Avast! This be Talk Like a Pirate Day! So if you be havin’ a question below, use your favorite dialect of the high seas!
The New England Journal of Medicine foisted a flag regardin’ mask wearin’. It appears masks reduce scurvy and COVID symptoms even in infected seafarers. This may be explainin’ why even with the large number of cases during the second wave, fatalities were low.
Friends, Sorry for the long wait for a new update, I’ve been helping put together a new COVID lab, and I’ve been working long days for the past week. Today, I’ll give the update, then talk about a new study concerning masks.
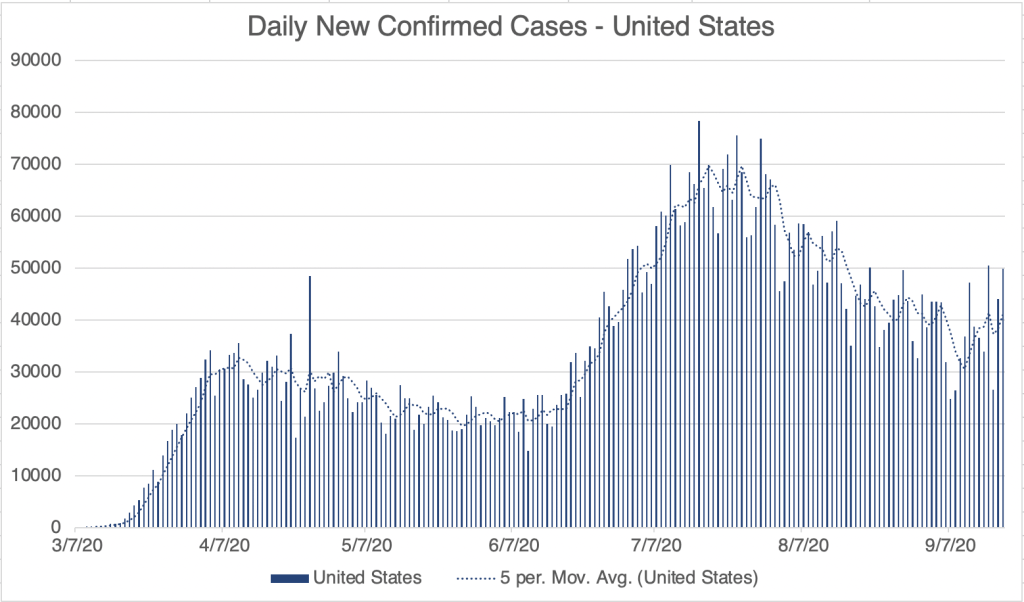
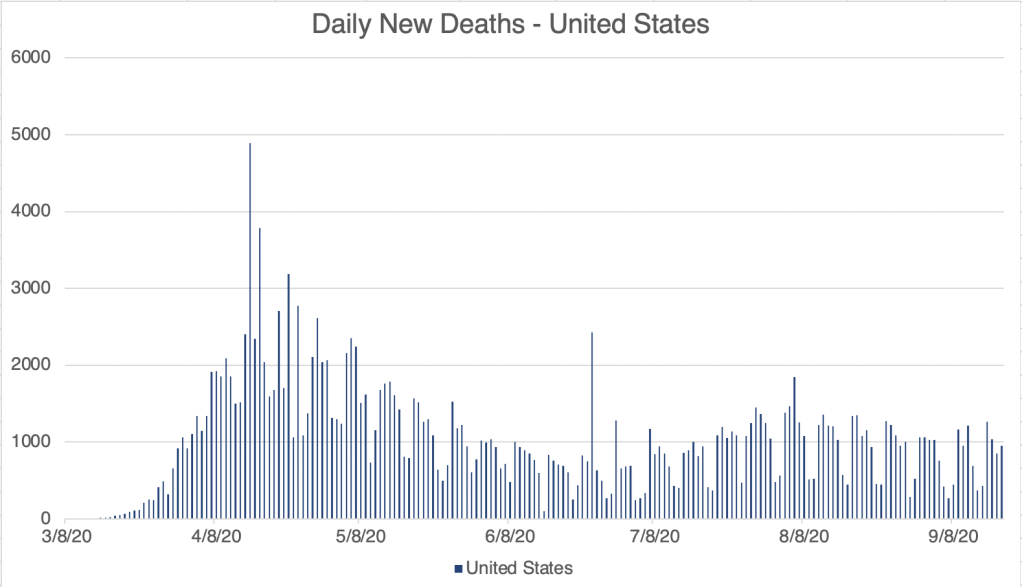
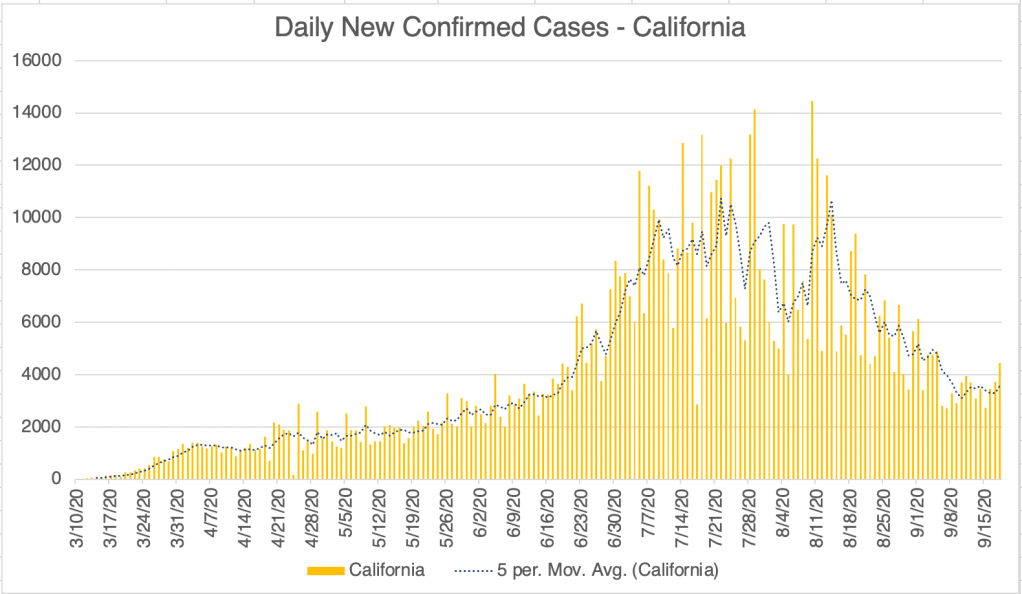
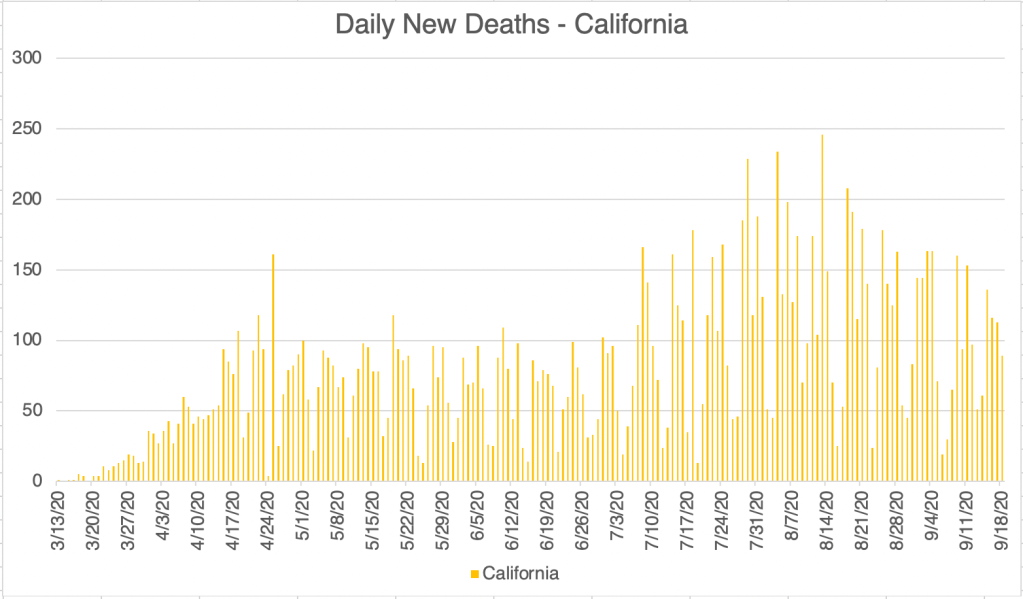
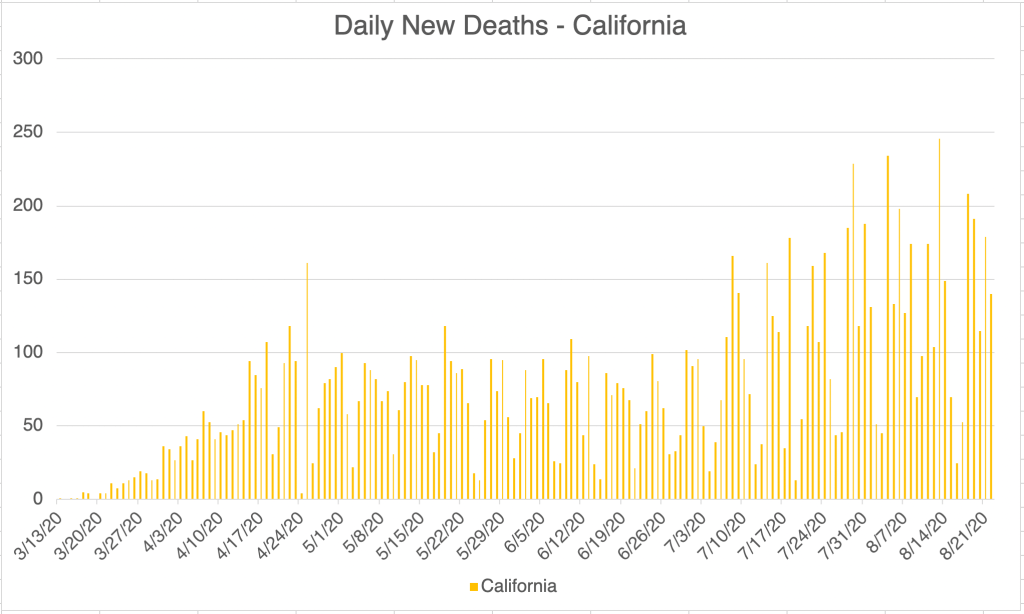
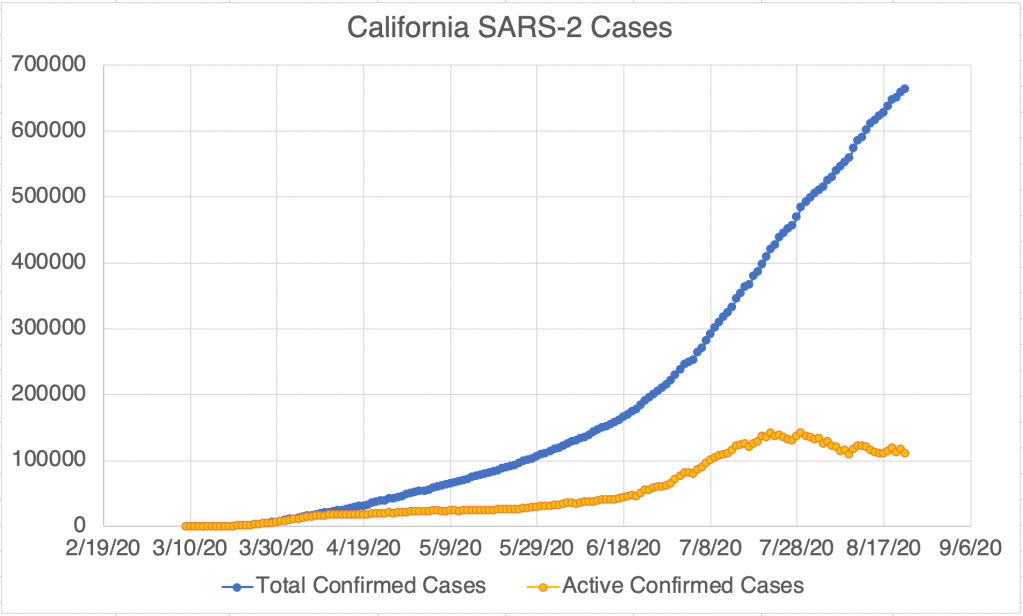
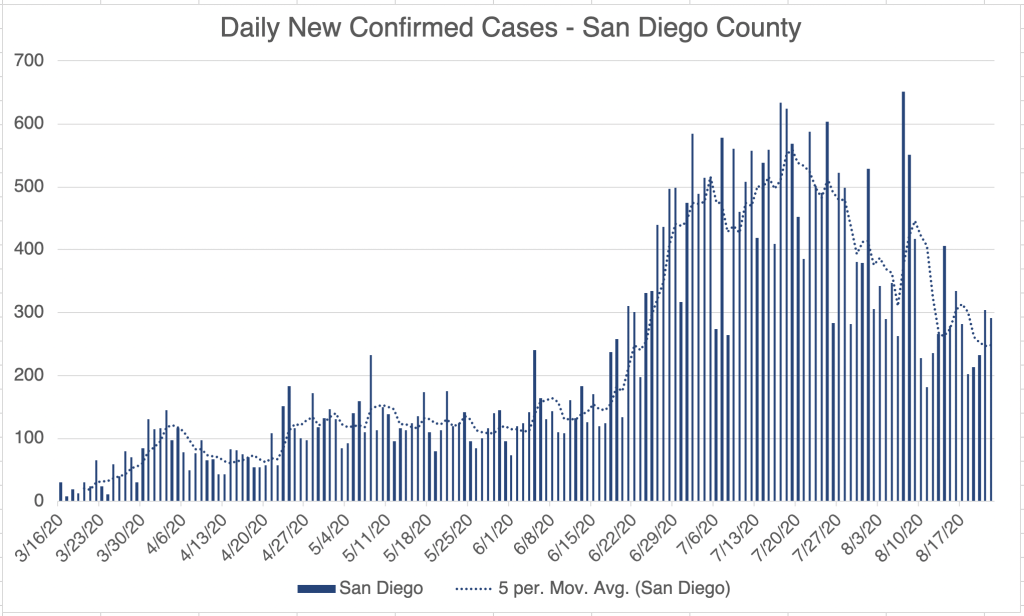
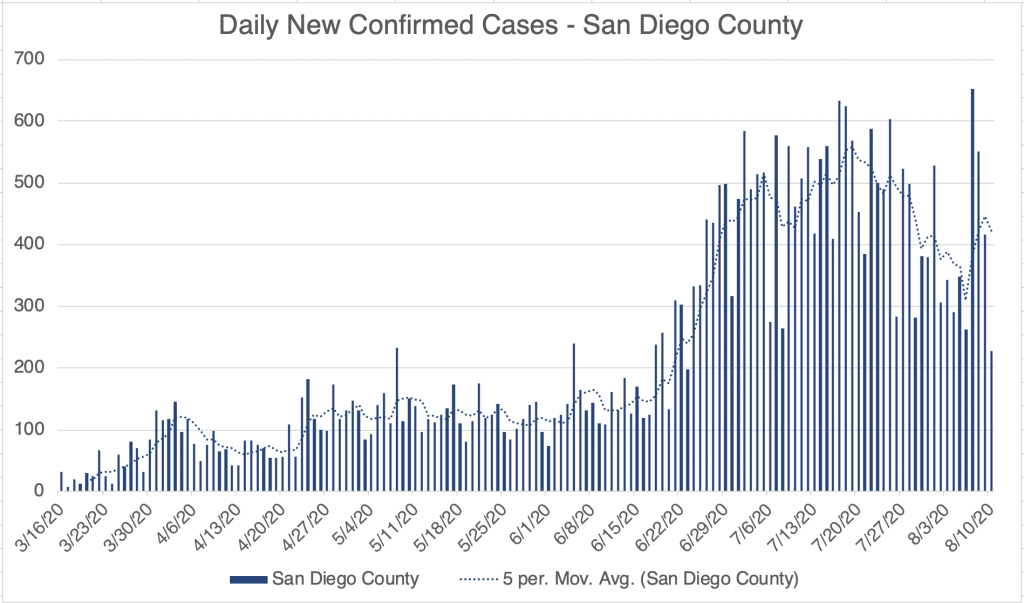
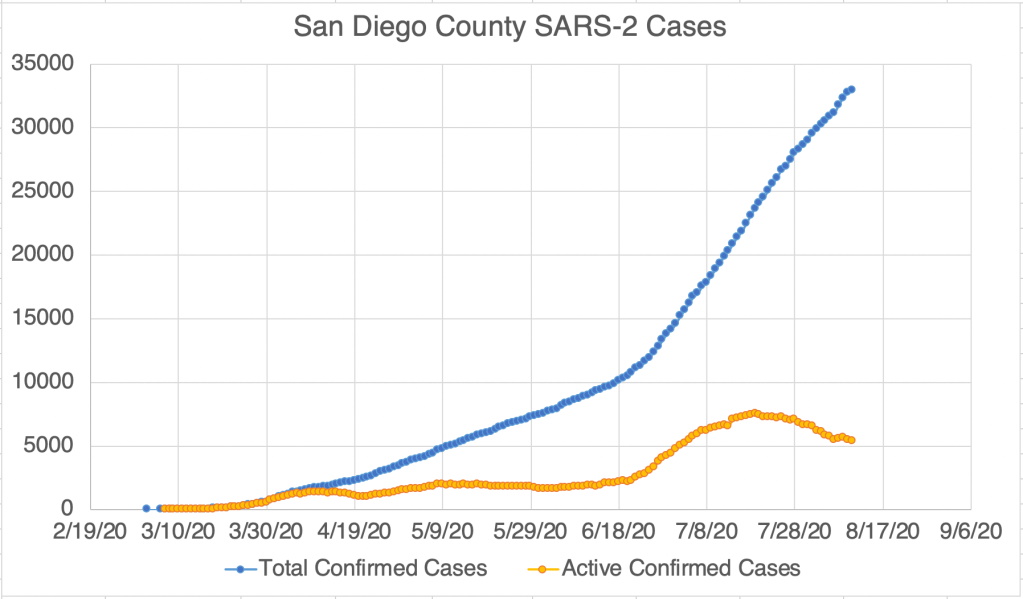
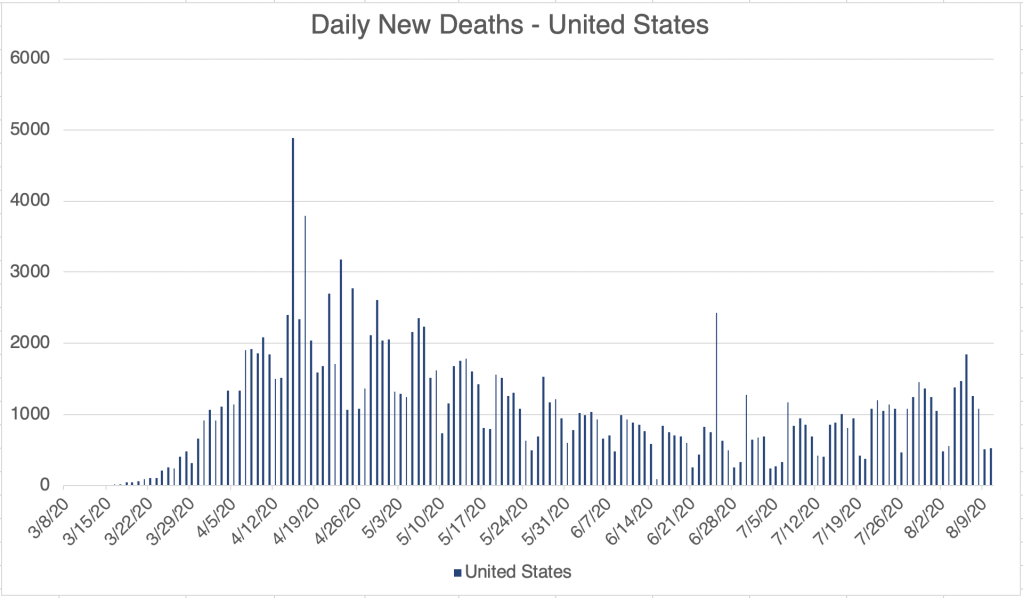
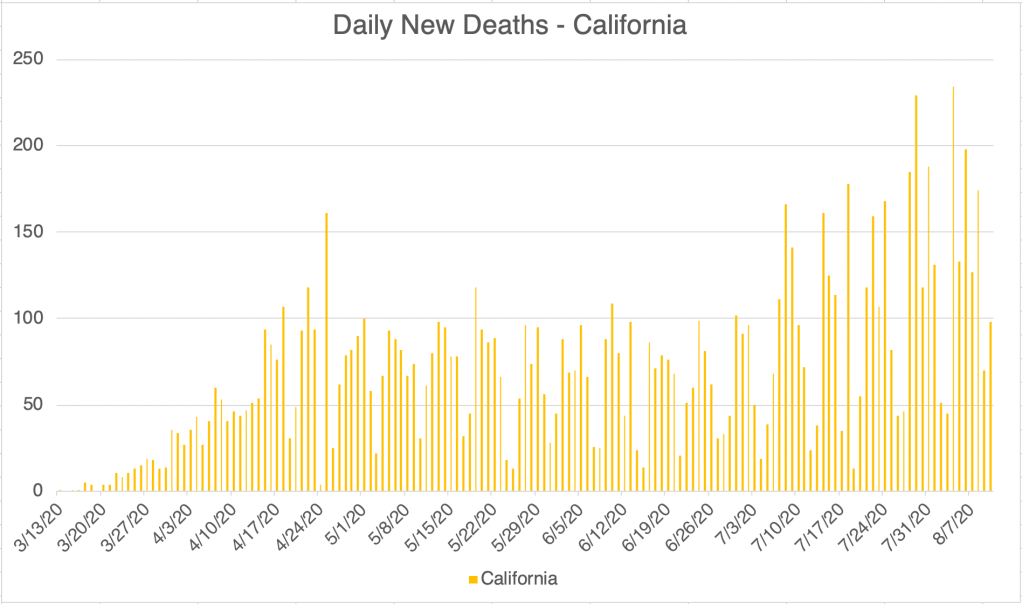
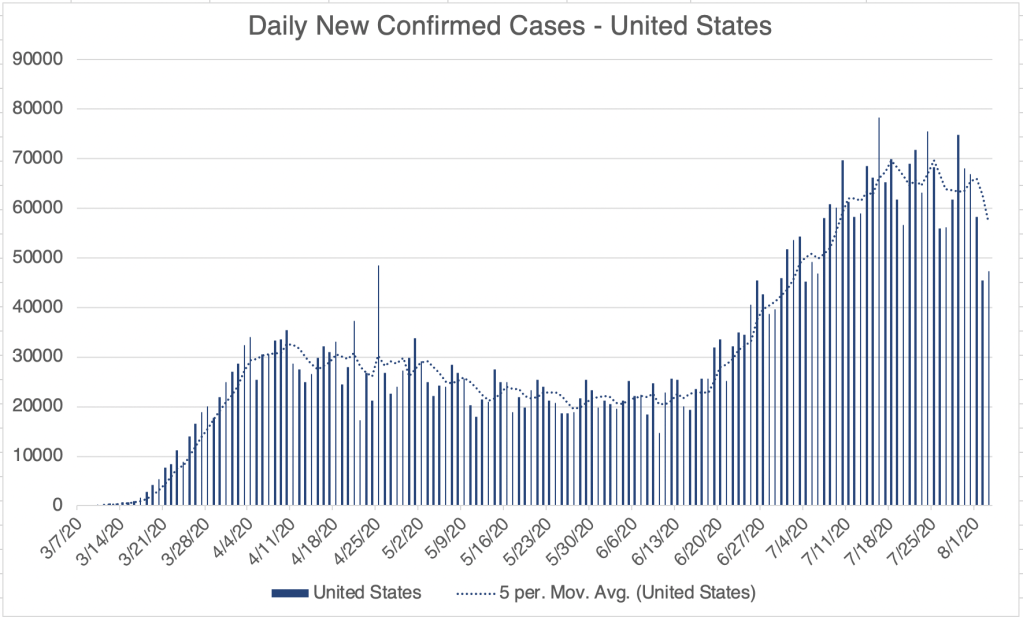
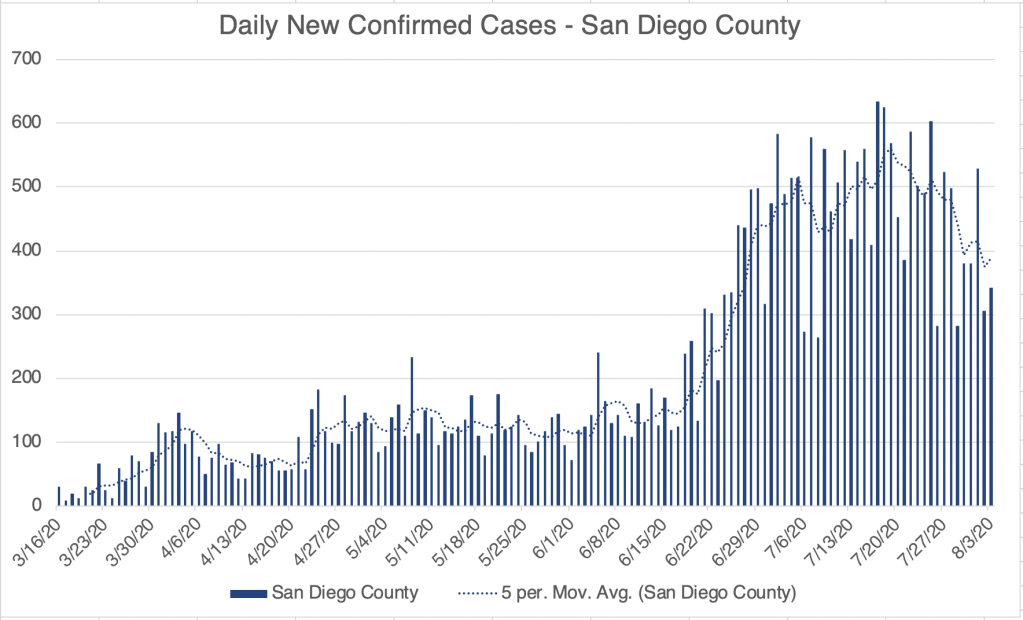
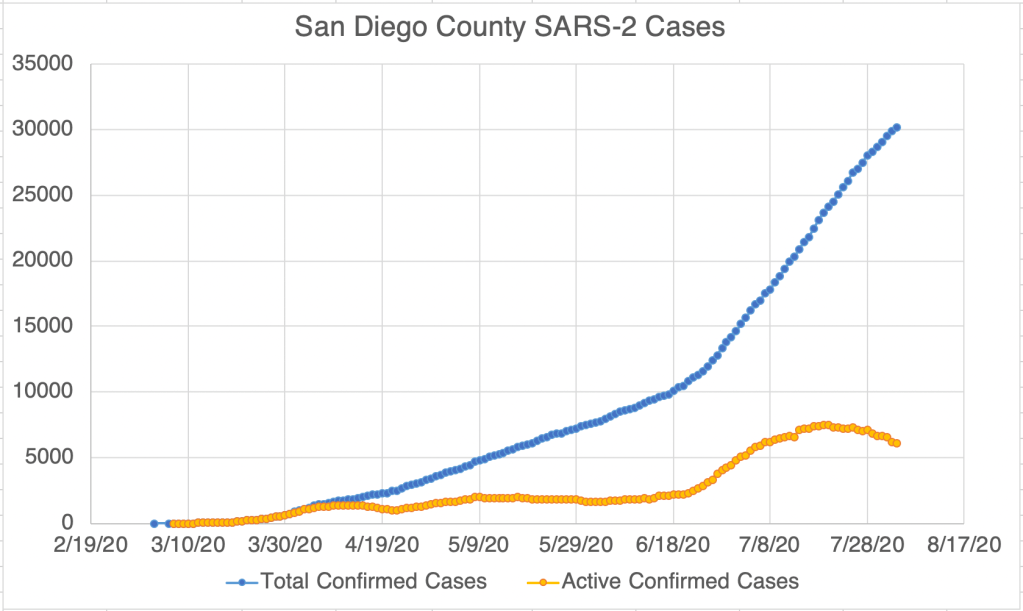
