This is a case update. I’ll also briefly discuss the future of the pandemic.
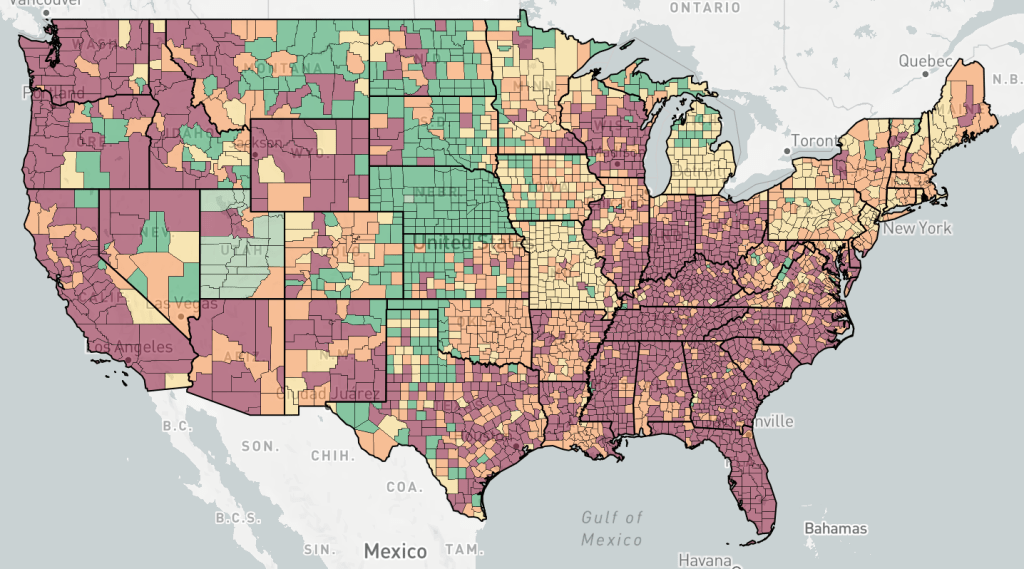
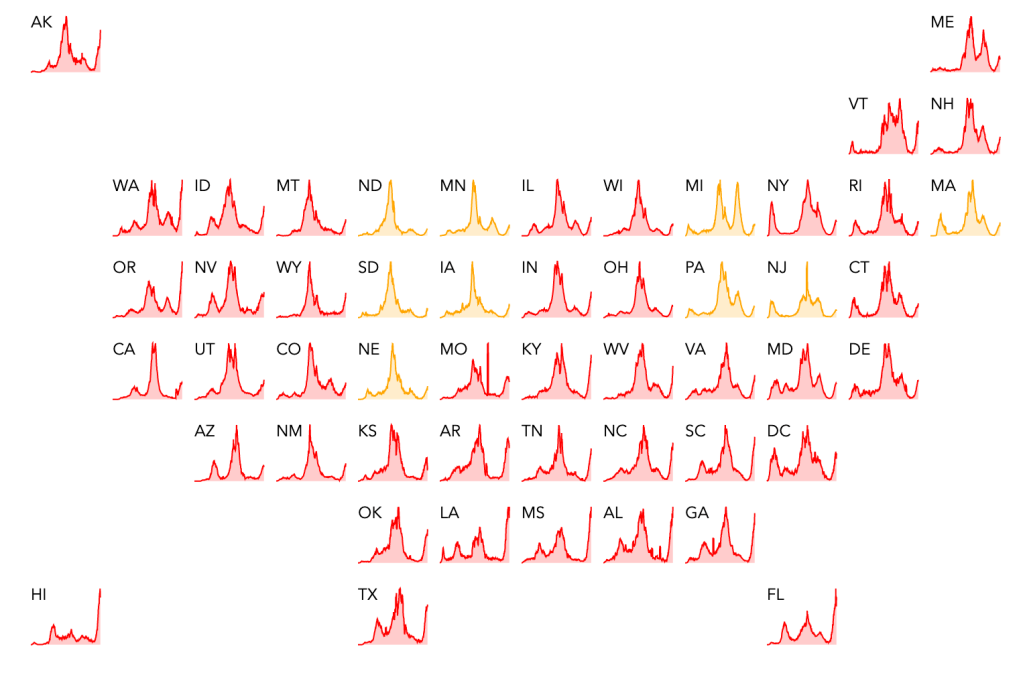
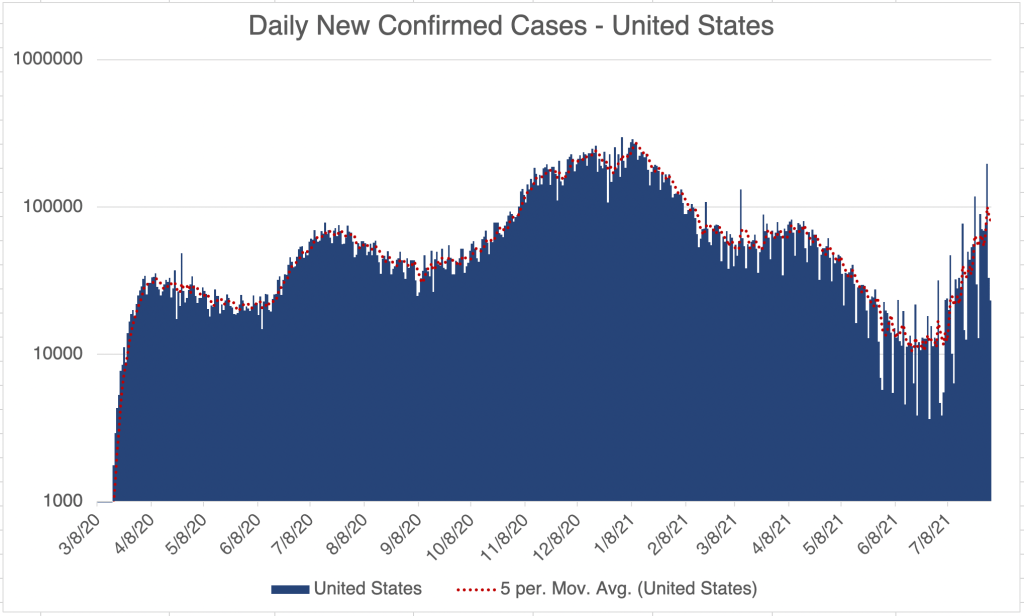
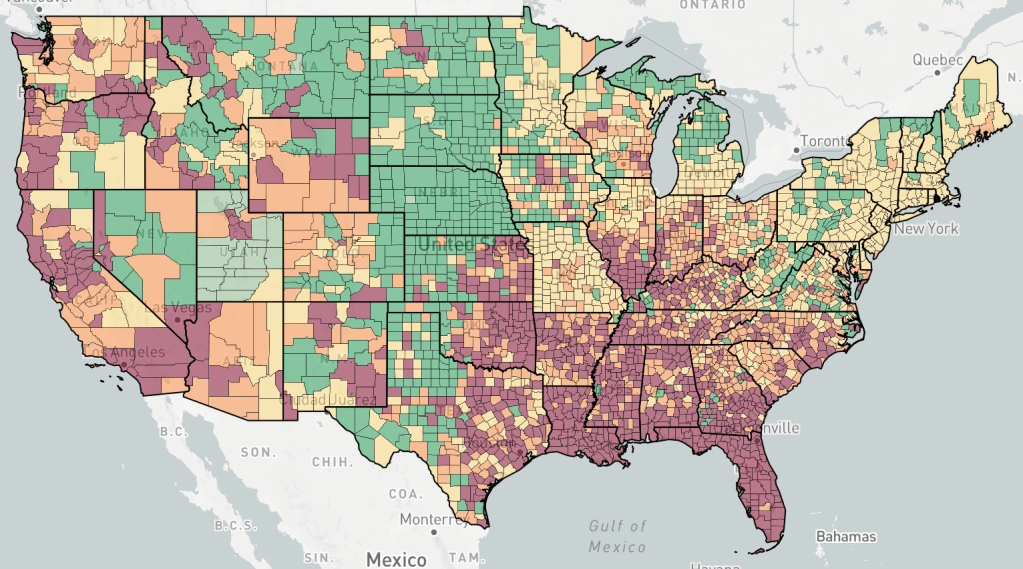
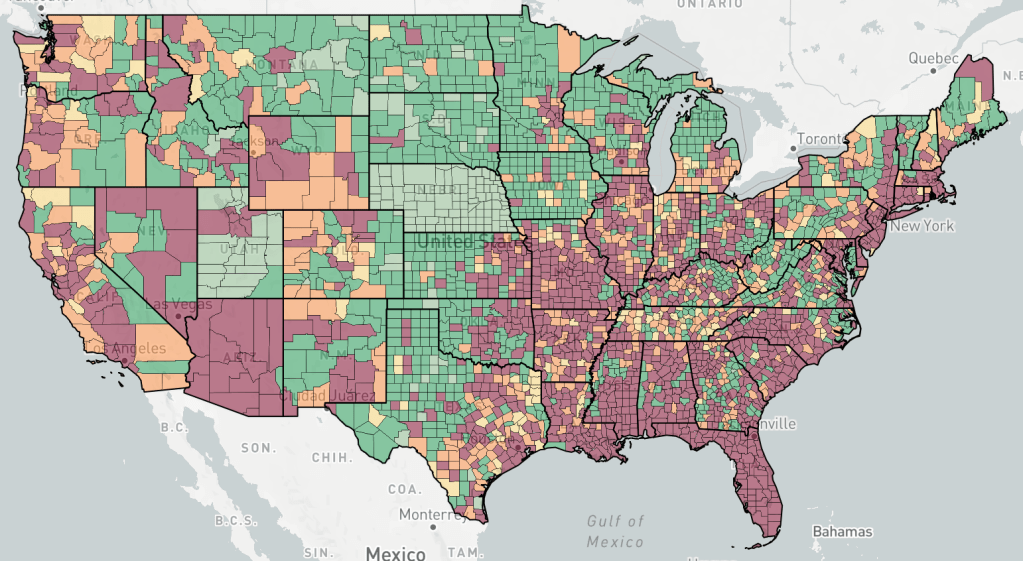
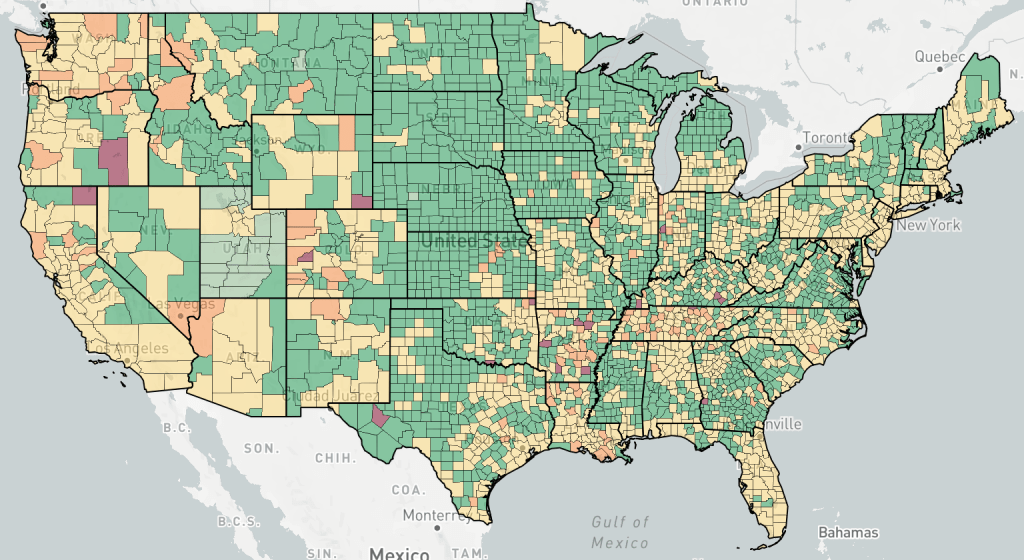
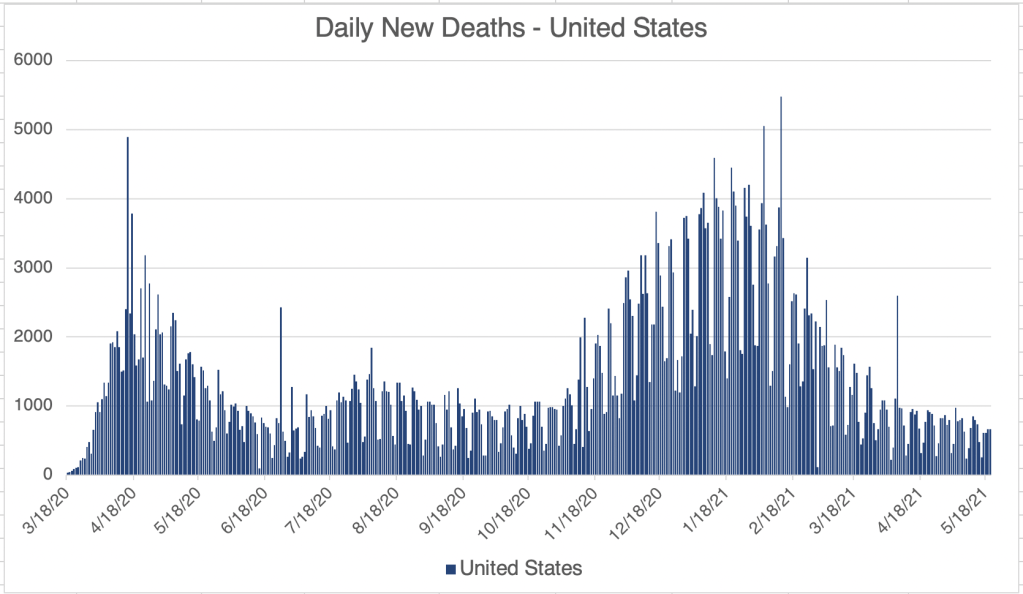
