It’s been more than a month since my last update! To recap, a PET scan showed that the primary tumor in my lung has shrunk a lot and the secondary tumor on my rib is essentially gone. While it seems to me like progress since then is more gradual than I’d like, I definitely see some nice milestones as I look back on the month. While I’m done with radiation and chemo, I’m still getting immunotherapy infusions.
First, I was able to quit taking my last opioid medications a few weeks ago! This granted me the wonderful freedom of being able to drive again! My first solo trip was to grab a carne asada burrito with some friends. I’ve really enjoyed being able to drive myself around again (not too far!), and Kathy has enjoyed a little time to herself at home!
I’m continuing with my physical therapy. My posture is much better, and I’m not so hunchy anymore. A lingering issue is that the muscles of my right lower torso are still quite grumpy. My PT thinks it’s because they are trying to stabilize my rib cage because of the broken rib. While my muscles are loosening up and I’m making progress, I won’t be totally back to normal until my rib completely heals. My oncologist thinks the remaining pieces are about a centimeter or 2 from each other now, so it will still be a while before they come together completely. It’s still a challenge to pick up something off the floor, or to pick up something heavy.
My lung capacity is not back to normal, but I have made big progress. We go for a walk in our neighborhood almost every day. When we first started, I could only make it about 25 yards before I had to come back. Just yesterday, we walked our pre-cancer route, which is 2 miles, with 2 uphill sections. I have to take it slow sometimes, but it’s very nice to know I can go that far. When I return to work, I’ll need to be able to walk quickly around airports to travel again!
That’s all for now. I may not send out another update until after my next PET scan, which will be late March.
Keep praying for better lung capacity, that my rib would heal quickly, and that my torso muscles would settle down.
Don’t fear, but be smart! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
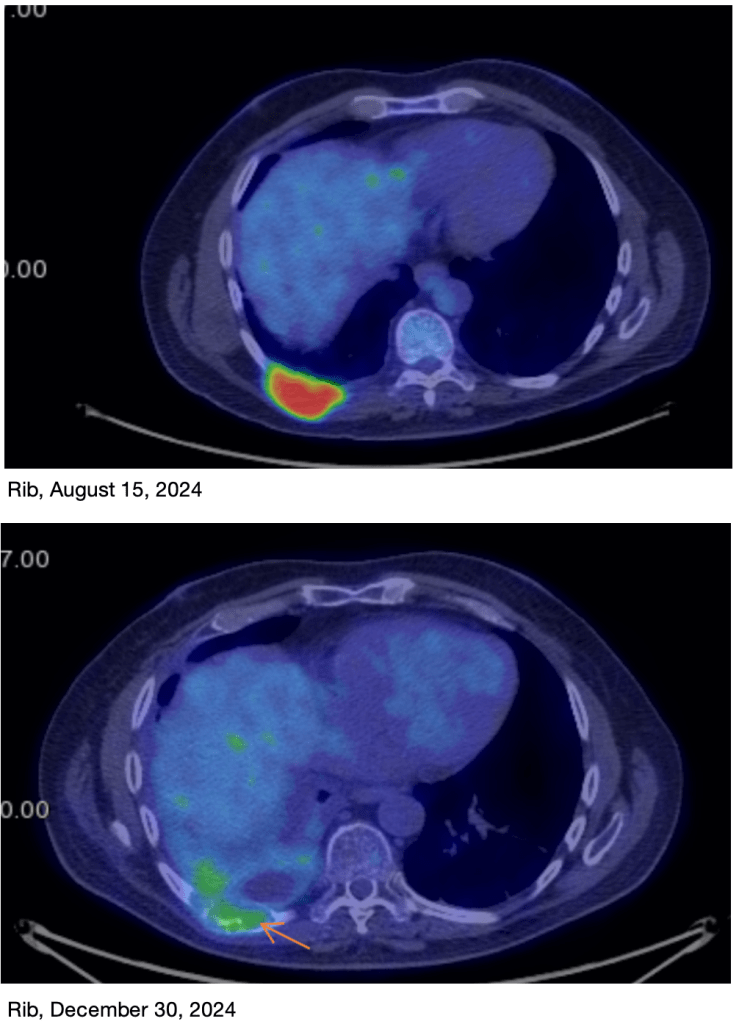
On Monday, I went in for my PET scan. In this procedure, radioactively labeled sugars are injected and allowed to be taken up by cells in the body. Because cancer cells particularly love sugar, the radioactivity mostly ends up in the cancer cells. Scanning for radioactivity highlights the location of tumor tissue.