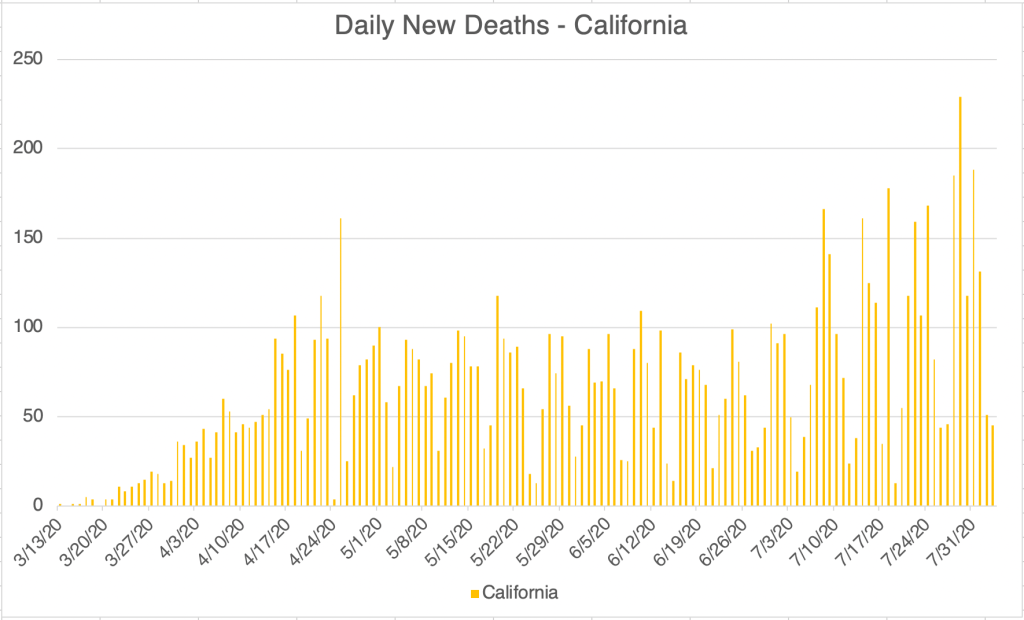
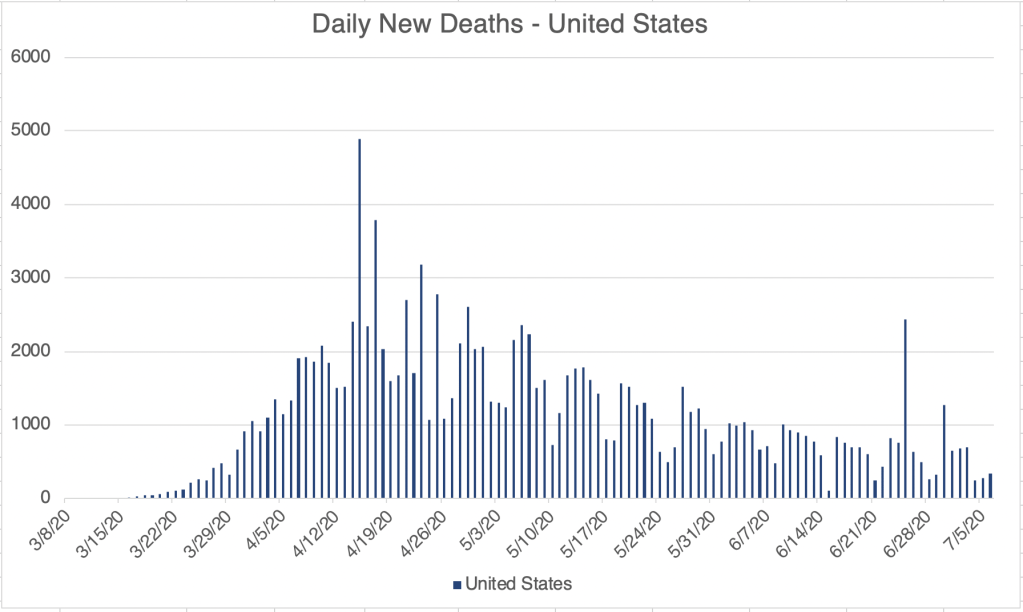
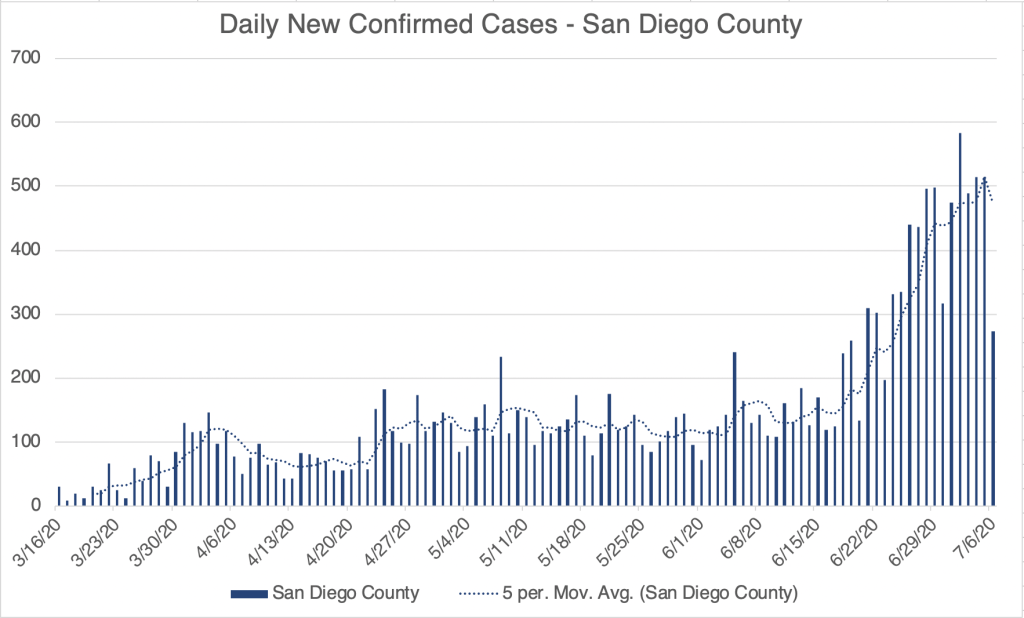
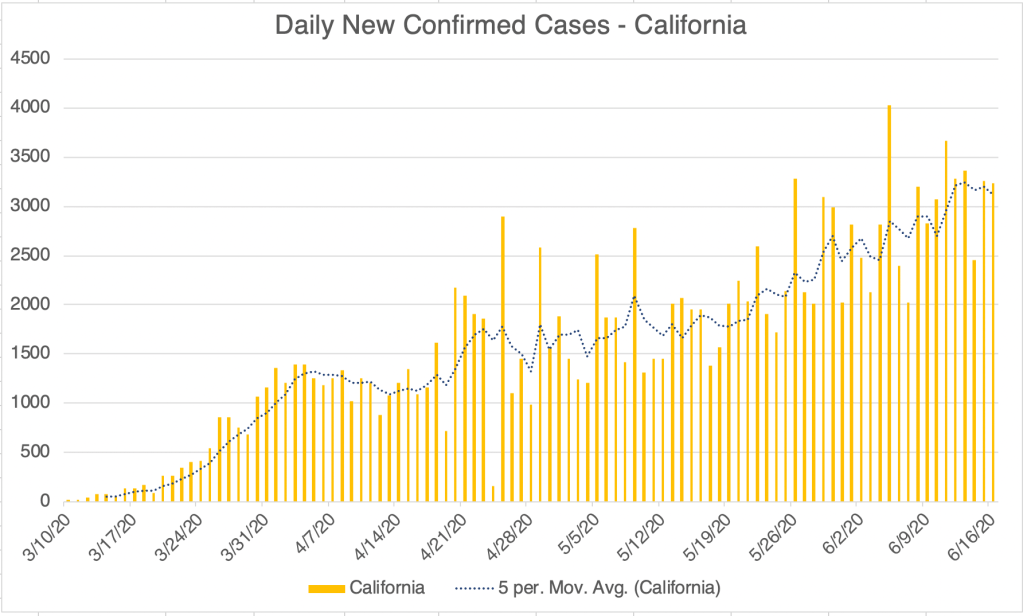
Update: New confirmed cases continue to go down for the US, California and San Diego County. For California, the numbers are kind of flat. The reporting system in California was broken for much of last week, but the state says it’s working again. Death rates are coming down from their second peak. Comparing the new daily case numbers and the new death numbers make it clear that the virus has become much more survivable than it was in March and April.