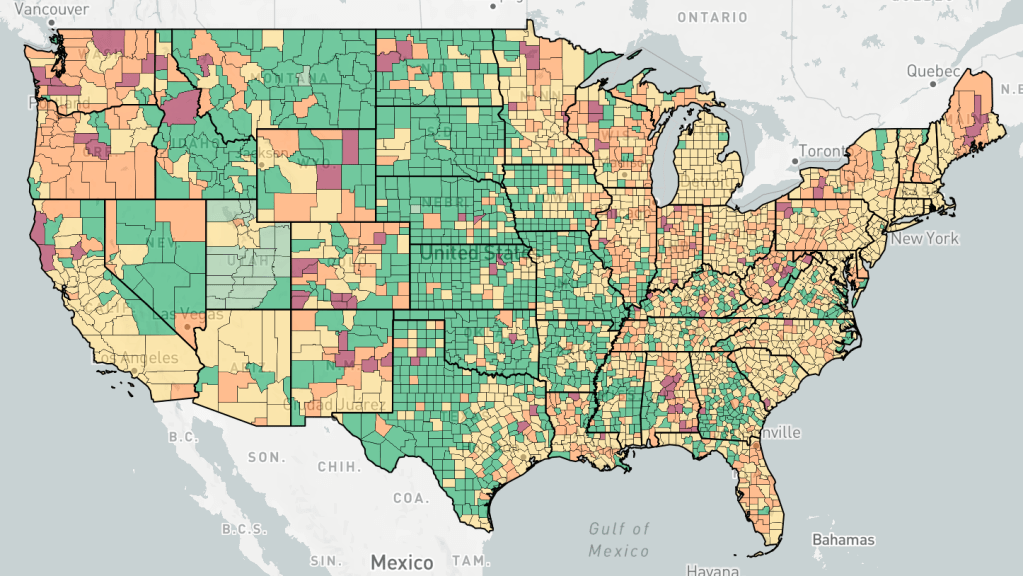
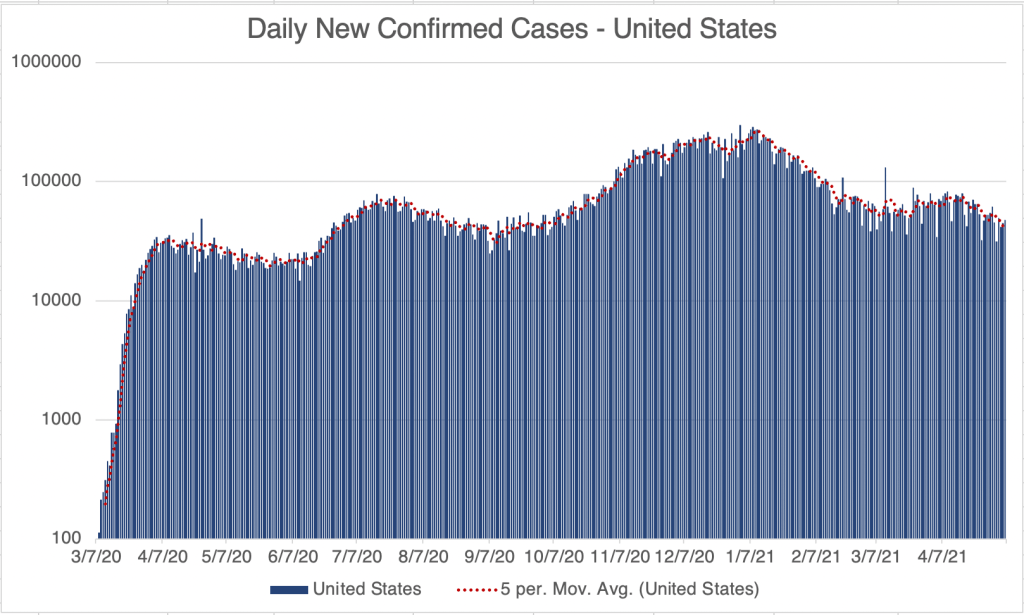
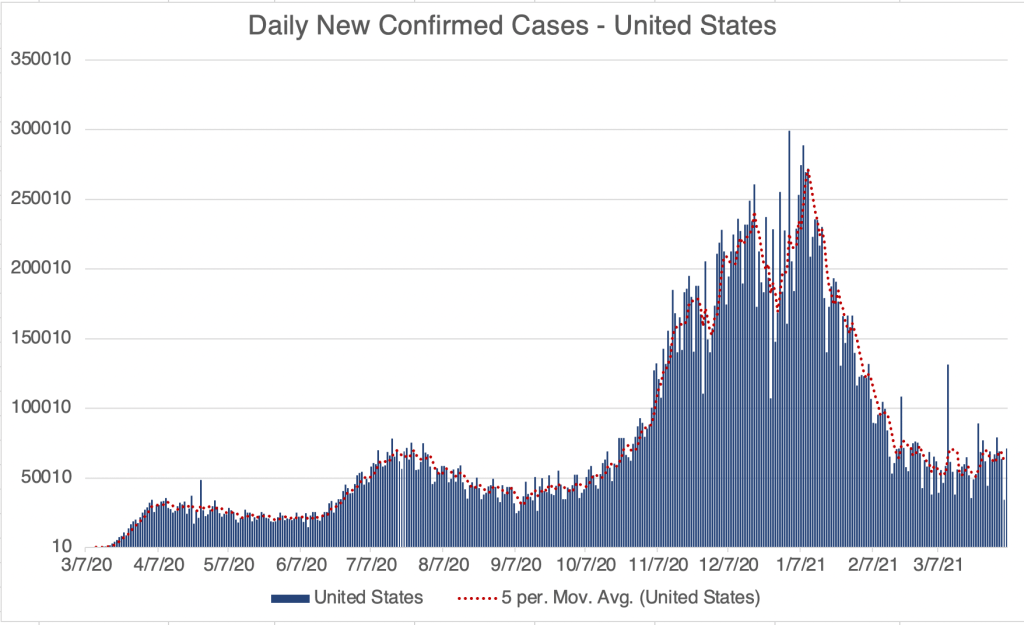
Numbers continue to rise in the US, but are definitely slowing in their increase. New cases are most prominent in the West and Southeast. New deaths are rising, but much more slowly than for other waves.
