. Trust me when I say that having a PhD does not mean that other scientists have to believe you. I’ve heard shouting matches at conferences over what to believe about seemingly simple things.
Real “Truth” transcends opinion. Things are true whether you believe them or not. Science is the search for the truth about the natural world, not the search for ways to force your view on others.
Which leads to…
3) The collection of facts currently believed by scientists who agree with me. When things are murky and not well understood, which is quite often in active fields, there can be 2 or more models of how a system is working. Sometimes the evidence that is out in the world can appear to be contradictory. This may be because some of the evidence is wrong, or because conclusions based on the evidence is wrong, or because a crucial piece of evidence is still missing, or because the system is just more complicated than anyone is aware of. At this point, a good scientist will try and rethink the available evidence or perhaps design a new experiment to try and get at something still unknown. Instead, some people, even good scientists in a moment of weakness, will simply declare that their view is correct prematurely. Scientists must always seek to be more persuasive, and not just shout louder.
4) The collection of facts currently believed by me, right now. This definition is common for those who believe an outlier view. It’s not bad to have a view that is outside the current orthodoxy, this is how scientific breakthroughs happen, but a person in this position must seek even more to persuade with evidence, not just be dogmatic. Do more internet work, read more literature, or design another experiment.
5) An atheistic worldview, as in “I believe science”. Science is great at discovering information about the natural world, but it can’t answer the big questions. What some call “science” in this way is really “naturalism”, the belief that only matter and energy exists. It rejects any worldview that includes a transcendent or supernatural component. Science alone does not support this worldview, because by definition, science can’t “prove” the non-existence of things outside the known universe. Other philosophical structures are necessary to support this view.
So how do you figure out what’s really true about a scientific opinion being presented. This can be difficult, but it can be a little easier to figure out if someone is abusing “science.” Here are some clues that science might be being misused. You’ll have to dig deeper to be sure:
A real scientific argument includes a conclusion supported by evidence. Does the person talking give any evidence for their position? Often, people just make an assertion, a claim without evidence. This is OK if they can back it up, but very often they can’t. Ask “can you clarify that?” or “how did you come to that conclusion?”
When questioned, a person should have evidence for their claim. If instead they call you anti-science, or *phobic or *ist, then they are abusing science.
If a story or comment starts with “X person is brilliant and has been in the business for years”, this is often a red flag for me. While a person’s qualifications are important, they must still present evidence. A title or degree is not enough for them to be automatically believed. The more glowing the terms used to describe a source, the more I’m suspicious that they are about to spout nonsense. Yes, this even applies to me. If you tell someone “This Facebook friend of mine is a real scientist and he says <something really smart>”, you should rightfully expect your friend to ask what evidence I had for my claim. If you don’t know, then re-read my post, or just message me! I’m happy to work through it with you, and I’ll tell you outright if I’m just speculating.
News articles are OK, but they are only a starting place. If a person references a news article, they still have homework. What news outlet? What evidence did the author use? Journalists often misunderstand or misrepresent information from scientific sources.
Real evidence can be a scientific paper, a study learned about on the radio (who presented it?), or a comment by an authoritative source (who is the source?). Each of these can in principle still be wrong, but they have more weight than other sources.
Often, we gain knowledge about the world from someone we trust, an authority on the matter. This is a fine way to learn things. Your parents were the first authority that you used for learning much of what you needed to know. But authorities, even good ones, are not always right. You learned this about your parents when you were a teenager. It’s OK to pick someone you trust as an authority on scientific matters, but still don’t believe everything you hear. The CDC, the WHO, Dr. Fauci, the President (either one), yes even me, have