This is a COVID update. Then I’ll discuss the high number of RSV and flu cases right now. I’ll also discuss the issue of vaccination induced blood clotting and the film “Died Suddenly”.
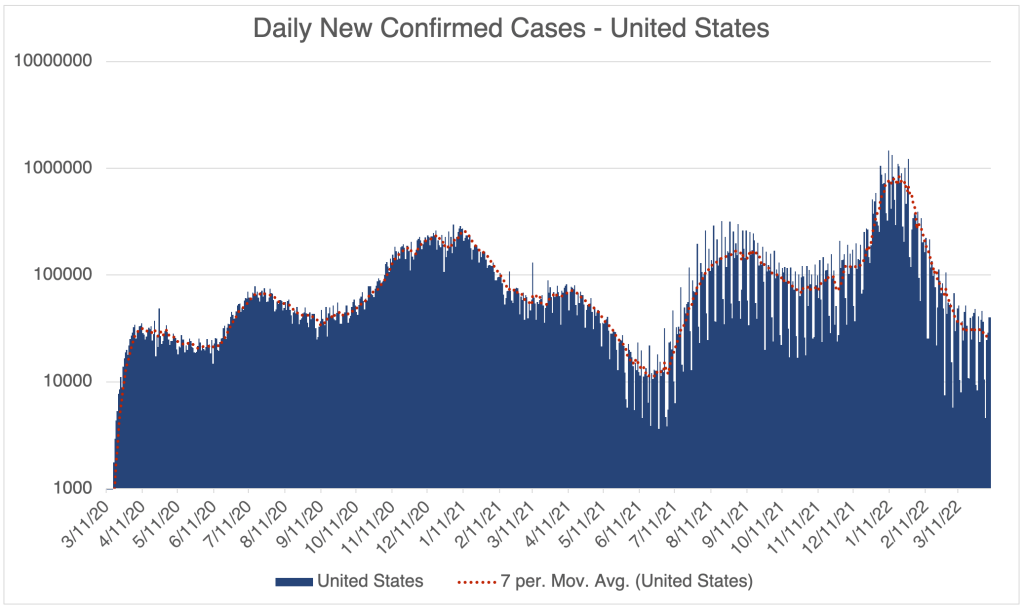
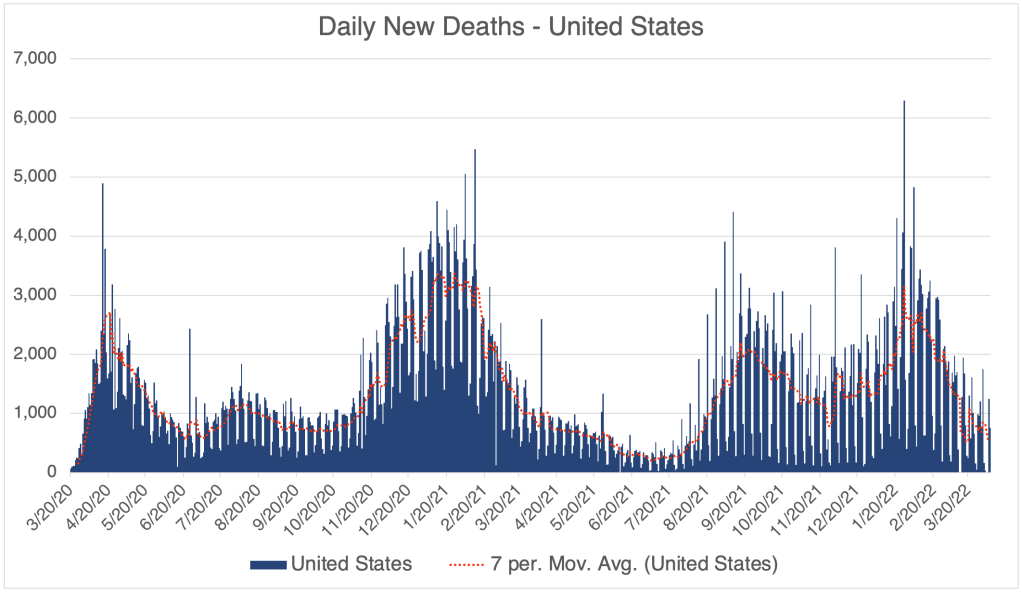
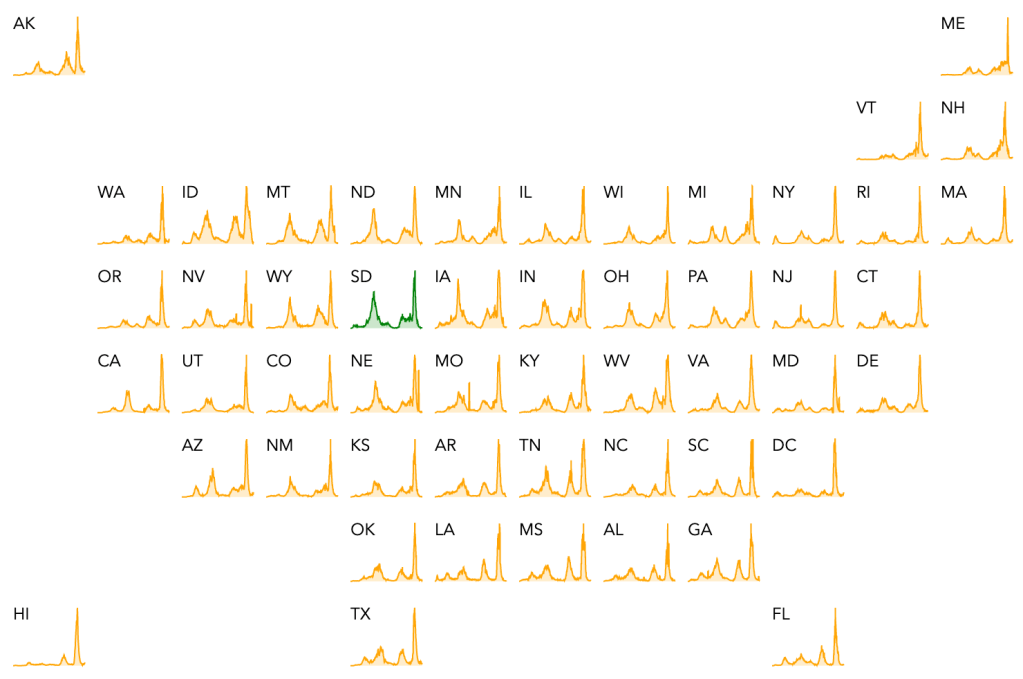
