Dr. Peter McCullough is a cardiologist who became well known during COVID for his ongoing skepticism of the vaccine, and also for advancing COVID treatments. He is a hero to many and a villain to many others. He and colleagues Dr. Brian Procter and Cade Wynn have just published a paper on the detoxification of COVID Spike protein from the body (Journal of American Physicians and Surgeons).
I have a PhD in molecular biology, specializing in infectious disease testing. I am not a physician! I have a very informed but not expert opinion on medical matters. Consider discussing with your doctor before following any medical advice.
As we’ve discussed before, the Spike protein of SARS-2 is the component of the virus that leads to the most damaging impacts of infection. It causes inflammation across the body in many different tissue types and also contributes to rampant blood clotting. Unfortunately, because the vaccines also cause your body to produce Spike protein in order to cause your immune system to make antibodies, the vaccines also cause some of the most pathogenic effects of the virus. Because it gets packaged by various body mechanisms, Spike protein can persist for months or years after infection or vaccination. Boosters also increase the amount of Spike in your body.
I know many people now who suffer a wide variety of effects likely from a vaccination or a booster, ranging from persistent tinnitus (ear ringing), to a very healthy friend who had a heart attack a month after getting a booster, with no history of cardiac issues. As for myself, I have an autoimmune disease, celiac disease, that also comes with generalized inflammation. I have plantar fasciitis, trigger finger, chronic tailbone pain, and bursitis in my knee. All these things have gone from very mild to moderate in the years since I had COVID. To be clear, I have never been vaccinated against COVID, so my symptoms are from SARS-2 infection.
Dr. McCullough’s paper recommends a combination of three over the counter supplements that he claims can help clear your body of accumulated Spike protein from either infection or vaccine. If you already have immunity, the Spike protein in your body is no longer of any use to you. You don’t need it anymore, and you should probably get rid of it!
Nattokinase: This enzyme comes from soy beans and is a digestive enzyme which can help digest Spike protein. It should be taken at a dose of 2000 units twice a day.
