As the news about Avian Flu broke last week, I was hoping that I could ignore it and it would go away. Unfortunately, discussion online has continued to heat up, so I wanted to give you some information. I’ll put the most important stuff in the next 2 paragraphs, and more details down below if you want them.
There is a new outbreak of an Avian Flu that is being discussed by various outlets. Avian Flu is a member of the flu family of viruses, but of a type that is very uncommon in humans. Transmission to humans is still extremely low, but because our immune systems are unfamiliar with them, symptoms in infected humans can be very severe and fatality rates are as high as 30%. Anytime a human is infected, there is some reason for caution. As of this writing, only 2 humans in the US are known to have been infected. Both individuals had direct contact with infected animals, both cattle and chickens. So far, there are no known cases of human to human transmission. For the large majority of us, the currently known chance that you or family will be infected is zero. I fully expect that there will NOT be a widespread outbreak of avian flu in humans.
If you have livestock animals like cattle, pigs, or chickens, you will want to take extra precautions. There has actually been an outbreak of avian flu among chickens in the US since 2020, so this is an active situation already. The risk is currently much higher to animals than it is to humans, and lots of animals have been culled during this time. Until we know more, quarantine new animals for a time as you bring them on to your property. Chickens can shed virus both in respiratory secretions and in poop. If you have sick or dead animals, wear safety goggles, gloves and an N95 respirator before handling them. Afterwards, wash your hands thoroughly before touching your eyes, nose or mouth. Dogs and cats can get bird flu if they eat infected animals or interact with them closely.
Because so many chickens are culled during large Avian Flu outbreaks, there may be an increase in chicken and egg prices.
The influenza family of viruses is native to aquatic birds, like ducks and geese. The flu arises every year from flocks living in southern China, and often spreads to farm animals like chickens and pigs before entering the human population. 2 surface proteins, hemagglutinin (HA) and neuraminidase (NA), both come in several different varieties, designated with numbers. Our typical yearly flu is either H1N1, H1N2, H3N2, or H2N2. Other strains always infect aquatic birds, and sometimes other birds or animals. Avian flus that have infected humans have been H5N1 and H7N9, while some other strains have caused outbreaks of disease in chickens.
While transmission to humans is still extremely low, experts are currently recommending that animal products be thoroughly cooked before consumption.
Today I’m going to give a super brief case update, then a discuss the potentially upcoming WHO Pandemic Treaty.
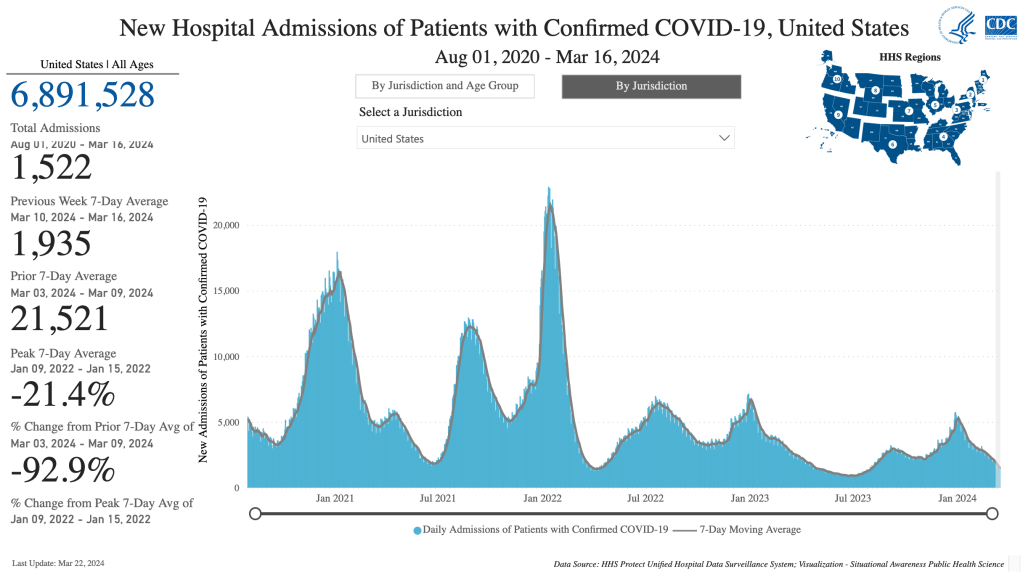
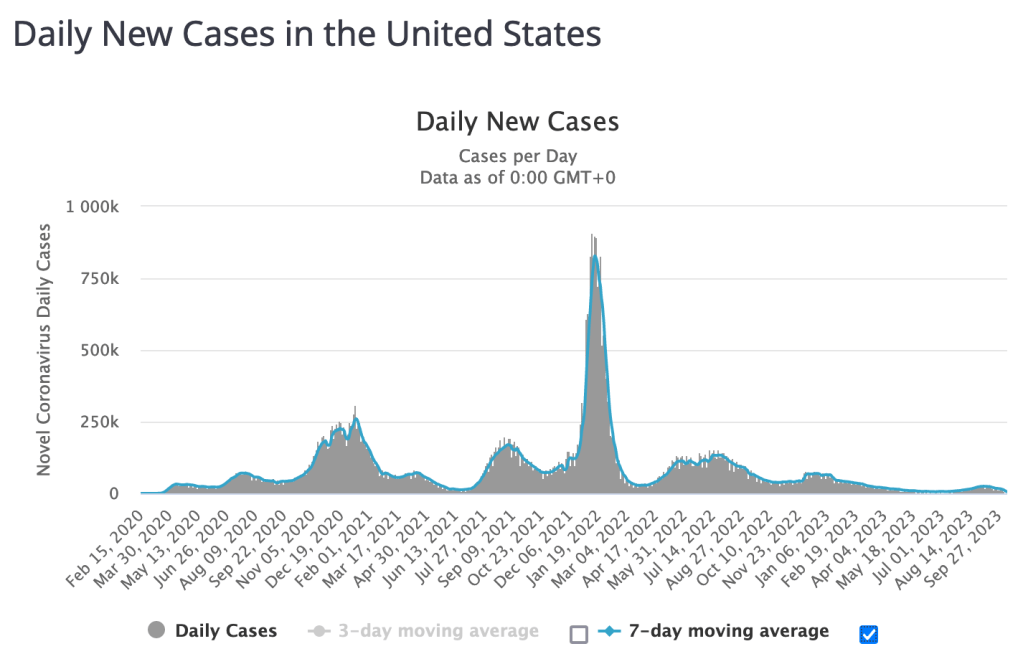
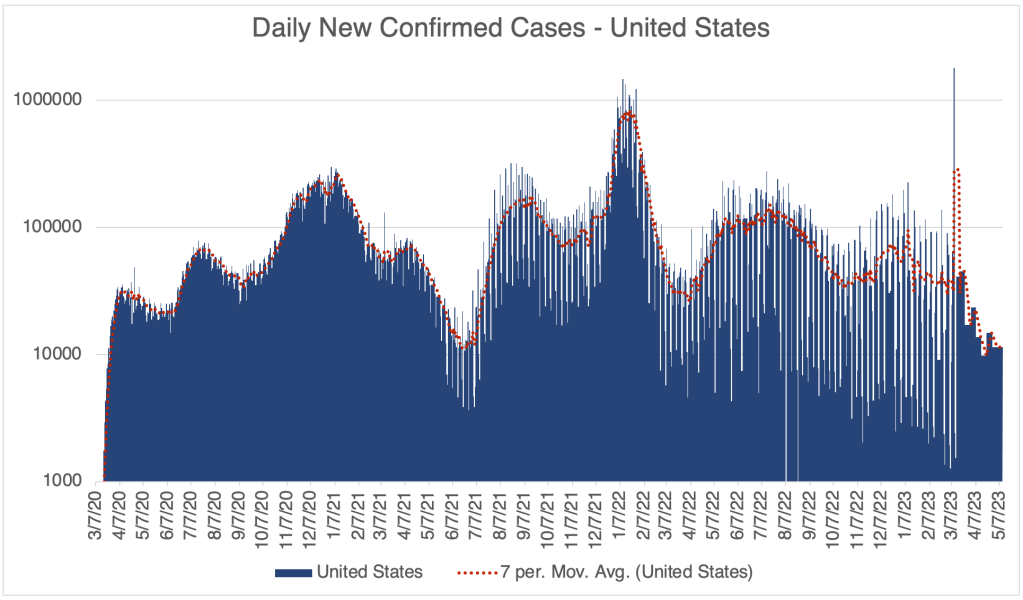
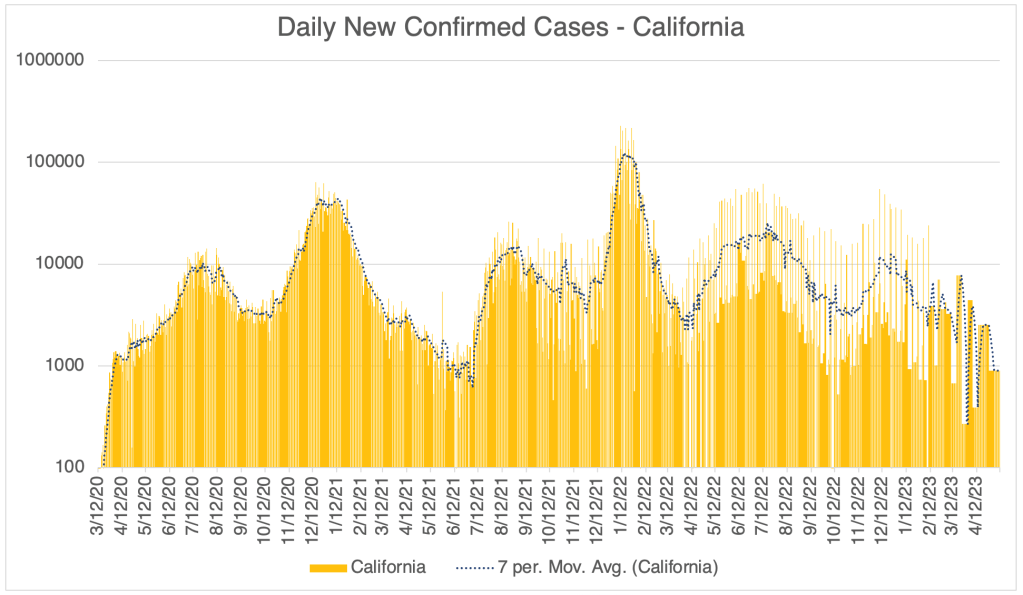
COVID Update: First, we had a wave of COVID cases late last Summer and another one this Winter. According to official reporting, both of these waves were small, with few officially recognized cases. A lot of people in my area of San Diego County had upper respiratory infections, but most people weren’t even that interested to know if it was COVID, a cold, or the flu. Several people I know had illnesses that turned into bacterial infections like sinusitis or bronchitis. COVID wasn’t known to generate bacterial infections, so these cases probably weren’t COVID. All this to say, COVID is now deep into the endemic phase, with COVID becoming just another respiratory infection for most people.
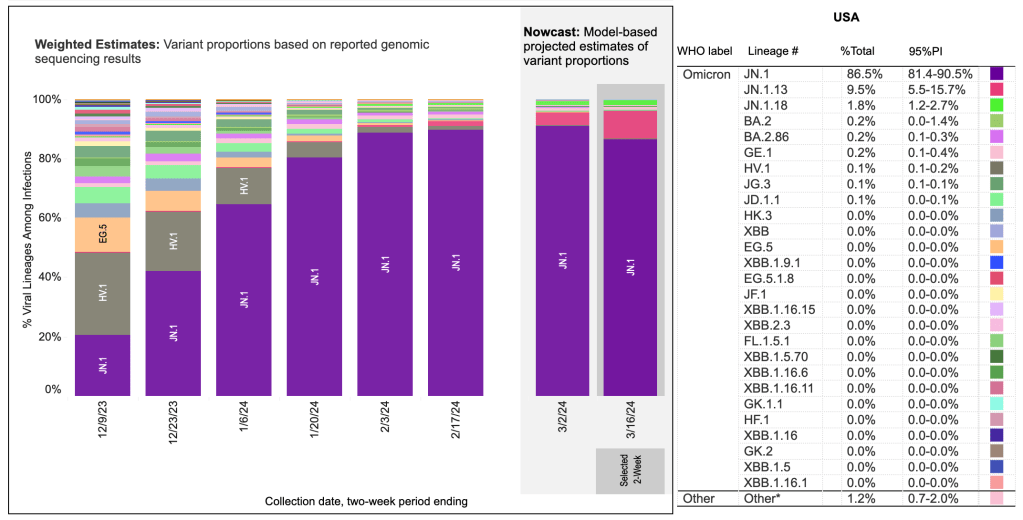
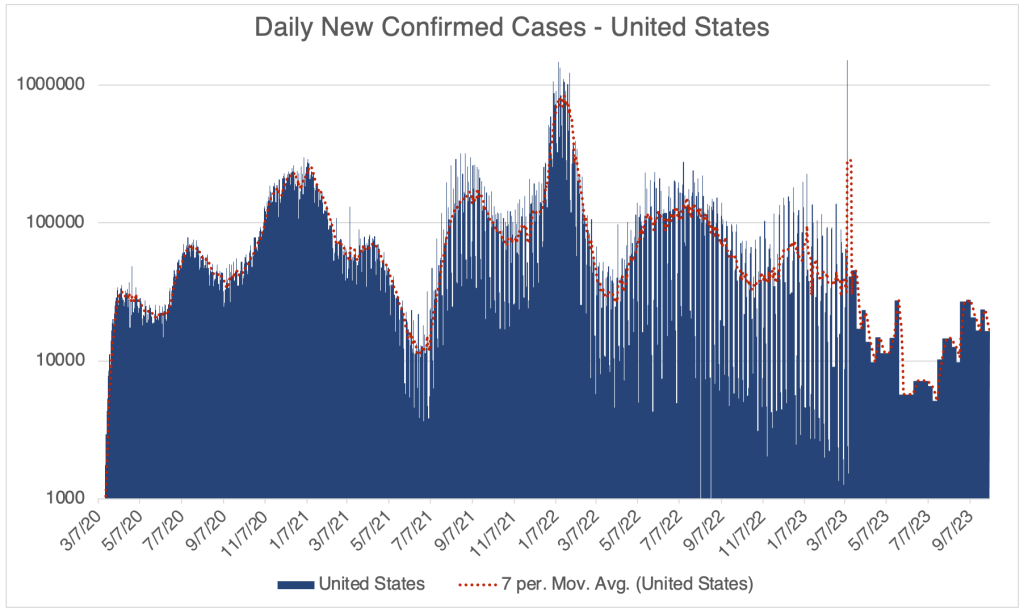
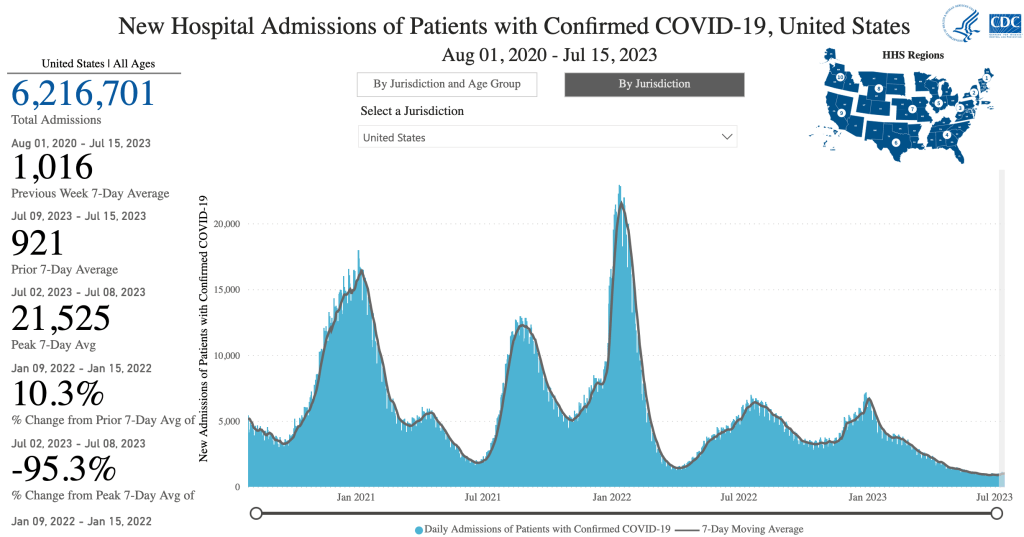
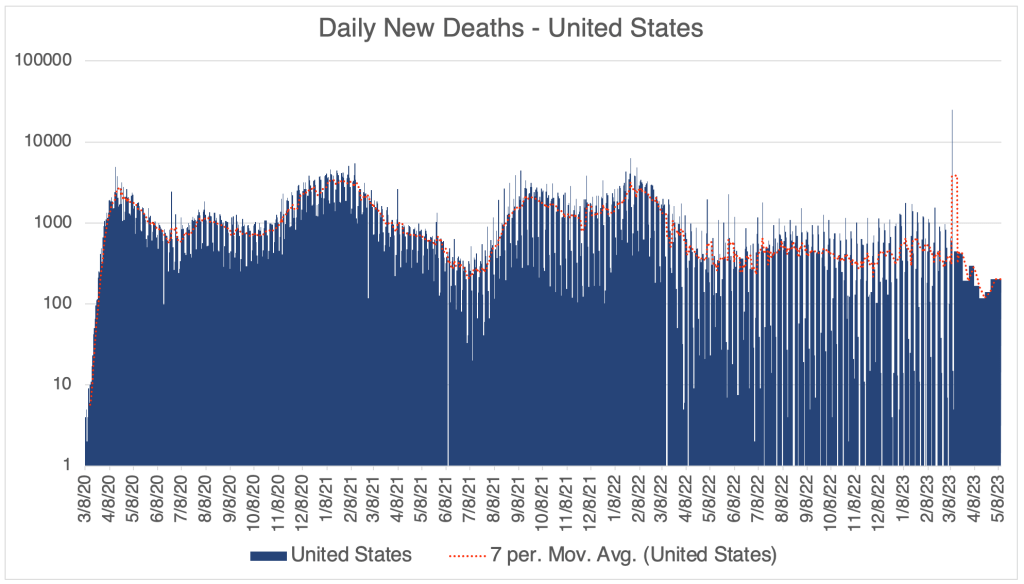
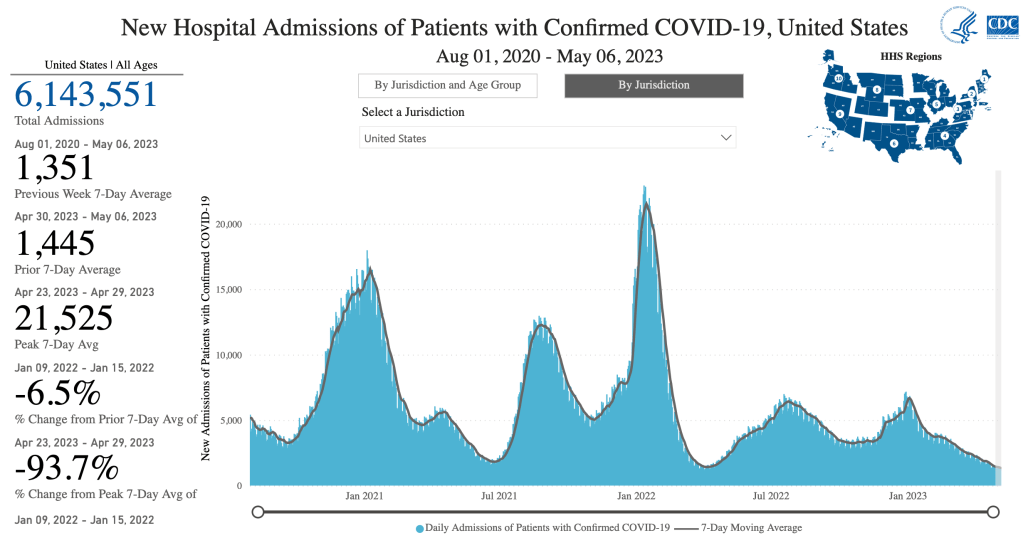
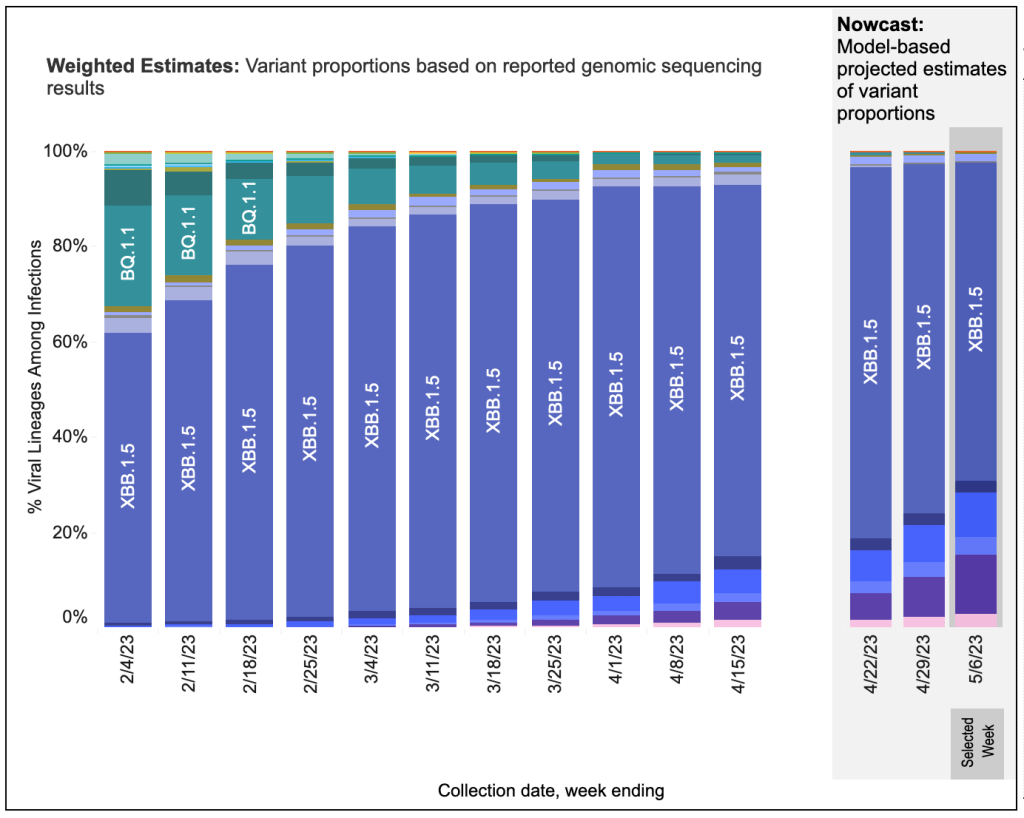
Daily US New Cases, Worldometer/coronavirus/us. The recent JN,1 wave is visible on the far right.Hospitalizations, from the CDC website.From the CDC page on Variant Proportions for the United States, March 16th, 2024. The current most common COVID variant is JN.1, an Omicron variant.