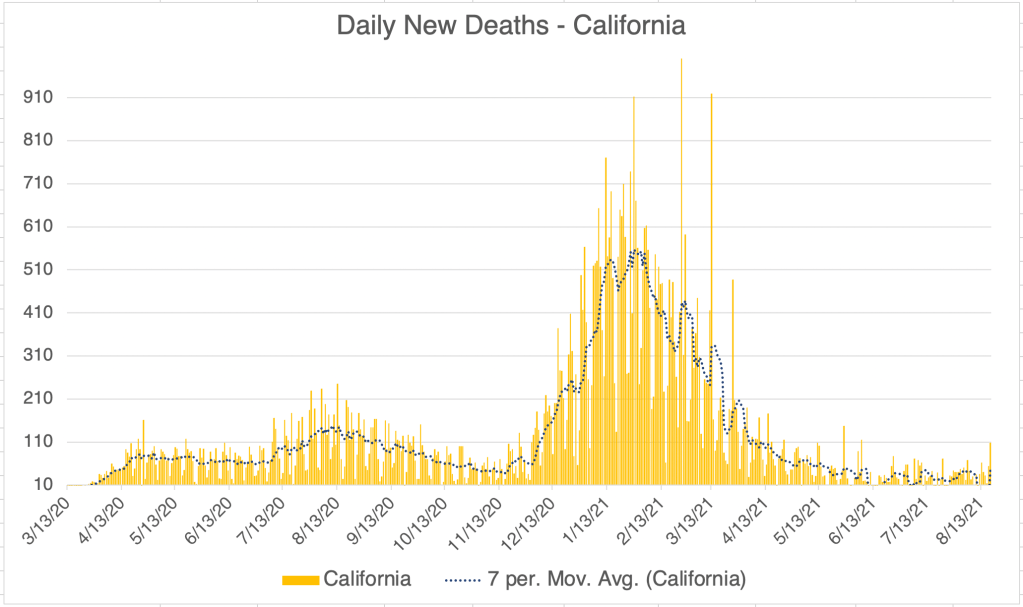
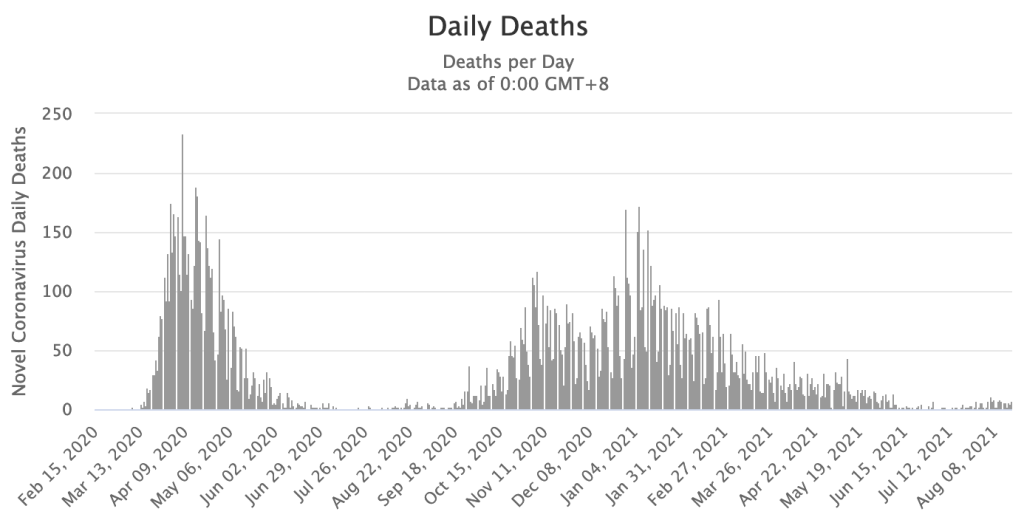
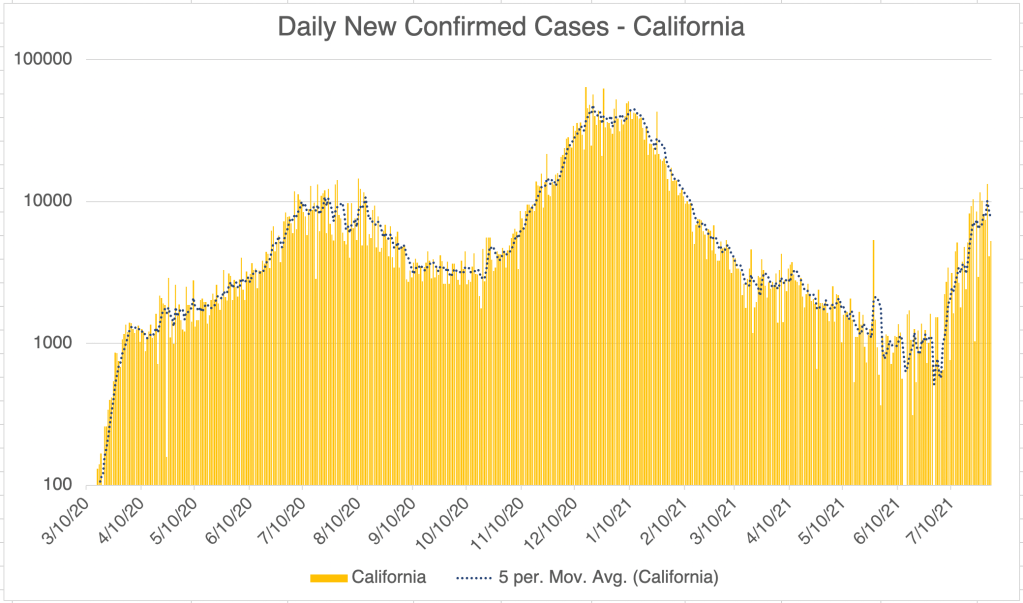
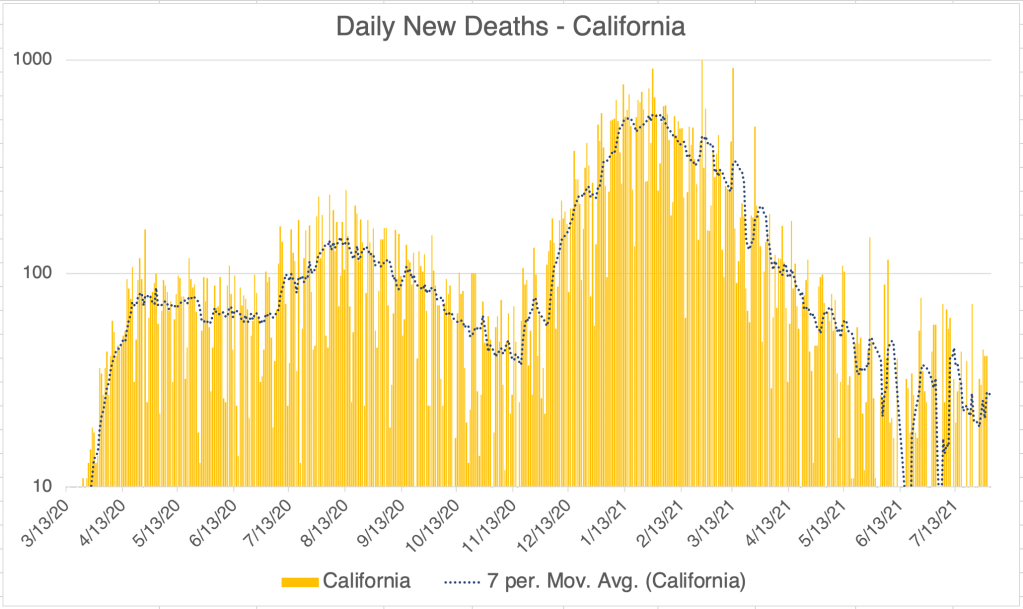
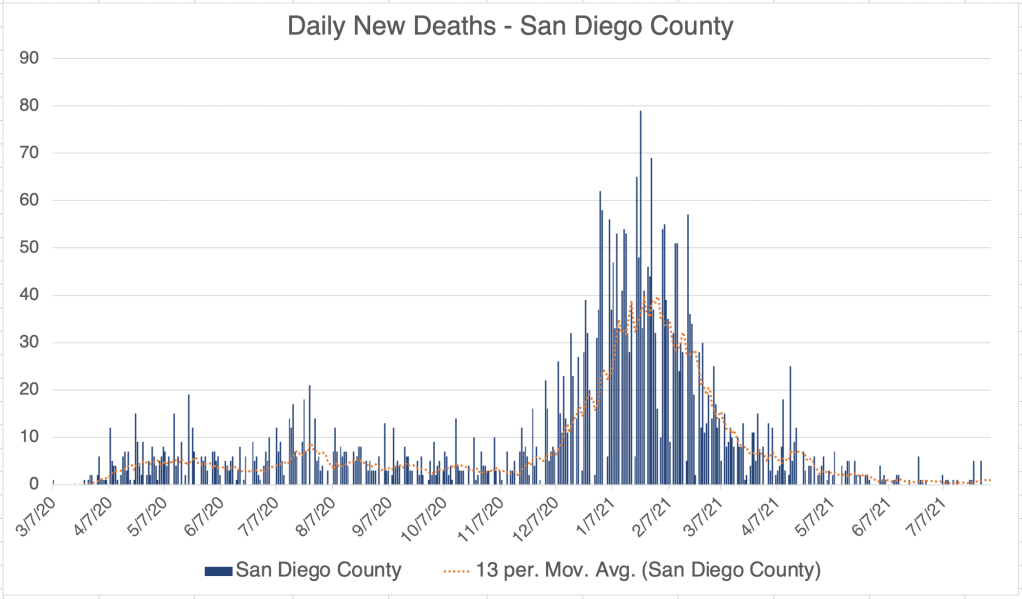
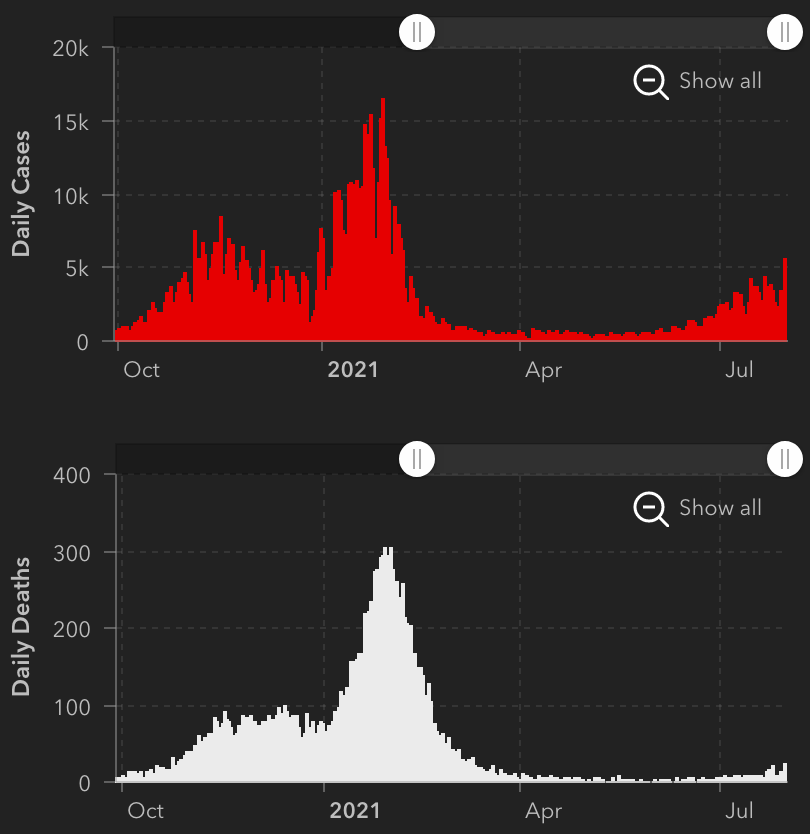
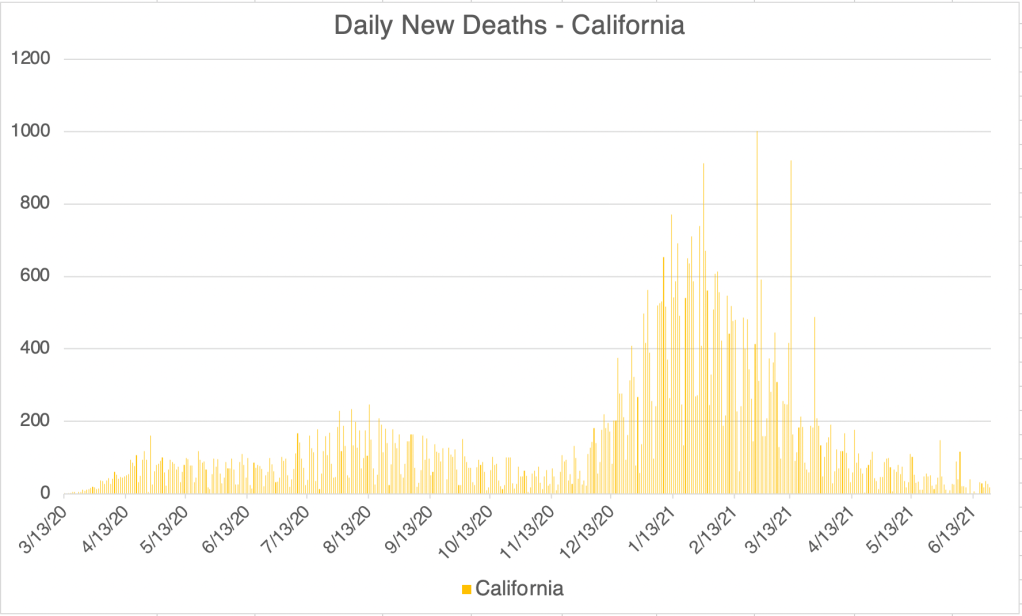
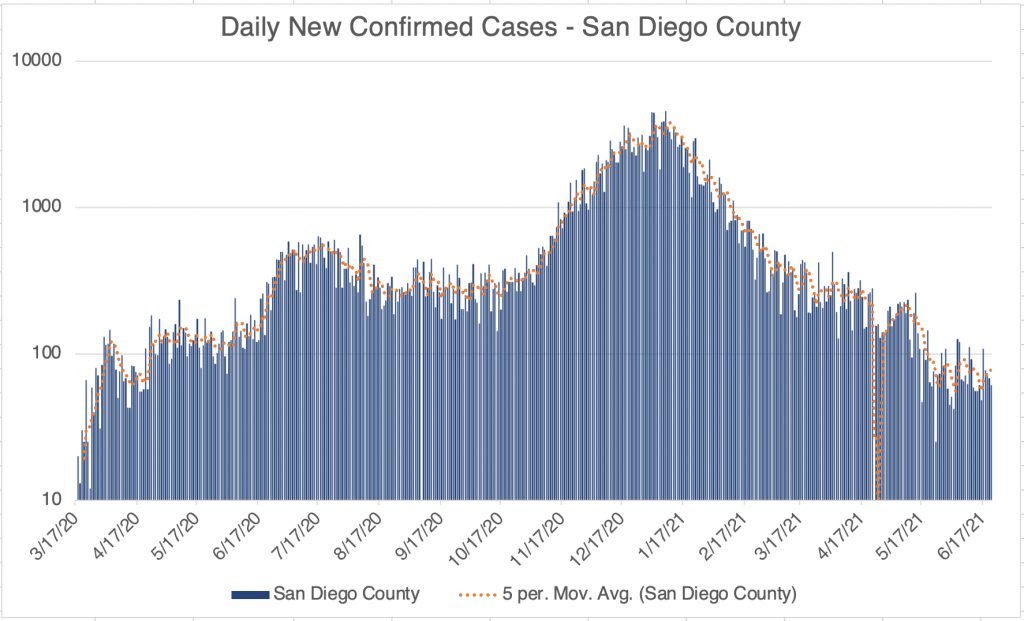
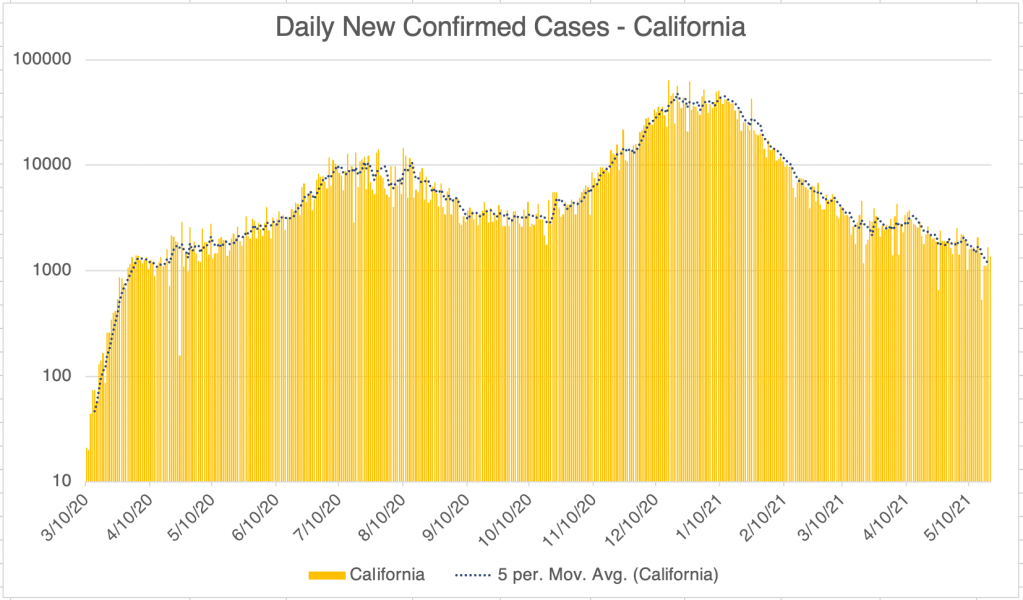
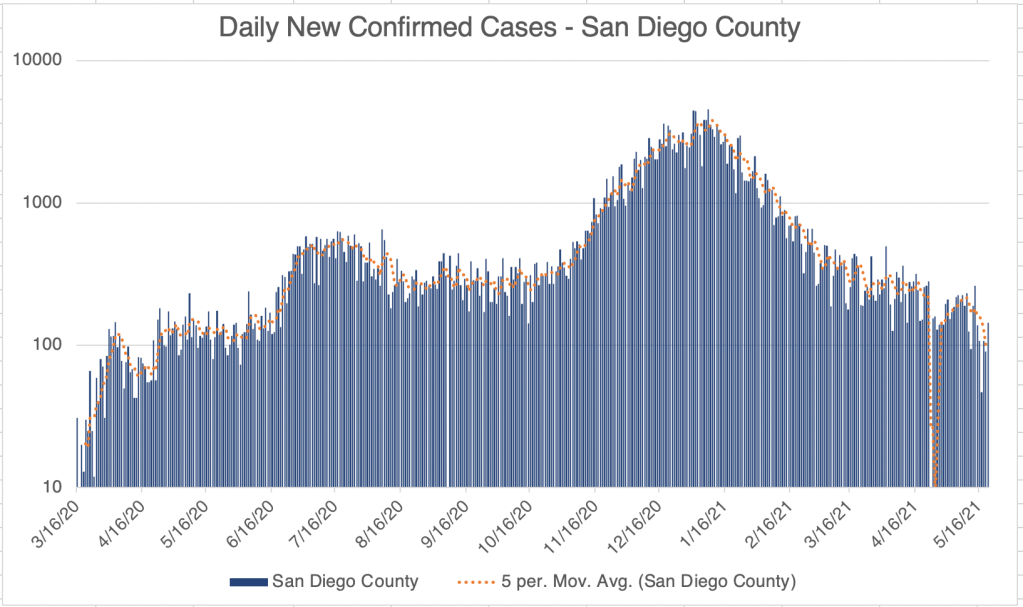
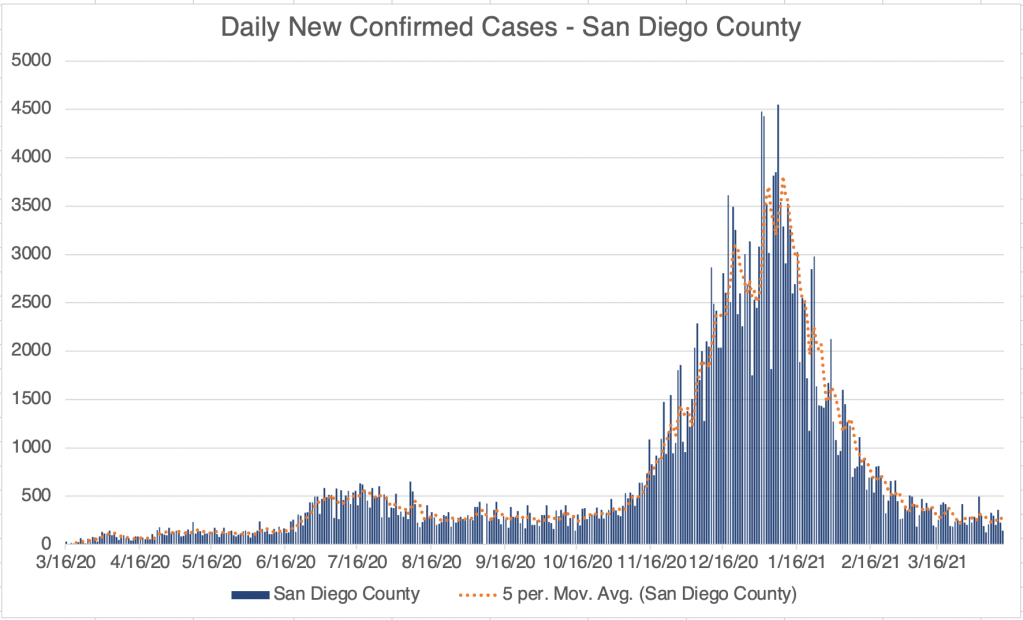
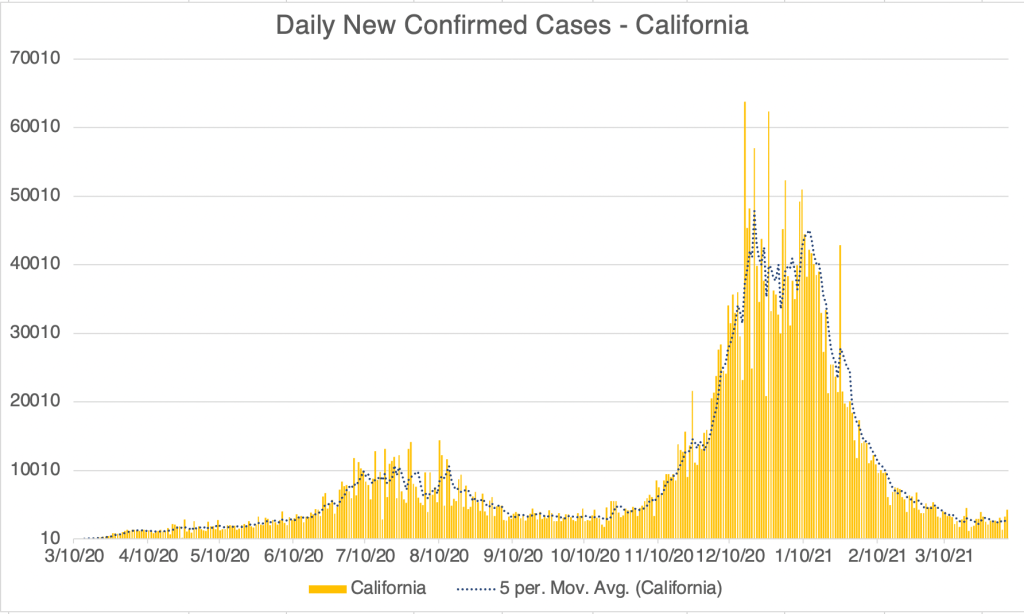
For California and San Diego, it looks like we have crested the wave and new cases are starting to head down. In both of these regions, new deaths are not really increasing at all. This supports the pattern that in vaccinated areas, large numbers of new cases due to the Delta Variant are not followed by large numbers new deaths. I mentioned a few weeks ago that deaths can trail new cases by as much as 4 weeks, but we are now 6 weeks into the Delta Wave in California and San Diego without seeing a significant rise in new deaths.
