This is a COVID Update. I’ll also talk about a recent meta-study by Jefferson et al about mask effectiveness.
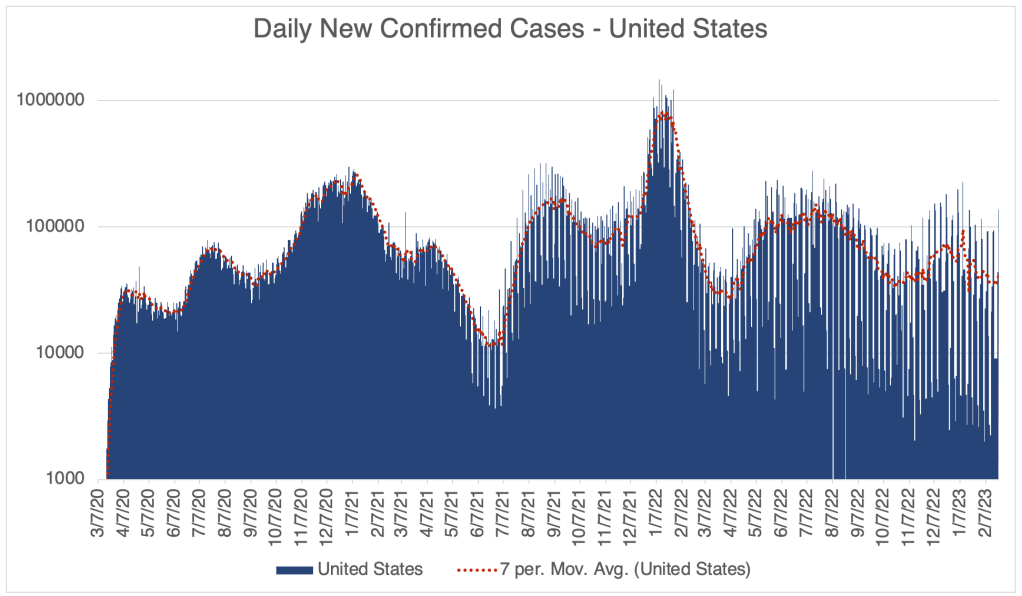
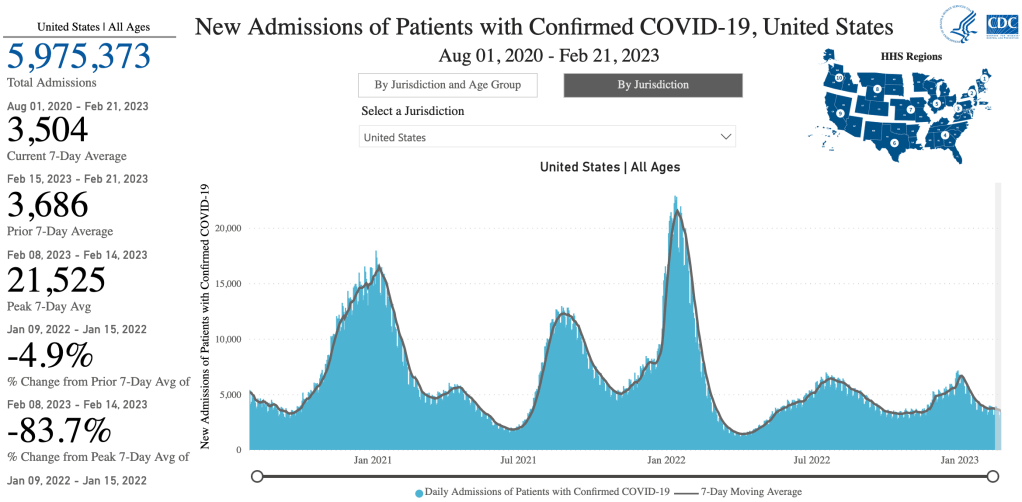
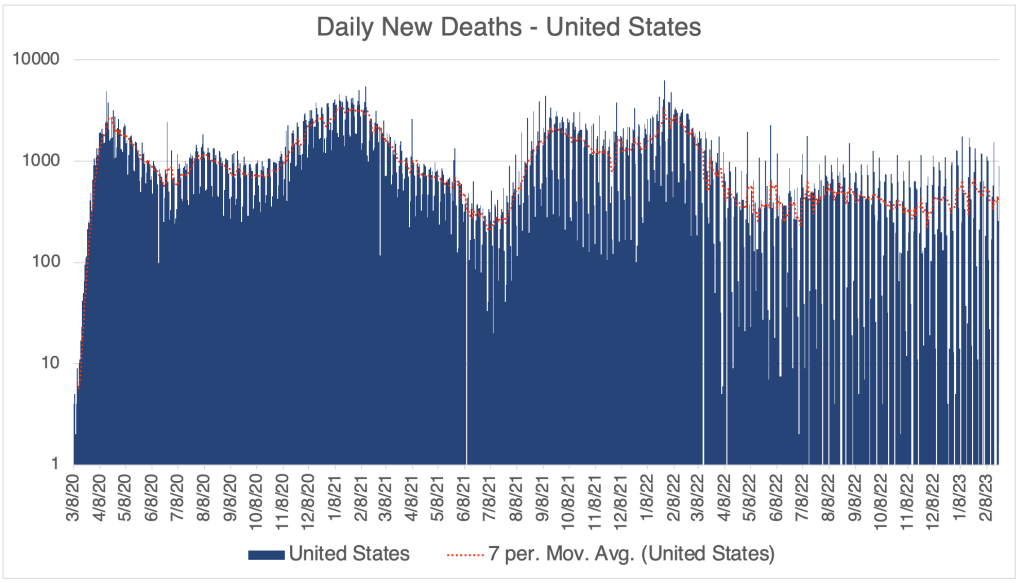
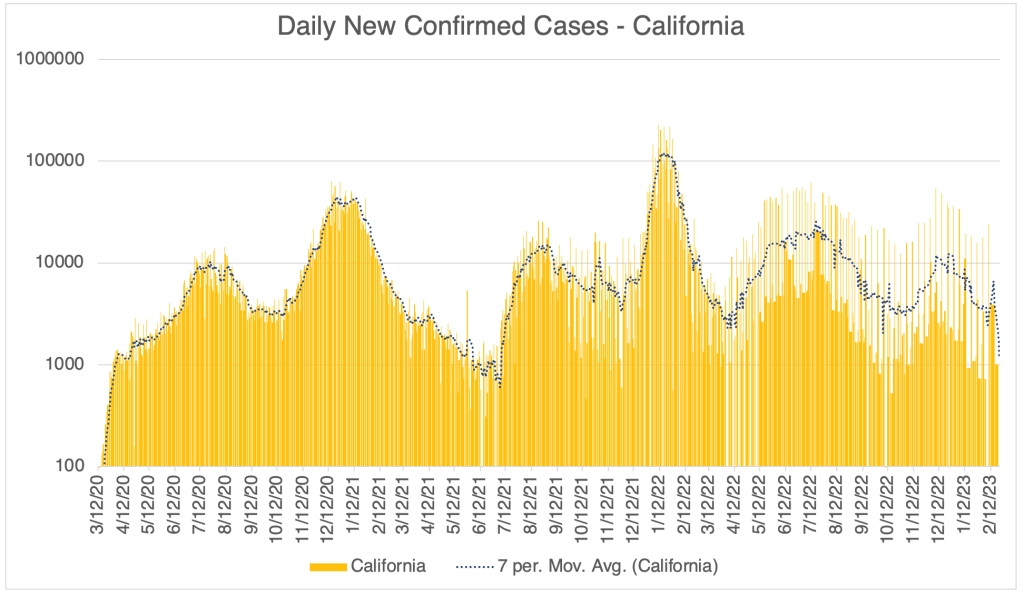
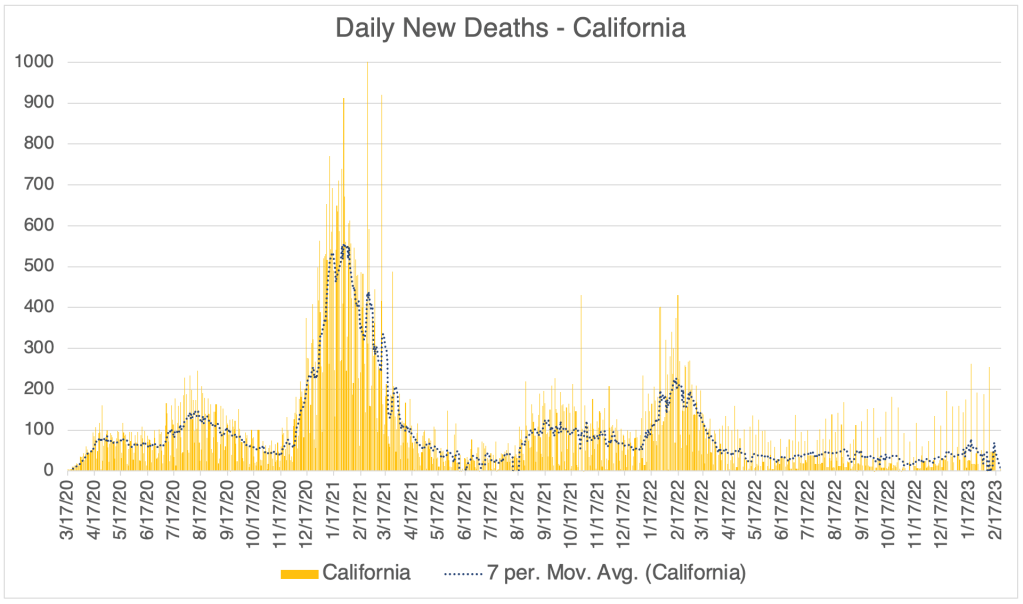
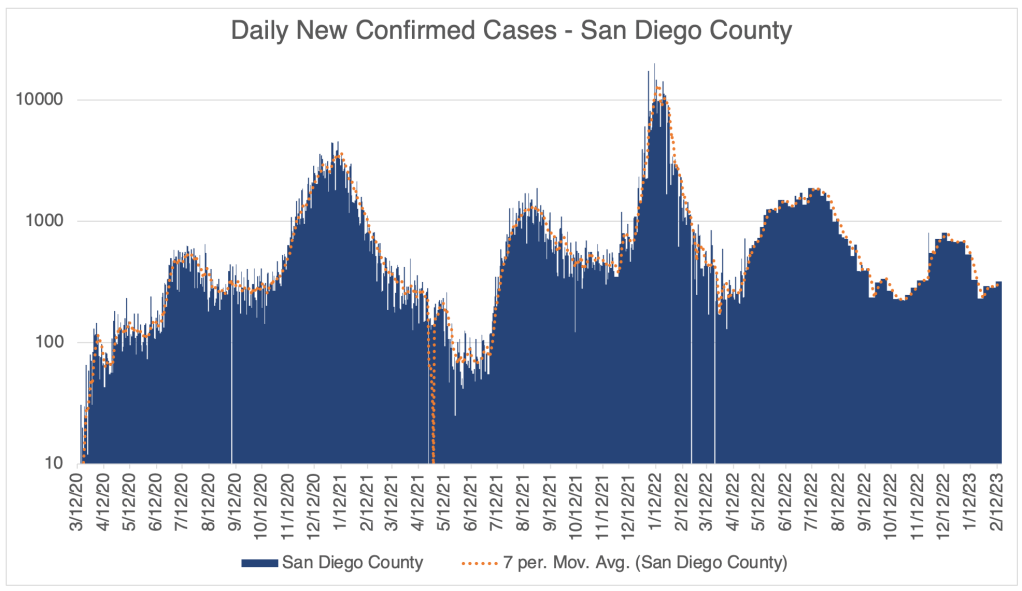
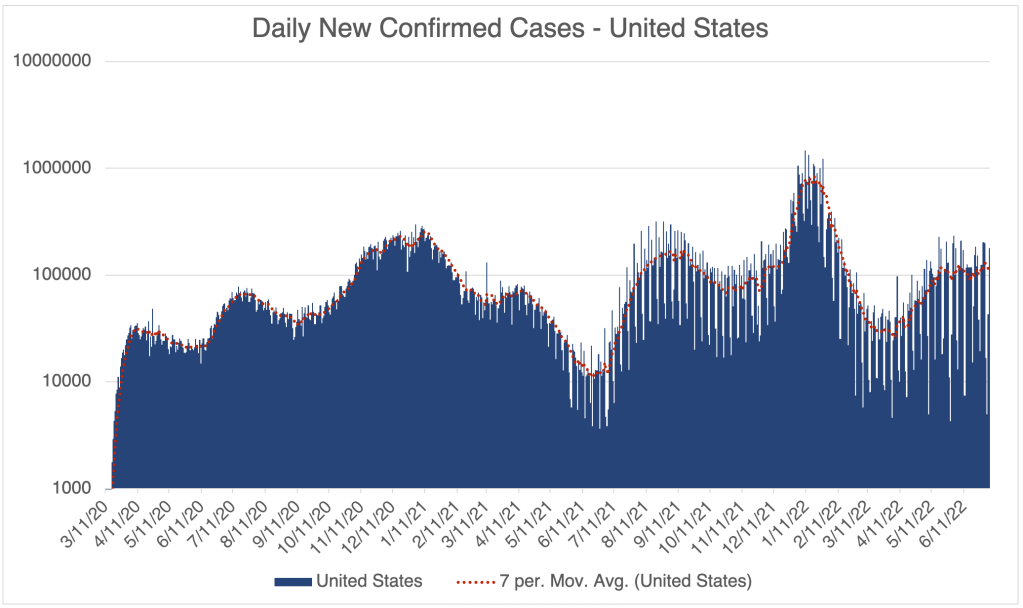
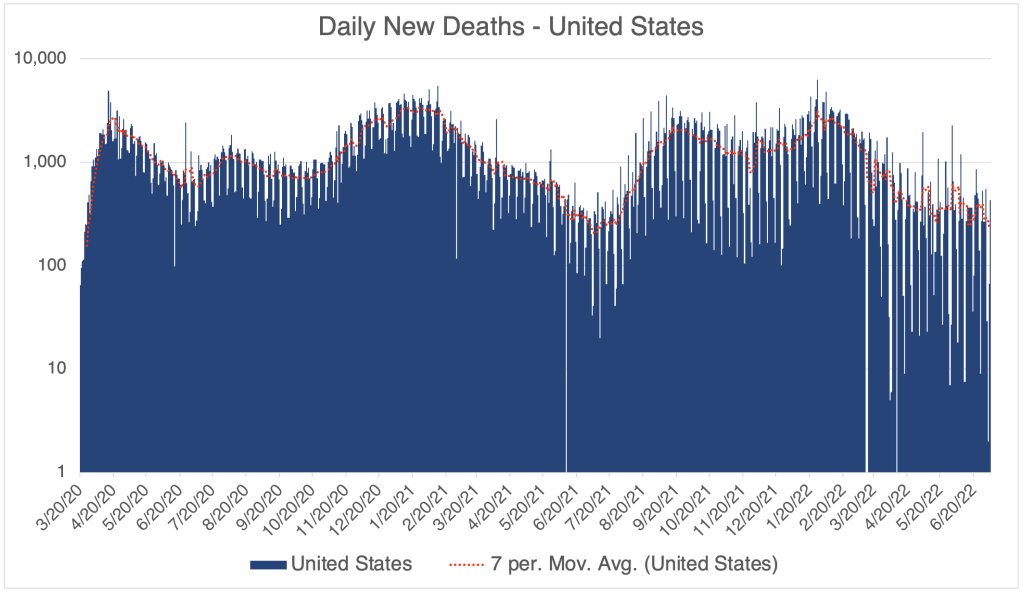
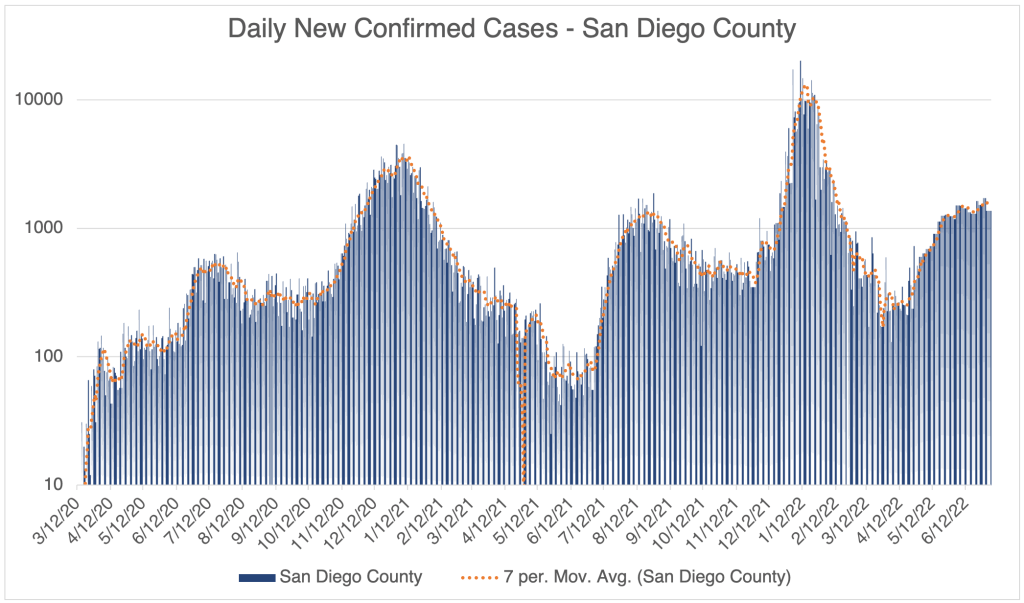
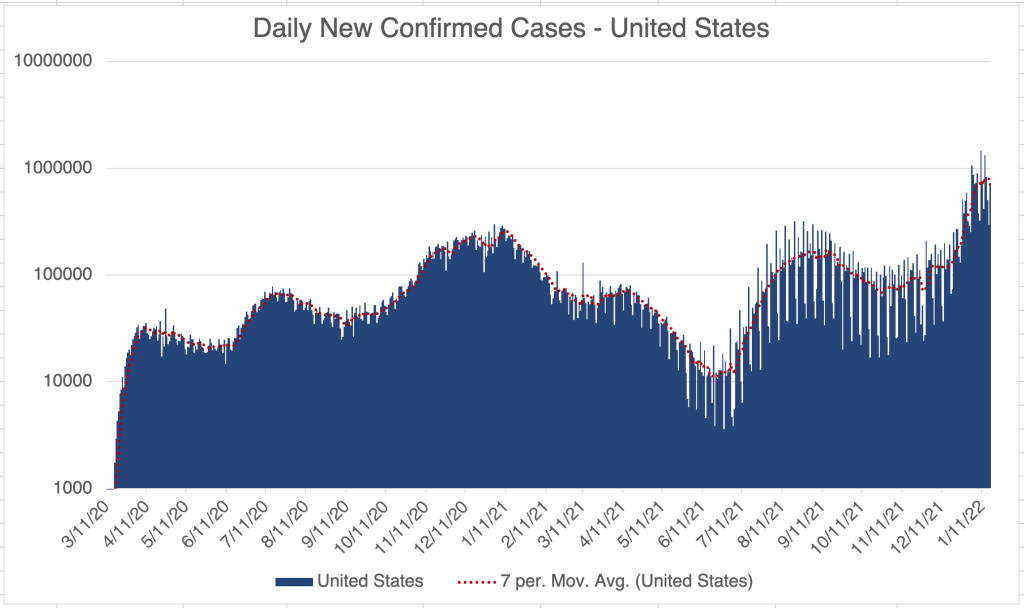
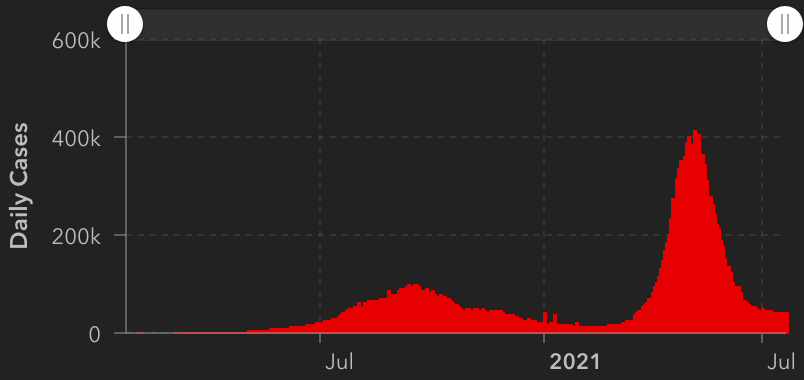
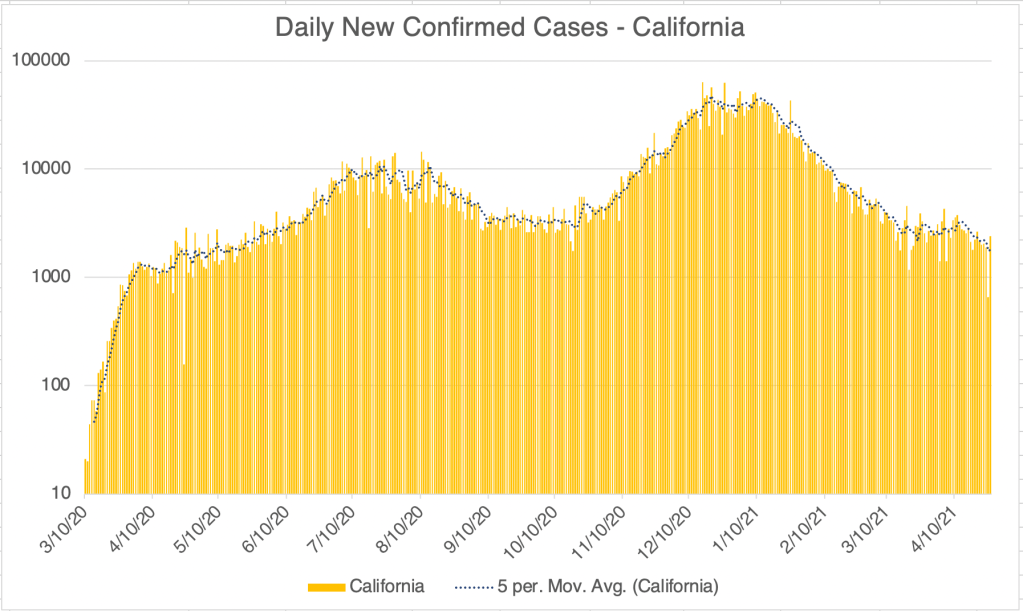
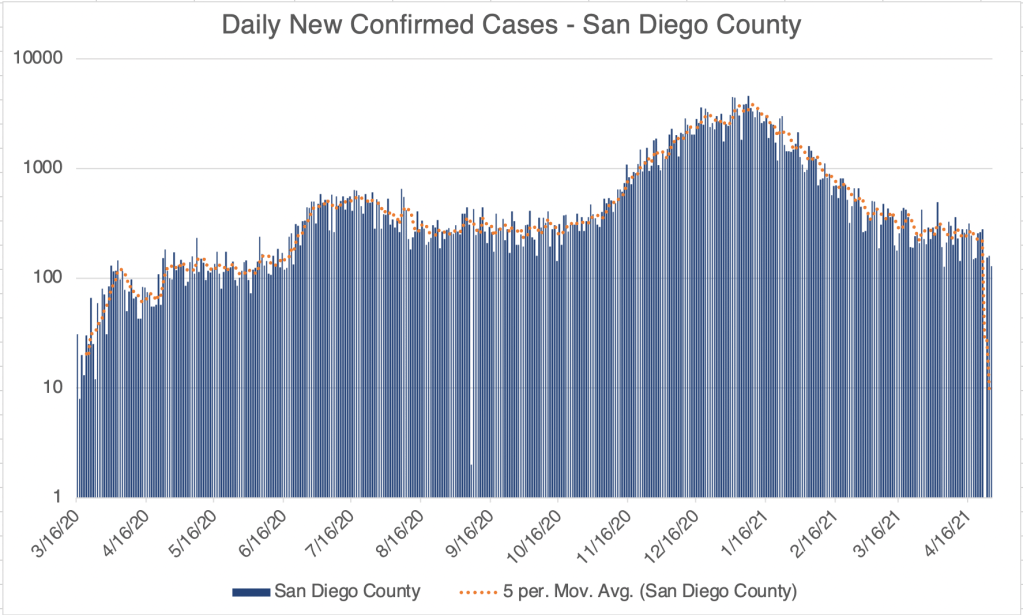