been right about some things and wrong about some things during COVID. During an evolving situation, expect opinions and “facts” to change as more information is gathered. Your favorite authority doesn’t know everything.
Of course, the debate on several COVID related topics have become politicized, which can make it difficult for scientists to do good work, and often VERY difficult for lay people to know the truth. I feel for you. It can be really difficult for folks to figure out what’s true about something that’s not in their field. I feel the same way about climate change, an important topic of frequent debate that’s not in my field. Don’t feel dumb if you have trouble figuring out what’s going on. Lots of folks are abusing science, trying to make you agree with them. Hopefully I’ve given you a few tips on how to discover the truth. Here’s an article on how to communicate scientific things!
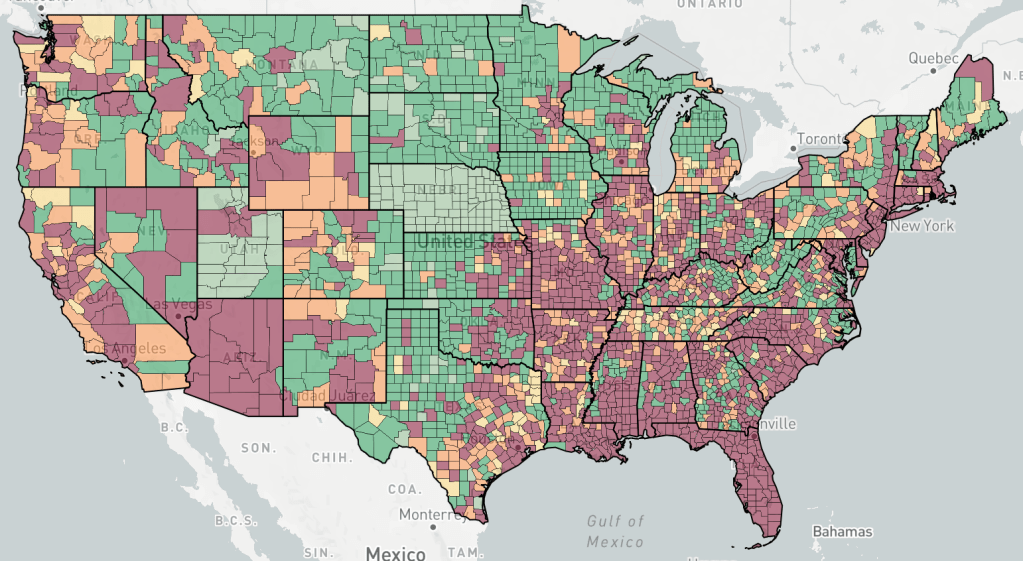
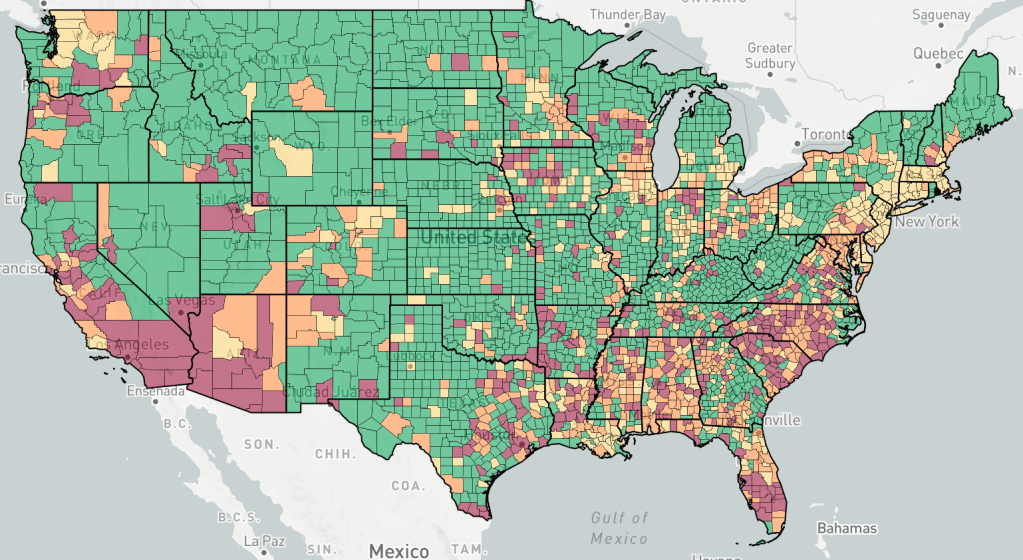
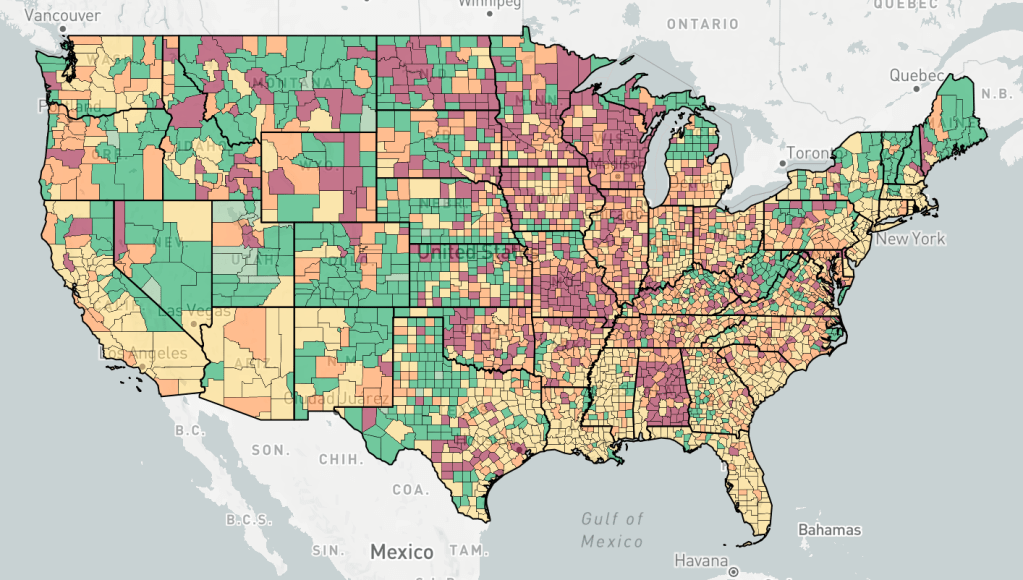
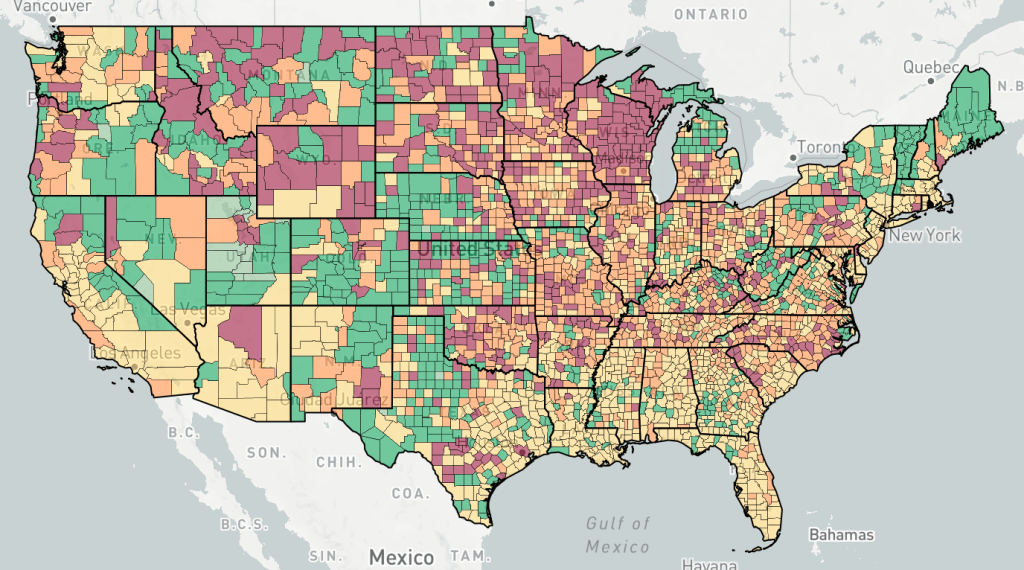
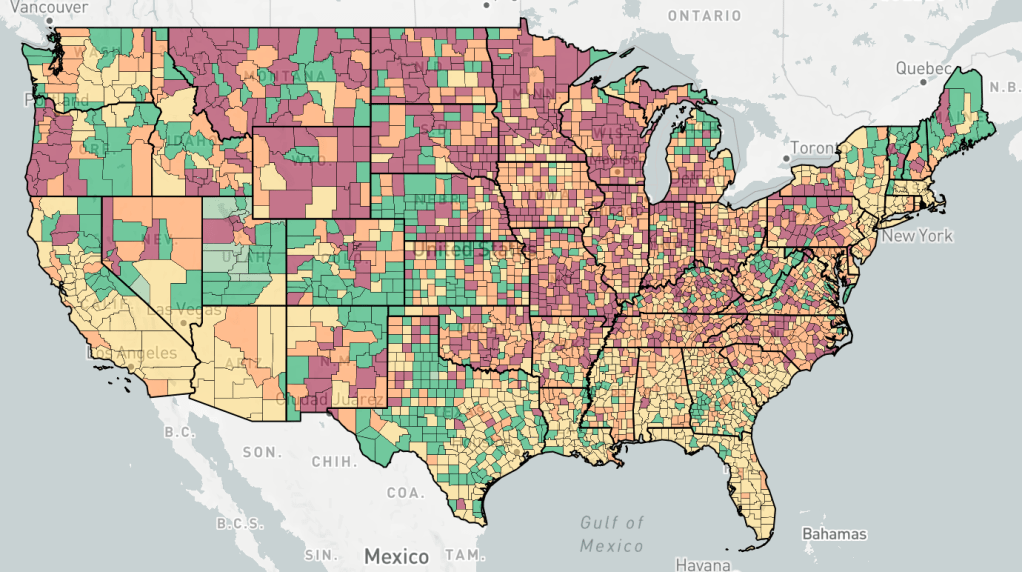
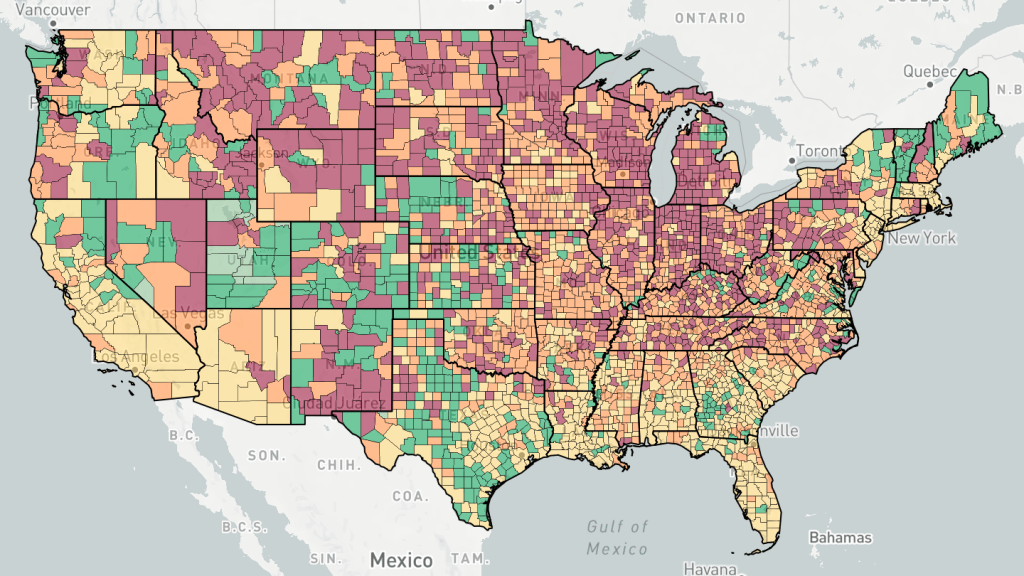
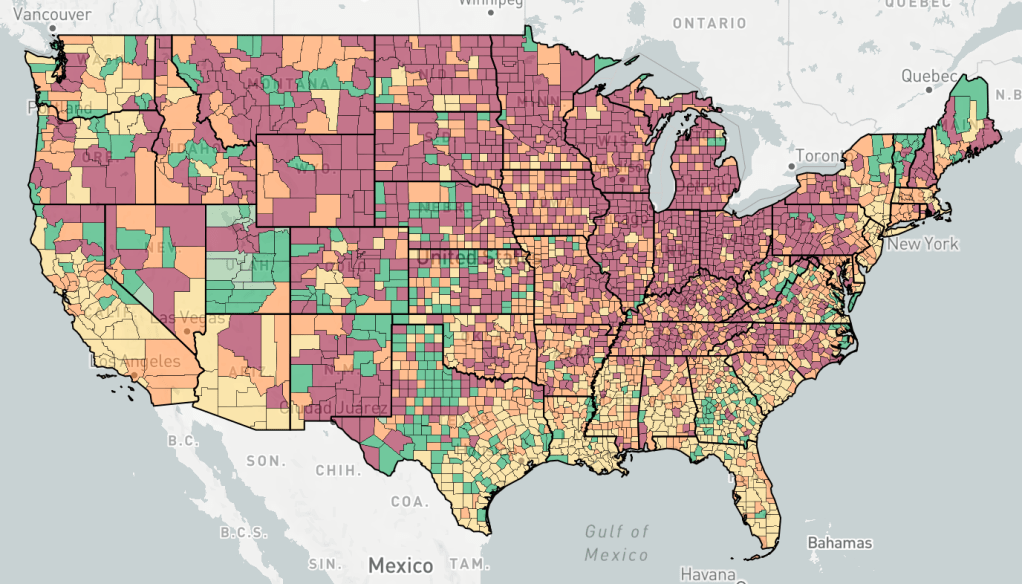
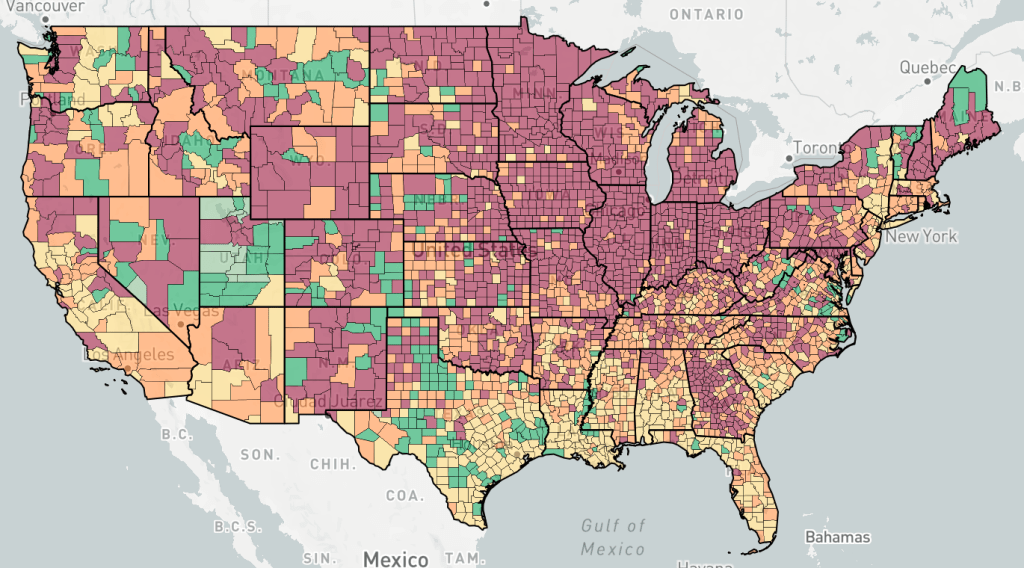