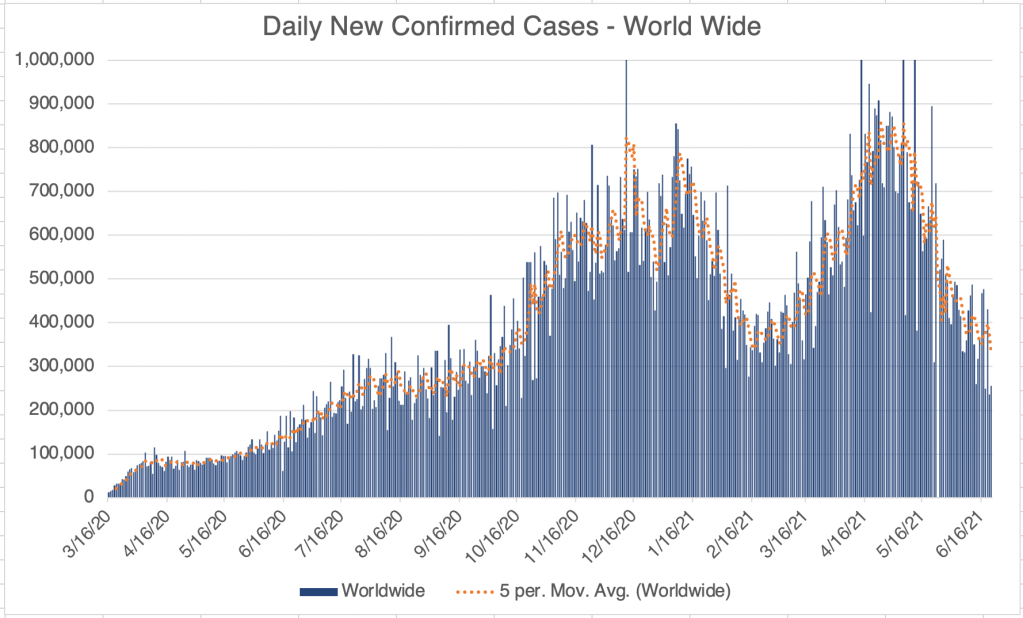
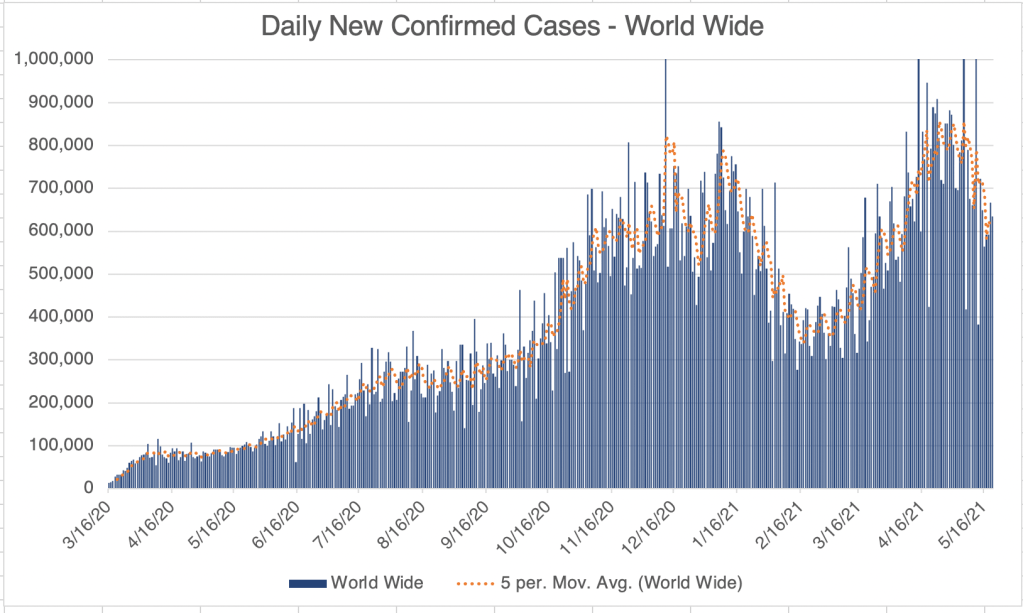
Internationally, new cases appear to perhaps have peaked world wide, but it will take some time to see if cases start to go down. As stated above, countries with vaccination programs are experiencing almost no new deaths due to Delta Variant. Numbers for the Netherlands are striking, and other countries like the UK, Sweden, Japan, and South Korea show a similar pattern.
Several sources I listen to are now saying that SARS-2 is now or will be endemic. For some background, an epidemic is an outbreak of a disease in a small area or region. Avian influenza and the first SARS outbreaks were epidemics, since they didn’t leave Asia. A Pandemic is an outbreak in a large area including several continents. A disease becomes endemic when it becomes a constant feature of life in an area. I would include malaria, seasonal flu, and HIV in the list of endemic diseases. Interestingly, Wikipedia still considers HIV to be a pandemic.
I have resisted calling COVID endemic. I don’t think it fits the criteria at this point. While there have been several new variants that have caused additional waves of cases, they are all at least partially impacted by the available vaccines, and presumably by natural immunity as well. While this is the case, I still think it is possible that we can eradicate the virus from the world at some point.When might SARS-2 become endemic? For me, that would happen if either new variants arose that were not mitigated by natural or vaccine driven immunity, or if immunity in vaccinated or naturally immune people ceased to be effective in preventing new infection. Both of these would allow SARS-2 to continue to circulate indefinitely.
Some have argued that vaccine mediated immunity is not as long lived as hoped. This may be why there have been many “breakthrough” cases in the last few weeks. However, Youtuber Dr. Zubin Damania suggests that while protected from new infection wanes over months, vaccine protection against severe disease is persistent, at least against the Delta Variant. This may explain our current pattern of low deaths despite high cases in vaccinated regions.
So is COVID endemic? I still say no, and hope it can be eradicated. However, some municipalities, including Norway and the state of Iowa, have declared that is endemic and will be a permanent feature of the world. If I decide that the data shows that SARS-2 is endemic, then that is the day that I will get vaccinated. ‘Cuz I do want to go back to normal life someday, but I don’t want to actually get COVID. Obviously, many vaccinated and unvaccinated folks have decided to go back to living normally, despite official calls to maintain vigilance.
Vaccination mandates: I have not been in favor of requiring vaccination in order to return to work, fly on commercial aircraft, or other activities. While I am all for precautions and continue to wear a KN95 indoors while in public, healthcare is a personal choice and should not be coerced. Some have even claimed that it is illegal to coerce a measure that does not have FDA clearance. While vaccination is a good choice for many, it does have liabilities that have made many resistant to vaccination. This should be honored.
I know several people in the healthcare industry who have not wanted to be vaccinated, and have quit or been fired from technical or nursing jobs. While an argument could be made that those working with patients should be vaccinated, it seems misguided to be letting go of nursing staff when there has been a long standing nursing shortage.
This is a case update, and it will come with a big correction from last week.
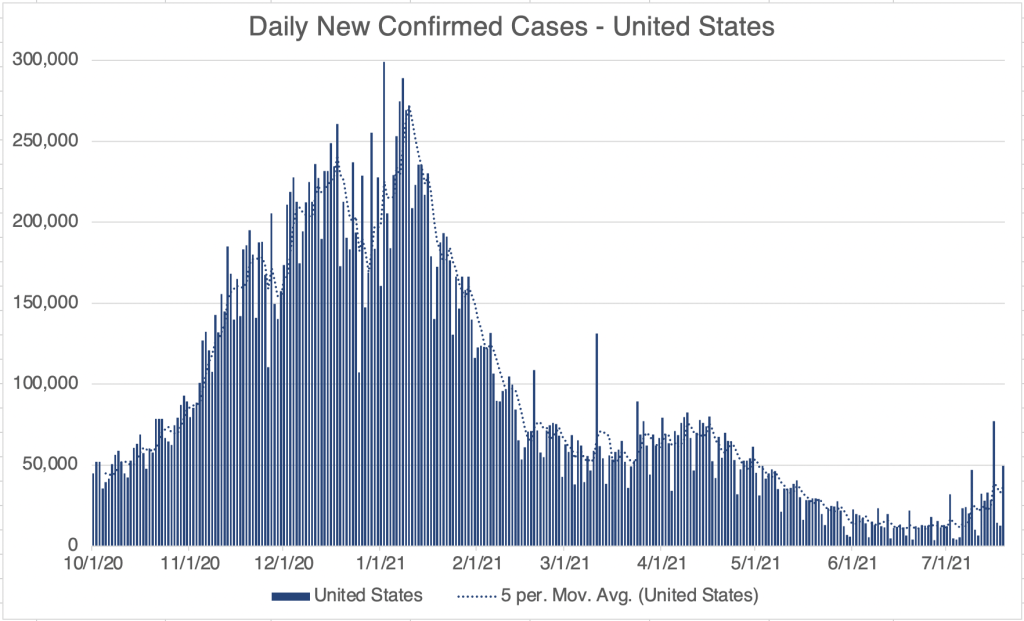
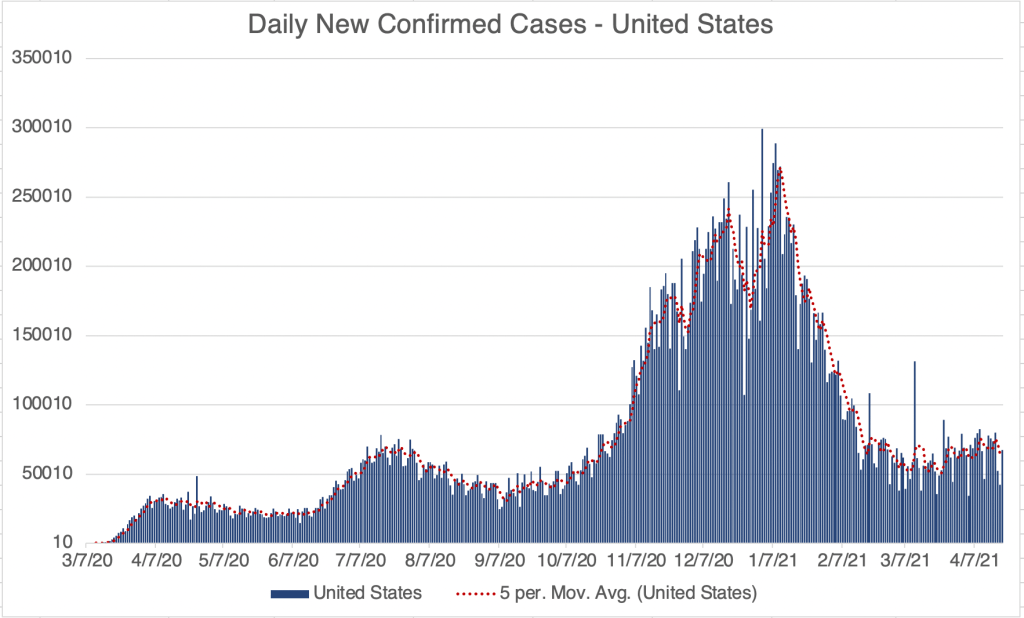
New confirmed cases continue to rise due to the Delta variant in the US, California, and San Diego County, although at a noticeably slower rate.
