This is a case update. I’ll also discuss the first pre-print paper on Omicron, from a lab in South Africa.
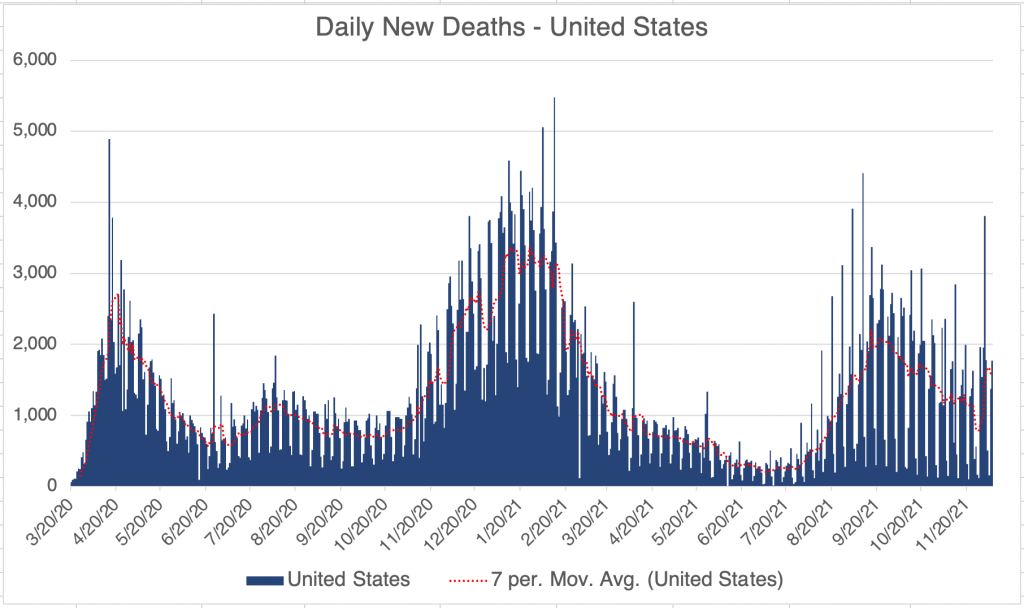
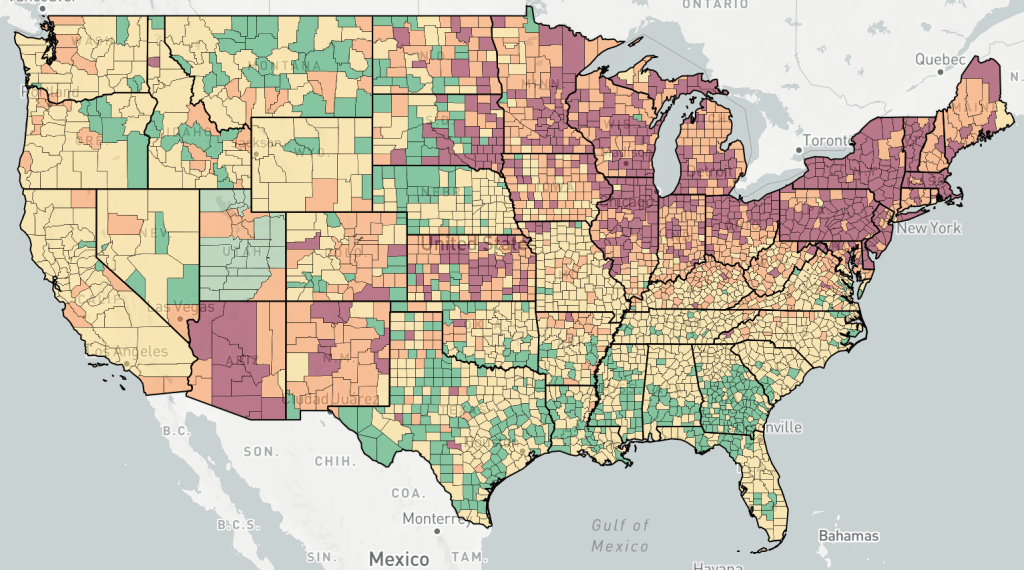
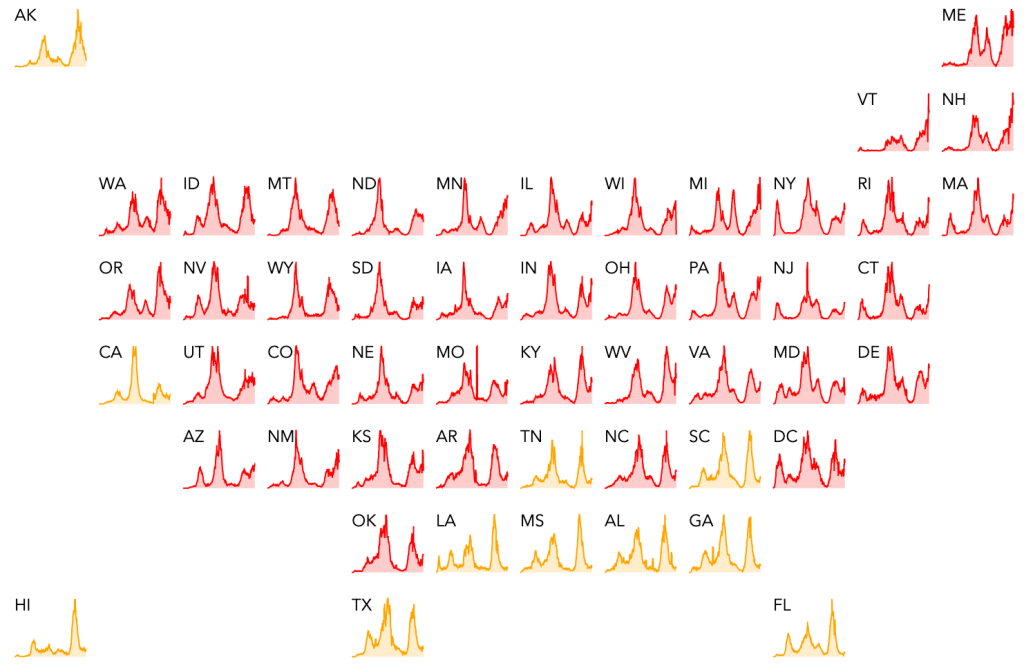
Cases are rising in the US and cases in the Northeast are rising