A brief note on Respiratory Syncytial Virus (RSV). The common cold is causes by any one of several classes of viruses, including Rhinovirus, Adenovirus, some Coronoviruses, and RSV. Everyone has had RSV several times in their life. While infants can have severe symptoms because of RSV, for adults, RSV infection will result in just a cold, although some can produce a bacterial infection. In my informed but not expert opinion, no adult, except perhaps new parents, needs an RSV vaccination. I’m a little baffled by the push for the RSV vaccine this year. I’ve never seen a campaign to encourage his before. Of course, always consult your physician when making medical decisions.
W.H.O. Pandemic Treaty: The World Health Organization (WHO), an agency of the United Nations, is currently negotiating an international treaty called the WHO Pandemic Agreement (full text). The agreement attempts to standardize pandemic responses internationally. Many medical freedom advocates have criticized the agreement for forcing countries to adopt practices that infringe on individual rights and also produced poor outcomes in many nations during COVID. The UN currently plans to hold a vote on the treaty in May of this year.
The WHO was the first international body to be public about the SARS-2 virus in January of 2020. Some of their claims at that time were demonstrably false, even when they were made, including that SARS-2 was not transmissible between humans, and that the virus was not transmissible through the air. They adopted some of the same draconian lockdown measures promoted by China at a time when the less restrictive measures used by Japan, South Korea, and Taiwan were proving to be more effective. Western nations, including the US and the CDC, quickly promoted the WHO as the standard for COVID practice and information. Disagreeing with or speaking out in opposition to WHO measures quickly became heavily discouraged on online platforms, and would even cause physicians, nurses, and pharmacists to lose their jobs. The California Physician Misinformation Act of 2022 attempted to have doctors lose their medical license for promoting information that contradicted the WHO.
The new Pandemic Treaty seeks to force countries to make laws enforcing the WHO pandemic plan. Aspects of the treaty include the restriction of “misinformation”, the automatic granting of licenses and liability waivers for vaccines, and surveillance of personal medical and social media information. It would also require an international vaccine passport.
In an interview with Kim Iversen, Dr. Meryl Nass argues that the treaty would violate the 1st, 4th, 5th, 10th, and 14th amendments to the US Constitution.
Given the terrible record of the WHO and the CDC during the pandemic, especially for restricting free communication. I absolutely oppose a WHO lead pandemic treaty.
Will the US adopt such a treaty? It’s hard to say right now. The current makeup of Congress suggests that it might be difficult to get a treaty passed, especially since a two thirds vote is necessary to ratify a treaty in the Senate. The President can make an agreement by executive order, but a future president can reverse this order just as easily.
The US vaccine mandate suggests that the Federal Government, some states, and many companies may implement many aspects of the treaty whether or not the US agrees to it. Remember that President Biden announced that he intended to issue a vaccine mandate in September of 2021. Details weren’t released until November that year, and the Supreme Court actually struck down the mandate before it could be implemented in January of 2022. So in actuality, the mandate never actually existed. Despite this, many states, federal agencies, hospitals, and companies implemented aspects of the mandate voluntarily, with Federal pressure never officially exerted. This is a bad sign for the WHO pandemic treaty.
The good news for some is that the 10th amendment may allow states to ignore an agreement if they want. The 10th amendment states “The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.” On the other hand, a treaty ratified by congress has the force of federal law and may bind the states. It remains to be seen how the Supreme Court would weigh an official treaty ratified by Congress against measures that would violate the constitutional rights of individual citizens.
A note on the words “treaty” and “agreement”. In the US, a treaty has the force of law and must be ratified by congress. An agreement can be made between any 2 parties, but does not legally bind anyone else. News outlets have been using “treaty” and “agreement” interchangeably, and the official name for the draft document from the WHO is “the WHO Pandemic Agreement”. Given that the WHO wants the agreement to carry the force of law, they really mean “treaty”. The confusion may be intended.
As I have stated many times before, the censorship of physicians, scientists, and others during the pandemic crippled our ability to respond correctly to the pandemic. Many, including me, lost trust in the CDC and the medical community as a whole. I regard this as one of the worst aspects of the US pandemic response, and particularly bitter for me as a member of the medical community. The WHO Pandemic Agreement would codify the worst aspects of the US COVID response.
As the May vote nears, write your representatives, both at the federal and state levels, and let them know if you want the agreement implemented in your area.
This is a brief case update and some good news about the AB 2098, the California Physician Misinformation Act.
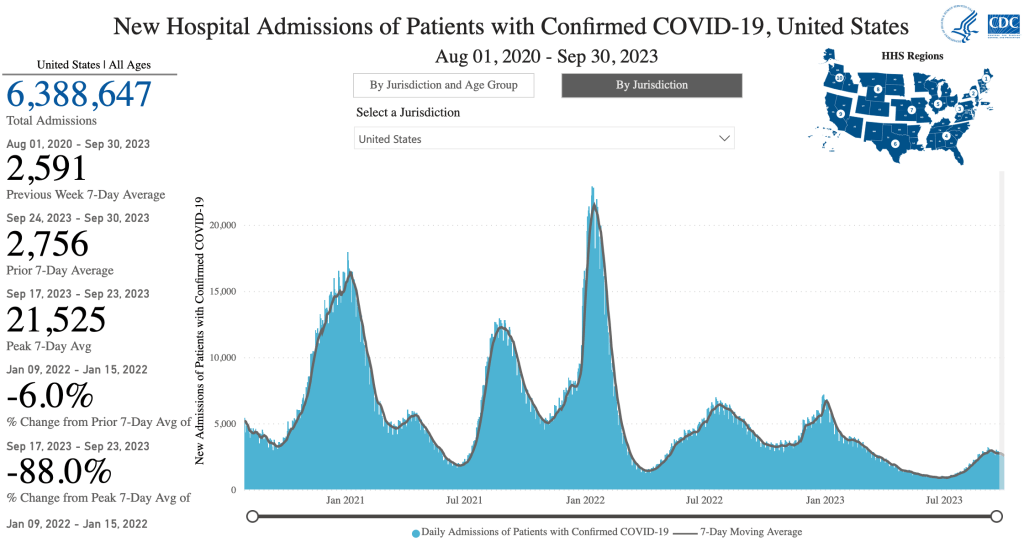
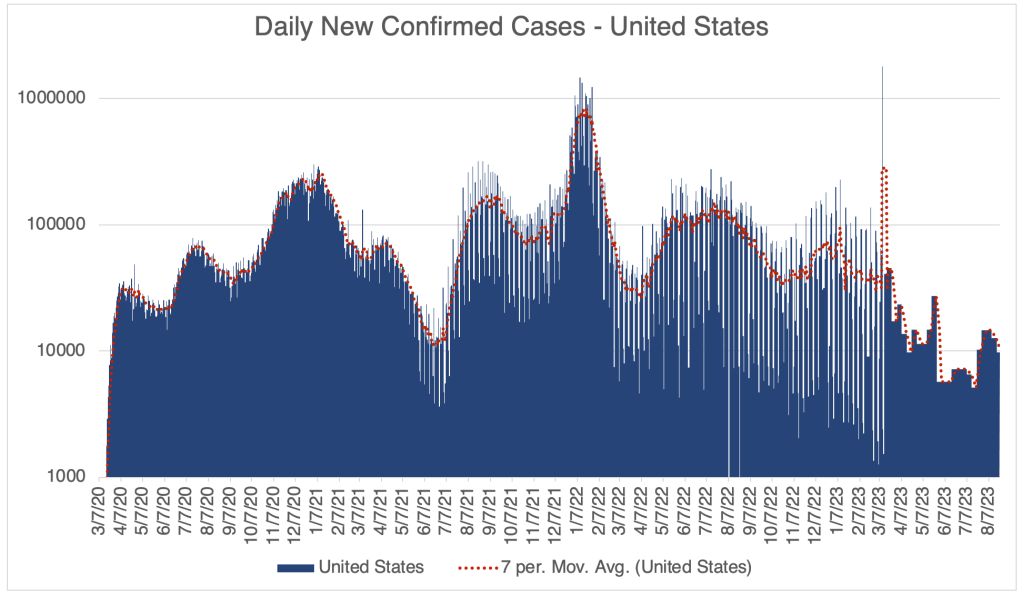
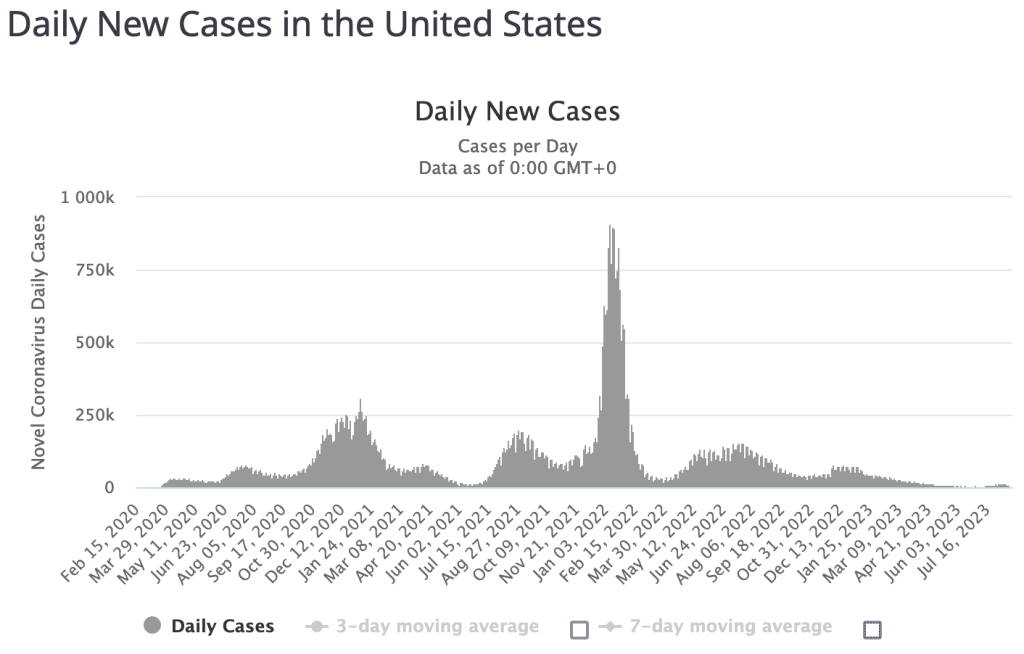
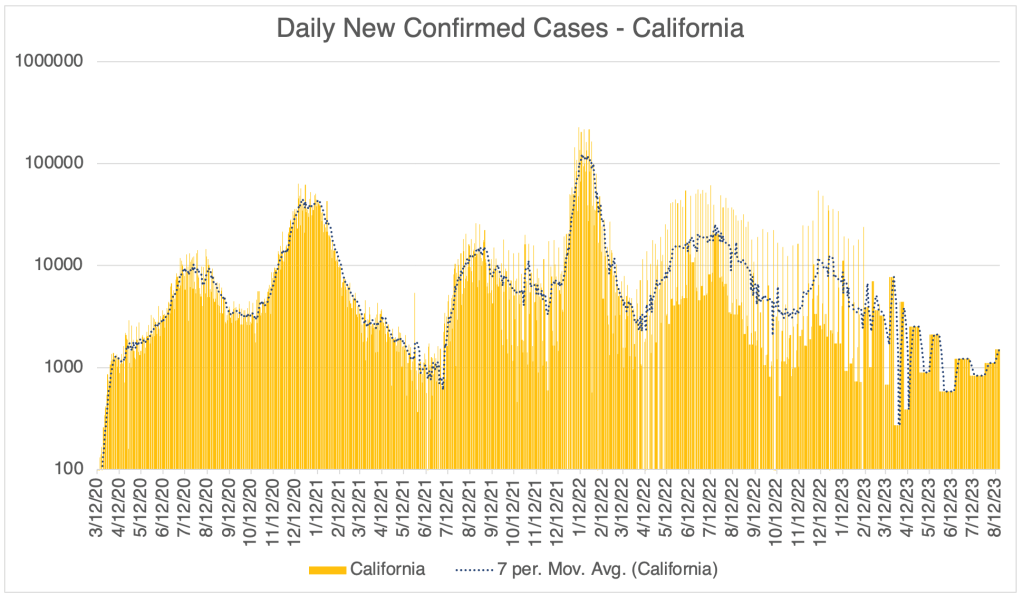
Case Update: The Fall 2023 wave is on a downslope, with cases going down in the US, California, and San Diego County. As discussed before, there was legitimately an increase in cases, but the number of new cases was tiny in comparison to previous waves. Given the large amount of pre-existing natural immunity, I never considered the current wave to be a serious threat to public health.
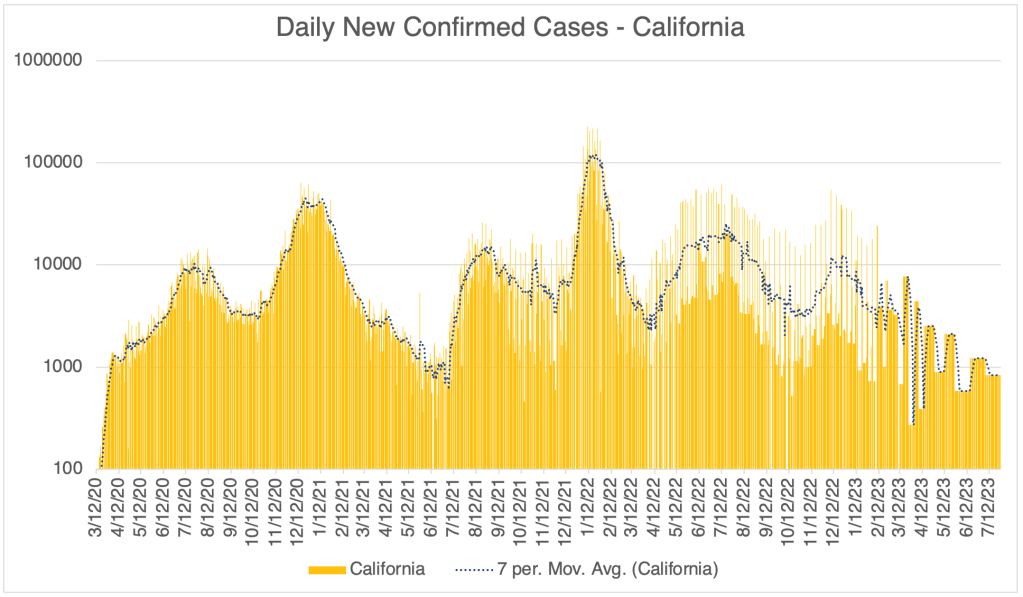
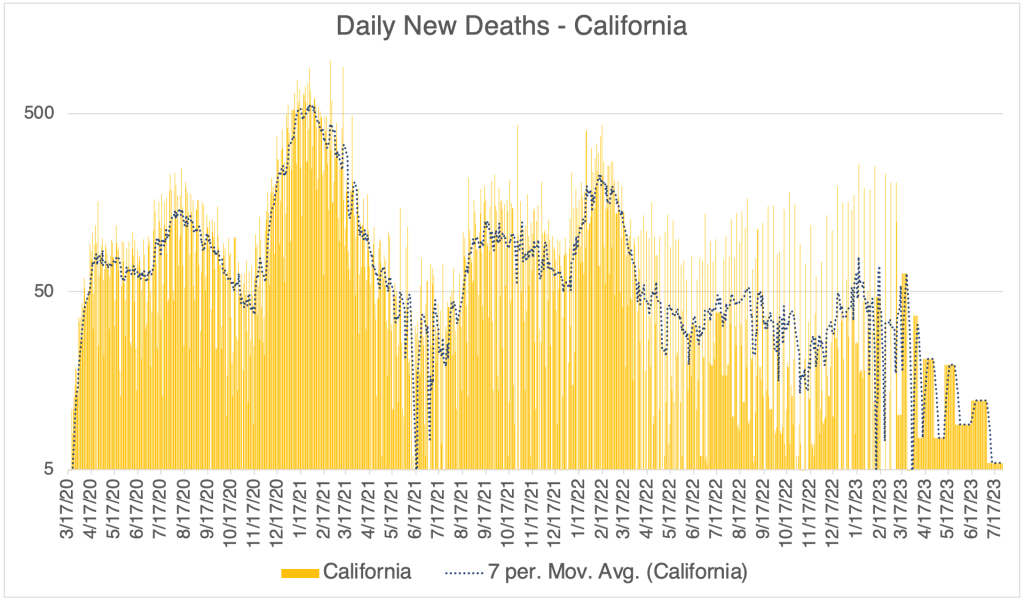
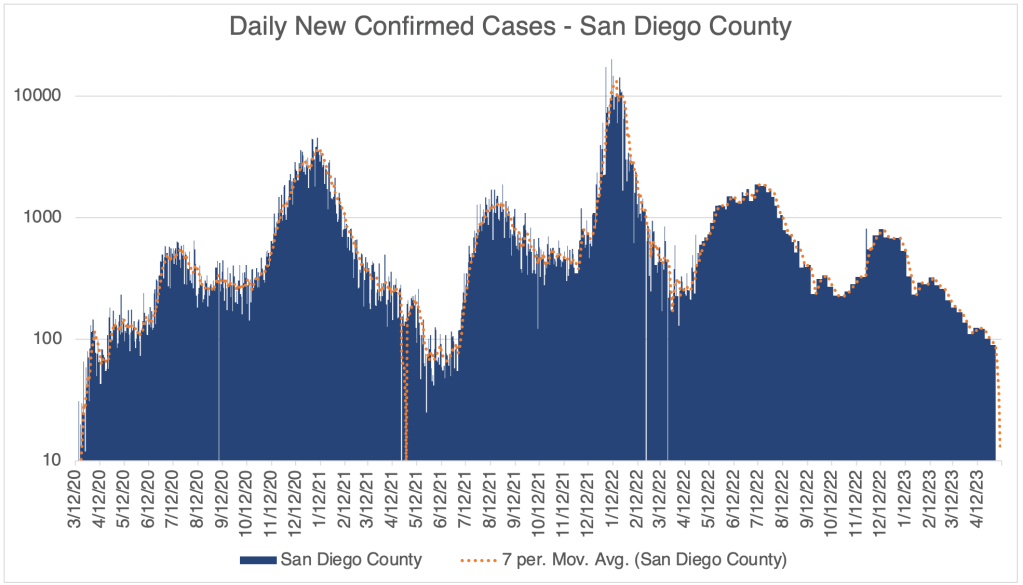
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format. Data since March 10, 2023 is from Worldometer.Hospitalizations, from the CDC website.The current EG.5 wave barely registers on the far right of this linear graph. Daily US New Cases, Worldometer/coronavirus/us.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.From the CDC page on Variant Proportions for the United States. Updated for September 30th, 2023.