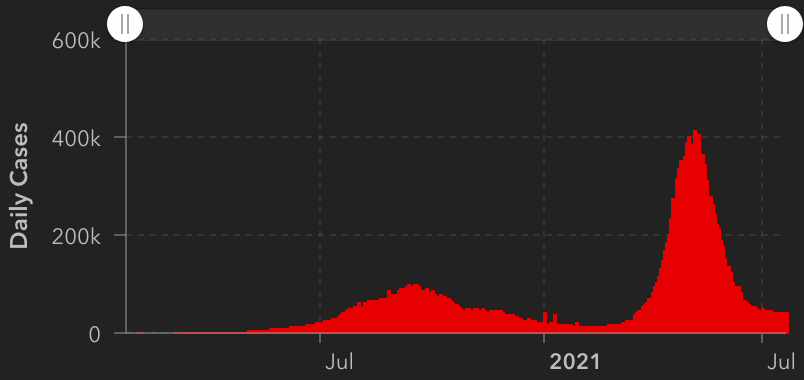
I said last week that we may see the peak in US cases this week because Sunday’s number was the same as the previous week’s. This week’s numbers were erratic, but continues to show an upward trend, with yesterday’s new case number being higher than last week’s. So we are still on an upward trend, but it is slowing.
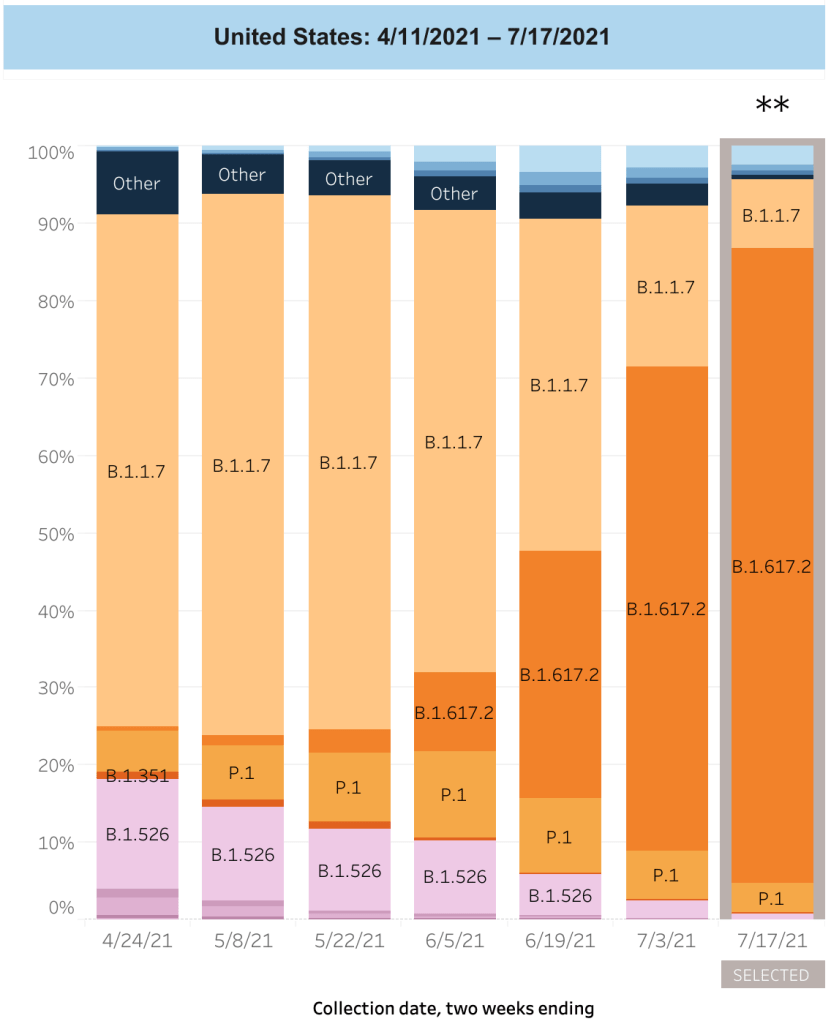
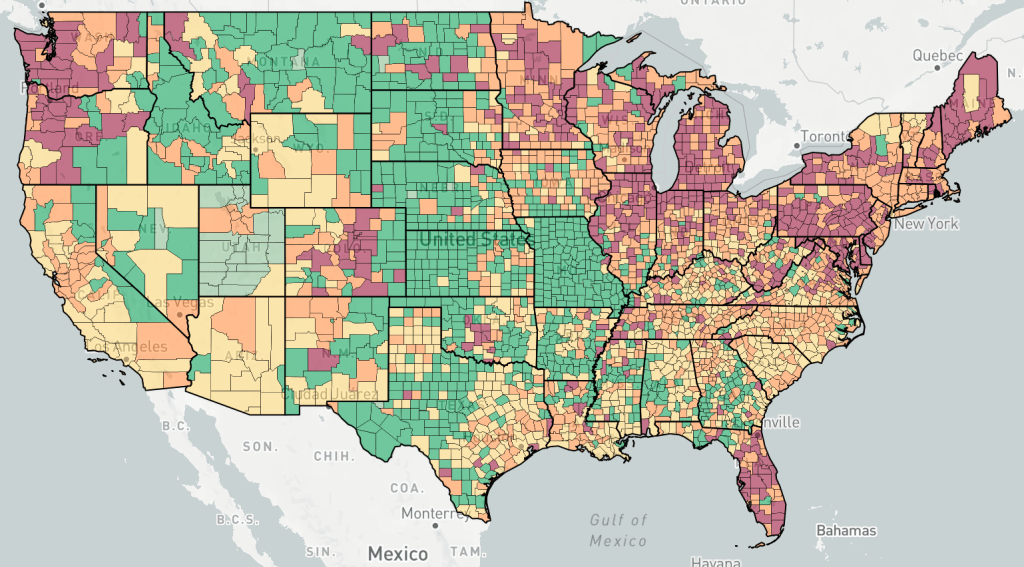
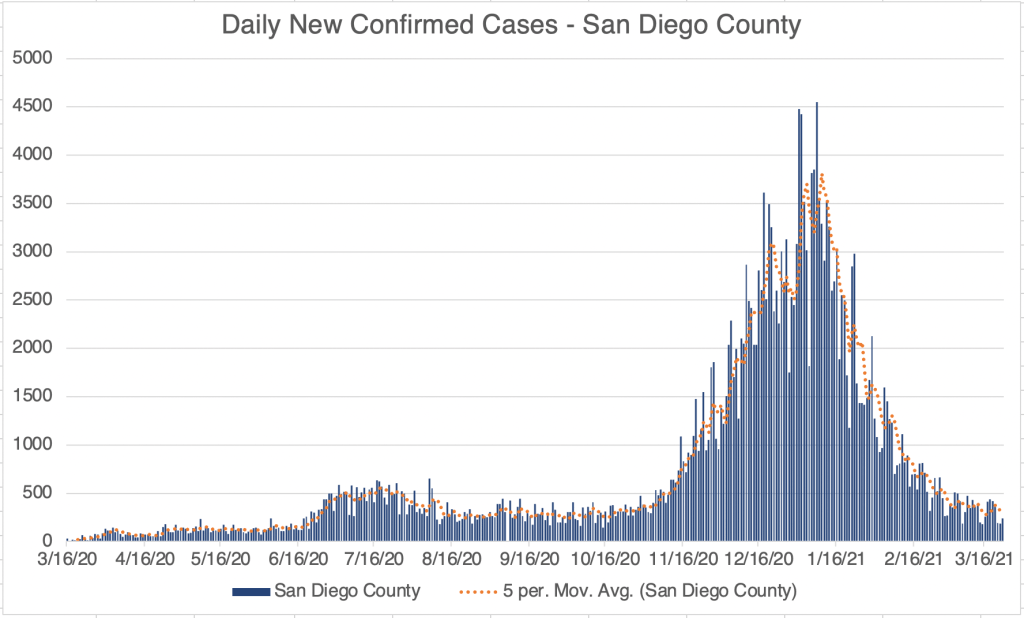
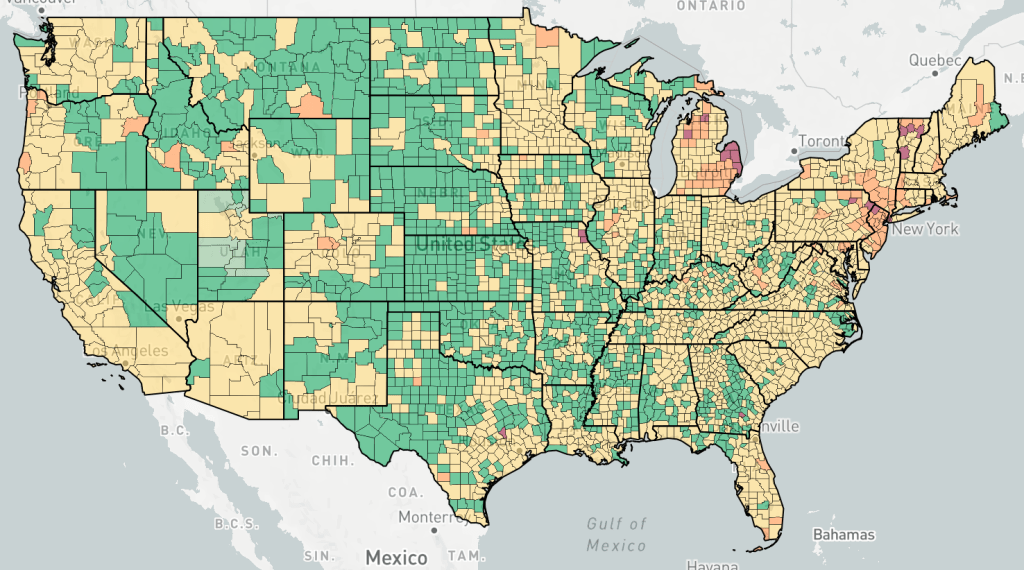
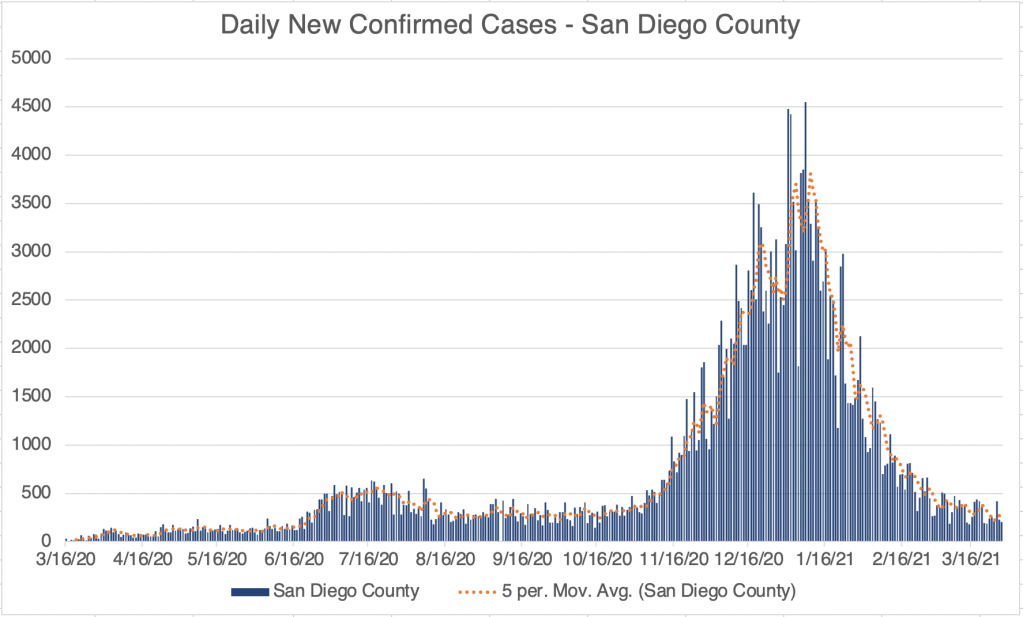
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Endcoronavirus County Level Map, August 1st, 2021Proportion of current cases from various SARS-2 Variants. The Delta/India variant (B.1.617.2) is in orange. From CDC data.