sharply at the moment. While the Omicron variant is now present in 19 states, most new cases are still from the Delta variant, and Omicron cases in the US are still very low.

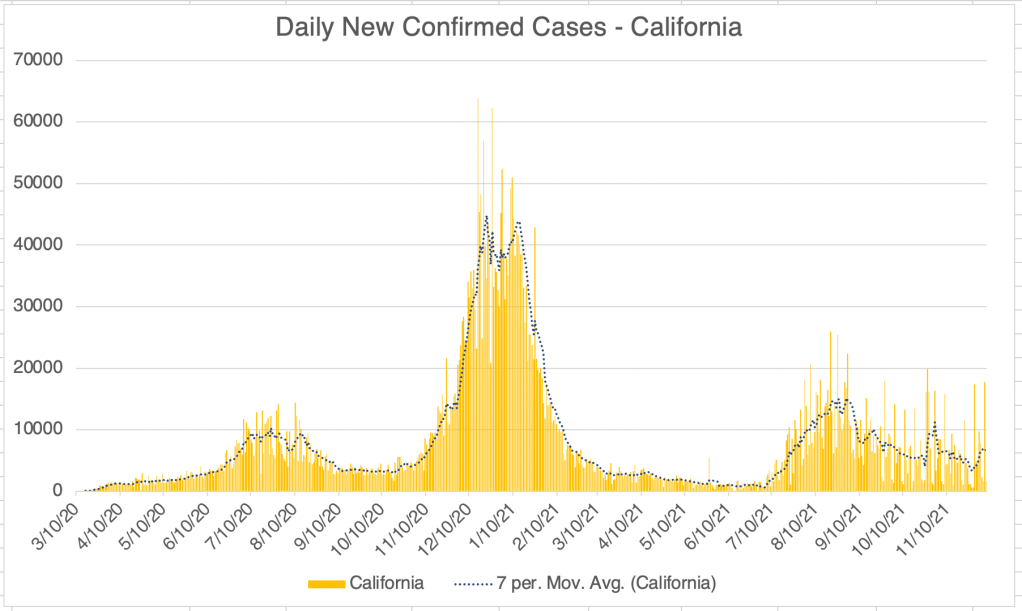
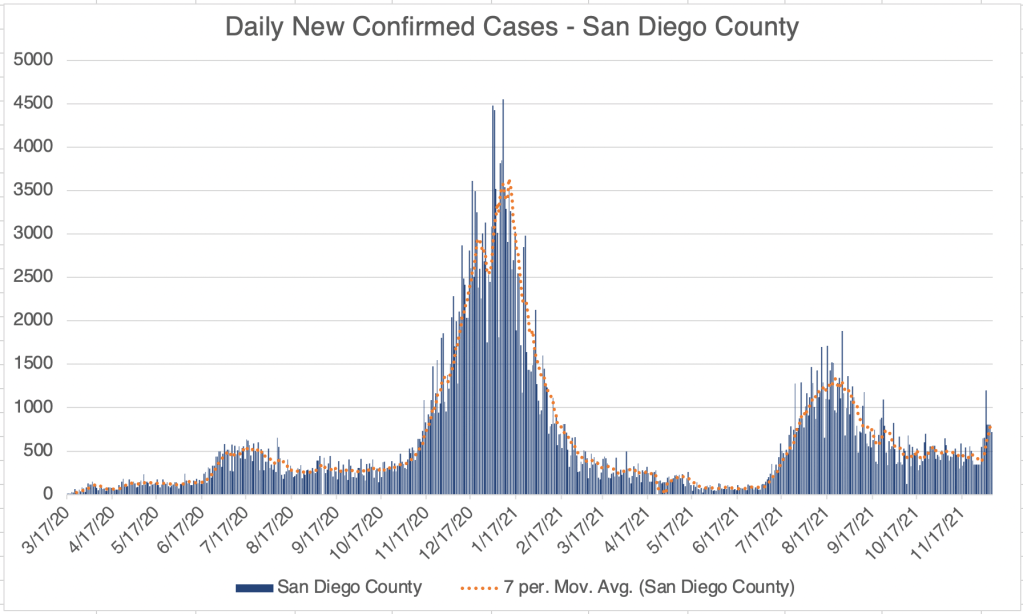
California is still not showing an increase in cases due to the Winter season, although the persistent number of cases after the Delta wave is still quite high, almost as high as last Summer’s wave.

In San Diego County, last week had a surge in new cases. We’ll have to see if this is the beginning of a new wave, or just temporary.