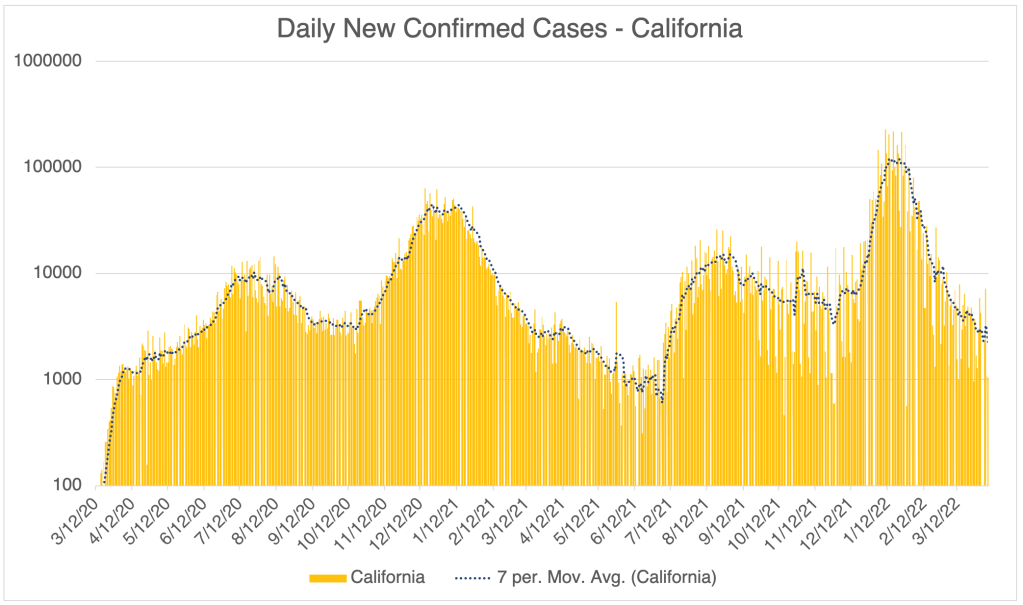
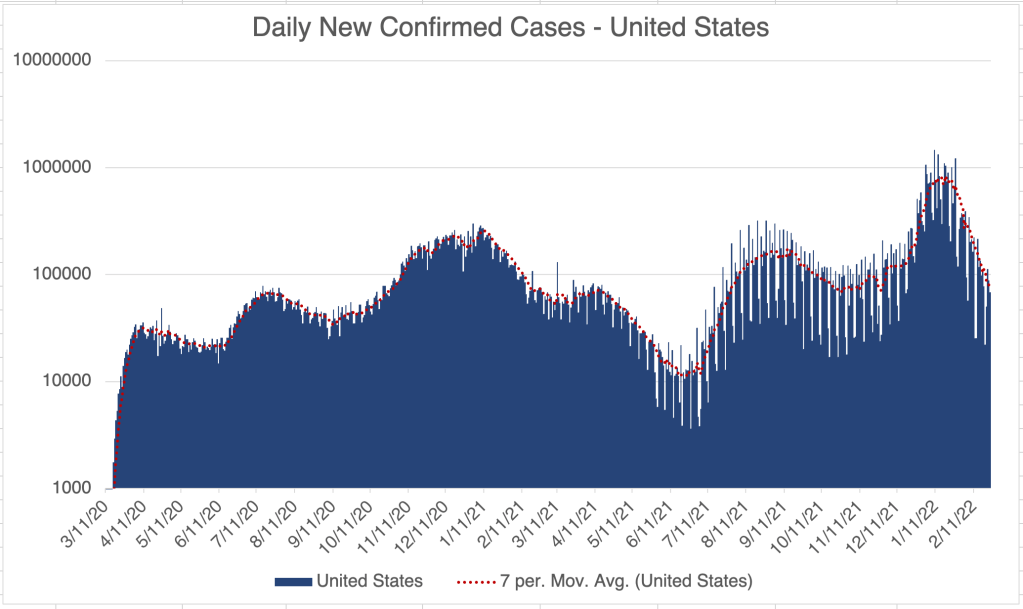
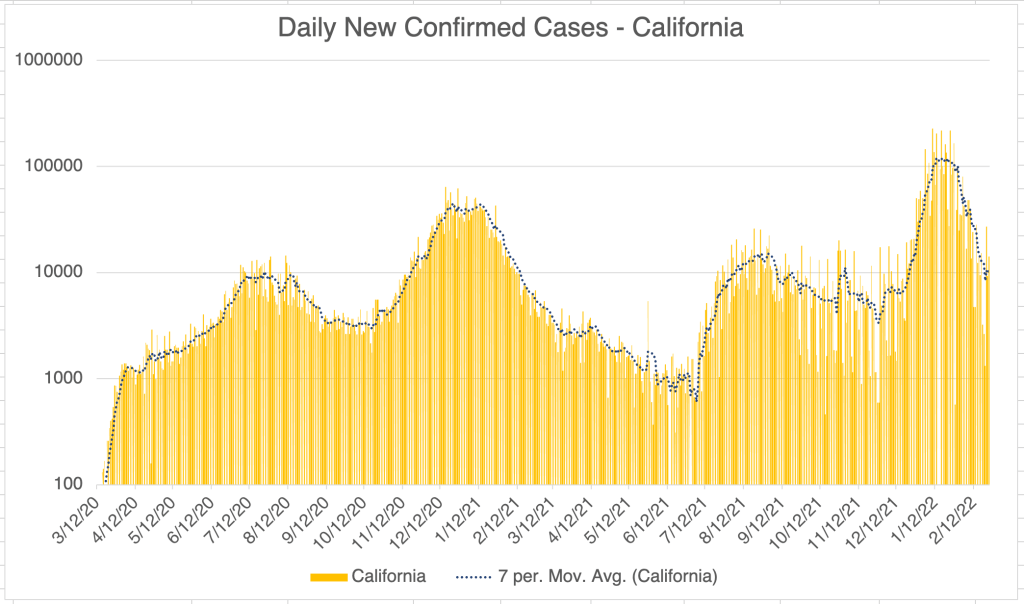
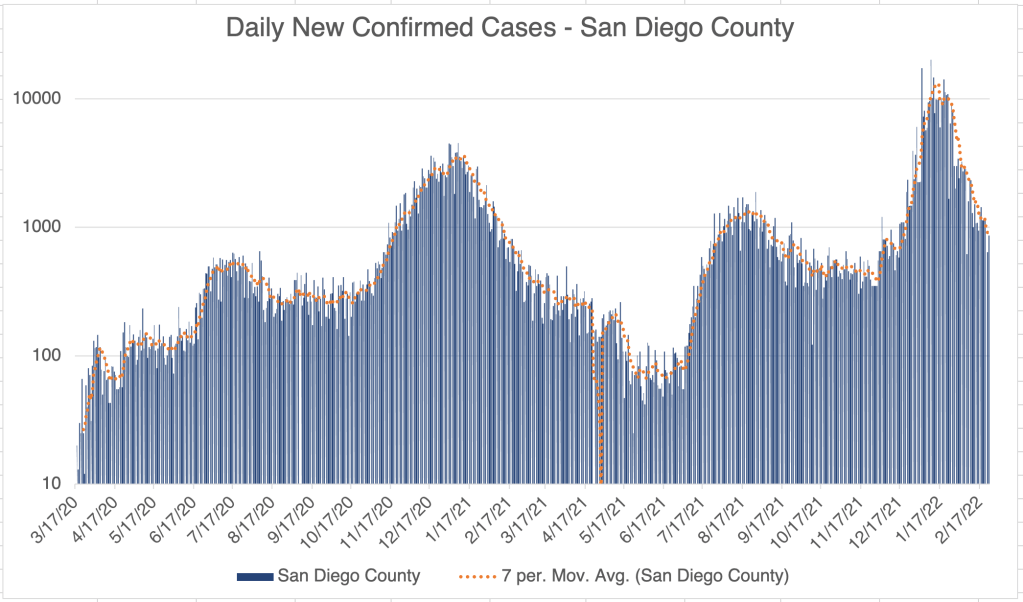
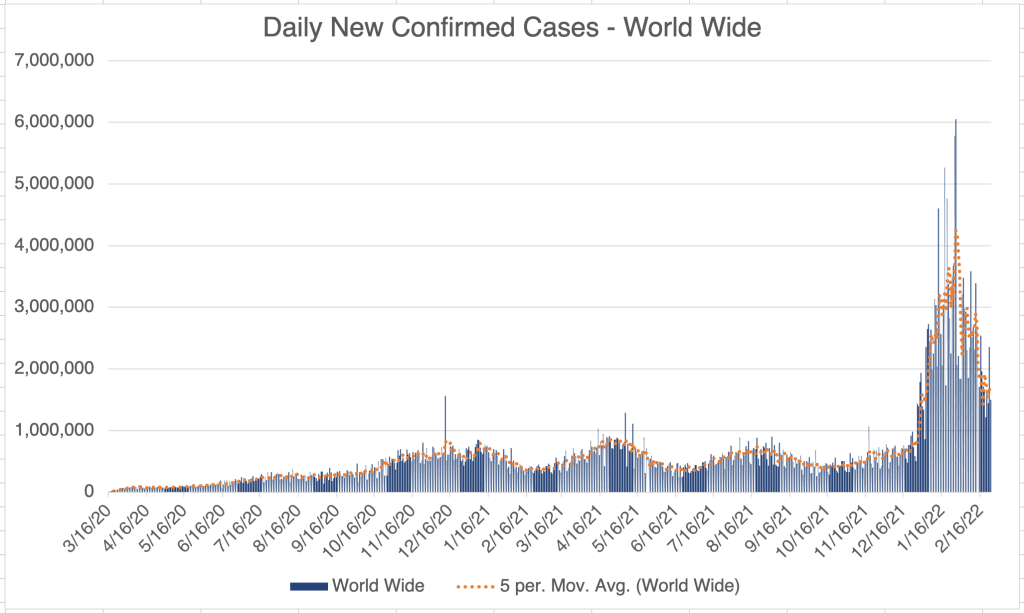
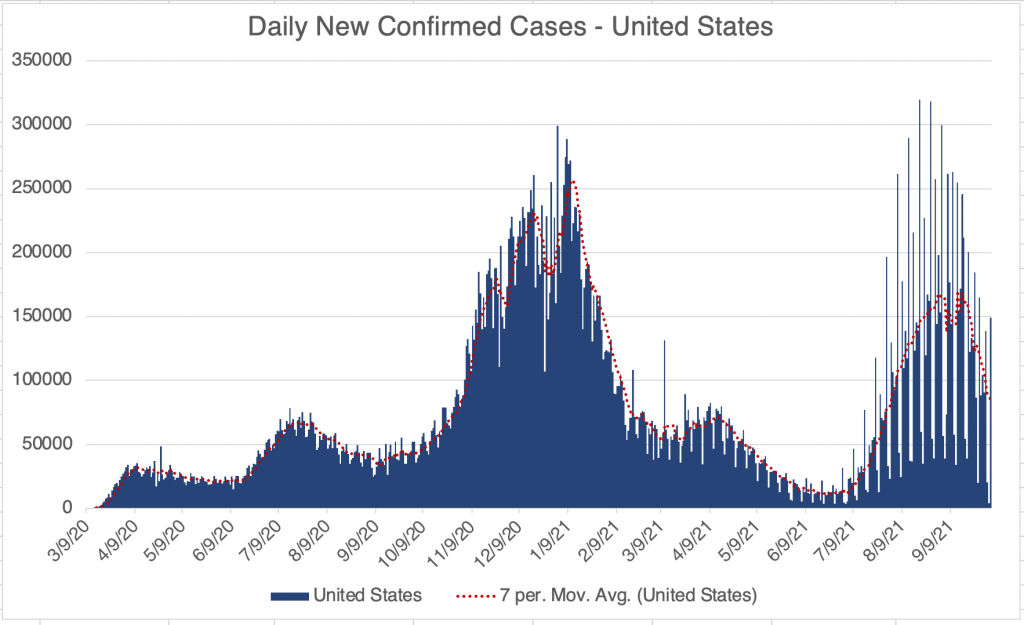
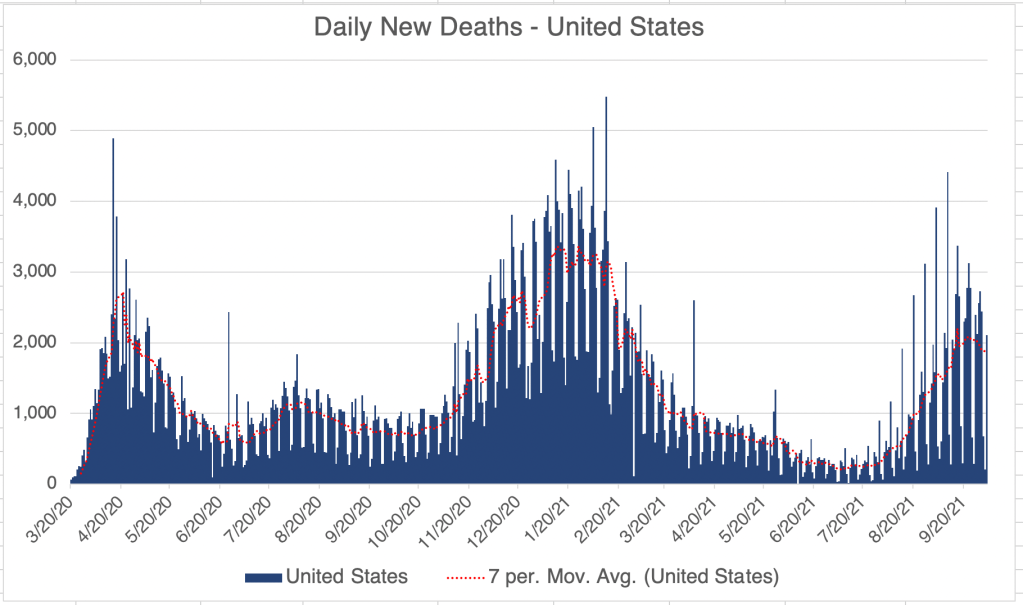