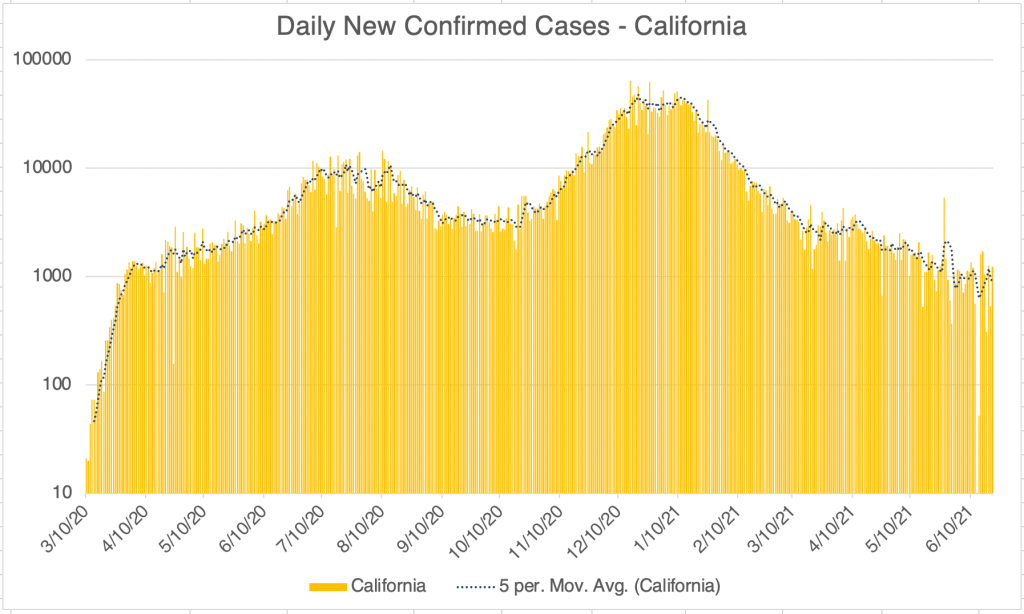
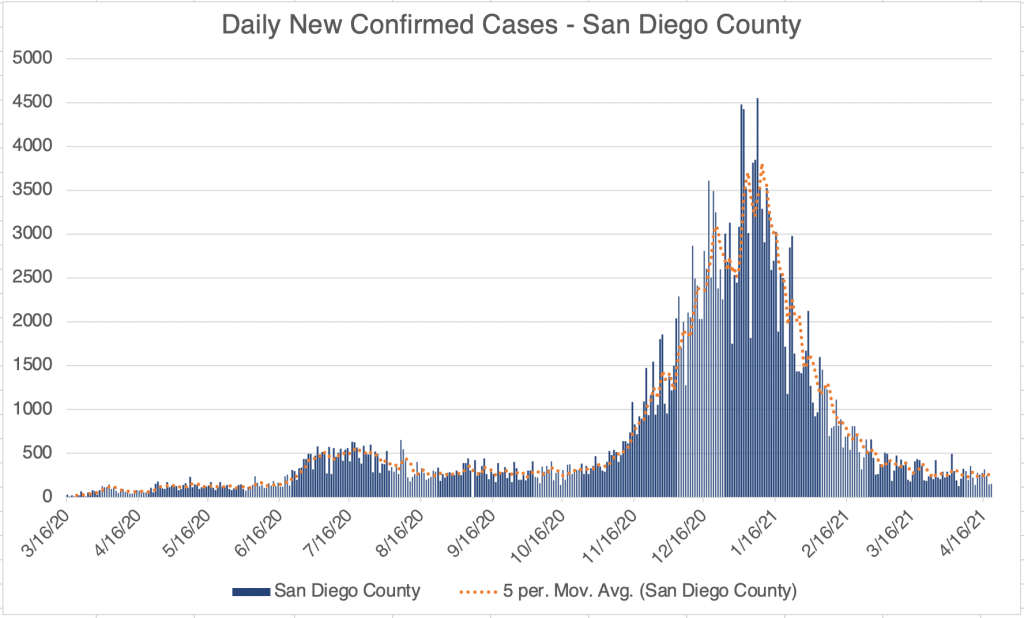
For California and San Diego County, new case numbers are definitely flattening, and we could very well start seeing a downward trend this week.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.
Correction on new deaths: Last week I said that new deaths were not rising at all as a response to the higher Delta peak case numbers. While this was true last week and is still true, I also have to say that I assumed that deaths generally followed cases by 2 weeks. After looking back at data from the US and other countries, deaths appear to trail new cases by anywhere from a few days to as many as 4 weeks. Since our current wave started at the beginning of July, it’s still too early to say if we will get a new peak in COVID deaths.
Several countries have indeed seen Delta peaks in cases without a peak in deaths so far. The UK and Portugal are both 6 weeks into their Delta variant peaks, without a substantial rise in deaths so far. My statements from last week may still end up being true. I will certainly keep you posted on this.
How many breakthrough cases? There has been a lot of discussion around breakthrough cases, a new COVID case in a person who has been fully vaccinated. According to the CDC, there have been 6,587 hospitalizations or deaths in 163 million vaccinated Americans as of July 26. This is a proportionally small number, but is obviously not zero.
I could only find data until April 30th for any SARS-2 infection, 10,262 infections for 101 million vaccinated Americans from January 1st, to April 30th. Note that this is before the Delta wave started in the US (early July). There were 12,376,975 confirmed infections in the US during that time, so the proportion of infections in vaccinated individuals is 0.083% according to CDC numbers.
While the proportion of infections and deaths in vaccinated is very low, I hear persistent unconfirmed stories about vaccinated people being infected. Hopefully, given the politicized environment, we will someday get good data on this.
This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Origin: Controversy over the origins of the SARS-2 virus began very early in the pandemic. The most common theories were that the virus arose naturally at a live animal market in Wuhan China, where animals from a wide variety of species are sold. The predominant theory is that the SARS-2 virus arose in bats, then transferred to another animal, perhaps a pangolin, before moving to humans. This has been the most accepted theory for the majority of the pandemic, promoted by the WHO, the CDC, and American media.
The lab leak theory, the idea that the virus arose from the Wuhan Institute of Virology, was present from the beginning, but was heavily disfavored by official channels for most of the pandemic. On May 23, 2021, the Wall Street Journal published an article that gave evidence for idea, followed closely by an article from Vanity Fair. The articles normalized discussion of the theory and as of this writing, polls show that a majority of Americans believe that the virus came from the WIV.
Emails between several virologists, public health officials and Dr. Fauci strongly suggest that this group believed that the virus may have come from the laboratory as early as January 31, 2020. However, this same group published a scientific article on February 9th supporting the natural origin theory. The paper was at odds with discussion in the email correspondence. If investigations show that the group published claims they knew to be false, this would represent a significant case of scientific fraud.
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, outdoor transmission of SARS-2 appears to be extremely rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable viral can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include:
age asthma or COPD heart conditions kidney conditions liver disease high blood pressure diabetes obesity auto-immune disease use of NSAID anti-inflammatory medications being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant) vitamin-D deficiency type A blood (Type O appears to be protective) inadequate sleep
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms. Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection or lowers the viral load of exposure. N95, KN95, and KF94 respirators are effective at filtering close to 95% of virus. A good mask is well fitting and filters the air moving in an out of your mouth and nose. The commonly used surgical masks and other loosely fitting masks do not filter air and I don’t recommend using them.
Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection. Social distancing may be more important for droplet transmission, like the flu, than for aerosol transmission in which microdroplets can stay suspended for much longer and travel much further.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US. Supplementing Vitamin C and Zinc is also recommended.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
I’ve been traveling all over the country, and have been in dozens of airports, gas stations, and stores. I get tested regularly and have always been negative. Here are the precautions I use:
1) Wear a mask or face covering indoors in public. Now that vaccines are available, I no longer avoid unmasked people indoors, but as an unvaccinated person, I still wear mine. 2) Keep 6 ft away from others. (I basically ignore this one if other precautions are in place, especially on an airplane!) 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. This is now voluntary now that we have vaccines, as an unvaccinated person, I still follow this rule. 4) Outdoor gatherings are fine, even without masks, if everyone maintains a distance. I have hosted several outdoor gatherings. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however. 6) Wear an N95 or KN95 mask when going to more high risk areas like airports or public areas where people may gather. These masks are rated to filter out 95% of viral particles. In my opinion, surgical masks and especially neck gators are nearly worthless in these settings. 7) I never take my mask off on the plane, and find an isolate spot in the airport to eat or drink on layovers.
Vaccinated people can relax many of these rules! Vaccines are 90-95% effective, so you still have a small chance of infection.
Testing: There are several kinds of tests, and they tell you different things.
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test. They can take longer to process because they need specialized equipment that most small labs don’t have, so most of the wait time is just for shipping to a specialized facility.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody. These tests are cheap and fast, but are more prone to false positives and false negatives than PCR tests.
Antigen: These tests use a very similar technology to Antibody tests, but instead of detecting a patients antibodies against virus, they use antibodies to detect viral proteins in a sample. An “antigen” in immunology lingo is just a protein that can induce an immune response. So in this context, an “antigen” is a SARS-2 protein that can be bound by an antibody. Like PCR tests, these tests detect an active infection, because they detect viral proteins currently in the body.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR but more prone to false negatives.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Antibody Dependent Enhancement:I’ve written about this a lot and I won’t describe it in depth here. In short, this pathway allows some viruses to create more severe disease on the 2nd time infecting a person than the first. It is theoretically possible, perhaps even likely with SARS viruses, which is why I have been careful to avoid infection and why I’m not going to get the vaccine unless perhaps my work requires it.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Supportive care: Most treatment is supportive care, treating symptoms while the patient recovers naturally. Anti-inflammatory medications are often used to prevent the immune system from over-reacting to the virus.
Ventilators/nasal cannula: While widely used early on, some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor oxygen therapy using a nasal cannula, using ventilators only as a last resort breathing if labored.
Remdesivir: This antiviral was used widely for much of the pandemic, but many sources now claim it has limited effectiveness.
Dexamethasone: Steroid used to treat patients with low oxygen levels.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. Treatment with Ivermectin is likely more beneficial in a wider range of disease state than HCQ.