The Repeal of the California Physician Misinformation Act: Last October, I wrote about a new California law which made “misinformation” a cause for physicians in California to lose their medical license. Misinformation was defined as “false information that is contradicted by contemporary scientific consensus contrary to the standard of care.” As I argued, it is common for new scientific ideas to be opposed by the majority of scientists before gaining acceptance.
The new law immediately became a target of legal action, one case being Høeg vs Newsom. On September 29th, 2023, Høeg’s attorney filed a request that the law be permanently barred from enforcement. Just a few days later, on October 1st, California Governor Gavin Newsom signed a repeal of the law. This is great news for California physicians and patients. California physicians are again free to communicate to their patients without fear of losing their license. This is also great news for the cause of freedom of speech in the US.
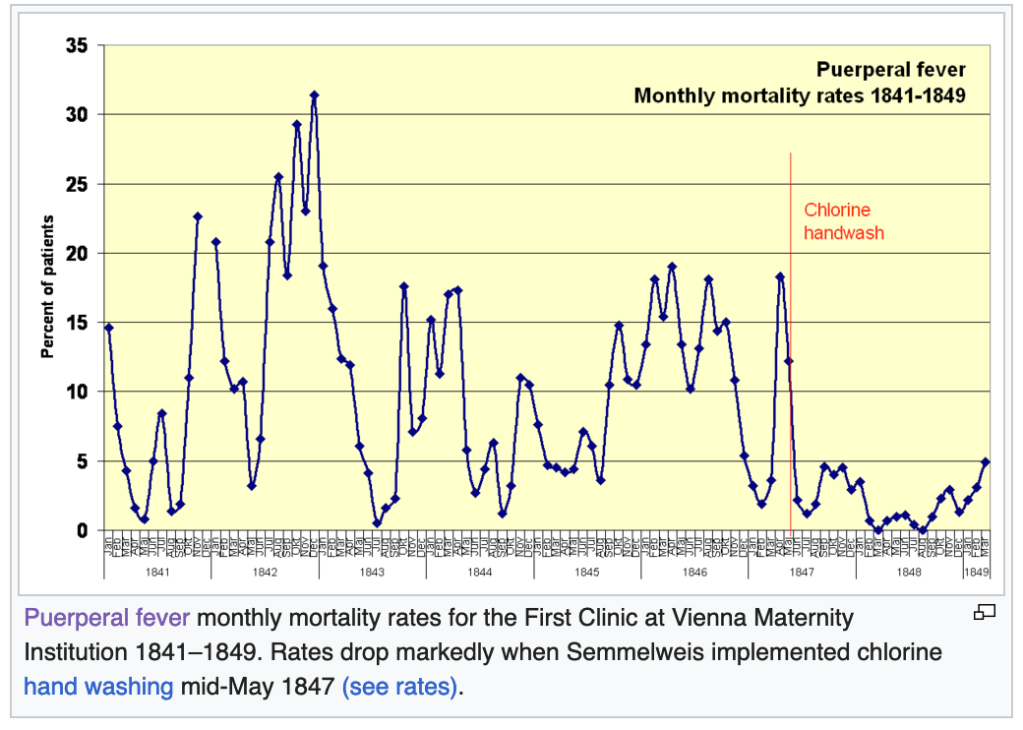
The fascinating yet tragic case of Dr. Ignaz Semmelweis:Ignaz Semmelweis was a physician at Vienna General Hospital in 1847. One of his jobs was to deliver babies in the maternity ward. Unfortunately, in his ward, the rate of fatality for new mothers was high, an average of 18.3%. Women were afraid to deliver in his hospital, and begged to deliver somewhere else!
Then one day, a colleague of Dr. Semmelweis died of Puerperal Fever, with symptoms very similar to the women in the maternity ward. His colleague had nicked himself with a scalpel while performing an autopsy on a cadaver. Dr. Semmelweis thought that maybe the fatalities in the maternity ward had something to do with the fact that Doctors where going straight from performing autopsies to delivering babies!
At this point, you’re probably holding your head and saying “What!?”, perhaps with some other colorful words added in. It’s obvious to us now that this was a terrible idea, but the Germ Theory of Disease had not yet been accepted in medicine. The field at that time had no idea that microscopic organisms could transmit disease.
Dr. Semmelweis started having physicians wash their hands in a chlorine solution after performing autopsies. The maternal death rate fell immediately to below 5%, some months having zero deaths. Dr. Semmelweis tried to tell others of his findings, but no one believed him. After increasingly passionate and ultimately embarrassing behavior, his friends and family had him committed to a mental institution. He was abused by guards and died in 1865.
That same decade, Louis Pasteur and Robert Koch were producing evidence supporting the Germ Theory, and Joseph Lister began popularizing the use of anti-septic procedures in surgery, greatly improving outcomes for surgical patients. Semmelweis’ ideas would be vindicated, but not until after his tragic death.
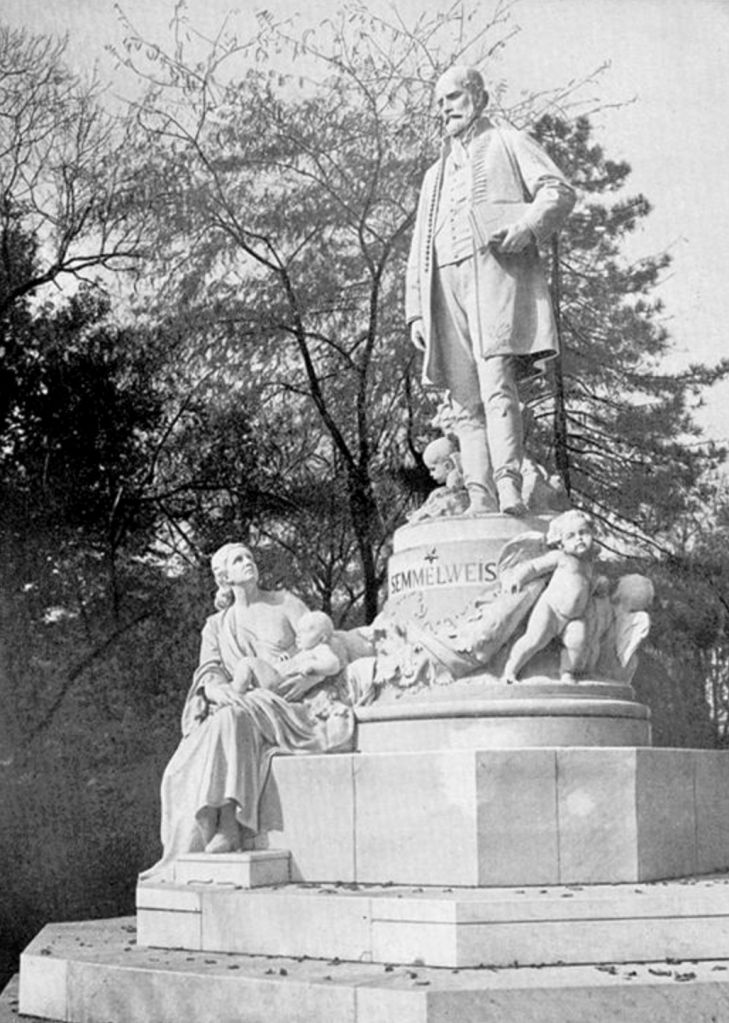
Semmelweis is now considered a hero of modern medicine, having a university, several hospitals, and even an asteroid named after him.
Statue of Semmelweis in front of Szent Rókus Hospital, Budapest, Hungary (erected in 1904, work of Alajos Stróbl). From the Wikipedia page for Ignaz Semmelweis.
Why did I tell this story? Under a law similar to the California Physician Misinformation Act, people like Semmelweis would have lost their licenses. Semmelweis’ story underscores the need for strict adherence to the Scientific Method, not the suppression of “misinformation.” We suppress unpopular ideas at our peril.
I have a case update, and also some news about a new variant, EG.5.
There has been a significant uptick in new cases in the US, California, and San Diego County in recent weeks. However, since cases have recently been very low, the uptick in cases still results in very few cases by pandemic standards, as many as we had in Spring of 2021 before Delta came around. Arguably, these new cases are already starting to subside.
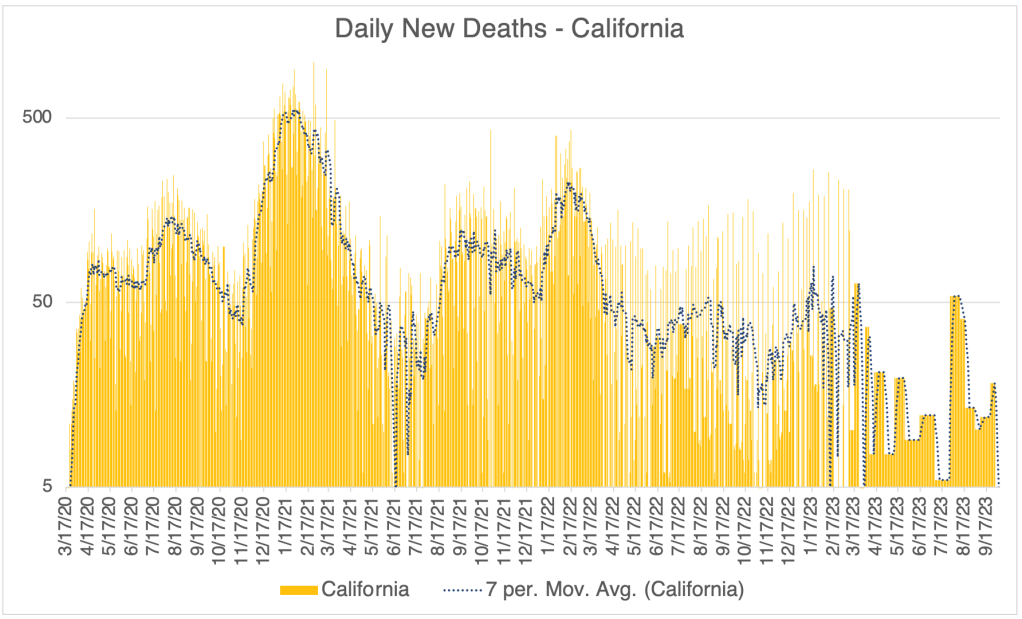
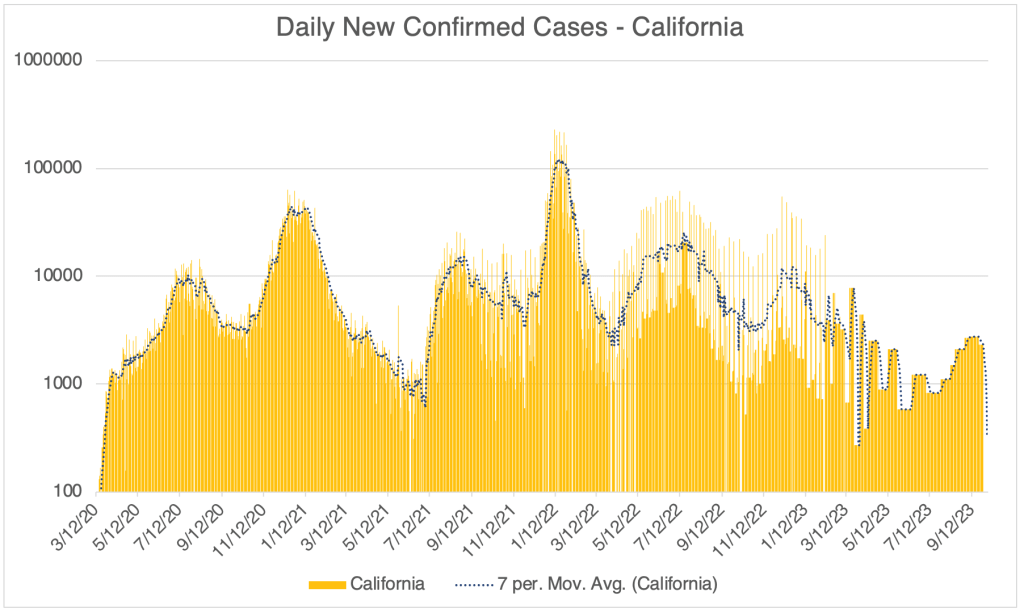
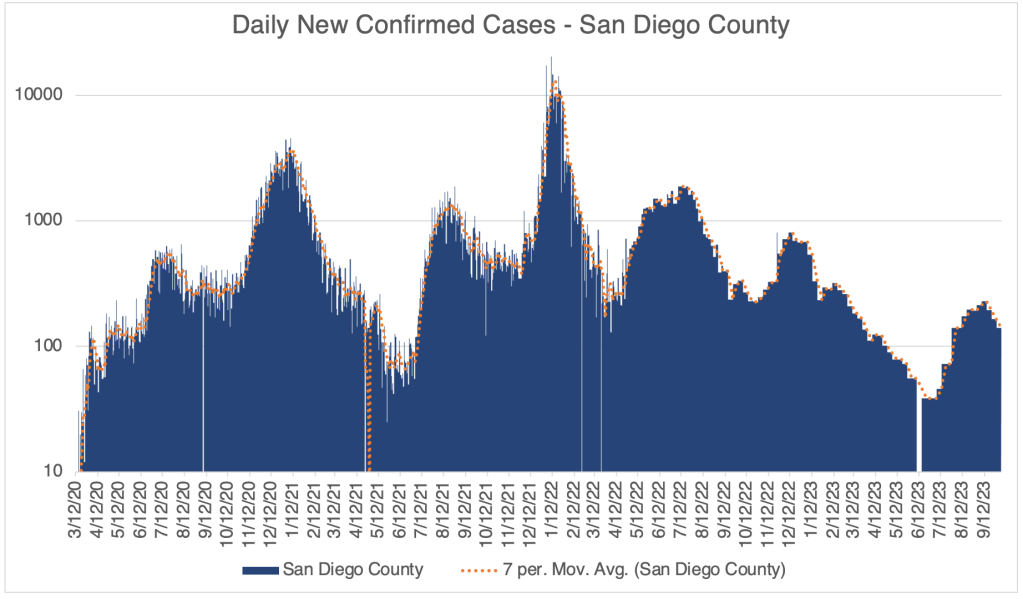