While not gone, the size of the lung tumor is much reduced. The chemo agents will continue to work for a few more weeks, and the immunotherapy will take care of the rest. Prognosis remains good!While some concentration of sugars is apparent at the rib site, my oncologist said the rib tumor is essentially gone.A 3D image, before and after for both tumors. The rib tumor is essentially gone. Technically, the dimensions of the lung tumor is a little smaller, but you can see that the tumor is much narrower and smaller by mass.
Earlier this morning, we met with our oncologist, and he was very happy with the results! There is some of the lung tumor left, but the rib tumor is essentially gone. He said we won’t need to do any more chemo, but we will continue with the immunotherapy. Even though we’re all done with chemo, it will actually continue to work for a few more weeks.
Since immunotherapy is so new, it’s not really known how long it we will use it. The initial studies were done for 2 years, so he’s saying we’ll potentially go for 2 years, but he also said there’s a good chance we’ll stop early, depending on how things go. I’ll get another PET scan in March to see how things are going.
So the news is good! I still have limited lung capacity, which I’m looking forward to getting over, but I’m steadily improving if slowly. My visits to physical therapy are producing improvements to my posture and strength too.
Thanks for your continued prayers! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
Last week was probably my last hard week after an infusion, as I probably won’t have another chemo infusion! So to extend my analogy from my “Wednesday” post, it’s now “Friday”! I should be feeling better from here on out. My chemo oncologist also said no more immunotherapy until they see the results from my PET scan on December 30th, so I get a nice little Christmas vacation from my immunotherapy too! My next update will probably be after the 30th, letting you know my PET scan results.
I was pretty sleepy this time, and my fatigue from chemo my have been compounded by the immunotherapy. There are other potential side effects from immunotherapy, but happily, I didn’t really experience any of those. The sleepiness just lasted a few extra days.
I had an appointment with my physical therapist for the first time in many months. I had a laundry list of things to work on, and it will take us a while to work through them all. I lost significant strength and muscle mass while in the hospital, so I worked on a bunch of exercises primarily designed to improve my leg and core strength, and to improve my posture, which has gone funky since my hospital stay. I’ve gotten started on doing my exercises at home and I’m looking forward to improvement.
Strengthening my upper back musclesThis looks like a wall sit, but it’s mostly for working on my posture.
Please continue to pray for improved lung capacity. I’m still short of breath, meaning that my Vital Capacity, the volume of air that I can breathe if I exhale as much as I can, then inhale as much as I can, is still lower than it should be, and I have to take more breaths when I go for a walk.
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
This is a cancer update. Yesterday I had my last of 4 expected chemo infusions, and my first of many immunotherapy infusions. I mentioned before that I take an anti-side effect medication for the first weekend, but I’ll be fatigued for some of next week. There may also be some additional side effects from the immunotherapy, Keytruda.
I’ve been very cautious about getting sick up until now, since I didn’t want to have to postpone treatments. But after next week, I’ll probably start being more free to “move about the cabin” as it were.
Writing this very blog, earlier today! Broose and his wife Penny bought me this sweet chair, which practically dumps me out of the chair if I want. Super comfy!
This last round has not been without drama. On the Sunday right after my last infusion, I passed out twice within a few minutes of each other. I was probably only out for a few seconds both times. I ended up going to the ER but my visit there was actually pretty uneventful. They couldn’t really find anything, and said it was pretty much just the chemo. So Kathy took me home after a few hours, and I’ll just need to remember to get low right away if I get lightheaded again. We’re always thankful when they don’t admit me!
My chemo side effects have been quite mild, which I’ve been very happy about. I threw up a lot after the first infusion, but not the others, which is great. I have another kind of amusing side effect of chemo that I’ve never been aware of. My skin is shedding a lot, kind of like full body dandruff! Kathy jokes that it’s like having her own personal snow globe! Every time I change my clothes, there’s a flurry of “snow” as I fold them! Kathy even says that I look younger with reduced age spots! And no, I don’t recommend this method of exfoliation! Anyone else have this side effect?