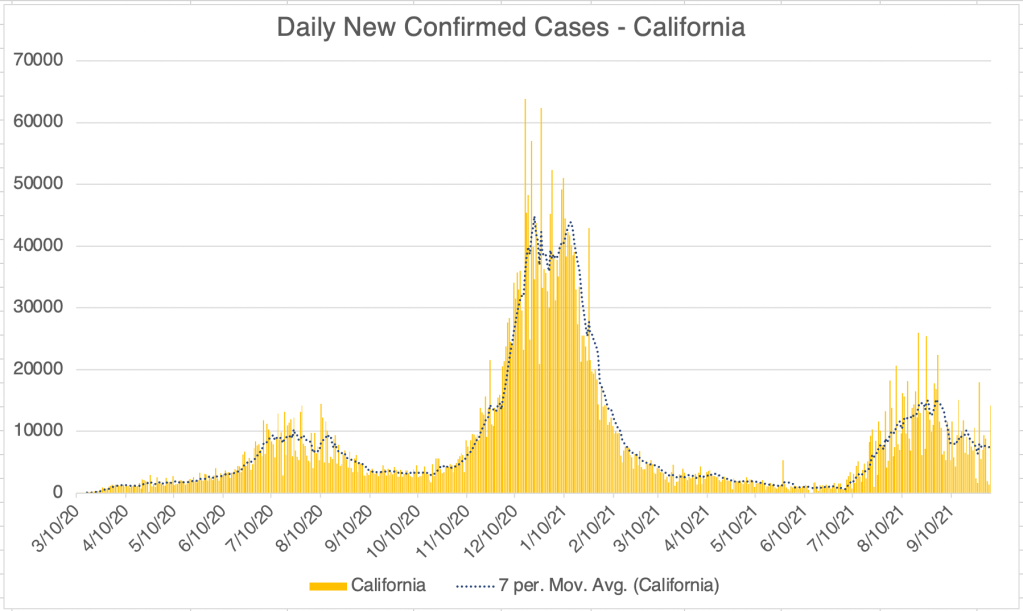
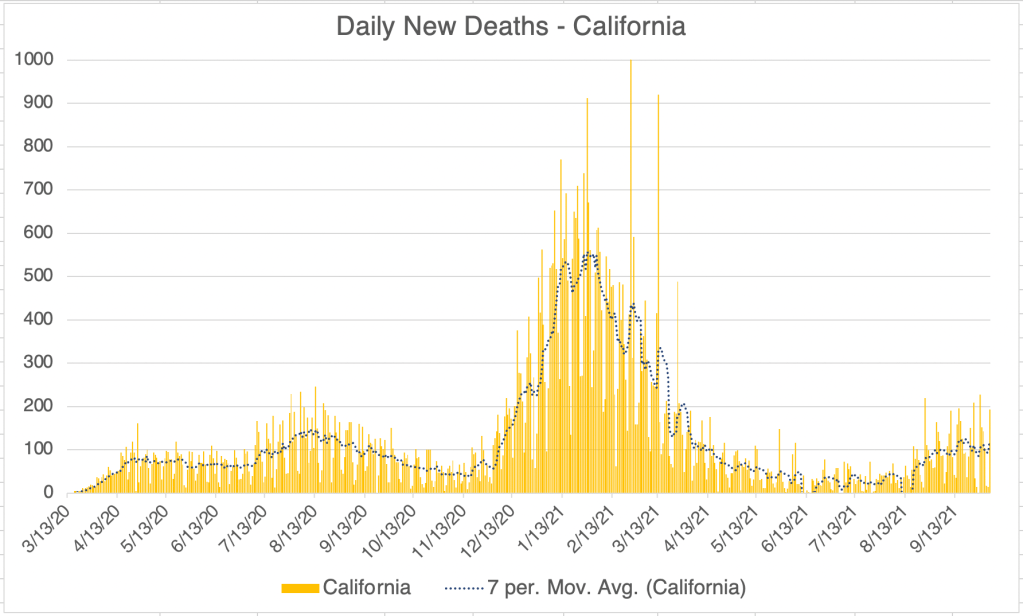
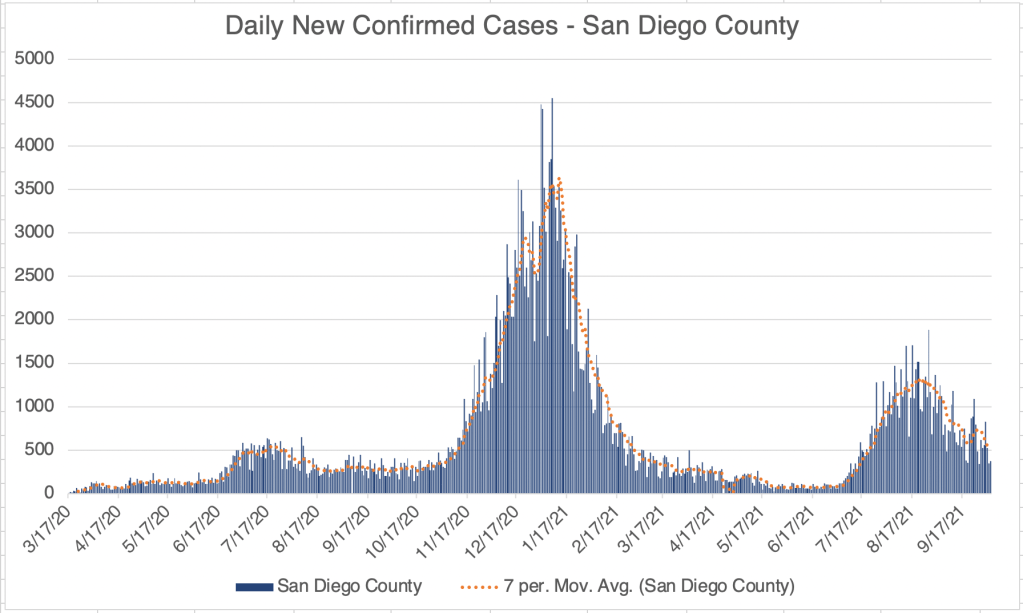
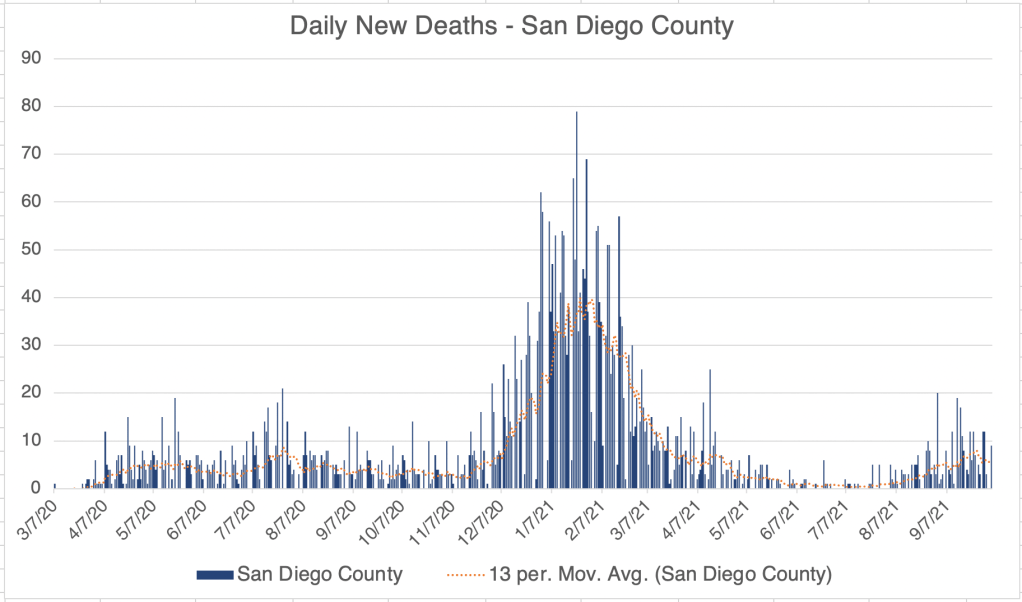
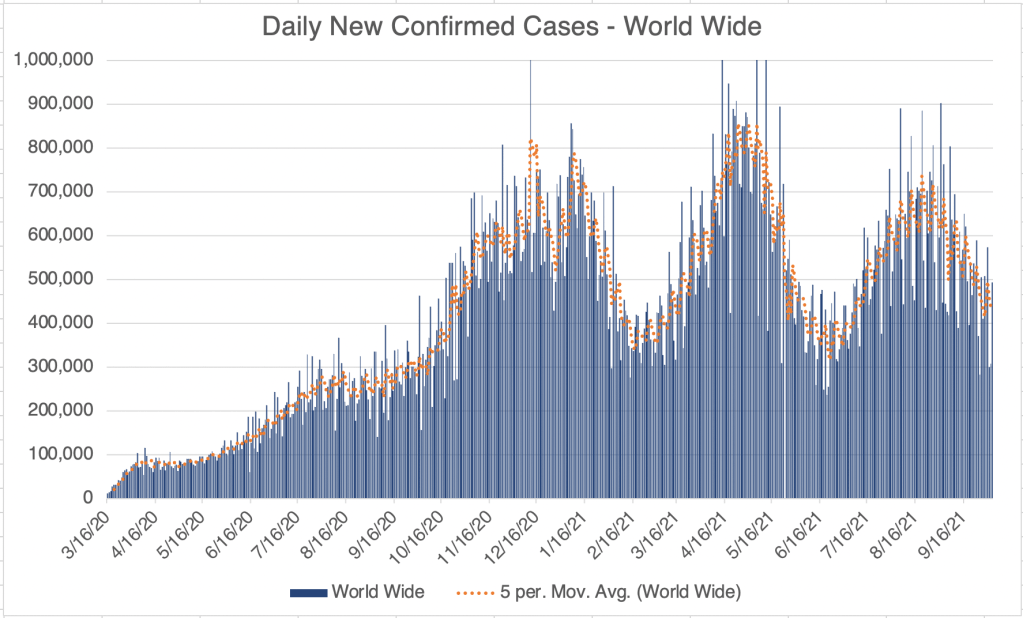
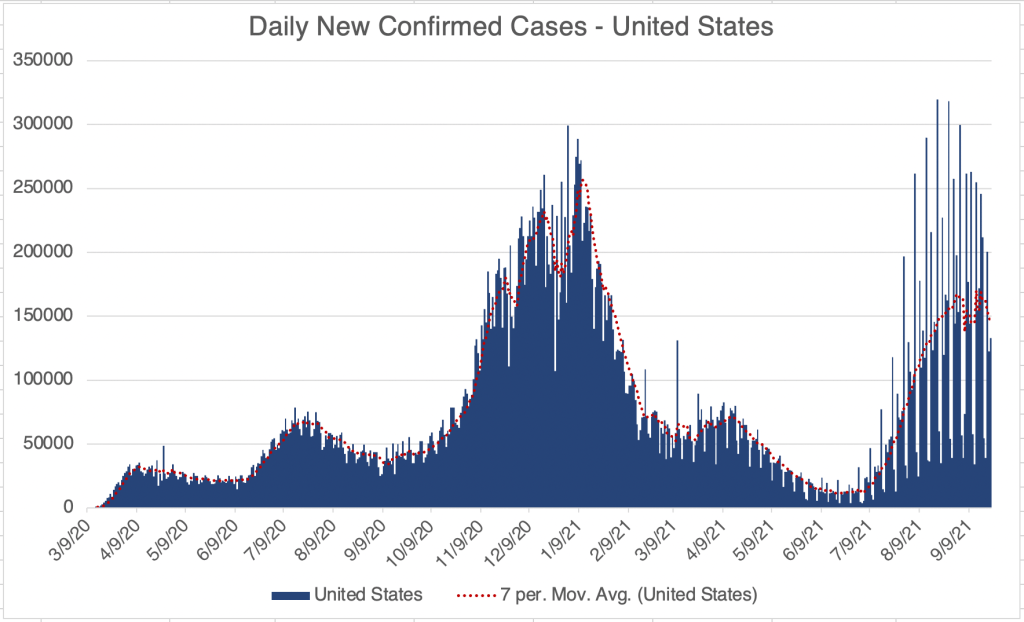
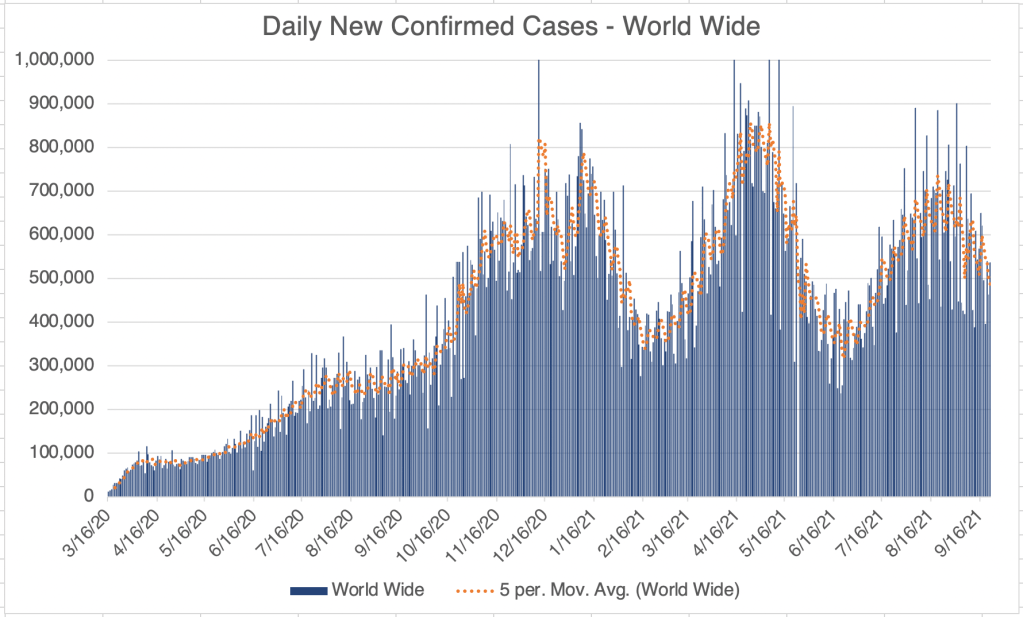