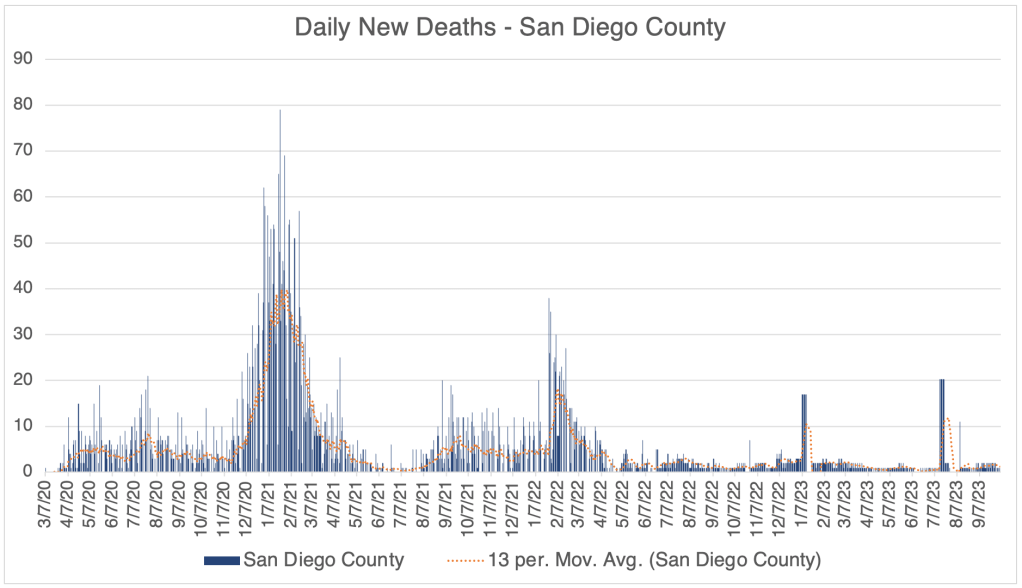
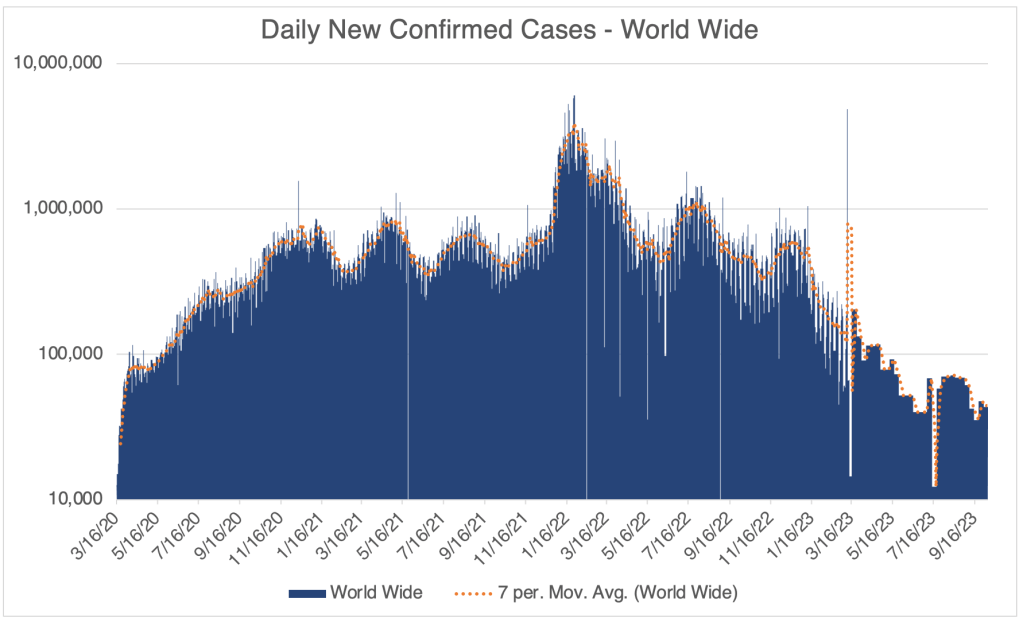
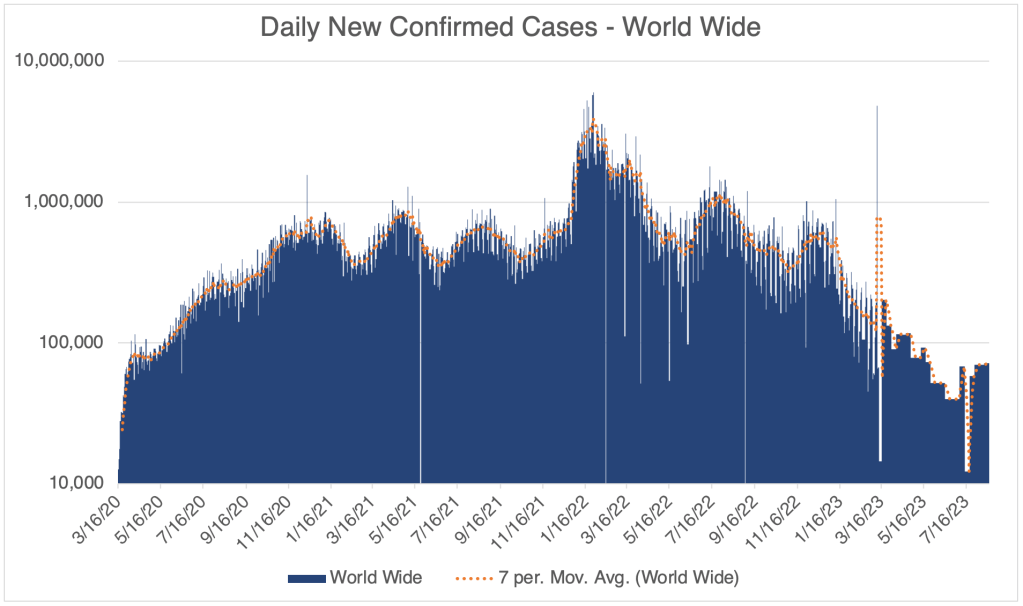
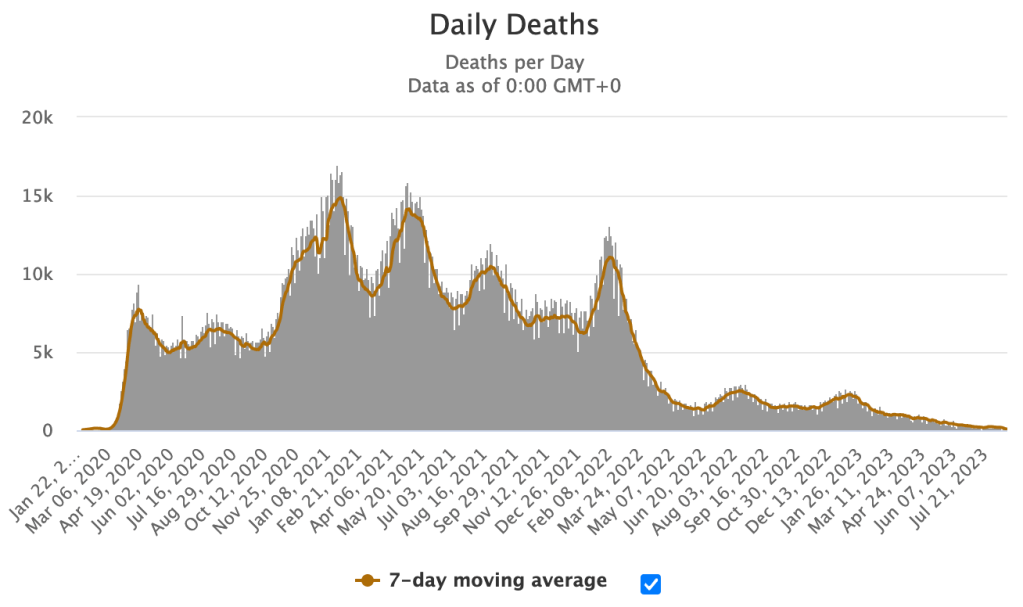
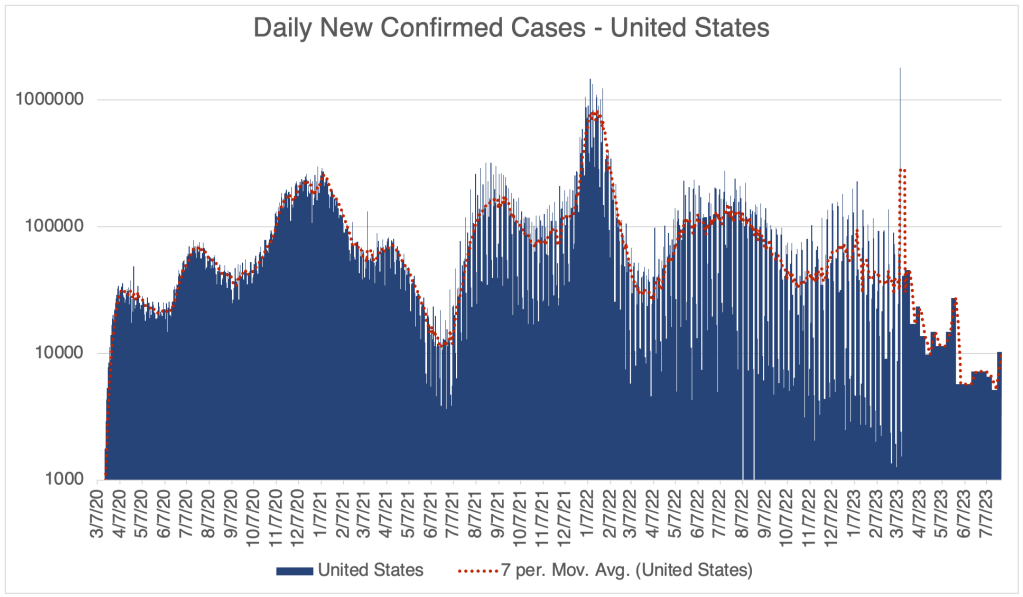
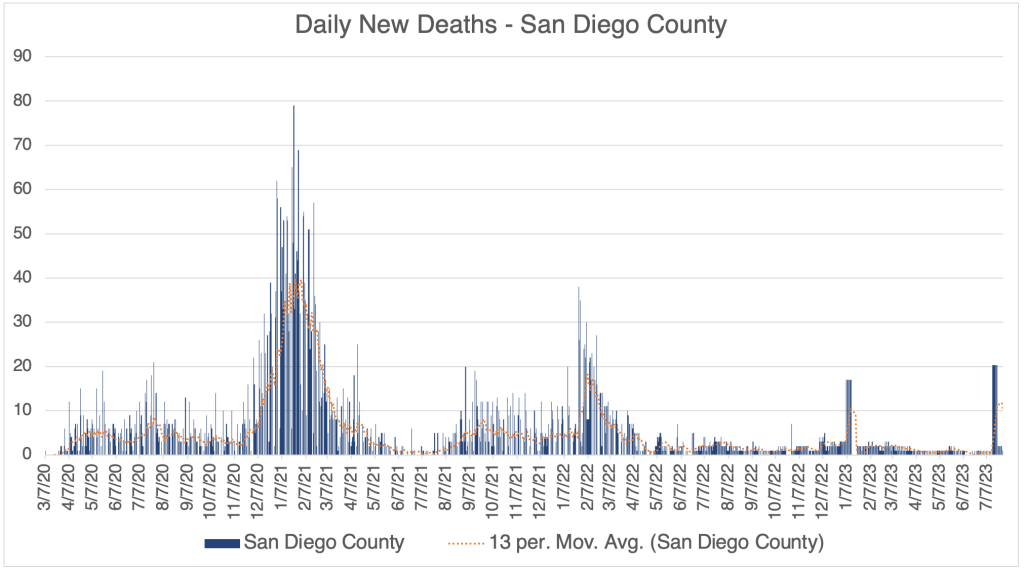
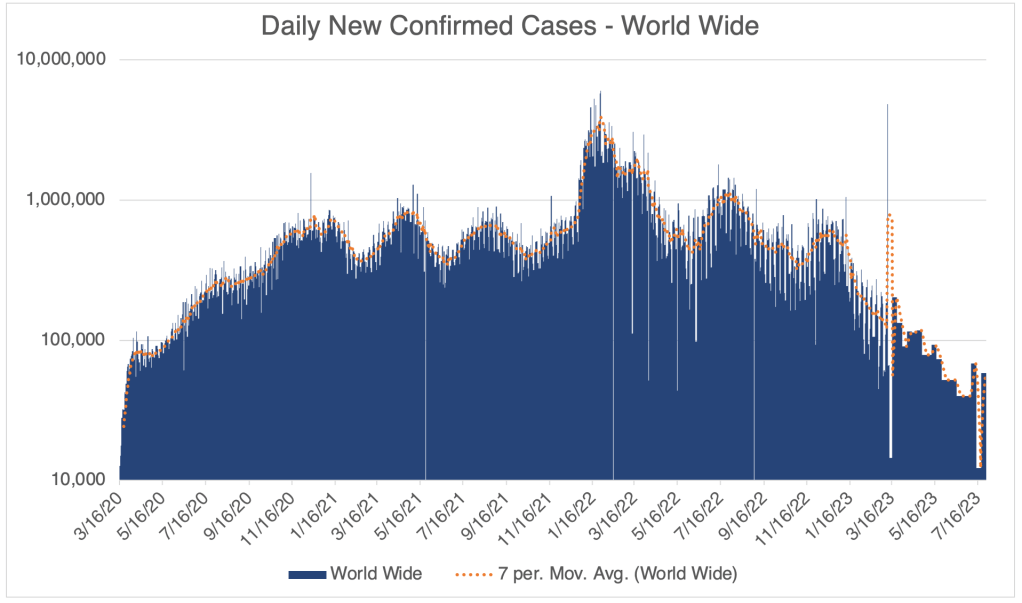
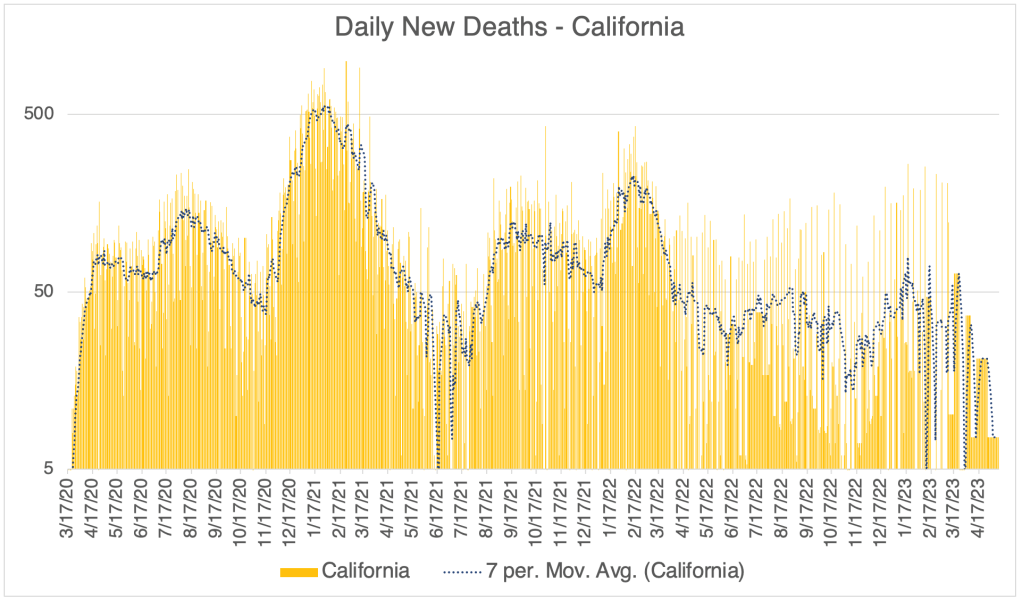
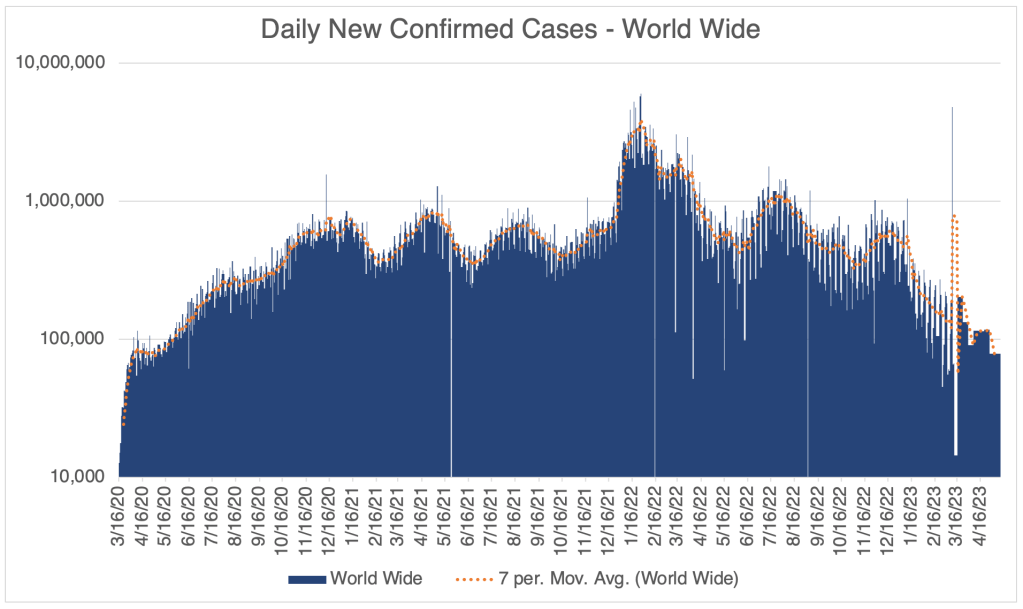
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Hospitalizations, from the CDC website.The current EG.5 wave barely registers on the far right of this linear graph. Daily US New Cases, Worldometer/coronavirus/us. Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information. Apparent spike in deaths in July 2023 likely represents a glut of cases reported all at once.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.World Wide Daily COVID Deaths, Worldometer/coronavirus.
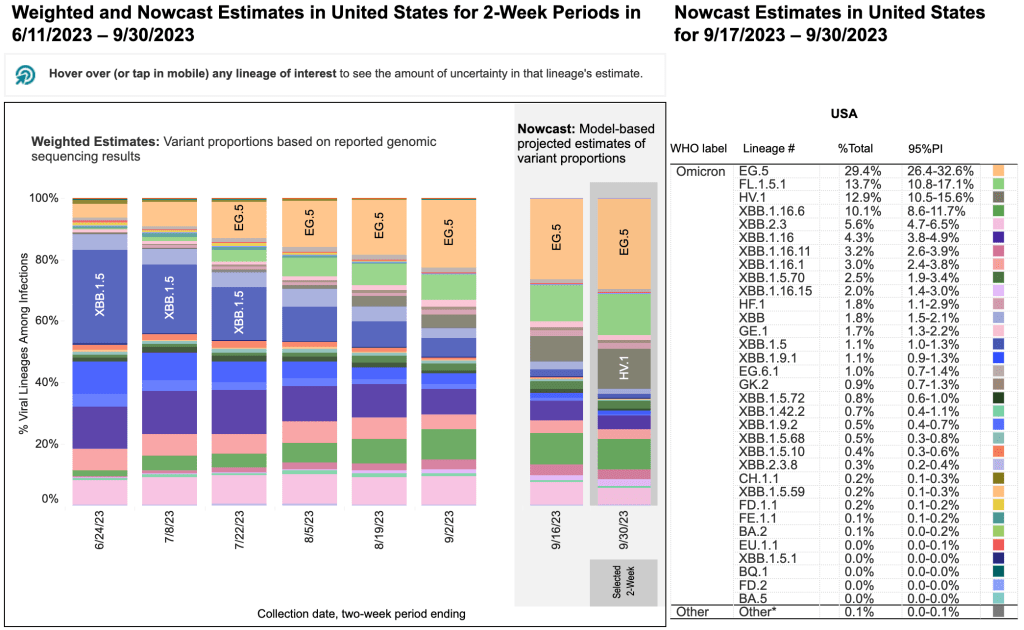
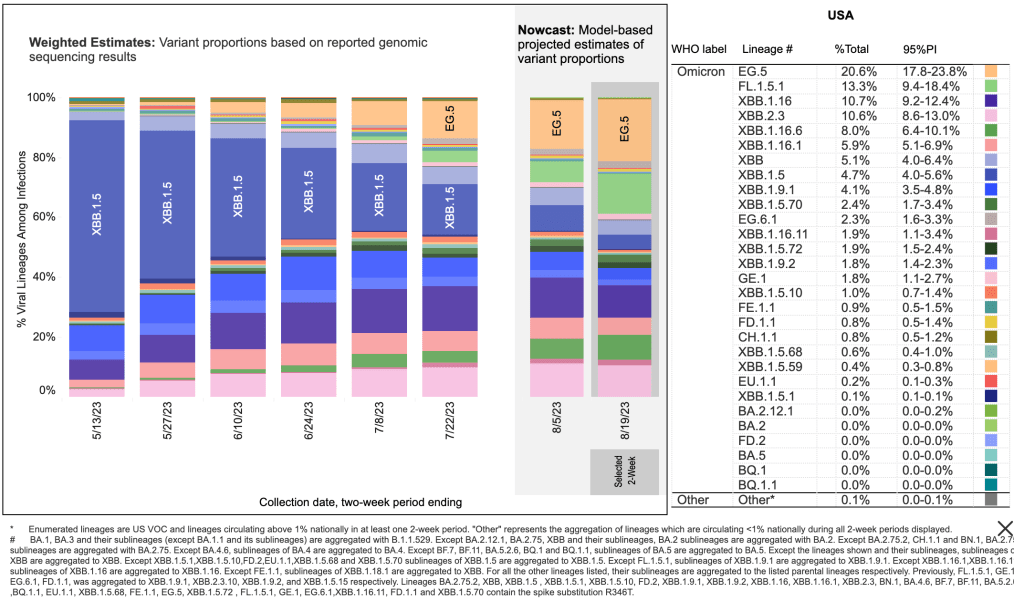
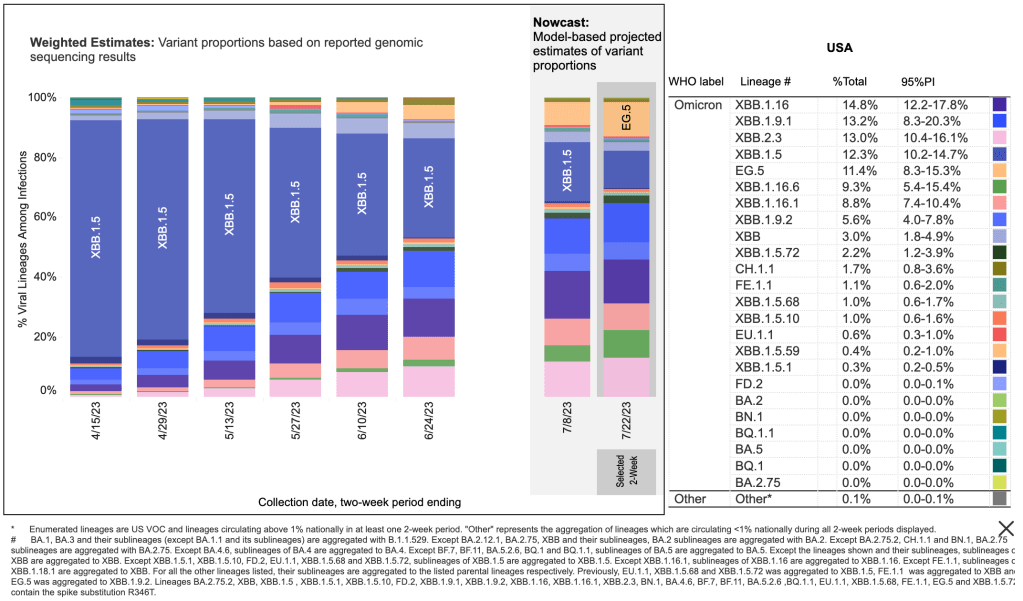
Variant EG.5 Why is this news? Rumors are circulating that this represents a dangerous new wave of COVID cases. Indeed, a new variant is currently spreading that many do not seem to have immunity to. Variant EG.5 has been spreading since May and now represents a majority of new cases. In fact several universities including Rutgers and Brown are bringing back COVID mandates, as well as some Hollywood studios.
From the CDC page on Variant Proportions for the United States. Updated for August 22th, 2023. EG.5 currently represents 20.6% of new cases.
Should you be concerned? There is not yet any evidence that EG.5 is any deadlier than other mild Omicron strains. If you’ve already had COVID, you needn’t be concerned. EG.5 may simply represent a free booster for you.
If you haven’t had COVID yet, I can no longer recommend a vaccine or booster for anyone, even those of you at high risk. If you’re concerned about getting COVID, I suggest wearing an N95 style mask while indoors in public. The mask must fit snugly, and must filter air coming into your nose and mouth. Do not wear a blue surgical mask. Blue surgical masks are not useful for preventing Omicron infection.
Don’t fear, but be smart, Erik
_______________________________________________ Update: September 1st, 2023
Is Pirola a concern? No, not really. While the new variant may evade the immune symptoms of many, infection appears to cause the same mild symptoms as a common cold, just like other recent Omicron variants. As for EG.5, those with natural immunity need not be concerned. As with EG.5, if you’re concerned about getting BA.2.86, I suggest wearing an N95 style mask while indoors in public. The mask must fit snugly, and must filter air coming into your nose and mouth. Do not wear a blue surgical mask. Blue surgical masks are not useful for preventing Omicron infection.
It’s been more than 2 months since my last post. Today, I’ll give a little update on new cases, plus a collection of brief but interesting stories. Michael Shellenberger claims to have interviewed 3 “patient zeros” from the Wuhan Institute of Virology. Then I’ll discuss a study from the Cleveland Clinic on booster effectiveness, a report from John Campbell on adverse events from vaccines, and a story about excess deaths pointing to vaccine injury, supported by another video from John Campbell.
I am only collecting data once a week now, just to monitor new cases, so my graphs are pretty low-resolution. New COVID cases are as low now as they were at the very beginning of the pandemic, even lower than the Spring of 2021 before Delta arose and spoiled the party. New deaths due to infection are also very low. There was an apparent spike in new deaths in San Diego County in mid-July, but this may have represented a bunch of hospitals reporting at once, and not a spike in actual deaths.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Daily COVID Deaths, World Wide, Worldometer/coronavirus.
A new Omicron variant, EG.5 is rising in prominence, but this new variant is apparently no deadlier than other Omicron variants, so is not of great concern.