Because Nattokinase is an enzyme, it should be taken between meals. Otherwise, instead of finding and chewing up Spike protein, it will just help you digest your lunch. Take Nattokinase at least an hour after a meal, or at least a half hour before one. You should not take Nattokinase if you have an allergy to soy.
Bromelain: This is a protein digesting enzymes purified from pineapple stems. Like Nattokinase, it can digest Spike protein, but it can also inhibit the interaction of Spike and the receptors that it uses to interact with human cells, helping to reduce inflammation. Recommended dosage is 500 milligrams once per day. Bromelain is also an enzyme. So like Nattokinase, it should be taken between meals.
Curcumin: This compound comes from the ginger plant and is similar to turmeric. Like bromelain, it also has the effect of inhibiting the interactions of Spike with our cells, and also reduced inflammation. Free curcumin isn’t absorbed by the body well, so it is recommended to take it in a form that is, “Nano” or “liposomal” curcumin. Instead, you can also take it with piperine (black pepper extract) which improves absorption. Recommended dose is 500 milligrams twice a day, in the Nano form.
Dr. McCullough suggests that this combination of supplements should be taken for at least 3 months.
An important word of caution! All three of these compounds have an anti-coagulant effect. So if you have trouble with a lack of blood clotting, you don’t stop bleeding after an injury, or are on any anti-coagulation medications, talk to your doctor first before taking any of these supplements. Also, you should not take Nattokinase if you have an allergy to soy.
This is a new protocol, and has not yet been formally tested! It has also not been used by large numbers of people. So if you’re cautious, you may want to wait and see how others do on this protocol before trying it yourself.
I can no longer recommend a booster for anyone, even if you have risk factors. But if you want to get a booster, don’t take these supplements for at least a month after your booster, or you will reduce your body’s ability to make antibodies.
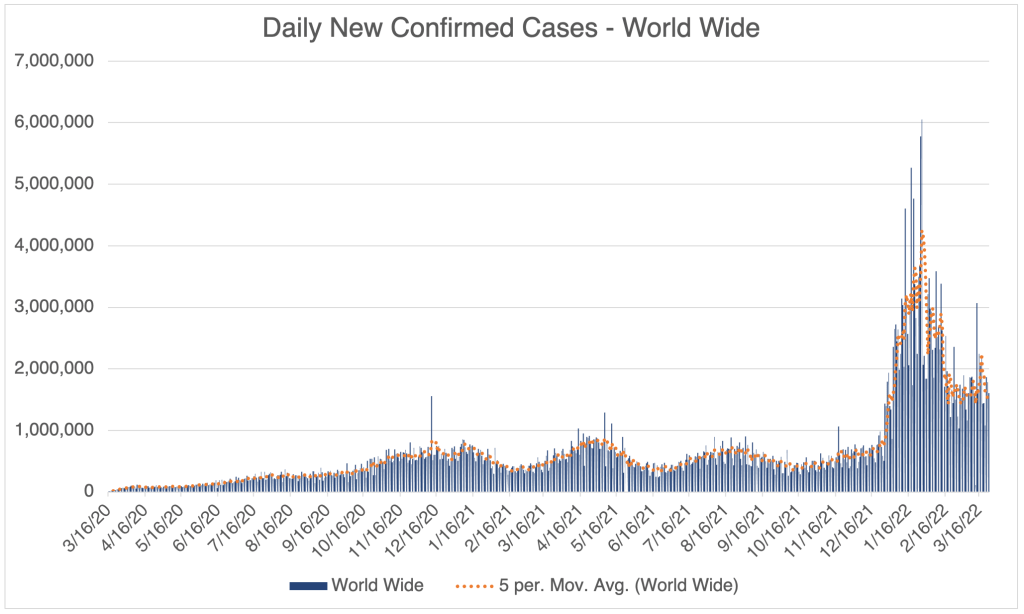
It’s been more than 2 months since my last post. Today, I’ll give a little update on new cases, plus a collection of brief but interesting stories. Michael Shellenberger claims to have interviewed 3 “patient zeros” from the Wuhan Institute of Virology. Then I’ll discuss a study from the Cleveland Clinic on booster effectiveness, a report from John Campbell on adverse events from vaccines, and a story about excess deaths pointing to vaccine injury, supported by another video from John Campbell.