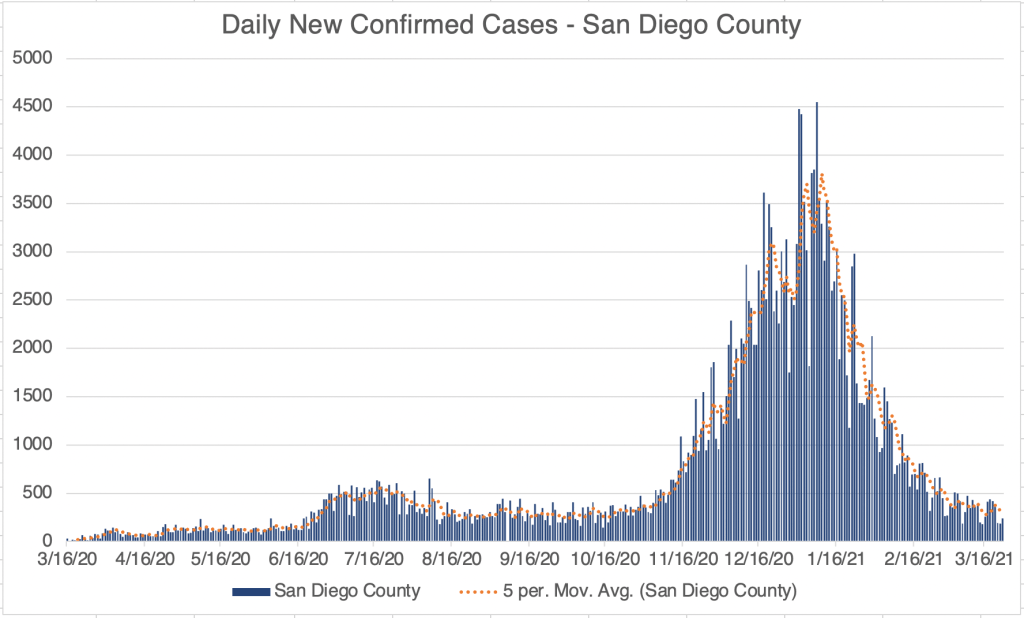
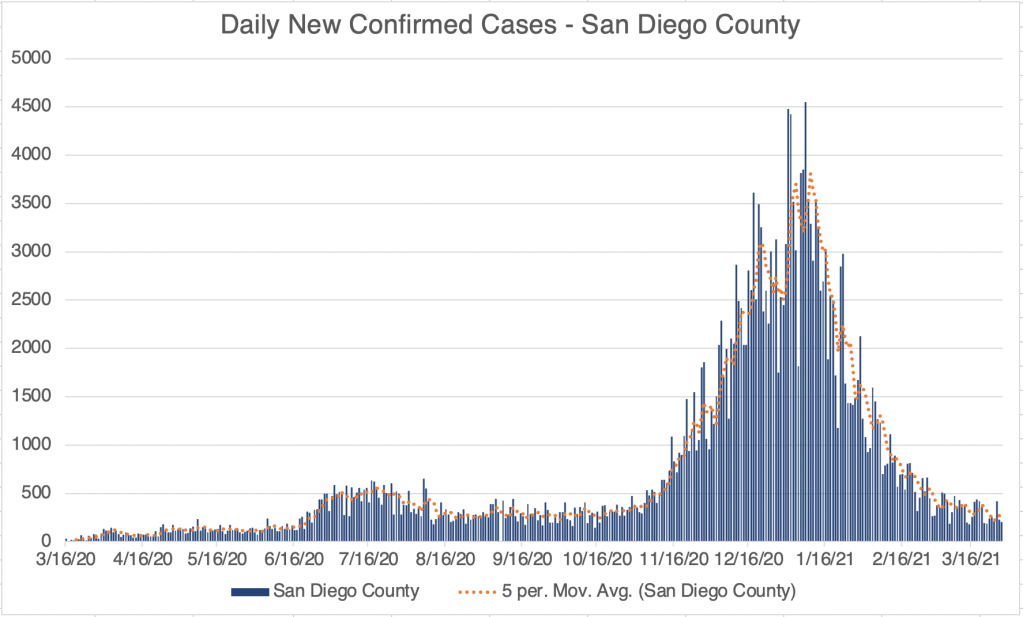
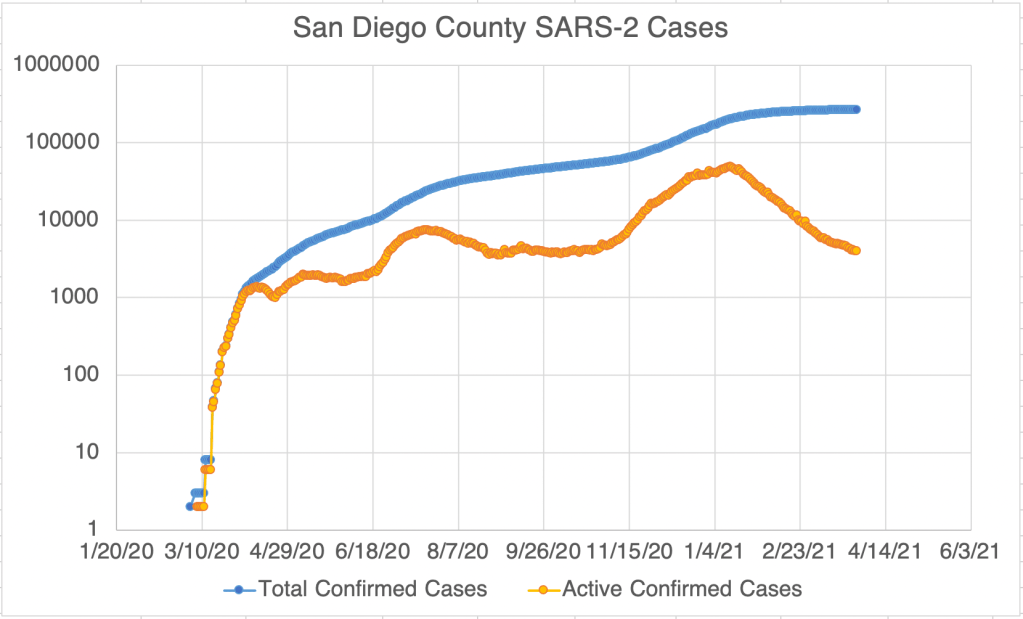
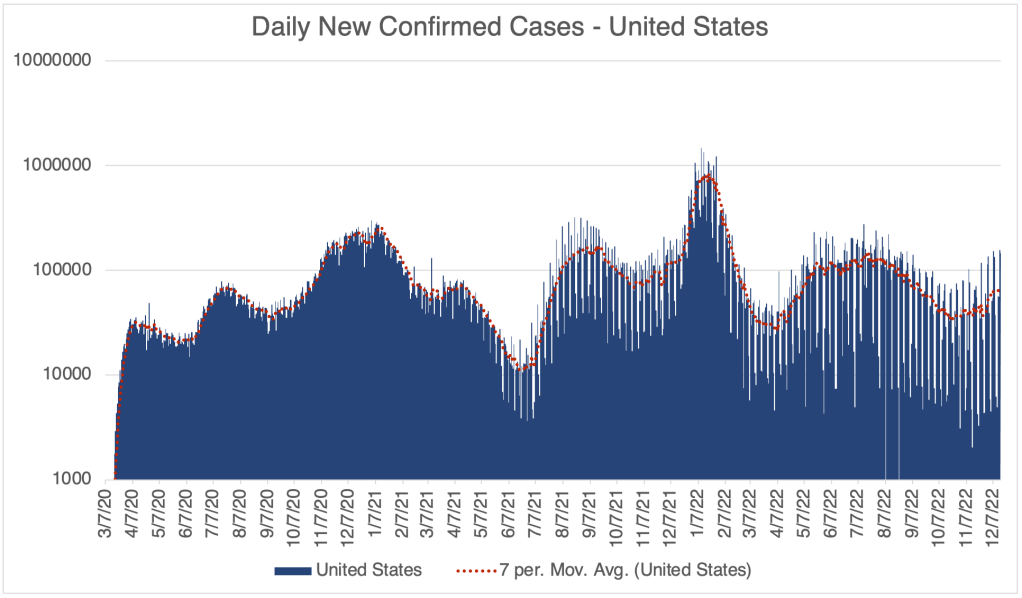
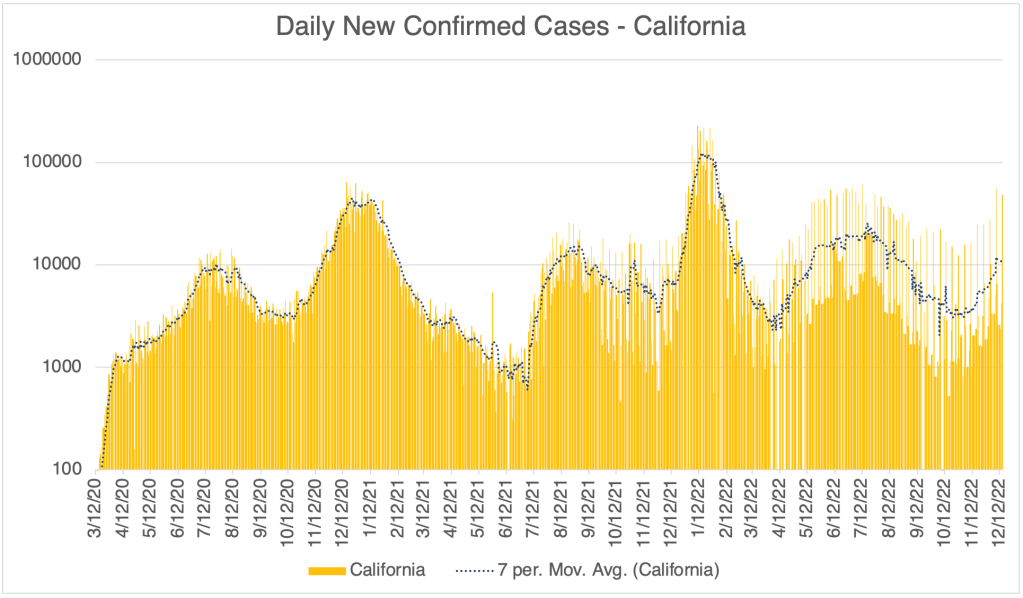
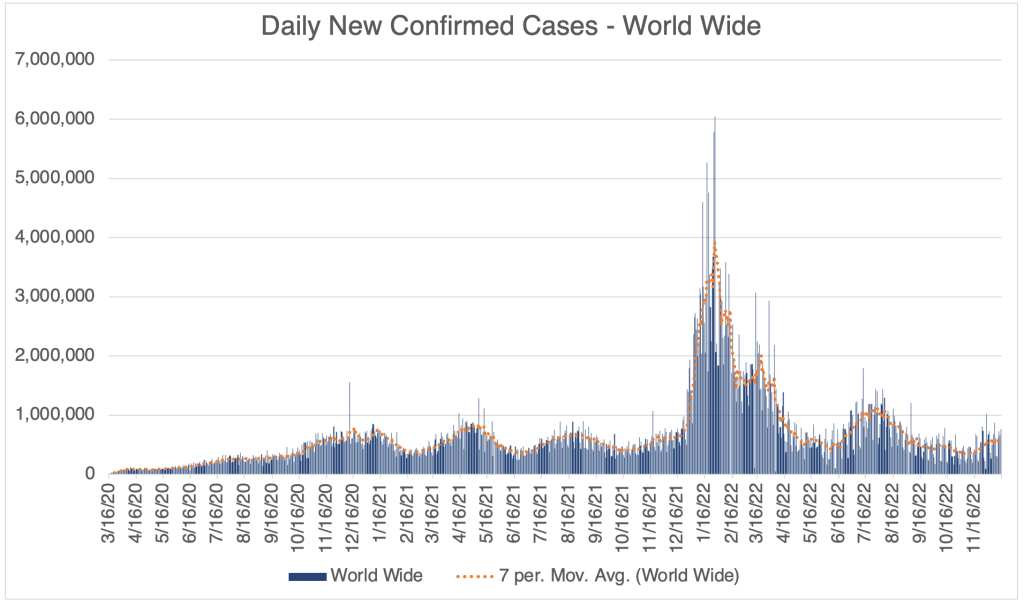
There has been a modest rise in cases in the past few weeks, suggesting that we will have a winter wave of cases. So far, this wave is not nearly as high as last December, when the Omicron variant first became dominant in the US. This is according to official testing data. Many are no longer being testing in a medical setting, so the number is likely much higher.