The Winter wave is over. Cases in the US, California, and San Diego County are about at the same level as they were in October. This the mildest COVID winter season since the pandemic started. COVID related deaths increased modestly during this time, but are now relatively low but persistent.
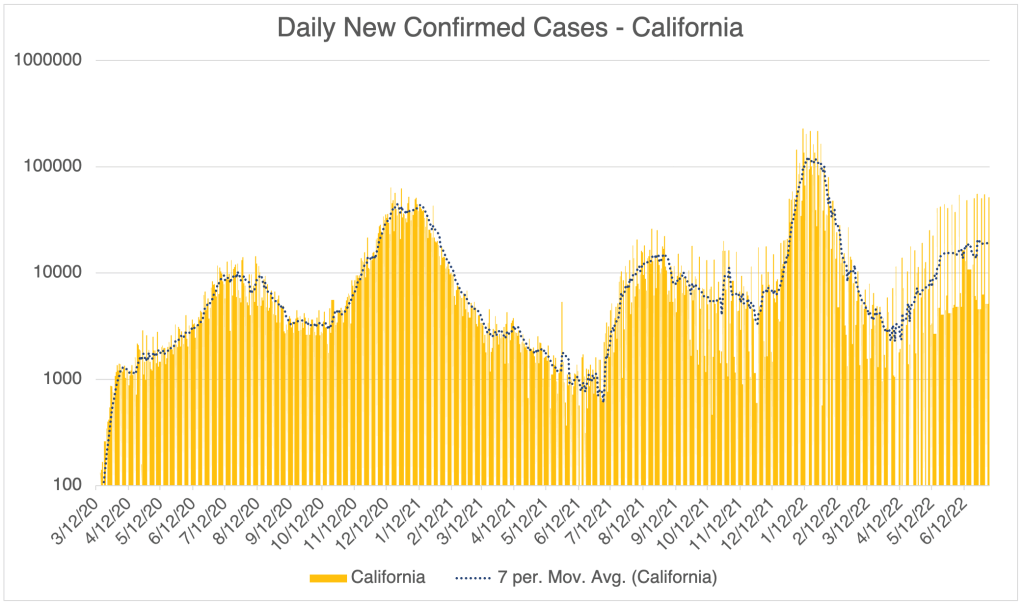
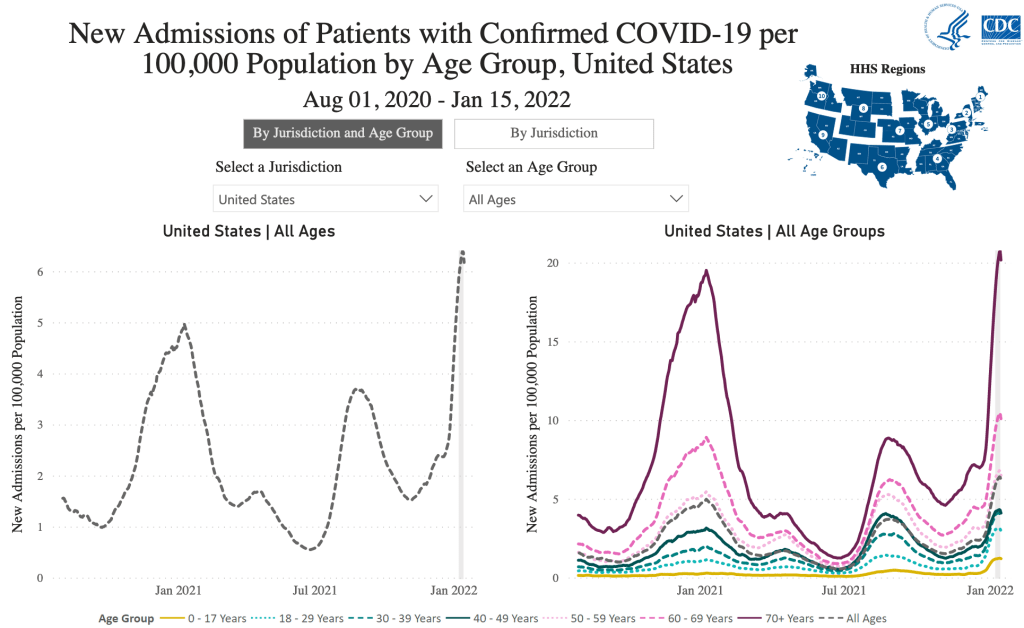
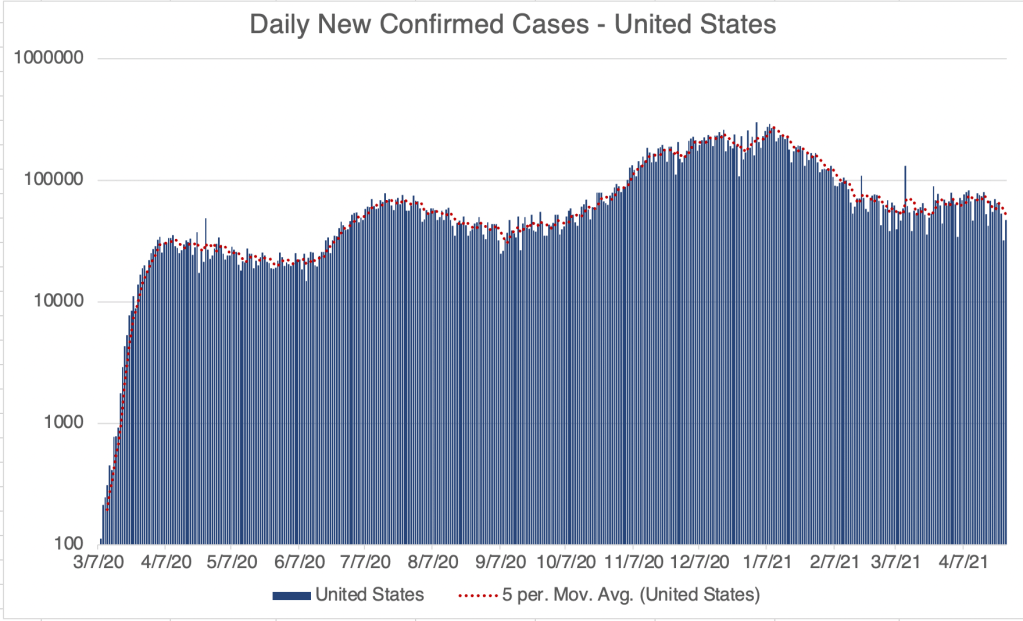
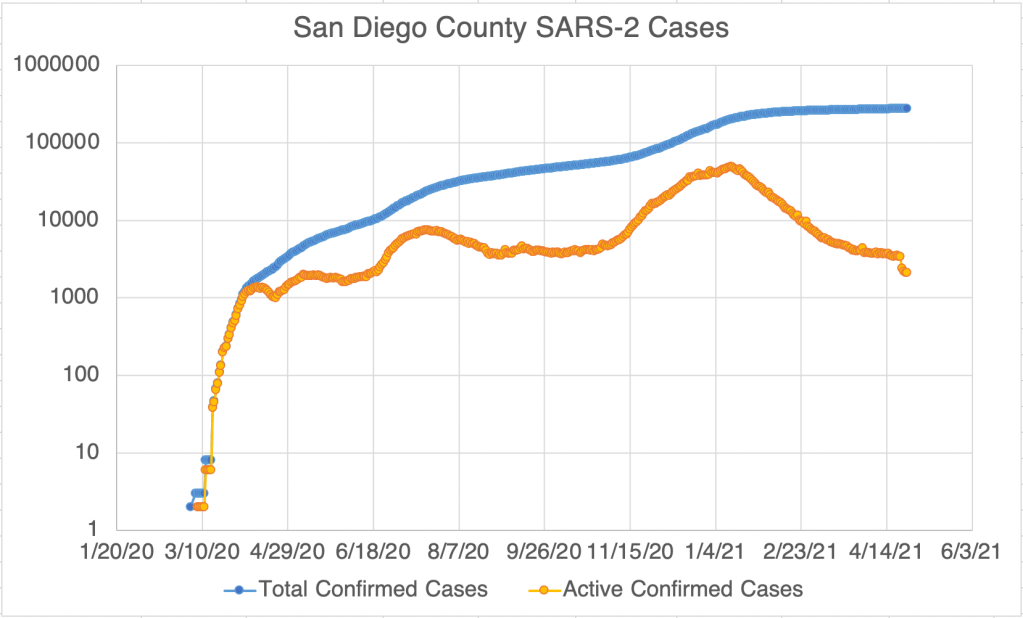
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.From the CDC page on Variant Proportions for the United States. Updated for February 18th.From the CDC page on Variant Proportions for the United States. Updated for February 18th.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.