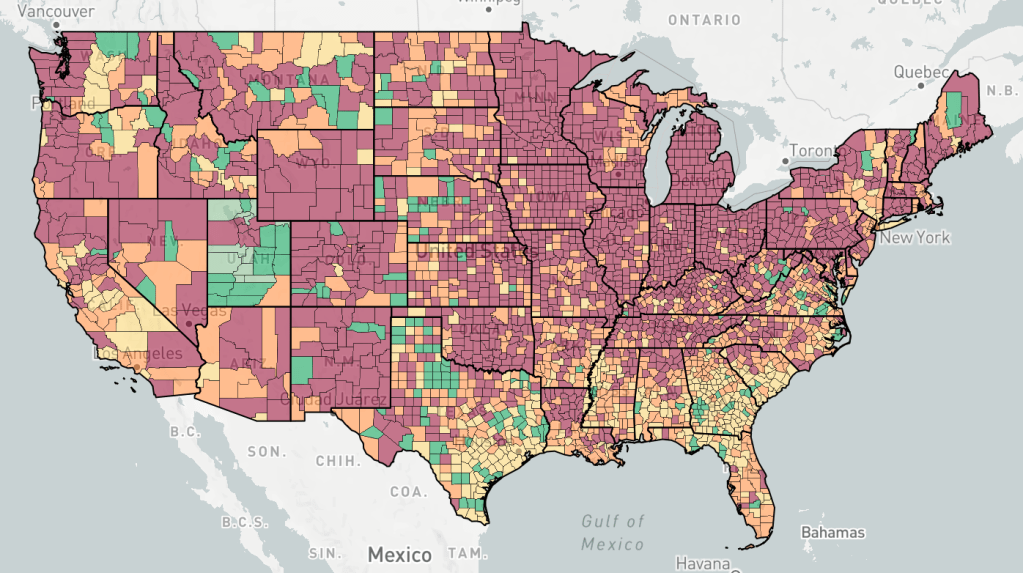
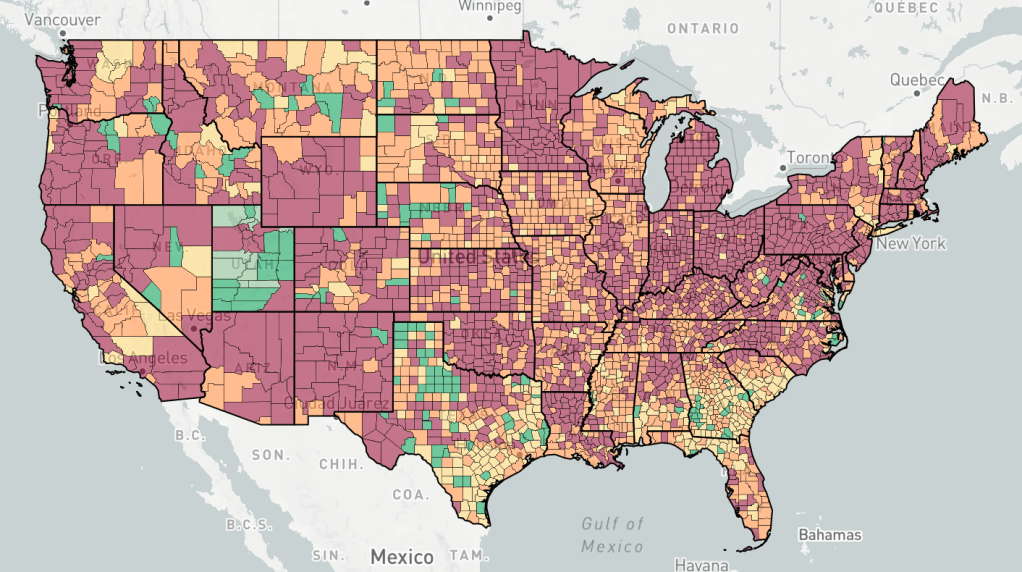
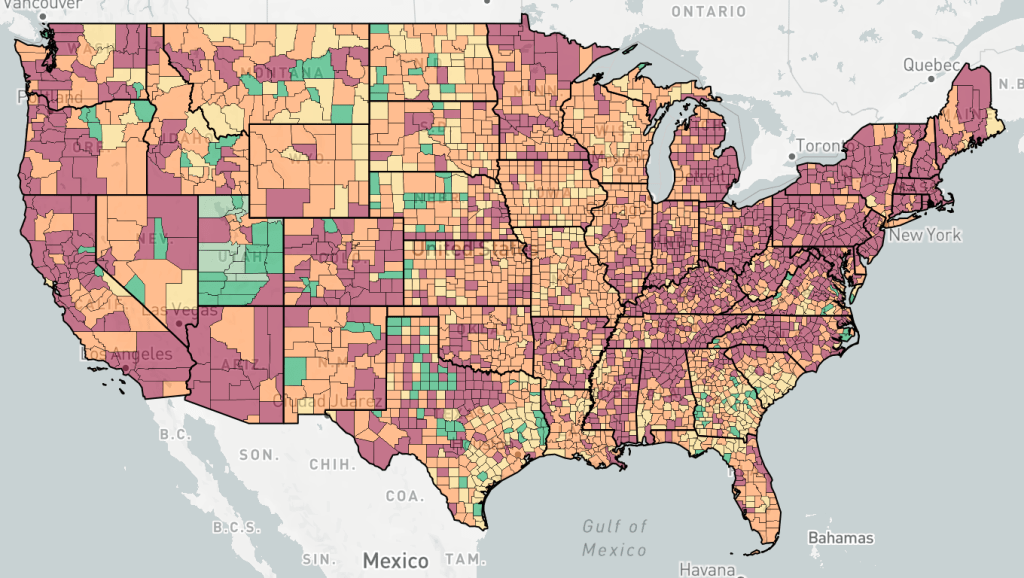
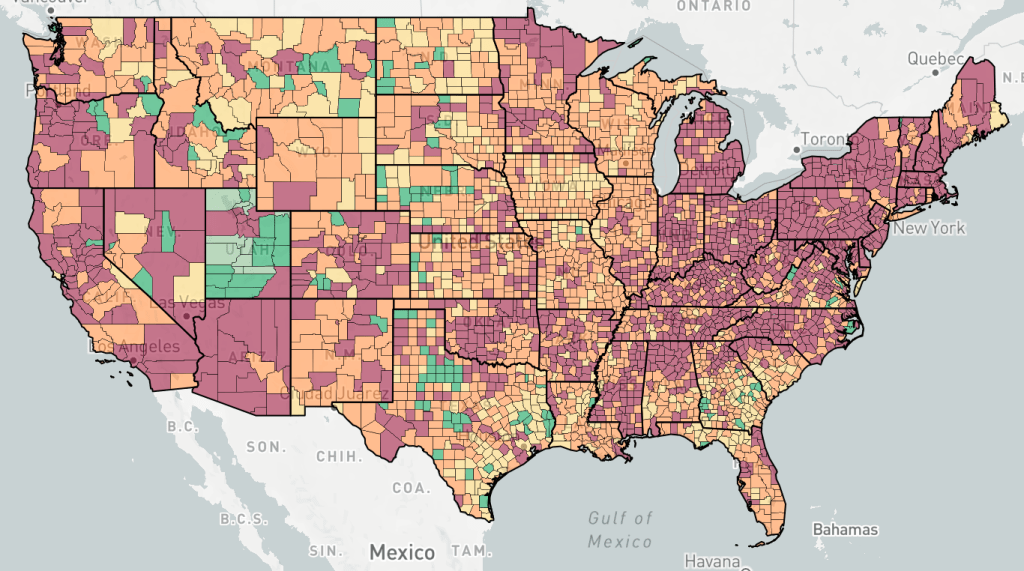
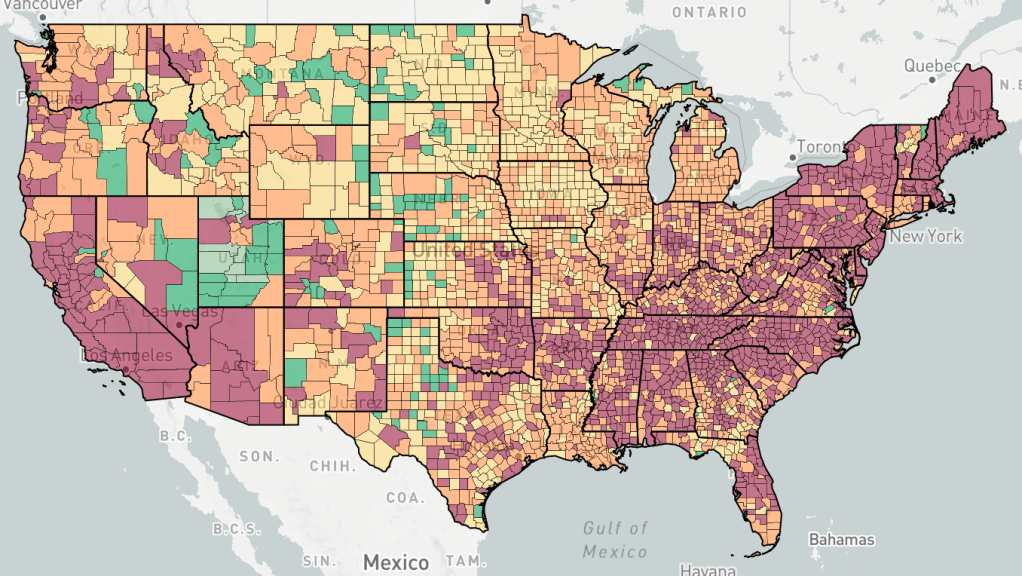
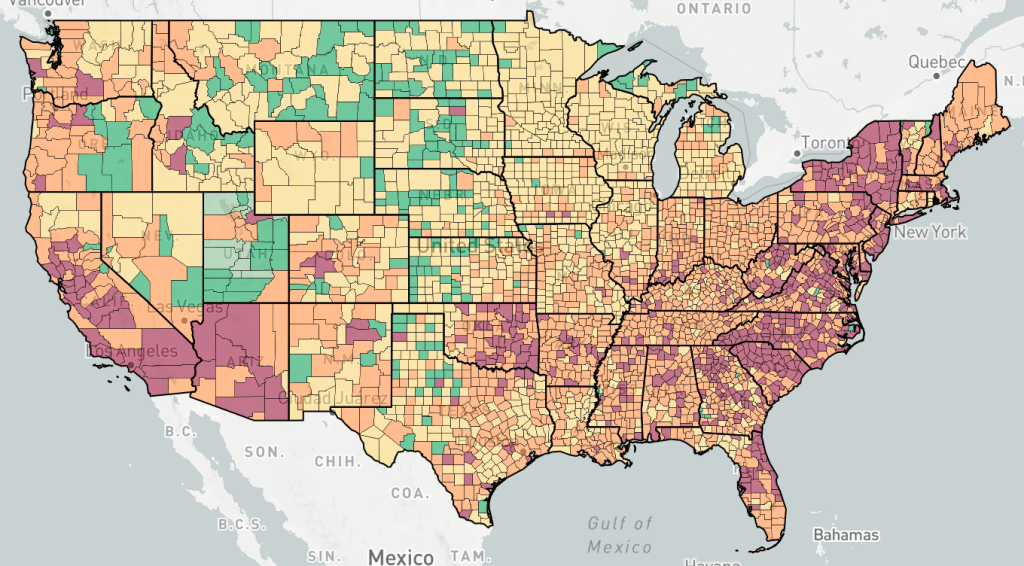
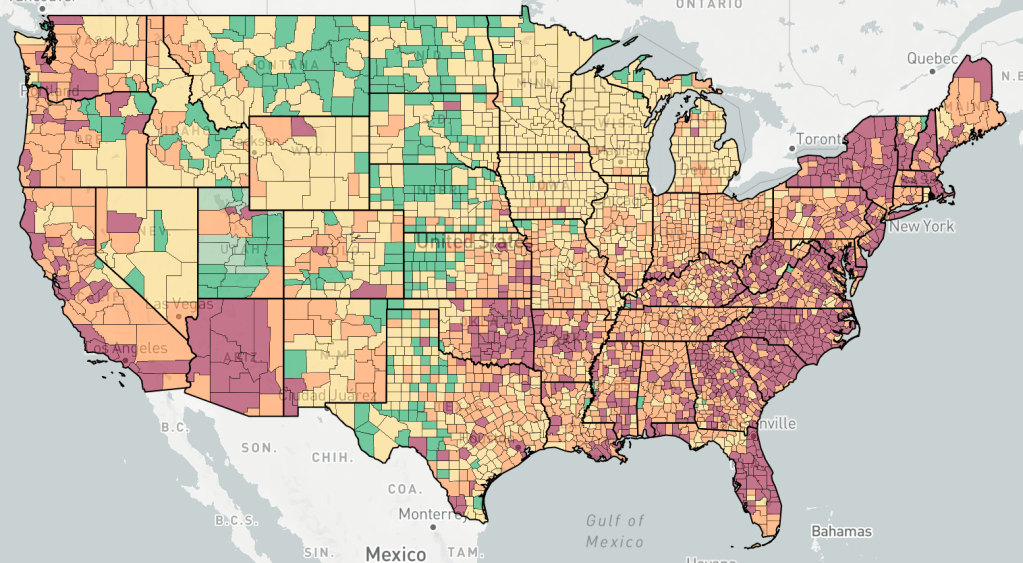
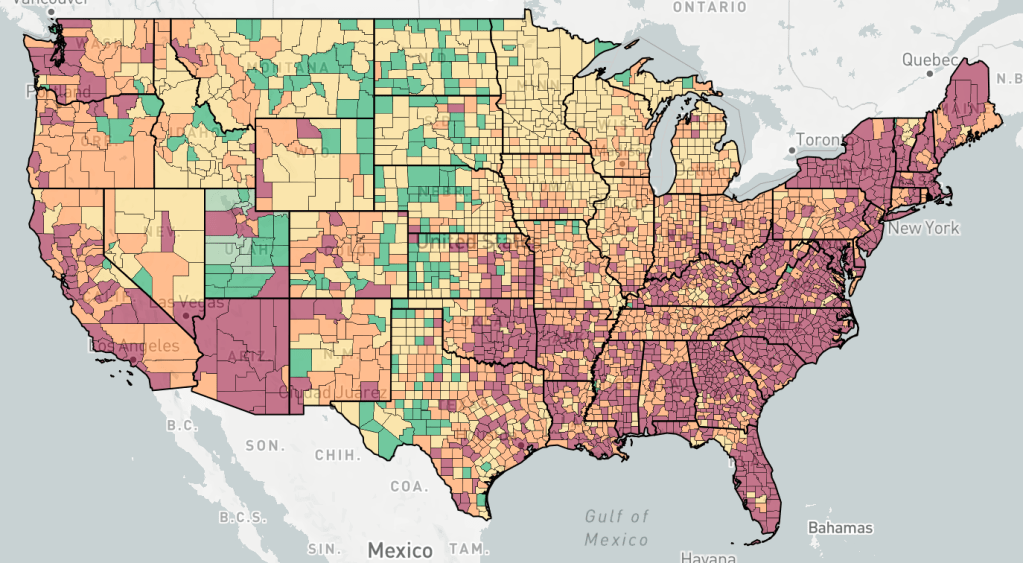
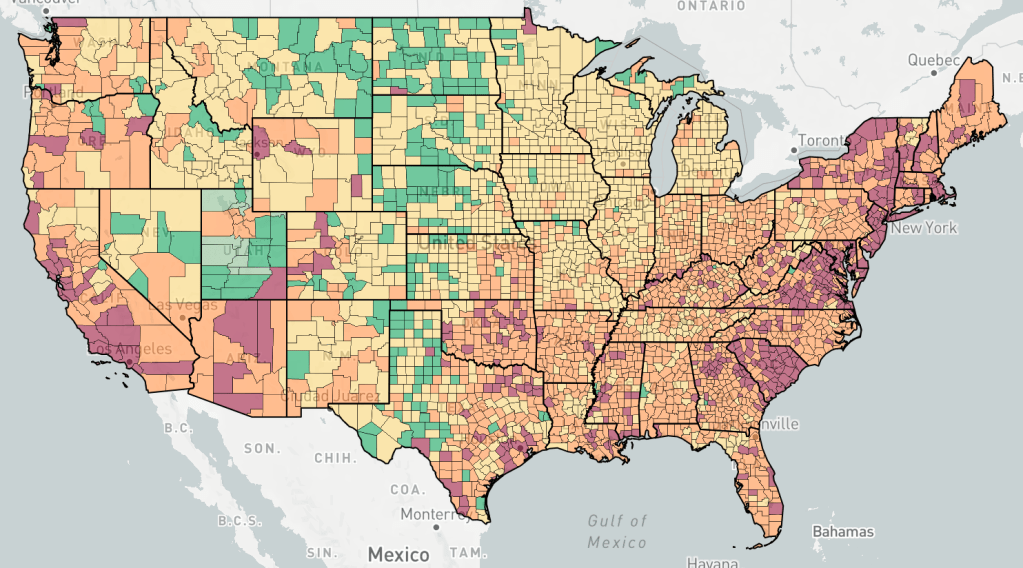
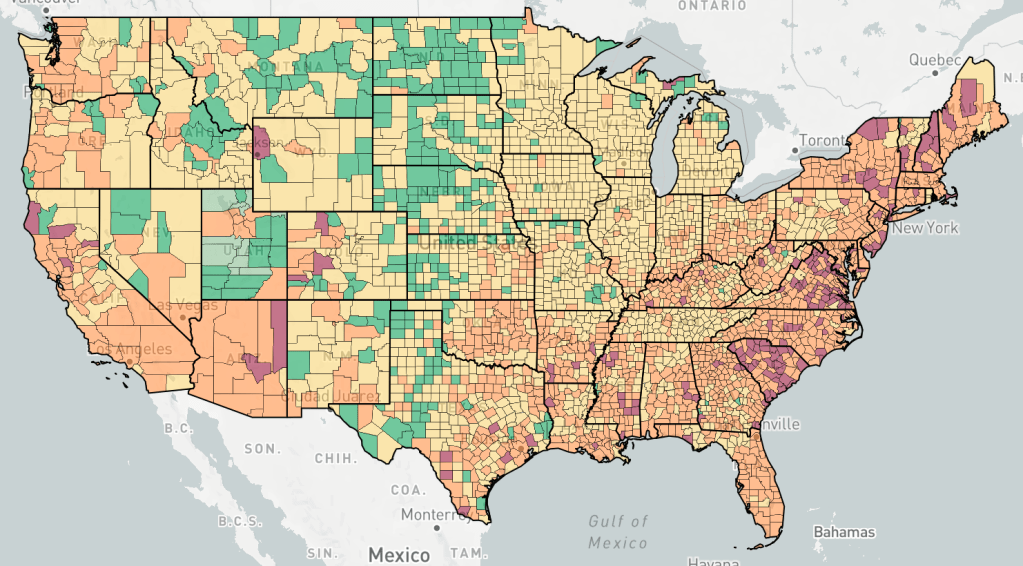
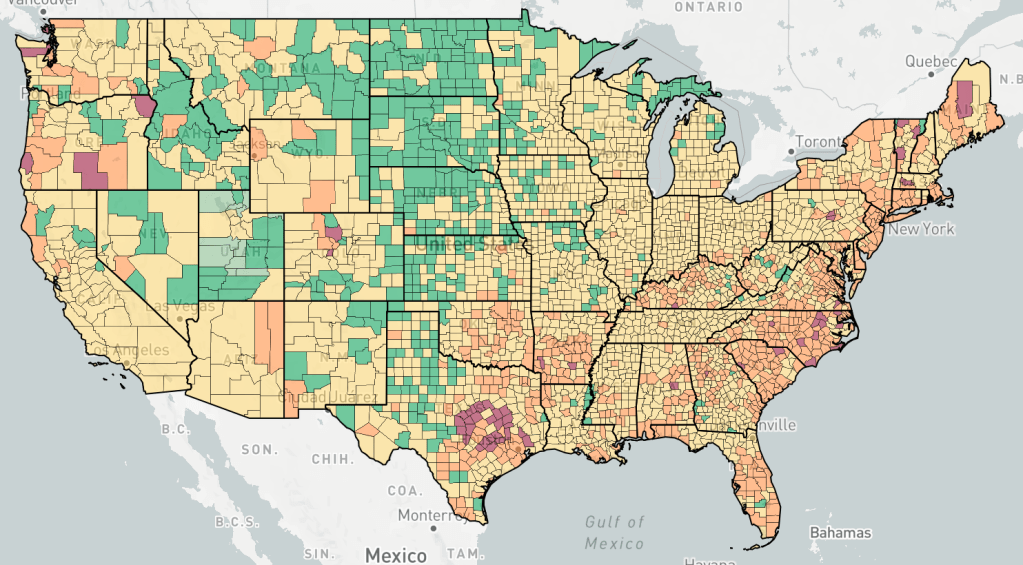
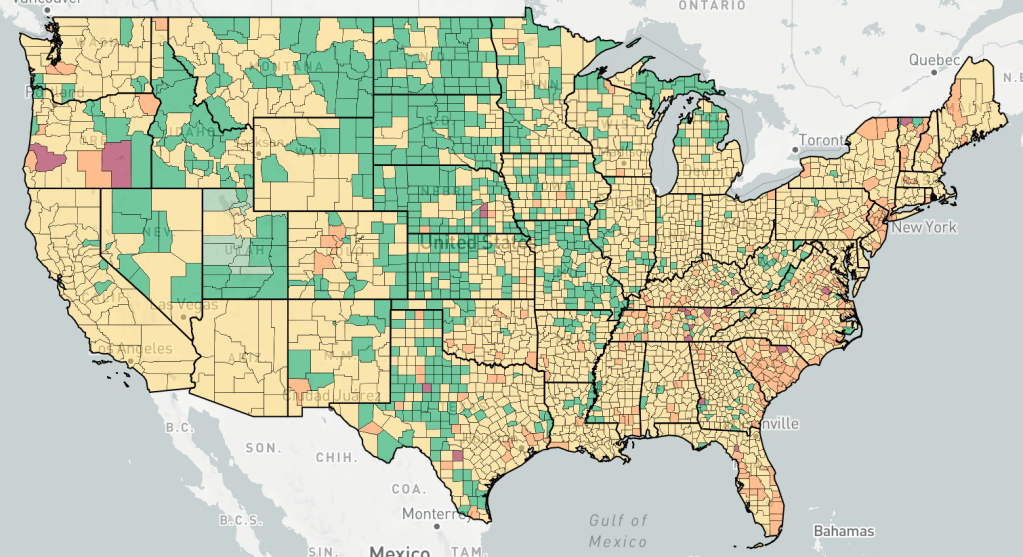
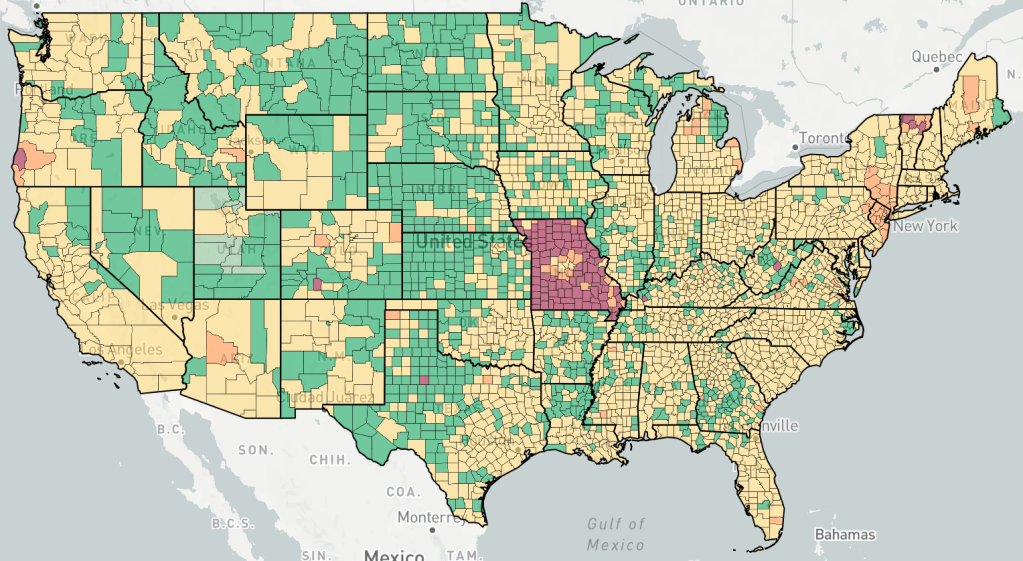
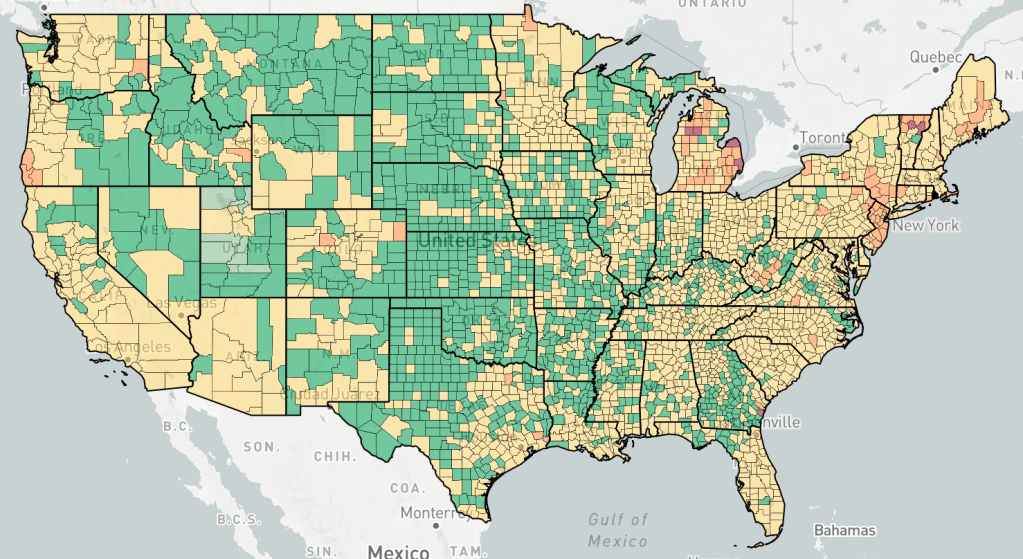
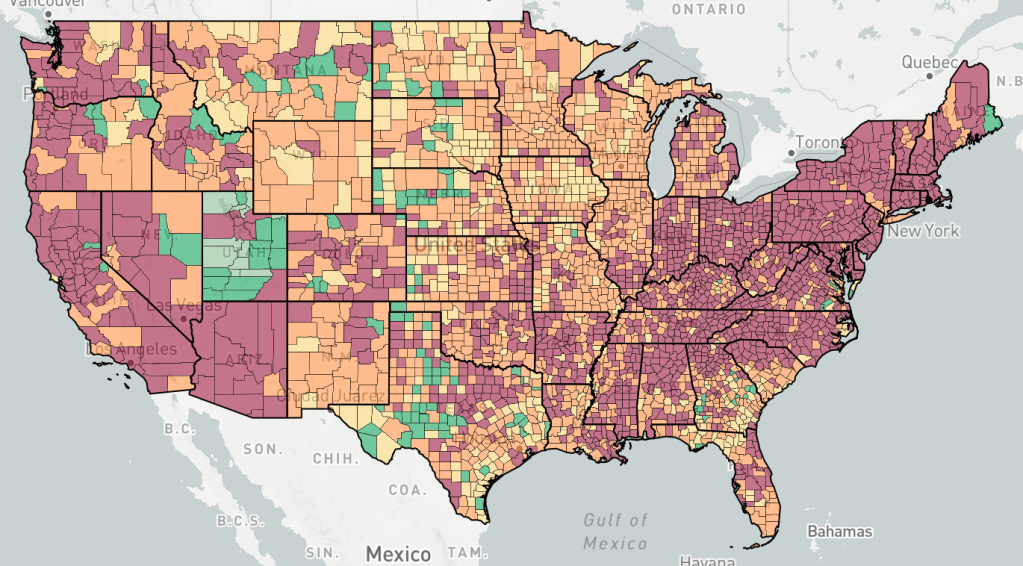
Below is an “animation” of sorts, photos from endcoronavirus, about a week apart, with one photo from June, and then a series starting in September. I’ve said that the Fall wave started in the North and then moved to the South as the wave progressed. I think you can see this in this series of photos. You can also see a flare up in new cases in January, right after Christmas.
Counties are colored based the change in cases, not the number of cases. Red is increasing cases, orange is falling or constant cases, yellow is cases almost under control, dark green is cases under control, light green is no cases.
