This post will be a very personal reflection of my personal mindset right now. I am not necessarily recommending this point of view to everyone, but some Christians in particular may find it helpful, at least in principle. Non-Christians may find it hard to relate to. I get it. You may choose to skip this post, or you can read on to understand how some Christians think about these topics.
What is our role?
As some may guess, I have struggled for many years, and especially during my cancer journey, on the topic of our role in our own affairs, versus the role God has in our lives. God is keenly interested in our lives and is intimately involved in our life events and our development. Despite His role, I believe strongly that we are not to simply incubate in life and let God do stuff to us, but that we also take an active role in our lives as well. Clearly, God commands certain things from His people (Jew and Christian alike) and we are responsible for our behavior. The book of Proverbs commands us to use wisdom in our daily lives and assures us that wisdom will lead to better outcomes and foolishness will lead to destruction.
So the question is, what is our role, and what is God’s role? How much of our lives are determined by what we do and how much is determined by what God does? I’ll lay the second question aside, since it’s more academic that the first. The first question helps us know how we should view decision making in our daily lives.
As a Type-A person, I have a strong tendency to want to control all the events of my life and have a general belief that I personally need to solve all of my problems. As a generally competent person, I usually am in fact able to solve my own problems, using my own resources. Many of you are smart, competent people who operate the same way. Of course, in many people, this can lead to a destructive arrogance that can actually come to derail life instead of helping things along. I have certainly fallen prey to this many times myself.
At the same time, the Bible encourages us to be wise, it also frequently commands us to trust in God.
“Trust in the LORD with all your heart and lean not on your own understanding; in all your ways submit to him, and he will make your paths straight.” Proverbs 3:5-6
“Trust in the LORD and do good; dwell in the land and enjoy safe pasture.” Psalm 37:3
“Be anxious for nothing, but in everything with prayer and supplication with thanksgiving make your requests be known to God. And the peace that passes understanding will guard your hearts and minds in Christ Jesus.” Philippians 4:6-7
“May the God of hope fill you with all joy and peace as you trust in him, so that you may overflow with hope by the power of the Holy Spirit.” Romans 15:13
100:100
There is a balance. We have a part and God has a part, a much bigger part. So what’s the division? How much do we do and how much does God do? In my life, I see this as a 100:100 proposition. We should do everything we can to produce the outcome we want, always of course using God’s commands and wisdom as a guide. On the other hand, we trust in God to do 100% on our behalf. He can do many more things than we can, and we can trust Him to guide us.
Here’s a great illustration of this from the Bible. Twice, Jesus feeds large crowds using a small meal provided by one person. In John 6, Jesus is preaching to a large crowd and they become hungry. So the disciples start panicking about feeding all of them. A small boy has a lunch with him, 5 pieces of bread and 2 small fish. Jesus takes the bread and the fish and feeds at least 5000 people with it, maybe many more. How much of the lunch does the boy donate? 100% of the lunch. How many of the people does Jesus feed with the lunch? At least 99.98%, so basically 100%. So the boy does everything he can to help, which isn’t much, and Jesus multiplies his contribution to feed everyone else. 100:100.