After a low weight of 165 lbs, I’m back up to 180, which is great. I’m going to take a little pause from the weight gain until I can start meeting with my physical therapist on the 16th. My target weight is 190 to 195, and I want to put on some muscle instead of fat! So I’m cutting back from 2 bowls of ice cream a day to just one!! Favorites are Mint Chip, Mocha, and Cherry from Tillamook. This is just an interesting detail. Please don’t leave a bunch of ice cream on my porch!
A little detail about my daily life is that we love Gospel music and I’ve have fallen into the habit of waking up to “You are the Living Word” and “Give Me a Clean Heart” by Fred Hammond. They’re great songs, with great bass lines, of course. I try and get out of bed before the first one is over!
Back to the medical side, my prognosis remains good and my tumors are shrinking faster than anticipated. I’ll get a PET-scan on the 30th. For this test, I have radioactive sugar injected, then wait 45 minutes for the cancer cells to suck it up. Cancer cells love sugar, and quickly absorb the radiolabeled glucose. Then I get scanned in a specialized scanner and see how the tumors look. PET scans are the most sensitive way to detect tumors and allow doctors to see even small tumors wherever they are. My chemo oncologist expects that my rib tumor will already be completely gone, and that my primary lung tumor will be much reduced. The chemo will continue working for awhile, and the immunotherapy will continue for to up to 2 years!
A word on immunotherapy. As mentioned in Update 7, immunotherapy agents cause T and B cells to attack tumor cells. Some tumor cells express a surface protein called PD-L1. This protein causes the immune system to see the tumor as “self” by binding to the PD-1 protein on T and B cells. Keytruda stops these proteins from binding to each other, causing the T and B cells to see the tumor as alien. Unfortunately, this can cause some normal cells to appear alien as well, leading to some side effects. My autoimmune disease is not expected to be impacted by all this, but I’ll need to be monitored to make sure. My oncologist says that since my tumors have a lot of PD-L1, this therapy may work especially well on my tumors. Depending on how I respond, I may end up being on Keytruda for up to 2 years!!
Please continue to pray that my tumors will become normal lung tissue and not scar tissue. I’ve also had some shortness of breath for the last 2 weeks, but I’ve seen some improvement over the last few days. Pray that my lung capacity improves!
Merry Christmas and Happy Hanukkah, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
My 3rd round of chemo started with an infusion yesterday. For the first few days of a new round, I’m on some extra medication that counteracts some of the negative side-effects of the chemo agents. So while I’m on those medications, I’m actually feeling really good! Those medications will run out on Sunday, so starting Monday is when I start “Fatigue Week”, which for me has been just sleepiness. Until then, I’m actually feeling good and can do my normal 2 short walks a day, and even do my stair exercises. “Fatigue Week” has generally lasted just from Monday to Thursday or so, and then I’ve been turning a corner on Friday, which I expect to happen this week as well.
I usually go on 2 short walks a day. Then I do 5 sets of stairs after my walk, trying to regain muscle mass after my long hospital stay. It’s already making a difference!
I caught a very mild viral infection this time, and had to be more strict on having visitors. Fewer visitors, and always meeting out on the patio from now on. Despite that, my White Blood Cell count remained fine for a person on chemo, so my 3rd round started on time. I also finished my radiation treatments on Friday, November 8th, so I’m very happy to be done with that. Now it’s just chemo, and immunotherapy starting with my next chemo round in early December. People tolerate immunotherapy very well.
Because I’m halfway through chemo, Kathy remarked that it felt like “Wednesday”, like we just have to endure a few more days before the welcome end. Everyone from students to adults in the workplace know what that feels like!
Right now, I’m thinking as if my chemo journey will end around December 14th, when I’ll emerge from my “bad week” for that round. Then I’ll need to start working out, regaining the strength I lost while in the hospital. It’ll take me a few months to get back to my ideal weight, and be ready to travel again. So by Christmastime, I should be mostly back to normal.
Results continue to be very good, and my prognosis remains very good!
Thanks again for all your prayers! We continue to pray that my tumor tissue will become lung tissue, and not just scar tissue, to maximize my hiking, backpacking and skiing abilities, some of my favorite activities!
Also pray that my broken rib will heal quickly! We still have no idea how long it will take, but it will be much longer than the usual 6 weeks, since the pieces are not sitting right next to each other yet, but have to grow together before they can mend.