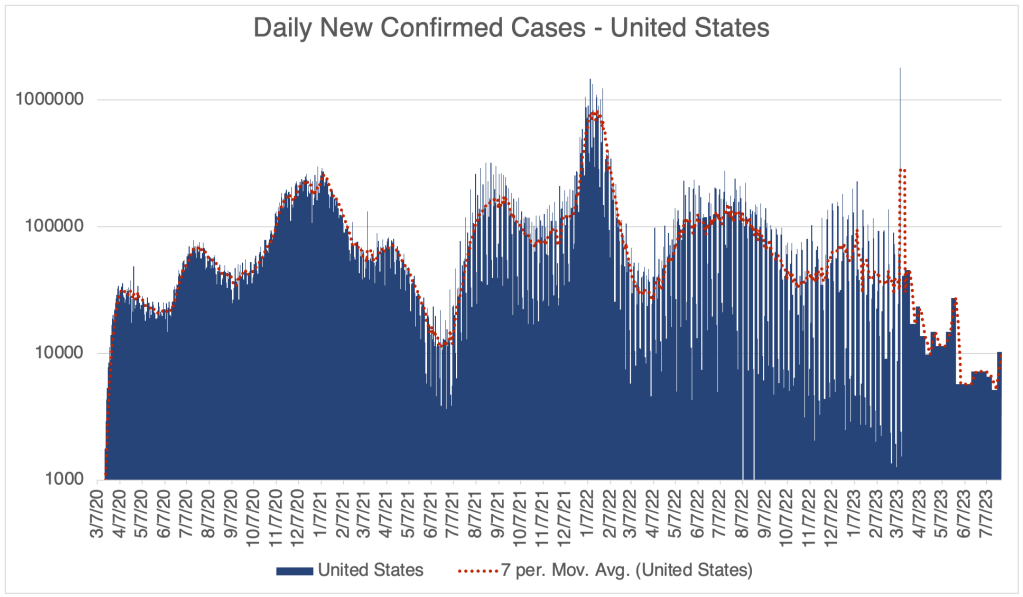
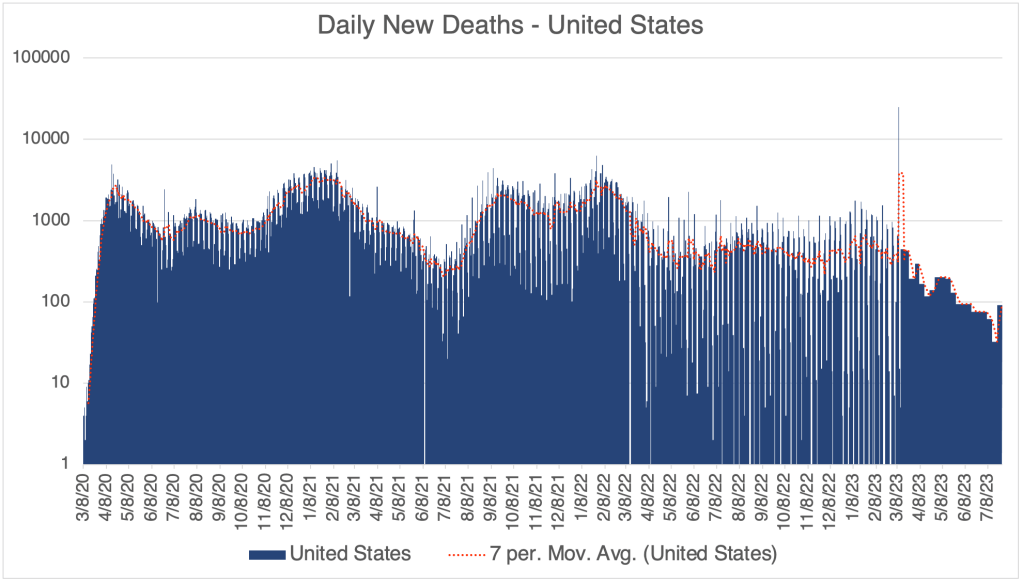
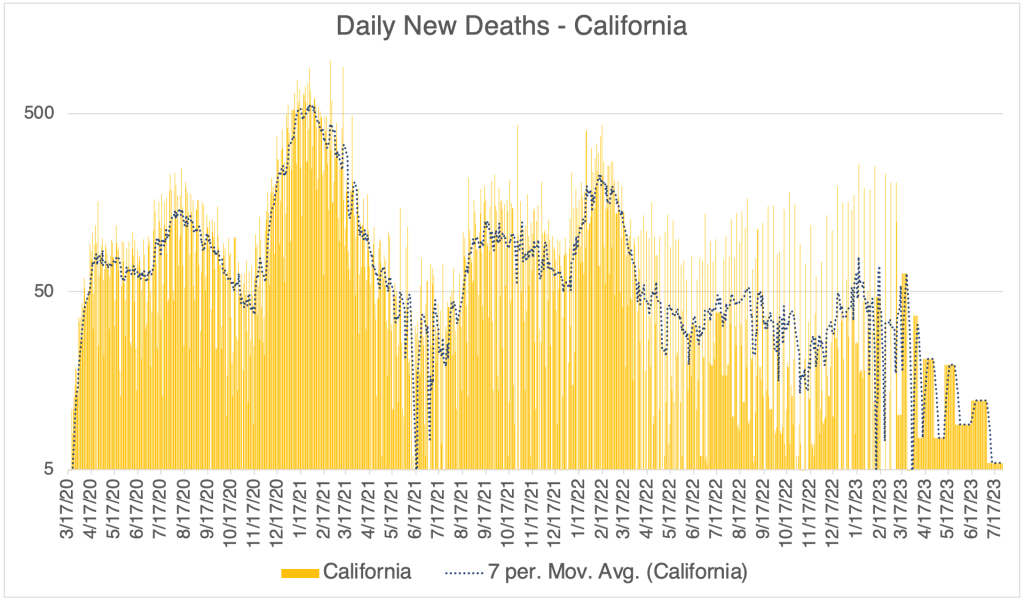
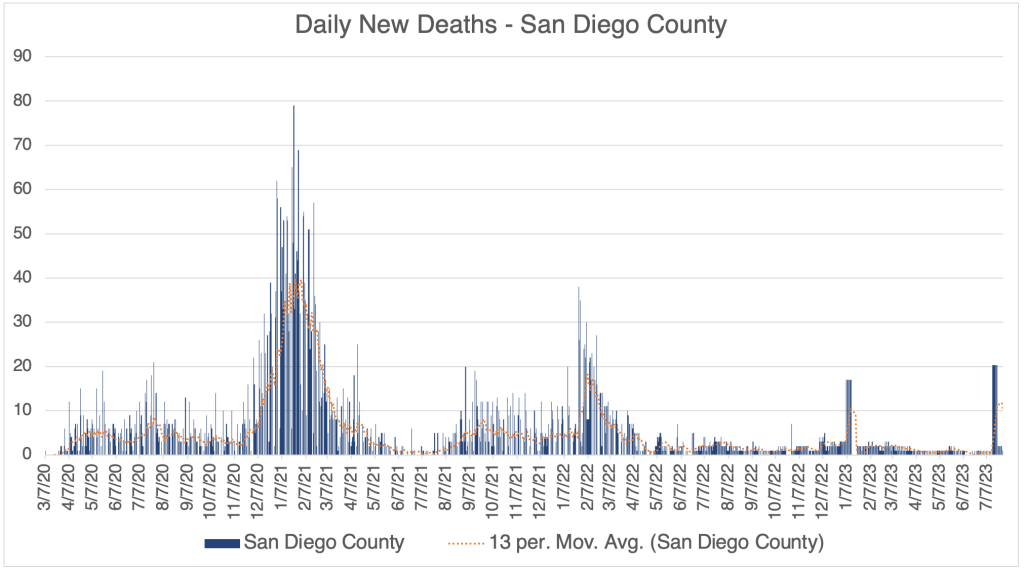
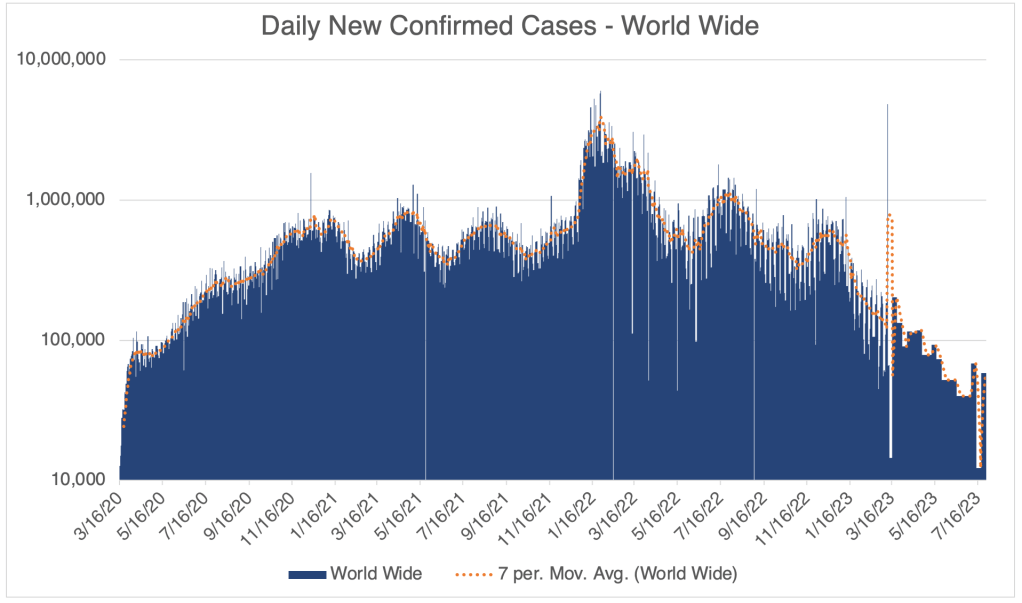
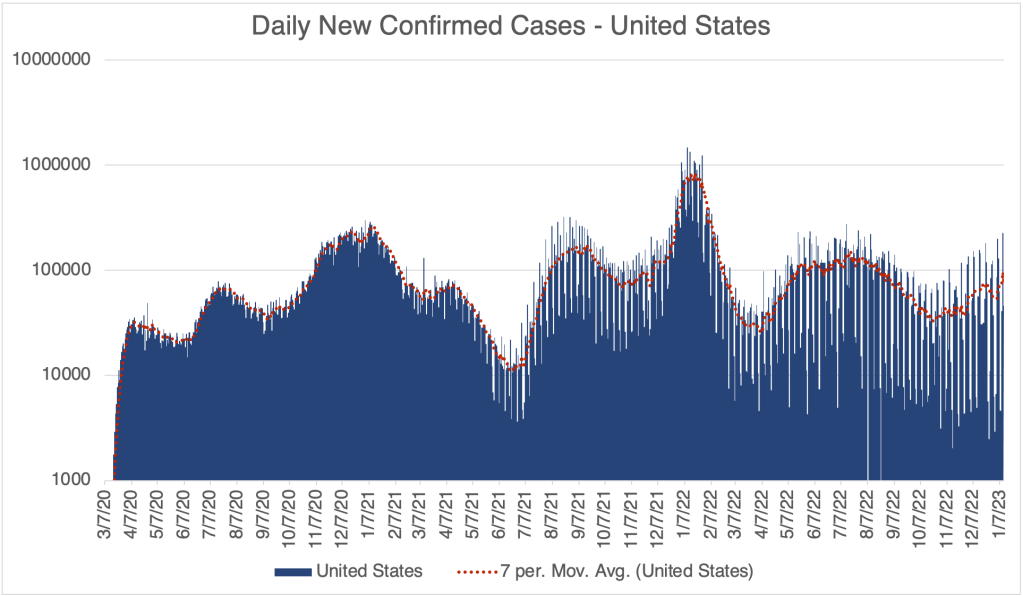
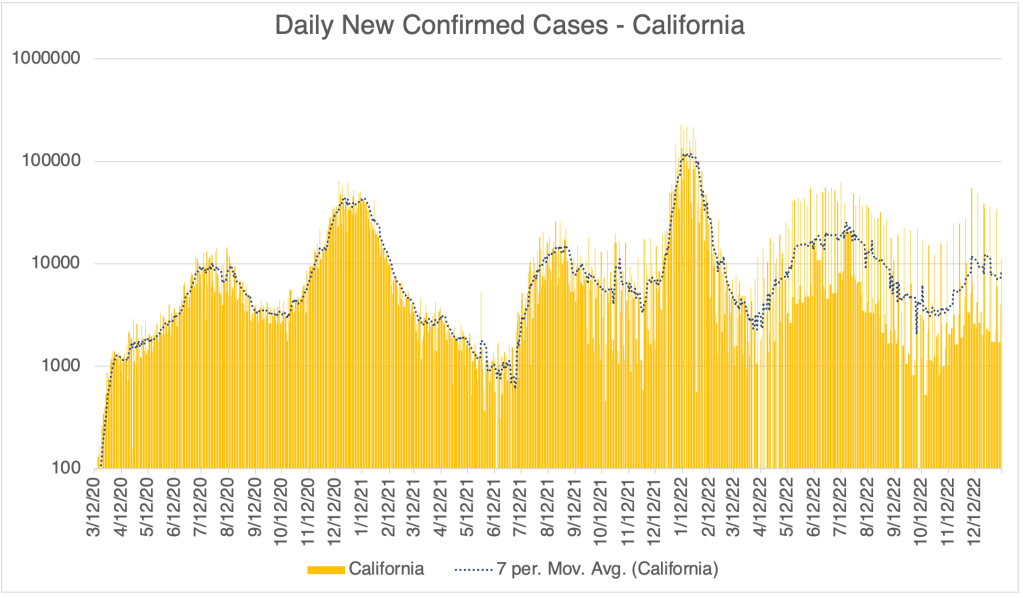
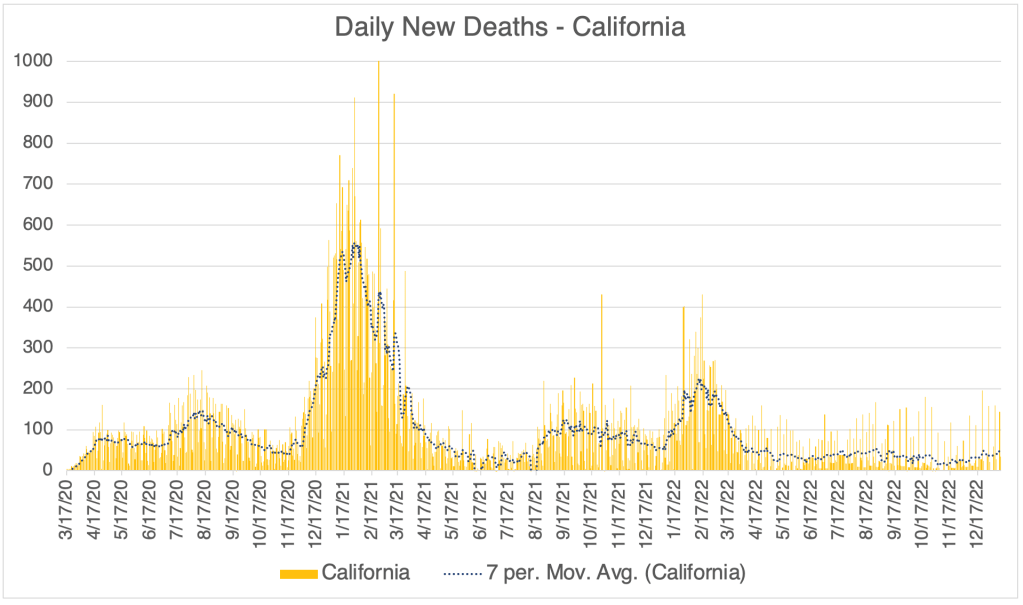
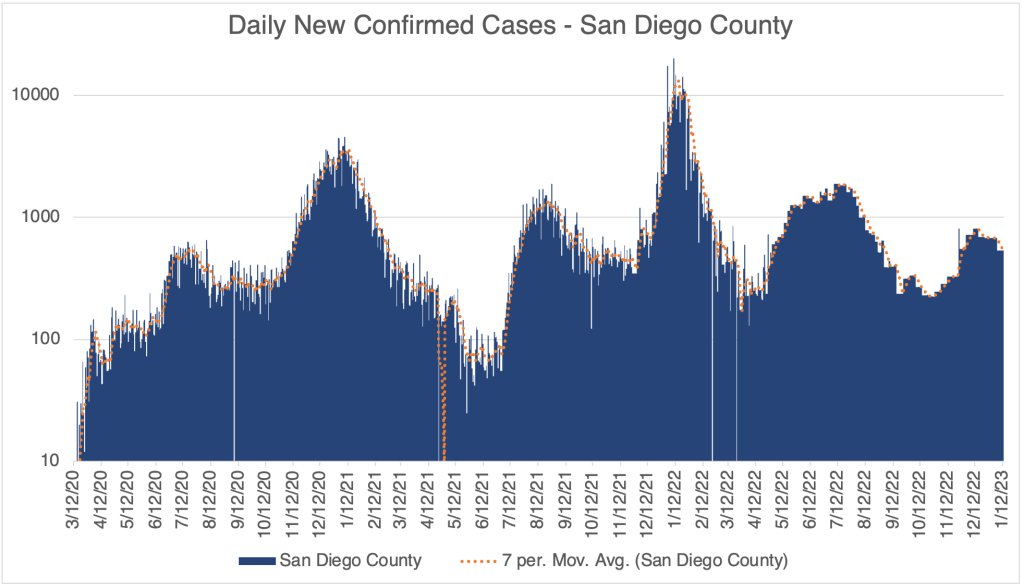
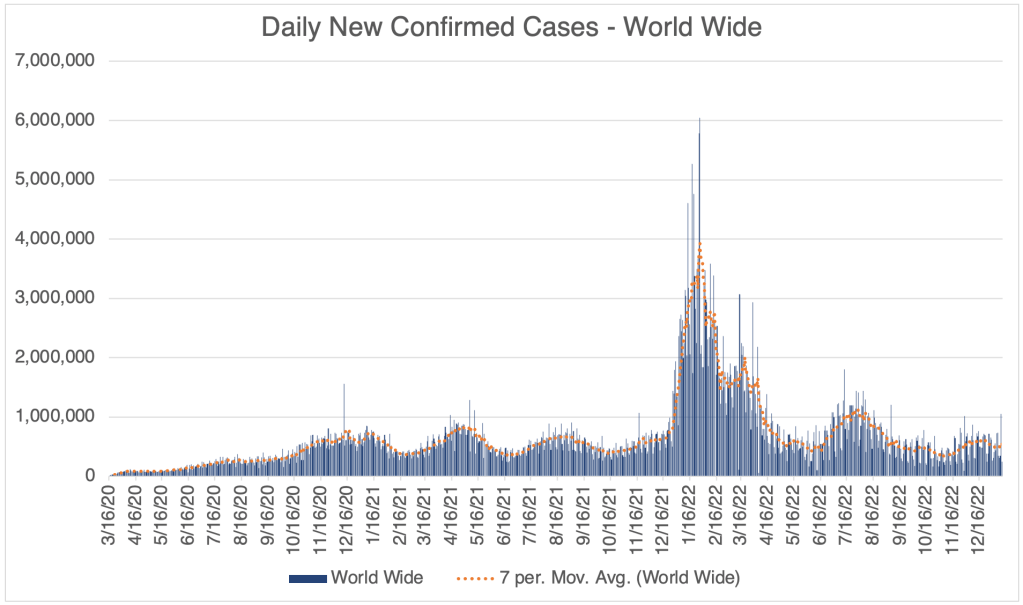
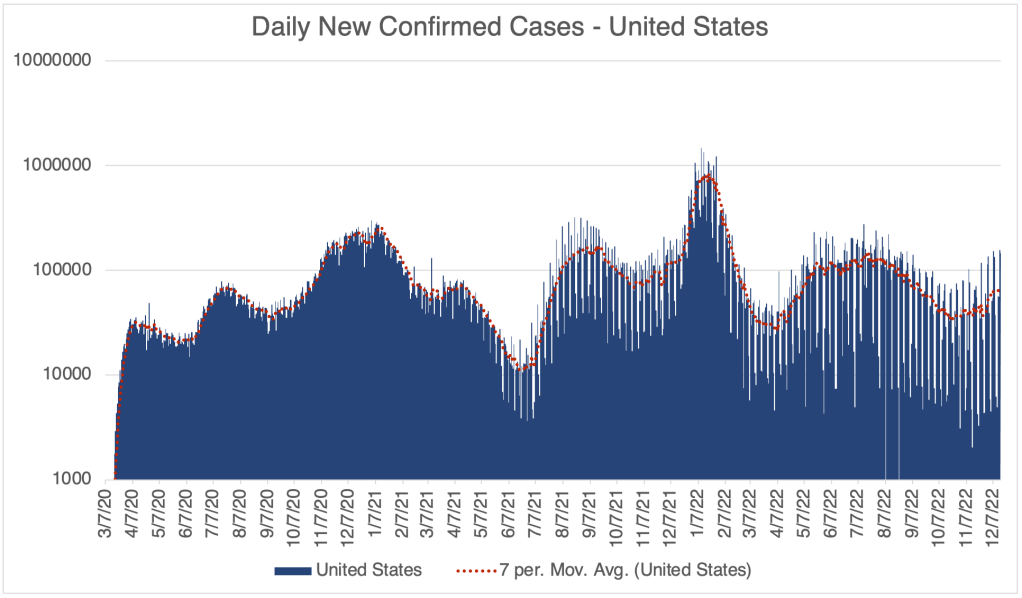
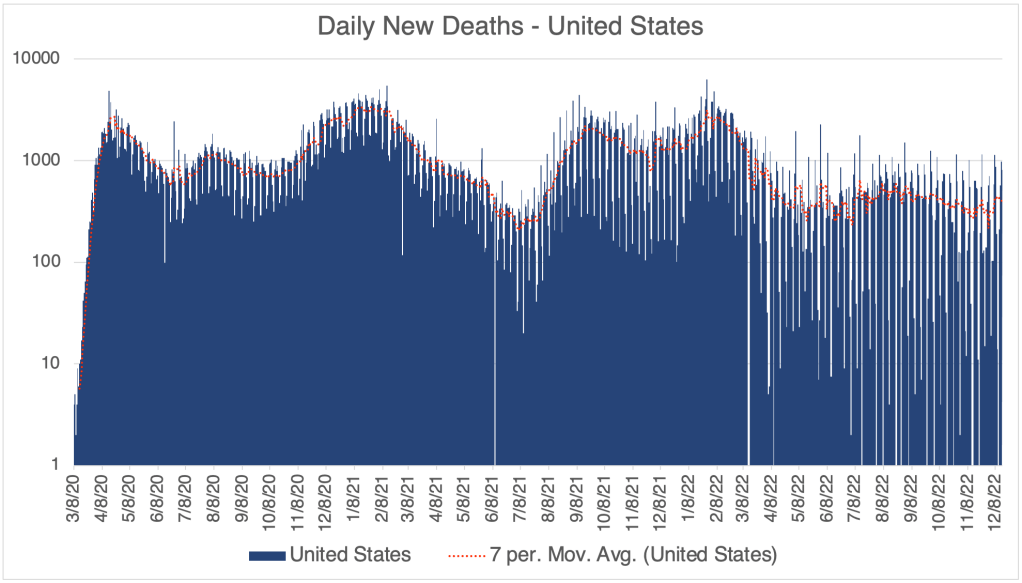
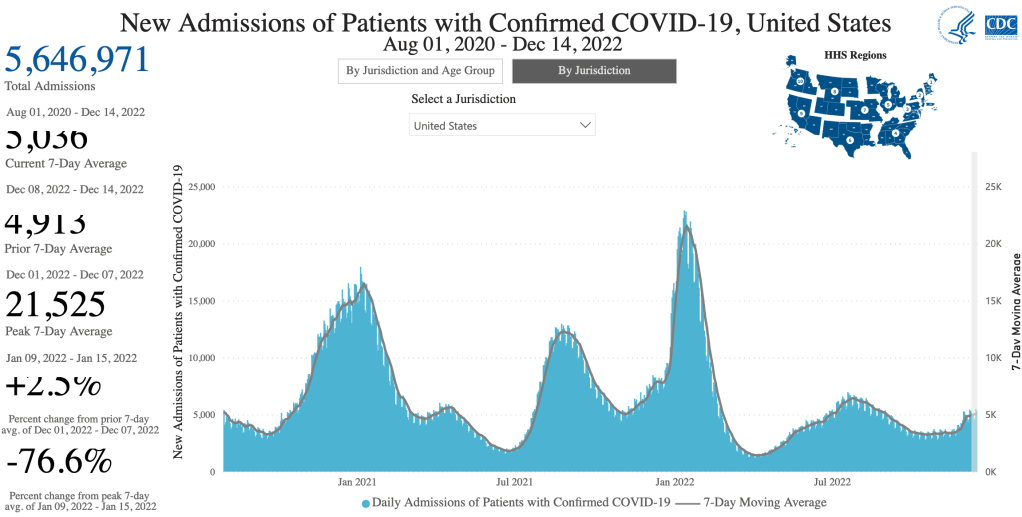
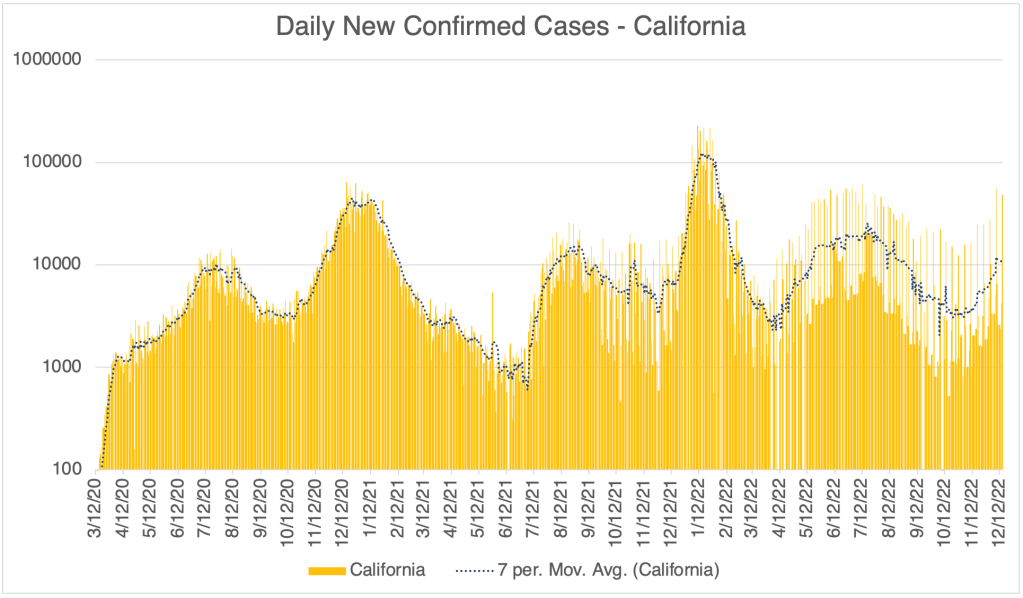
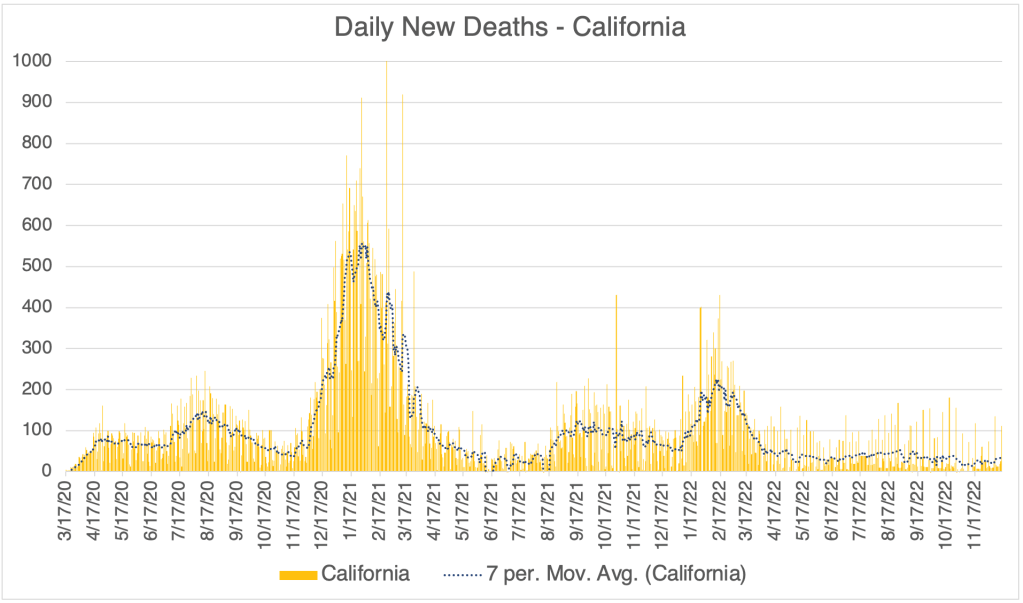
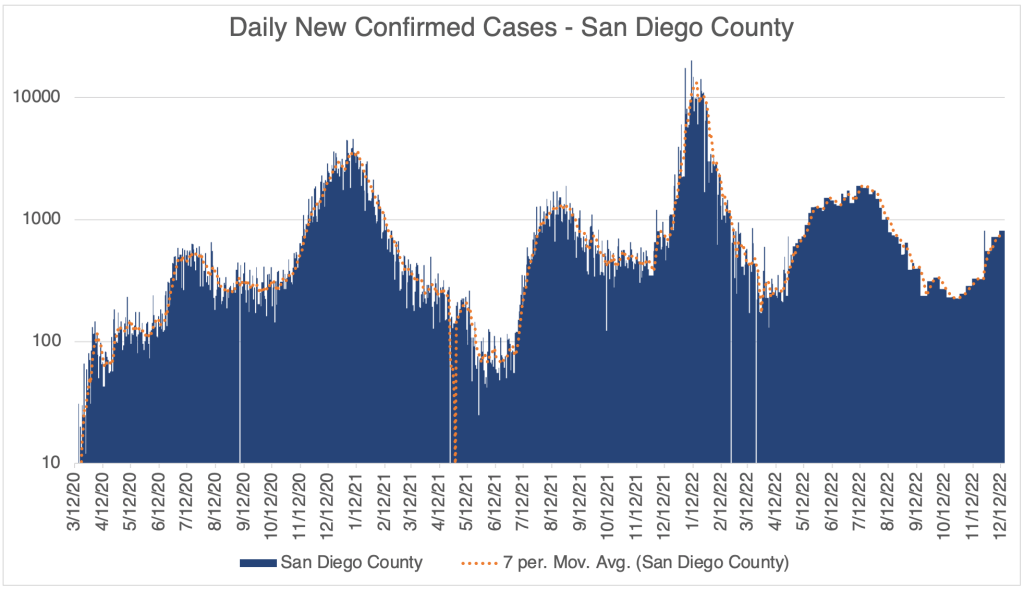
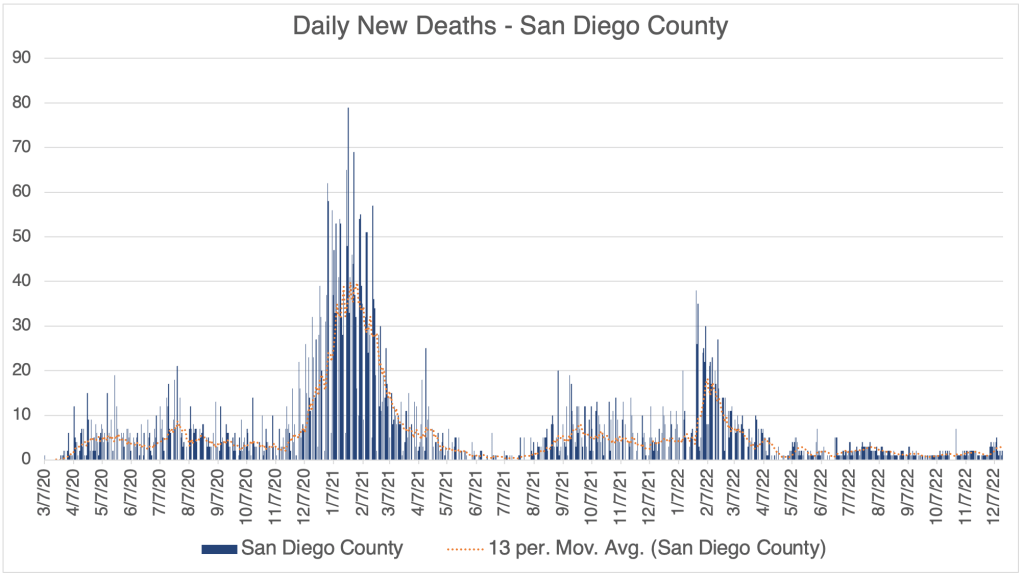
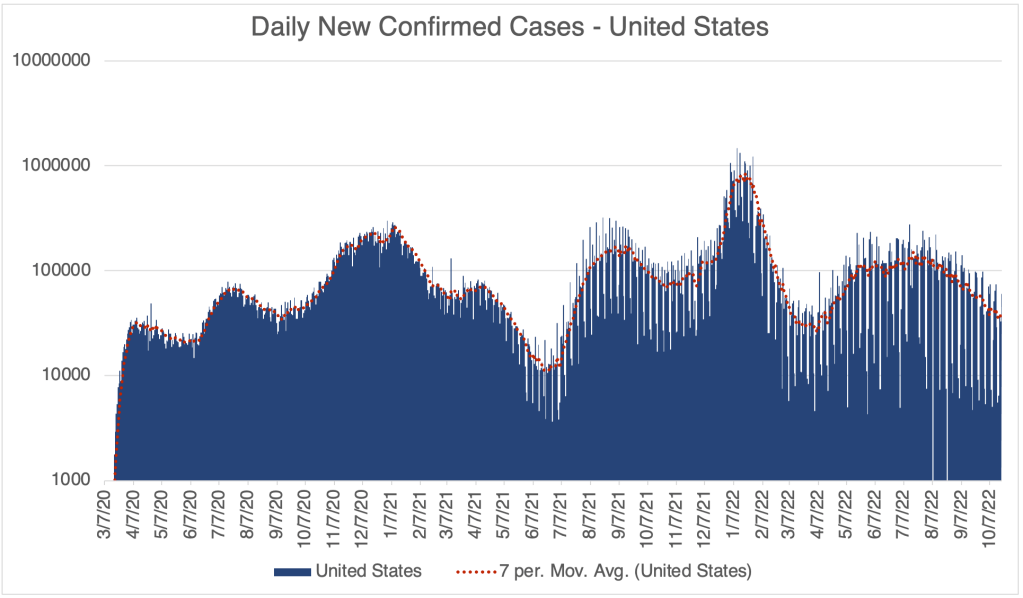
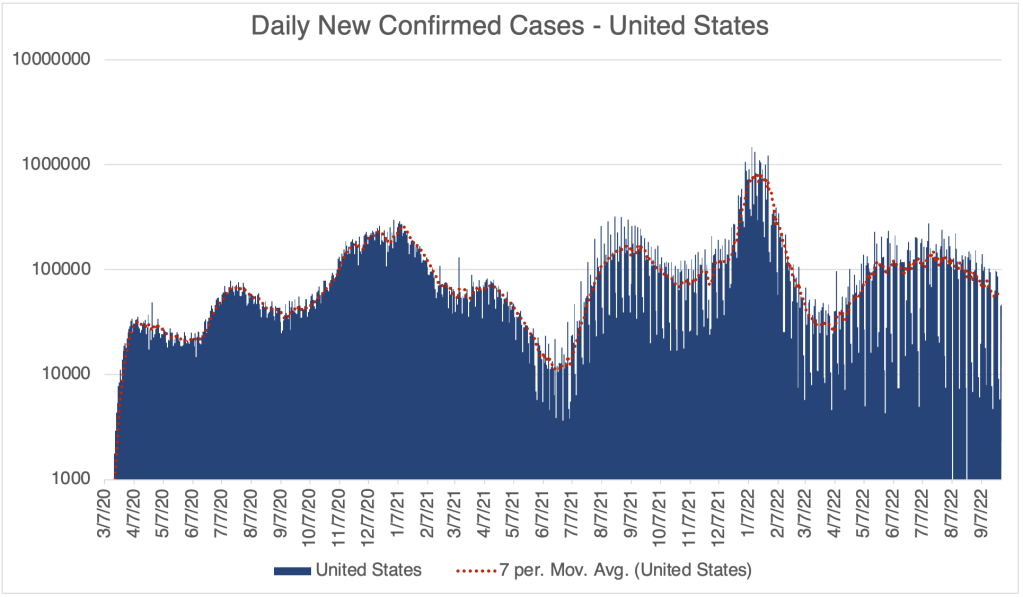
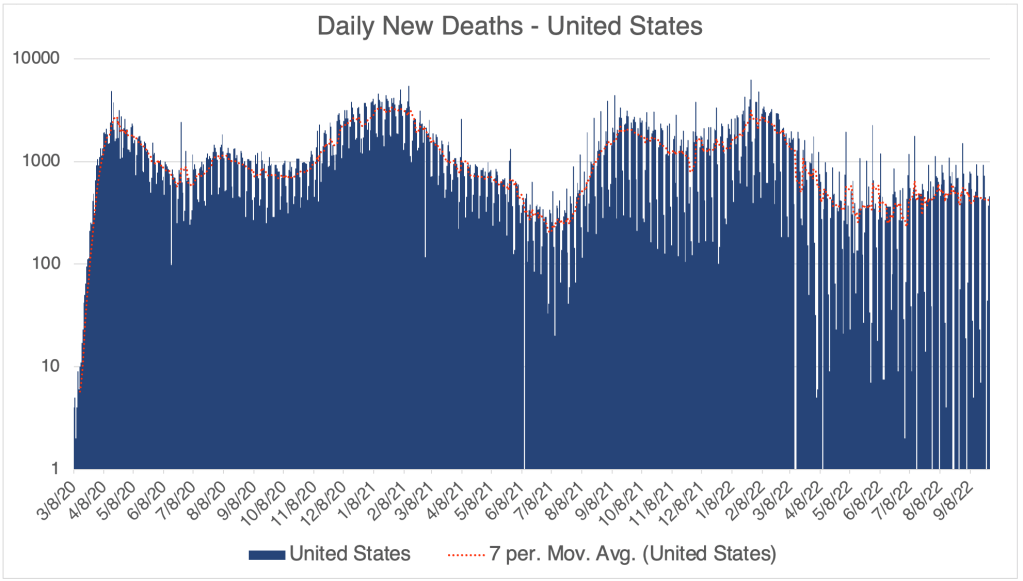
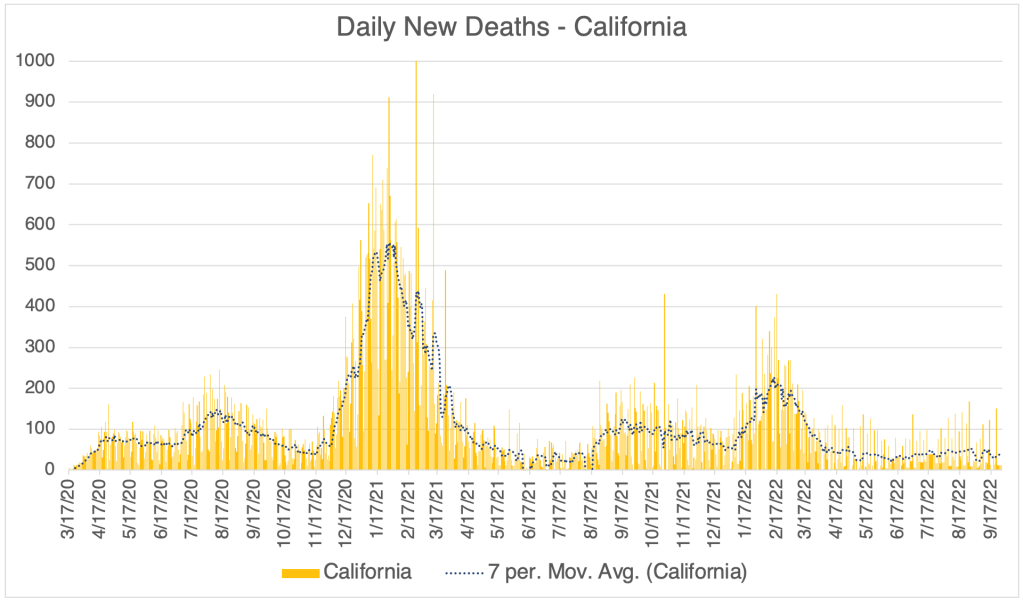
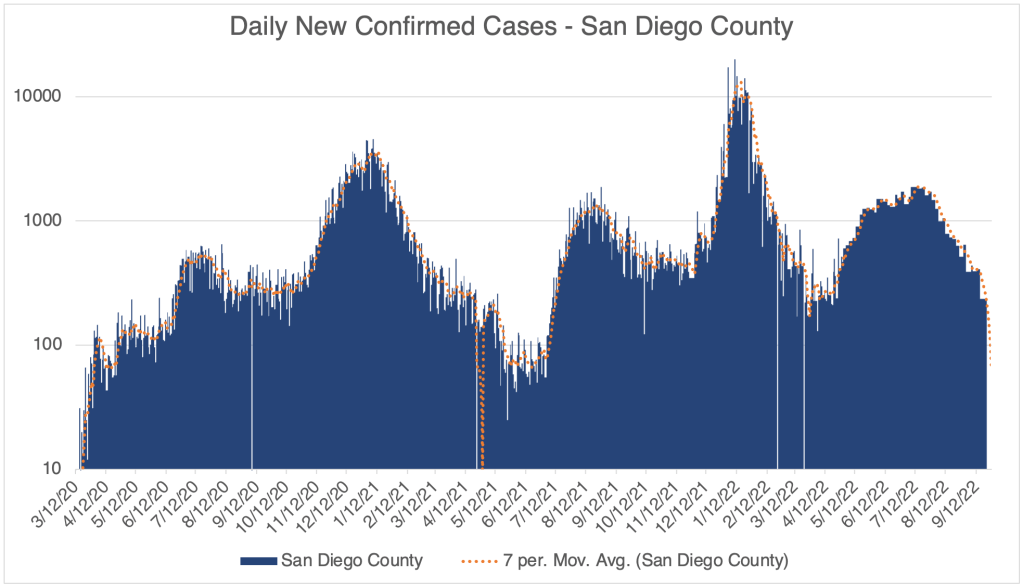
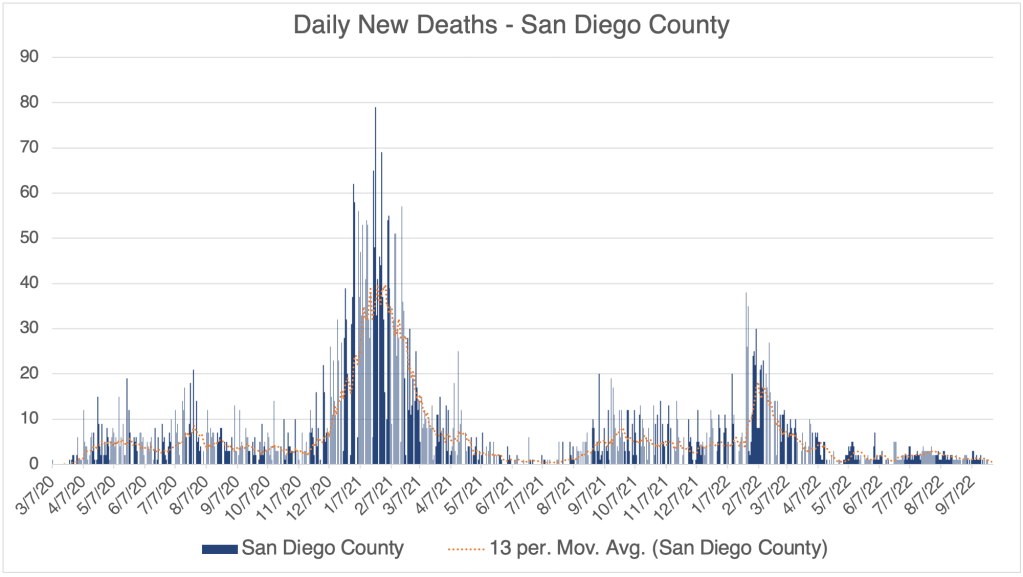
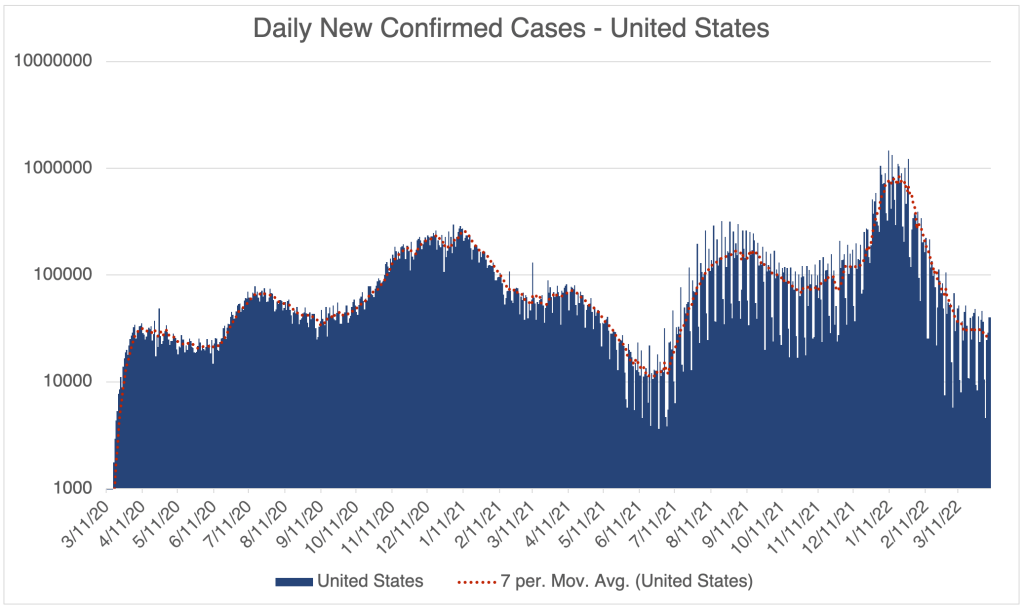
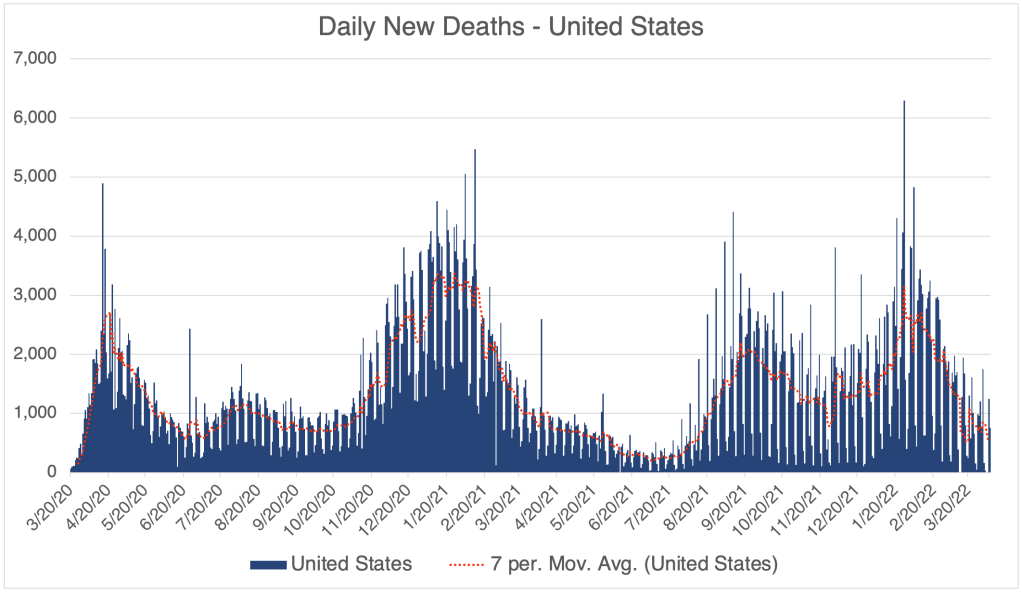
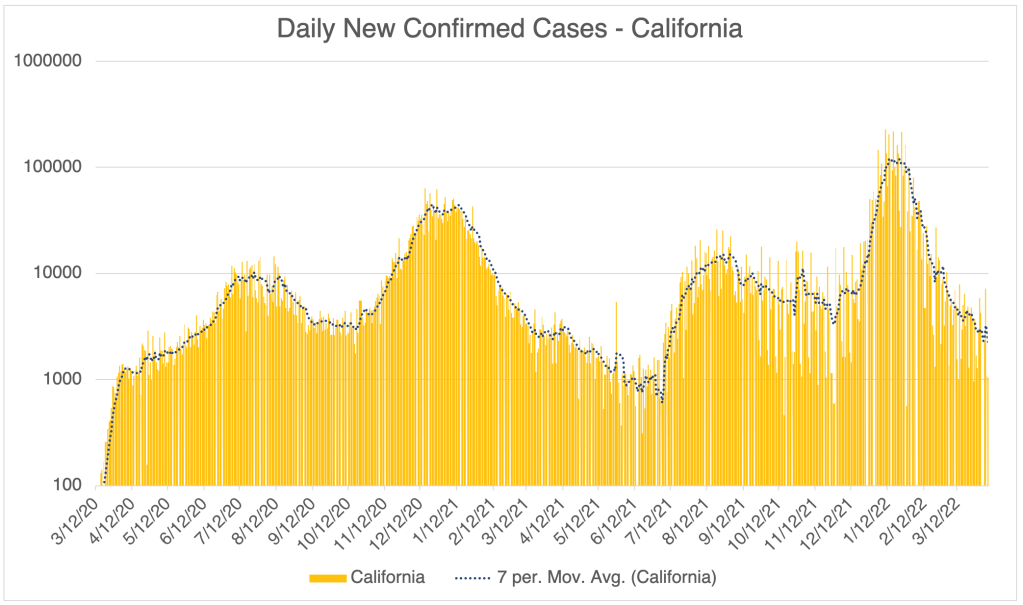
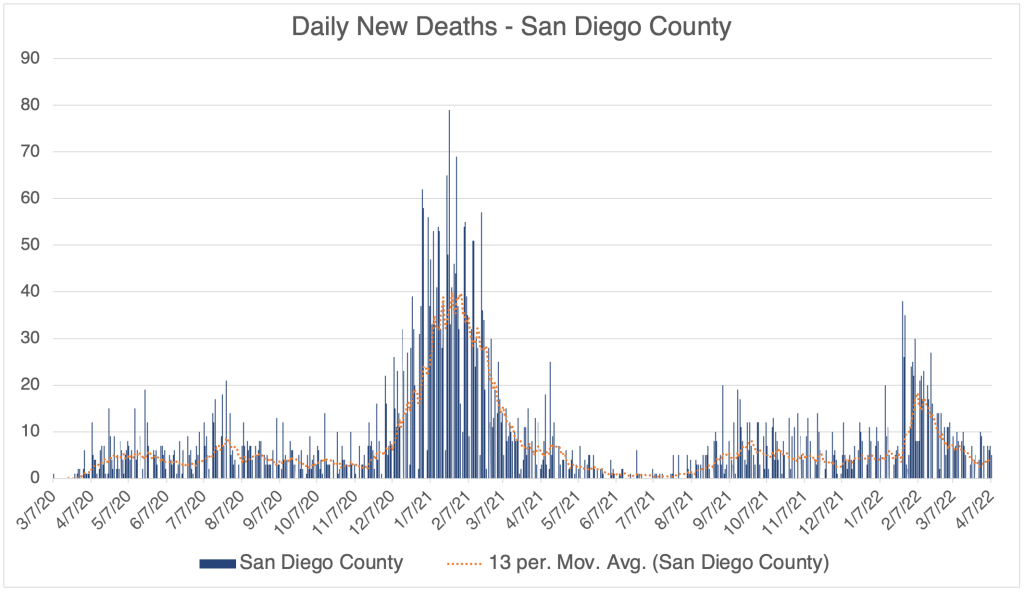
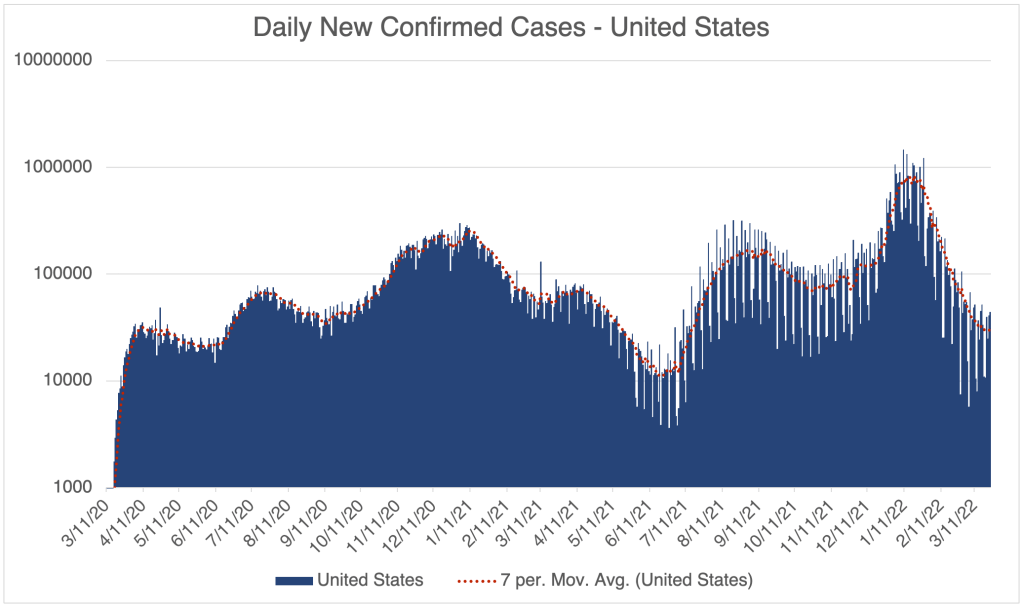
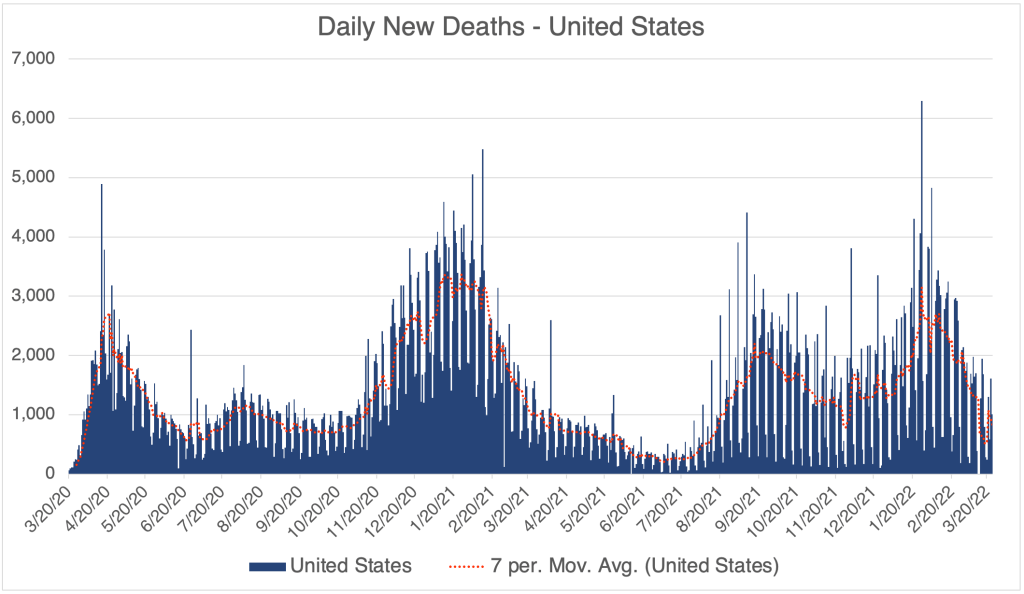
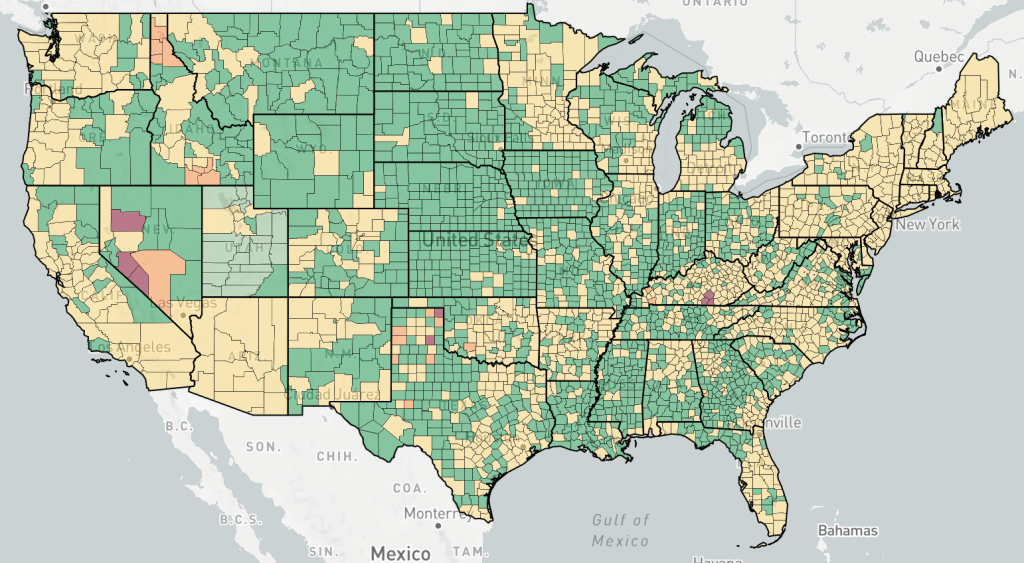
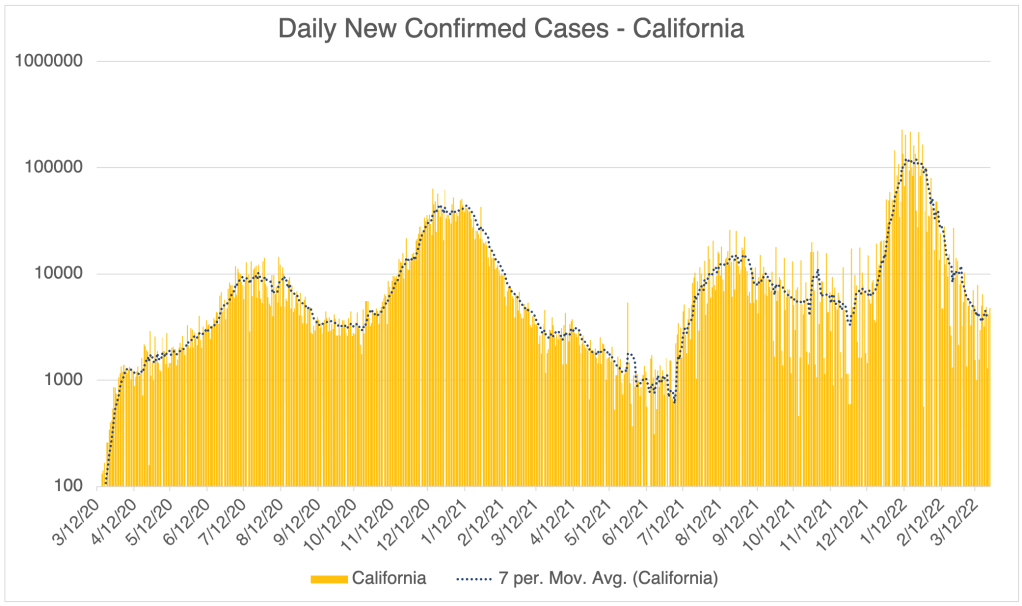
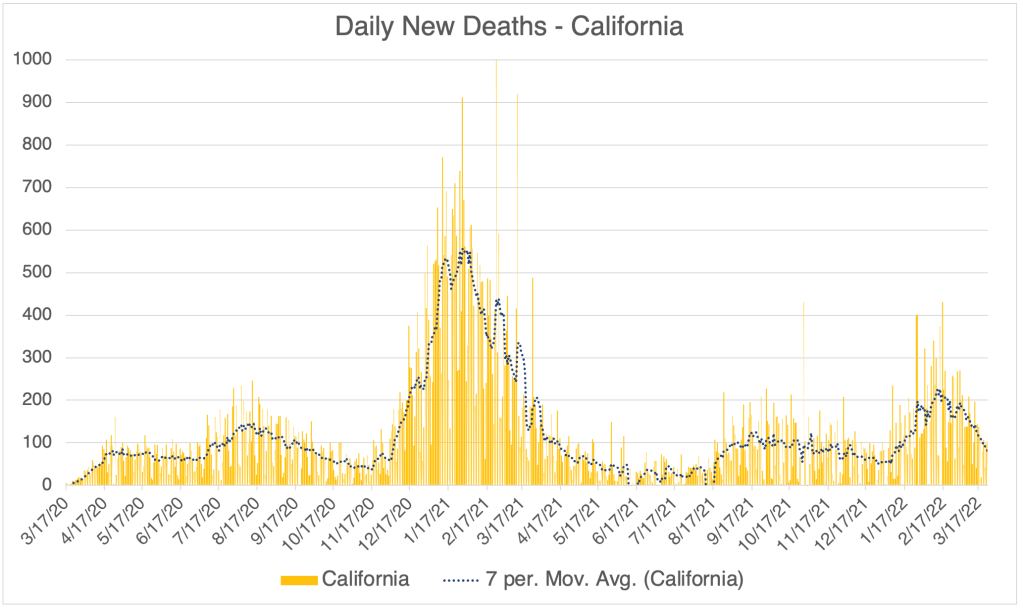
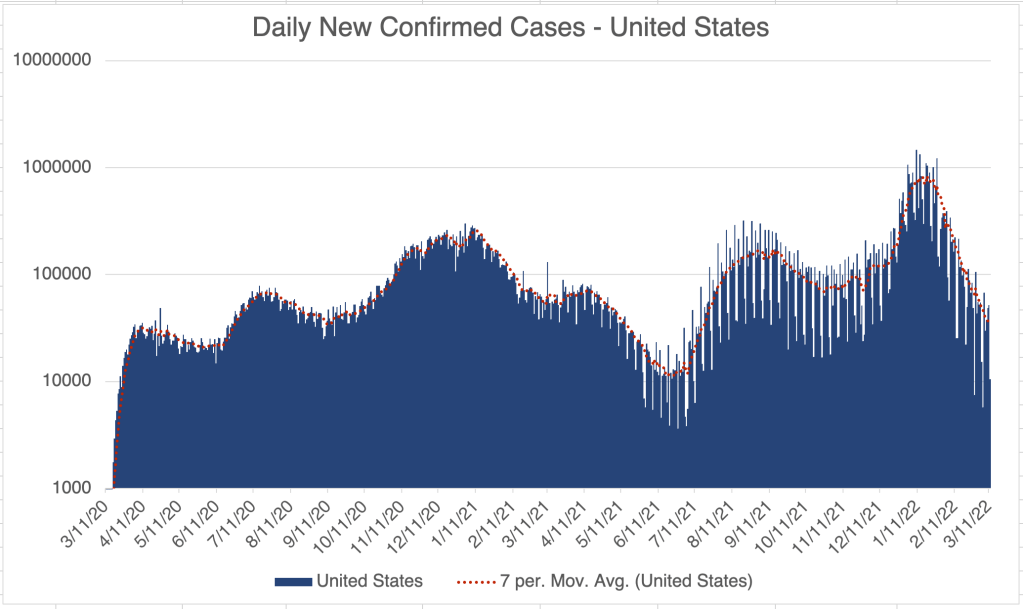
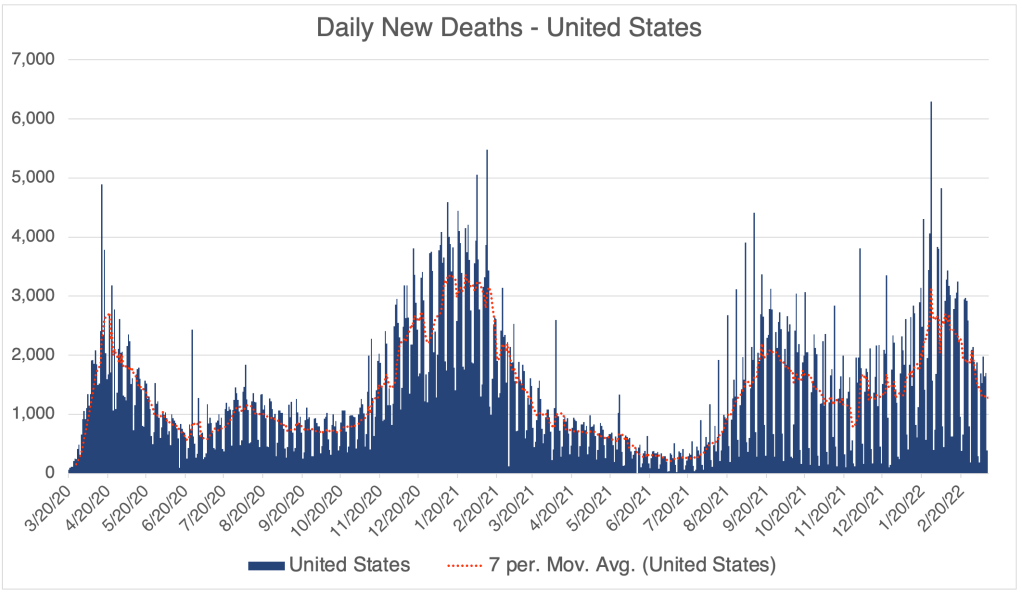
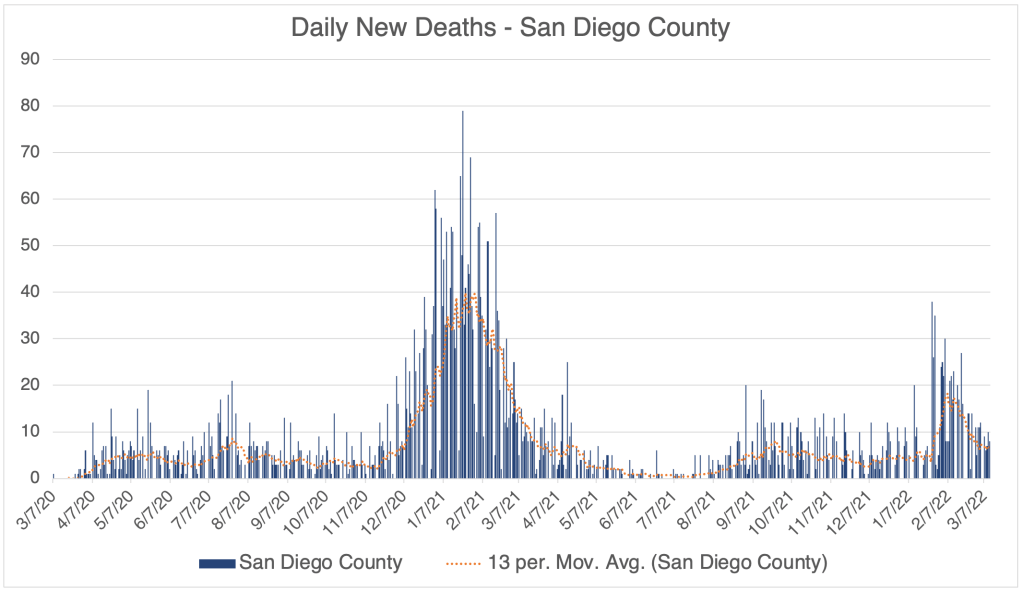
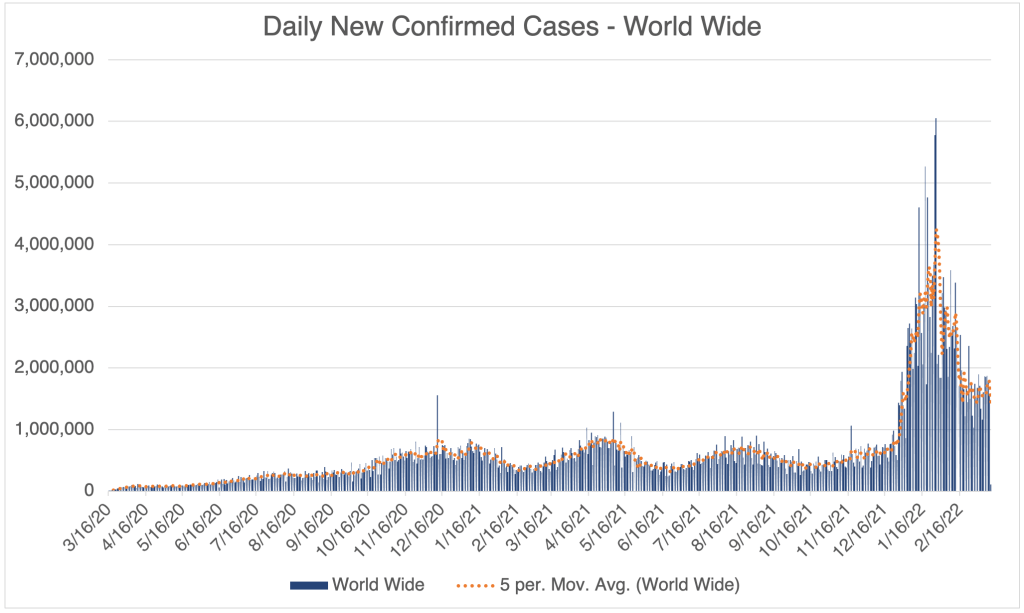
I am only collecting data once a week now, just to monitor new cases, so my graphs are pretty low-resolution. New COVID cases are as low now as they were at the very beginning of the pandemic, even lower than the Spring of 2021 before Delta arose and spoiled the party. New deaths due to infection are also very low. There was an apparent spike in new deaths in San Diego County in mid-July, but this may have represented a bunch of hospitals reporting at once, and not a spike in actual deaths.
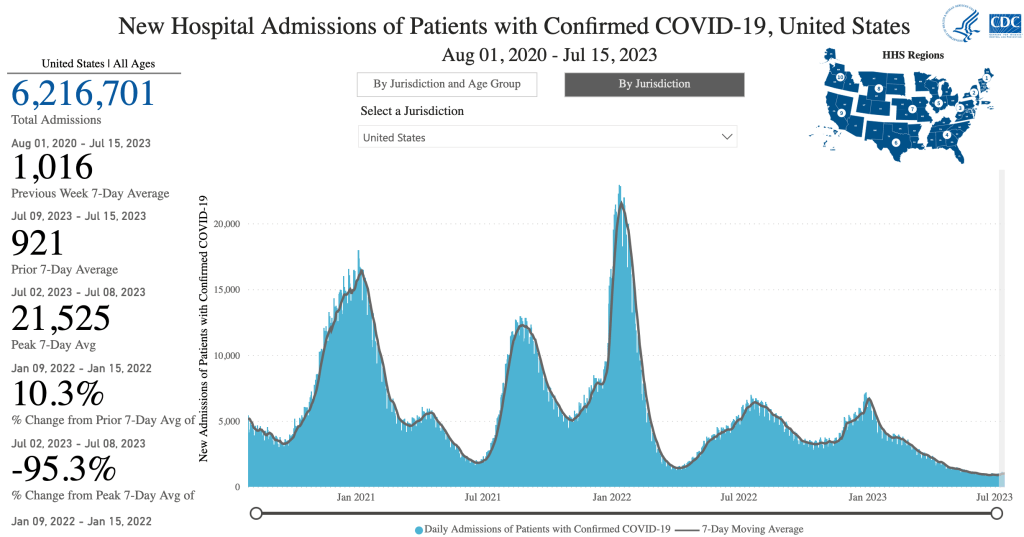
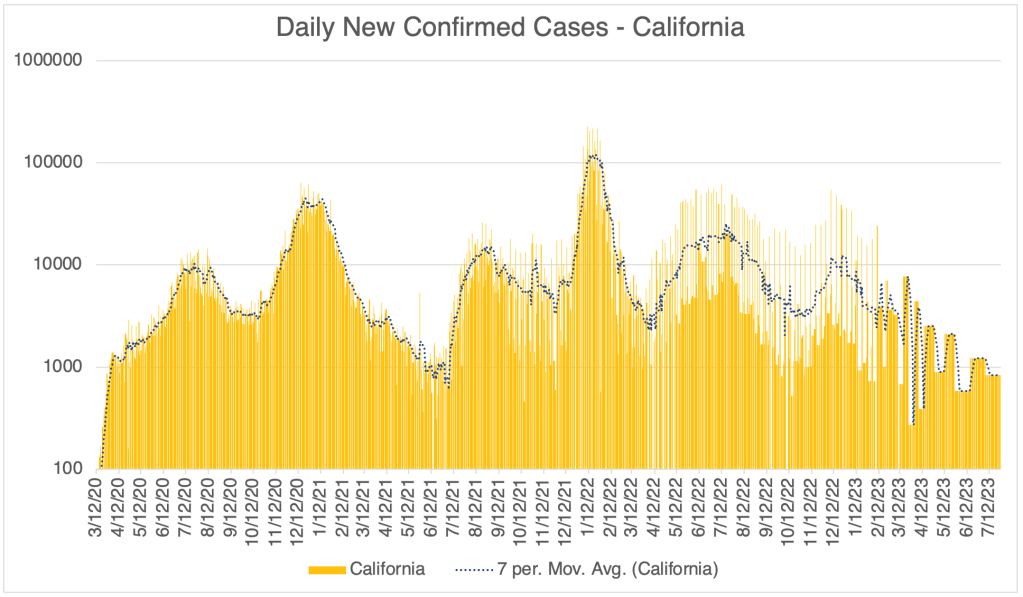
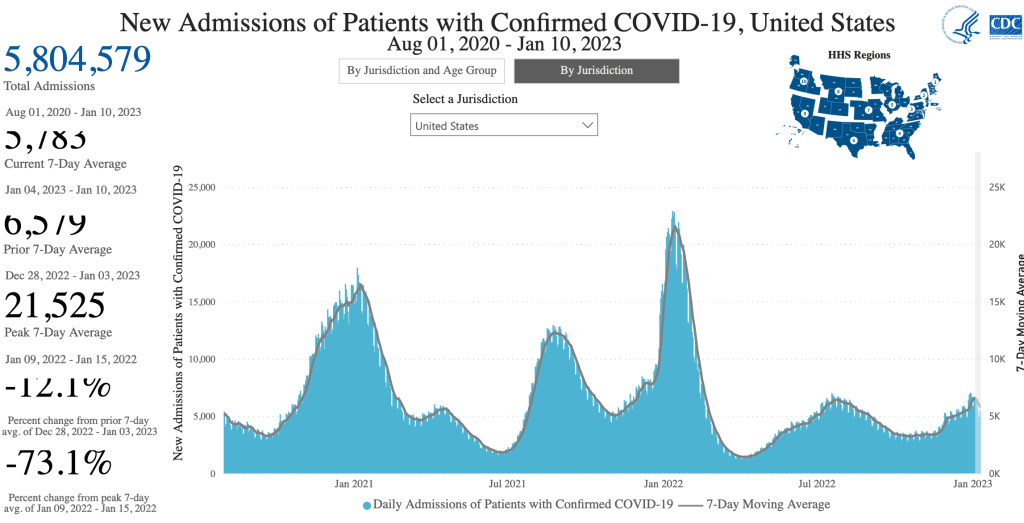
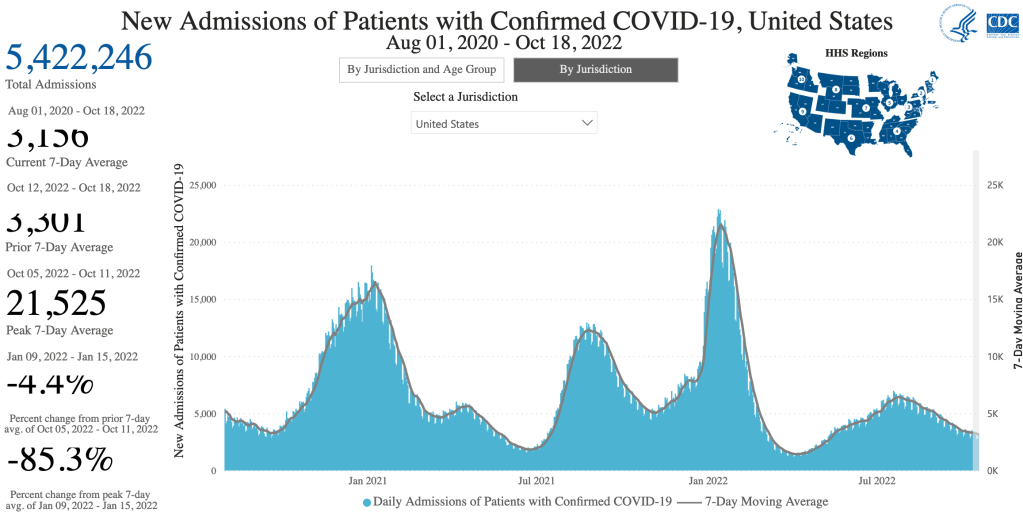
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Daily COVID Deaths, World Wide, Worldometer/coronavirus.
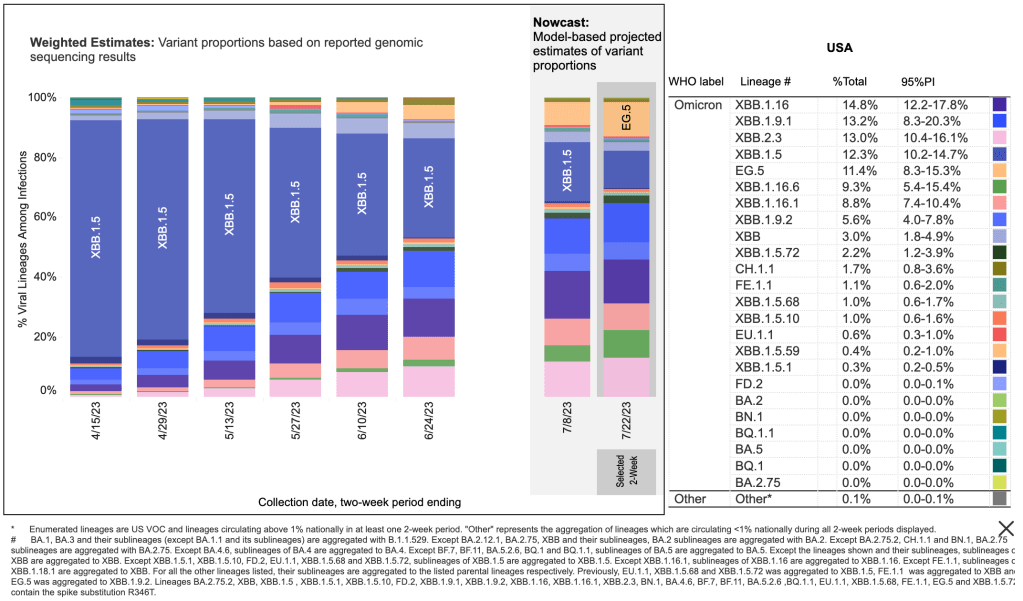
A new Omicron variant, EG.5 is rising in prominence, but this new variant is apparently no deadlier than other Omicron variants, so is not of great concern.