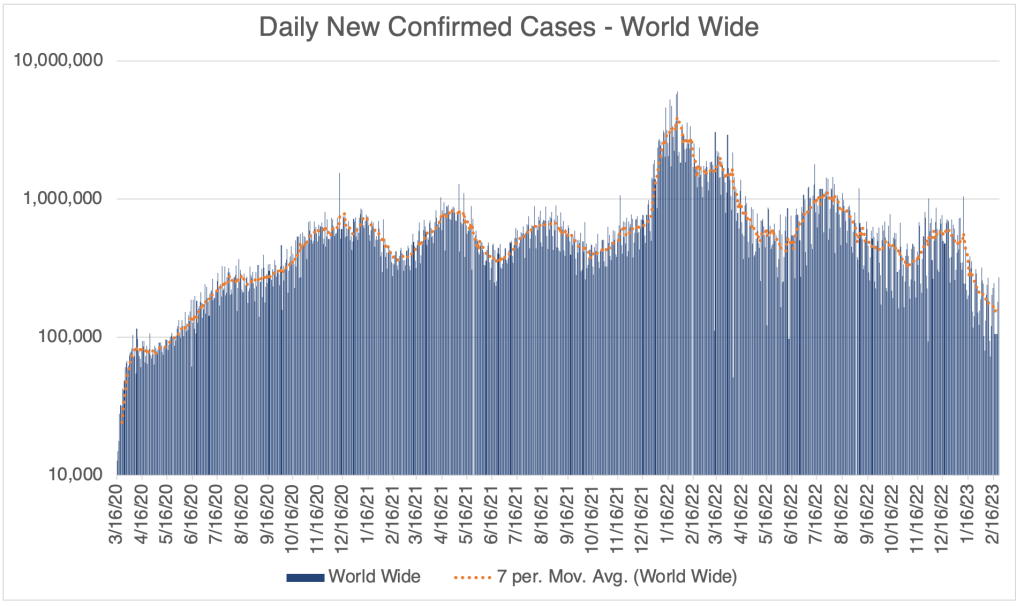
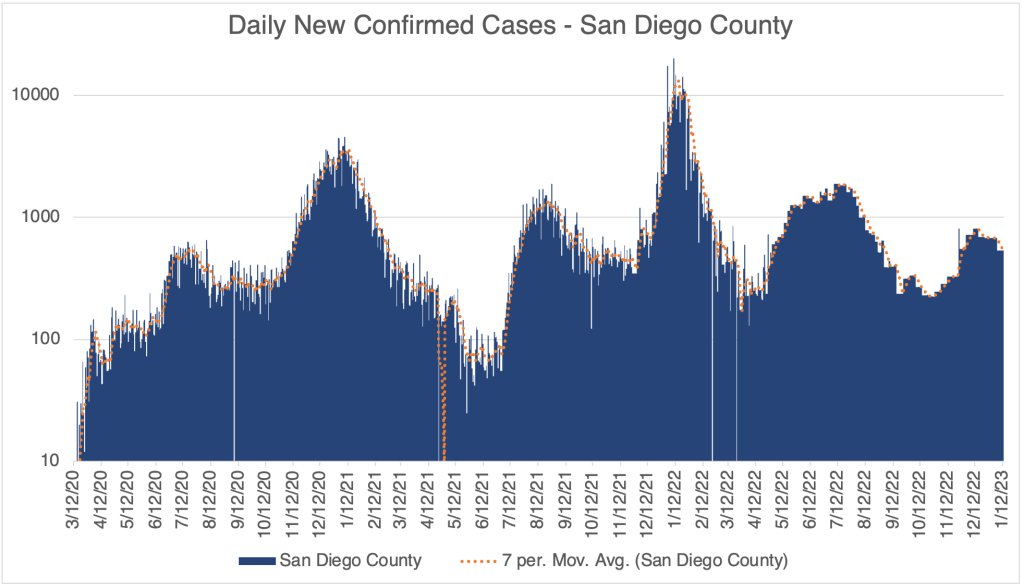
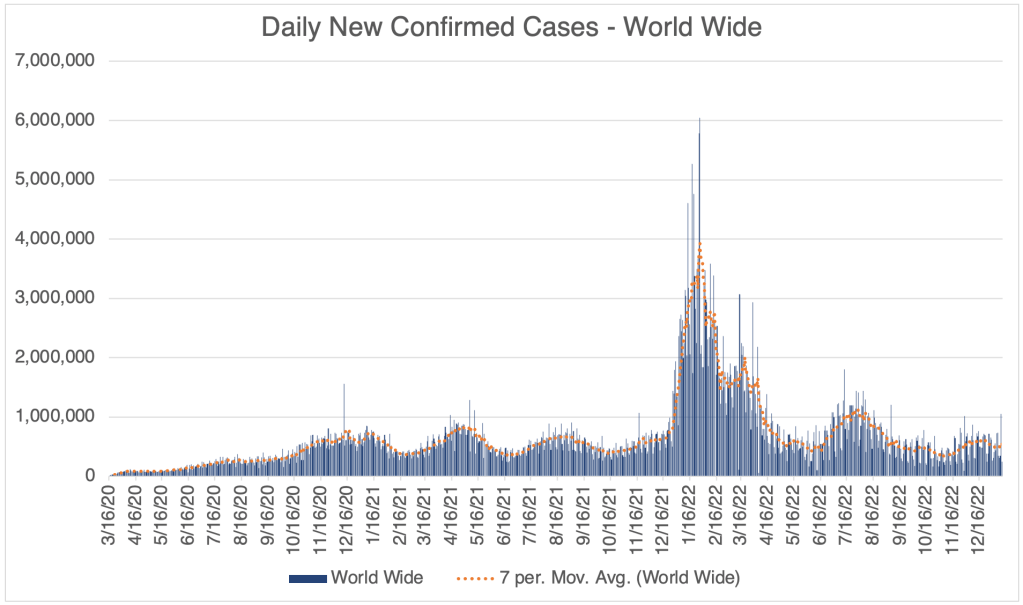
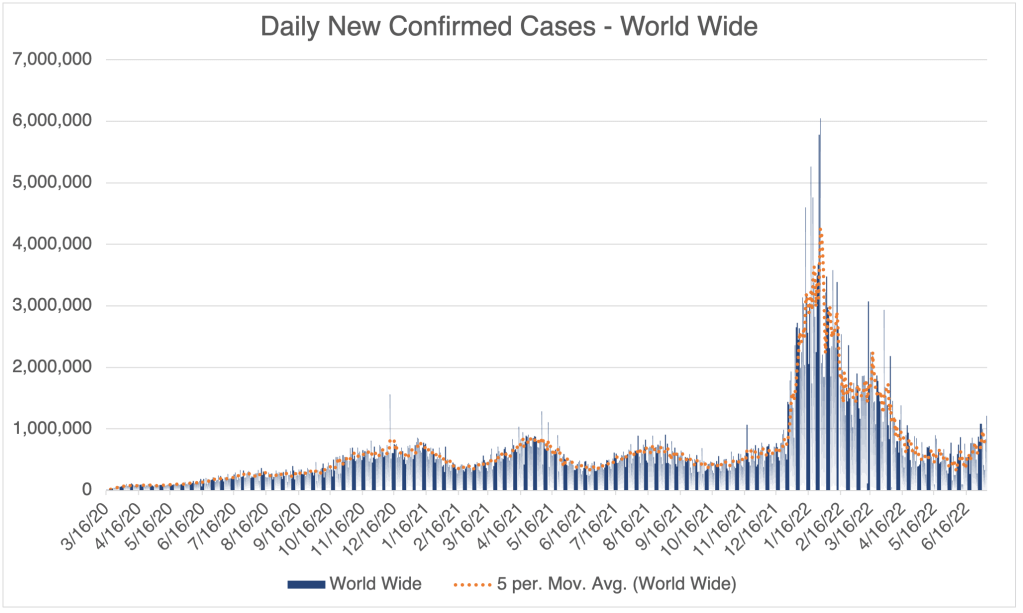
World wide, cases are as low now as they were way back in the Summer of 2020. Of course, I have to mention that testing was not as available in 2020 as it is now. On the other hand, many people currently are testing themselves with over the counter tests, and don’t report the results to the medical system, so there is a lot of uncertainty as to the actual number of cases.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.
Cochrane Report on the Effectiveness of Masks: Jefferson et al released a meta-study through Cochrane Reviews on the effectiveness of medical masks (surgical masks) and medical respirators (N95) in public settings. A meta-study is a study in which the authors gather information from published articles and try to draw conclusions from a large body of data. They do not gather a new set of data.
The Jefferson et al study reviewed 78 different studies, including data from pre-COVID flu outbreaks. Their conclusions are sobering. First, the authors suggest that there is virtually no benefit to wearing a medical surgical mask over not wearing a mask in most settings. If you’ve been reading my blog for long, you will know that this conclusion does not surprise me. Blue surgical masks have large gaps in the sides and do not filter air leaving the mouth and nose. They were designed to prevent droplets from a medical worker from contacting a patient, not to prevent transmission of aerosol based agents. This is a problem, since most mask wearing people in public during the pandemic were wearing surgical masks. These people thought they were protected from aerosols, but they were not.
The study also concludes, however, that N95 masks didn’t perform much better. In fact, for lab tested COVID, the difference was statistically insignificant, meaning that the difference between wearing N95s or surgical masks was so small, it could not be proven to be a real difference statistically.
I have to point out that the Jefferson meta-study points out that many of the studies they reviewed had various failings that may have made them unreliable. Much of the data was collected through self-reporting of participants, which is a source of inaccuracy, and participants were often non-random, making application to the general population difficult. So some of the conclusions may have suffered from these kinds of errors.
As you know, I’ve been a proponent of wearing N95, KN95, or KF94 masks when indoors during the pandemic. Unfortunately, N95s are tight and intolerable for most people for long periods, so most people didn’t want to wear them at all. Those that did were not careful to make sure the mask fits properly, making the mask ineffective. This is part of the reason I wore a KF94 (Korean) during the later stages of the pandemic when I had choices.
So have I been wrong this whole time? Well, yes and no. I wore a KN95 in all kinds of environments while traveling during the pandemic. When I finally got COVID in January of 2022, I was not wearing my mask, working in a “gray area” environment with people that I later found out had COVID. I was technically indoors, but the room had a lot of ventilation, so I thought I would be OK. Obviously, I was incorrect. All this to say, I think my KN95 was effective for much of the pandemic. On the other hand, I am a scientist in the infectious disease field, and have had a lot of experience wearing and fitting these masks to myself, so I am not a typical user. It may certainly be that my experience does not translate to non-scientists.
If you still have not had COVID and are not high risk, I might say that the current version has an extremely low fatality rate, and it may now be worth the risk to say good-bye to the mask. I know the large majority of you have done this already.
If you are at high risk, I still think an N95, KN95, or KF94 can be effective for you. In order for it to be effective, however, you need to make sure it is properly fitted, making sure you don’t have gaps between your nose and cheek. The mask should filter the air coming into your nose and mouth.
Since I had COVID last January, I no longer wear a KN94, and enjoy eating indoors in restaurants again. I’ve basically been back to normal for a long time.
Happy New Year! I have a brief COVID update for you. Then I’ll talk about a new variant, XBB.1.5. I’ll also have comments on a smattering of evolving stories, like California AB 2098, “Physicians and surgeons: unprofessional conduct”, and a new Twitter Files thread on vaccine misinformation.
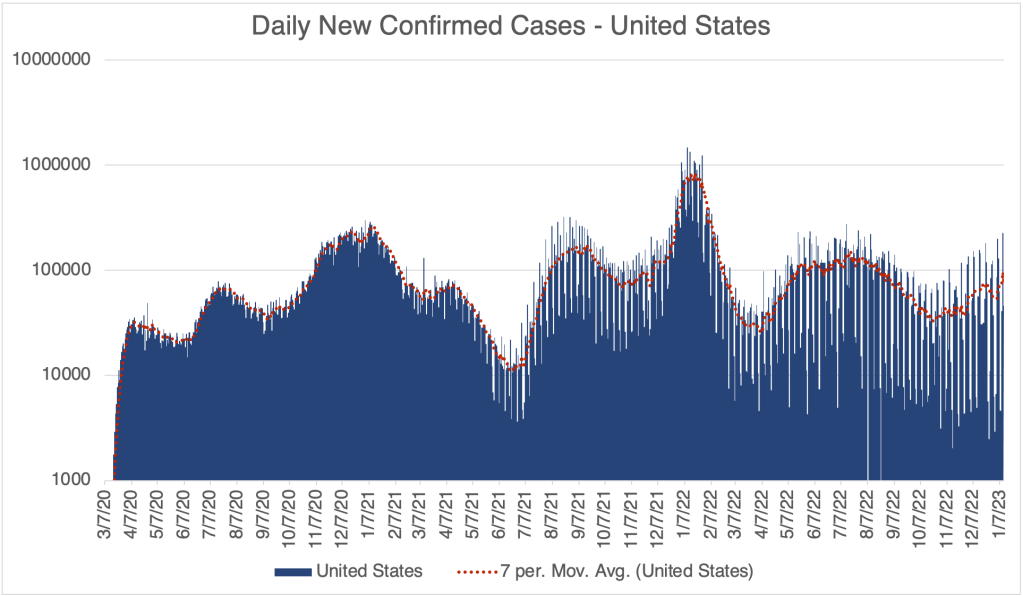
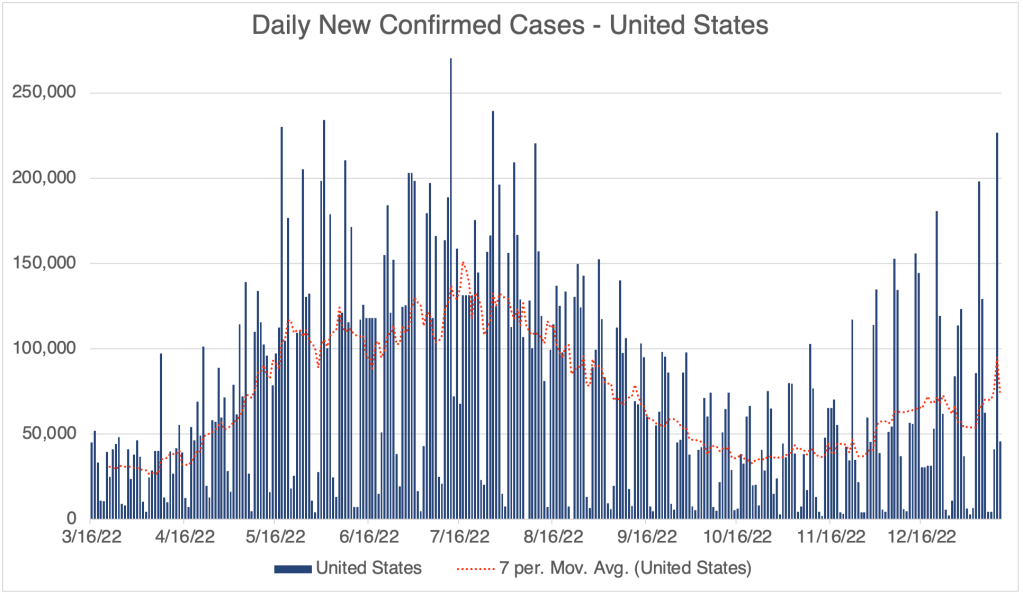
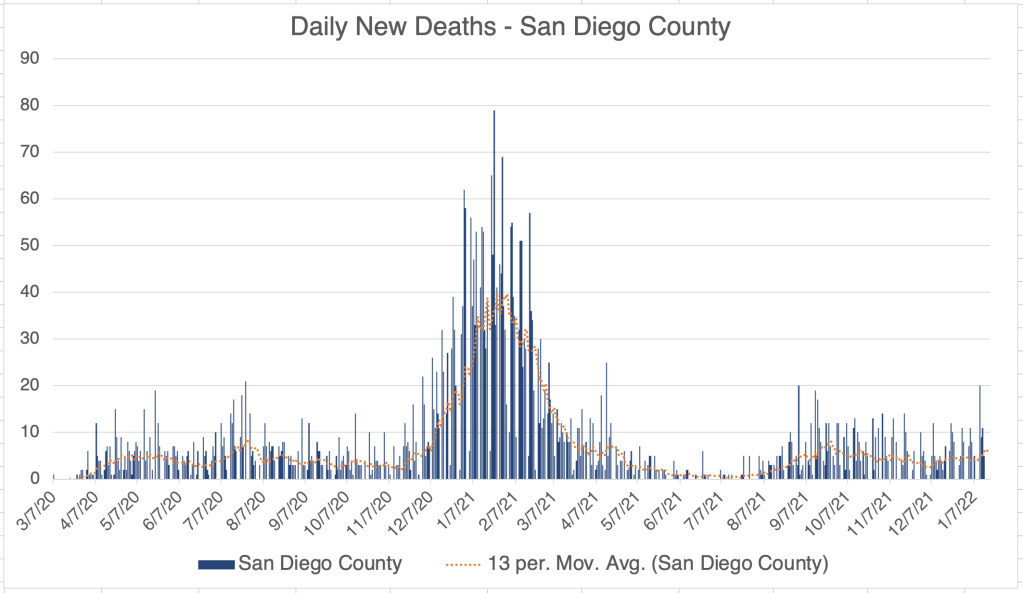
We have already reached the peak of the December wave. Cases in the US, California, and San Diego, and even world wide, peaked at around Christmas. Deaths never really had a peak during this December wave, except in San Diego County.