Don’t fear, but be smart, Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
I’m going to share a brief update, and then give you some information on how my treatments work! In my private discussions with some of you, there is some curiosity about radiation, chemo, and the immunotherapy that I’m using to get well. So I thought I’d give some details on those things.
I also want to say before I start, that I’ve also learned from several of you that you are going through your own journeys with major health problems right now, including cancer. Know that I am praying for you! May God take care of you just as He has been taking care of me!
Update: My first infusion was October 3rd. The nurse told us that the worst days were 4-10 days after infusion and she was right! I was miserable and wiped out the following Tuesday!
I’m doing much better now, and enjoying the break. My next infusion is this week, on the 24th. I’m half way done with radiation treatments on my primary tumor, and my last radiation is on November 8th. So my last 2 infusions will happen after radiation is over. So this next one will likely be the worst, but the last 2 infusions are likely to be easier than the first 2!
My last infusion is on December 5th, and I’m looking forward to feeling much better in December. Hopefully by Christmas, I’ll basically be back to normal.
My pain is low enough now that I’ve started to work myself down from the opioids, which is lowering some of the negative side effects from an already low dose. The doctors are pleased at this news! I’m also able to eat more, so I’m working on gaining some weight.
We are so thankful for the support of friends and neighbors that we continue to get. Your prayers have been an important part of my progress, so keep it up!
Radiation: Radiation is a common cancer treatment because it’s less invasive than surgery, but it’s still quite effective at killing cancer cells. It works by damaging the DNA of cancer cells, leading to the self-destruction of the cells.
X-ray radiation is the most common. An emitter looks like a giant microscope and moves around the patient, firing hundreds of X-ray beams in sub-lethal doses. Only the tumor receives a lethal dose of X-rays. The CT scan measurements are exact and treatment plans are done by a physicist for each patient. In fact, a physicist and doctor need to be present and approve how the machine is lined up with the tumor every day before they start the radiation treatment!
An X-ray therapy instrument. The large piece with a glass pane right behind the patient’s head is a CT machine that does a mini-scan every time I go in, to make sure that my body is properly aligned with the map that they have. The gray plate on the right detects the x-rays from the CT machine after they go through the patient.
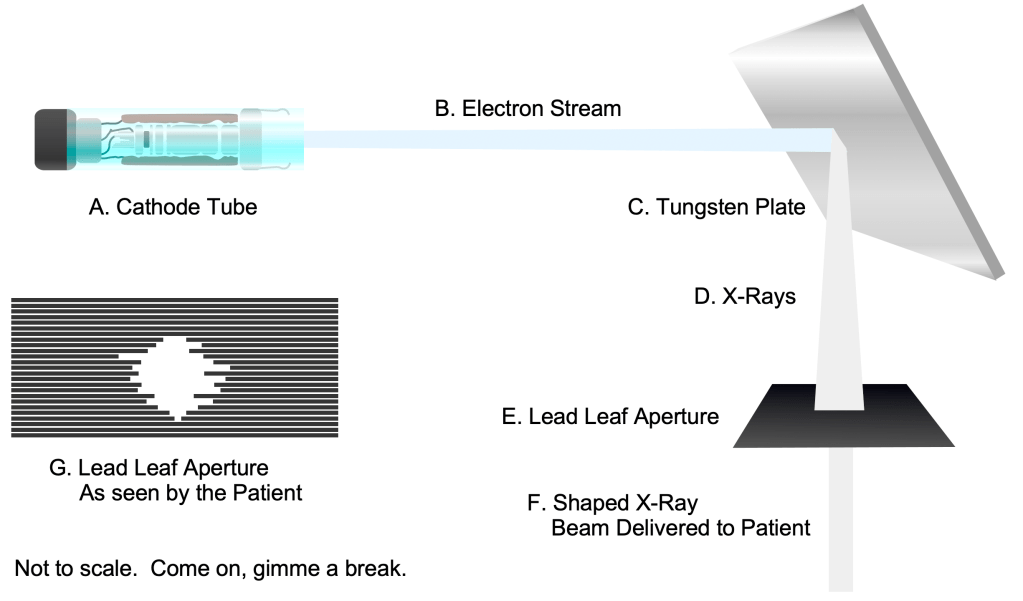
Inside the instrument, an electron beam is created by a cathode ray tube, much like the ones that used to be in the old tube televisions. The electron beam strikes a tungsten plate The electron beam is absorbed by the plate and transformed into X-rays that are emitted by the tungsten plate. These X-rays then pass through a lead aperture that shapes the beam into just the right configuration for the shape of the tumor at that angle. This aperture is made of lead “leaves” that actually move to shape the beam as the emitter moves around the patient. Yes, I can actually see the aperture changing shape as the emitter moves around me!