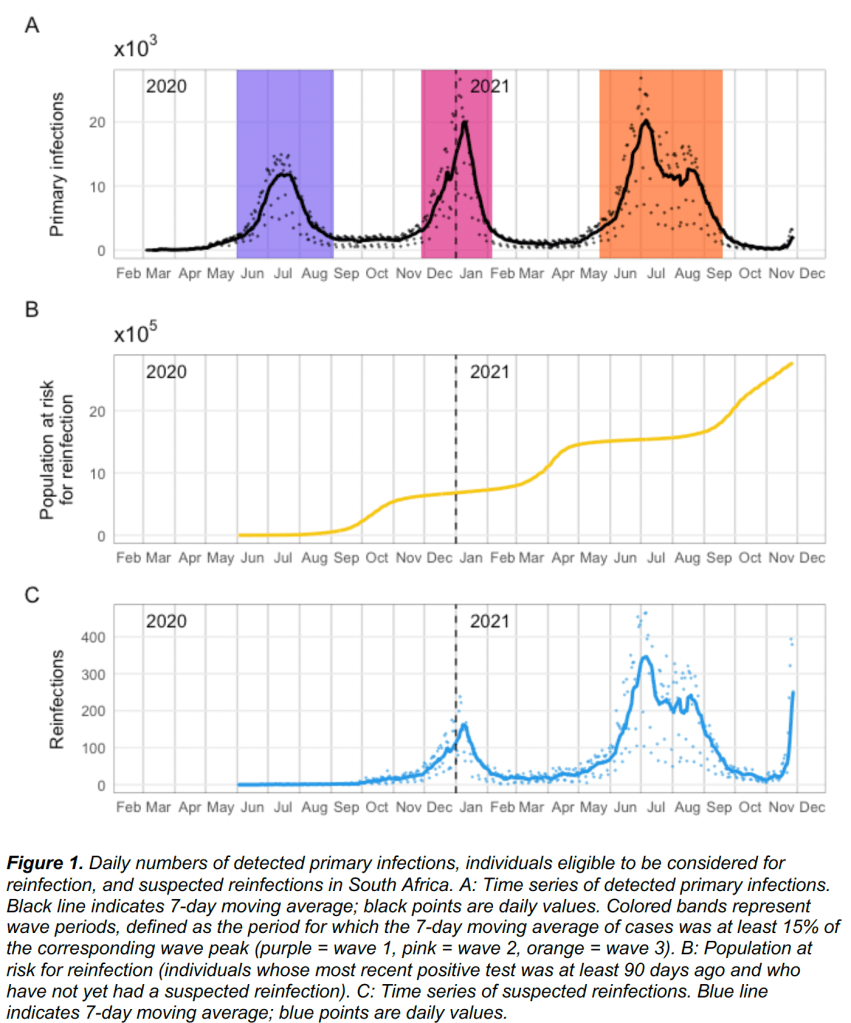
Omicron causes increased co-infection: A pre-print paper has been released from a lab in South Africa, Pulliam et al. The paper looks at Omicron infections and also previous history with other SARS-2 variants. Since vaccination is relatively low in South Africa, the ability of vaccination to prevent infection by Omicron is not accessed.
The big take away from the paper is that while previous infection with a Wuhan strain prevented infection with Beta or Delta variants, it does not prevent infection with Omicron, at least according to this study! In fact, Omicron may be using the ADE pathway to reinfect patients, as risk of infection with Omicron appears to go up if a person has had a previous version.
The paper does not directly address whether vaccination will prevent infection with Omicron, but at this point, it seems unlikely. Unfortunately, the paper also does not discuss case severity in Omicron patients. A previous report from Dr Angelique Coetzee suggested that symptoms from Omicron are mild.
This data suggests that getting one of the current vaccinations will NOT help to prevent infection with Omicron. If you have not been vaccinated at this point, I suggest you NOT get vaccinated now, but instead take precautions until we find out how severe infection with Omicron will be. Of course, I am a molecular biologist, not a physician. Consult with your physician when making medical decisions.
If you’re interested, see this detailed analysis from John Campbell.
Monoclonal antibodies: Monoclonal antibodies are a common and effective treatment against SARS-2. They work similar to your own antibodies, but are often used early in disease before a person’s own immune system has yet been able to produce an immune response.
Medically useful antibodies can be obtained from a variety of sources, even purified from another person who has already had a disease. Monoclonal antibodies are made by first purifying immune B-cells from an infected animal or person, growing many copies of this cell in a lab, then purifying out the desired antibodies. These antibodies can then be injected into a patient to give them a boost in immune response.
And no, getting antibodies created from animal cells will not make you grow a tail or get beady little eyes.
If you get COVID, don’t hesitate to accept monoclonal antibodies if they are offered to you. They do not contain any vaccine components, nor do they involve any of the questionable ethical issues surrounding vaccines that are of concern to some.
Don’t fear, but be smart,
Erik