3 “Patient Zero”s identified:Journalist Michael Shellenberger claims that the identities of 3 “patient zero” individuals are now known, and all of them worked at the Wuhan Institute of Virology. These people were likely the very first people in the world to be infected with SARS-CoV-2. One of these individuals is Ben Hu, the 2nd in command at the WIV, and someone who was directly involved in Coronavirus research. Shellenberger was not shocked to discover that the initial patients were from the WIV. Rather, he was shocked and dismayed that he had to discover this for himself, rather than the information be released by the WHO, the CDC, the FBI, or a number of other agencies who should have informed the public. Shellenberger is now 100% convinced that the SARS-CoV-2 virus came from the lab in Wuhan.
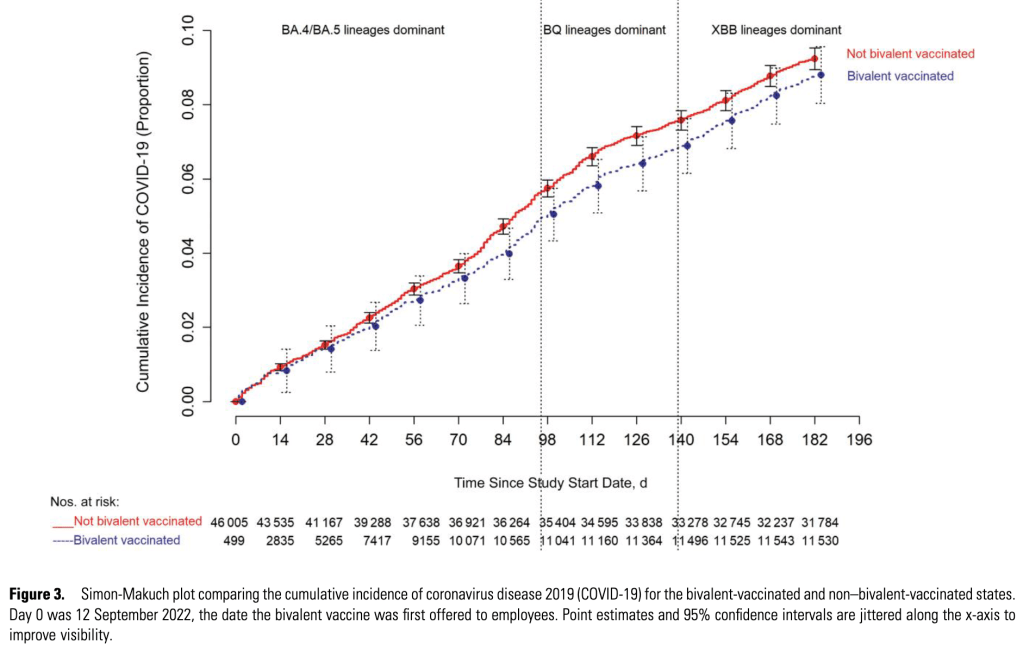
Boosters increase likelihood of reinfection: A study from the Cleveland Clinic claims that the likelihood of reinfection with COVID-19 actually increases with more vaccine boosters. The study began in the Summer of 2022, during the BA.5 outbreak, and shows increased likelihood of infection by later variants the more boosters a person had! It’s unknown why this phenomenon occurs, but it may be a mechanism similar to Antibody Dependent Enhancement (ADE) which I was concerned about early on. Happily, available data doesn’t appear to show that ADE has caused more severe symptoms in COVID patients.
The paper also shows that the new Bivalent boosters, containing both the original Wuhan strain and an Omicron strain, has only a mild benefit to prevent infection.
Adverse events were batch dependent: A paper from a lab in Denmark appears to show that the number of adverse events associated with vaccines, referred to as “suspected adverse effects” (SAEs), were dependent on the batch in question. Adverse events appeared to cluster in 3 groups, some vaccine batches produced very few events, while others produced thousands. This difference probably contributed to the confusion and the difficulty of identifying real problems. The worst batches produced adverse events at a rate of almost 9%, and also produced the most severe effects.
These results should provide some clues as to what went wrong with the vaccine rollout. Unfortunately, this data comes from cases in Denmark so is less relevant to the US. This is the kind of information that is the CDC’s job to produce. The fact that the CDC is not producing data like this is a big worry, and shows that the agency is in dire need of reform.