Inside the instrument, an electron beam (B) is created by a cathode ray tube (A), much like the ones that used to be in the old tube televisions. The electron beam strikes a tungsten plate (C). The electron beam is absorbed by the plate and transformed into X-rays (D) that are emitted by the tungsten plate.
These X-rays then pass through a lead aperture (E) that shapes the beam into just the right configuration (F) for the shape for the tumor at that angle. This aperture is made of lead “leaves” (G) that actually move to shape the beam as the emitter moves around the patient.
Yes, there is a risk that the X-rays themselves will cause a new cancer tumor to form, but the likelihood is that if one does, it will take many years for the new tumor to cause a problem, after the patient will have passed away from natural causes.
Proton beam radiation is much less common and much more expensive than X-ray treatment. Protons can more easily be concentrated on the tumor and are less likely to cause a new tumor. For these reasons, proton therapy is more commonly used on younger patients, to avoid the likelihood of producing a new tumor within the patient’s lifetime.
Chemotherapy: Normal human cells have many molecular checks to their growth, making sure the cells don’t get out of control. Cancer cells have mutations that turn off these checkpoints. This is why cancer cells grow rapidly and can become dangerous. Chemotherapy agents selectively kill cells that are growing rapidly. Since cancer cells are growing very rapidly, chemotherapy agents kill them first. Unfortunately, some normal cells in the body grow faster than others, like hair, gut, and blood cells. This is why patients can lose hair, experience nausea and digestive problems, and suffer from low blood cell counts, or even become immunocompromised.
The good news is, on balance, chemotherapy is usually very effective at killing cancer cells, and many people have been saved through the use of these agents.
As I said in my first 1st update, Next Generation Sequencing (NGS) testing can help doctors know if a patient will need to use certain chemotherapy agents. My tumors don’t happen to be particularly interesting in this regard, so I’m just getting a “normal” first try set of chemotherapy agents. NGS has definitely increased the survivability of cancer by helping chemotherapy work on the first try!
Immunotherapy: The PD-1 protein exists on the surface of certain T and B cells of the immune system. They work to inhibit the function of these cells in most conditions, making them tolerate “self” cells in the human body, helping to prevent autoimmunity. If a person has cancer, “turning off” these proteins can make these T and B cells no longer recognize cancer cells as “self”, and attack them! Immunotherapy agents like Keytruda inhibit the PD-1 protein, causing the immune system to attack some tumor types, like the cancer I have, non-small cell lung cancer.
Prayerrequests: I’m doing much better eating, and my goal is to maintain my weight through the next round of chemo, and to gain some after that. Pray that I will be able to eat enough calories for that! Thanks!
Don’t fear, but be smart! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.
I came home from the hospital on September 15. It’s been great to be home! My focus has mostly been on healing, following directions, and getting ready for my chemotherapy sessions to start. An ongoing issue has been that I lost weight in the hospital, which I should try and get back before chemo.
So I’ve been exercising as much as I can, going for short walks, and doing limited workouts in my chair.
Chemo I had my first chemo session on Thursday, October 3, on schedule. The infusion took about 2 hours, and everything went fine. I’ll have 4 sessions total, each 3 weeks apart, the last one taking place on December 5th.
My first infusion. Yes, I’m saying “Let’s do lunch!”
Tumors Shrinking! Thursday was a very busy day. After my chemo session, I actually had a late radiation session and a meeting with my radiation oncologist. He told me that my tumors, both of them, were shrinking faster than anticipated. Yes, both of them! Even before chemo, he noticed that my primary tumor in my lung was shrinking as well. It was shrinking about 3 times as fast as normal. My doctor said “I can’t really explain such a change.” He seemed quite pleasantly surprised, and baffled at the some time.