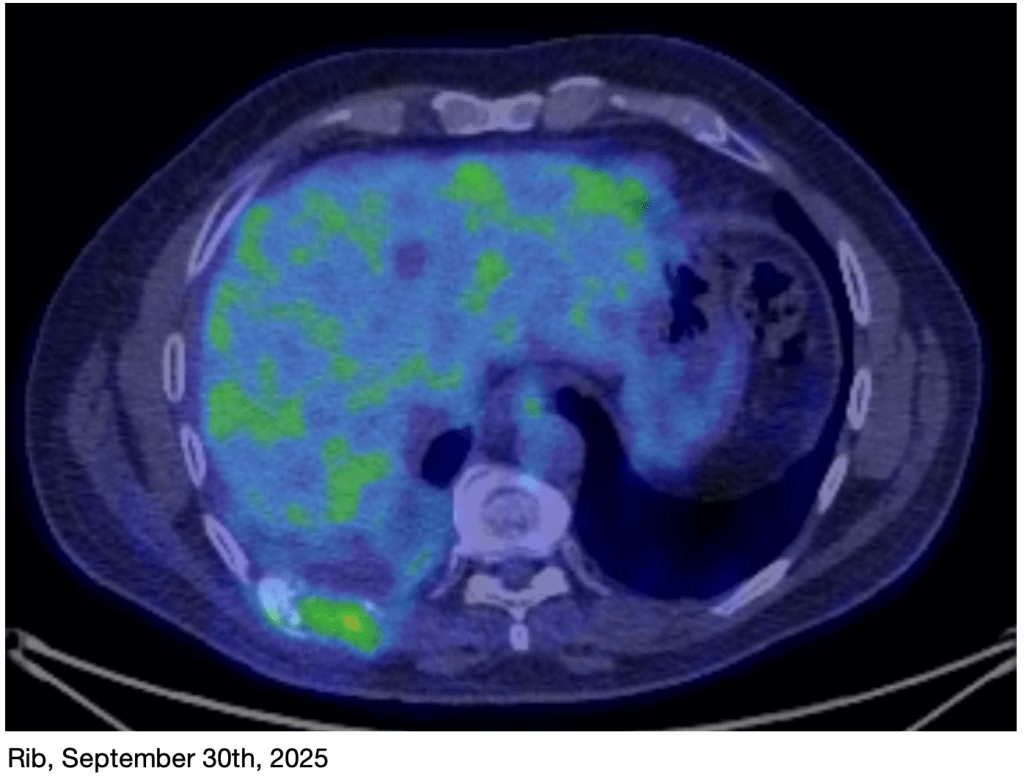
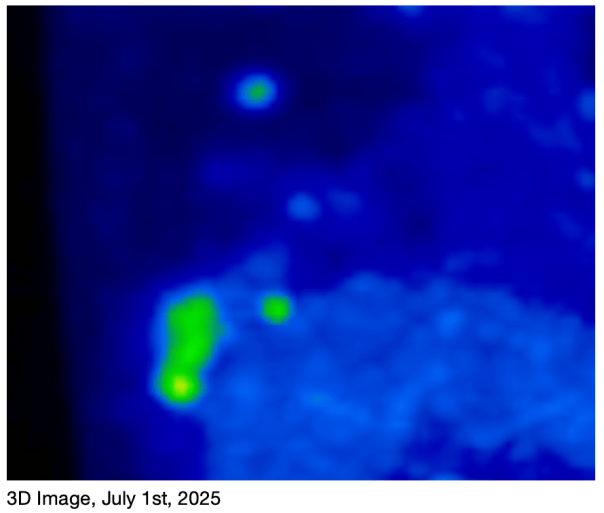
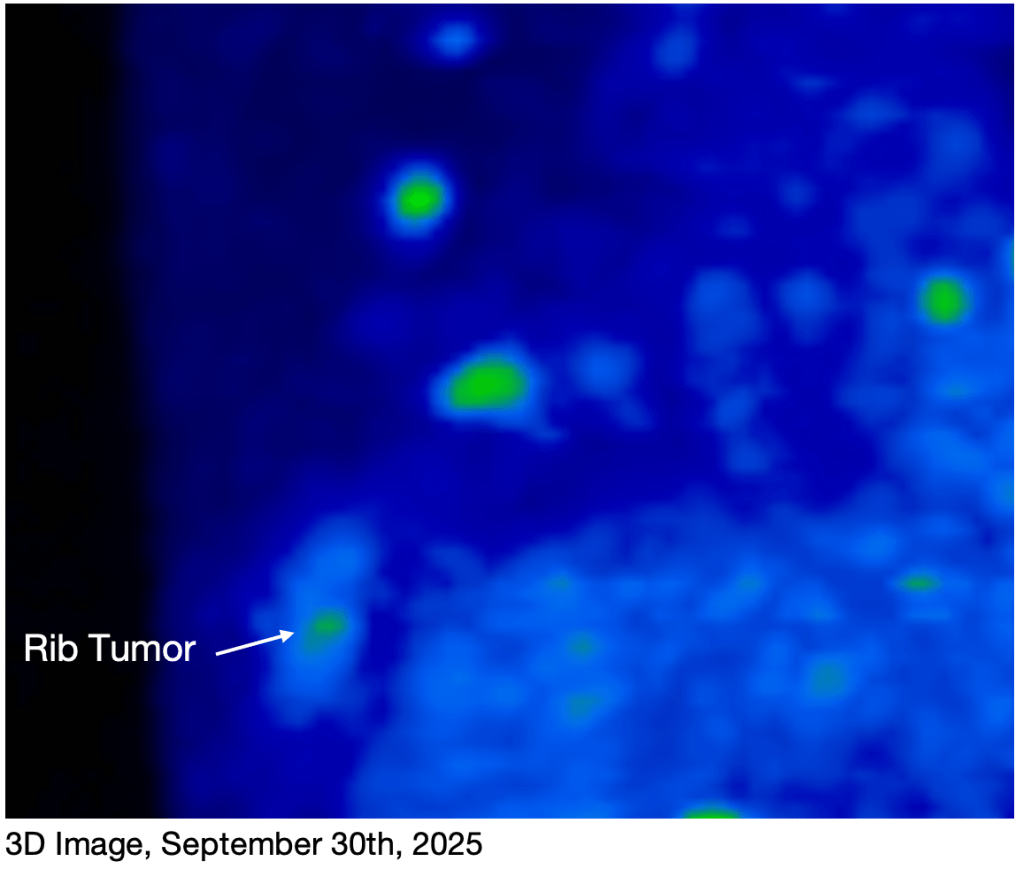
My approach to cancer has been to do everything I can to contribute to my healing. I’m obeying all my doctor’s orders, going through multiple rounds of chemo and radiation, and now doing multiple “extracurricular” treatments like Hyperbaric Oxygen, Red Light treatment, PEMF, intermittent fasting, focused supplementation, dietary restriction, walking, and physical therapy. I’m doing everything I can to contribute to my healing.
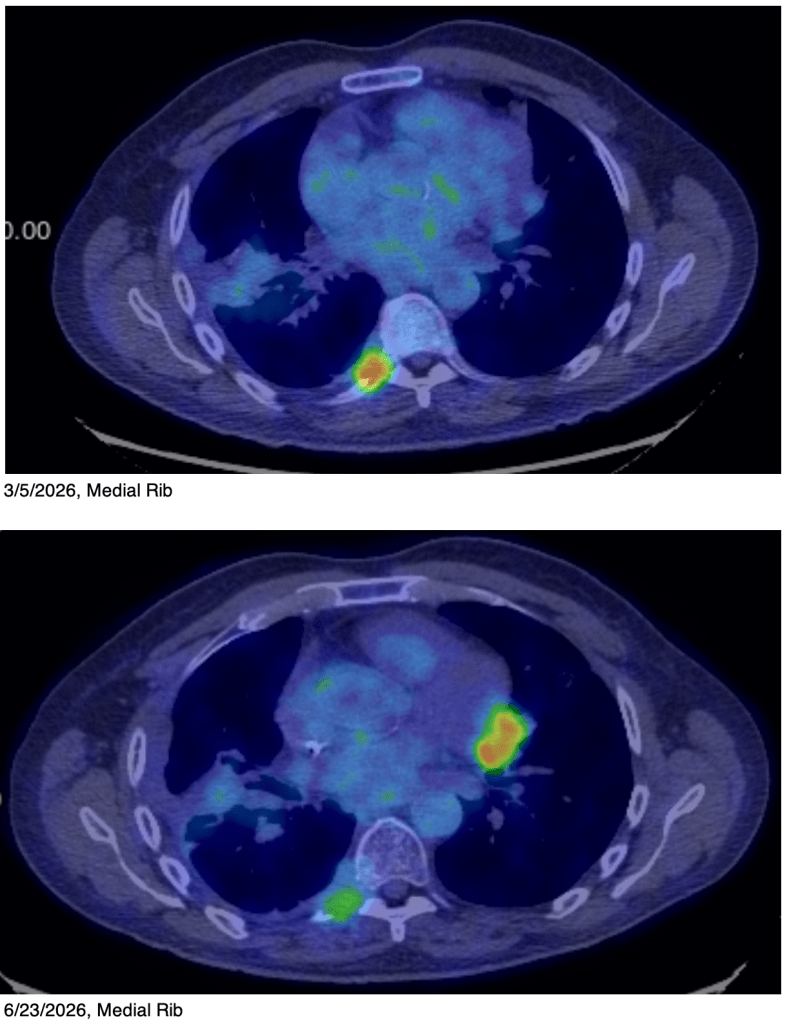
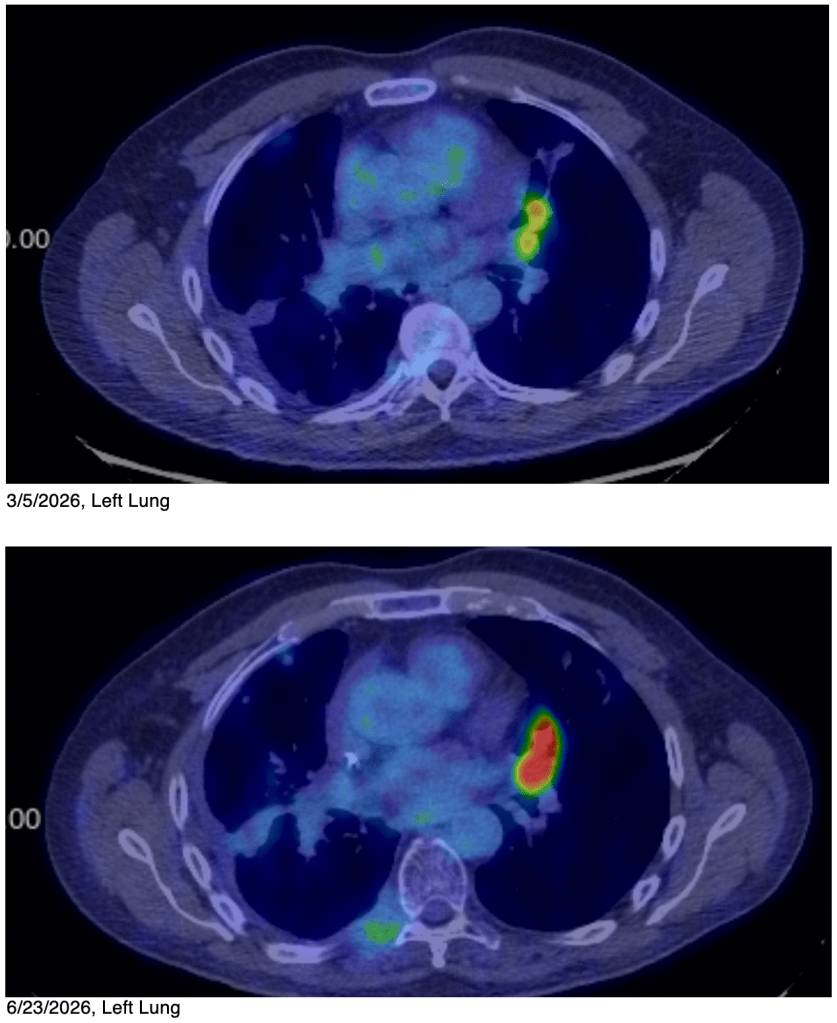
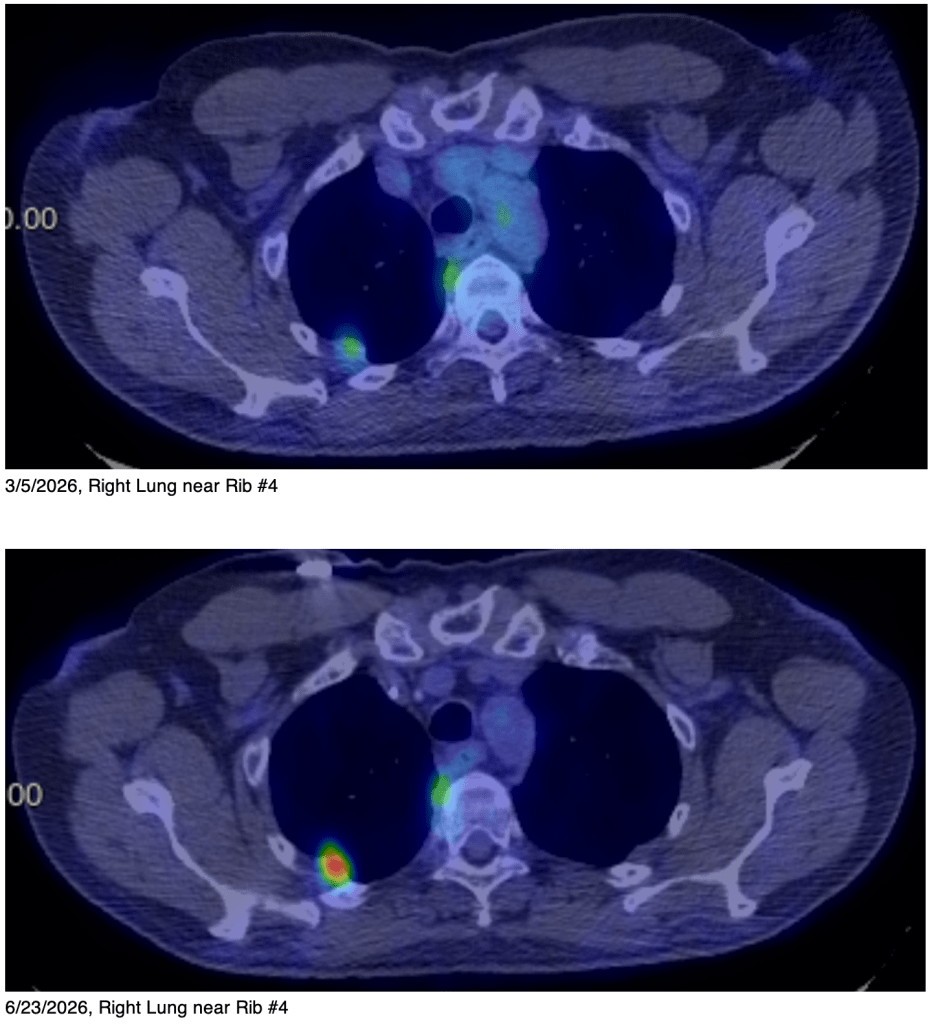
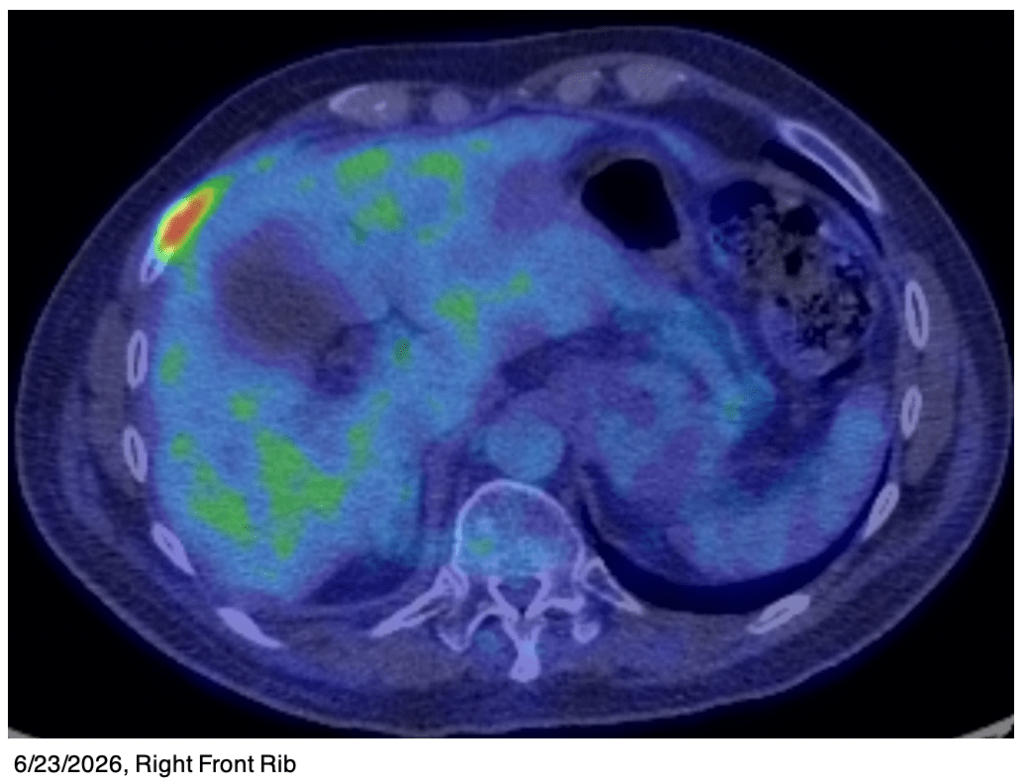
But as you read from my last blog, so far it hasn’t been enough. I will need God to make His mighty contribution. Thankfully for us, He has a mighty right arm, and uses it on our behalf.