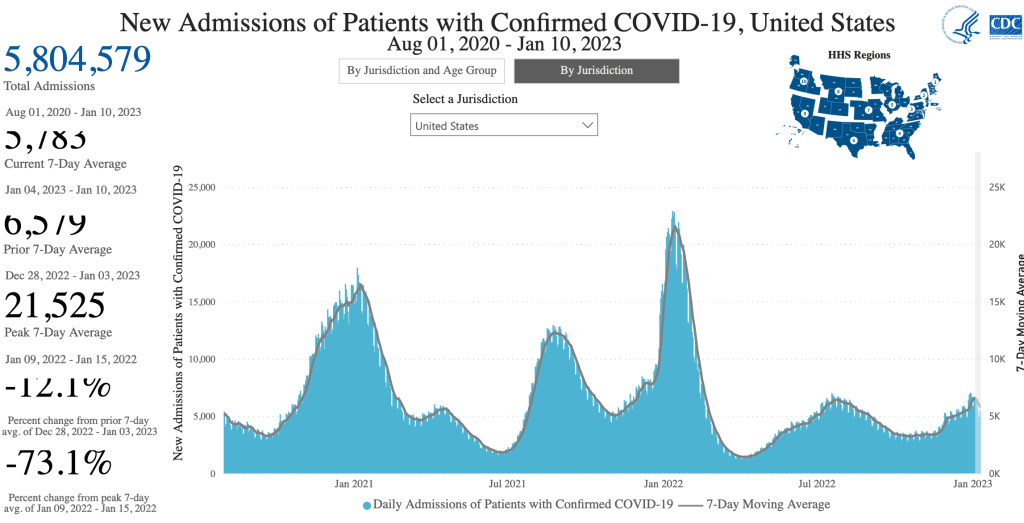
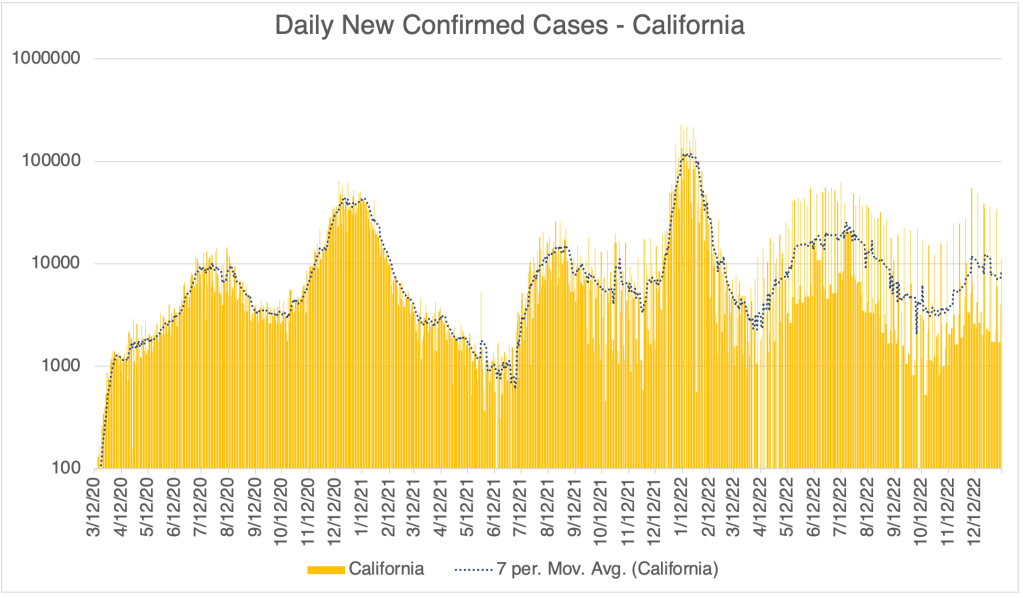
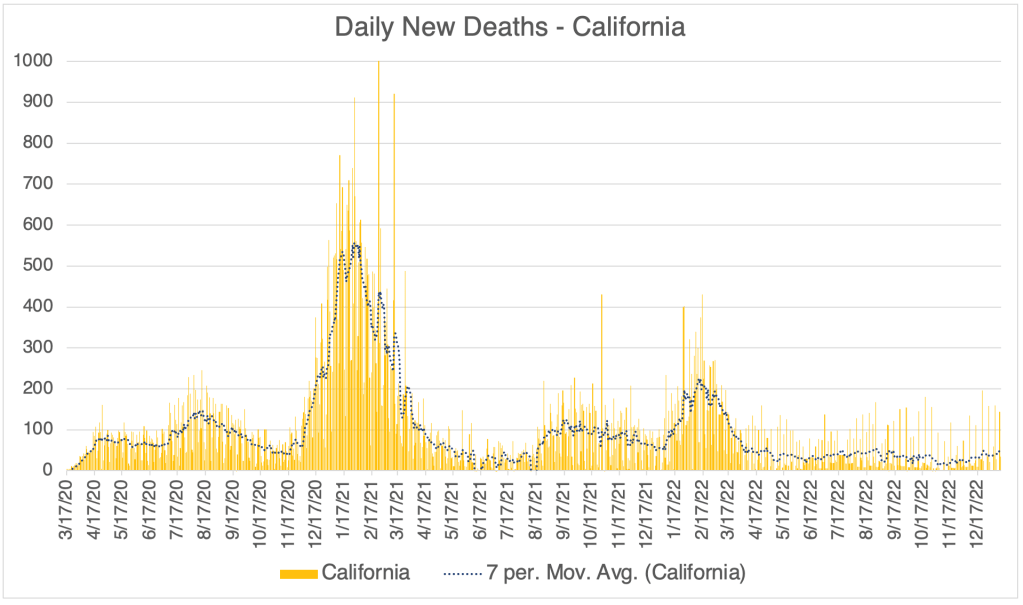
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Daily Confirmed Cases – United States, March 16, 2022 to January 12, 2023. Peak of the first Winter Wave was on around Christmas Day. We may already be seeing the start of an XBB.1.5 peak. Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
However, we may see a second Winter wave this year…
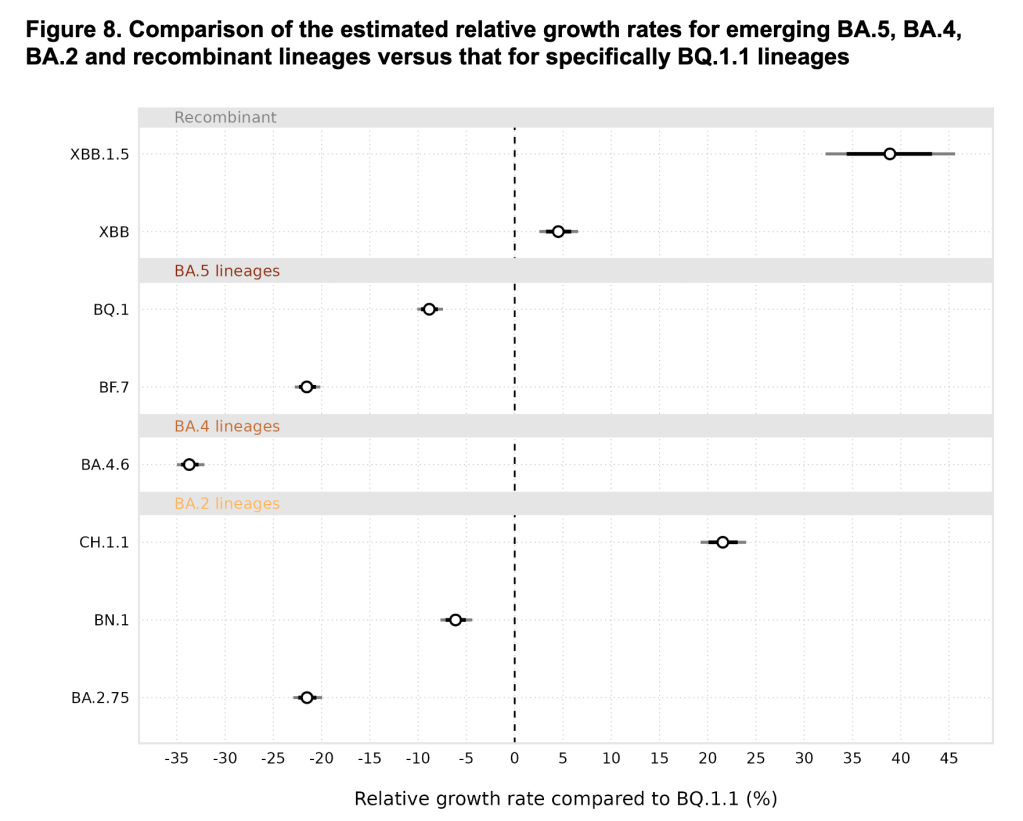
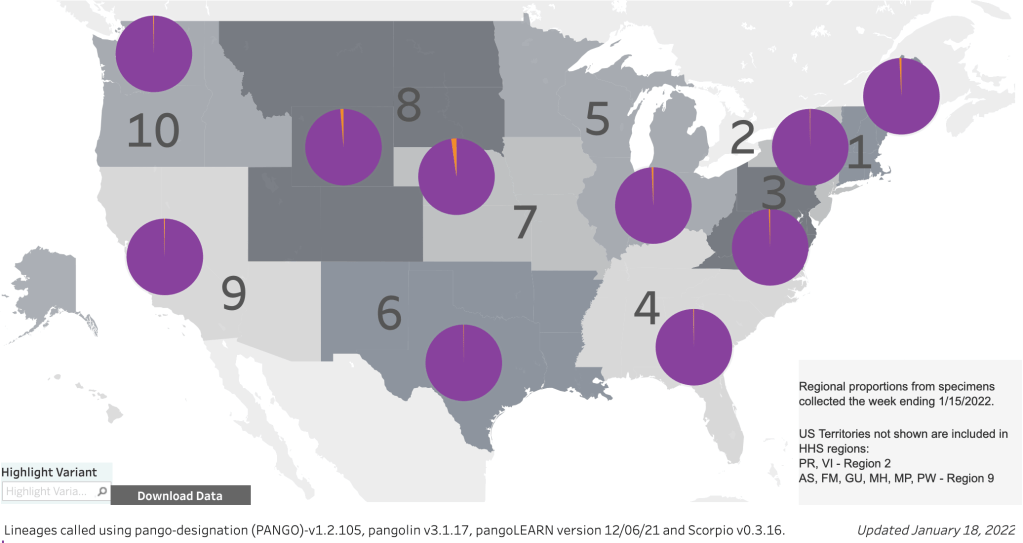
New Variant XBB.1.5: A new variant is spreading extremely rapidly in the US right now. Variant XBB.1.5 is about 43% of the SARS-2 virus in the US right now. A UK study suggests that this new variant is the most transmissible yet. John Campbell, in another excellent analysis, suggests that about 80% of us will get it. Antibody studies suggest that even those with prior COVID infections do not produce many antibodies that can neutralize XBB.1.5, so even those who have had COVID before are likely to get it again. The good news is, XBB.1.5 is another Omicron strain, and will produce very mild symptoms in the vast majority of cases. I’ve had COVID twice already, and I will treat XBB.1.5 as a chance to get a free booster.
From the CDC page on Variant Proportions for the United States. Updated for January 14th.From the CDC page on Variant Proportions for the United States. Updated for January 14th.XBB.1.5 is the most infectious of the current variants, and perhaps the most infectious variant to date. From the UK Health Security Agency, Technical Briefing 49.
Despite the likely mildness of XBB.1.5, do others a favor and stay at home if you have COVID. The over-the-counter antibody based COVID tests do not work very well, so if you are sick but have a COVID negative antibody test, you should assume you have COVID. Only a PCR test can tell you if you’re really negative.
If you haven’t yet had COVID, I can no longer recommend that you get a vaccination or a booster, even if you are in an at-risk group. If you are concerned about getting COVID, consider taking precautions instead. Wear a N95, KN95, or KF94 rated medical respirator when indoors in public. It’s also important to make sure your mask fits snugly. The mask must filter air coming into your nose and mouth. Loosely fitting masks with large gaps will not do this. Do not wear a cloth or surgical mask. These masks will not protect you from XBB.1.5.
California Physician Misinformation Act: On October 4th, 2022, I wrote about California AB 2098. This new law went into effect on January 1st and adds “the dissemination of misinformation or disinformation related to the SARS-CoV-2 coronavirus” to the definition of unprofessional conduct for physicians in California. Unprofessional conduct can result in the suspension or loss of license for physicians in California.
Just yesterday, I had lunch with a friend of mine who is a doctor in California. I asked him how he is dealing with this new law. He said most of the doctors at his hospital follow the official guidance promoting vaccination, and the few who don’t have become very quiet about vaccines. Doctors can’t say anything negative about the vaccine, for the risk of their medical license.
In 2021, this same doctor was coerced into getting the vaccine to retain his position at the hospital. He got a booster later in the year. A month after receiving his booster, despite being very physically fit for his age, he had a heart attack. His cardiologist said he had none of the arterial plaques that typically cause heart attacks. My friend cannot prove this, but he strongly suspects that clotting due to the vaccine contributed to his heart attack. Despite all this, he does not feel at liberty in California to give information to patients that would reflect negatively on the vaccines.
Because this law is so new, I don’t yet know how it will be handled by the Medical Board of California. If they choose to ignore it, then doctors won’t be under threat. However, doctors and pharmacists have lost their licenses in the last few years for violating CDC guidelines, so the threat is a real one.
If you live in California, you cannot expect your doctor to give you their honest opinion about vaccines. This is literally illegal now. Consider writing your state senator or assemblymember and ask them to support the repeal of AB 2098.
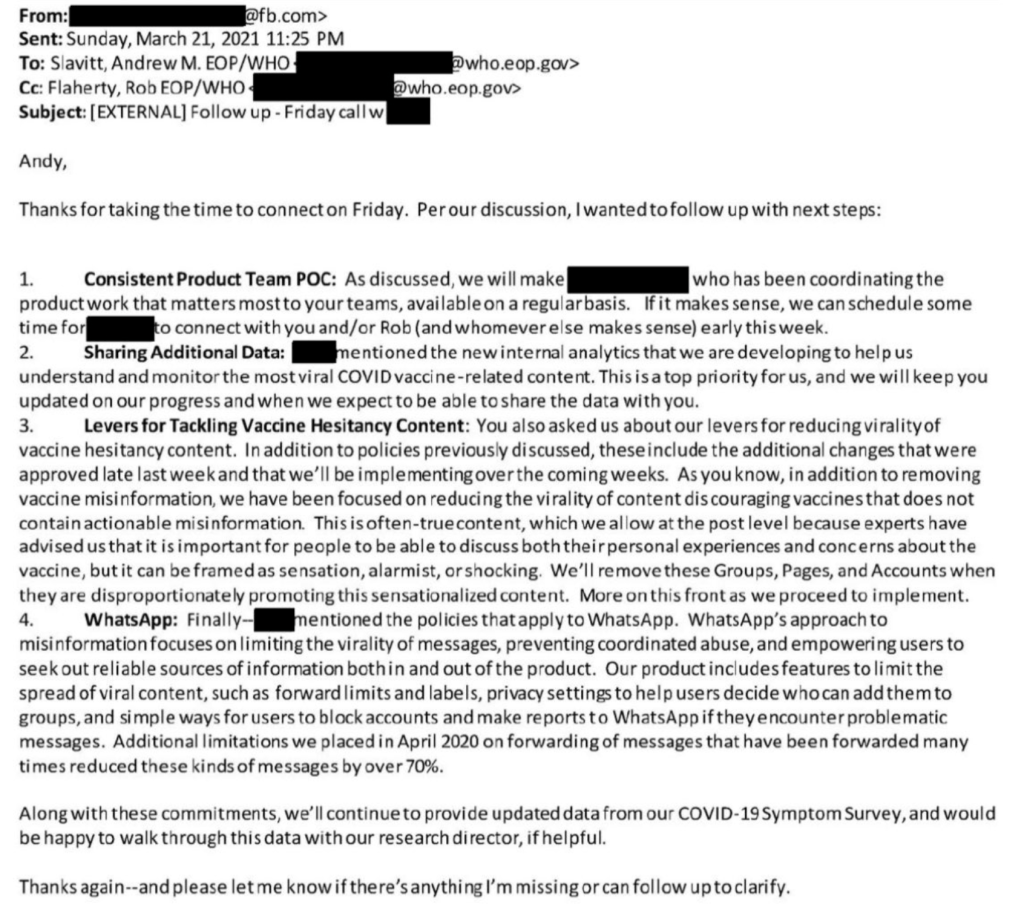
The Twitter Files have exposed a trove of evidence that official government agencies have been coercing several social media companies to censor COVID related information. In an amazing post from Michael Shellenberger, a F@¢eb00k official recently revealed that F@¢eb00k was reducing content not because they thought it was misinformation, but simply because it had a sensationalist tone. In an email to a Whitehouse official, the F@¢eb00k employee wrote:
“As you know, in addition to removing vaccine misinformation, we have been focused on reducing the virality of content discouraging vaccines that does not contain actionable misinformation. This is often-true content, which we allow at the post level because experts have advised us that it is important for people to discuss both their personal experiences and concerns about the vaccine, but it can be framed as sensation, alarmist, or shocking.”
Obviously, these efforts to limit expression by a government agency is a violation of the first amendment, our most important freedom. There are now many, many examples of this in the Twitter files, relating to COVID, and other matters.
This is a case update. I’ll also discuss important new data in regards to BA.4 and BA.5 variants which you may want to take into account as you move around in our “post-COVID” world. You should especially read this if you’re one of the few who have never had COVID. I’ll also suggest a range of strategies that you may employ to keep yourself safe.
The update is actually not much different in the US from last week. Cases are medium-high but flat right now, and we have happily not yet seen increased deaths due to Omicron BA.2.12.1, BA.4, and BA.5 variants.