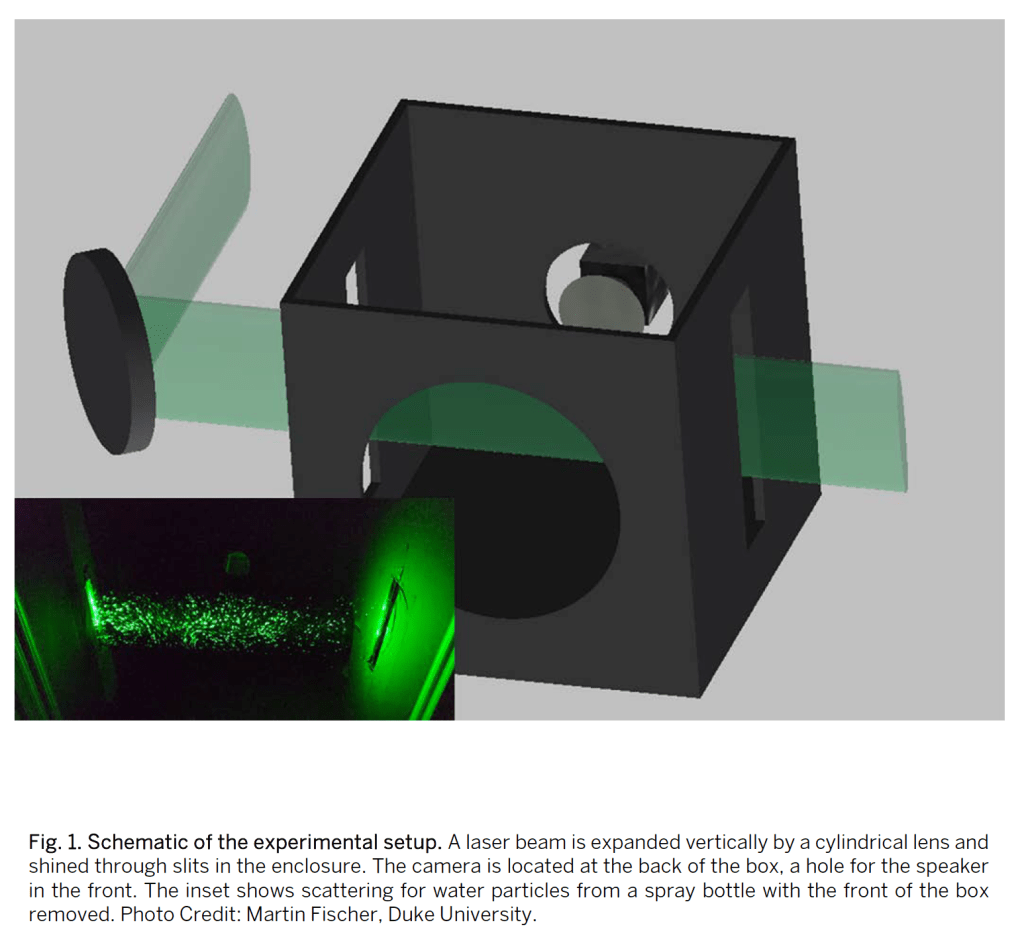
New study on droplet transmission from various masks: A study was pre-published a few weeks ago that studied droplet transmission from various popular masks (Fischer EP, et al., Low-cost measurement of facemask efficacy for filtering expelled droplets during speech, Science Advances, pre-released August 7, 2020). The study used a system in which a speaker wearing a mask would say a prescribed phrase several times into a box through which a laser was shining. A camera would then capture droplets that were illuminated by the laser. The study used a relative scale for mapping mask benefit, with the N95 getting a relative score of 0, and no mask at all getting a score of 1. See the results in the photos.
Surgical masks did the second best after the N-95, and a 2 ply cotton mask with a sheet of polypropylene (like blue Shop Towel) fabric did third. I’m particularly happy to see the cotton and poly mask do so well, because that’s what I use! Performing poorly are knitted masks, bandanas, and especially the neck gaiter, which actually did worse than nothing! The authors speculate that this is because the fleece material may break up larger droplets into smaller ones instead of stopping them.
Shout out to my sister-law Penny who has made hundreds of masks in her home. The 2 ply cotton masks she makes have a pocket for inserting a filter or piece of poly like I use, and these masks did very well in this study! For extra credit, say the phrase “masks she makes” ten times fast.
I have never been a fan of the surgical mask because of the large side spaces that allow air to pass easily into and out of the mask from the side. I was surprised to see these masks do so well in this study. The answer may be in the experimental design, which captured droplets coming from the front of the mask, but excluded ones from the side. I would like to see a study that captures that too! This just shows that experimental design matters, and just because a study shows something, doesn’t mean the study was designed to detect all relevant things!
Mask wearing has become controversial, but the data supports the idea that masks reduce viral transmission, and that lower viral load on exposure leads to better medical outcomes!
Here’s the weekly update. The US, California, and San Diego County continue to improve. New confirmed cases continue to drop. I have to qualify this however, since California had a problem with their cases reporting system for much of last week. It’s back working normally, but cases may still be erratic in number for the next few days. This may impact the San Diego numbers as well.
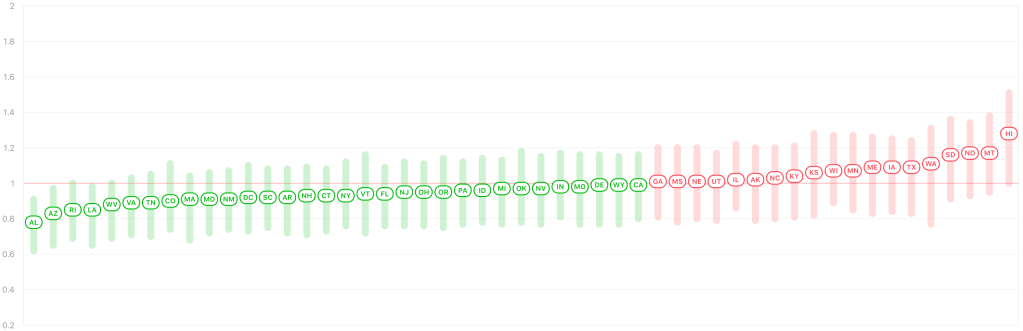
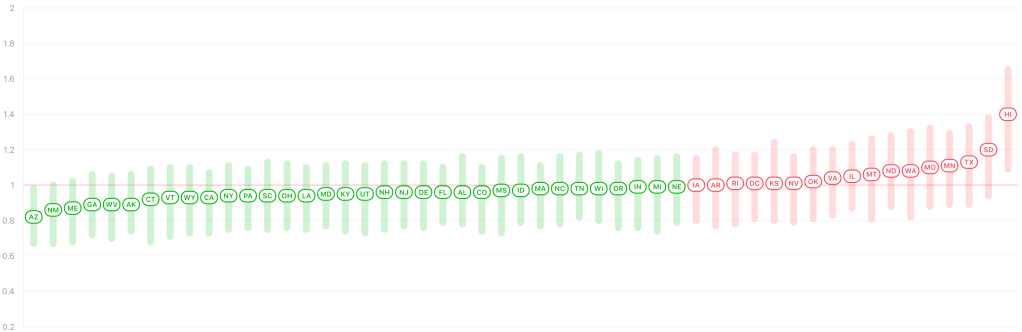
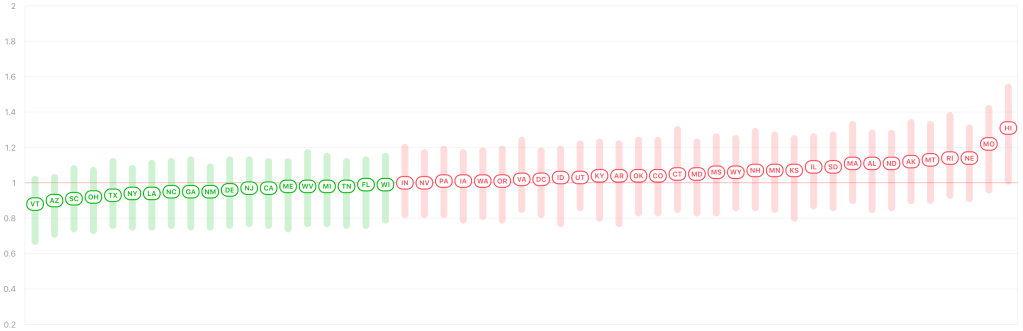
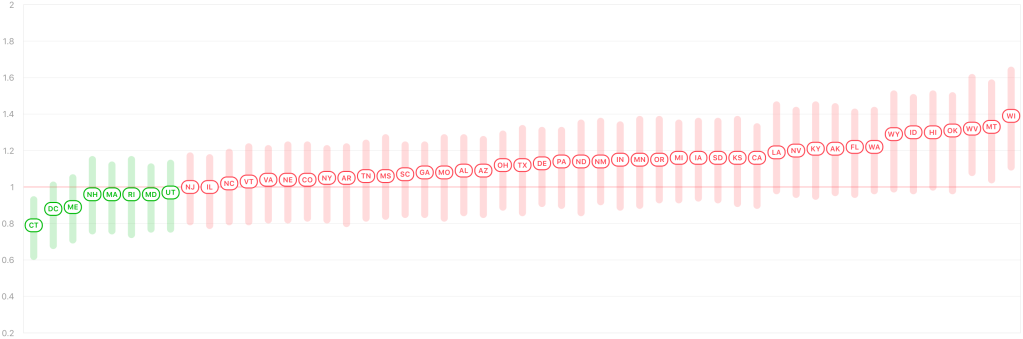
According to Rt Live, more than half the states in the US now have an Rt of below 1.0 again. This suggests that those states are on the downslope of the last peak, and virus is slowly going away in those states. This is great news.