Surrender
As I’ve mentioned before, I believe I will survive. However, I’ve had some more instruction on this recently. A few weeks ago, my chiropractor, a Christian who hears from the Lord, told me “Peace, healing, surrender for you. The less you resist, the less you will suffer.” This really took me aback, because I’ve been praying about everything a lot, and have you wonderful people praying for me a lot. I’ve also surrendered lots of things, given up many things, repented of many things, and tried to clear my life, body, mind, and even my house of bad influences so that I can be ready for whatever is next. So what else do I have to surrender?
Of course because I’m Type-A, I had to wring my hands about this for a few weeks. My chiropractor had offered a clarification, but I wasn’t taking notes, so I didn’t remember what she said. So just the other day, I texted her to see if she remembered what the clarification was. She texted back: “It was letting go of any and all expectations of what you want. Being truly in the present moment. Even though you heard God say you will live, letting go of that expectation.”
Yikes! He wants me to surrender my life! I was taken aback again. I’d certainly have to ponder this for a while too. But I prayed and indeed surrendered my life to Him.
No, this does not mean I’m giving up. I’m still going to fight hard and do all the things that will contribute to my healing. And I still believe I will survive. But I’m no longer going to focus on this outcome but just let it go. God is telling me that my mindset is not helping, but rather hindering my progress, so I need to let it go.