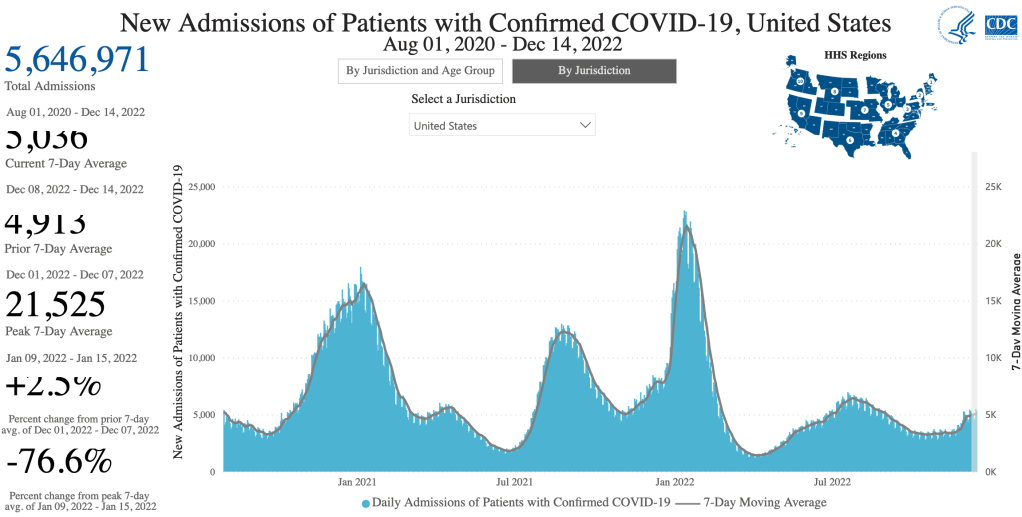
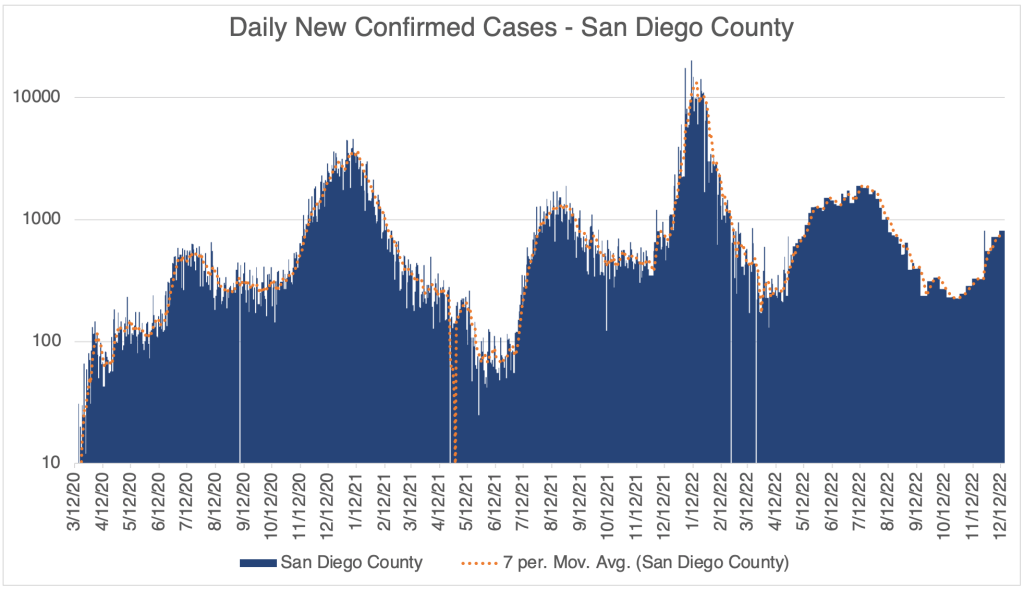
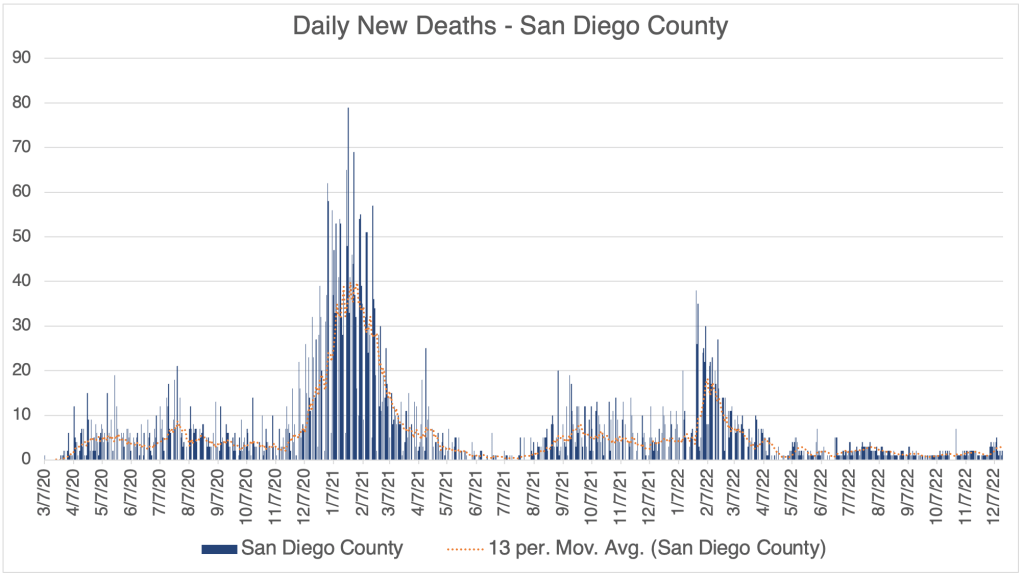
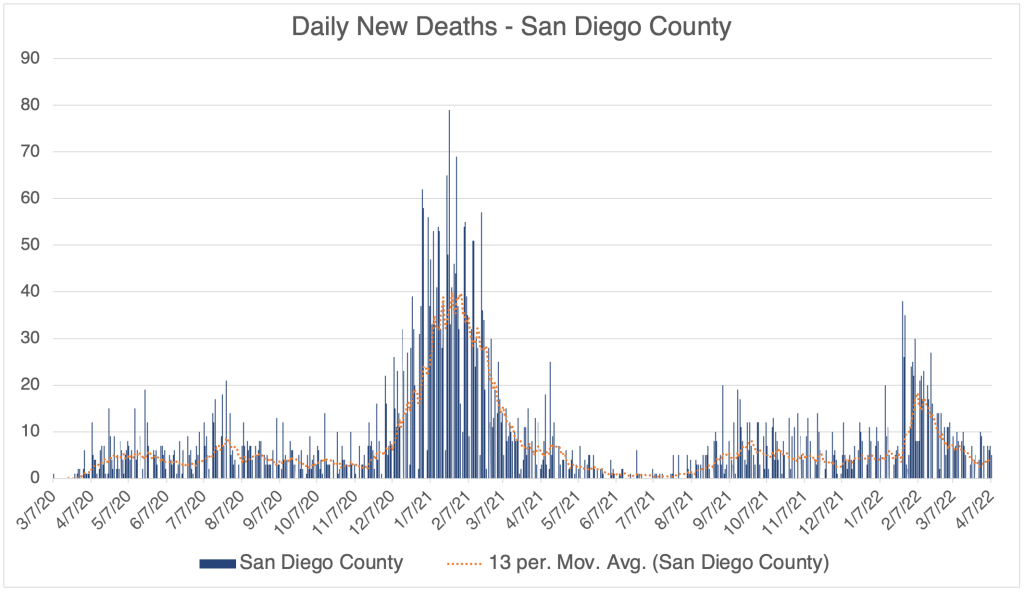
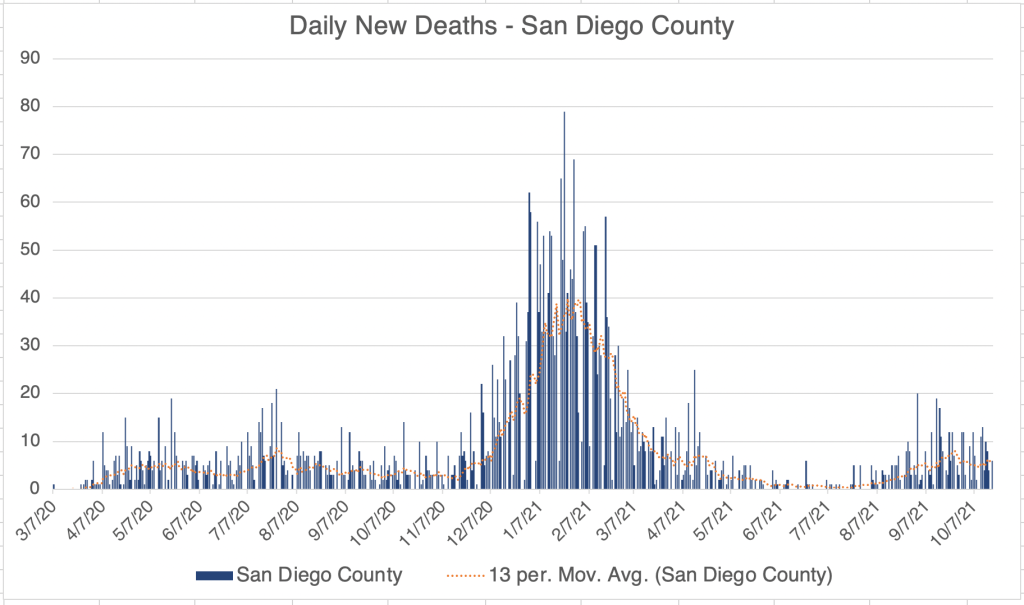
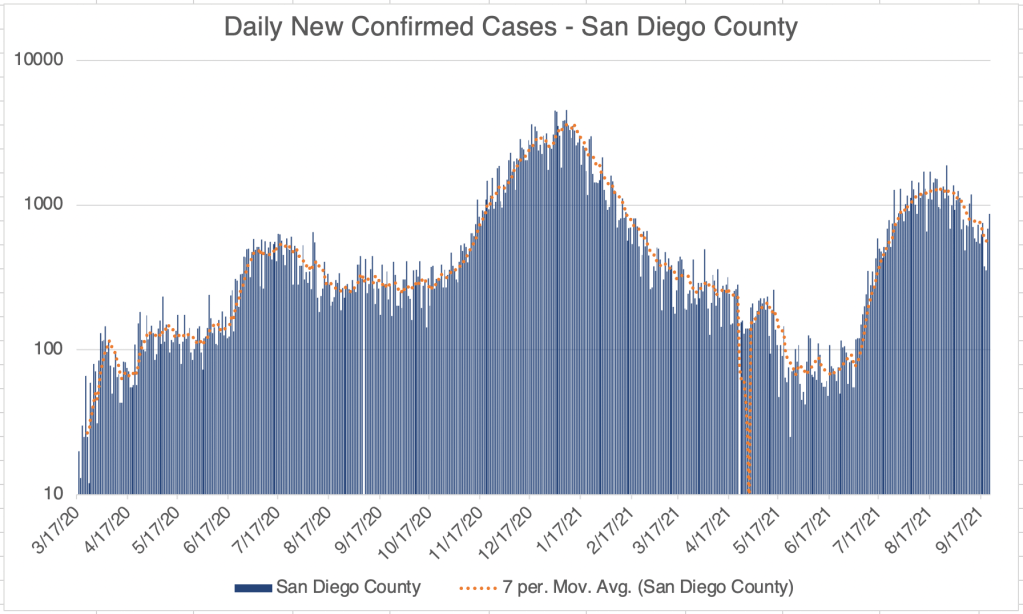
Hospitalization data provides a better relative view of cases, since it shows how many are actually entering the medical system with moderate to severe cases, but San Diego County is no longer providing this information on their website.
As we’ve discussed before, the drug store tests are not nearly as sensitive as a PCR test, and I know several people who were negative by this kind of test for days after symptoms began. The drug store tests can tell you if you have COVID, but false negatives are common, so if you get a negative result, it doesn’t mean much. If you really need to know if you have COVID, get a PCR test.
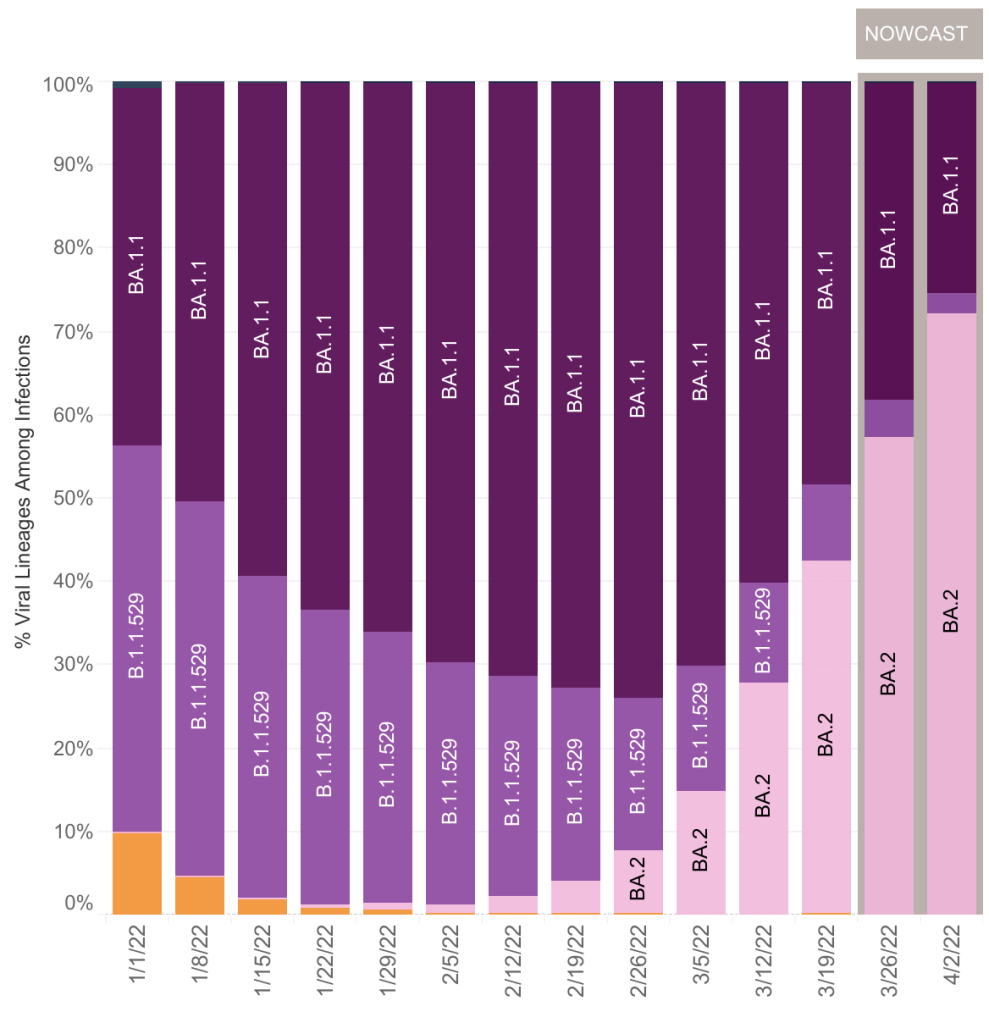
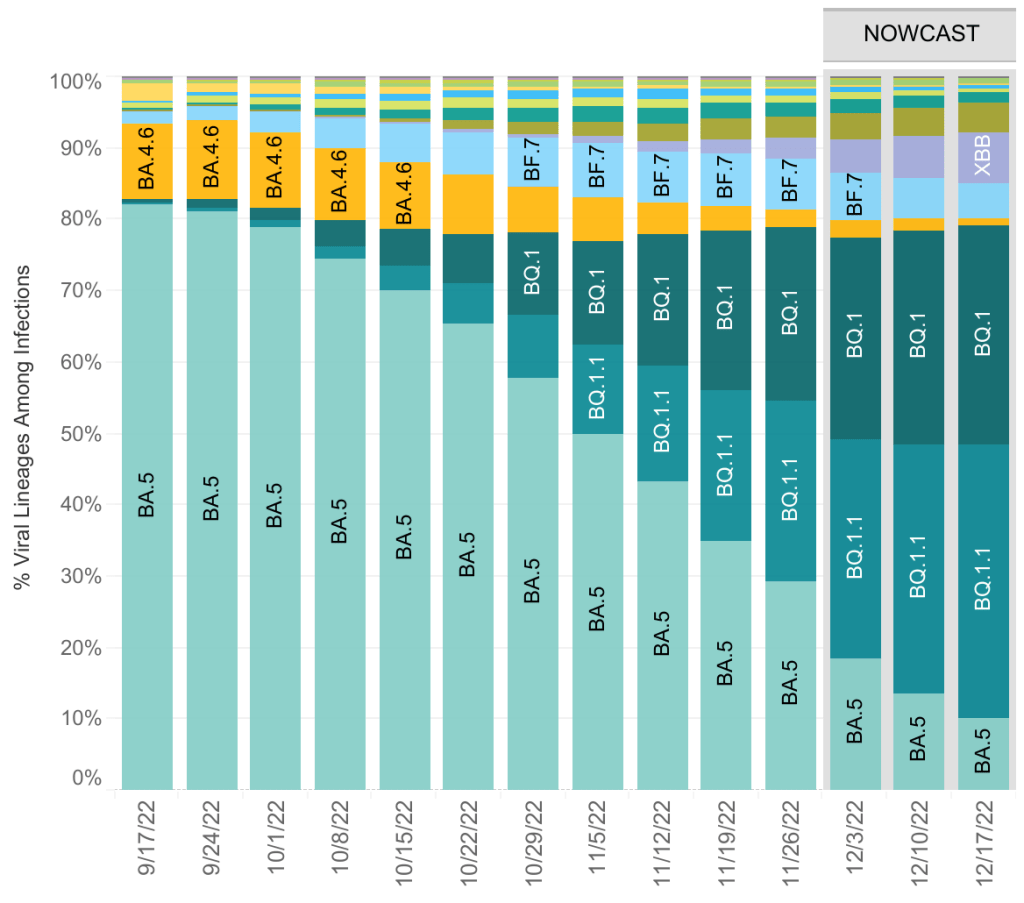
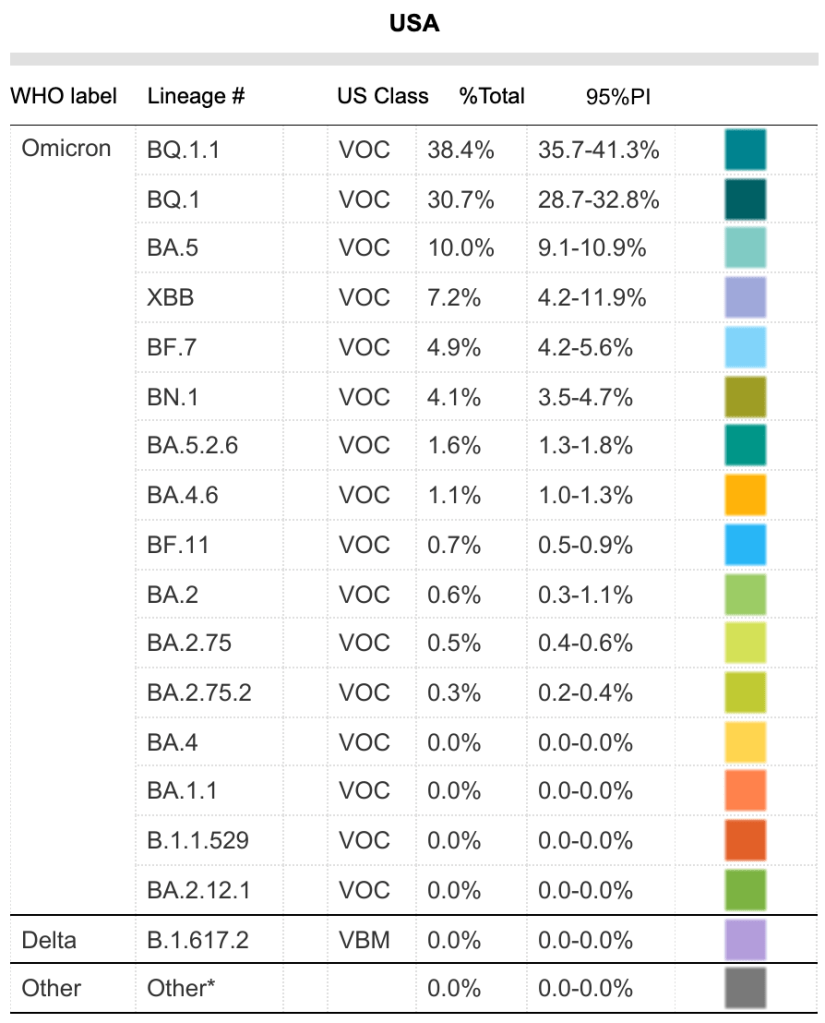
The BA.5 variant now represents only 10% of currently circulating COVID variants. There are currently 12 variants circulating in significant numbers, the most common being BQ.1.1.
Tridemic: A physician friend of mine who works in urgent care joked that we are currently in a “tridemic”, by which he meant that there a lot of COVID, Flu, and RSV cases right now. Everyone knows about the flu, but many are unfamiliar with RSV. Well, actually, you are. Respiratory Syncytial Virus (RSV) is one of the several viruses that are responsible for what we call the common cold. You have likely had it many times in your life.
For most people, RSV is just an annoyance, but it can be serious for infants, causing bronchiolitis, a swelling of lung tissues. If your infant is coughing a lot, breathing rapidly, wheezing, or just breathing noisily, contact your doctor. Those with infants in their life may consider taking extra precautions to avoid passing along a cold. The blue surgical masks are not a good defense against COVID, but they are effective to prevent droplets which transfer colds and flus.
Many guess that RSV has become more serious because we have been so cautious for the last few years. I don’t know for sure if this is true, but it seems like a reasonable idea.
Long blood clots due to vaccines: Chris Martenson has a new video regarding the long blood clots that many embalmers have discovered in the arteries of COVID vaccine recipients. The phenomena started occurring in May of 2021, a few months after vaccination became common. Dr. Martenson is a pathologist and has done many autopsies in his career.