I spoke to testing professional this week who said that viral load, the number of viruses in a patient’s test sample, started coming down in April, when mask wearing became common place. This supports my claim that even if a person gets exposed to the virus, they receive less virus if they’re wearing a mask. This may also be why the virus has been more survivable in the past few months.
I have a grab bag of things to discuss today, starting with the weekly update, a note about the new KN95s, a new version of the Coronavirus (D614G), and where outbreaks are located, at least in San Diego County.
The positive trend continues! Cases are dropping in the US and San Diego, and are flat in California, which is actually better than it sounds, since the state has been steadily increasing in cases since mid-April. Active cases continue to decline in San Diego. Even in Los Angeles County, the epicenter of new cases in the entire country for the last few months, new daily confirmed cases are finally coming down.
KN95 masks: I’ve started to see a new kind of mask being worn, the KN95. They are rated to filter out 95% of virus particles, but are made and certified in China and carry the European CE mark. The FDA has allowed their use in the US as an emergency measure. They fit a little less snugly than an N95. Perhaps their greatest benefit is that they’re available. If you’re still using a surgical mask consider upgrading to the KN95, which will be an improvement!
A KN95 mask.
New strain D614G: A new strain appeared in the US and worldwide probably in May or June. Called D614G, it carries a mutation at the 614th position of the Spike protein. This mutation makes the virus more infectious by 4-5 times, and may have contributed to wave Ib of the virus that we saw in June and July. Dr. Deborah Birx, White House Coronavirus Response Coordinator, has speculated that this mutation may be why we saw more widespread virus outside urban areas during the last jump in cases.
Coronaviruses are RNA viruses. Enzymes that replicate RNA tend to be very error prone which is why RNA viruses change so rapidly. This is true for Coronaviruses as well as for the flu and for HIV. We can continue to expect more naturally occurring mutations in the future. The good news is, over the course of years, viruses generally become less virulent and more mild.
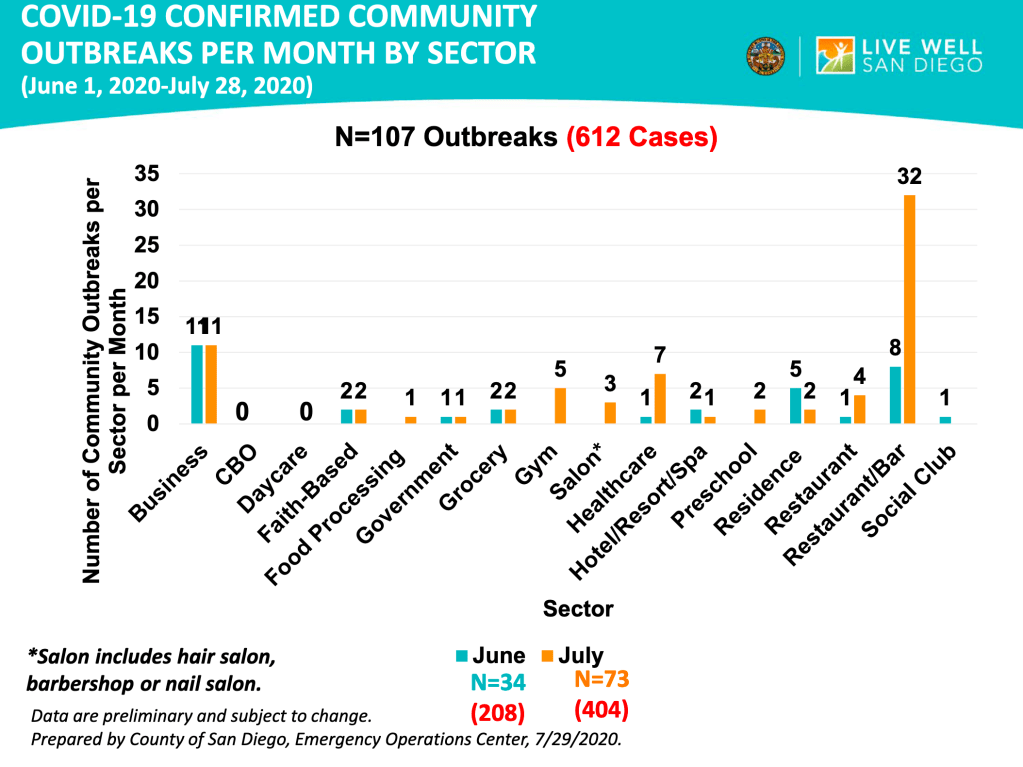
The location of outbreaks in San Diego County: San Diego Public Health has published a graph on the locations of outbreaks as part of their regular slide package. Out of 134 the top most common places for outbreaks are restaurants with a bar (40), businesses (27), the healthcare environment (15), and residences (9), further down the list, faith based organizations and government offices are tied at 5. As a business traveler myself, I’m happy to see that hotels are only at 3. Restaurants without a bar only had 5 events.
Things are starting to get better! But remember that an epidemic is like a wildfire, getting containment doesn’t mean it’s over! We need to remain diligent in order to put it down for good. Keep up your efforts!
A quick note, I posted an update yesterday, but I accidentally only sent it to one person, so for the weekly update, check your feed for yesterday morning, or check my timeline.
Many people have asked me about a video that was posted yesterday by a group called “America’s Frontline Doctors”. The original video has since been removed from Facebook, YouTube and the group’s website has even been dropped by the host, Squarespace. All this to say, you may have a hard time watching it if you want to. I found a different version.
As I’ve said before, politics and science should never go together. Whenever a scientific issue becomes political, it becomes very difficult for free scientific inquiry to move forward, and nearly impossible for non-scientists to figure out what the truth is. So I’m sorry to those of you who are confused and are trying to pursue the truth. The video was put together by the Tea Party Patriots and Breitbart News, 2 right leaning organizations. This is a red flag for me because I know that the message will have a political angle, and that I’ll need to watch with extra care. As I said in my July 14th post, however, just because you disagree with someone in general doesn’t mean they have nothing good to contribute to the discussion. Especially with politically charged issues, we need to get information from a variety of sources in order to be as informed as we can. I know for many of us, it’s nearly impossible to have time for that, so we often just pick someone we trust to get our information from. I definitely have political opinions, but whenever a scientific issue comes up, I do my best to set those aside and look at the evidence. I hope this has been valuable to you. You may have noticed that some of my thoughts about the Coronavirus have been “left-wing” and others have been “right-wing.” I’m doing my best to be objective. And yes, I consider it a tragedy that opinions on scientific issues can be categorized as either left or right.
I want to discuss some of the main points of the video and offer my informed but not expert opinion. I am a Ph.D. molecular biologist specializing in infectious disease testing. I am not a physician or an epidemiologist. I will give my opinion and also why I think that way.
Hydroxychloroquine (HCQ): The video focuses to a great degree on HCQ as a potential “cure” for the Coronavirus. As soon as President Trump mentioned it as being potentially helpful for treating Coronavirus, it became a subject of immediate and hot controversy. Democrats seemed to reflexively dismiss HCQ, and Republicans seemed to reflexively support it. President Trump dug in his heels and seemed to support its use before all the evidence was in. Obviously, this is not how science should be done. Careful and well-reasoned studies should be done, and conclusions made based on evidence. Early studies seemed to support both conclusions. Opponents claim that HCQ doesn’t work and is even harmful to patients, causing heart problems in some. Supporters claim that HCQ works when given early in the disease, and with Zinc and perhaps azithromycin.
Dr. Immanuel made an impassioned case for the use of HCQ, having successfully used it to treat over 300 patients. This kind of evidence is what scientists call “anecdotal”. Anecdotal evidence, basically stories, is often not considered scientific because in a large pool of people, you can find stories supporting all kinds of claims. Anecdotal evidence also usually does not carefully consider other factors that may contribute to a conclusion. An example would be “I ate ice cream and then I got attacked by a shark, so eating ice cream leads to shark attacks.” This is obviously a silly example, but many pieces of anecdotal evidence you hear suffer from the same lack of critical thinking. However, this is not at all to say that anecdotal evidence is not useful! These kinds of stories may not be scientific per se, but can often trigger more rigorous studies that prove the claims of a story.
Several scientists I’ve heard from will point out that HCQ is useful when given early and given in combination with Zinc, and also in appropriate dosages. I actually agree that some of the studies arguing against HCQ use have given it too late or in inappropriately high dosages. I would like more rigorous studies to be done, however at the moment, I think HCQ is well worth consideration by the medical community. Other treatments also exist and may actually be better, such as the MATH+ protocol I described in my summary post on June 22nd, Dexamethasone, Remdesivir, and perhaps Budesonide. For the HCQ protocol, it appears that Zinc is actually most responsible for anti-viral activity, with HCQ mostly helping Zinc enter cells to interact with the virus.
Some have pointed out that Dr. Immanuel has some beliefs that are well outside accepted scientific views. As I pointed out before, even folks who you generally disagree with can bring helpful information to the table. Her HCQ experience may be true despite her unorthodox beliefs. So even if you justifiably don’t consider a person reliable, you should resist the urge to dismiss them outright.
Lastly on the issue of HCQ, physicians have the right to use drugs “off-label” meaning they are granted by their medical degree the right to try medications in ways that are not necessarily supported by the literature or guidelines. This right is granted in the interest of patients, because careful studies can take a prohibitively long time to be published, and to encourage the development of helpful new protocols. In my opinion, government agencies should not be restricting the use of HCQ by doctors at this time.
School reopening: In some ways, there is reason to re-open schools in the Fall. It appears to be true that children under 10 do not get infected at high rates, do not carry a high viral load when infected, do not get severe disease, and do not seem to spread virus to others. So there is a case to be made for reopening schools for young children. However, because of the ADE issue I’ve written about before, I am not currently in support of re-opening schools in the Fall. Just to recap, ADE (Antibody Dependent Enhancement) is the phenomena in which some viruses can use antibodies presented on immune cells to infect those cells and cause more severe disease. So a second infection with a similar strain can lead to much worse symptoms. SARS-1 and MERS, cousins of SARS-2, can both use this pathway, so with current evidence, it seems likely that SARS-2 will as well. But we won’t know for sure until another SARS strain develops and we see how people respond to it. I will point out in full disclosure, that almost no-one is talking publicly about ADE. Dr. Fauci has mentioned it, but just in passing. So I could be out to lunch about this, but it is a major concern of mine. I have had a few epidemiologists mention in private conversations that they think ADE is a real issue, but they aren’t comfortable talking publicly about it either.
Sweden and Herd Immunity: Dr. Dan Erickson, who made a video back in April, also spoke. I was critical of his original video because his analysis of the death rate used the wrong number for total cases. This time he spoke mostly about the lock-downs, and most of his comments were more measured. He argued against lock-downs and suggested Sweden as a model.