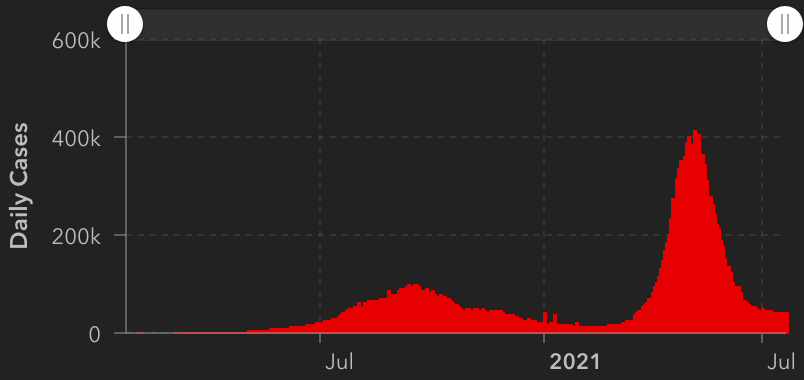
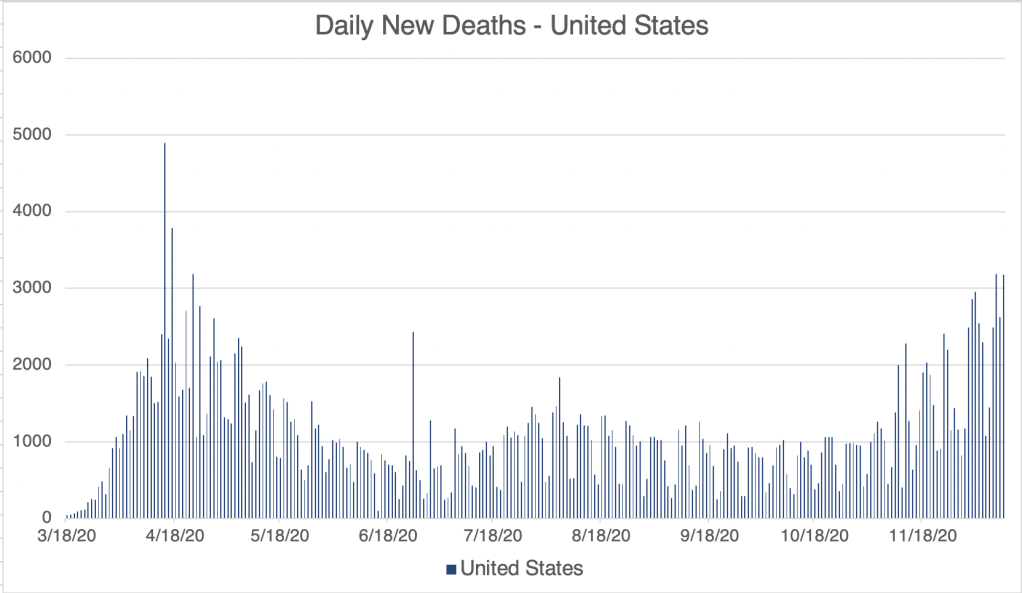
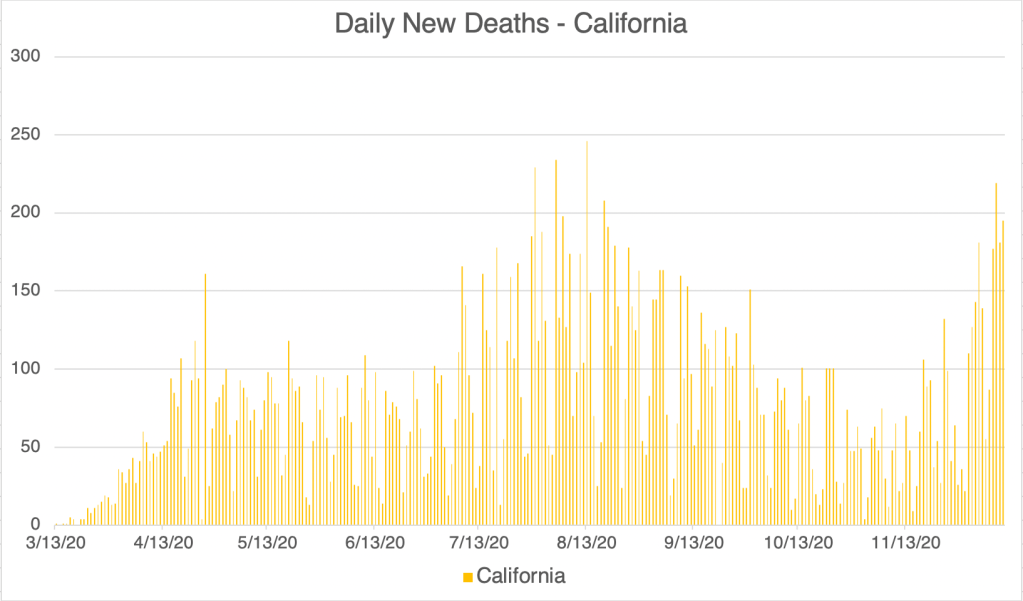
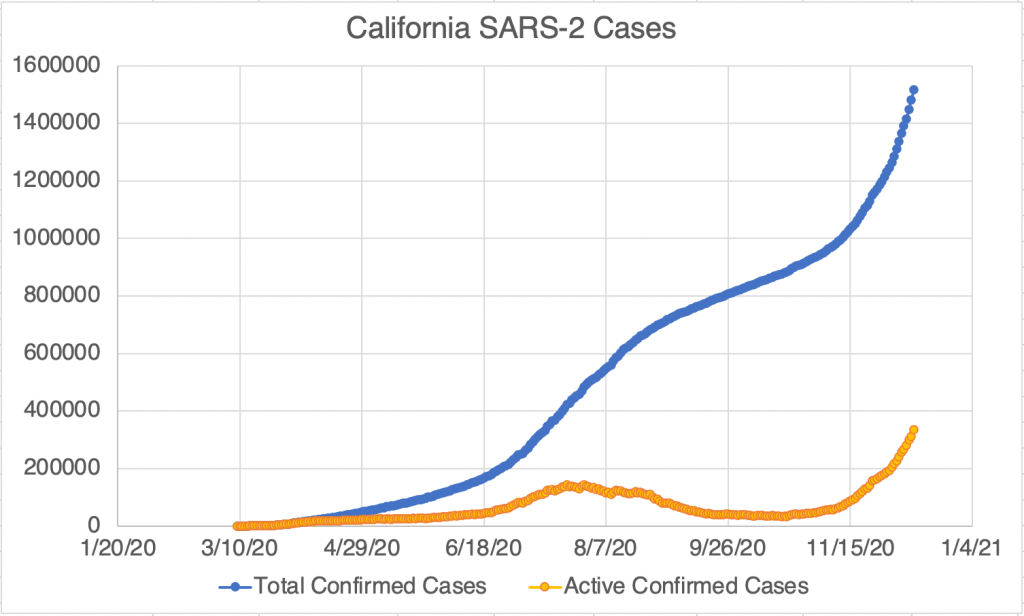
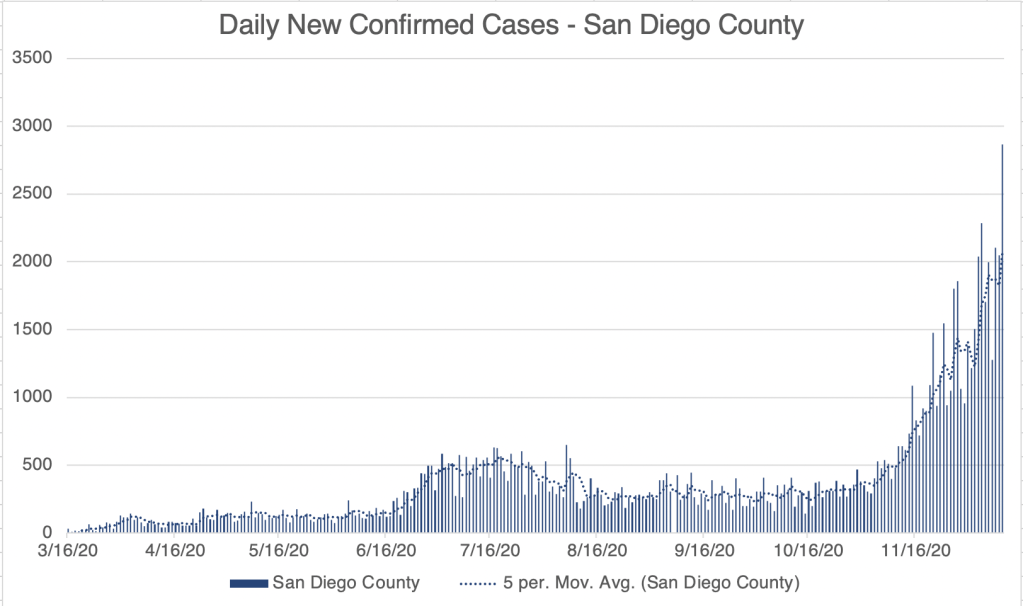
Here’s an overdue case update. Cases continue to rise for the US, California, and San Diego County. The timing of the current US peak makes it clear that the bump is directly related to the Thanksgiving holiday, starting less than a week after Thanksgiving, and after cases had started to come down. LA County currently has more that 100,000 active cases, more than twice the number than the next highest county, Cook County, the home of Chicago.
More on ADE and Vaccines: Some potential very good news for me on the vaccine front. For months I’ve been warning about ADE, the phenomena that some viruses can be even more dangerous in a second infection than the first. Karen Parrott, a former colleague at Quest Diagnostics, often provides me with interesting COVID related stuff. This week she sent me a podcast featuring Paul Offit, the developer of the first Rotavirus vaccine and an author of many books on immunology and vaccine production. I am not an immunologist but he is. More importantly, he’s the first authoritative person that I’ve heard in the media speak at length on the ADE issue and how it relates to COVID. He claims in the attached clip (time stamped at 14:40) that the current vaccines do not appear to trigger the ADE pathway in animal models, and human trial subject never displayed the signs that ADE was involved in secondary exposures. This difference from SARS-1 and MERS may be related to the fact the SARS-2 is much less virulent than these other 2 viruses.
This makes me more optimistic that the vaccine will be safe from an ADE perspective. I won’t be able to get the vaccine for some time, but I am more willing to get it now than ever before. Several physicians I know are eager to get it as soon as it is available. This is great news!
In the interest of full disclosure, I will point out the some patients receiving the vaccine the UK have experienced some injection site irritation, especially in those with allergies. This is actually somewhat normal for vaccines, and appears to pass within a few days.
In addition, now that mRNA vaccines have been produced for the first time, future development of this new kind of vaccine should be even faster than this time!