Excess deaths may be related to vaccine induced inflammation:Ed Dowd was on the Dr. Drew podcast. Dowd has an interesting take on adverse events. He is an analyst for an investment firm, and looks for trends to help in making investment decisions. He often uses information from insurance claims to analyze trends in worker health, illness, accidents, and death. He noticed that in the UK, there were approximately 500,000 excess deaths in both 2021 and 2022, many among younger people. This effect was correlated to being in the Millennial generation and being employed. He says that in late 2021, excess deaths among Millennials was 84% above normal.
He says that hematological (blood related) illnesses were up 522% in 2022, during the time when Omicron was dominant. That’s 61 standard deviations above the expected trend. For those of you who know statistics, you know that this is far, far, above what you would expect for a random event. Dowd is asking physicians to help his team interpret this data.
At this point, it seems unlikely that we will get accurate information on adverse events in the US. Unfortunately, the CDC is too politicized to perform its function.
I’m not a physician. But in my informed opinion, there is no longer a benefit to getting a COVID vaccine booster, even if you are at high risk.
Happy New Year! I have a brief COVID update for you. Then I’ll talk about a new variant, XBB.1.5. I’ll also have comments on a smattering of evolving stories, like California AB 2098, “Physicians and surgeons: unprofessional conduct”, and a new Twitter Files thread on vaccine misinformation.
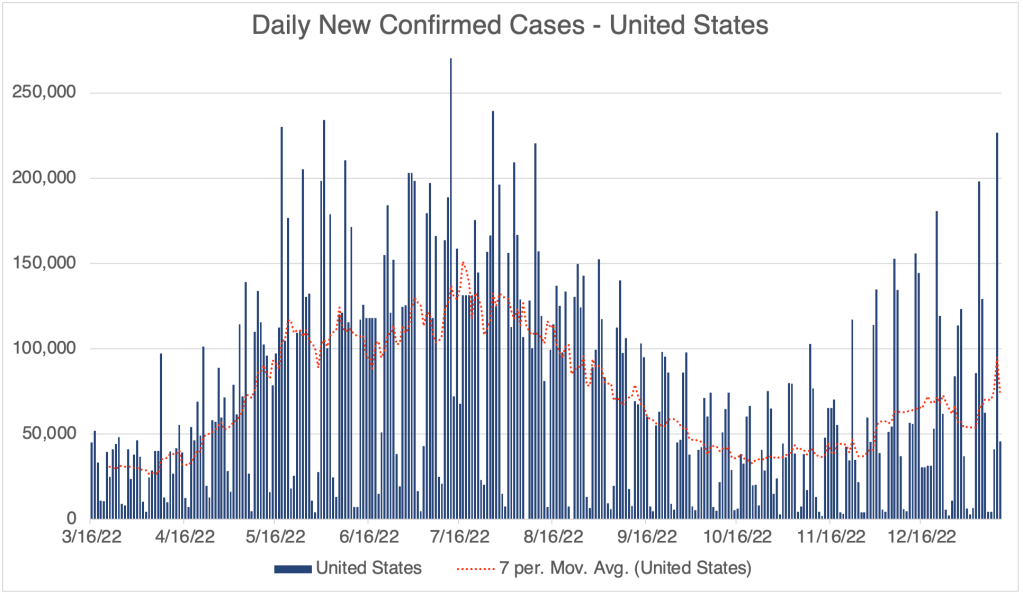
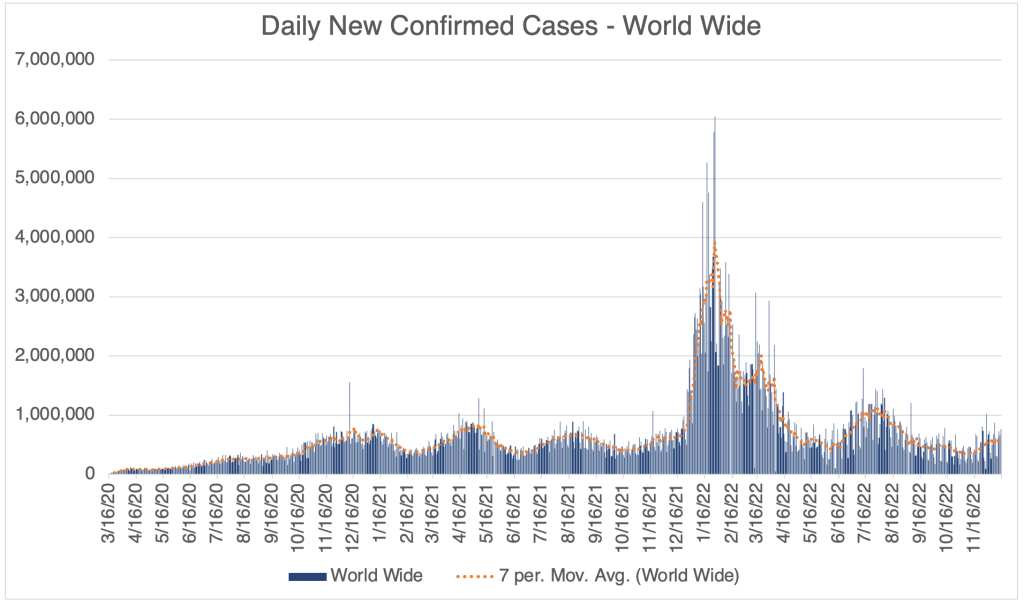
We have already reached the peak of the December wave. Cases in the US, California, and San Diego, and even world wide, peaked at around Christmas. Deaths never really had a peak during this December wave, except in San Diego County.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Daily Confirmed Cases – United States, March 16, 2022 to January 12, 2023. Peak of the first Winter Wave was on around Christmas Day. We may already be seeing the start of an XBB.1.5 peak. Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
However, we may see a second Winter wave this year…
New Variant XBB.1.5: A new variant is spreading extremely rapidly in the US right now. Variant XBB.1.5 is about 43% of the SARS-2 virus in the US right now. A UK study suggests that this new variant is the most transmissible yet. John Campbell, in another excellent analysis, suggests that about 80% of us will get it. Antibody studies suggest that even those with prior COVID infections do not produce many antibodies that can neutralize XBB.1.5, so even those who have had COVID before are likely to get it again. The good news is, XBB.1.5 is another Omicron strain, and will produce very mild symptoms in the vast majority of cases. I’ve had COVID twice already, and I will treat XBB.1.5 as a chance to get a free booster.
From the CDC page on Variant Proportions for the United States. Updated for January 14th.From the CDC page on Variant Proportions for the United States. Updated for January 14th.XBB.1.5 is the most infectious of the current variants, and perhaps the most infectious variant to date. From the UK Health Security Agency, Technical Briefing 49.
Despite the likely mildness of XBB.1.5, do others a favor and stay at home if you have COVID. The over-the-counter antibody based COVID tests do not work very well, so if you are sick but have a COVID negative antibody test, you should assume you have COVID. Only a PCR test can tell you if you’re really negative.
If you haven’t yet had COVID, I can no longer recommend that you get a vaccination or a booster, even if you are in an at-risk group. If you are concerned about getting COVID, consider taking precautions instead. Wear a N95, KN95, or KF94 rated medical respirator when indoors in public. It’s also important to make sure your mask fits snugly. The mask must filter air coming into your nose and mouth. Loosely fitting masks with large gaps will not do this. Do not wear a cloth or surgical mask. These masks will not protect you from XBB.1.5.
California Physician Misinformation Act: On October 4th, 2022, I wrote about California AB 2098. This new law went into effect on January 1st and adds “the dissemination of misinformation or disinformation related to the SARS-CoV-2 coronavirus” to the definition of unprofessional conduct for physicians in California. Unprofessional conduct can result in the suspension or loss of license for physicians in California.
Just yesterday, I had lunch with a friend of mine who is a doctor in California. I asked him how he is dealing with this new law. He said most of the doctors at his hospital follow the official guidance promoting vaccination, and the few who don’t have become very quiet about vaccines. Doctors can’t say anything negative about the vaccine, for the risk of their medical license.
In 2021, this same doctor was coerced into getting the vaccine to retain his position at the hospital. He got a booster later in the year. A month after receiving his booster, despite being very physically fit for his age, he had a heart attack. His cardiologist said he had none of the arterial plaques that typically cause heart attacks. My friend cannot prove this, but he strongly suspects that clotting due to the vaccine contributed to his heart attack. Despite all this, he does not feel at liberty in California to give information to patients that would reflect negatively on the vaccines.
Because this law is so new, I don’t yet know how it will be handled by the Medical Board of California. If they choose to ignore it, then doctors won’t be under threat. However, doctors and pharmacists have lost their licenses in the last few years for violating CDC guidelines, so the threat is a real one.
If you live in California, you cannot expect your doctor to give you their honest opinion about vaccines. This is literally illegal now. Consider writing your state senator or assemblymember and ask them to support the repeal of AB 2098.
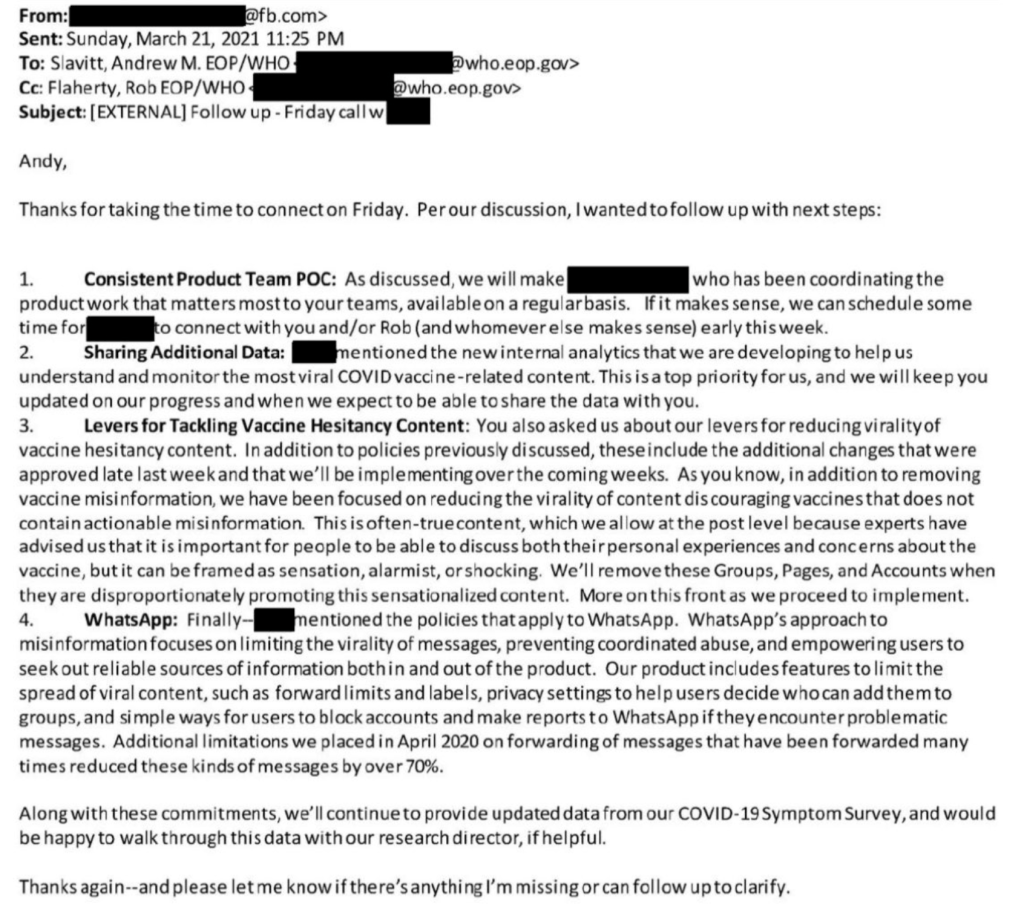
The Twitter Files have exposed a trove of evidence that official government agencies have been coercing several social media companies to censor COVID related information. In an amazing post from Michael Shellenberger, a F@¢eb00k official recently revealed that F@¢eb00k was reducing content not because they thought it was misinformation, but simply because it had a sensationalist tone. In an email to a Whitehouse official, the F@¢eb00k employee wrote:
“As you know, in addition to removing vaccine misinformation, we have been focused on reducing the virality of content discouraging vaccines that does not contain actionable misinformation. This is often-true content, which we allow at the post level because experts have advised us that it is important for people to discuss both their personal experiences and concerns about the vaccine, but it can be framed as sensation, alarmist, or shocking.”
Obviously, these efforts to limit expression by a government agency is a violation of the first amendment, our most important freedom. There are now many, many examples of this in the Twitter files, relating to COVID, and other matters.
This is a COVID update. Then I’ll discuss the high number of RSV and flu cases right now. I’ll also discuss the issue of vaccination induced blood clotting and the film “Died Suddenly”.
There has been a modest rise in cases in the past few weeks, suggesting that we will have a winter wave of cases. So far, this wave is not nearly as high as last December, when the Omicron variant first became dominant in the US. This is according to official testing data. Many are no longer being testing in a medical setting, so the number is likely much higher.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
Hospitalization data provides a better relative view of cases, since it shows how many are actually entering the medical system with moderate to severe cases, but San Diego County is no longer providing this information on their website.
As we’ve discussed before, the drug store tests are not nearly as sensitive as a PCR test, and I know several people who were negative by this kind of test for days after symptoms began. The drug store tests can tell you if you have COVID, but false negatives are common, so if you get a negative result, it doesn’t mean much. If you really need to know if you have COVID, get a PCR test.
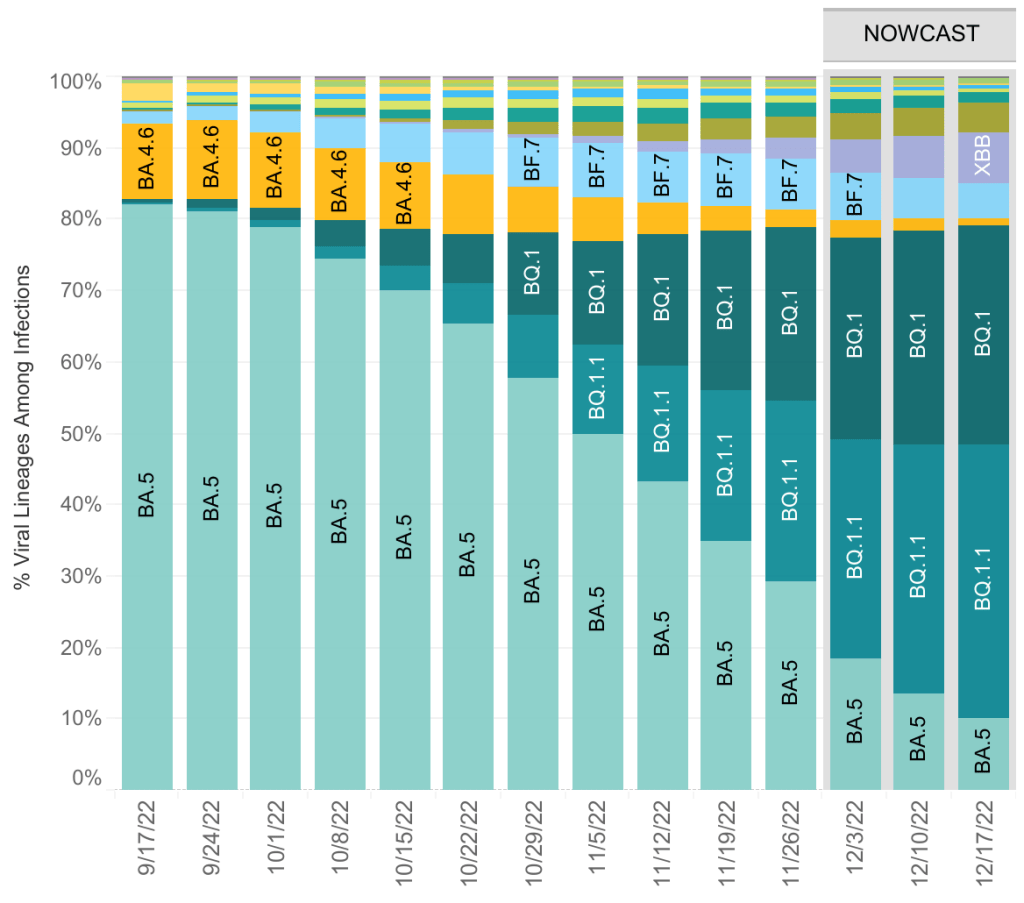
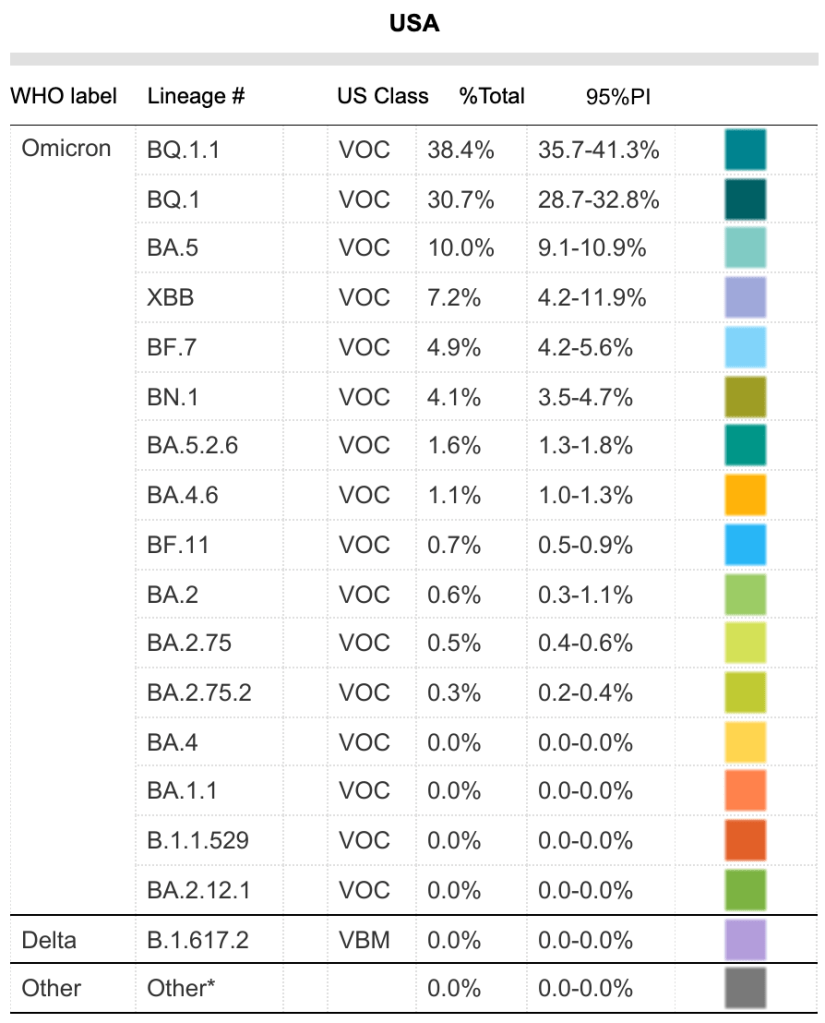
The BA.5 variant now represents only 10% of currently circulating COVID variants. There are currently 12 variants circulating in significant numbers, the most common being BQ.1.1.
From the CDC page on Variant Proportions for the United States. Updated on December 17th.From the CDC page on Variant Proportions for the United States. Updated on December 17th.
Tridemic: A physician friend of mine who works in urgent care joked that we are currently in a “tridemic”, by which he meant that there a lot of COVID, Flu, and RSV cases right now. Everyone knows about the flu, but many are unfamiliar with RSV. Well, actually, you are. Respiratory Syncytial Virus (RSV) is one of the several viruses that are responsible for what we call the common cold. You have likely had it many times in your life.
For most people, RSV is just an annoyance, but it can be serious for infants, causing bronchiolitis, a swelling of lung tissues. If your infant is coughing a lot, breathing rapidly, wheezing, or just breathing noisily, contact your doctor. Those with infants in their life may consider taking extra precautions to avoid passing along a cold. The blue surgical masks are not a good defense against COVID, but they are effective to prevent droplets which transfer colds and flus.
Many guess that RSV has become more serious because we have been so cautious for the last few years. I don’t know for sure if this is true, but it seems like a reasonable idea.
Long blood clots due to vaccines: Chris Martenson has a new video regarding the long blood clots that many embalmers have discovered in the arteries of COVID vaccine recipients. The phenomena started occurring in May of 2021, a few months after vaccination became common. Dr. Martenson is a pathologist and has done many autopsies in his career.
Chris Martenson on vaccine related blood clots:
In the video, he addresses a recently released documentary called “Died Suddenly”. The documentary claims that at least 140,000 people have died due to these vaccine induced blood clots. In Martenson’s video, he points out that detractors of the “Died Suddenly” film argue that these clots are post-mortem, meaning they arise after the person has died. Dr. Martenson argues that the clots in vaccinated patients are definitely pre-mortem (before death), not post-mortem as some have claimed. He gives specific features that lead him to this conclusion.
Dr. Martenson is one of my favorite commentators. He is knowledgeable, open-minded, and evidence based.
I got a question about whether these clots only happen in vaccinated people. Late stage COVID disease is well known to cause clotting. But COVID related blood clotting mostly cause strokes and thrombosis. Obviously, these can also be very serious and lead to death. The vaccine related clots are different, completely blocking vessels. It’s not yet known how large they are pre-mortem. Dr. Mortenson argues they are pre-mortem, but that doesn’t mean they won’t continue to grow before an autopsy.
Searching “COVID blood clot” and “vaccine blood clot” on Pubmed will both bring up a lot of papers. I haven’t read enough of these yet to know if the large clots only happen with vaccination. The fact that you don’t need to get COVID to have clotting is obviously very important.
Died Suddenly: Several people have asked my thoughts on this film. I will say that many COVID-era documentaries have a definite bias, so I always have my guard up when watching them. Claims without sufficient evidence are common.
The opening credits juxtapose images regarding blood clots and potential vaccine related deaths with images from other unproven theories, some that most regard as untrue or even ridiculous, like bigfoot and UFOs. This seems intentional, as if the makers intend for the viewer to pair these ideas. This seems to me to be ill-advised, if they intend to convince the viewer that blood clots can be tied to COVID vaccines. It almost begs the viewer to associate their thesis with nonsense.