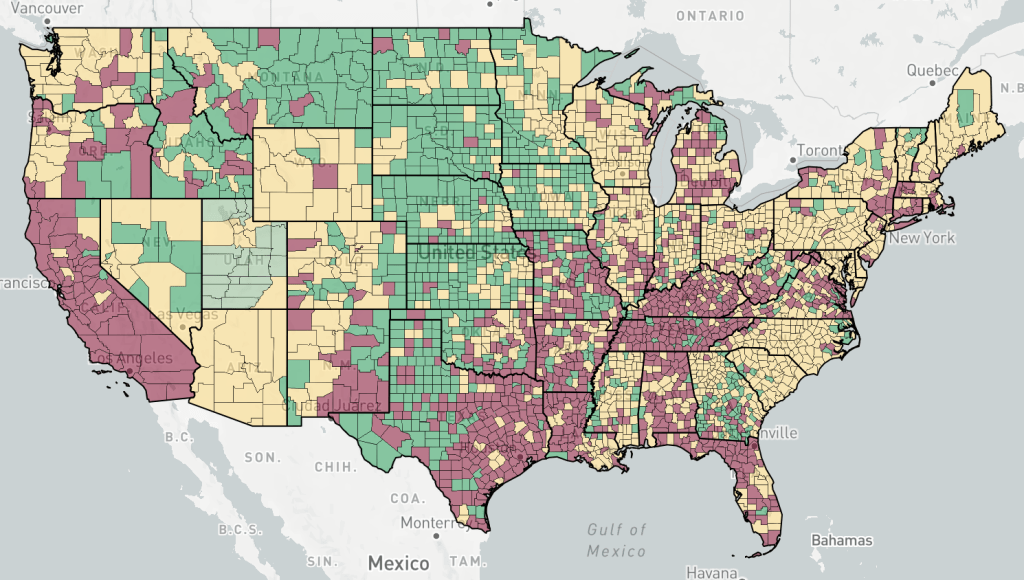
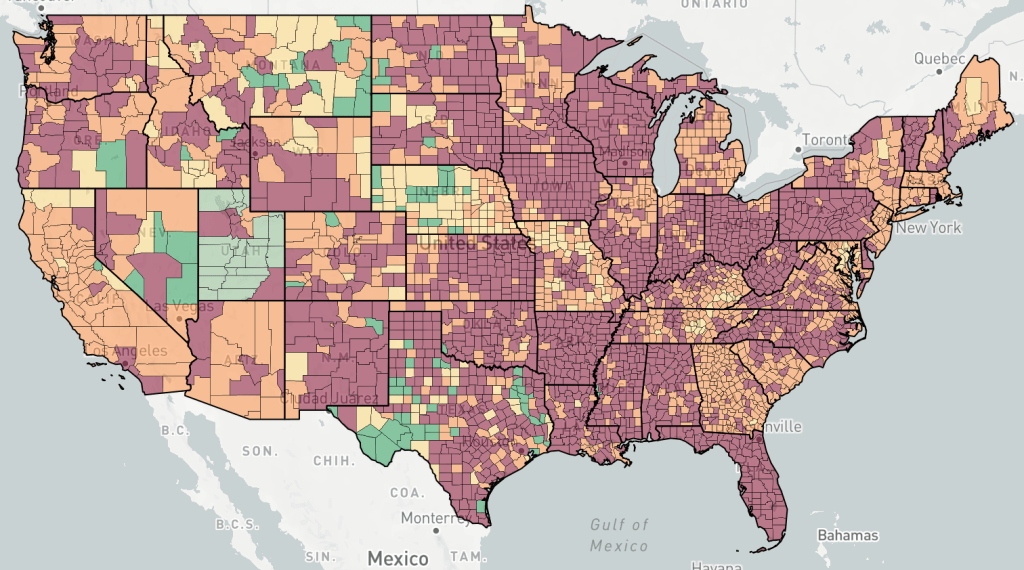
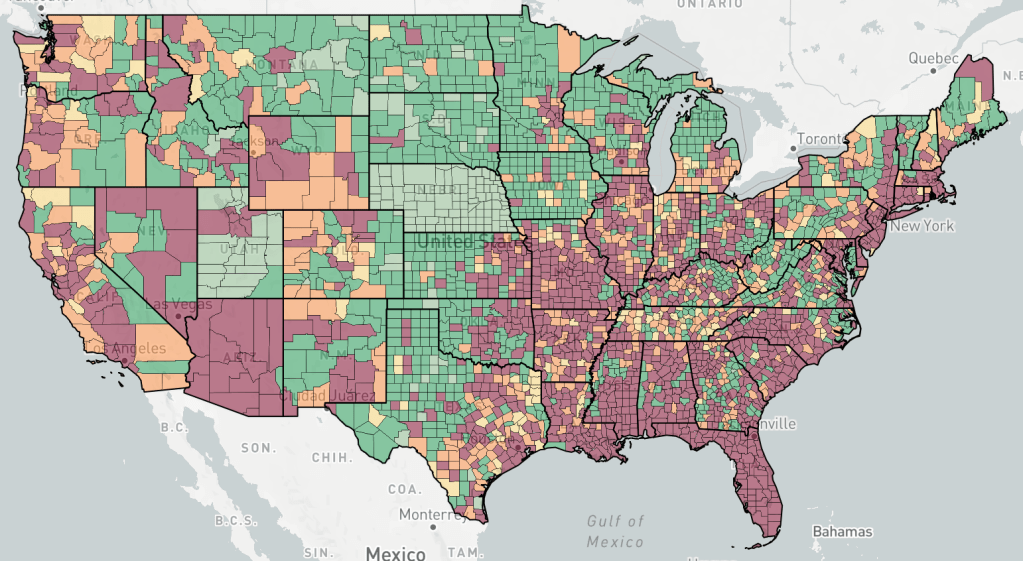
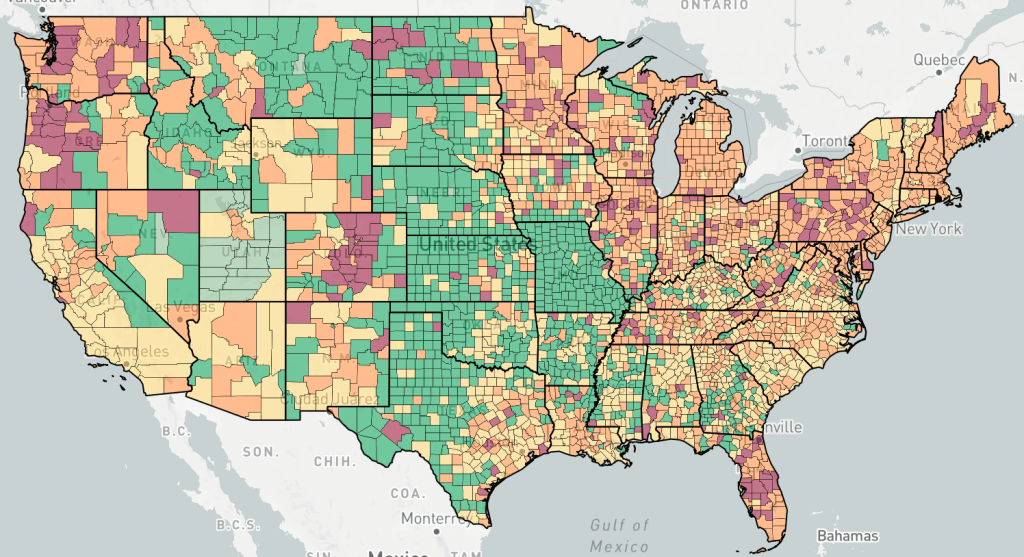
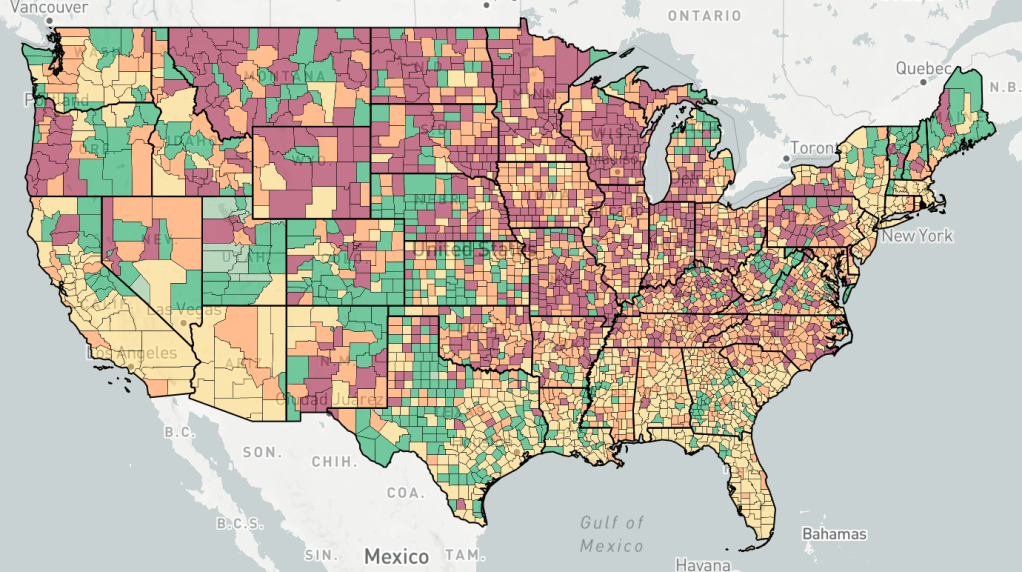
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Endcoronavirus County Level Map, July 6th, 2022Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
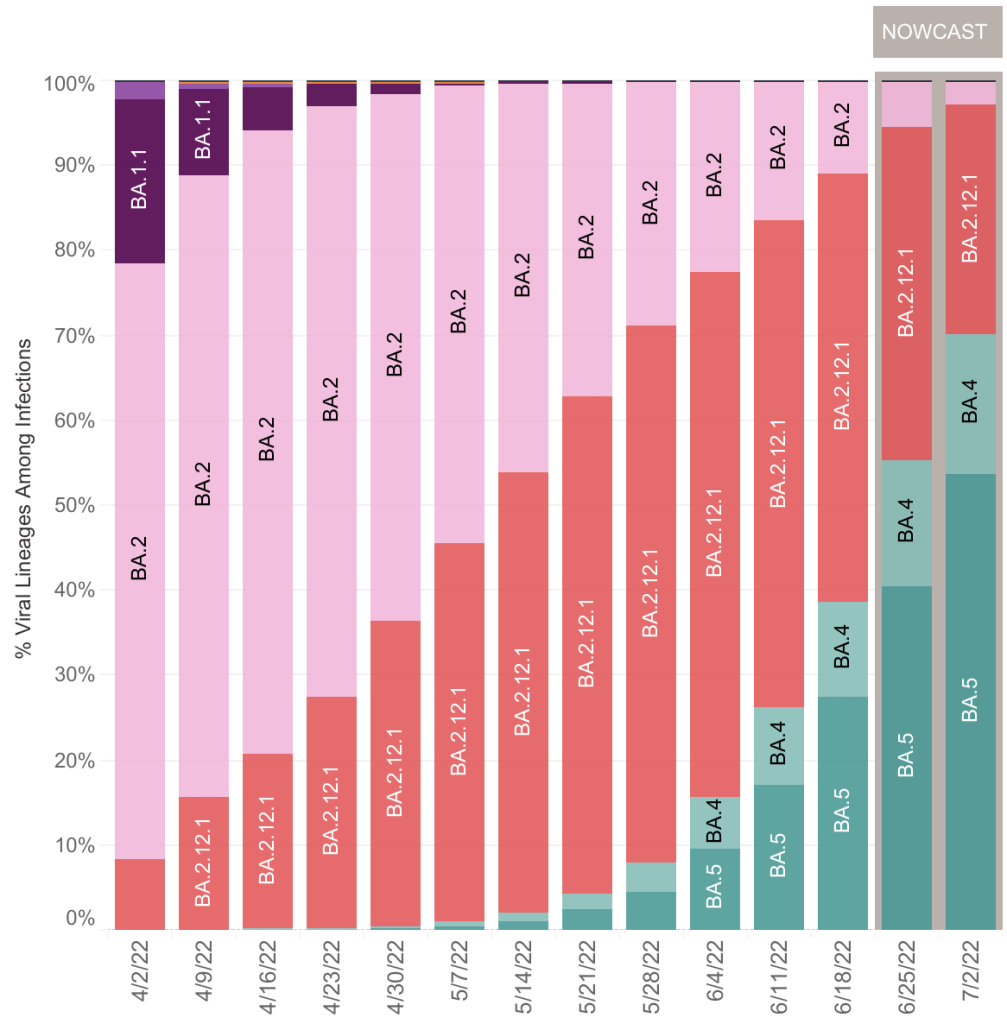
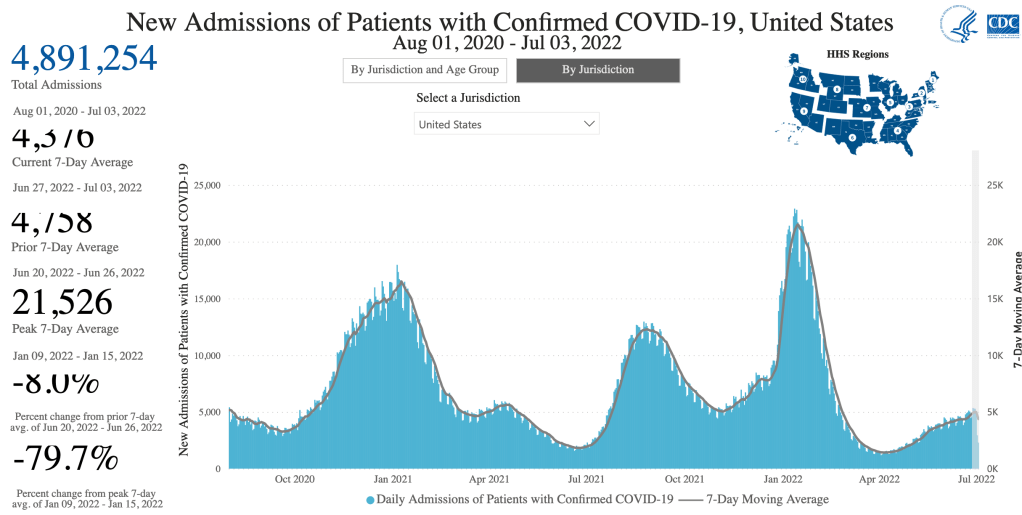
BA.4 and BA.5 now predominate in the US, being 17% and 54% of cases respectively. Together, they are 70% of new cases. Hospitalizations are up slightly, but not nearly so high as in January, at the height of the Omicron wave.
Keep in mind that many and perhaps most people who have COVID right now are not getting tested by a health care provider, and are not being treated, so they are not a “case” and do not appear in current statistics. While it’s great news that we haven’t yet seen increased deaths in the US, there is sobering news which may cause a change in this in the next few weeks.
BA.5 reinfecting Omicron patients: A few weeks ago, an urgent care doctor friend of mine said that he had seen some patients who have had Omicron twice. Just this week, some friends of mine who had Omicron in January, just like me, came down with it again. They have COVID right now. Like me, they were pretty miserable in January for a full 2 weeks. Happily, their symptoms are moderate now, like a bad cold, just for 2 or 3 days.
Just yesterday, John Campbell released a video regarding BA.4 and BA.5. While he has a pretty bland delivery and focuses on the UK, he’s honest, balanced, and one of the only pundits still covering COVID in any detail.
Dr. Campbell’s newest video has some sobering information about BA.4 and BA.5 variants. As you can see from the data above, BA.5 is more infectious than BA.2 and BA.4, and will probably become dominant in the US in the next few weeks.
While still being called an Omicron variant, I wouldn’t be surprised if BA.5 gets it’s own Greek letter. Maybe Pi or Rho.
Unfortunately, Dr. Campbell claims that BA.5 is different enough from earlier Omicrons that they do not provide robust protection against BA.5 infection. He says Omicron is “poorly immunogenic”, but later clarifies in the video that this is likely because SARS-2 variants are changing very rapidly right now. The current COVID vaccines are having little impact, and the virus is changing so rapidly that updated vaccines are not practical to produce, meaning that the age of COVID vaccines is really already over.
For some good news, reinfections are usually milder than previous cases. So if you’ve already had COVID, BA.5 is likely nothing to be worried about.
Portugal had a lot of BA.4 and BA.5 in May and June, and they experienced more hospitalizations and deaths. Some worry that BA.5 may produce more severe cases in “naive” people, those with neither natural nor vaccine mediated immunity. Drs. Kei Sato and Stephen Griffin claim that BA.5 is growing deep in the lungs, like pre-Omicron versions, which makes it more likely to produce pneumonia. Most Omicron variants grow primarily in the trachea, which is why they are less likely to produce severe disease.
Last, Dr. Campbell argues from a letter by Hachmann et al, that prior infection plus vaccination offers better protection than either alone, but that BA.5 is still escaping neutralization. In my personal view, vaccination carries risks of it’s own, so if you are still not vaccinated, I would suggest taking increased precautions rather than vaccination at this point.
Cases in the UK are rising quickly right now, and often is a few weeks ahead of the US in any recent COVID trend. If data from Portugal and the UK hold true in the US, we may expect increasing cases in the US and perhaps more deaths as well.
Viruses have a tendency to become more infectious and less pathogenic over time. While this has been shown to be true many times in the last century, this is only a tendency and does not always hold true. While BA.5 is more infectious than previous versions, it’s tendency to grow in the lungs may make it more dangerous, so BA.5 is bucking the trend.
Strategies: Of course, it can be very hard to predict what will happen next. We also have a lot of different COVID experiences in the US in terms of whether someone has had COVID, what variant they had, whether they were vaccinated, etc. So any suggestions I make may not pertain to you.
Since I had COVID in January, I’ve been behaving in public as if I’m totally protected against a new infection. This may have been warranted, since I haven’t been infected again. I’ve even visited people with COVID at their house, treating it as an opportunity for a free booster. But this new information gives me pause. I may be more vulnerable to BA.5 than I had hoped.
On the other hand, even BA.5 is mild in those with previous infections, so I will likely be OK if I get BA.5. I am still not vaccinated and don’t intend to be. So going forward, I am going to continue to behave as normal, without masking in public at this point.
My main reason for being so careful before I got infected was the Antibody Dependent Enhancement (ADE) issue. Now that I’ve been infected, it’s not useful for me to continue with my previous caution. In fact, the “free booster” method may now help me with future versions more than avoiding infection would.
If you have never had COVID, you may choose to take increased precautions to prevent infection. Wear an N95, KN95, or KF94 mask when indoors in public. Don’t wear a cloth or blue surgical mask. These masks will not protect you from BA.5. Vaccination alone is not likely to be of much protection from BA.5.