So in the future in these posts, I will no longer use the phrase “I believe I will survive” or even hint at that belief. As I said, I’m not giving up, I’m just clearing my head so that I can be ready for whatever God has for me. As I write this, this just happened yesterday. Ironically, over the last 24 hours, I have not been gripped with despair or with horrific visions of the grave. Rather, I’ve felt more relaxed, more freedom, and less responsibility for making sure I get the outcome I want. It’s in God’s hands now. Of course I invite you to keep praying for me, and for my attitude.
I have been focusing on trusting God for my healing. For many, this may be what they should do. But for me, right now, I need to give that up, forget about healing for the moment and focus on just letting God do whatever He wants. If you are in a difficult circumstance right now, pray and ask God how you should approach these things.
Imagine I’m a kid, in a car, on road trip. I’ve been asking “Are we there yet? Are we there yet? Are we there yet?” I think God is saying, “We’ll get there. But how about just enjoying my company? We can play some car games, look at the scenery, and just enjoy the ride!”
“Trust in the LORD with all your heart and lean not on your own understanding; in all your ways submit to him, and he will make your paths straight.” Proverbs 3:5-6
“Be anxious for nothing, but in everything with prayer and supplication with thanksgiving make your requests known to God. And the peace that passes understanding will guard your hearts and minds in Christ Jesus.” Philippians 4:6-7
Fear not, but be salt and light,
Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
You can read all of my cancer updates here.