Chris Martenson on vaccine related blood clots:
In the video, he addresses a recently released documentary called “Died Suddenly”. The documentary claims that at least 140,000 people have died due to these vaccine induced blood clots. In Martenson’s video, he points out that detractors of the “Died Suddenly” film argue that these clots are post-mortem, meaning they arise after the person has died. Dr. Martenson argues that the clots in vaccinated patients are definitely pre-mortem (before death), not post-mortem as some have claimed. He gives specific features that lead him to this conclusion.
Dr. Martenson is one of my favorite commentators. He is knowledgeable, open-minded, and evidence based.
I got a question about whether these clots only happen in vaccinated people. Late stage COVID disease is well known to cause clotting. But COVID related blood clotting mostly cause strokes and thrombosis. Obviously, these can also be very serious and lead to death. The vaccine related clots are different, completely blocking vessels. It’s not yet known how large they are pre-mortem. Dr. Mortenson argues they are pre-mortem, but that doesn’t mean they won’t continue to grow before an autopsy.
Searching “COVID blood clot” and “vaccine blood clot” on Pubmed will both bring up a lot of papers. I haven’t read enough of these yet to know if the large clots only happen with vaccination. The fact that you don’t need to get COVID to have clotting is obviously very important.
Died Suddenly: Several people have asked my thoughts on this film. I will say that many COVID-era documentaries have a definite bias, so I always have my guard up when watching them. Claims without sufficient evidence are common.
The opening credits juxtapose images regarding blood clots and potential vaccine related deaths with images from other unproven theories, some that most regard as untrue or even ridiculous, like bigfoot and UFOs. This seems intentional, as if the makers intend for the viewer to pair these ideas. This seems to me to be ill-advised, if they intend to convince the viewer that blood clots can be tied to COVID vaccines. It almost begs the viewer to associate their thesis with nonsense.