If you do end up being infected with BA.5, regardless of the severity of your symptoms, stay home until you’re COVID negative to protect those around you who may be vulnerable.
Will COVID be endemic? A client of mine was kind enough to recommend my posts to his board, saying that my COVID predictions always come true! I would love this to be that case, but I can’t claim that kind of record. I have certainly been wrong during the pandemic. In particular, I’ve said that Omicron will end the pandemic, and that it will won’t likely have a new dangerous variant. BA.5 may end up proving me wrong on both counts. The lightning speed that new variants are developing also challenges my previous statements. I can’t claim to always be right, but I will tell you as soon as possible if I’ve been wrong.
So will COVID last forever? In spite of BA.5, I still say no. While it has exceptions, the tendency for new viruses to be less pathogenic still holds true. I still expect new variants to generally be less dangerous than older ones. In fact, BA.5 will likely still have less impact than previous versions simply because so may people have previous infections.
In yesterday’s post, I outlined some of the factors that resulted in the very high COVID case rate in the US. Today I will discuss how we can prepare for the next pandemic.
I have a PhD in molecular biology, and I specialize in infectious disease testing. I am not a physician or epidemiologist. I have an informed but not expert opinion.
Identifying the threat:
First, most new infectious diseases do not pose a global threat. SARS-2 was so dangerous because of its high infectivity, long incubation time, and asymptomatic spread. Most diseases do not have these parameters. Whenever a new disease comes around, and they will, we should soberly and cautiously assess the real threat. Coming to the wrong conclusions about the threat will lead to the wrong conclusions about combating it.
There have been several important new infectious disease outbreaks in the last few years, including Hantavirus (1993), SARS (2003), Avian Influenza (2004), H1N1 Swine Flu (2009), Ebola (2013), Zika (2015), and of course HIV in the 80s. They all have different disease parameters which make them behave very differently. Most of these diseases did not have global impact. The first SARS for example was much less infectious than SARS-2, but much deadlier, so it was contained quickly and didn’t spread much beyond Asia. HIV can be spread by asymptomatic victims for a full 8-10 years, avoids the immune system, and evades vaccination efforts, so it has become endemic in much of the world.
The following parameters determine how a new disease will behave:
Mechanism of spread
Infectivity
Asymptomatic/ambulatory spread – can the victim walk around and spread disease?
Incubation period
Fatality rate
Vector – what carries the virus to a new host
Non-human reservoir – diseases that come from non-humans are harder to control and cannot be eradicated.
Obviously, we cannot respond to different diseases in the same way. Part of the reason we failed to contain the virus was that we used measures that were designed for viruses that spread by droplet transmission against a virus that spreads through aerosol transmission. Using the wrong measures was less effective.
Much of my concern with the SARS-2 virus was the Antibody Dependent Enhancement issue, which is very uncommon among viruses, so is not usually a concern.
Be cautious. Whenever a new threat arises, it is wise to be extra cautious until information can be gathered. Although many of our precautions turned out to be unnecessary, I still support taking extra precautions early on. Remember that early estimates were that the fatality rate for COVID was 3.68%. With the 82 million confirmed cases in the US, this would have been over 3 million deaths if the fatality rate had really been this high. As it stands, we have had almost 1 million COVID related deaths, a death rate of approximately 1.2%. Yes, I know we can debate how many of these are deaths really resulted from COVID and how many infections there really were. But we cannot discount that COVID had an enormous impact.
What if COVID were deadlier? Or what if it had selectively killed children, or caused more long-term symptoms like polio did? Things would have been much different.
All this to say, I think caution was warranted in the beginning of COVID, and we should continue to be cautious in future pandemics. On the other hand, we should also learn to abandon precautions that are not effective. Maintaining ineffective precautions wastes resources, causes extra economic and social suffering, and causes people to lose confidence in government agencies. It started to become clear to me by May of 2020 that lockdowns were ineffective, and that transmission was happening mostly indoors, but I still see people wearing masks outside to this very day.
Persuasion, not coercion: From the beginning of the pandemic, public communication was terrible. Official guidelines were confusing and often contradictory. Far worse, explanation or evidence was rarely given for policies. Instead, disagreement was met with accusations of being anti-science, rather than persuasion. This approach contributed to the loss in confidence in official channels.
Going forward, officials need far better communication skills when dealing with emergencies. Give evidence rather name-calling, and respect the population enough to tell the whole truth.
Then came the vaccine mandates. Many people I know were coerced into getting vaccinated against their will, and many others were fired. All at a time when information about the vaccines was being hidden from the public. This is unacceptable, and no way to run an emergency.
Restoring Trust: Both the CDC and FDA hid information from the public. In order to restore confidence, senior leadership needs to be replaced and new leadership should explain how things will be better in the future. Is likely to happen? No, it is not.
Government agencies need to be far more transparent. Lack of transparency forces people to wonder what is going on, and create their own theories. Government agencies often decry conspiracy theories, but they had a big role in creating them.
Misinformation: Freedom of speech, censorship, and misinformation had a major role in the public discussion over the pandemic. Doctors and scientists were frequently censored, shunned, or fired for sharing ideas that went against WHO or CDC guidelines. This includes ideas like the lab leak hypothesis that later turned out to be likely.
Freedom of speech is a foundational principle of American life. It’s in our DNA, as some would say. We are not America without it. Some will say that too much freedom of speech leads to misinformation and conspiracy theories. While it’s true that this freedom allows the spread of falsehoods, it also allows all ideas to be debated, true ideas to be raised up, and false ideas to be discredited. Freedom of speech is the solution to misinformation, not the cause. Most of the leaders in world history that wanted to control freedom of speech had something to hide. It is essential that we maintain this basic right.
State emergency powers: As discussed in yesterday’s post, the US federal government has surprisingly little power to deal with a public health crisis. The CDC can develop guidelines, but most of the real work is done at the state and local level. State officials need to step up and realize it’s their responsibility to respond well. Citizens need to hold state and local officials accountable.
Manufacturing: The US needs to maintain manufacturing capacity for certain essential items like personal protective equipment, testing kits and equipment, and medications. Tax incentives need to exist to encourage companies not to send these functions overseas.
In addition, we should have national and state stockpiles of certain equipment. I know many hospitals and labs are now creating stockpiles of their own.
Testing: Most countries that did well produced lots of COVID testing early. In the US, the CDC tried to manage all the testing themselves, and quickly became overwhelmed. By the time private labs were allowed to develop their own tests, it was way too late. Testing capacity didn’t become nearly adequate until at least July of 2020. Next time, the CDC needs to allow testing by private labs right away. Ideally, anyone who wants a test and anyone potentially exposed to an agent should be tested.
Quarantine, not Lockdown: Countries that did well did not quarantine healthy individuals, although some of these countries had more restrictions during the big Winter waves. Instead, only COVID positive people should be quarantined. This is only effective when tests are readily available.
Later in the pandemic, some outlets acknowledged that most infections were happening in private settings. Basically, people would get infected outside, then bring COVID home to infect everyone in the household.
Here is a very interesting video using computer models to show why our model of lockdown was not effective. Computer models are only as good as they are programmed to be, so this is only for demonstration purposes, and is not data.
Contact tracing: Contact tracing was very successful in some countries, but the long incubation time of COVID made this difficult. Successful programs involved tracking of individuals by cell phone and credit card data, practices that would probably not be tolerated in the US. Such programs would need to be voluntary to not trigger the creepiness factor and violate constitutional rights.
Masking: I was a big proponent of wearing a medical grade respirator (N95, KN95, or KN94) indoors during the pandemic. Because COVID spread as an aerosol as well as droplet form, cloth and blue surgical masks were ineffective. Simpler masks can be effective against colds and flu, however. So the choice of mask depends on the agent in question. CDC guidelines need to reflect the method of spread of the agent in question.
So what should Dr. Fauci have said early on? Something like this:
“N95 masks offer the best protection against infection by the SARS-2 virus. However, our current supply is very low, and we desperately need to save these masks for our medical professionals. Please do not purchase N95 masks at this time. In the mean time, there are some options that will help reduce the risk…”
In actuality, of course, I didn’t see an N95 in a store from March 2020 until at least February of 2021, so I couldn’t have bought one if I’d wanted to!
Treatment: Most medical facilities in the US didn’t treat COVID until a patient was experiencing respiratory distress. By then, treatment options were limited. To their credit, intubation was largely abandoned by the medical community when it was learned that this treatment was largely ineffective.
However, controversy swirled over potential treatments that became disfavored by the medical community. Doctors are usually granted the right to prescribe “off label” medications, meaning they can use medications for treatments outside the guidelines of the manufacturer. But drugs like Hydroxychloroquine, Ivermectin, and others quickly become forbidden, and some doctors even got fired for prescribing them. Research on these drugs were minimal.
I am not arguing here that these drugs are effective against COVID. I’m simply saying that forbidding doctors from working with or publishing papers about these drugs was a big mistake. While it is of course wise for a doctor to consider guidelines, treating a novel virus may require some “outside the box” thinking.
Let me know in the comments if I missed something important!
Today I’ll discuss the approach to the pandemic in the United States, and all the factors which contributed to our very high case load during the pandemic. This article ended up being longer than I thought, so I’ll have a separate post later in the week about how we can prepare for the next pandemic. I have a PhD in molecular biology, and I specialize in infectious disease testing. I am not a physician or epidemiologist. I have an informed but not expert opinion.
The COVID-19 pandemic finally seems to be drawing to a close. For most of the pandemic, the US had the highest number of daily cases, and has had the most cases over all. As I write this on May 17th, 2022, the US has 82,629,736 total confirmed cases, approximately 25% of the population, and an unknown but likely very large number of unconfirmed infections.
Meanwhile, the US has the most technologically advanced and well funded medical system in the world. So what happened? This is a very important question because answering it correctly will help us respond to the next pandemic.
First, we can ask what policies the US had in place, and contrast them with policies that were successful.
Countries that initially did well were Taiwan, Japan, Singapore, and South Korea. These countries are right next to China, which is the natural source for the seasonal flu. This is because flu viruses exist natively in aquatic birds from southern China, and there is no practical way to eradicate the flu. We can expect dangerous respiratory viruses to arise from China from time to time. Neighboring countries know this and are naturally vigilant. The citizens of Asian countries are used to wearing a mask whenever they have the sniffles, and they are prepared for local epidemics.
South Korea had the following strategy:
Early free testing for anyone who wanted a test.
Contact tracing of people exposed to infected individuals. Cell phone and credit card data was used to track residents and produce contact information for infected people.
Quarantine COVID positive patients at home, fines imposed for breaking quarantine.
Nearly all citizens wore masks in public.
Treatment of patients with moderate symptoms.
No “Lockdowns”, that is quarantining COVID negative individuals, but schools, cinemas, and gyms were closed. Most stores were open. Vaccine passports allowed access to high risk areas during the Fall and Winter of 2021/22.
By contrast, the US, and most of the Western world, had the following policies:
Testing only for symptomatic people.
Treatment only for severe cases.
Early “Lockdowns” of all but essential workers.
Contact tracing applied too late to be effective.
Early communication on masks was incorrect and even deceptive to avoid a run on N95s which happened anyway. Mask wearing remained controversial and unevenly applied, medical grade respirators unavailable or rarely used for most of the pandemic.
I will point out that most countries, even Japan, South Korea, and Taiwan, had major outbreaks during the Omicron wave. These countries did have some COVID related restrictions during the Winter of 2020/21 and during the Omicron wave. I leave China out of the analysis because I don’t trust their data.
Most respiratory viruses like cold and flu are spread by droplet or contact transmission. However, SARS-2 is spread by aerosol transmission. Droplets and aerosols are similar, but an aerosolized droplet is much smaller and can linger in the air for much longer than a droplet, more like a cloud than a spray.
Several precautions than became common and even required are designed to prevent droplet transmission rather than aerosol transmission. These precautions include 6 foot distancing, cloth and blue surgical masks, and those plastic shields at the store. These measures are mostly ineffective at preventing the spread of aerosols because they do not prevent the movement of small particles. As you know, I was a strong advocate of masks indoors during the pandemic, but only the medical grade respirators like N95s, KN95s and KF94s.
Peculiarities of the US: In addition to prevention policies, the US has several cultural and demographic factors which contribute to our high infection numbers.
Population: Americans know that the 2 most populace countries in the world are China and India, with about 1 billion people each. These populations appear to dwarf our own estimated population of 330 million. But we forget that the US is the 3rd most populace country in the world, with number 4 being Indonesia at 272 million. Japan has 125 million, and the most populace European country, aside from Russia is Germany at only 82 million.
Mobility: The US is an enormous country, and Americans are used to traveling much more than other peoples. We may not fly to other continents as much as the Germans do, but we don’t hesitate to drive several hours for the weekend, or fly across the continent. I was having lunch with an Englishman once who said they might plan for weeks to take a trip that would involve a 3 hour drive. Many Americans may only plan for a few hours for such a trip. Our high mobility certainly contributed to our high COVID numbers.
Independence: Our independent nature has been an enormously useful quality, contributing to our high innovation, personal freedom, and economic prosperity. So I’m certainly not arguing against American individualism. But I have to acknowledge that our fierce sense of independence did contribute to non-compliance with government recommendations. And yes, I totally understand that many official recommendations were ineffective or unlawful. But this factor is part of the equation that we will need to consider in order to deal with future pandemics.
Federalism: The US Government has a lot less power than most people think. The 10th amendment states:
The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.
This means that the only powers the federal government has are those expressly given to it in the Constitution. Much of what the US government does now goes beyond the powers given by the Constitution, and is only done because no one has stopped them. New federal powers are often popular, so they go forward unchecked.
The pandemic has caused many to lose trust in several previously trusted federal agencies, and States have started to pull back power from the US. Many were surprised to discover how limited the President’s power was during the pandemic, limited to suggesting guidelines and creating regulation for federal property and interstate travel. The vaccine mandate attempted to use private companies to enforce vaccination, but even this was struck down by the Supreme Court.
Emergency powers outlined in the Constitution only apply in the case of an insurrection or invasion. Unless a Constitutional amendment is passed, the Federal Government can only impose martial law if an emergency forces the courts to close (Duncan v. Kahanamoku, 1946).
States have much broader powers. In California, the Emergency Services Act allows the Governor to declare a state of emergency at any time, a state which grants him broad powers, including the power to suspend certain laws. Some have said that this state can only last 90 days without approval from the Assembly, but the ESA allows the Governor to end the state of emergency whenever he deems it necessary, “at the earliest possible date that conditions warrant.” (§8629).
All this to say, the states have much more power to address a pandemic than does the federal government. Whether you find this good or bad news depends on your own political leanings, and the state you live in!
Manufacturing: The national shortage of N95 masks early on in the pandemic painfully revealed that our domestic capacity for manufacturing certain necessary items fell woefully short. Other items in short supply were hospital gowns, gloves, disinfectant, certain medications, and yes, even toilet paper.
This shortage meant that almost no-one had effective masks early on. In addition, confused messaging from Dr. Fauci and the CDC later produced a condition in which ineffective masks were common in public areas. This certainly had a big negative impact on our case load.
Misinformation and freedom of speech: I have written on this before, so I won’t repeat this now. Suffice it to say that many Americans lost confidence in government agencies, including the CDC and FDA during the pandemic. Lost trust is hard to regain and it can take a long time to get back. I’ll discuss this more in my next post.
Political polarization: Similar to the erosion of trust in government agencies, the response to the pandemic quickly became a “team sport” with some responses being typical of the “blue team” and others typical of the “red team”. Unfortunately, both sides often opposed reasonable ideas simply because they came from the other side. Also, some terrible ideas had a longer life span than they should have because they were favored by certain political groups. As I’ve said many times before, science and politics are a terrible combination. When politics gets involved in science, the results are usually terrible.
Frankly, things have become so polarized that I am pessimistic about the future. Republicans and Democrats seem to disagree strongly about nearly everything these days, having fundamental worldview differences, not just differences in approach. I know lots of people who lost contact with friends and even family during the pandemic, as have I myself.
Let me know in the comments what factors you think contributed to our response. Later this week, I’ll post on the next pandemic, and how we can prepare.
This is a case update. I’ll also give an update on the state of Omicron in the US, and show some data from a great new paper from California. I’ll also comment on the new mask guidance by the CDC.