The basic premise of the film, the phenomena of vaccine related clots, seems to be at this point to be well founded and well evidenced. The film offers several disturbing images of these clots being removed from cadavers. The film also shows many examples of individuals passing out suddenly, while driving, speaking in public, even performing surgery. The existence of this phenomena seems beyond dispute. Interestingly, the detractors Martenson references in his video claim that the clots are post-mortem, not that the clots don’t exist at all. Clotting has been a well known aspect of late stage COVID disease.
In addition to the potentially valid idea that vaccines have contributed to blood clotting in patients, the film makes the explosive claim that the deadly effects of the vaccine are actually intentional. I haven’t seen any data to suggest this connection. I’m not saying this is untrue, just that I haven’t seen evidence of this yet, so I don’t see a reason to believe it at this time.
The SARS-CoV-2 Spike protein has several toxic effects. First, it causes an inflammatory response in many tissue types in the body, leading to diverse symptoms, including myocarditis, inflammation of heart tissue. This new phenomena shows that the spike protein can also cause blood proteins like fibrin to form an amyloid, an unnatural collection of proteins. Amyloid plaques also have a role in Alzheimer’s disease.
Should you get the updated booster? COVID vaccines appeared to be working well in the Spring of 2021, but their effectiveness began to wane with the Delta variant. When Omicron became the dominant variant, vaccine effectiveness dropped even further. As knowledge of possible harms due to the spike protein has increased, I now think the harms of vaccination outweigh benefits in our current environment. In my opinion, there is no longer any reason to get a vaccine or booster, even for those with risk factors.
If you’ve been vaccinated, this information will likely cause you some concern. I don’t know how long vaccine related spike protein has the potential to cause injuries. Blood clots appear to form around 5 months after vaccination. If you haven’t been vaccinated or boosted in the last 7 months or so, you may be in the clear. I’m sorry I don’t know more.
I have to point out that official channels claim that the information in “Died Suddenly” has been de-bunked. When posting this information on Facebook, I was met with several warnings about posting. To be fully informed on this issue, you should read several sources of information and judge for yourself which are most reliable.
Even though many think the pandemic is basically over in the US, there was still a ton of COVID news this last week. As usual, I’ll tell you what I’m going to talk about in the intro, and you can check the headlines down below to read what interests you. Some sections will be more detailed than many care about, and I have labeled those sections.
This is a COVID case update. I’ll also discuss yet more COVID variants, and a new paper from Greece about vaccines and inflammation. I’ll also discuss a preprint paper from Boston University in which they claim to have created a hybrid SARS-2 virus. Last, I’ll talk about a recent study which sheds some light on the number of people in the US who have actually had COVID as of February.
Case Update: Cases continue to go down in the US, California and San Diego County. This has been a steady trend since mid-July. Cases are about the same as in the Spring, before BA.5 arose. Despite several new variants, deaths have not had a new peak, and are still relatively low, but not as low as the Summer of 2021, before the Delta variant arose.
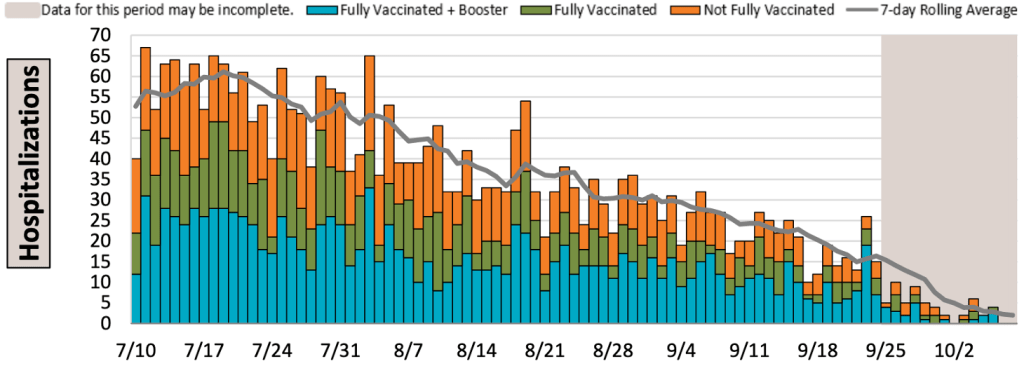
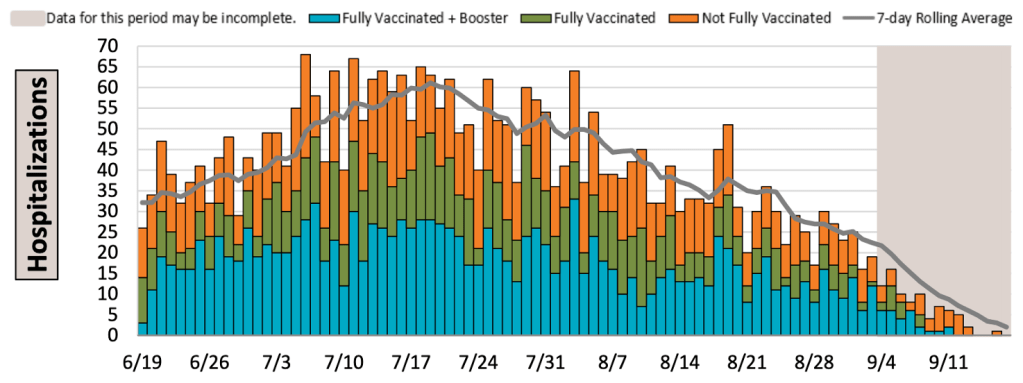
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format. Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Hospitalizations in SD County, July 10th to October 10, 2022. Gray area represents time-frame in which data is still being collected. Note that a significant number of hospitalizations are among the vaccinated.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
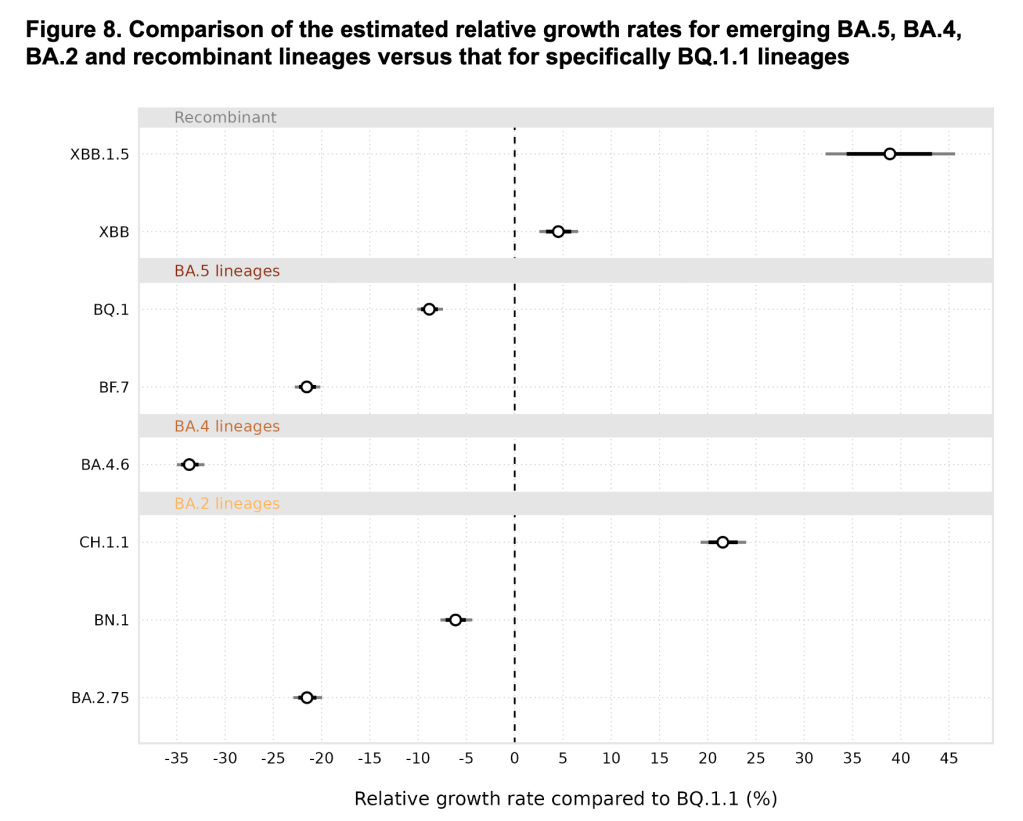
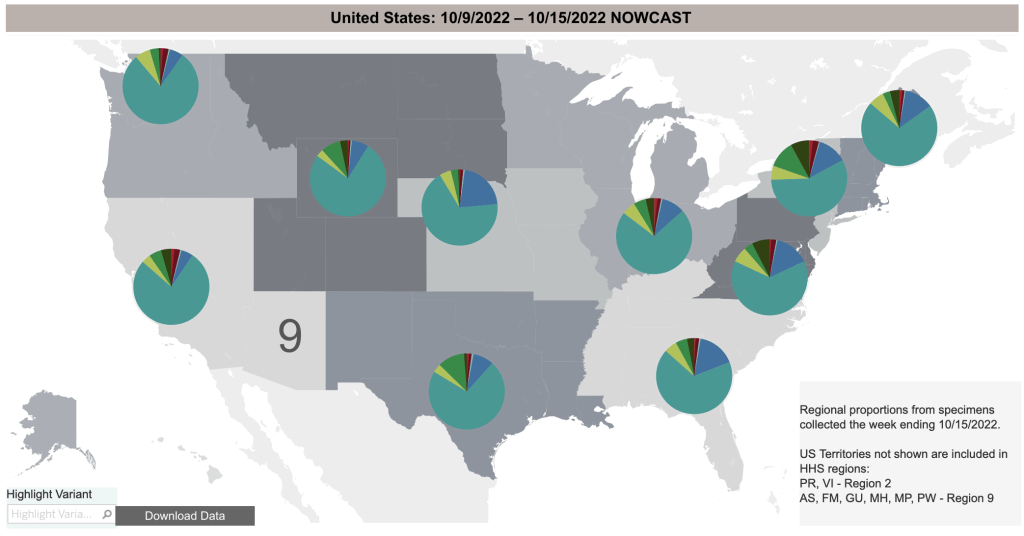
New variants: There are more new variants. They continue to follow the trend of being more infectious than previous versions. Some outlets are raising alarms about these new variants (BF.7, BQ.1, XBB), but there is not yet concrete evidence that they are more pathogenic than other recent versions. There was concern that BA.5 was truly more pathogenic than other Omicron versions, but it still didn’t produce a new wave in deaths, perhaps because so many Americans now have either vaccine or natural immunity. How many? See below!
From the CDC page on Variant Proportions for the United States. Updated on October 15th.From the CDC page on Variant Proportions for the United States. Updated on October 15th.From the CDC page on Variant Proportions for the United States, by region. Updated on October 15th.
Spike protein may contribute to adverse events: A July opinion paper from Greece claims that the Spike protein produced by vaccines cause inflammation and may be responsible for adverse events. The paper was published by Cell Press, one of the premiere science journal publishers.
If you’ve been reading my posts for a while, you will know that I first wrote about the link between the Spike protein and adverse events way back July of 2021. For many months, the idea that vaccines were causing a lot of adverse events, and that the Spike protein itself was toxic was considered misinformation by the American medical establishment, yes, even by me. Now this idea is becoming a topic of debate and perhaps even accepted.
If you look up the words “adverse events covid vaccine” on PubMed, the site biologists use to search scientific articles, you will now see dozens of papers linking vaccines, the spike protein, inflammation, and adverse events. Sorry, I still do not know just how many adverse events there are, as this information has not been adequately collected and/or shared by the CDC.
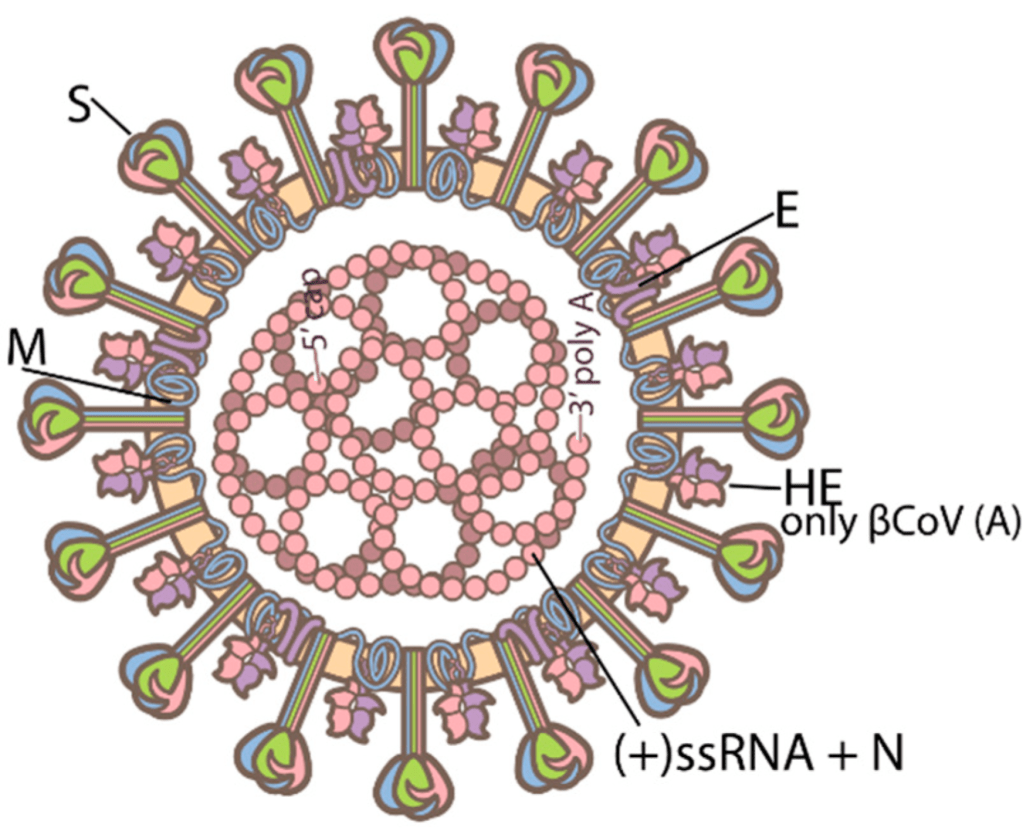
Details: Many scientists are now suggesting that the vaccine should have used the Nucleocapsid protein rather than the Spike protein. Nucleocapsid is a SARS-2 protein that helps package the RNA genome. It does not change as rapidly as the Spike protein and does not interact directly with human proteins, so is not toxic. For these reasons, it would have been safer to use the Nucleocapsid protein instead.
Structure of SARS-2. Spike is the tall outer protein, Nucleocapsid is the internal pink protein. From Sriwilaijaroen, N.; Suzuki, Y. Host Receptors of Influenza Viruses and Coronaviruses—Molecular Mechanisms of Recognition.
The downside is that a vaccine using Nucleocapsid would not have prevented initial infection. Why would it have been useful then? When the immune system destroys a virus, proteins from the virus end up getting displayed on the outside of cells, either infected cells, or immune cells. This gives the immune system a chance to either detect these viral proteins and use them or make antibodies, or as a signal that a cell is infected and needs to be destroyed.
If the Nucleocapsid protein were used in a vaccine, SARS-2 could still infect human cells, since Nucleocapsid is inside the virus where the immune system can’t see it. However, after a cell is infected, it displays Nucleocapsid on the outside. If a person is immunized, immune cells will detect these proteins and destroy the infected cell. While using Nucleocapsid in a vaccine wouldn’t prevent infection, it would probably greatly reduce viral load and symptoms.
Keep in mind that this is Monday morning quarterbacking. Scientists didn’t know that the Spike protein itself was toxic when they created the vaccines, and internal viral proteins aren’t generally used in vaccines, so it didn’t occur to anyone to do this at the time. It is being discussed now, though, and may change vaccine design in the future.
Of course, we all now know that the Spike vaccines did not prevent infection by the Delta and Omicron variants.
Hybrid SARS-2 Virus Created in the Lab: This Monday, a lab at Boston University reported that they had created a strain of SARS-2 virus that killed 80% of infected mice. The internet freaked out and subsequent reports said that it wasn’t all that bad, etc. So I wanted to discuss this paper, tell you want exactly they did, and what I think about it. There will be some detail, but I’ll give you a summary at the end if you want to skip to that.
The Boston group led by Mohsan Saeed took the Spike protein from an Omicron variant, and knitted it into the backbone of the original Wuhan virus. The goal was to see what made the Wuhan virus more pathogenic, and the Omicron virus less pathogenic. Was it the Spike protein, which determines transmissibility, or the internal viral proteins which determine other factors like how fast it replicates in a cell.
The resulting virus, called Omi-S was in fact much more pathogenic than Omicron, but not as pathogenic as the original Wuhan strain. In the now infamous 80% kill rate experiment, it is important to know that the mice were infected in a very efficient manner, so that they were likely to have a severe case. Also, the ancestral Wuhan strain killed 100% of these mice (6 mice died out of 6 mice tested). The Omicron strain killed 0%. So if Omi-S were to escape into the population, it wouldn’t kill 80% of the population, only 80% of the number that Wuhan killed. So if Wuhan killed 1 – 3% of victims, Omi-S might only kill 0.8 – 2.4%. Using several measures, Omi-S was much more pathogenic than Omicron, but less pathogenic than the Wuhan strain.
On the other hand, Omicron was well known to be much more transmissible than the Wuhan strain. Presently, even countries that did well early in the pandemic have been unable to control Omicron and have experienced big outbreaks this year. So it is likely that Omi-S could spread extremely rapidly, and still kill more people than the original Wuhan strain.
So was this result worth the risk? Most infectious disease scientists know that the 1918 flu was so dangerous not just because of its unique surface proteins, but also because the internal proteins were especially robust. The result with Omi-S paper shows much the same thing. To me, the paper gave a result which was unsurprising. Scientists will disagree on whether this new variant should have been created. In my view, it was not worth the risk to create such a potentially dangerous variant to get a “water is wet” result.
Does Omi-S still pose a threat? Experiments like this in the US are usually monitored by the CDC or other agencies. Labs are generally required to destroy dangerous agents when the experiment is over. It is likely that Omi-S no longer exists. But given the unintentional release of SARS-2 in the first place, I think Americans may feel justified in being a little nervous about these experiments.
As an aside, in many infectious disease experiments, scientists go through a lot of effort to create test viruses or bacteria that cannot survive outside the lab environment. They do this by making versions that are incomplete, or need to be provided specific nutrients to survive.
Summary of the Hybrid SARS-2 virus: The Boston lab created a virus that combined the internal workings of the more pathogenic Wuhan strain with the more transmissible Omicron Spike protein. They found that the internal proteins were likely responsible for the higher pathogenicity of the Wuhan strain. In light of what is known about the 1918 flu virus, this result is not surprising. While this hybrid virus likely no longer exists, my view is that the incremental knowledge gained was not worth the risk of creating this strain.
Headlines that the virus killed 80% of mice were true but misleading. Under the conditions of the experiment, 80% of mice were killed by the new virus, but 100% of mice were killed by the original Wuhan strain. So this virus would be approximately 80% as deadly in infected people as the Wuhan strain.
How many people have had SARS? The CDC published a paper in April describing “Seroprevalence” in the American population. “Seroprevalence” basically means the number of people who have antibodies for a particular virus. The study detected antibodies against the Nucleocapsid protein in patients between September 2021 and February 2022. They did not have a random sample of patients, but rather used lab samples gathered when the people tested went to the doctor for any reason. So the subjects were skewed to people who were sicker or otherwise more engaged with health care than others.
Because they detected antibodies against Nucleocapsid and not Spike, the study did not detect vaccinated people, only those who have had COVID. Interestingly, the results showed that 75% of children up to 11 have had COVID, and the number was lower in each higher age group. Of those 65 and older, only 33% have had COVID.
This post is about a new California law seeking to limit misinformation.
California’s Governor Gavin Newsom signed AB 2098 into law on Friday. The new law allows the Medical Board of California to punish health care providers for spreading misinformation. The law does this by adding the act of spreading misinformation to the definition of “unprofessional conduct” used by the Medical Board of California. Unprofessional conduct is punishable in California by up to the suspension or loss of a license to perform medicine.
The law defines “misinformation” as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.”
There are many, many examples of ideas in science and medicine that were opposed by the scientific consensus and later accepted as true. There are so many examples of this, that it should be considered as a normal part of the scientific process. Examples include:
The Earth revolves around the Sun
Not cleaning surgical tools between operations can lead to increased mortality in patients
Ulcers are caused by the bacteria H. pylori, not by spicy food
Viruses can cause cancer
Cells produce energy by passing electrons through a membrane
The universe began at a discrete moment, and then expanded to its current form, creating both space and time in the process
The SARS-2 virus was created in a laboratory in Wuhan*
The idea that misinformation can reasonably be defined as an idea that is contradicted by scientific consensus is itself contradicted by centuries of scientific practice.
Scientific ideas come to be seen as true not merely by achieving consensus, but also by surviving challenge by new ideas. No scientific idea is immune to this process. Science is not a set of facts set in stone, but a constantly changing set of ideas guided by the scientific process, a process which includes debate among scientists. Requiring that new ideas achieve consensus immediately would freeze the advance of science in place, the current, and often wrong, ideas remaining dominant forever.
Of course, I have not yet addressed the obvious First Amendment violation this new law creates. The First Amendment clearly allows freedom of speech, a cornerstone of American life. This law will quickly be challenged by First Amendment advocates and will almost certainly be struck down.
As I’ve stated before, freedom of speech is not the cause of misinformation. It is the antidote. Only if we allow the free flow of ideas can these 3 things happen:
All ideas to be aired Good ideas to be confirmed and adopted Bad ideas to be discredited
Dr. Mobeen Syed points out several other negative impacts this law will have:
Doctors will be suspicious of their patients, compromising the doctor/patient relationship.
Doctors will only give consensus advice, making going to the doctor more like going to a call center.
Laws will expand to include other kinds of “misinformation” further compromising the exchange of ideas.
Law will be used unequally to silence only certain kinds of speech.
Doctors may choose not to practice in California.
If I’m being too subtle, I’ll just say that this is a bad, unconstitutional law and should simply be ignored.
Don’t fear, but be smart, Erik
* I’m taking a little liberty on this one. This idea was rejected totally early in the pandemic. It is not yet universally recognized as true, but many scientists, including me, see it as most likely to be true.
_____________________________________________ Update: January 13, 2023
California Physician Misinformation Act: On October 4th, 2022, I wrote about California AB 2098. This new law went into effect on January 1st and adds “the dissemination of misinformation or disinformation related to the SARS-CoV-2 coronavirus” to the definition of unprofessional conduct for physicians in California. Unprofessional conduct can result in the suspension or loss of license for physicians in California.