Abscopal Effect? If anything, he said he might attribute this to a phenomenon called the Abscopal Effect. Basically, debris that is formed as the rib tumor starts to fall apart due to the first set of radiation treatments end up becoming material that the immune system uses to mount a defense against the second tumor. The radiation starts killing the rib tumor, creating a vaccine that tells the immune system how to attack the primary tumor! Just to emphasize, even to my radiation oncologist, the Abscopal Effect is still theoretical, and is a very rare phenomenon to see.
I recently graduated from a walker to a hiking stick.
Today, Monday October 7, before my radiation treatment, they actually did a new mapping scan in order to re-calibrate because of the extra tumor shrinkage.
In short, your prayers are working! Thank you so much for your prayers and keep it up! I actually need extra prayer because chemo is making it hard to keep food down. Hopefully this will just be happening the first week.
Don’t fear, but be smart! Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page.
On Sunday, September 15, I got out of Scripps Encinitas Hospital after a 2 week stay. In the next few updates, I’ll tell you what I was doing there and how I’m doing now.
Complications On Sunday, September 1st, I was experiencing a lot of pain, sometimes 8 on a scale of 1-10.
We went to the ER and after some testing, they discovered 2 major complications. 1 was a pleural effusion, a bag of fluid between my lung and chest cavity that was limiting my lung capacity. The pleural cavity is usually a very narrow cavity between the lungs and the rest of the body. Just around the lung is a thin tissue called the parietal pleura. Normally, this cavity contains just enough fluid to allow the lungs to glide along this tissue as they expand and contract. Sometimes, however, this fluid inside this cavity doesn’t drain properly, and fills will fluid. This is a rare condition. The problem with this is that the extra fluid can compress the lung and reduce lung capacity, making it harder to breathe.
They had to install a chest tube so the fluid could drain.
The inside of the lung is actually “outside” the body, because it is open to the outside world. The pleural cavity is just outside the lung. This is the area that can fill with fluid to create an effusion.
Additionally, they found an infection, a bacteria called Granulicatella adiacens, a species that is difficult to grow in a lab, and so unknown even to most microbiologists. The infection was related to the effusion, so the next day, they put in a chest tube so they could drain fluid from the effusion.
So now instead of one potentially deadly condition, I now had 3.
Insurance When Kathy lost her job last year, we lost our traditional health insurance, which was really good. We signed up for a cost sharing program. To use one of these programs, you need to tell medical providers that you are self-pay. You pay everything with cash or credit card. You get an itemized receipt from the provider, then submit to your program. We will get reimbursed by our program roughly 3 months after we pay the expense.
There are big pros and cons to these programs.
Cons:
1. Cost sharing programs are new, so most providers still don’t know how to handle them. They reflexively want to bill insurance, so they are always asking what program we have. To prevent them from sending our program a bill, we always just say that we’re self-pay.
2. It’s almost been a full-time job for Kathy to collect itemized bills from hospitals, individual doctors, and laboratories. Happily, Kathy is running her art business full time now, so she has the flexibility to do this.
Pros:
1. Providers usually give huge discounts for self-pay. My recent hospital stay was expensive, but we will get a 50% discount.
2. The monthly cost of our sharing program is far less than insurance premiums for the both of us for the month. So we actually opted not to get insurance from my new job.
3. One big problem with health care is that you can’t just ask your provider how much something costs. Insurance companies still cut mysterious deals with providers, so no-one seems to know what anything costs. Cost sharing programs may be a way around this. We get bills with actual numbers on them for the services we use.
First world countries have a variety of approaches to health care. Nationalized services have the problems of high taxation and long waits for care. The US now has high costs for insurance premiums and high deductibles. I think cost sharing, when it’s more accepted, may be the future of health care payments.
Opioids I started taking opiate medications, which made me mildly hallucinate and become nervous about addiction.
I’m not at all excited about taking opioids. Coming in several forms, opioids are highly addictive, and have other unfortunate side effects. I’m a very disciplined, type-A person, so I’m hopeful I won’t have too much trouble working my way off of them, but friends who have done so say it took them some time. I also have friends, very good people, who ended up having to go to rehab so they could be supervised. You can certainly pray for me during this process when the time comes.
If you end up having to take opioids, make sure you work with your doctors to find the right regimen, and follow your doctor’s orders. You can change your prescription and orders, but don’t take more than your doctor prescribes. This will help keep you from having trouble.
Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page.