3 “Patient Zero”s identified:Journalist Michael Shellenberger claims that the identities of 3 “patient zero” individuals are now known, and all of them worked at the Wuhan Institute of Virology. These people were likely the very first people in the world to be infected with SARS-CoV-2. One of these individuals is Ben Hu, the 2nd in command at the WIV, and someone who was directly involved in Coronavirus research. Shellenberger was not shocked to discover that the initial patients were from the WIV. Rather, he was shocked and dismayed that he had to discover this for himself, rather than the information be released by the WHO, the CDC, the FBI, or a number of other agencies who should have informed the public. Shellenberger is now 100% convinced that the SARS-CoV-2 virus came from the lab in Wuhan.
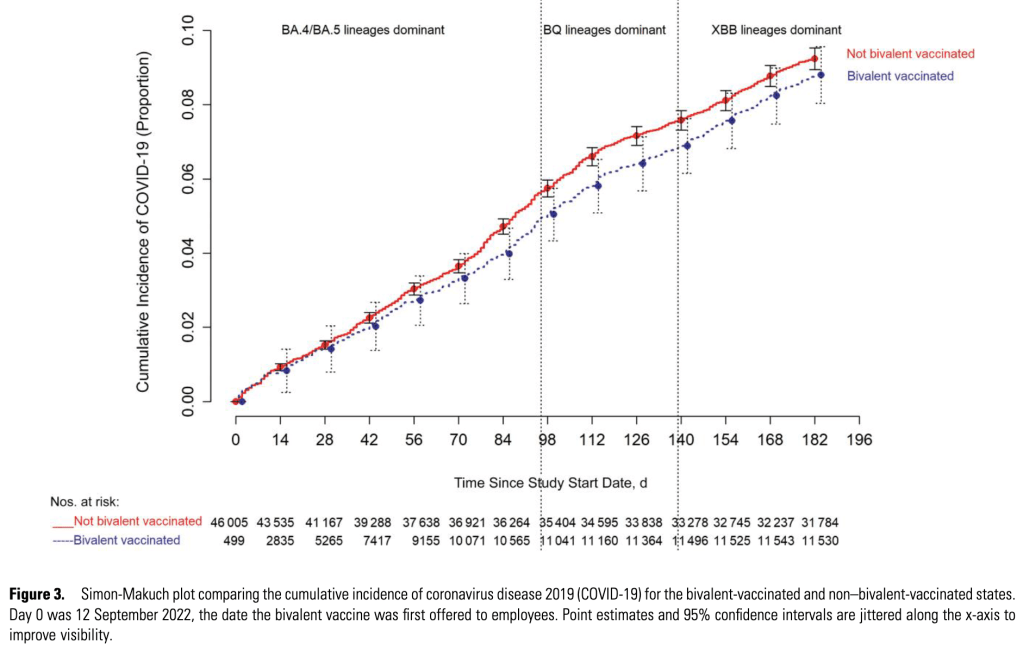
Boosters increase likelihood of reinfection: A study from the Cleveland Clinic claims that the likelihood of reinfection with COVID-19 actually increases with more vaccine boosters. The study began in the Summer of 2022, during the BA.5 outbreak, and shows increased likelihood of infection by later variants the more boosters a person had! It’s unknown why this phenomenon occurs, but it may be a mechanism similar to Antibody Dependent Enhancement (ADE) which I was concerned about early on. Happily, available data doesn’t appear to show that ADE has caused more severe symptoms in COVID patients.
The paper also shows that the new Bivalent boosters, containing both the original Wuhan strain and an Omicron strain, has only a mild benefit to prevent infection.
Adverse events were batch dependent: A paper from a lab in Denmark appears to show that the number of adverse events associated with vaccines, referred to as “suspected adverse effects” (SAEs), were dependent on the batch in question. Adverse events appeared to cluster in 3 groups, some vaccine batches produced very few events, while others produced thousands. This difference probably contributed to the confusion and the difficulty of identifying real problems. The worst batches produced adverse events at a rate of almost 9%, and also produced the most severe effects.
These results should provide some clues as to what went wrong with the vaccine rollout. Unfortunately, this data comes from cases in Denmark so is less relevant to the US. This is the kind of information that is the CDC’s job to produce. The fact that the CDC is not producing data like this is a big worry, and shows that the agency is in dire need of reform.
Excess deaths may be related to vaccine induced inflammation:Ed Dowd was on the Dr. Drew podcast. Dowd has an interesting take on adverse events. He is an analyst for an investment firm, and looks for trends to help in making investment decisions. He often uses information from insurance claims to analyze trends in worker health, illness, accidents, and death. He noticed that in the UK, there were approximately 500,000 excess deaths in both 2021 and 2022, many among younger people. This effect was correlated to being in the Millennial generation and being employed. He says that in late 2021, excess deaths among Millennials was 84% above normal.
He says that hematological (blood related) illnesses were up 522% in 2022, during the time when Omicron was dominant. That’s 61 standard deviations above the expected trend. For those of you who know statistics, you know that this is far, far, above what you would expect for a random event. Dowd is asking physicians to help his team interpret this data.
At this point, it seems unlikely that we will get accurate information on adverse events in the US. Unfortunately, the CDC is too politicized to perform its function.
I’m not a physician. But in my informed opinion, there is no longer a benefit to getting a COVID vaccine booster, even if you are at high risk.
The pandemic is officially ending today in the US. Also, I’ll give a case update.
The CDC has announced that the state of emergency due to the COVID-19 pandemic is officially ending at the end of the day today, May 11, 2023. This will end all federal restrictions for travel, as well as make some regulatory changes to testing, treatments, and funding. Some things are not changing, and the list of changes is complicated. Most people have been behaving as if the pandemic is basically over in my area for many months now, and you may not notice any differences to your life.
Most scientists agree the SARS-2 virus is now endemic, and will continue to circulate. Those with natural immunity will probably not be effected by this, and new cases of COVID will be mild for most. If you are one of the few who haven’t had COVID yet, you may want to continue to take precautions, but most even high risk people I know have chosen to go back to normal life.
Case update: There are still cases around, but the numbers are low, and we haven’t had a big wave of deaths since the Omicron variant arrived in December and January of 21/22.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Hospitalizations, from the CDC website.From the CDC page on Variant Proportions for the United States. Updated for May 6th, 2023.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. Data since March 10, 2023 is from Worldometer.Daily COVID Deaths, World Wide, Worldometer/coronavirus.
As I stated above, the SARS-2 virus is now endemic, and we’ll probably never be completely rid of it. But it’s significance will continue to decline as new variants continue to become less pathogenic, and the human population continues to build resistance.
I’m going to re-post my lessons from the pandemic below.
This is NOT a case update! In fact, there may be no more case updates from me!
In another sign that the pandemic is basically over, Johns Hopkins University announced that as of 5:21 am, March 10, 2023, they would no longer refresh their COVID page which supplied so many of us with current COVID information. This page was regarded by most to be the most authoritative repository of COVID information, although it depended on governmental bodies to supply them with information. With this resource gone, anyone wanting to keep track of data will need to go to less authoritative or less convenient sources.
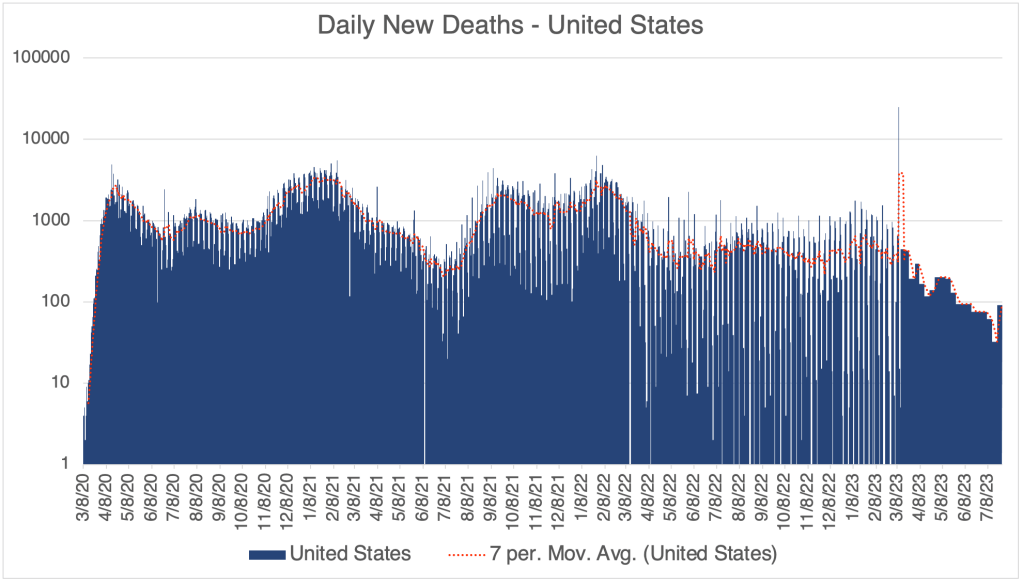
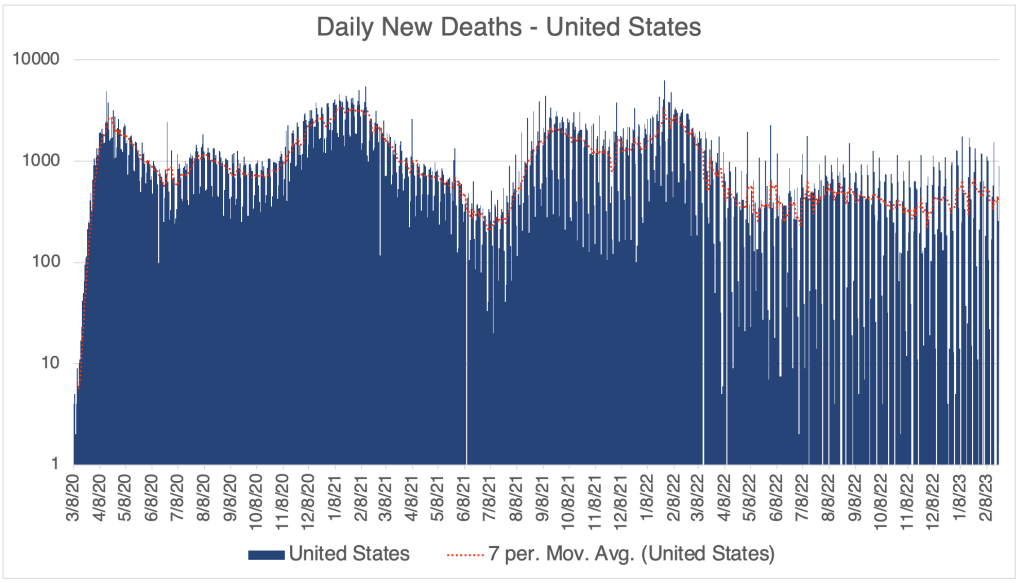
Since the rise of Omicron, COVID hasn’t been nearly as deadly as previous variants. So after December and January of ‘21/’22, there has not been a big deadly wave of cases. Despite this, many news outlets continued to talk about the next big variant as a source of concern. My primary reason for my updates in the last year has been to simply show you that while cases may ebb and flow, deaths were not really on the rise. I wanted to give you the raw data so you could see this for yourselves.
Now that the JHU site will be going away, I’ll probably post even less, or maybe not at all, only when newsworthy items appear. If an issue arises involving case numbers, I’ll try my best to find good information, perhaps from Worldometer, to pass along.
In the future, just remember that viruses tend to become more infectious and less pathogenic over time. So when some news source comes out and talks about how terrifying a new variant is because it’s so infectious, just realize it’s also probably less pathogenic than previous versions. If you’ve had COVID before, it most likely won’t be a concern for you at all.
By the way, some of you may wonder why I don’t comment on some of the COVID related news that comes out. Usually, this is because I’ve written about it before, or because I don’t really have anything new to add to the conversation. I’ve always wanted to be as concise and impactful as possible, and so I’ve kind of avoided the “Water is Wet” stories. If you want me to cover something in particular, feel free to reach out.
Don’t fear, but be smart, Erik
____________________________________________ Update: March 14th, 2023
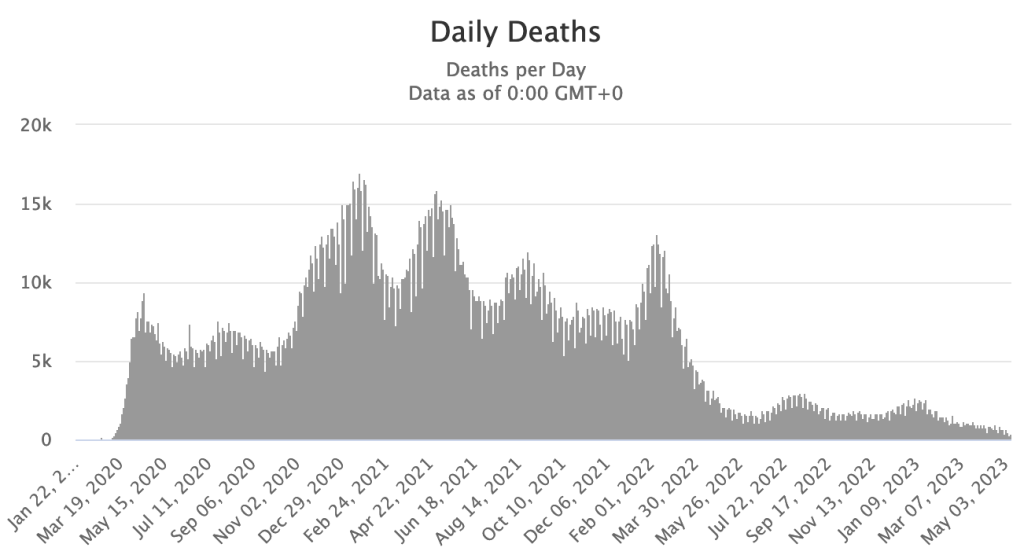
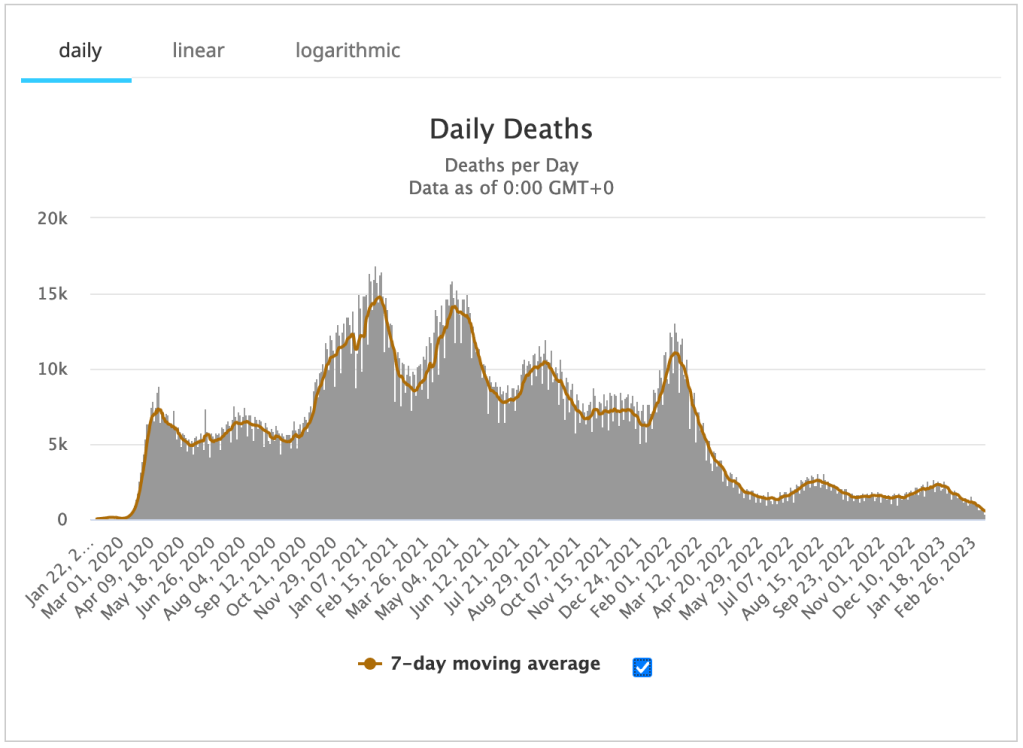
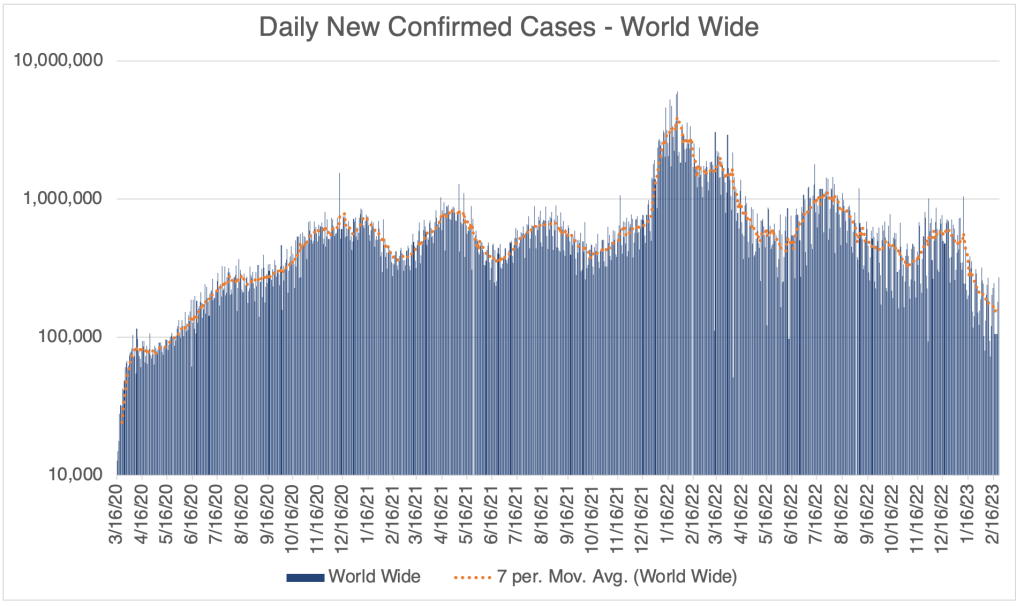
A brief post with another piece of good COVID news that I’ve never noticed before. I was just looking at Worldometer‘s graph of Daily COVID Deaths world wide, a number I haven’t been tracking. Notice how low daily deaths have been since just after the Omicron variant appeared in late 2021. After a big spike that Winter, deaths have been much lower world wide. Truly, Omicron washed Delta away and likely saved many lives! Amazing!
This is a COVID Update. I’ll also talk about a recent meta-study by Jefferson et al about mask effectiveness.
The Winter wave is over. Cases in the US, California, and San Diego County are about at the same level as they were in October. This the mildest COVID winter season since the pandemic started. COVID related deaths increased modestly during this time, but are now relatively low but persistent.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.From the CDC page on Variant Proportions for the United States. Updated for February 18th.From the CDC page on Variant Proportions for the United States. Updated for February 18th.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.
World wide, cases are as low now as they were way back in the Summer of 2020. Of course, I have to mention that testing was not as available in 2020 as it is now. On the other hand, many people currently are testing themselves with over the counter tests, and don’t report the results to the medical system, so there is a lot of uncertainty as to the actual number of cases.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.
Cochrane Report on the Effectiveness of Masks: Jefferson et al released a meta-study through Cochrane Reviews on the effectiveness of medical masks (surgical masks) and medical respirators (N95) in public settings. A meta-study is a study in which the authors gather information from published articles and try to draw conclusions from a large body of data. They do not gather a new set of data.
The Jefferson et al study reviewed 78 different studies, including data from pre-COVID flu outbreaks. Their conclusions are sobering. First, the authors suggest that there is virtually no benefit to wearing a medical surgical mask over not wearing a mask in most settings. If you’ve been reading my blog for long, you will know that this conclusion does not surprise me. Blue surgical masks have large gaps in the sides and do not filter air leaving the mouth and nose. They were designed to prevent droplets from a medical worker from contacting a patient, not to prevent transmission of aerosol based agents. This is a problem, since most mask wearing people in public during the pandemic were wearing surgical masks. These people thought they were protected from aerosols, but they were not.
The study also concludes, however, that N95 masks didn’t perform much better. In fact, for lab tested COVID, the difference was statistically insignificant, meaning that the difference between wearing N95s or surgical masks was so small, it could not be proven to be a real difference statistically.
I have to point out that the Jefferson meta-study points out that many of the studies they reviewed had various failings that may have made them unreliable. Much of the data was collected through self-reporting of participants, which is a source of inaccuracy, and participants were often non-random, making application to the general population difficult. So some of the conclusions may have suffered from these kinds of errors.