I am also critical of lock-downs as they were done in much of the US, with people asked to stay home at all times. However, I am not supportive of the Swedish model either, in which few precautions are taken. While I am not for people staying at home, and I think people should find ways to get back to work, I also think people should wear masks while indoors in public. Small outdoor meetings are fine, even without masks, but large outdoor gatherings with closely packed people are dangerous in my opinion. Again because of the ADE issue, I am not in support of the idea of obtaining herd immunity as a way out of the crisis.
Masks: Some have taken away from the video the idea that we should not wear masks. I didn’t get this from the video. Dr. Gold explicitly said she thinks masks should be worn indoors, but not necessarily outside. I agree with this approach.
As you can see, I agree with some aspects of the video, and disagree with others. When possible, study all sides of the issues, and make the best most reasoned choices for you and your family.
My basic rules are as follows:
1) Wear a mask or face covering in public. Avoid places with unmasked people. 2) Keep 6 ft away from others. 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. 4) Small outdoor gatherings are fine, even without masks, if everyone maintains a distance. Have guests bring their own food. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however.
Don’t fear, but be smart!
Erik
A version of the America’s Frontline Doctors video: NOTE: The below video was removed by YouTube a day after this blog posted.
Dear Friends, This is a case update. I’ll also have an important message about antibody dependent enhancement.
Cases continued to rise unchecked in the US, California and San Diego County in the last week, although the long holiday weekend did have impacts on reporting. Some good news is that the number of deaths reported in the US has been slowly declining despite the case increase. Keep in mind however, that deaths will lag behind cases by as much as 2 weeks, so we may yet see an impact from the higher caseload. The number of deaths have been trending flat in California.
Rt Live is reporting that all but 8 US states or territories have Rt values above 1.0, meaning that the virus is expanding in those states.
I’m going to bring up an issue that I’ve been avoiding talking about for some time. I’ve been avoiding talking about it because it’s not a certainty, and also because the possibility will be scary for some. The reason I feel compelled to talk about it now is that many are having a hard time understanding why I am still so concerned about the virus when the fatality rate is low and dropping, and folks want to get back to normal life. I’m even hearing about young people having COVID parties in which people gather with a sick individual so they can all get infected and be immune from the virus thereafter.
Before I share this, I’ll also say that the medical community is doing a better job treating patients with COVID, and the disease is becoming more survivable. In addition, we now know a lot about how the virus is spread, and if a person wants to remain uninfected, they can do that, while still getting together with friends and family, and still working and getting on with life. You can be reasonably certain you will not get infected if you do the following:
1) Wear a mask or face covering in public. Avoid places with unmasked people. 2) Keep 6 ft away from others. 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. 4) Small outdoor gatherings are fine, even without masks, if everyone maintains a distance. Have guests bring their own food. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however.
Antibody Dependent Enhancement: Several years ago, scientists were developing a vaccine against Dengue Fever, a mosquito borne disease which causes debilitating joint pain in patients. Some time after trial vaccination, several vaccinated patients died suddenly of Dengue Fever. This became the most studied example of Antibody Dependent Enhancement (ADE). Normally, for the annual flu let’s say, a person gets infected by the flu, is sick for a few days, and the immune system develops a response by creating antibodies against that specific strain of the flu. If they are exposed again in a month, nothing will happen. If the patient is exposed to a different strain the following year, they may still get sick, but the antibodies they developed the year before may help them have less severe disease and recover more quickly. Part of the immune response is that some immune cells display antibodies on their surface to capture new invaders.
With Dengue and some other viruses, the first stages are normal. A person gets infected and develops a response. If they get re-infected a month later, nothing happens. But if they get infected with a slightly different strain months or years later, instead of being protected, the virus attaches to antibodies displayed on immune cells and uses the antibodies as a site of entry into the immune system. The immune system is quickly infected, and the patient has a more severe disease with the second infection. Some estimates are that disease may be 3-4 x more severe in these patients.
As it turns out, SARS-1, which arose in 2002, and MERS, which has small outbreaks every year, are both Coronaviruses and both appear to be able to use the ADE pathway. This raises the possibility that SARS-2, the current virus, can also use the ADE pathway. This means that a person infected for a second time with a different strain of SARS-2, or any other Coronavirus for that matter, may be at much higher risk for severe disease.
This is why I’m not in favor of pursuing herd immunity as a pathway out of this crisis, because it will prime people for ADE related problems if a similar strain should strike next year.
This is not a new idea. If you search for “ADE” or “Antibody Dependent Enhancement”, you will see many articles, some peer reviewed from respected journals, on the phenomena. Dr. Fauci has even referenced it using the term “enhancement” when talking about vaccine development.
Why haven’t the government public health departments been more open about this? They tend to make statements only based on what they can be reasonably certain of, which is why they have been so slow to react to many aspects of the current crisis.
Again, it’s not certain that ADE will play a role next year. It’s too early to know. I’m informing you of the possibility so you can make wise decisions for you and your family.
This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, they are much more rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable virus can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim recently that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include respiratory conditions like asthma or COPD, heart conditions, kidney conditions, liver disease, diabetes, obesity, auto-immune disease, use of NSAID anti-inflammatory medications, being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant), vitamin-D deficiency, type A blood (Type O appears to be protective), inadequate sleep.
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms.
Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection, or lowers the viral load of exposure. Some, but not all, also prevent the wearer from inhaling airborne virus. N95 style masks without a valve are best if you can obtain one.
Best option: An N95 mask with no valve.
Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
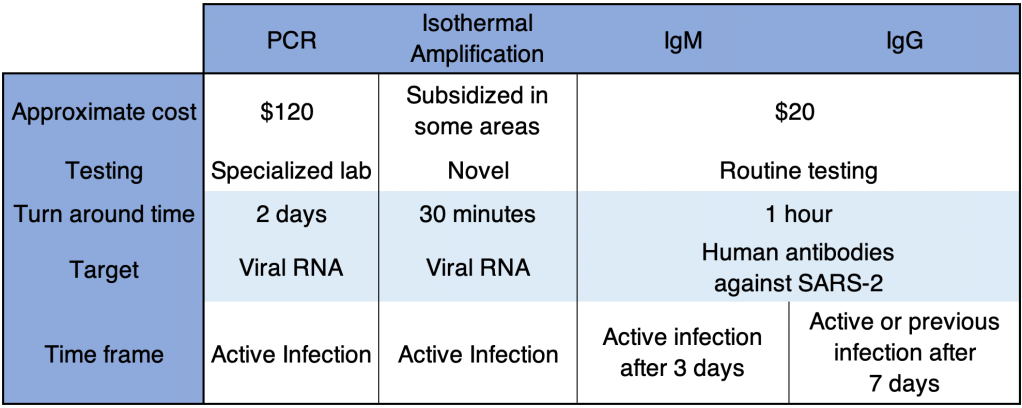
Testing: There are several kinds of tests, and they tell you different things.
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR and are both sensitive and very fast.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Ventilators: Some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor a nasal cannula, using ventilators only as a last resort if breathing is labored.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. I’m still holding a “wait and see” posture with this treatment.
MATH+: This regimen uses Methylprednisolone (an anti-inflammatory), Vitamin C, Thymine, and Heparin, as well as optional other treatments including Vitamin D and Zinc. Early reports suggest success with this treatment.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Early estimates for a Coronavirus vaccine were around 18 months. My guess is that this is too optimistic. Personally, I wouldn’t count on a vaccine for at least a few years. In addition, some studies have suggested that Coronavirus vaccines in particular may cause side effects that may make vaccine development challenging. My standard practice for my family is to wait on new drugs for a few years before using them myself. While I pro-vaccine in general, I would personally recommend waiting for a few years before getting a Coronavirus vaccine.
Herd Immunity: Some are promoting herd immunity as a way to move through the crisis faster. The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. This is a good idea when a vaccine is available, but not when there is no vaccine. Putting many people in harm’s way to protect fewer others is not wise and is not standard medical practice.
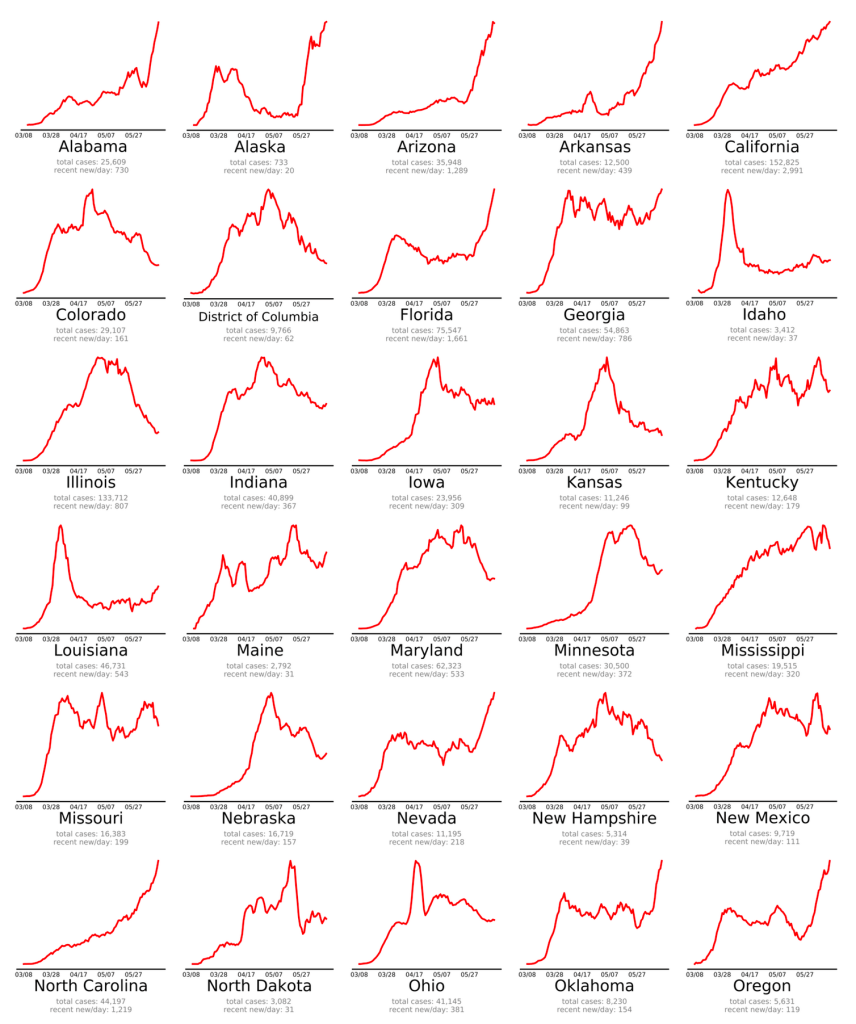
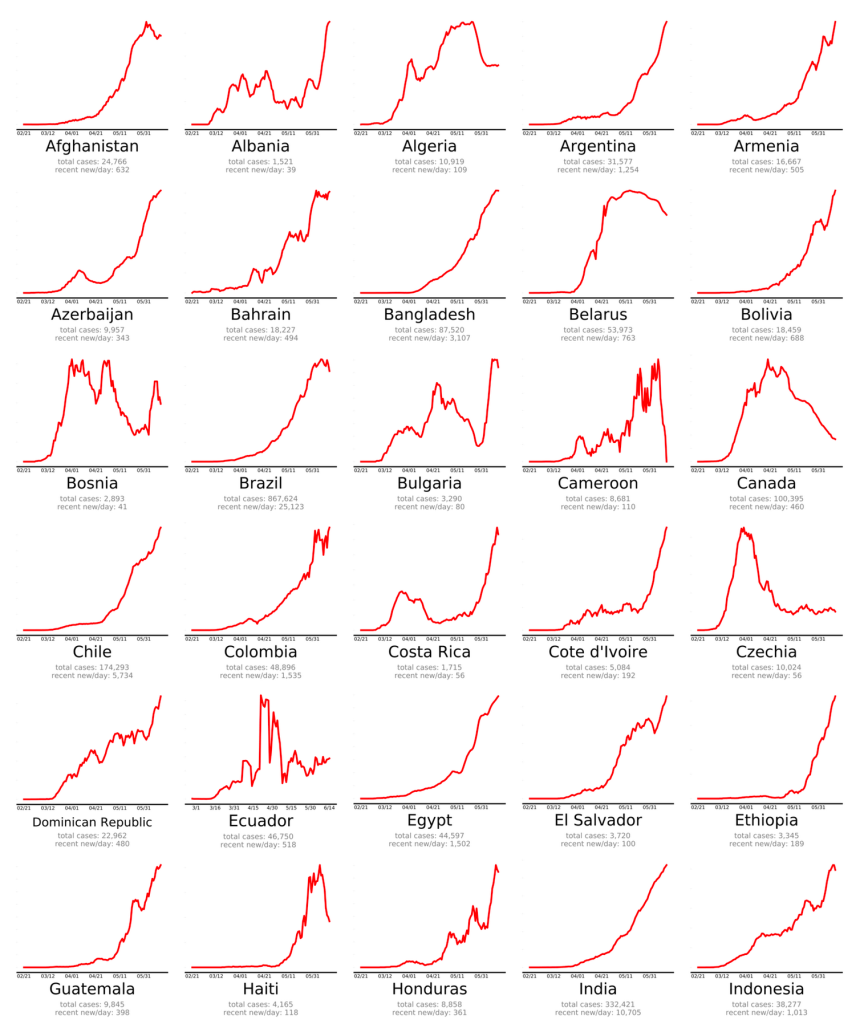
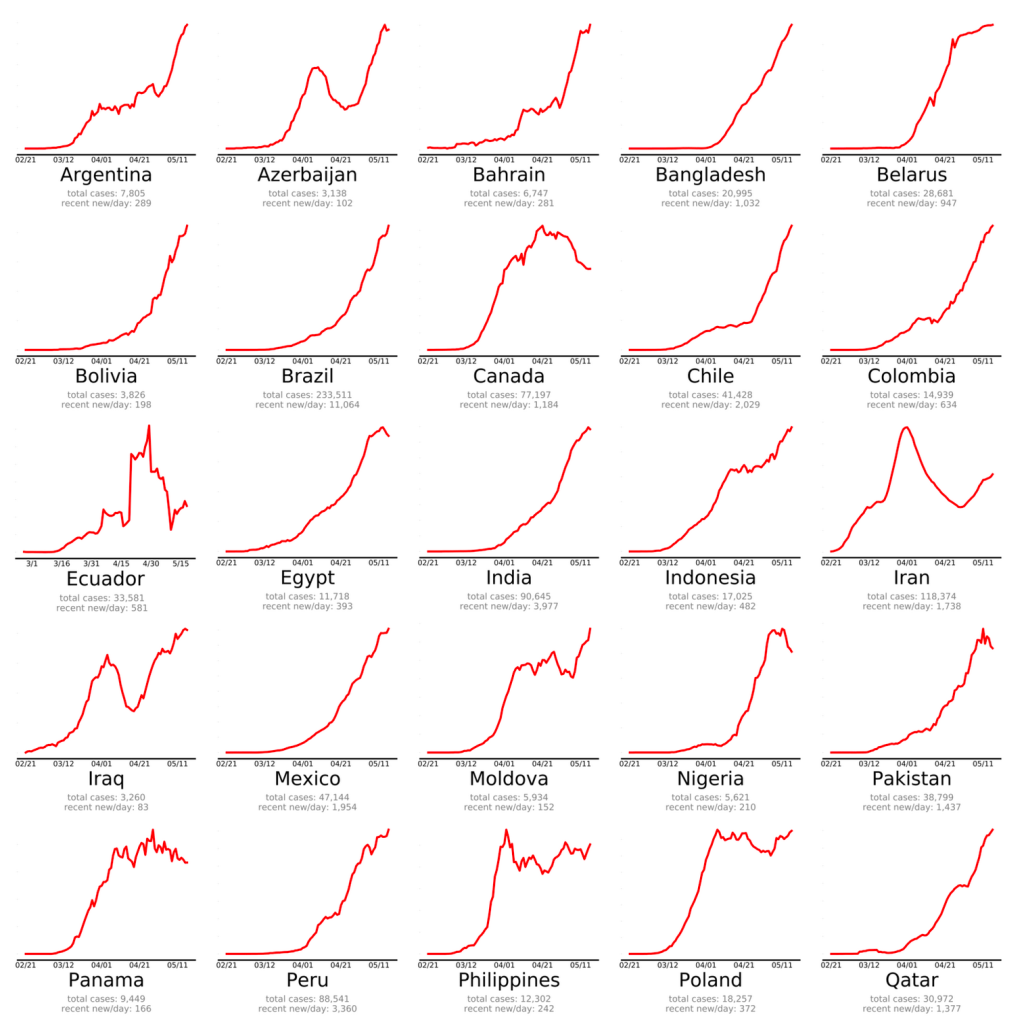
The Future: Of course, it’s impossible to know what will happen next. My initial prediction was that the first wave would be over by July, and at this point, this doesn’t look likely. New confirmed cases have started to rise or rise faster in the 3 areas I monitor most closely, the US, California, and San Diego County, and cases are rising fast in some countries previously unaffected, especially Brazil, Russia, and India. So I’m starting to think we may not be out of the first wave before the Fall season.
In addition, RNA viruses, such as Coronavirus, can mutate very quickly because the proteins used to copy their genomes are very error prone. This means that a virus may change to a new form that can re-infect a person who has already had a previous version. Some reports suggest that this may already be happening with SARS-2. Some good news is that on the very long term (years), novel viruses tend to evolve to be less virulent, because it’s not in the “interest” of the virus to make the host very sick. The message is, we may need to adapt to a new reality for the next few months or years. We can’t really afford to be “locked down” anymore, but mask wearing and elbow bumps may be a part of the landscape for some time.
This is a case update. New confirmed cases are starting to trend upward for the US again for the first time since about April 9. In 19 US states, the Rt number is higher than 1.0, suggesting that the virus is spreading in these states. On endcoronavirus.org, you can clearly see recent spikes of new cases in some states, and in many countries.
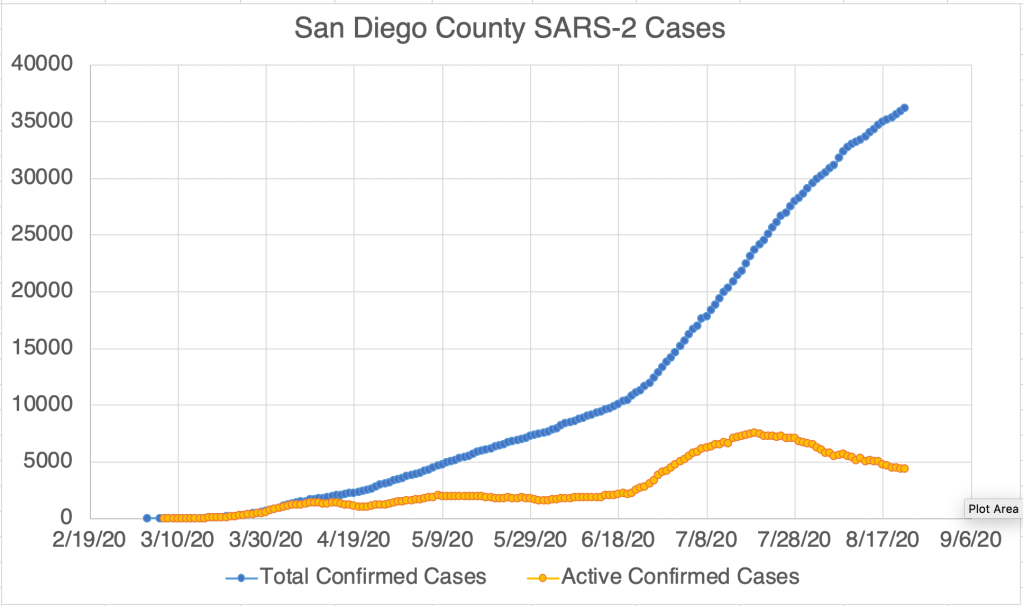
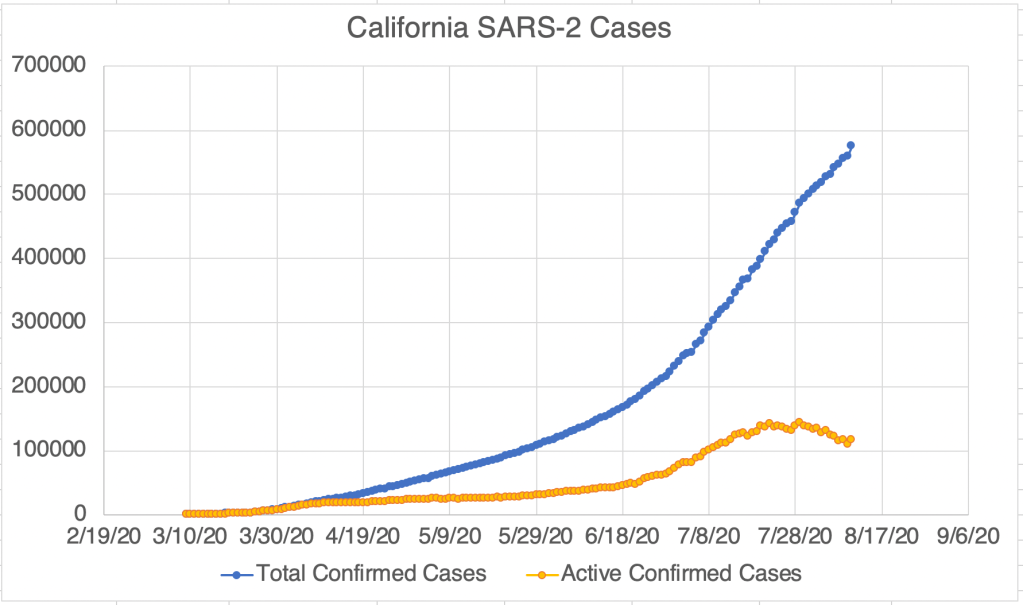
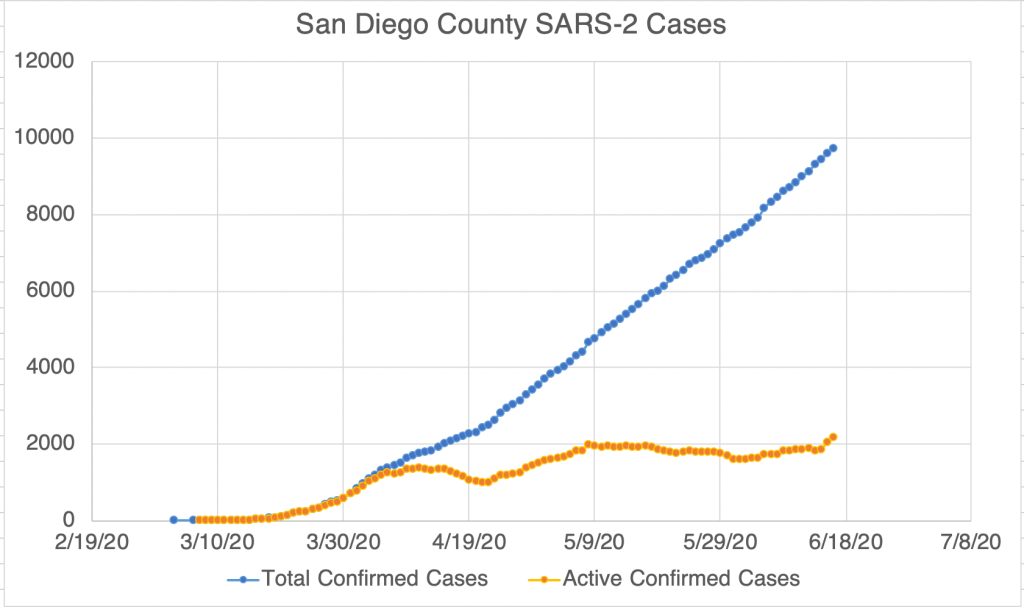
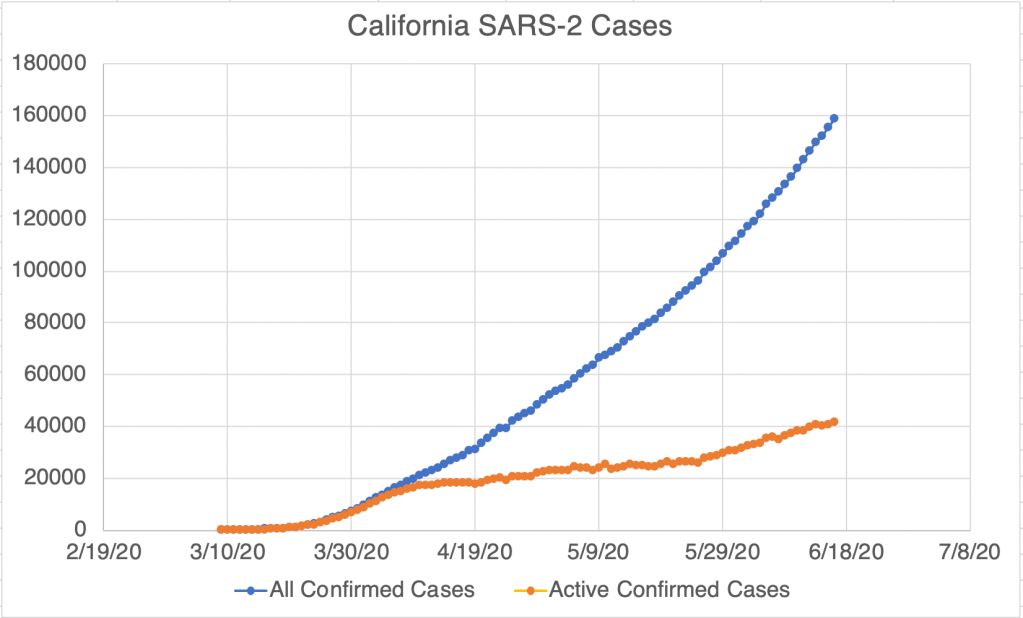
In California, the number daily new cases continues to accelerate. San Diego has started to go up too. San Diego County has started to publish the number of recovered patients. My graph of cases in SD County now includes active cases, taking recovered people into account. Some of these points of data on my graph are given by SD County, the others are calculated by me based on the data points. Looking carefully at the SD County data, the number of recovered people is approximately the number of total cases from 17 days previous. The suggestion is that it takes approximately 17 days to recover after being confirmed as a COVID case, so I’ve made a similar calculation for California. Just to be clear, in my graph of active cases in California, the data points are based on assumptions about recovery time, not actual data.
For San Diego, active cases have been hovering around 2,000 for several weeks, without much change, but for an increase in the last few days. For California, we’ve seen a steady trend upward in active cases from 20,000 in early April, to 40,000 cases today. There are of course lots of potential reasons for these increases, from gradual re-opening to the protests and riots stemming from the George Floyd incident. I was once optimistic that the first wave of cases would be over this Summer, but new trends have called this into question. I’m now feeling totally unable to predict how things will go.
I heard a radio commentator talking about a recent study that I haven’t been able to find. The study said that while Social Distancing account for maybe a 50% drop in new cases, the lockdown accounted for only a 5% additional drop. Given the economic and social cost of the lockdown, the study suggested they were not on the whole worth the cost. If you’ve seen the actual study, please post it in the comments!
So please continue to social distance and wear your masks in public! But it’s time to figure out how we can get the economy running again! We have big problems to solve, time to get to work!
Yesterday right after I posted, Mark Rasmussen sent me an article that ran in Science Magazine, one of the 2 most highly regarded science journals in the world. It’s a news article, not a peer-reviewed journal article, but it attempts to pull together information from different sources, and I think clarifies the picture regarding SARS-2 viral spread. The take-away message of the article is that while the R0 appears to be between 2.5 and 3 (more on that later), it’s not true that the average individual will pass the virus on to 2 or 3 others. Rather, most infected people don’t pass the virus on to anyone at all, rather a few infected people are “super-spreaders”, infecting a large number of people at once. There are many documented cases of super-spreading, from choir practices, funerals, concerts, fitness classes, and meat packing plants. The commonality appears to be indoor locations with lots of people in a small space, with some of them shouting or singing. While the risk in outdoor venues isn’t zero, indoor venues account for 19 times the number of super-spreading events, according to a Japanese study.