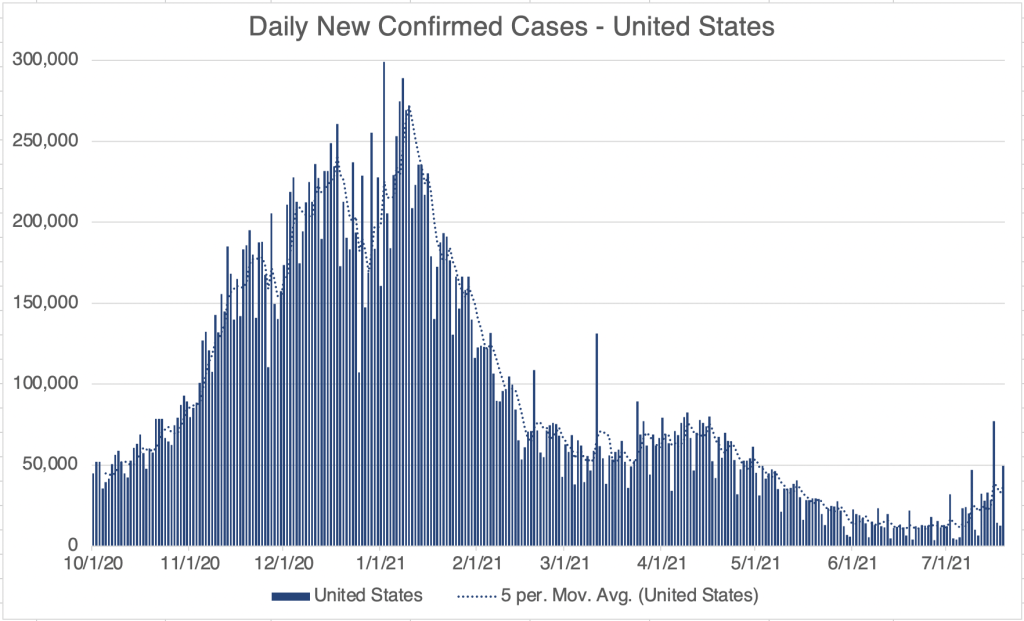
New cases have apparently peaked in the US over the past week, reaching a high of 1.5 million cases in 1 day. Cases are now declining for the US as a whole, driven by declines in several Eastern states like New York, New Jersey, and Florida. Cases have not yet declined in most US states, although many may be peaking right now as new cases have slowed. So far, deaths are only slightly up for the US. Hospitalizations appear to have peaked as well.
California and San Diego County new cases appears to be still going up, but new cases have slowed, and I suspect will start declining soon, maybe this week. Again, deaths have not yet started to increase. Deaths usually follow cases by between 2 and 4 weeks.
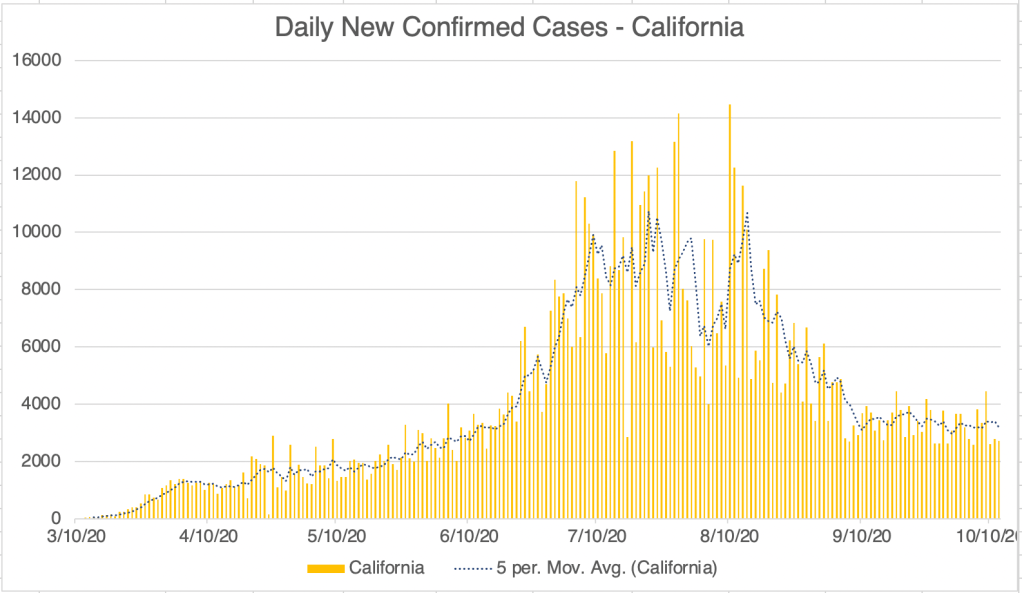
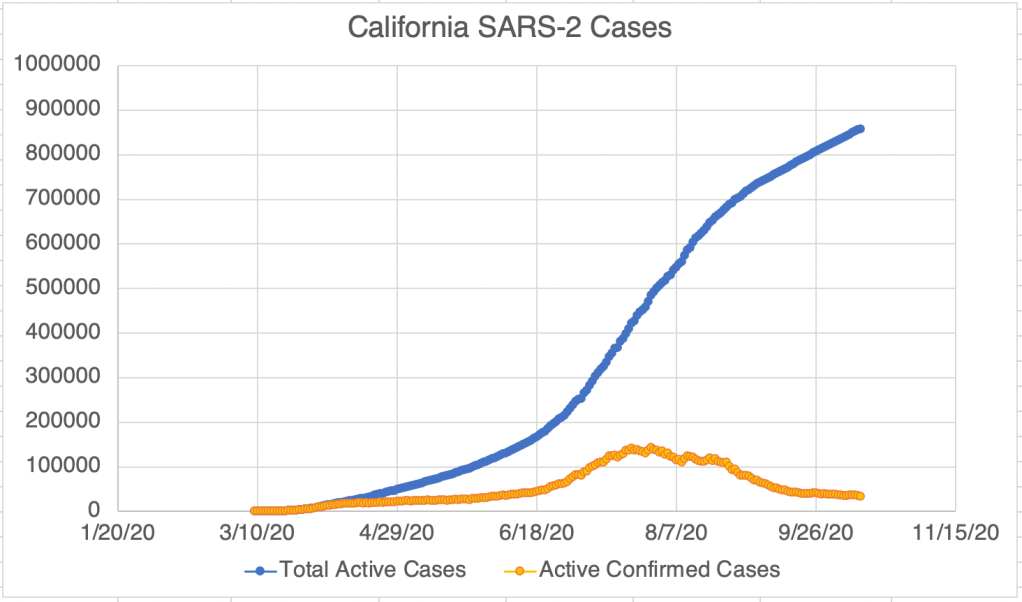
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
Omicron Update: Omicron infections now represent 99.6% of infections in the US. Omicron has now almost completely eliminated Delta in the US. It continues to appear that Omicron represents the end of the pandemic, although it will go out with a bang!
I finally got COVID!: Last Friday I tested positive for COVID! I almost certainly got it while in a “gray area” situation that had some risk, but might have been OK with a previous variant. Most symptoms have been very mild, but I was super achy for a day. I’m still not feeling strong and I nap a lot. No loss of taste and smell, or shortness of breath, but I did have a fever during my achy day. As of yesterday, I still test positive, so my body is still fighting.
Omicron much milder than Delta, but evades vaccines much more: As I’ve stated before, it’s a little scandalous how few useful papers have come out of the US this last year. But a UC Berkley lab has a great new paper in pre-print right now. They had the foresight to collect data for a time period in December when both Delta and Omicron were present in the population. The paper is a little opaque because much of the information is in dense tables, with less than useful headings (SGTF = Omicron, non-SGTF = Delta) but has some great information nonetheless.
Table S10 is the most interesting to me. I’ve turned some of the data into graphs to make the meaning more clear. The table compares the number of infections by Delta or Omicron in unvaccinated persons, those with differing levels of vaccination, and with documented previous infection (natural immunity). Vaccination definitely helps prevent infection by the Delta variant, but Delta still infects vaccinated individuals. This may be because vaccine efficacy goes down over time, the Delta variant is too different to be completely stopped by the Wuhan based vaccines, or some combination of both.
Graph is by me, from data in Lewnard et al, Table S10. Cases with Natural Immunity were multiplied by 6 to normalize for the number of documented infected individuals in the population. In San Diego County, there are roughly 500,000 documented COVID-19 cases, out of a population of approximately 3 million in the county.Graph is by me, from data in Lewnard et al, Table S10. Cases with Natural Immunity were multiplied by 6 to normalize for the number of documented infected individuals in the population. In San Diego County, there are roughly 500,000 documented COVID-19 cases, out of a population of approximately 3 million in the county.
Omicron is far more infectious in general, and also is far more infectious in vaccinated individuals. In fact, more people in this study were infected by Omicron if they had 2 doses of the Pfizer or Moderna vaccines. Since a majority of Southern Californians are vaccinated, it this does not necessarily mean that vaccination made it more likely to be infected by Omicron, but it’s a striking result. Yes, Antibody Dependent Enhancement may play a role in this result, although the exact reasons are likely a complicated combination of factors.
Another interesting result is that infections are far lower among those with previous infections. For the graphs I include, I’ve even normalized this number for the proportion of people who have been infected by multiplying the given number by 6 (see graph for details). In spite of this, infections are FAR lower in those previously infected. This is consistent with the data from Israel suggesting that natural immunity is far better than vaccination at preventing future infection.
Most European countries and Israel include previous infection in immunity requirements. The US still does not accept previous infection as prove of immunity. As we continue to argue about vaccine mandates, it would be wise to include previous infection as proof of immunity.
Better super late than never I suppose: After many months of treating all masks as essentially equal, the CDC released new guidelines regarding masks that points out that simple cloth masks are not as effective as medical grade respirators like N95s, KN95s, and KF94s. They still don’t go far enough in my opinion, since they still promote surgical masks as effective. Blue surgical masks are loose fitting on the side and allow air to enter and exit without being filtered. If you wear a mask, wear a medical grade respirator, not a blue surgical mask.
I believe we are a few weeks away from the end of the pandemic! As for me, I’m really looking forward to eating indoors at a restaurant again!
I know a lot of this post is dense and complicated. Your questions will help me be more clear.
This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Origin: Controversy over the origins of the SARS-2 virus began very early in the pandemic. The most common theories were that the virus arose naturally at a live animal market in Wuhan China, where animals from a wide variety of species are sold. The predominant theory is that the SARS-2 virus arose in bats, then transferred to another animal, perhaps a pangolin, before moving to humans. This has been the most accepted theory for the majority of the pandemic, promoted by the WHO, the CDC, and American media.
The lab leak theory, the idea that the virus arose from the Wuhan Institute of Virology, was present from the beginning, but was heavily disfavored by official channels for most of the pandemic. On May 23, 2021, the Wall Street Journal published an article that gave evidence for idea, followed closely by an article from Vanity Fair. The articles normalized discussion of the theory and as of this writing, polls show that a majority of Americans believe that the virus came from the WIV.
Emails between several virologists, public health officials and Dr. Fauci strongly suggest that this group believed that the virus may have come from the laboratory as early as January 31, 2020. However, this same group published a scientific article on February 9th supporting the natural origin theory. The paper was at odds with discussion in the email correspondence. If investigations show that the group published claims they knew to be false, this would represent a significant case of scientific fraud.
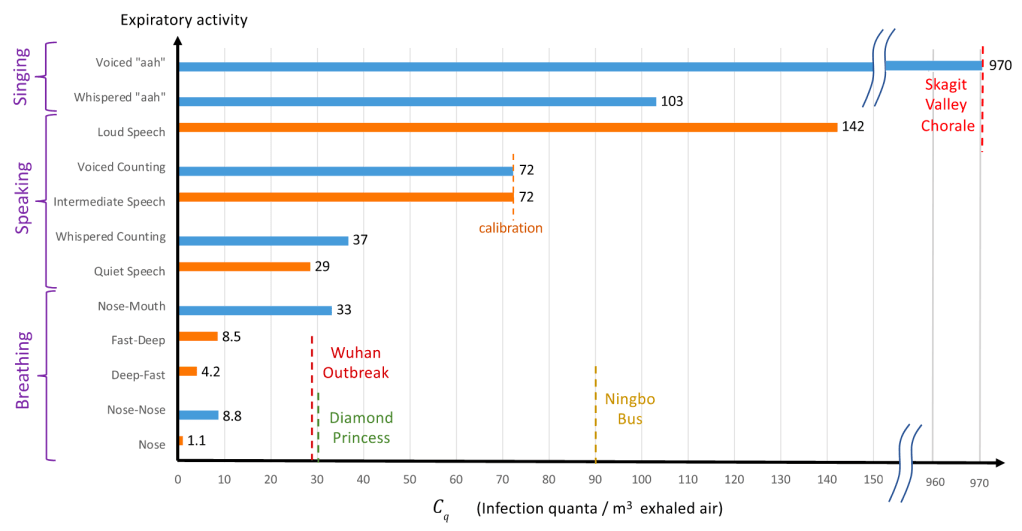
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, outdoor transmission of SARS-2 appears to be extremely rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable viral can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include:
age asthma or COPD heart conditions kidney conditions liver disease high blood pressure diabetes obesity auto-immune disease use of NSAID anti-inflammatory medications being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant) vitamin-D deficiency type A blood (Type O appears to be protective) inadequate sleep
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms. Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection or lowers the viral load of exposure. N95, KN95, and KF94 respirators are effective at filtering close to 95% of virus. A good mask is well fitting and filters the air moving in an out of your mouth and nose. The commonly used surgical masks and other loosely fitting masks do not filter air and I don’t recommend using them.
Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection. Social distancing may be more important for droplet transmission, like the flu, than for aerosol transmission in which microdroplets can stay suspended for much longer and travel much further.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US. Supplementing Vitamin C and Zinc is also recommended.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
I’ve been traveling all over the country, and have been in dozens of airports, gas stations, and stores. I get tested regularly and have always been negative. Here are the precautions I use:
1) Wear a mask or face covering indoors in public. Now that vaccines are available, I no longer avoid unmasked people indoors, but as an unvaccinated person, I still wear mine. 2) Keep 6 ft away from others. (I basically ignore this one if other precautions are in place, especially on an airplane!) 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. This is now voluntary now that we have vaccines, as an unvaccinated person, I still follow this rule. 4) Outdoor gatherings are fine, even without masks, if everyone maintains a distance. I have hosted several outdoor gatherings. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however. 6) Wear an N95 or KN95 mask when going to more high risk areas like airports or public areas where people may gather. These masks are rated to filter out 95% of viral particles. In my opinion, surgical masks and especially neck gators are nearly worthless in these settings. 7) I never take my mask off on the plane, and find an isolate spot in the airport to eat or drink on layovers.
Vaccinated people can relax many of these rules! Vaccines are 90-95% effective, so you still have a small chance of infection.
Testing: There are several kinds of tests, and they tell you different things.
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test. They can take longer to process because they need specialized equipment that most small labs don’t have, so most of the wait time is just for shipping to a specialized facility.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody. These tests are cheap and fast, but are more prone to false positives and false negatives than PCR tests.
Antigen: These tests use a very similar technology to Antibody tests, but instead of detecting a patients antibodies against virus, they use antibodies to detect viral proteins in a sample. An “antigen” in immunology lingo is just a protein that can induce an immune response. So in this context, an “antigen” is a SARS-2 protein that can be bound by an antibody. Like PCR tests, these tests detect an active infection, because they detect viral proteins currently in the body.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR but more prone to false negatives.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Antibody Dependent Enhancement:I’ve written about this a lot and I won’t describe it in depth here. In short, this pathway allows some viruses to create more severe disease on the 2nd time infecting a person than the first. It is theoretically possible, perhaps even likely with SARS viruses, which is why I have been careful to avoid infection and why I’m not going to get the vaccine unless perhaps my work requires it.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Supportive care: Most treatment is supportive care, treating symptoms while the patient recovers naturally. Anti-inflammatory medications are often used to prevent the immune system from over-reacting to the virus.
Ventilators/nasal cannula: While widely used early on, some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor oxygen therapy using a nasal cannula, using ventilators only as a last resort breathing if labored.
Remdesivir: This antiviral was used widely for much of the pandemic, but many sources now claim it has limited effectiveness.
Dexamethasone: Steroid used to treat patients with low oxygen levels.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. Treatment with Ivermectin is likely more beneficial in a wider range of disease state than HCQ.
Ivermectin: A anti-parasitic medication used since 1981, Ivermectin has reportedly been used by doctors around the world, notably India and Mexico, to reduce COVID fatalities. Reports claim that Ivermectin is beneficial in a wide range of disease state, from pre-disease prevention to late stage disease. Like Hydroxycholoroquine, promising data was often labeled “misinformation” by outlets in Western countries, and western doctors were strongly discouraged from prescribing it. Thus, experimentation with Ivermectin was hindered and the drug’s potential is still unknown.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Several vaccines against SARS-2 were finally released to the public in December of 2020. The vaccines released to the public are in 2 types:
Attenuated vaccine: This type has been commonly used for decades for a variety of viruses. The technique makes a severely weakened form of the virus that still makes viral proteins that provoke an immune response. With this type of vaccine, the patient is infected by a weak form of the virus that they quickly recover from, usually with no symptoms other than occasionally the flu like symptoms that are your body’s natural response to invasion.
mRNA vaccine: This is a brand new technology that has been worked on for years. The SARS-2 vaccines are the first ones that have been introduced to the public using this technology. The vaccine includes a piece of mRNA inside a lipid bilayer that mimics the cell wall. The mRNA is inserted into the cell where it is translated into a copy of the viral Spike protein. These vaccines are 90-95% effective against infection, and even those infected have less severe symptoms. However, they are not 100% effective, so some infections of vaccinated individuals has occurred.
As has often happened, the vaccines have generated significant controversy. As you know, I have been careful to avoid being infected and also getting the vaccine because of the potential of ADE. My concern with the vaccine actually has nothing to do with the new mRNA technology, I actually have no reservations about the mRNA vaccines. From an ADE perspective both the attenuated vaccines (Johnson & Johnson) and the mRNA vaccines (Pfizer and Moderna) produce Spike protein that may trigger an ADE response should a new strain of SARS virus appear, not a variant, a new SARS strain, like a “SARS-3”.
When the vaccines were released, rumors of side effects, sometimes severe, arose immediately. For some time, I minimized these as a risk of any vaccine. All vaccines carry the risk of side effects and even death. However, a video podcast featuring Robert Malone, the inventor of mRNA vaccine technology, convinced me that the Spike protein itself has toxic properties of its own, separate from the vaccine technology used. This is because the Spike protein can bind to cells all over the body and may have wide ranging effects.