The basic premise of the film, the phenomena of vaccine related clots, seems to be at this point to be well founded and well evidenced. The film offers several disturbing images of these clots being removed from cadavers. The film also shows many examples of individuals passing out suddenly, while driving, speaking in public, even performing surgery. The existence of this phenomena seems beyond dispute. Interestingly, the detractors Martenson references in his video claim that the clots are post-mortem, not that the clots don’t exist at all. Clotting has been a well known aspect of late stage COVID disease.
In addition to the potentially valid idea that vaccines have contributed to blood clotting in patients, the film makes the explosive claim that the deadly effects of the vaccine are actually intentional. I haven’t seen any data to suggest this connection. I’m not saying this is untrue, just that I haven’t seen evidence of this yet, so I don’t see a reason to believe it at this time.
The SARS-CoV-2 Spike protein has several toxic effects. First, it causes an inflammatory response in many tissue types in the body, leading to diverse symptoms, including myocarditis, inflammation of heart tissue. This new phenomena shows that the spike protein can also cause blood proteins like fibrin to form an amyloid, an unnatural collection of proteins. Amyloid plaques also have a role in Alzheimer’s disease.
Should you get the updated booster? COVID vaccines appeared to be working well in the Spring of 2021, but their effectiveness began to wane with the Delta variant. When Omicron became the dominant variant, vaccine effectiveness dropped even further. As knowledge of possible harms due to the spike protein has increased, I now think the harms of vaccination outweigh benefits in our current environment. In my opinion, there is no longer any reason to get a vaccine or booster, even for those with risk factors.
If you’ve been vaccinated, this information will likely cause you some concern. I don’t know how long vaccine related spike protein has the potential to cause injuries. Blood clots appear to form around 5 months after vaccination. If you haven’t been vaccinated or boosted in the last 7 months or so, you may be in the clear. I’m sorry I don’t know more.
I have to point out that official channels claim that the information in “Died Suddenly” has been de-bunked. When posting this information on Facebook, I was met with several warnings about posting. To be fully informed on this issue, you should read several sources of information and judge for yourself which are most reliable.
Don’t fear, but be smart,
Erik