As you know, I’ve been a proponent of wearing N95, KN95, or KF94 masks when indoors during the pandemic. Unfortunately, N95s are tight and intolerable for most people for long periods, so most people didn’t want to wear them at all. Those that did were not careful to make sure the mask fits properly, making the mask ineffective. This is part of the reason I wore a KF94 (Korean) during the later stages of the pandemic when I had choices.
So have I been wrong this whole time? Well, yes and no. I wore a KN95 in all kinds of environments while traveling during the pandemic. When I finally got COVID in January of 2022, I was not wearing my mask, working in a “gray area” environment with people that I later found out had COVID. I was technically indoors, but the room had a lot of ventilation, so I thought I would be OK. Obviously, I was incorrect. All this to say, I think my KN95 was effective for much of the pandemic. On the other hand, I am a scientist in the infectious disease field, and have had a lot of experience wearing and fitting these masks to myself, so I am not a typical user. It may certainly be that my experience does not translate to non-scientists.
If you still have not had COVID and are not high risk, I might say that the current version has an extremely low fatality rate, and it may now be worth the risk to say good-bye to the mask. I know the large majority of you have done this already.
If you are at high risk, I still think an N95, KN95, or KF94 can be effective for you. In order for it to be effective, however, you need to make sure it is properly fitted, making sure you don’t have gaps between your nose and cheek. The mask should filter the air coming into your nose and mouth.
Since I had COVID last January, I no longer wear a KN94, and enjoy eating indoors in restaurants again. I’ve basically been back to normal for a long time.
Happy New Year! I have a brief COVID update for you. Then I’ll talk about a new variant, XBB.1.5. I’ll also have comments on a smattering of evolving stories, like California AB 2098, “Physicians and surgeons: unprofessional conduct”, and a new Twitter Files thread on vaccine misinformation.
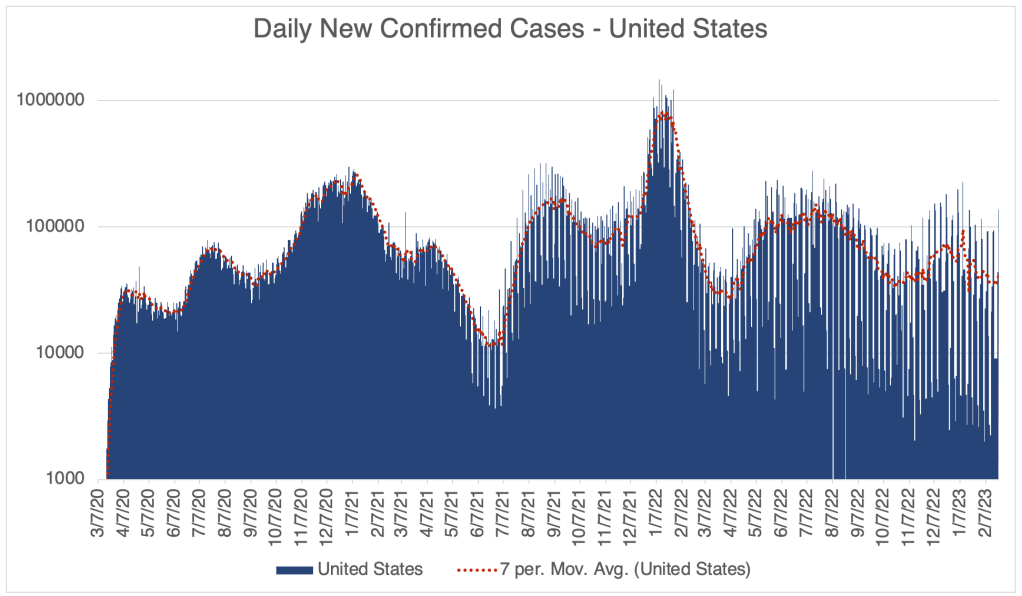
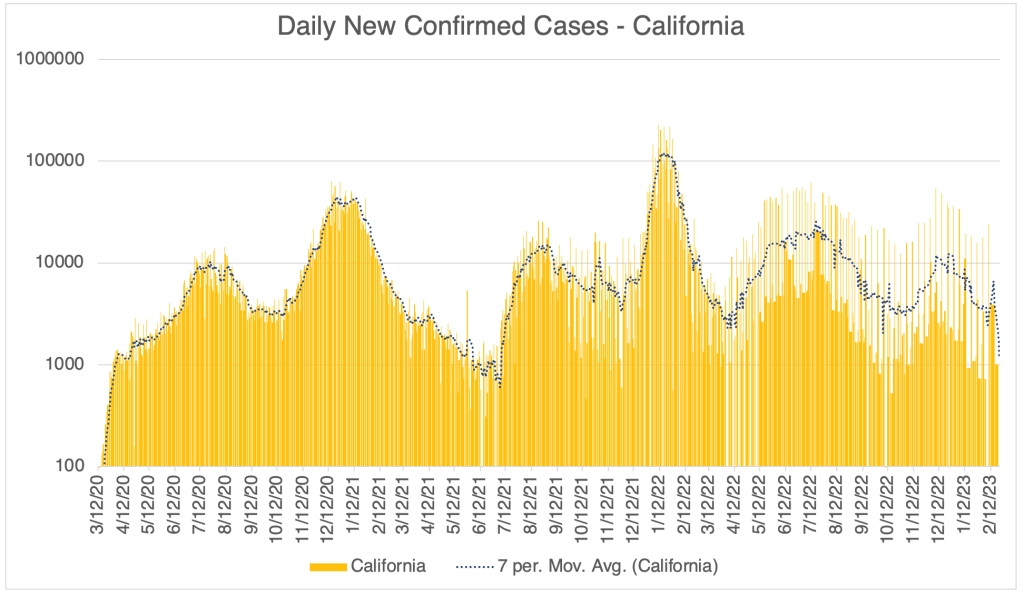
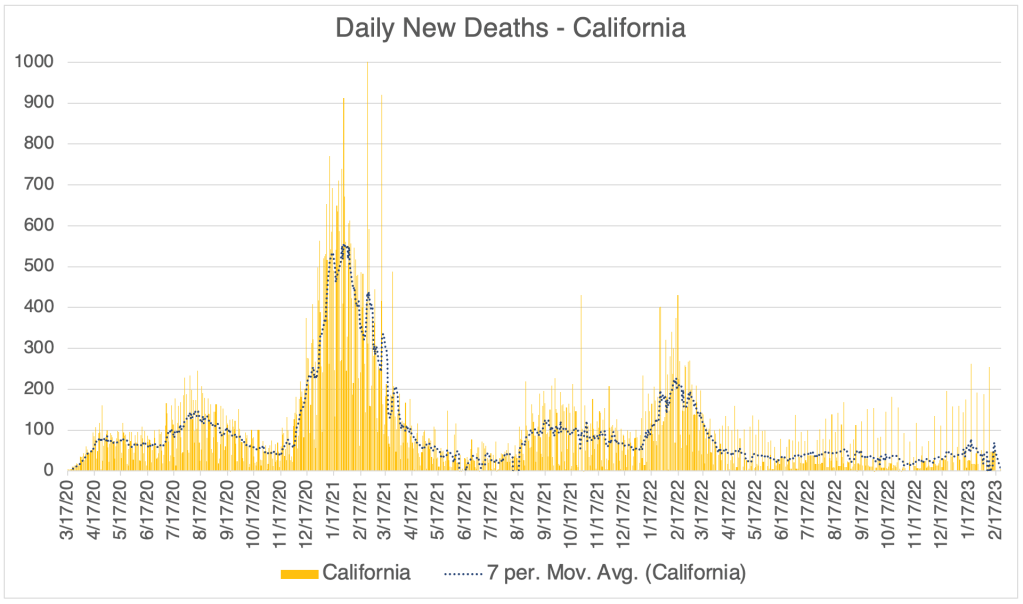
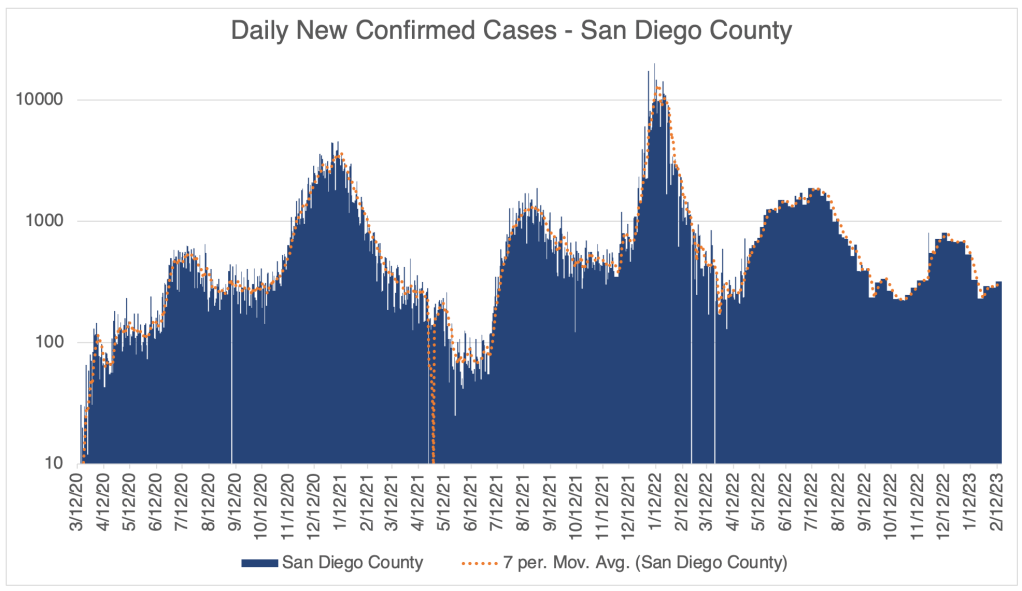
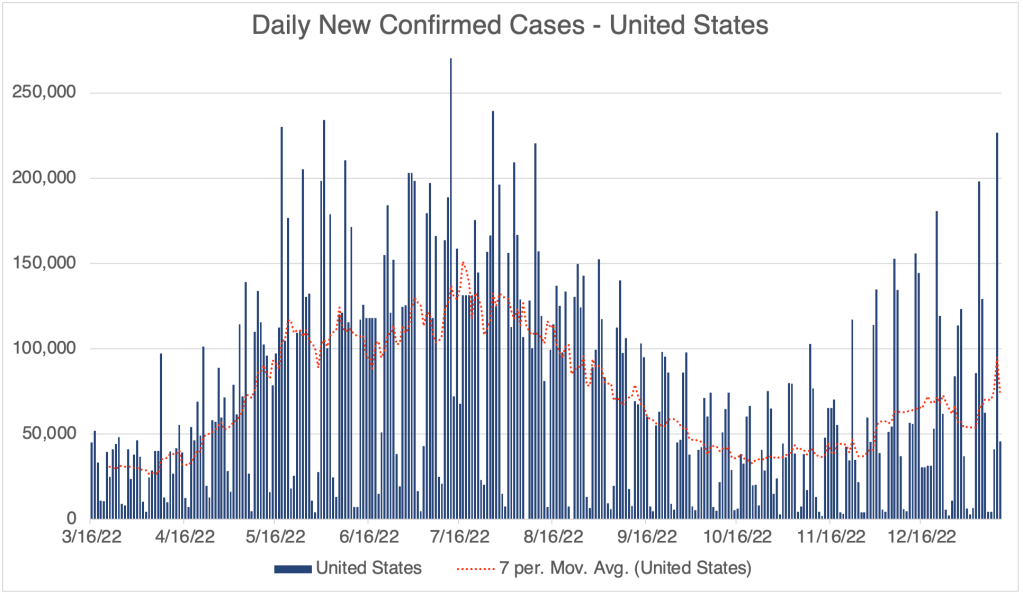
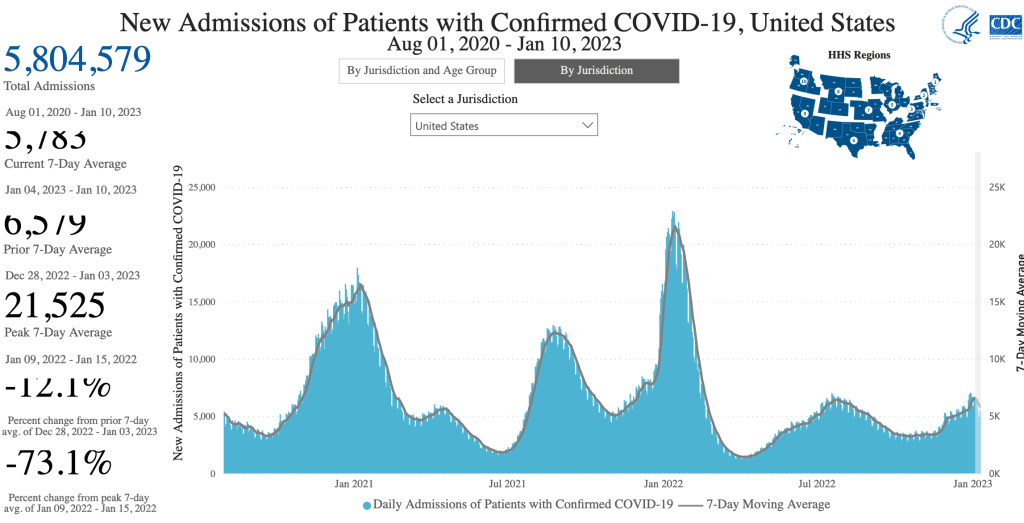
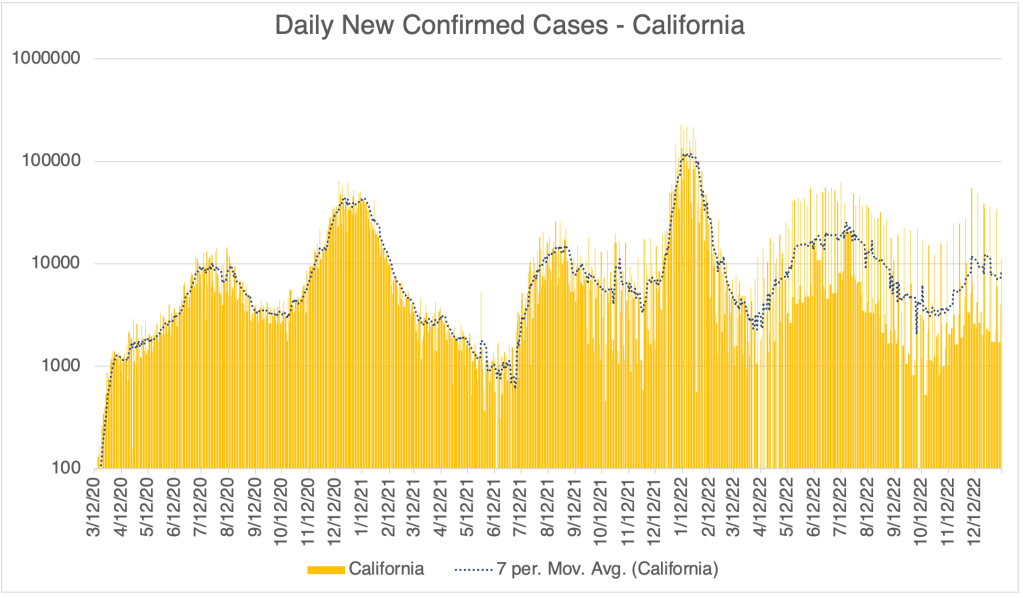
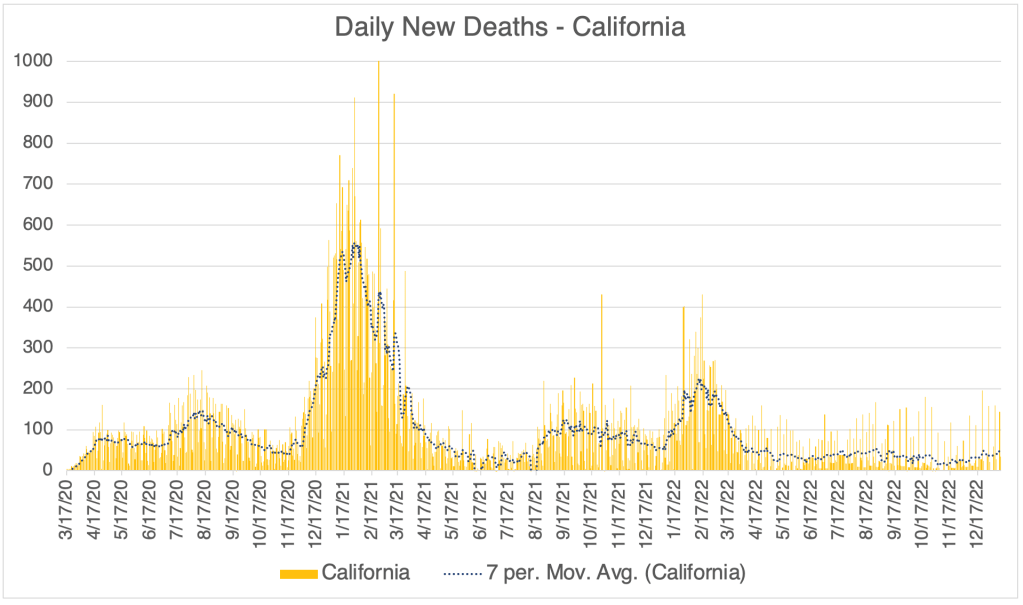
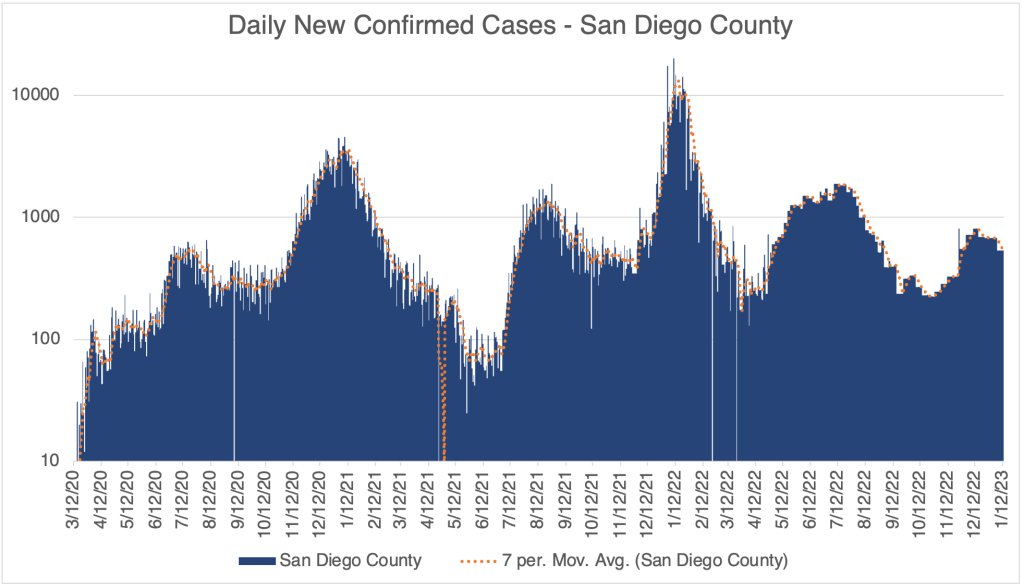
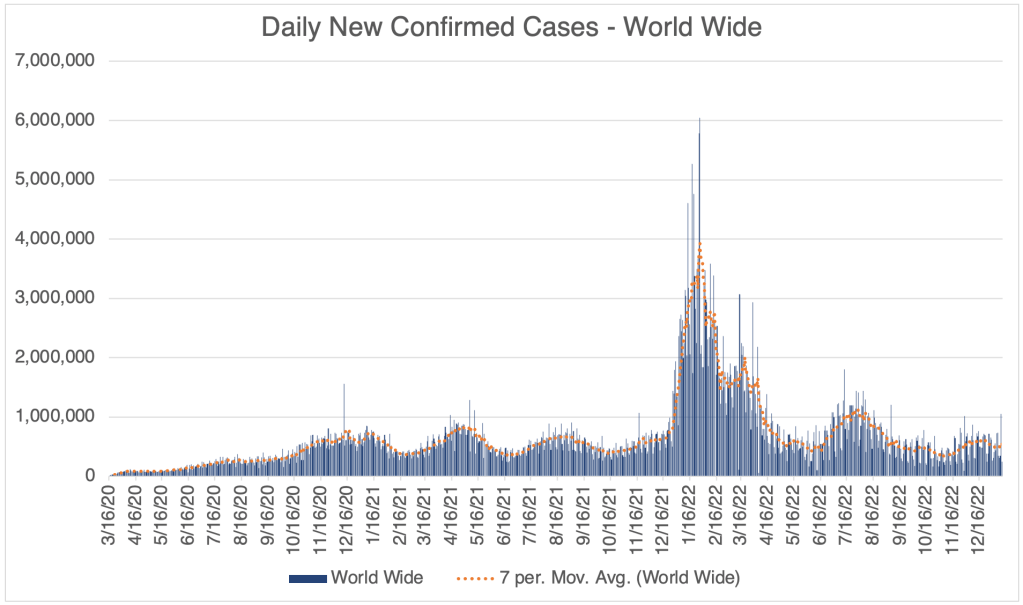
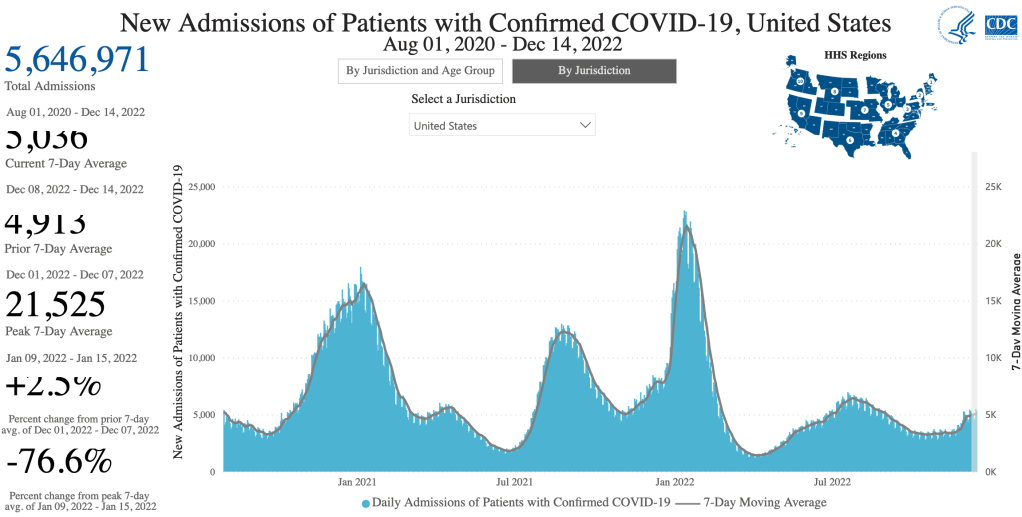
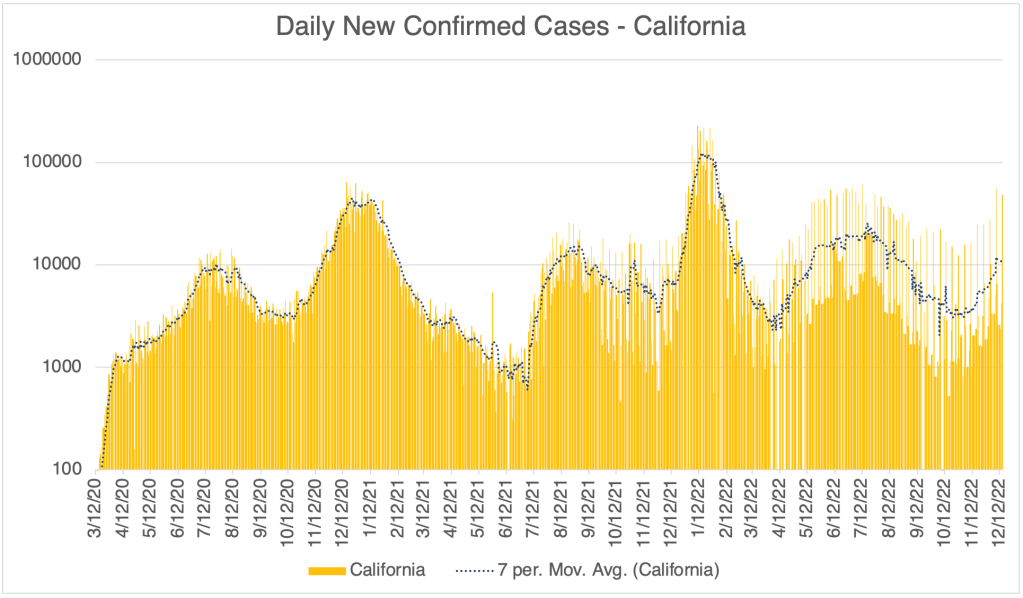
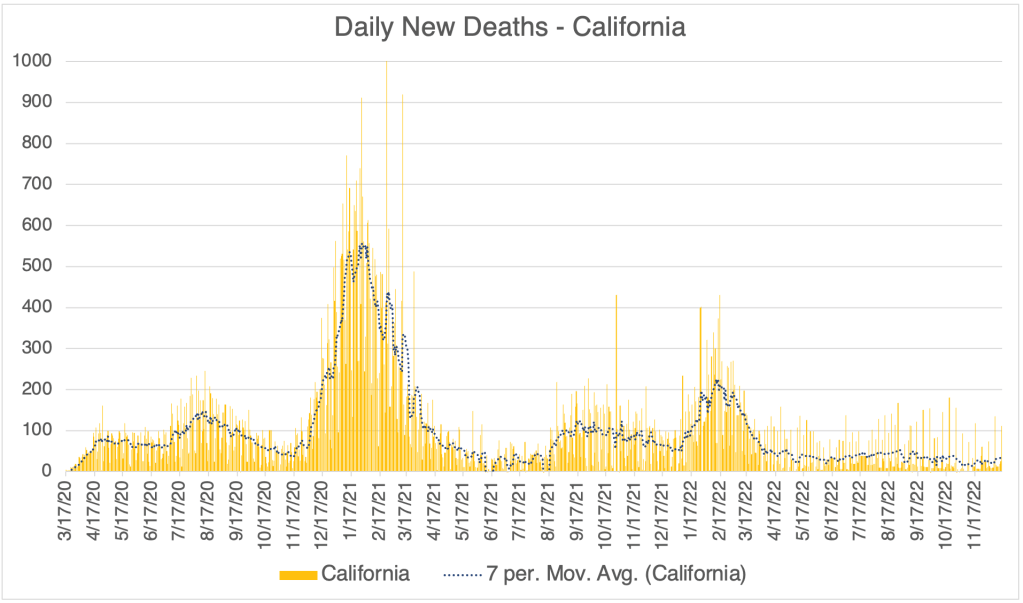
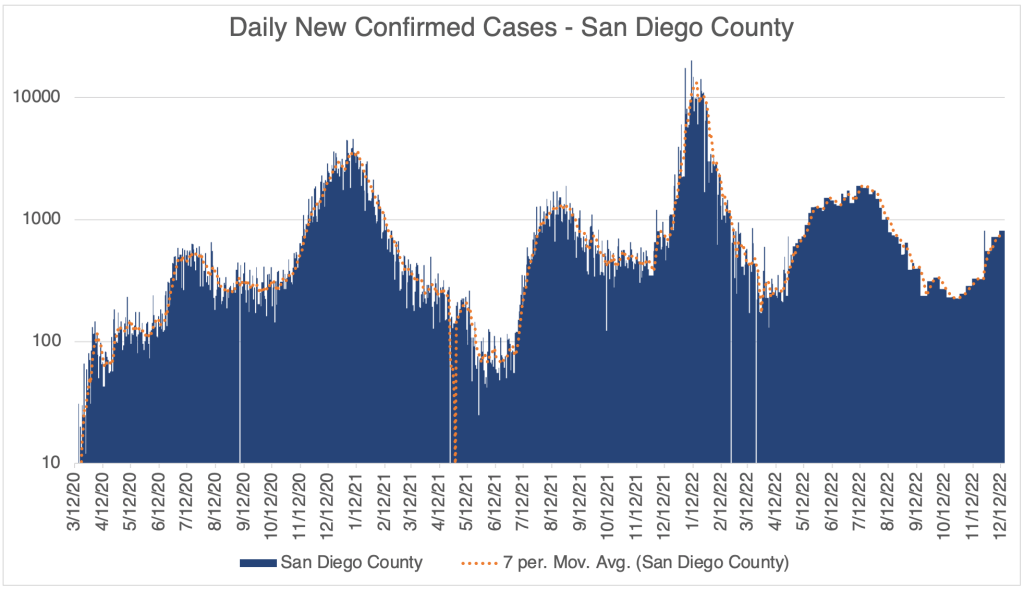
We have already reached the peak of the December wave. Cases in the US, California, and San Diego, and even world wide, peaked at around Christmas. Deaths never really had a peak during this December wave, except in San Diego County.
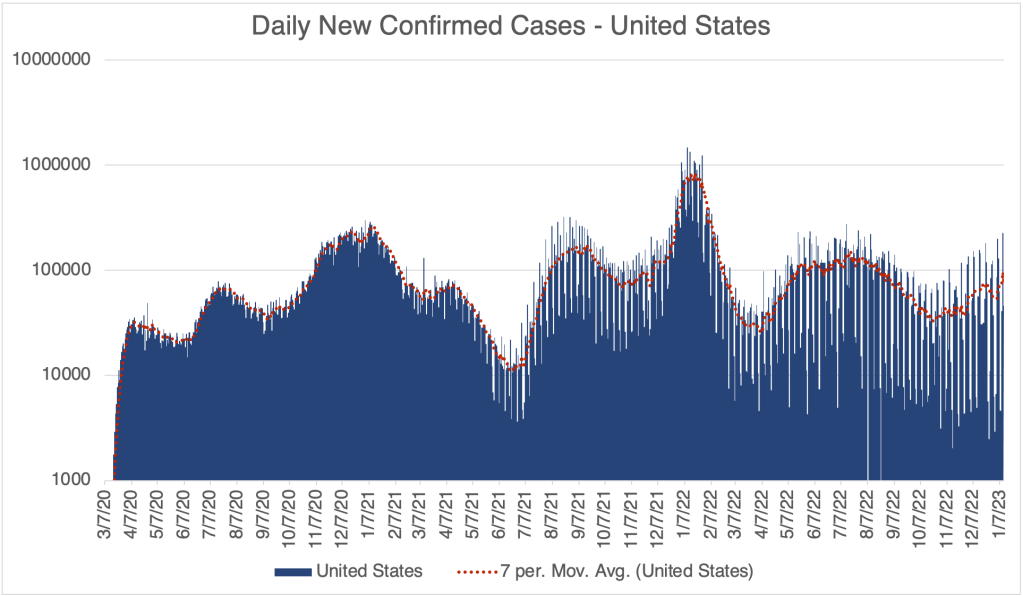
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Daily Confirmed Cases – United States, March 16, 2022 to January 12, 2023. Peak of the first Winter Wave was on around Christmas Day. We may already be seeing the start of an XBB.1.5 peak. Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
However, we may see a second Winter wave this year…
New Variant XBB.1.5: A new variant is spreading extremely rapidly in the US right now. Variant XBB.1.5 is about 43% of the SARS-2 virus in the US right now. A UK study suggests that this new variant is the most transmissible yet. John Campbell, in another excellent analysis, suggests that about 80% of us will get it. Antibody studies suggest that even those with prior COVID infections do not produce many antibodies that can neutralize XBB.1.5, so even those who have had COVID before are likely to get it again. The good news is, XBB.1.5 is another Omicron strain, and will produce very mild symptoms in the vast majority of cases. I’ve had COVID twice already, and I will treat XBB.1.5 as a chance to get a free booster.
From the CDC page on Variant Proportions for the United States. Updated for January 14th.From the CDC page on Variant Proportions for the United States. Updated for January 14th.XBB.1.5 is the most infectious of the current variants, and perhaps the most infectious variant to date. From the UK Health Security Agency, Technical Briefing 49.