Just yesterday, I had lunch with a friend of mine who is a doctor in California. I asked him how he is dealing with this new law. He said most of the doctors at his hospital follow the official guidance promoting vaccination, and the few who don’t have become very quiet about vaccines. Doctors can’t say anything negative about the vaccine, for the risk of their medical license.
In 2021, this same doctor was coerced into getting the vaccine to retain his position at the hospital. He got a booster later in the year. A month after receiving his booster, despite being very physically fit for his age, he had a heart attack. His cardiologist said he had none of the arterial plaques that typically cause heart attacks. My friend cannot prove this, but he strongly suspects that clotting due to the vaccine contributed to his heart attack. Despite all this, he does not feel at liberty in California to give information to patients that would reflect negatively on the vaccines.
Because this law is so new, I don’t yet know how it will be handled by the Medical Board of California. If they choose to ignore it, then doctors won’t be under threat. However, doctors and pharmacists have lost their licenses in the last few years for violating CDC guidelines, so the threat is a real one.
If you live in California, you cannot expect your doctor to give you their honest opinion about vaccines. This is literally illegal now. Consider writing your state senator or assemblymember and ask them to support the repeal of AB 2098.
The Repeal of the California Physician Misinformation Act: Last October, I wrote about a new California law which made “misinformation” a cause for physicians in California to lose their medical license. Misinformation was defined as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.” As I argued, it is common for new scientific ideas to be opposed by the majority of scientists before gaining acceptance.
The new law immediately became a target of legal action, one case being Høeg vs Newsom. On September 29th, 2023, Høeg’s attorney filed a request that the law be permanently barred from enforcement. Just a few days later, on October 1st, California Governor Gavin Newsom signed a repeal of the law. This is great news for California physicians and patients. California physicians are again free to communicate to their patients without fear of losing their license. This is also great news for the cause of freedom of speech in the US.
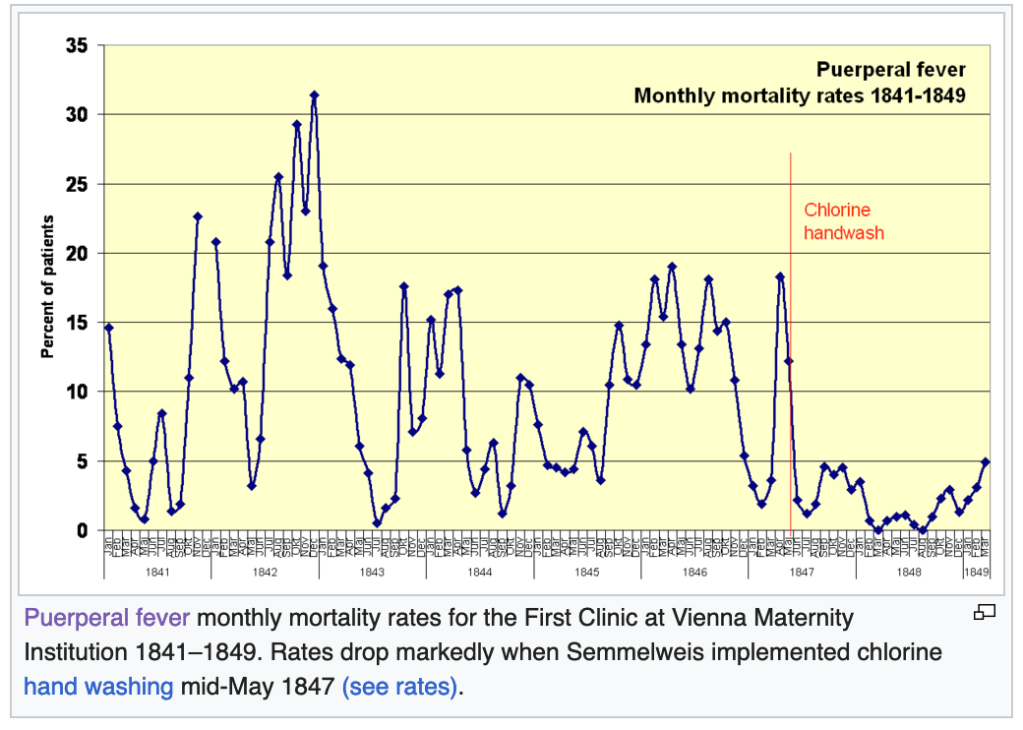
The fascinating yet tragic case of Dr. Ignaz Semmelweis:Ignaz Semmelweis was a physician at Vienna General Hospital in 1847. One of his jobs was to deliver babies in the maternity ward. Unfortunately, in his ward, the rate of fatality for new mothers was high, an average of 18.3%. Women were afraid to deliver in his hospital, and begged to deliver somewhere else!
Then one day, a colleague of Dr. Semmelweis died of Puerperal Fever, with symptoms very similar to the women in the maternity ward. His colleague had nicked himself with a scalpel while performing an autopsy on a cadaver. Dr. Semmelweis thought that maybe the fatalities in the maternity ward had something to do with the fact that Doctors where going straight from performing autopsies to delivering babies!
At this point, you’re probably holding your head and saying “What!?”, perhaps with some other colorful words added in. It’s obvious to us now that this was a terrible idea, but the Germ Theory of Disease had not yet been accepted in medicine. The field at that time had no idea that microscopic organisms could transmit disease.
Dr. Semmelweis started having physicians wash their hands in a chlorine solution after performing autopsies. The maternal death rate fell immediately to below 5%, some months having zero deaths. Dr. Semmelweis tried to tell others of his findings, but no one believed him. After increasingly passionate and ultimately embarrassing behavior, his friends and family had him committed to a mental institution. He was abused by guards and died in 1865.
That same decade, Louis Pasteur and Robert Koch were producing evidence supporting the Germ Theory, and Joseph Lister began popularizing the use of anti-septic procedures in surgery, greatly improving outcomes for surgical patients. Semmelweis’ ideas would be vindicated, but not until after his tragic death.
Semmelweis is now considered a hero of modern medicine, having a university, several hospitals, and even a minor planet named after him.
Why did I tell this story? Under a law similar to the California Physician Misinformation Act, people like Semmelweis would have lost their licenses. Semmelweis’ story underscores the need for strict adherence to the Scientific Method, not the suppression of “misinformation.” We suppress unpopular ideas at our peril.
This is a case update. I’ll also comment on new variant, new boosters, and the President’s announcement that the pandemic is over.
Cases continue to go down in the US, California and San Diego County. Again, since most people are now testing themselves using over the counter tests, the official case numbers are probably a gross underestimation of actual cases. Hospitalizations are a better measure, and they are also going down.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Hospitalizations in SD County, June 19th to September 14, 2022. Gray area represents time-frame in which data is still being collected. Note that a significant number of hospitalizations are among the vaccinated.
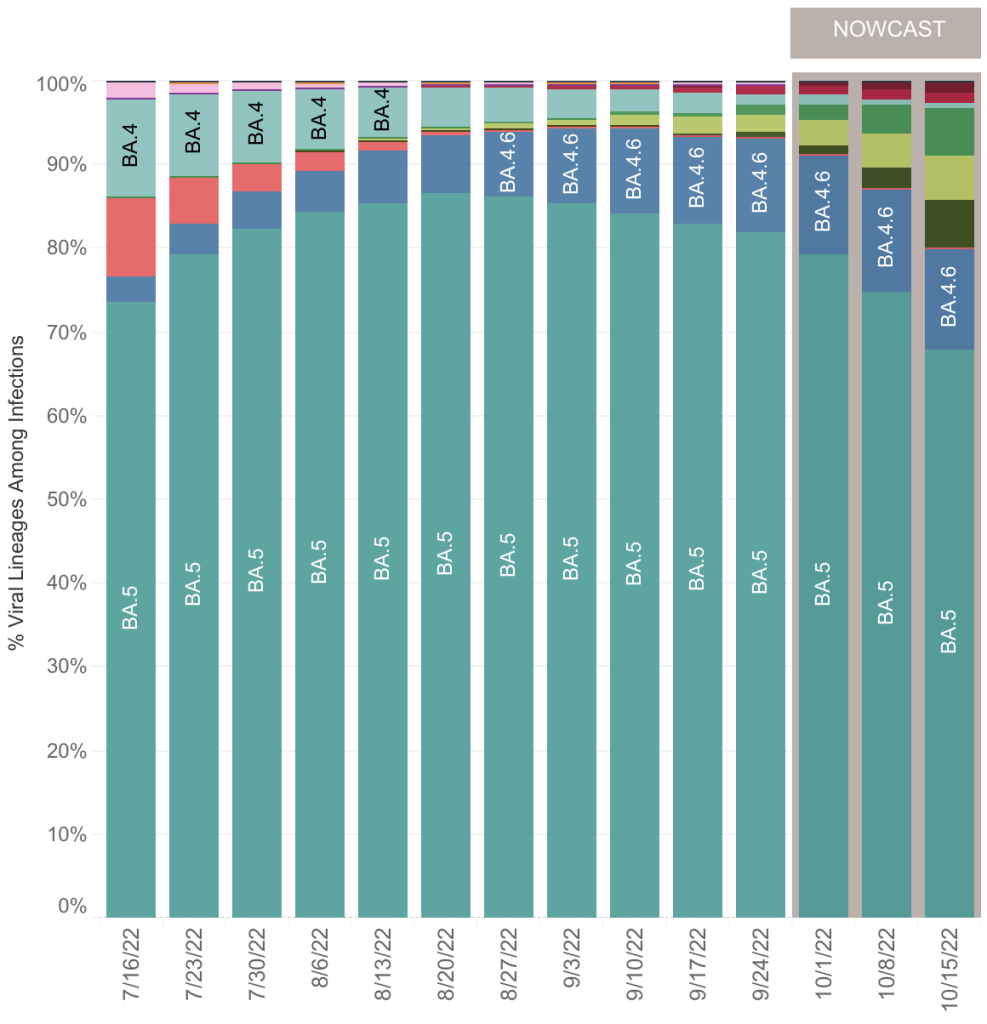
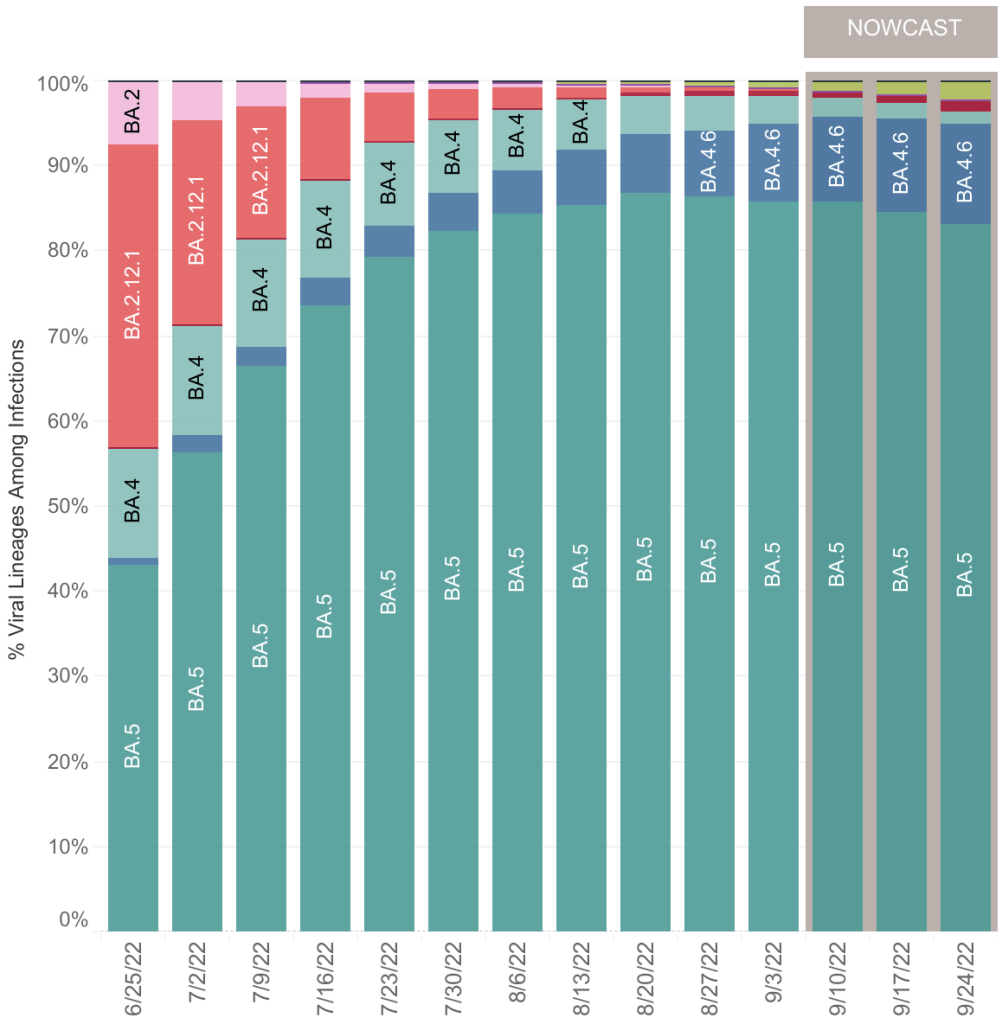
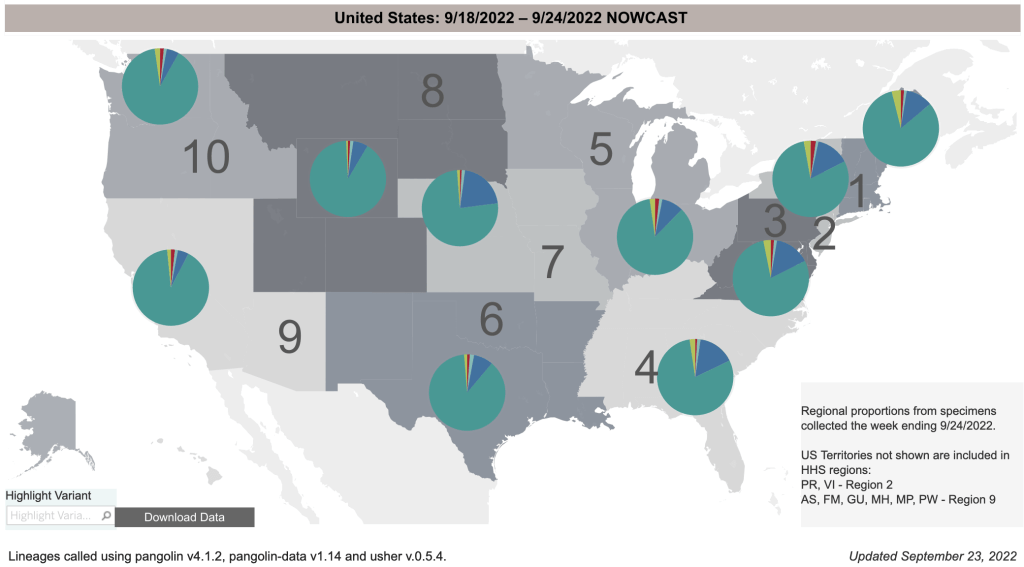
Variants BA.4.6 and BF.7: In my last post, I introduced a new variant BA.4.6. While hospitalizations are down, this new variant is now 11% of COVID cases in the US, and 20% of cases in the Midwest. Still, I don’t think this new variant is likely to have a big impact on the pandemic at the moment, and I expect cases to continue to go down. Deaths remain relatively low compared to the Omicron variant in April after the Winter wave. A newer variant, BF.7, is already growing in prevalence, but so far, there isn’t a lot of news about it.
From the CDC page on Variant Proportions for the United States. Updated on September 24th.From the CDC page on Variant Proportions. Updated on September 24th. Notice that BA.4.6 (dark blue wedge) is most prominent in the Midwest.From the CDC page on Variant Proportions for the Midwest. Updated on September 24th.
New boosters including Omicron strains: In August, the FDA announced emergency authorization of new boosters by Pfizer, Moderna, and Novavax. This new class of boosters produces spike proteins from the original Wuhan strain, but also from Omicron variants BA.4 and BA.5. People have been asking me my opinion about these new boosters. To preface my comments, I’ll say again that I am not a physician, epidemiologist, or immunologist, so my opinion is informed but not expert.
While the inclusion of BA.4 and BA.5 targets will make these new boosters an improvement over previous versions, I think most people will not benefit from them. For anyone who has had COVID, which is now arguably most of us, they will not really benefit you. Natural immunity has been shown in many studies to be equal or superior to vaccine mediated immunity in preventing infection and severe disease.
If you have never had COVID, you may benefit from the new booster. Keep in mind however that we have never really gotten clear data about adverse events after vaccination. In fact, Pfizer documents suggest that adverse events have been much more numerous than have been officially acknowledged. The new boosters have not yet been FDA cleared, and according to a video by John Campbell, Pfizer’s testing only included eight mice in their testing group. No human testing has yet been performed. Because variants are arising so quickly these days, I think the usefulness of new boosters is effectively over.
I suggested that my own parents get vaccinated in the Spring of 2021. But I am not suggesting that they receive the new booster. If you do choose to get the new booster, try and find a provider who will aspirate before injection.
President Biden announces that the pandemic is over: On September 19, CBS News released a video in which President Biden stated that the pandemic is over. In the interview, the President said “The pandemic is over. We still have a problem with COVID. We’re still doing a lotta work on it. … But the pandemic is over.” Of course, this triggered a debate on whether the pandemic is really over. At least a few health care officials said the health crisis is still ongoing, and that caution is still warranted. Debates are now ongoing as to the appropriateness of ongoing emergency measures like vaccine mandates and emergency use authorizations.
As for me personally, I had difficult time with COVID in January, and a much more mild case in July. I am basically behaving normally at this point. Most places I go, even in California, are basically going back to normal.
On other hand, hospitals are still seeing COVID patients and laboratories are still doing lots of COVID testing, so for them, COVID is still a reality they have to deal with.
If you’ve never had COVID, I would still recommend wearing a high quality medical respirator indoors in public (N95, KN95, or KF94). Blue surgical and cloth masks are not effective against Omicron variants.
This is a case update. I’ll also talk about a report from Kim Iverson from The Hill regarding finding in the trove of documents release by Pfizer in March and April.
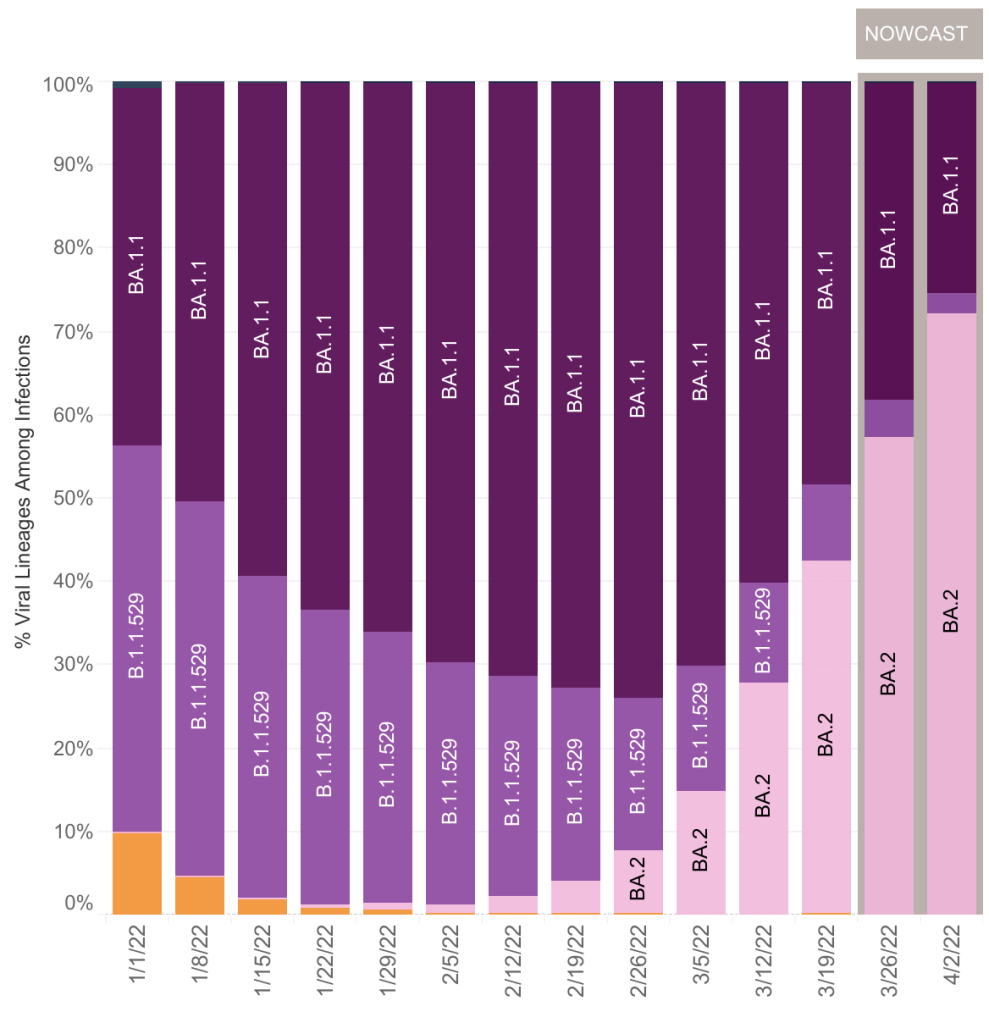
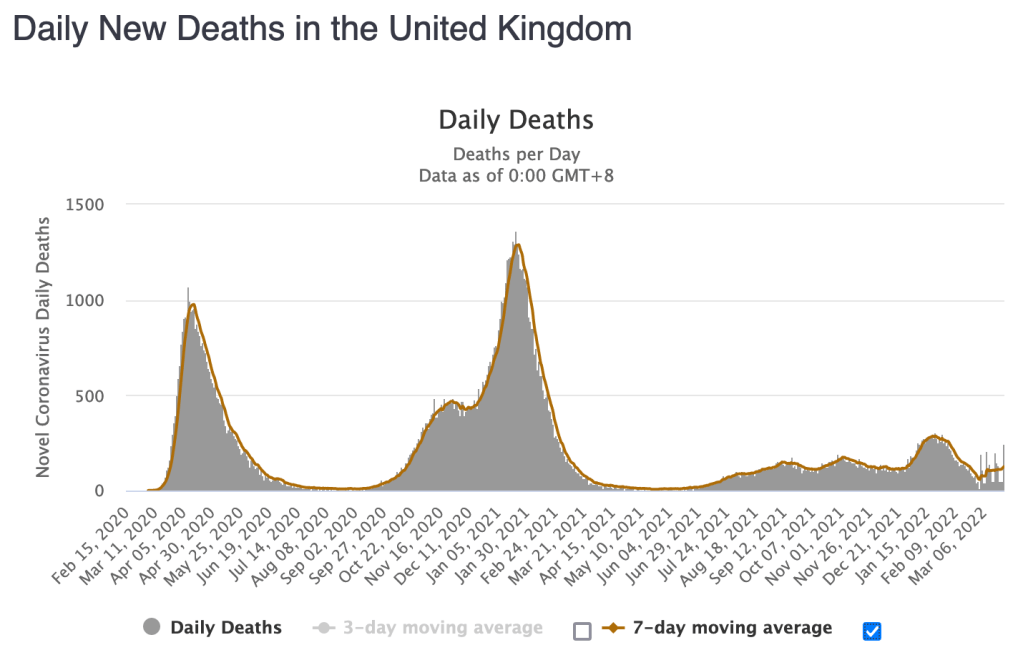
Cases are currently flat in the US. During the Omicron wave in December and January, the US lagged behind cases in the UK by 2 weeks. While the Omicron subvariant BA.2 produced a wave in the UK, it has not yet produced a wave in the US, despite it being 5 weeks since the BA.2 wave started in the UK. I’m going to go out on a limb and say that the slowing of the decrease of cases in the US is all we are going to see of the BA.2 wave in the US. I’ll let you know if this changes. BA.2 cases now constitute 72% of cases in the US.