Despite ADE and issues with side effects, I actually still believe some will benefit from the vaccine. These include the following groups:
Anyone over 60 Anyone with 1 or more risk factors:
obesity certain auto-immune diseases use of NSAID medications heart, lung or kidney condition immunocompromised patients (HIV, cancer and transplant patients) respiratory condition such as asthma or COPD.
Frequently working with the public Musicians who sing in indoor settings Medical personnel
Again, I am not a physician, so check with your healthcare provider while making decisions about getting the vaccine or changing your medication.
If you’ve had the vaccine or had COVID and are concerned about ADE, remember that it will only become a factor if a significantly new strain arises (“SARS-3”). If this happens, then the procedure for you would be to be very careful initially, then get the “SARS-3” vaccine as soon as possible. The new vaccine will protect you from the new virus. In the future, vaccines against Coronaviruses will be produced even more quickly than this time.
The vaccines have pros and cons. I’m in support of vaccines for some but not necessarily for others. Each person needs to weigh the risks for themselves. I am not for companies or government agencies coercing individuals to get the vaccine.
Herd Immunity: The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. The idea is useful, but in my opinion, efforts to push people into getting vaccinated to achieve herd immunity are misplaced. Before a vaccine is available, the only way to reach herd immunity is to expose large numbers of people to the virus, which is counter productive. Now that the vaccine is available, those who are concerned should just get the vaccine themselves and not harangue others about getting it. Gentle persuasion may be convincing, but haranguing rarely is. Given even the pre-pandemic resistance to vaccines, a forceful effort to vaccinate is likely to back-fire.
Variants: During the course of the pandemic, several variants have arisen that have a slightly different Spike protein sequence from the original Wuhan strain. Confusingly, naming conventions have changed several times, making it difficult to keep them all straight. As a general rule, the variants have all been more infectious than the Wuhan strain, but have not been more pathogenic. Fortunately, the vaccines have been effective against all of the variants, although are not as effective against some variants.
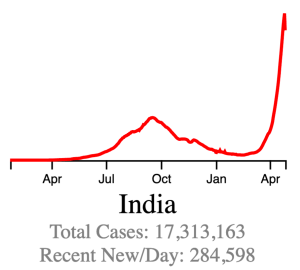
The Delta Variant: The UK/Alpha variant caused waves of new infections in some countries and was more infectious than the original Wuhan strain. In late 2020, a new variant arose in India, the India/Delta variant. This variant was significantly more infectious than other strains and has caused huge peaks in cases in several countries. As of this writing, several countries are still experiencing waves of new cases most likely due to the Delta Variant, including the United States.
While the Delta Variant has caused large numbers of new cases and an increase in hospitalizations, data suggests it may be less pathogenic than the Wuhan or UK variants.
Current Status: In late Spring, at least in the US, life began to get back to normal, with approximately 50% of the US population vaccinated, much lower new case numbers, and reduced restrictions. Currently however (July 21, 2021) a wave of infections, likely caused by the Delta variant, is causing concern and some calls for new restrictions. Several other countries scattered across the globe are also currently experiencing peaks in cases.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format and includes only the Fall/Winter 2020, Spring ’21, and Delta Variant peaks.Endcoronavirus County Level Map, July 20th, 2021Daily new confirmed cases in India, from data collected from Johns Hopkins University COVID site. The Delta Variant peak is the large one on the right. Notice the sharp upward and downward trends. The new persistent daily case numbers are higher than before the Delta peak began.
The Future: Since vaccination started in the US, there have been many fewer new cases. This has led many to basically go back to behaving normally. The Delta Variant is rightly causing concern, but I’m still hopeful that the current peak in new cases will be short lived. In other countries with Delta related waves, the peak has been very sharp, with quickly increasing, then quickly decreasing case numbers. However, I’ve started to be a little more cautious in public again, while we wait for the increase in cases to slow.
Several other countries are still experiencing an elevated case load. The pandemic won’t be truly over until cases are low in all countries. I’m hopeful that this will happen this year, but it’s certainly too early to know for sure. So far, all new variants have been susceptible to the vaccines and natural immunity. There is a small chance however, that we may see new versions that are not. If this happens, SARS may become endemic, circulating seasonally like the flu does. So far, I don’t see evidence that this will happen.
In the future, we may have a “SARS-3” a new virus from the SARS family that will be similar, but different enough to trigger the ADE pathway. If this happens, those of you that have had COVID or been vaccinated should be very careful to avoid infection initially, then get the “SARS-3” vaccine as soon as it is available.
In a future post, I’ll give my recommendations for what should be done differently if a new pandemic should arise.
I’m going to discuss the hypothesis that the SARS-2 virus arose from the Wuhan Institute of Virology. While I will attempt to avoid being overtly political, and the topic of the pandemic should not be political at all, we all know that many topics have taken on an unfortunate political tone and discussing them at all can become “problematic”. So I’m going to be problematic. In fact, F@¢3b00k may remove my post, so I’ll link to my blog page in a separate post.
You are free to disagree with my conclusions, but keep it civil. I retain the right to delete comments that don’t advance the discussion in a productive way.
Lab Leak Hypothesis: Since the beginning of the pandemic, rumors were swirling about the lab leak hypothesis. Also from the beginning, the idea was often discussed as if it were obviously a crazy conspiracy theory. I always thought it sounded plausible, and actually came to think it was likely by last summer. I didn’t write about it because I couldn’t prove it. It still can’t really be proven, but there is some evidence pointing toward the idea.
Please note: I do NOT currently see any evidence that the Chinese Communist Party intentionally released the virus as a form of bi0w∑@pon. I currently believe the release was accidental.
Until just a few weeks ago, the idea was basically forbidden to be taken seriously in polite society and would get you banished from F@¢3b00k, YouTube or Google. This changed suddenly when the Wall Street Journal and Vanity Fair published articles on the topic. Mysteriously, this made the dam burst, and now media from all over the political spectrum are taking the story seriously.
What evidence exists for the WIV being the source of SARS-2? Several pieces of circumstantial evidence and a few pieces of scientific evidence suggests a lab origin.
The first patients appeared in Wuhan China, the home of the Wuhan Institute of Virology (WIV). The lab conducts research into bat coronavirus, close cousins of the SARS-2 virus. The wet market often blamed for the outbreak is about 300 yards from the WIV.
Public records surveyed by Matthew Tye suggest that in late November, the lab posted a call for new employees for work on a dangerous new virus. Around the same time, a scientist at the lab, Huang Yan Ling, went missing. Her information was removed from the lab’s website. As of this writing, she had not yet publicly reappeared. Many suspect she is dead.
Tye used to reside in China, is married to a Chinese woman, and posts under the name Laowhy86. He is very critical of the Chinese Communist Party for several reasons, but not of the Chinese people generally.
The WIV had been doing experiments with “Gain of Function” research in which virus are given the ability to infect human cells in order to study them in a system relevant to humans. This practice is very controversial even among scientists, with many believing they are too dangerous to be done. The director of the WIV coronavirus program, Dr. Zhengli-Li Shi, co-wrote articles featuring this research (more on this later).
A paper was published by Andersen et al claiming that the virus was natural. However, the paper includes a sequence comparison showing a feature called a “polybasic cleavage site” that exists in SARS-2 but not in closely related coronaviruses. Similar sites exist in the most infectious Flu viruses, including the 1918 virus. Since this site does not appear in closely related coronaviruses, many speculate that this site is evidence of laboratory manipulation. More on this paper later.
From Andersen et al. The polybasic sequence is shown in green.
It is nearly obvious to many, including me, that an investigation into the origins of the virus is warranted, including data, documents, logs, and protocols from the WIV. The Chinese government has strenuously objected to any investigation. As of this moment, no serious on-site investigation has been performed.
Fauci Emails: A few days ago, Buzzfeed released the results for a Freedom of Information Act (FOIA) request for emails to and from Tony Fauci regarding the pandemic. Since then, journalists and others have been combing through the emails looking for interesting tidbits. And they have found some.
An exchange between Fauci and a group of other scientists and public officials occurred between January 31st and February 4th.
On January 31st, Kristian Andersen wrote to Tony Fauci. His comments include, “The unusual features of the virus make up a really small part of the genome (<0.1%) so one has to look really closely at all the sequences to see that some of the features (potentially) look engineered.” and “Eddie, Bob, Mike, and myself all find the genome inconsistent with expectations from evolutionary theory.”
On February 1st, a group including Andersen and Fauci had a conference call discussing the issue. The details of the call are not available.
On February 4th, members of the same groups discussed wording of a paper to be submitted. The paper is the same one I mentioned in number 4 above, and argues that the virus had a natural source. 4 of the 5 authors on the paper were on the February 1st conference call. The paper was submitted for publication on February 9th, just over a week after Andersen’s comments to Fauci on January 31st. Remember, the paper argues that the virus had a natural source, but the January 31st email suggests that several authors believed it was engineered.
I personally read this paper last year, and it convinced me, at least for a few months, that the virus was natural. It’s amazing and personally offensive to me that the authors duped me and many others.
I mentioned in a post a few weeks ago that while science is an extremely useful tool for learning about the natural world, it cannot answer the main questions of life. Philosophical tools are needed for that. In fact, science depends on philosophical ideas to work. Science depends on scientists being honest and transparent when they write! To publish material that is knowingly false is scientific fraud, and can be extremely damaging. In the scientific arena, authors who commit fraud are often publicly shamed, can be restricted from publication, and lose funding.
In a separate February 5th email to a friend, Dr. Fauci said “Masks are really for infected people to prevent them from spreading infection to people who are not infected rather than protecting uninfected people from acquiring infection. The typical mask you buy in the drug store is not really effective in keeping out virus, which is small enough to pass through material. It might, however, provide some slight benefit in keep out gross droplets if someone coughs or sneezes on you.”
Of course, Fauci’s statements on masks have been inconsistent. At times he’s said:
We don’t need masks We should have them but can’t because the medical community needs them We should be required to wear them We should wear 2 masks
As you know, my position is that good masks (N95s, KN95s, KF94s, and some homemade masks) are very useful in indoor settings, but are not necessary outdoors, except in crowds. I’ve also said that surgical masks, neck gators, and bandanas are nearly useless against an aerosolized virus. Fauci’s February 5th email is difficult to interpret, but I think it’s consistent with my position. When he says that masks don’t work, he’s talking about the very common masks that people wear, blue surgical masks and other loose fitting masks. Needless to say, the February 5th email will surely add to the confusion regarding Dr. Fauci’s position on masks.
_________________________ Update, June 16: In an interview on MSNBC posted on June 9th, 2021, Fauci was discussing the recent criticism of him. In the interview, he stated that “…attacks on me quite frankly are attacks on science.” and “You’re really attacking not only Dr. Anthony Fauci, you are attacking science.”
It is inappropriate for a leader to equate him or herself with a country, business, church, or practice like science*. When they do this, they are trying to protect themselves by borrowing the loyalty and good will people have for those things and applying it to themselves. The loyalty and good will people have for science is not owed to Tony Fauci or any individual scientist. A scientist only gets to claim “science” when they are practicing science. What is at issue is whether Fauci has actually been practicing science in regards to the issue of the connection between SARS-2 and the WIV. He doesn’t get to just claim this. He needs to provide evidence to support his view. As stated in my post on science, a scientist must provide evidence for their view, not just call you anti-science.
*Napoleon, in a speech to the French Senate in 1814, said “I am the State.” _____________________________
Collins on Gain of Function research. Hugh Hewitt recently interviewed Francis Collins, the current director of the NIH. I have been a big fan of Collins. However, in the interview, Collins seems to argue that collaborating on gain of function projects with researchers in China is a good idea. Frankly, with the increased belligerence of the Chinese government for many of its neighbors in recent years, I find Collins comments disturbing.
Podcast episode “We are Indebted to those Who Volunteered for the Vaccine Trials”. Search “Hewitt Collins” in podcast software.
Outdoor protests and COVID: Since I’m already in deep trouble today, I might as well pile on. A paper published in November of 2020 compared the number of Black Lives Matter protests to increases in COVID cases in the cities involved. The paper argues that there was a statistically significant but still small number of COVID cases arising from the Black Lives Matter protests. This gives more evidence that outdoor spread of COVID is minimal, even in large groups. Of course this also suggests that anti-lockdown protests were also unlikely to generate large numbers of new cases.
This is a case update. I’ll also talk about a new paper discussing indoor transmission as well as new CDC guidance.
This US is recovering from the 4th wave. Yes, the wave was much smaller than others, and if you don’t want to call it a wave, I won’t argue with you. Michigan bore the brunt of new cases, but cases are going down. Only Washington, Oregon, and Colorado are still experiencing higher case loads.
California and San Diego County continue to have fewer confirmed new cases. In fact, California had just 661 new cases on Sunday. The state hasn’t had fewer than 1000 new cases since almost exactly a year ago on April 28th. Yes, Sunday always has the fewest cases of the week, but it does indicate that cases are trending lower.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.
Internationally, a large peak is starting to improve. India has been particularly hard hit by the current wave of cases. The higher cases are likely impacted by the more infectious new variants as well as slower vaccination rates.
Indoor transmission: Several news outlets have been talking about a new paper on indoor transmission of SARS-2 published by a lab at MIT. It makes several interesting points. First, the paper points out that the Six Foot Rule was designed to mediate infection from large droplets like we see for the flu. Large droplets usually only travel from a person to the ground in 6 feet or less. SARS-2 on the other hand, appears to be transmitted as small droplets in an aerosol. The micro-drops stay in the air much longer and can travel much further. Transmission in indoor settings are a function of the number of people in a space, and the time of exposure. Ventilation helps reduce transmission.
The authors also point out that the likelihood of transmission outdoors is very low. One paper they reference has data from 7,324 transmission events, only 1 happening outdoors. They also say that masks have much more effectiveness in preventing transmission than lockdowns or social distancing, adding more evidence that the virus spreads as an aerosol.
Are you surprised by the papers conclusions? If you’ve been reading my posts, then probably not. I’ve been writing similar things since May 27th of last year. So why are people talking about this now? I certainly have my opinions, and I’ll bet some of you can guess. Meanwhile, several news outlets are saying that the CDC is about to release new guidance that vaccinated individuals can now go outdoors without masks. At the risk of running counter the CDC, I’ll just mention that I’ve been going outdoors without a mask since March of last year, at my most concerned. I almost always wear a mask indoors, but almost never wear a mask outdoors.
I’ve been traveling a LOT recently and just skipped last week’s update. Sorry for the long delay.
The US continues a slow trend upward in new confirmed cases. According to endcoronavirus, most of these new cases are arising in the Northern states, although the upward trend seems to be creeping south. This seems to confirm my suspicion that the new uptick in cases is caused by colder weather, and people being indoors together more often. If this suspicion is correct, we may be in for a long broad 3rd wave of cases this winter. You may remember that the Southern states (California all the way to Florida) drove new cases this summer. During the summer of course, people in Southern states tend be indoors with their air conditioners more often. This is my theory for the time being.
After the end of the 2nd wave, California is experiencing a persistent 3000 new confirmed cases a day, and San Diego County has a persistent 300 new confirmed cases a day. Unfortunately, I’m firmly convinced at this point that COVID may be with us at least until next Spring. As you know if you’ve been reading my posts, I think we will need to adapt to this situation, and open up our economy and normal life as much as possible, while still taking precautions.
As I’ve mentioned before, I am doing a lot of traveling these days, and get tested almost every week, and I’m always negative so far. I use air travel and go into all kinds of gas stations and stores. I do the following:
1) Wear a mask or face covering in public. Avoid places with unmasked people. 2) Keep 6 ft away from others. (I basically ignore this one if other precautions are in place, especially on an airplane!) 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. 4) Small outdoor gatherings are fine, even without masks, if everyone maintains a distance. Have guests bring their own food. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however. 6) Wear an N95 or KN95 mask when going to more high risk areas like airports or public areas where people may gather. These masks are rated to filter out 95% of viral particles. In my opinion, surgical masks and especially neck gators are nearly worthless in these settings. 7) I never take my mask off on the plane, and find an isolate spot in the airport to eat or drink on layovers.
Voting: If you haven’t heard, there is an election coming up. As with many issues, mail-in voting has become a politicized issue. The New York Times recently had a story expressing reservations about mail in voting, claiming that mail in ballots are more likely to be disqualified than in person voting. This is because filling out and mailing in these ballots can be complicated and prone to errors that disqualify these ballots. Some stories even claim that people have been sanitizing their ballots, ruining the ink and disqualifying be ballot. It is therefore my recommendation that everyone vote in person if possible. Follow the above precautions, and I’m confident you can do so safely. Dr. Fauci claims that in-person voting is safe if proper precautions are taken.
Reinfection: There is a recently published study of a confirmed case of re-infection in an American man. Apparently, this is the first confirmed and well characterized case in the US, although there have been other suspected cases. His symptoms were more severe with the second case, suggesting that my fears of ADE may be warranted. However, there have been only 22 confirmed cases of reinfection world wide, so it’s still apparently a very rare phenomena. The paper also states the 2nd infecting strain is distinct from the first, consistent with the ADE model.
The paper suggests that there may have been dozens of circulating strains since the beginning of the pandemic. While this case of re-infection appears consistent with ADE, the rarity of the re-infection phenomena along with the many circulating strains suggests that ADE, while theoretically possible, may not have large real-world significance.
New 3D structure: Last, for those of you who want a deep dive, the New York Times has a nice story with a collection of 3D structures of the virus from different sources.