According to the article, SARS-2 has a tendency to cluster in this way more than other respiratory diseases such as the flu or colds. This may be partially because of the “viral load” effect mentioned in the Erin Bromage article I posted on May 12th. In that article, it appears that the initial number of viruses an individual is exposed to partially determined if they will be infected, and how sick they will get. This also explains why so many medical workers in Italy got very sick or died in the early stages of the pandemic. Many medical procedures such as intubation create a bloom of floating virus from a sick patient, exposing unprotected workers to high viral loads.
The science article suggests that while the virus is still dangerous and outdoor venues are not completely without risk, it may be appropriate to relax restrictions on some outdoor activities. So here’s my informed but not expert advice on how to adapt to life with COVID:
Staying at home all the time may no longer be the best approach, although it was probably very helpful in the early stages of the pandemic. Going outside to get some fresh air and exercise is probably a good thing, although still not without risk.
When doing outdoor activities, it’s probably OK to not wear a mask, but maintain at least 6-10 ft from others you don’t live with. Locations with a gentle breeze will help move virus away from you!
At work or shopping, wear a mask when around others to reduce the viral load that you are wafting into air should you be infected without your knowledge. Any reduction in viral load will help.
If you suspect you may have been exposed, contact your physician and see if you can get a test.
If you have a yard, invite a few friends over for lunch or dinner at a safe distance. Since Summer is starting, an evening outdoor dinner will be a welcome break from the isolation. You may want to have your guests bring their own food and utensils. Don’t invite a large number of friends, and sorry to say, don’t invite those friends who can’t resist hugging everyone! Young children may require supervision to be safe.
Now that restaurants are open in California, I would personally only be comfortable with outdoor seating at the moment. If you’re comfortable, visit your favorite local restaurants to give them some business, sit outside, and leave your server a big tip if you’re able!
I am a church goer, and I want to see my peeps again, but singing in a congregation is still a high-risk activity. Churches will need to be creative to open up again safely. Consider lower density services without singing, and/or hold services outdoors.
Regarding the R0 value for SARS-2. I saw a CDC website last week that gave the R0 value as 2.5. After 10 minutes of looking, I couldn’t find this site again. The Sanche paper I’ve referenced before (High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2, EID, July 2020), published in the official CDC journal, Emerging Infectious Disease, gave the R0 as 5.7. So the CDC itself seems confused about what the R0 number is. My guess is, it’s somewhere between 2.5 and 5.7. That was a joke. Obviously, this range is far too large to be useful, and 2.5 and 5.7 are very different as applied to an R0 number. 2.5 is a very infectious disease, 5.7 is a super-infectious disease.
I’ve mentioned this before, but I want to remind everyone. Herd immunity is only a goal when a vaccine is available. Seeking herd immunity when there is no vaccine is not a good idea, because it will put large numbers of people at risk. Additionally, I am generally very pro-vaccine, but because of the risks of side-effects with this particular virus, a vaccine may not be available for several years. We will need to adapt to this reality. My hope is that we will start seeing daily cases come down this Summer.
Today I’m going to discuss the JP Morgan study on transmission (among other things), how the Moral Matrix effects how people see the fight against the virus, and the boom stage in many Southern Hemisphere countries.
JP Morgan has produced a study suggesting among other things that lockdowns are ineffective in fighting Coronavirus (see also a summary from Daily Mail). The reasoning for this is primarily that transmission is most common in households if a member becomes infected.
Frankly, when I think about anti-coronavirus efforts, I have tended to lump lockdowns and social distancing together, especially since many use these terms interchangeably. Notably, the study separates these 2 concepts and suggests that will social distancing (staying a distance away from people in public) may be valuable, lockdowns (staying in your home) is not.
You might say there have been 2 primary models for dealing with the pandemic in the last month after we’ve flattened the curve, but have not brought the numbers down, at least not in the US. I’ll call those models the Lockdown and the Re-opening models. Some want to continue the lockdowns to keep everyone safe from the virus, others want to re-open right away without restrictions. For several weeks, I have been gravitating toward a third Adaptive model. Of course, there can be many flavors of this model. Personally, I think masks, even bad ones, are far better than nothing, especially when worn by everyone, and can help us get back out of our houses and help us re-start the economy with reasonable safety. So I’m very open to the idea that the lockdowns have not been beneficial. Some of you will disagree.
The JP Morgan study is at odds with the endcoronavirus.org study, which recommends brief, very strict lockdowns. It could actually be that these 2 studies actually agree, depending on the time frame you’re talking about. I do think the lockdown was very helpful in the initial “boom” stage of the epidemic here in the US, but may have lost its usefulness later.
The Moral Matrix: ZDoggMD is a physician and medical YouTuber with a very silly screen name, but who posted VERY interesting video on how different people see the pandemic we are all facing. Using Jonathan Haidt’s work on the Moral Matrix, he talks about how different people’s moral framework shapes how we are viewing different efforts to address the issue. I was aware of Haidt’s work, but not had yet applied it to the pandemic in my mind. As someone who is sometimes exasperated with people who disagree with me (as they are with me I’m sure), this video is helping me remember to see their point of view. If you’re exasperated with your friends or family, I HIGHLY recommend you watch this video.
Upsurge in the Southern Hemisphere: Lastly, I just want to mention that many countries which have been relatively little effected until now, are now experiencing a big upsurge in cases. These countries include Russia, Brazil, and Mexico, and many are in the Southern Hemisphere, which is in the late Autumn months right now. Let’s hope they are able to get things under control quickly.
Don’t fear, but be smart!
Erik
PS. We went hiking in nearby Calaveras Park today for the first time in months, without our masks. There were a lot of people on the trail, and most were well behaved. When I can’t avoid someone on a narrow trail, I use an old SCUBA diving trick for ascending without getting the bends. Just close your mouth and blow slowly out of your nose as you pass someone. You’ll gently move any virus away from your nose! To maintain my friendliness, I greet people early, with plenty of time to start this little maneuver!