Despite the likely mildness of XBB.1.5, do others a favor and stay at home if you have COVID. The over-the-counter antibody based COVID tests do not work very well, so if you are sick but have a COVID negative antibody test, you should assume you have COVID. Only a PCR test can tell you if you’re really negative.
If you haven’t yet had COVID, I can no longer recommend that you get a vaccination or a booster, even if you are in an at-risk group. If you are concerned about getting COVID, consider taking precautions instead. Wear a N95, KN95, or KF94 rated medical respirator when indoors in public. It’s also important to make sure your mask fits snugly. The mask must filter air coming into your nose and mouth. Loosely fitting masks with large gaps will not do this. Do not wear a cloth or surgical mask. These masks will not protect you from XBB.1.5.
California Physician Misinformation Act: On October 4th, 2022, I wrote about California AB 2098. This new law went into effect on January 1st and adds “the dissemination of misinformation or disinformation related to the SARS-CoV-2 coronavirus” to the definition of unprofessional conduct for physicians in California. Unprofessional conduct can result in the suspension or loss of license for physicians in California.
Just yesterday, I had lunch with a friend of mine who is a doctor in California. I asked him how he is dealing with this new law. He said most of the doctors at his hospital follow the official guidance promoting vaccination, and the few who don’t have become very quiet about vaccines. Doctors can’t say anything negative about the vaccine, for the risk of their medical license.
In 2021, this same doctor was coerced into getting the vaccine to retain his position at the hospital. He got a booster later in the year. A month after receiving his booster, despite being very physically fit for his age, he had a heart attack. His cardiologist said he had none of the arterial plaques that typically cause heart attacks. My friend cannot prove this, but he strongly suspects that clotting due to the vaccine contributed to his heart attack. Despite all this, he does not feel at liberty in California to give information to patients that would reflect negatively on the vaccines.
Because this law is so new, I don’t yet know how it will be handled by the Medical Board of California. If they choose to ignore it, then doctors won’t be under threat. However, doctors and pharmacists have lost their licenses in the last few years for violating CDC guidelines, so the threat is a real one.
If you live in California, you cannot expect your doctor to give you their honest opinion about vaccines. This is literally illegal now. Consider writing your state senator or assemblymember and ask them to support the repeal of AB 2098.
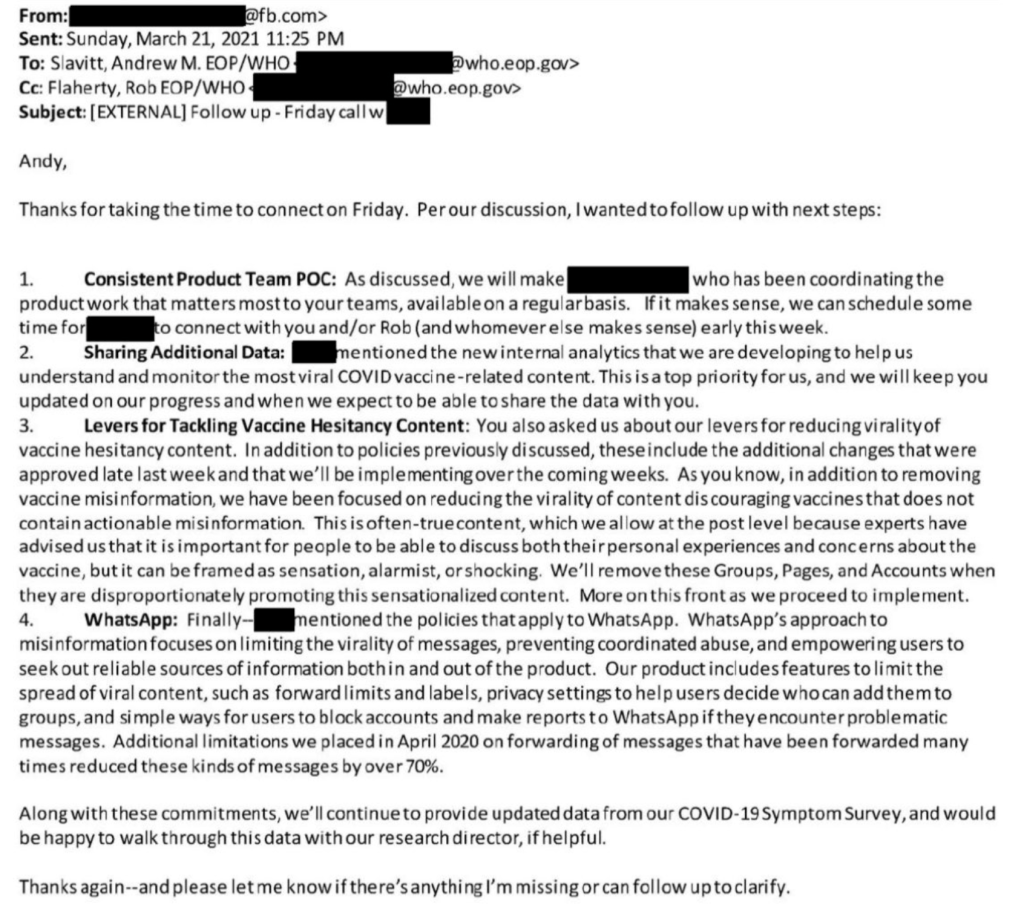
The Twitter Files have exposed a trove of evidence that official government agencies have been coercing several social media companies to censor COVID related information. In an amazing post from Michael Shellenberger, a F@¢eb00k official recently revealed that F@¢eb00k was reducing content not because they thought it was misinformation, but simply because it had a sensationalist tone. In an email to a Whitehouse official, the F@¢eb00k employee wrote:
“As you know, in addition to removing vaccine misinformation, we have been focused on reducing the virality of content discouraging vaccines that does not contain actionable misinformation. This is often-true content, which we allow at the post level because experts have advised us that it is important for people to discuss both their personal experiences and concerns about the vaccine, but it can be framed as sensation, alarmist, or shocking.”
Obviously, these efforts to limit expression by a government agency is a violation of the first amendment, our most important freedom. There are now many, many examples of this in the Twitter files, relating to COVID, and other matters.
This is a COVID update. Then I’ll discuss the high number of RSV and flu cases right now. I’ll also discuss the issue of vaccination induced blood clotting and the film “Died Suddenly”.