Cases continue to go down in California and San Diego County.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.
XE variant: Just a few days ago, news emerged of a new COVID variant called XE in the UK. The variant is a hybrid of Omicron variants BA.1 and BA.2 and is more transmissible than BA.1. Since XE is very similar to other Omicron variants, I don’t expect it to cause a large wave of cases in the US.
Pfizer Document Analysis from Kim Iverson:Kim Iverson of The Hill released a video claiming that newly released documents from Pfizer confirm what many knew already. The shocking claim is that Pfizer has known the following for a long time:
Natural immunity is as effective as vaccine mediated immunity.
The rate of adverse events is at least 10/100,000 (33,000 for the US population). It’s unclear from Iverson if this is just for Myocarditis or for all adverse events.
It is unknown if the reproductive systems of women are impacted by vaccination. This contradicts public claims that vaccination does not affect reproduction.
A more severe case of COVID triggered by Antibody Dependent Enhancement could not be ruled out. The Lewnard et al paper a surveillance report from the UK have confirmed that higher Omicron infection rates in vaccinated people are likely due to ADE. As far as I’ve seen so far, ADE has not lead to more severe cases.
The documents were obtained because of a Freedom of Information Act (FOIA) lawsuit which required the FDA to produce the documents. Yes, this means that the FDA has had this information and did not disclose these conclusions to the public, instead often releasing information which contradicted these conclusions.
There will continue to be more document releases every month until the end of the year. There will likely be more bombshells, but most of the releases will simply confirm what people have suspected for months but couldn’t prove. I will discuss the most interesting, but not all of these releases.
If you have risk factors like obesity, age, or respiratory problems, you should consider getting a booster. Also, as I said last week, since vaccine effectiveness is substantially reduced after 3 months, those who have been vaccinated with risk factors will need to get a booster every 3-6 months. Try and find a provider who will aspirate before injection! There is no medical reason for someone who has had Omicron or Delta variants to get vaccinated or a booster. Talk to your doctor when making medical decisions.
I am posting about every 2 weeks now instead of every week. I’ll likely post even less unless interesting news comes out.
This is a brief case update. I’ll also make some more comments on BA.2 related waves in Europe, a new paper suggesting that vaccine mRNA persists in the lymph nodes. Also, new evidence from the UK suggests that vaccines lose potency after 6 months and certain vaccinated individuals are more likely to be infected than unvaccinated people.
Cases continue to go down in the US, although the rate of decrease is slowing. As you’ll read below, some suspect that an Omicron variant, BA.2, may cause cases to rise in the US.
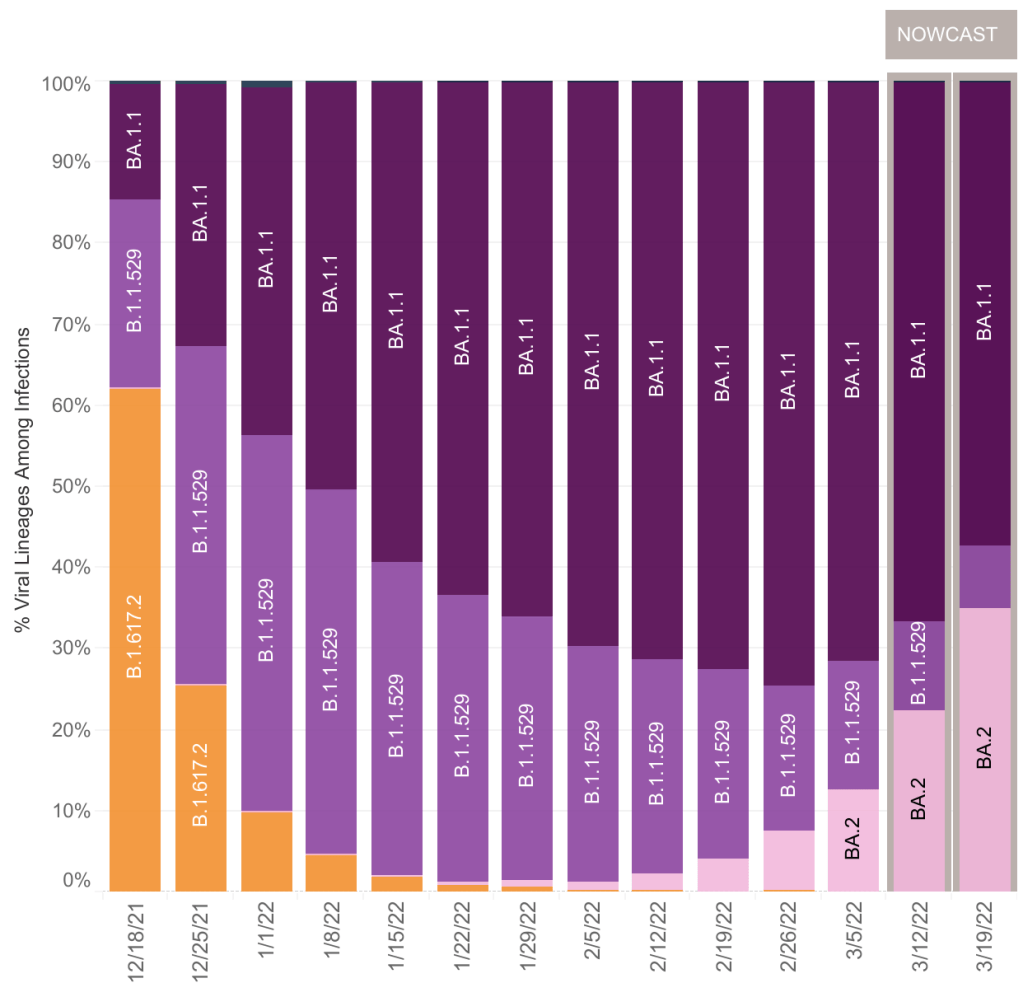
More on BA.2: I have commented on BA.2 before. This variant is a version of the Omicron variant, which is slightly more infectious than Omicron itself. It continues to follow the general trend of new variants being more infectious than older ones. Like the original Omicron, equal portions of B.1.1.529 and BA.1.1, BA.2 has a low fatality rate as compared to previous versions, including Delta.
I originally held that BA.2 is not particularly interesting because of its similarity to the first Omicron strains. This still may be true, but some countries like the UK and the Netherlands have seen significant new peaks after BA.2 became prominent. BA.2 is likely contributing to rising cases globally.
Right now in the US, BA.2 is increasing in prevalence, and is currently 1/3 of SARS-2 found in the US. It’s similarity to previous Omicron versions means that it is displacing B.1.1.529 and BA.1.1, just like Omicron displaced Delta before it. We now have 0% Delta in the US.
Does BA.2 significantly change the picture? I still say no, since the fatality rate with BA.2 is still very low, perhaps even lower than with other Omicrons. We may or may not see a significant BA.2 wave, depending on how many Americans already have resistance to BA.2. If you had Delta or Omicron, you almost certainly won’t get BA.2. Vaccination is only partially effective against Omicron variants.
Most people in my area, northern San Diego County, are basically going back to normal. This is warranted for most. If you have risk factors like age, obesity, or respiratory issues, you will want to remain vigilant and consider a booster. I do not recommend a booster for those without risk factors, and certainly not for those with natural immunity. Talk to your doctor when making medical decisions.
mRNA and Spike Protein Persist in Lymph System for up to 8 weeks: The Journal Cell just published a paper (Röltgen et al) which argues that mRNA and spike protein are present in vaccinated individuals for up to 8 weeks after vaccination. Cell is the third most highly respected journal in cell and molecular biology.
The cells in your body are surrounded by a fluid called “interstitial fluid”. This fluid carries nutrients from nearby blood vessels to your cells, and also carries waste back to the blood vessels. The lymph system is a one-way circulatory system that carries excess interstitial fluid from the extremities of your body back to veins near your arm pits. On the way, they pass through the lymph nodes, a biological filter and part of your immune system that checks for invading particles.
The Röltgen et al paper suggests that vaccine mRNAs from the interstitial fluid collect in the lymph nodes and can persist there for many weeks. They continue to produce spike protein during this time. Remember that vaccines are intended to be given in an intra-muscular manner, meaning that they are intended to be injected to a muscle and stay there. This paper shows that they are able to migrate to the lymph nodes.
The paper does not discuss the medical importance for this in terms of adverse events. Given the relative rarity of adverse events, I would guess that the presence of vaccine mRNA does not produce adverse events, and that these events are caused by vaccine injection into a vein. Again, the data is not conclusive on this, so this is just my guess at this point.
mRNA technology note: At this point, I have no evidence to suggest that the problem with the new vaccines is the mRNA technology. In my estimation, the likely reason the new vaccines lead to adverse events is that they produce the SARS-2 Spike protein which likely causes inflammation throughout the body. This may only be in vaccine recipients who receive a vaccination in a vein rather than an intra-muscular injection. If you choose to get a vaccination or booster, ask the health care provider to aspirate before injection.
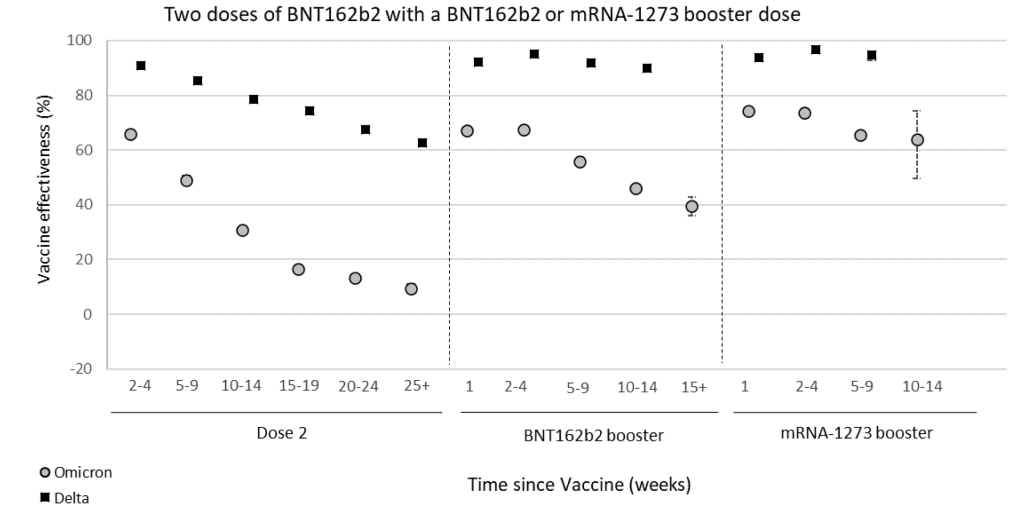
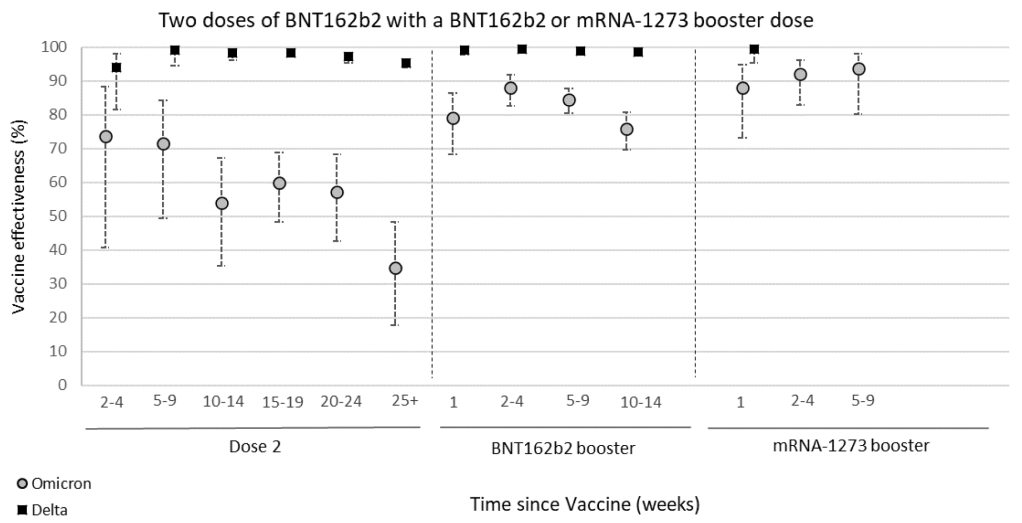
Certain vaccinated individuals are more likely to be infected by Omicron than the unvaccinated: A UK surveillance report shows that vaccine effectiveness against symptomatic Omicron infection goes from around 65% effective soon after 2 doses of vaccine, to around 5% 6 months later. Protection from hospitalization goes down to just 35% after 6 months. These findings suggest that to maintain full protection against Omicron, a vaccinated person will need to get a booster every 3 to 6 months.
From UK Surveillance Report, March 17, 2022, Table 1b. Effectiveness of Pfizer vaccine at preventing symptomatic COVID infection after 2 doses, and after a Pfizer or Moderna booster.From UK Surveillance Report, March 17, 2022, Table 2b. Effectiveness of Pfizer vaccine at preventing hospitalization after 2 doses, and after a Pfizer or Moderna booster.
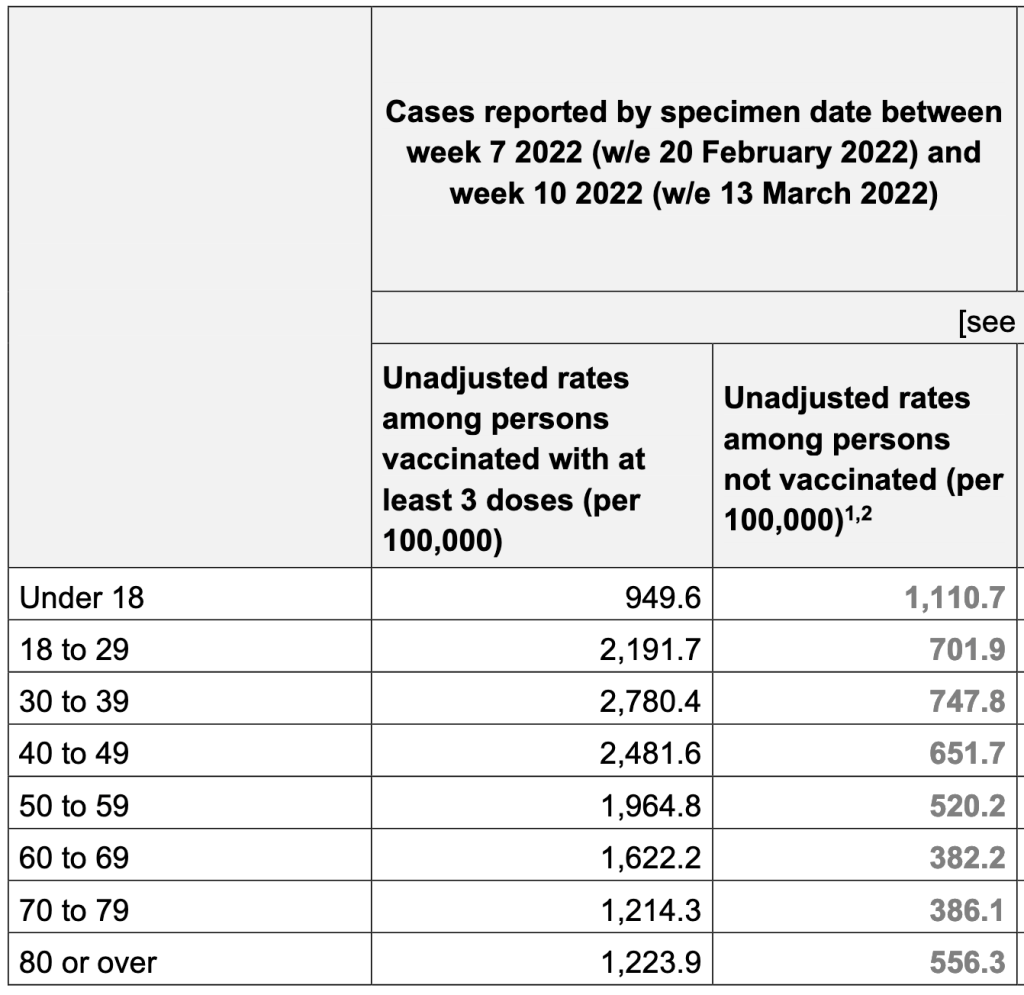
In another finding from the report, people with 3 doses of vaccine are 3x more likely to be infected with Omicron than unvaccinated individuals. This is the clearest evidence yet that Omicron may be using Antibody Dependent Enhancement (ADE) to infect people. The Lewnard et al paper from a few months ago has a similar finding. For both studies, a certain number of vaccine doses are more likely to increase the chance of infection. If viruses are using the ADE pathway, this effect would be explained more by the timing than by the number of doses per se. For ADE to work, a person needs to have a mediocre immune response to an agent, not a strong or weak one. Since we know vaccine mediated immunity goes down over time, then a person becomes more likely to be reinfected as their immune response goes from strong to mediocre.
From UK Surveillance Report, March 17, 2022, Table 13. New case rates among UK residents with at least 3 doses of vaccine, and with no vaccination. Numbers are normalized for the percentage of people in each group.
So should you get a booster? Again, if you have risk factors like age, obesity or respiratory problems, you might want to get a booster every 3 – 6 months. Otherwise, you may choose instead to just take extra precautions as Omicron cases continue to fall in the US. If you choose to get a booster, ask them to aspirate before injection. Talk to your doctor when making medical decisions.
I know this is all very complicated. Your questions will help me make this more clear.
Here’s a brief case update. I’ll also have a brief comment about vaccine mandates.
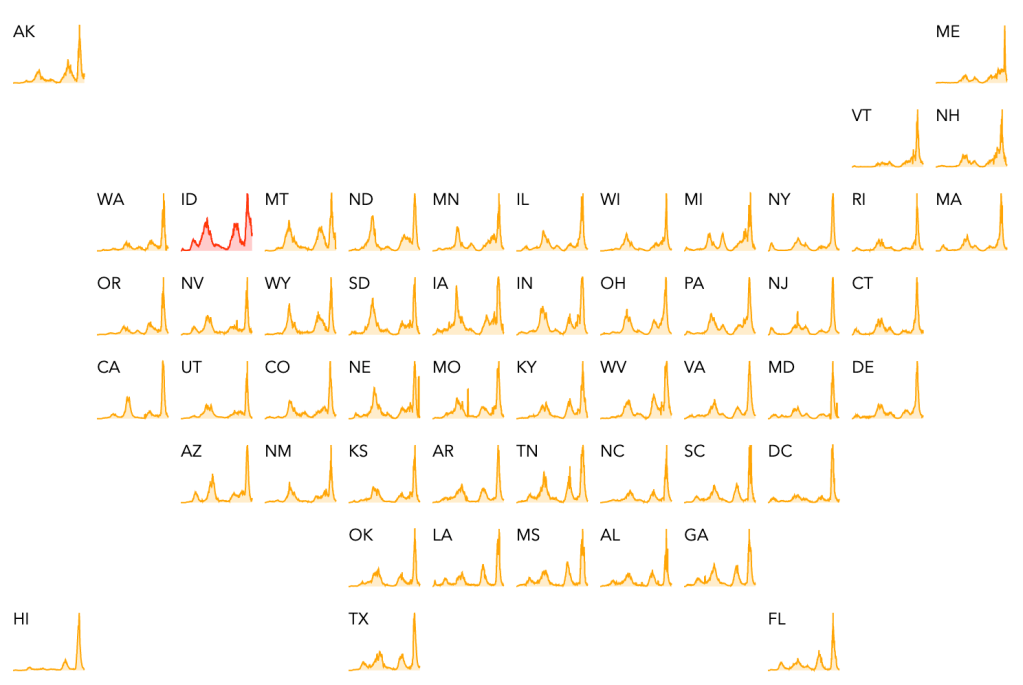
Cases continue to come down in the US, California and San Diego County. Cases in the US are now approaching being as low as they were in the Spring before Delta started. The only current outbreaks, according to endcoronavirus, is in the Twin Falls area in Idaho. Cases are dropping in San Diego County too, but unfortunately, not as fast as other places. LA and San Diego Counties are now #1 and #2 for new case numbers in the US.
World wide, the US is now in 8th place for countries with the most new COVID cases in the last month. This is a welcome change, since the US has spent large majority of the pandemic in 1st place. Ironically, the country in first place right now is South Korea, which has been doing well for the majority of the pandemic, serving as an example for other countries to follow. The majority of cases country wide have happened in the last month, due to the super infectious but less virulent Omicron variant.
Vaccine mandates still enforced: In January 2022, the Supreme Court struck down the vaccine and testing mandate for all but a few health care workers. Mandates for federal workers are still working their way through the courts. In spite of this, some companies and municipalities are still enforcing the mandates. They often cite vaccine mandates, but the vaccine mandates still do not officially exist, having been struck down. So these entities are enforcing mandates entirely on a voluntary basis, and of their own volition. These entities do not acknowledge the now well known data that natural immunity is better than vaccine mediated immunity at preventing infection and the spread of SARS-2.
As you may have noticed, I’ve been tapering off the frequency of my updates as the pandemic recedes. As things continue to improve, I will post more infrequently.