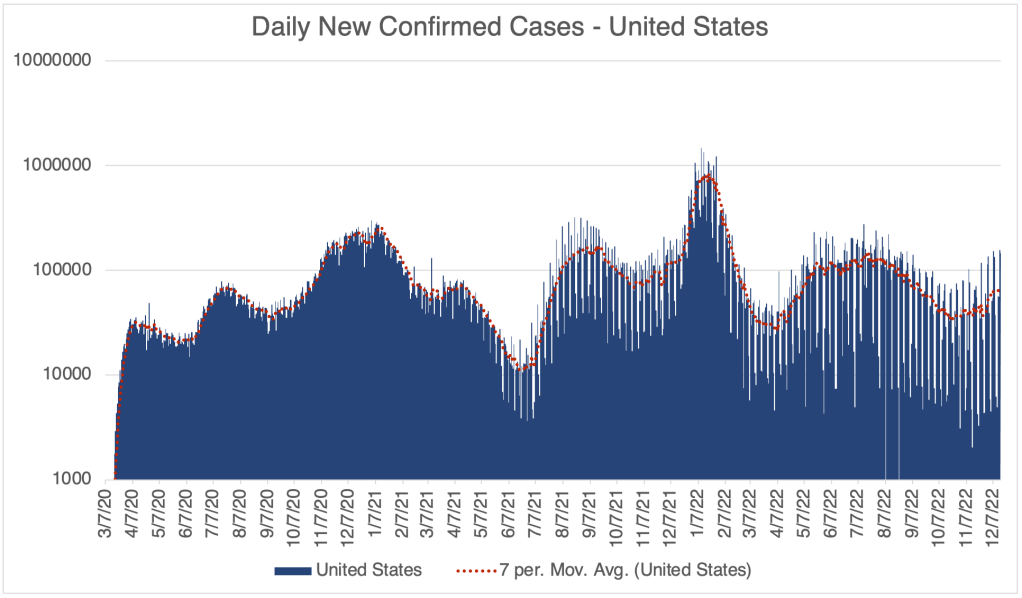
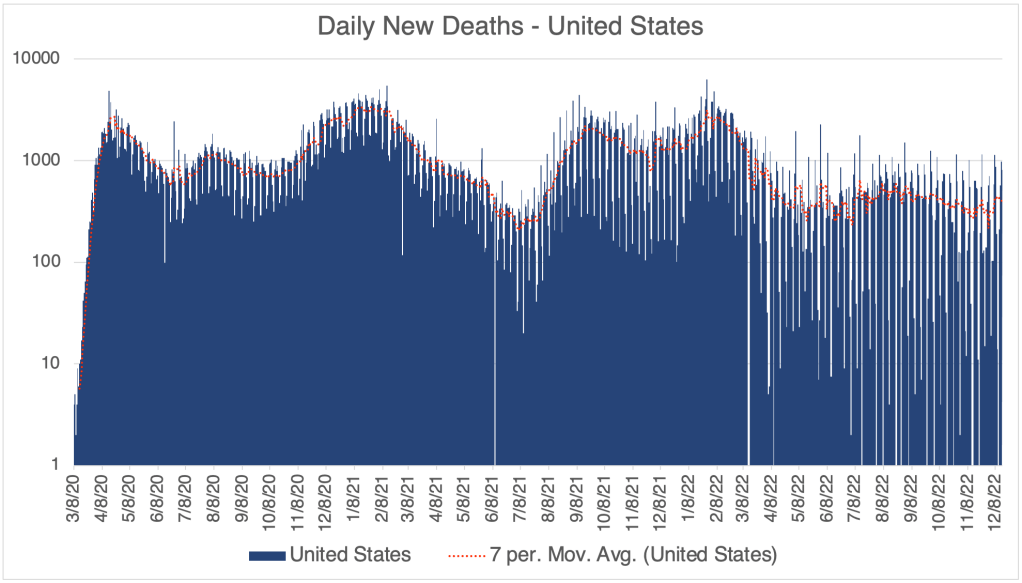
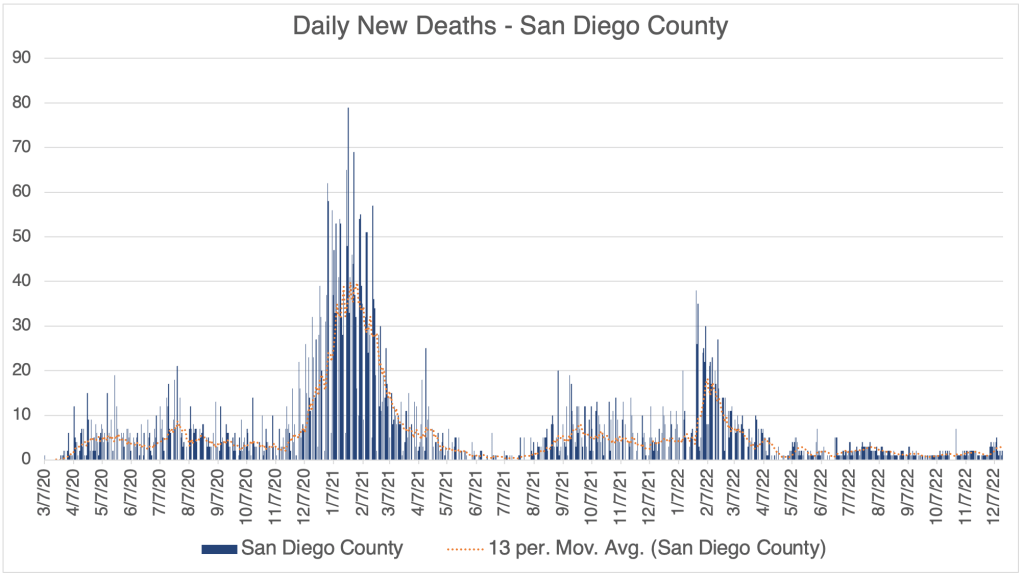
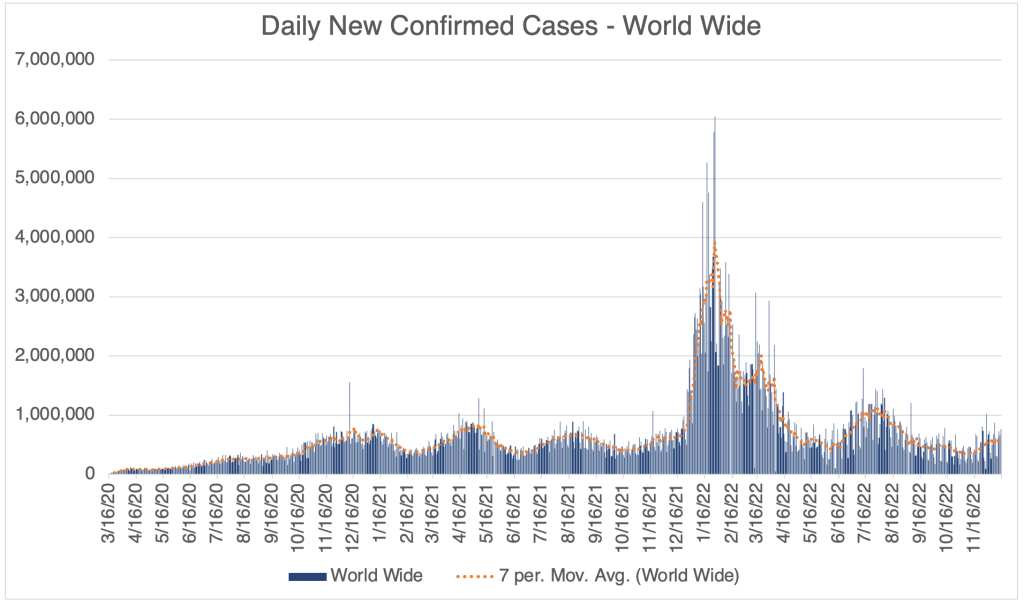
There has been a modest rise in cases in the past few weeks, suggesting that we will have a winter wave of cases. So far, this wave is not nearly as high as last December, when the Omicron variant first became dominant in the US. This is according to official testing data. Many are no longer being testing in a medical setting, so the number is likely much higher.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information on Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
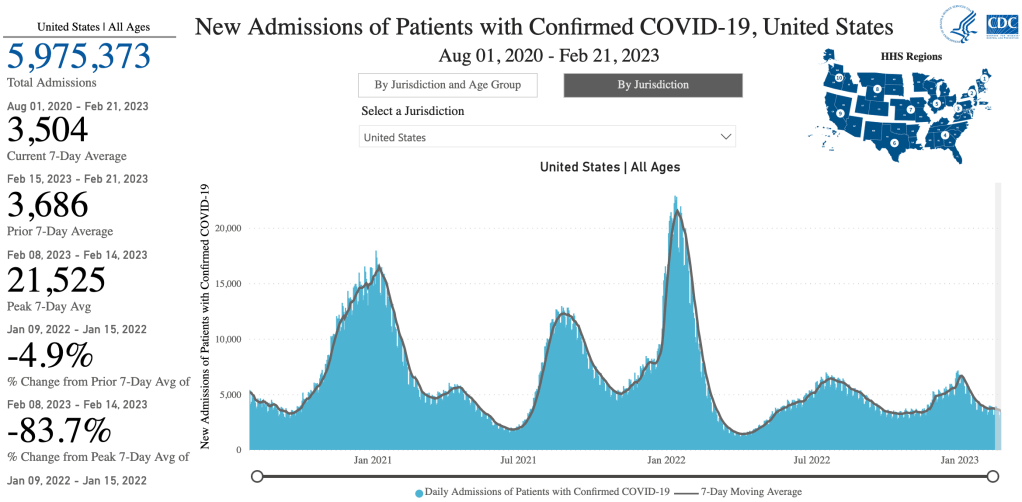
Hospitalization data provides a better relative view of cases, since it shows how many are actually entering the medical system with moderate to severe cases, but San Diego County is no longer providing this information on their website.
As we’ve discussed before, the drug store tests are not nearly as sensitive as a PCR test, and I know several people who were negative by this kind of test for days after symptoms began. The drug store tests can tell you if you have COVID, but false negatives are common, so if you get a negative result, it doesn’t mean much. If you really need to know if you have COVID, get a PCR test.
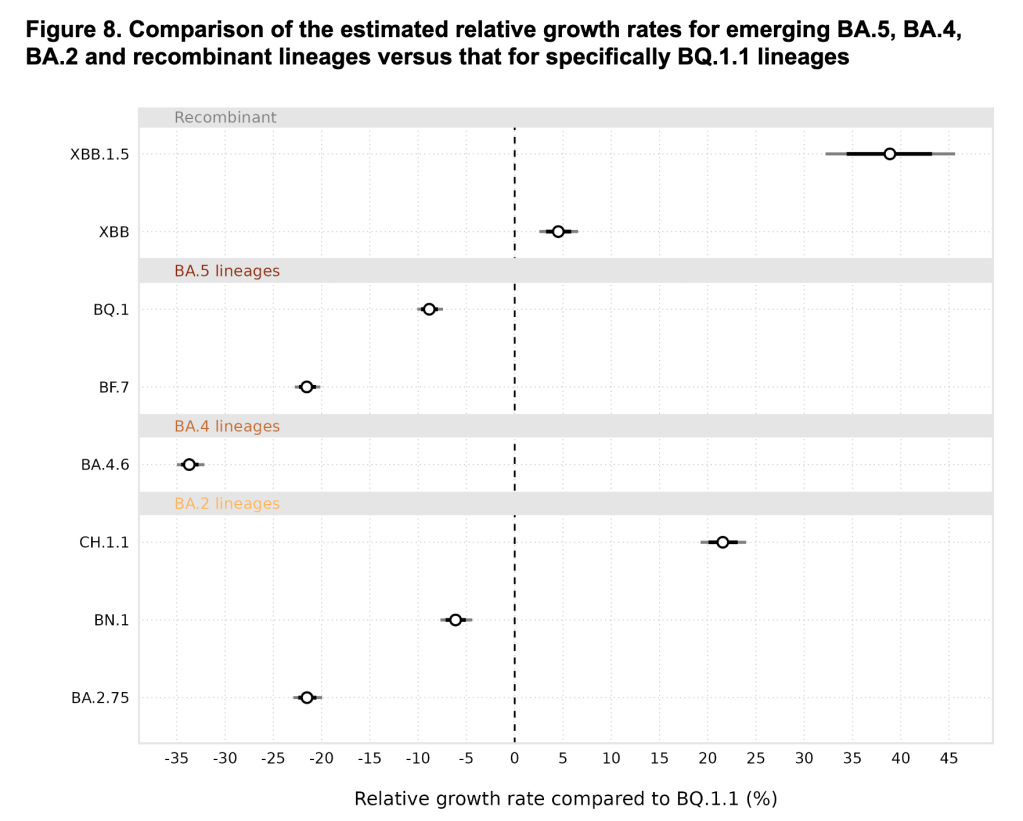
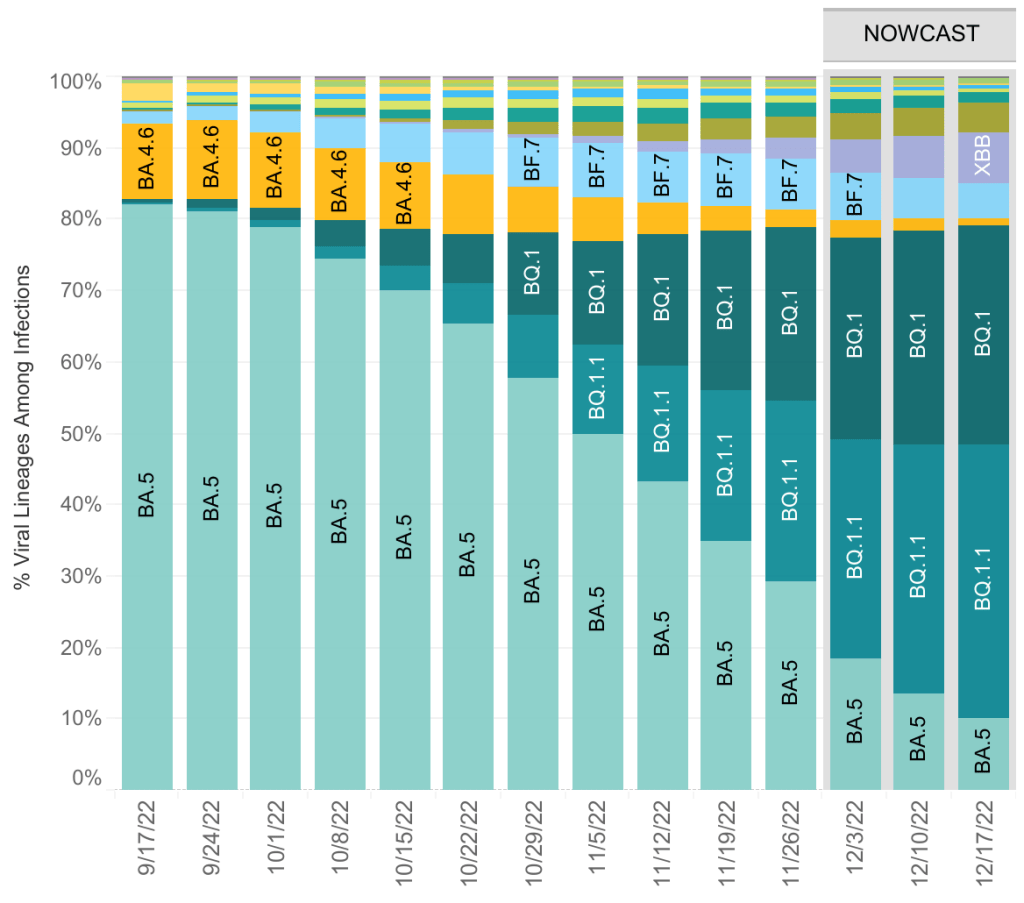
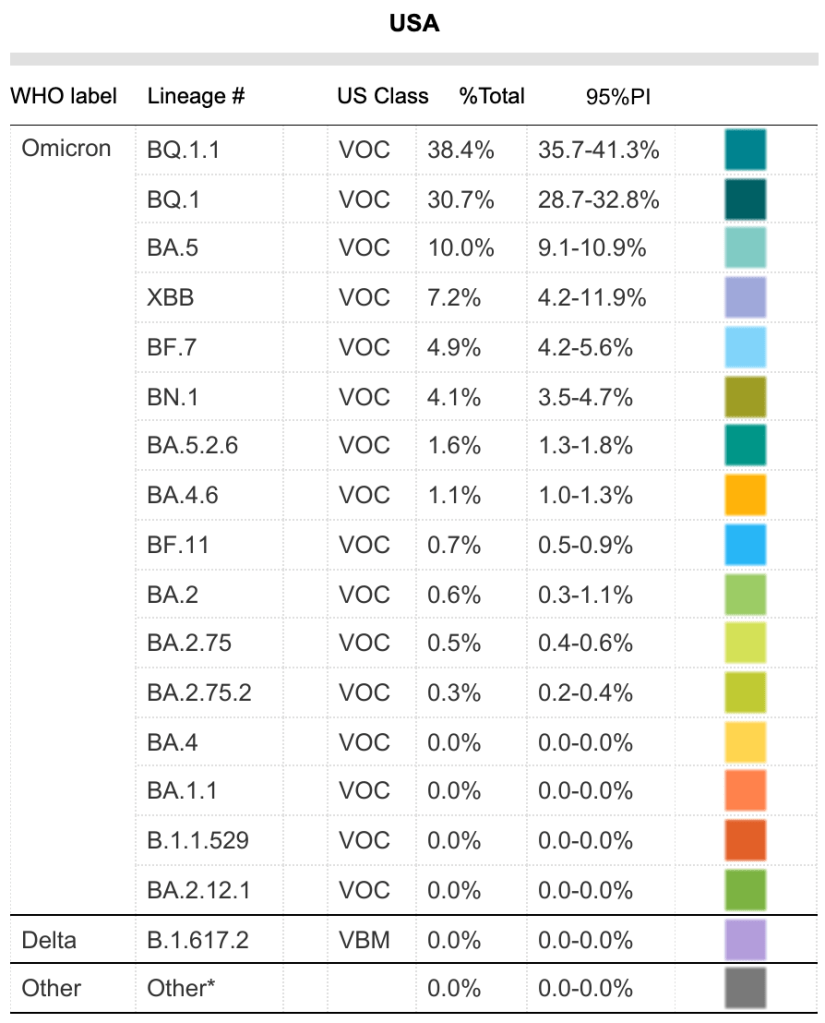
The BA.5 variant now represents only 10% of currently circulating COVID variants. There are currently 12 variants circulating in significant numbers, the most common being BQ.1.1.
From the CDC page on Variant Proportions for the United States. Updated on December 17th.From the CDC page on Variant Proportions for the United States. Updated on December 17th.
Tridemic: A physician friend of mine who works in urgent care joked that we are currently in a “tridemic”, by which he meant that there a lot of COVID, Flu, and RSV cases right now. Everyone knows about the flu, but many are unfamiliar with RSV. Well, actually, you are. Respiratory Syncytial Virus (RSV) is one of the several viruses that are responsible for what we call the common cold. You have likely had it many times in your life.
For most people, RSV is just an annoyance, but it can be serious for infants, causing bronchiolitis, a swelling of lung tissues. If your infant is coughing a lot, breathing rapidly, wheezing, or just breathing noisily, contact your doctor. Those with infants in their life may consider taking extra precautions to avoid passing along a cold. The blue surgical masks are not a good defense against COVID, but they are effective to prevent droplets which transfer colds and flus.
Many guess that RSV has become more serious because we have been so cautious for the last few years. I don’t know for sure if this is true, but it seems like a reasonable idea.
Long blood clots due to vaccines: Chris Martenson has a new video regarding the long blood clots that many embalmers have discovered in the arteries of COVID vaccine recipients. The phenomena started occurring in May of 2021, a few months after vaccination became common. Dr. Martenson is a pathologist and has done many autopsies in his career.
Chris Martenson on vaccine related blood clots:
In the video, he addresses a recently released documentary called “Died Suddenly”. The documentary claims that at least 140,000 people have died due to these vaccine induced blood clots. In Martenson’s video, he points out that detractors of the “Died Suddenly” film argue that these clots are post-mortem, meaning they arise after the person has died. Dr. Martenson argues that the clots in vaccinated patients are definitely pre-mortem (before death), not post-mortem as some have claimed. He gives specific features that lead him to this conclusion.
Dr. Martenson is one of my favorite commentators. He is knowledgeable, open-minded, and evidence based.
I got a question about whether these clots only happen in vaccinated people. Late stage COVID disease is well known to cause clotting. But COVID related blood clotting mostly cause strokes and thrombosis. Obviously, these can also be very serious and lead to death. The vaccine related clots are different, completely blocking vessels. It’s not yet known how large they are pre-mortem. Dr. Mortenson argues they are pre-mortem, but that doesn’t mean they won’t continue to grow before an autopsy.
Searching “COVID blood clot” and “vaccine blood clot” on Pubmed will both bring up a lot of papers. I haven’t read enough of these yet to know if the large clots only happen with vaccination. The fact that you don’t need to get COVID to have clotting is obviously very important.
Died Suddenly: Several people have asked my thoughts on this film. I will say that many COVID-era documentaries have a definite bias, so I always have my guard up when watching them. Claims without sufficient evidence are common.
The opening credits juxtapose images regarding blood clots and potential vaccine related deaths with images from other unproven theories, some that most regard as untrue or even ridiculous, like bigfoot and UFOs. This seems intentional, as if the makers intend for the viewer to pair these ideas. This seems to me to be ill-advised, if they intend to convince the viewer that blood clots can be tied to COVID vaccines. It almost begs the viewer to associate their thesis with nonsense.
The basic premise of the film, the phenomena of vaccine related clots, seems to be at this point to be well founded and well evidenced. The film offers several disturbing images of these clots being removed from cadavers. The film also shows many examples of individuals passing out suddenly, while driving, speaking in public, even performing surgery. The existence of this phenomena seems beyond dispute. Interestingly, the detractors Martenson references in his video claim that the clots are post-mortem, not that the clots don’t exist at all. Clotting has been a well known aspect of late stage COVID disease.
In addition to the potentially valid idea that vaccines have contributed to blood clotting in patients, the film makes the explosive claim that the deadly effects of the vaccine are actually intentional. I haven’t seen any data to suggest this connection. I’m not saying this is untrue, just that I haven’t seen evidence of this yet, so I don’t see a reason to believe it at this time.
The SARS-CoV-2 Spike protein has several toxic effects. First, it causes an inflammatory response in many tissue types in the body, leading to diverse symptoms, including myocarditis, inflammation of heart tissue. This new phenomena shows that the spike protein can also cause blood proteins like fibrin to form an amyloid, an unnatural collection of proteins. Amyloid plaques also have a role in Alzheimer’s disease.
Should you get the updated booster? COVID vaccines appeared to be working well in the Spring of 2021, but their effectiveness began to wane with the Delta variant. When Omicron became the dominant variant, vaccine effectiveness dropped even further. As knowledge of possible harms due to the spike protein has increased, I now think the harms of vaccination outweigh benefits in our current environment. In my opinion, there is no longer any reason to get a vaccine or booster, even for those with risk factors.
If you’ve been vaccinated, this information will likely cause you some concern. I don’t know how long vaccine related spike protein has the potential to cause injuries. Blood clots appear to form around 5 months after vaccination. If you haven’t been vaccinated or boosted in the last 7 months or so, you may be in the clear. I’m sorry I don’t know more.
I have to point out that official channels claim that the information in “Died Suddenly” has been de-bunked. When posting this information on Facebook, I was met with several warnings about posting. To be fully informed on this issue, you should read several sources of information and judge for yourself which are most reliable.