Ivermectin: A anti-parasitic medication used since 1981, Ivermectin has reportedly been used by doctors around the world, notably India and Mexico, to reduce COVID fatalities. Reports claim that Ivermectin is beneficial in a wide range of disease state, from pre-disease prevention to late stage disease. Like Hydroxycholoroquine, promising data was often labeled “misinformation” by outlets in Western countries, and western doctors were strongly discouraged from prescribing it. Thus, experimentation with Ivermectin was hindered and the drug’s potential is still unknown.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Several vaccines against SARS-2 were finally released to the public in December of 2020. The vaccines released to the public are in 2 types:
Attenuated vaccine: This type has been commonly used for decades for a variety of viruses. The technique makes a severely weakened form of the virus that still makes viral proteins that provoke an immune response. With this type of vaccine, the patient is infected by a weak form of the virus that they quickly recover from, usually with no symptoms other than occasionally the flu like symptoms that are your body’s natural response to invasion.
mRNA vaccine: This is a brand new technology that has been worked on for years. The SARS-2 vaccines are the first ones that have been introduced to the public using this technology. The vaccine includes a piece of mRNA inside a lipid bilayer that mimics the cell wall. The mRNA is inserted into the cell where it is translated into a copy of the viral Spike protein. These vaccines are 90-95% effective against infection, and even those infected have less severe symptoms. However, they are not 100% effective, so some infections of vaccinated individuals has occurred.
As has often happened, the vaccines have generated significant controversy. As you know, I have been careful to avoid being infected and also getting the vaccine because of the potential of ADE. My concern with the vaccine actually has nothing to do with the new mRNA technology, I actually have no reservations about the mRNA vaccines. From an ADE perspective both the attenuated vaccines (Johnson & Johnson) and the mRNA vaccines (Pfizer and Moderna) produce Spike protein that may trigger an ADE response should a new strain of SARS virus appear, not a variant, a new SARS strain, like a “SARS-3”.
When the vaccines were released, rumors of side effects, sometimes severe, arose immediately. For some time, I minimized these as a risk of any vaccine. All vaccines carry the risk of side effects and even death. However, a video podcast featuring Robert Malone, the inventor of mRNA vaccine technology, convinced me that the Spike protein itself has toxic properties of its own, separate from the vaccine technology used. This is because the Spike protein can bind to cells all over the body and may have wide ranging effects.
Despite ADE and issues with side effects, I actually still believe some will benefit from the vaccine. These include the following groups:
Anyone over 60 Anyone with 1 or more risk factors:
obesity certain auto-immune diseases use of NSAID medications heart, lung or kidney condition immunocompromised patients (HIV, cancer and transplant patients) respiratory condition such as asthma or COPD.
Frequently working with the public Musicians who sing in indoor settings Medical personnel
Again, I am not a physician, so check with your healthcare provider while making decisions about getting the vaccine or changing your medication.
If you’ve had the vaccine or had COVID and are concerned about ADE, remember that it will only become a factor if a significantly new strain arises (“SARS-3”). If this happens, then the procedure for you would be to be very careful initially, then get the “SARS-3” vaccine as soon as possible. The new vaccine will protect you from the new virus. In the future, vaccines against Coronaviruses will be produced even more quickly than this time.
The vaccines have pros and cons. I’m in support of vaccines for some but not necessarily for others. Each person needs to weigh the risks for themselves. I am not for companies or government agencies coercing individuals to get the vaccine.
Herd Immunity: The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. The idea is useful, but in my opinion, efforts to push people into getting vaccinated to achieve herd immunity are misplaced. Before a vaccine is available, the only way to reach herd immunity is to expose large numbers of people to the virus, which is counter productive. Now that the vaccine is available, those who are concerned should just get the vaccine themselves and not harangue others about getting it. Gentle persuasion may be convincing, but haranguing rarely is. Given even the pre-pandemic resistance to vaccines, a forceful effort to vaccinate is likely to back-fire.
Variants: During the course of the pandemic, several variants have arisen that have a slightly different Spike protein sequence from the original Wuhan strain. Confusingly, naming conventions have changed several times, making it difficult to keep them all straight. As a general rule, the variants have all been more infectious than the Wuhan strain, but have not been more pathogenic. Fortunately, the vaccines have been effective against all of the variants, although are not as effective against some variants.
The Delta Variant: The UK/Alpha variant caused waves of new infections in some countries and was more infectious than the original Wuhan strain. In late 2020, a new variant arose in India, the India/Delta variant. This variant was significantly more infectious than other strains and has caused huge peaks in cases in several countries. As of this writing, several countries are still experiencing waves of new cases most likely due to the Delta Variant, including the United States.
While the Delta Variant has caused large numbers of new cases and an increase in hospitalizations, data suggests it may be less pathogenic than the Wuhan or UK variants.
Current Status: In late Spring, at least in the US, life began to get back to normal, with approximately 50% of the US population vaccinated, much lower new case numbers, and reduced restrictions. Currently however (July 21, 2021) a wave of infections, likely caused by the Delta variant, is causing concern and some calls for new restrictions. Several other countries scattered across the globe are also currently experiencing peaks in cases.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format and includes only the Fall/Winter 2020, Spring ’21, and Delta Variant peaks.Endcoronavirus County Level Map, July 20th, 2021Daily new confirmed cases in India, from data collected from Johns Hopkins University COVID site. The Delta Variant peak is the large one on the right. Notice the sharp upward and downward trends. The new persistent daily case numbers are higher than before the Delta peak began.
The Future: Since vaccination started in the US, there have been many fewer new cases. This has led many to basically go back to behaving normally. The Delta Variant is rightly causing concern, but I’m still hopeful that the current peak in new cases will be short lived. In other countries with Delta related waves, the peak has been very sharp, with quickly increasing, then quickly decreasing case numbers. However, I’ve started to be a little more cautious in public again, while we wait for the increase in cases to slow.
Several other countries are still experiencing an elevated case load. The pandemic won’t be truly over until cases are low in all countries. I’m hopeful that this will happen this year, but it’s certainly too early to know for sure. So far, all new variants have been susceptible to the vaccines and natural immunity. There is a small chance however, that we may see new versions that are not. If this happens, SARS may become endemic, circulating seasonally like the flu does. So far, I don’t see evidence that this will happen.
In the future, we may have a “SARS-3” a new virus from the SARS family that will be similar, but different enough to trigger the ADE pathway. If this happens, those of you that have had COVID or been vaccinated should be very careful to avoid infection initially, then get the “SARS-3” vaccine as soon as it is available.
In a future post, I’ll give my recommendations for what should be done differently if a new pandemic should arise.
This is a COVID update. I also have a short note on the Delta Variant and sobering new information on vaccines.
New case numbers continue to trickle down in the US, California, and San Diego County. New cases in San Diego County have been less than 100 a day for most of last week. Unfortunately, new cases aren’t really plummeting, just trickling down, but we are still making progress.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site.Endcoronavirus County Level Map, June 18, 2021Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it. The County is often making adjustments to various numbers and sometimes they do not update numbers for several days. As a result, this graph is becoming less reliable. This is likely impacted by the low number of cases, so that anomalies have a greater impact on overall trends. I may not post this graph for much longer.Graph is by me, from data collected from Johns Hopkins University COVID site.
I did some traveling this week, and in several places, including airports, about half of the people there did not have masks on. I was OK with this, since I know most people are now vaccinated, but this is reflective of our ongoing transition back into normality.
The Delta Variant: Way back in October of 2020, a new variant arose in India. First called the India Variant, the naming of variants has changed again in the last few weeks, and it’s now being called the Delta Variant (B.1.617.2). As with other variants, it’s much more infectious than the original Wuhan strain, but it doesn’t appear to cause more severe disease. The current vaccines appear to be effective against the Delta variant, so if you’re vaccinated, you are likely protected against this variant.
___________________________________ Updated from June 29th, 2021 post: As I’ve stated before, the Delta Variant is significantly more infectious than the original Wuhan strain, as well as more infectious than the UK Variant. I said last week that it is not more pathogenic. I have to adjust that assessment. While it hasn’t so far produced more deaths than other versions, it does seem to produce more hospitalizations, so it does appear to be more pathogenic at least by that measure.
I’m going to way out on a limb and suggest that the Delta Variant will not cause large numbers of new cases in the US because of our natural immunity and our large number of vaccinations. That being said, there have been reports of fully vaccinated individuals contracting the Delta Variant. None of their symptoms were severe. I may of course end up being wrong about this and I will keep you posted on new confirmed case numbers.
Some municipalities are considering new lockdown measures. I have not supported “lockdowns” since last Spring, but as an unvaccinated person, I still wear a mask in indoor spaces in public. ____________________________________
Vaccines and Spike protein toxicity: Now for a topic that is even more likely to get me cancelled than last time. I ran into a video with Bret Weinstein, Dr. Robert Malone, and Steve Kirsch. Robert Malone is the scientist that was instrumental in the development of the mRNA vaccines, like the Pfizer and Moderna vaccines. He speaks very authoritatively on the vaccine issue.
Dr. Malone is very pro-vaccine in general, and certainly believes that the mRNA vaccine is effective in principle. However, he also has come to believe that while mRNA vaccines in general are safe, the SARS-2 vaccine in particular does have a big liability. This is that the Spike protein made by the SARS-2 vaccine has a toxic effect on multiple cell types. This explains the higher than normal rate of complications related to the SARS-2 vaccines.
Part of the reason SARS-2 is such a difficult virus is that the Spike protein attaches to a cellular receptor called ACE2. The ACE2 receptor is present on many cells types in the body. This is why the SARS-2 virus can infect so many different cell types, including immune cells.
In response to the vaccine, cells make Spike protein so that the immune system can develop a response to the virus. This is true of all vaccines. However, since the Spike protein can attach to so many different cell types, there is a wide range of symptoms a person may experience in response to the vaccine. Of course, most experience no symptoms at all.
So what if you got the vaccine? Should you be concerned? It’s too early to tell how prolonged an impact Spike protein in the vaccine will have on an individual person. My guess is the impact will subside after a few days, when the Spike protein in cells is degraded. However, since the Spike protein interacts will cells and impacts their functioning, some reactions may take longer to resolve. If you had no reaction to the vaccine, you probably won’t ever have one.
If you haven’t had the vaccine, should you still get it? There is no denying that the vaccine has had a positive impact on the re-opening process and has likely saved many lives. On the other hand, it obviously carries risk. If you are in a high risk group or work with the public, you are still very likely to benefit. As you know, I haven’t gotten the vaccine because of the ADE issue and also because I’m reasonably certain I can avoid getting the virus, especially now since cases are so low. I will be less likely to get the vaccine now.
I believe that the censorship of ideas present in our current culture has had a profound and negative impact on the progress of the pandemic, and on our culture in general. As I’ve said repeatedly, politics and science are a terrible mix. We’ve seen many examples this year. I deeply hope we can find our way out of this mess as soon as possible.
Since things are starting to wind down in the US, my COVID posts will probably be less frequent, but comprehensive. This is a case update, and I’ll also discuss the new CDC guidance and talk about vaccine safety.
New case numbers continue to fall in the US, California, and San Diego County. Numbers now appear to be as low as they were last March when everything blew up here. In fact, since we have so much more testing now, it’s likely that our actual new case numbers are likely much lower than they were last March.
New CDC Guidance: The CDC has been slow from the beginning to update their guidance, often seeming out of step with events. This is not new! They have been like this since at least 2004 when I started working at Quest. They’ve just recommended that fully vaccinated people can go indoors without masks. This is overdue, but many are concerned that they can’t identify who has had the vaccine and who has not. A big change that has happened in the last few weeks is that anyone over 16 who wants a vaccine can now get it. This means that instead of being concerned about behavior of others, you can simply get vaccinated and be reasonably certain that either you won’t get the virus, or if you do, you will have mild symptoms. Yes, it’s true that a few vaccinated people have gotten infected, but this is rare. So I’m now in favor of making masks indoors voluntary.
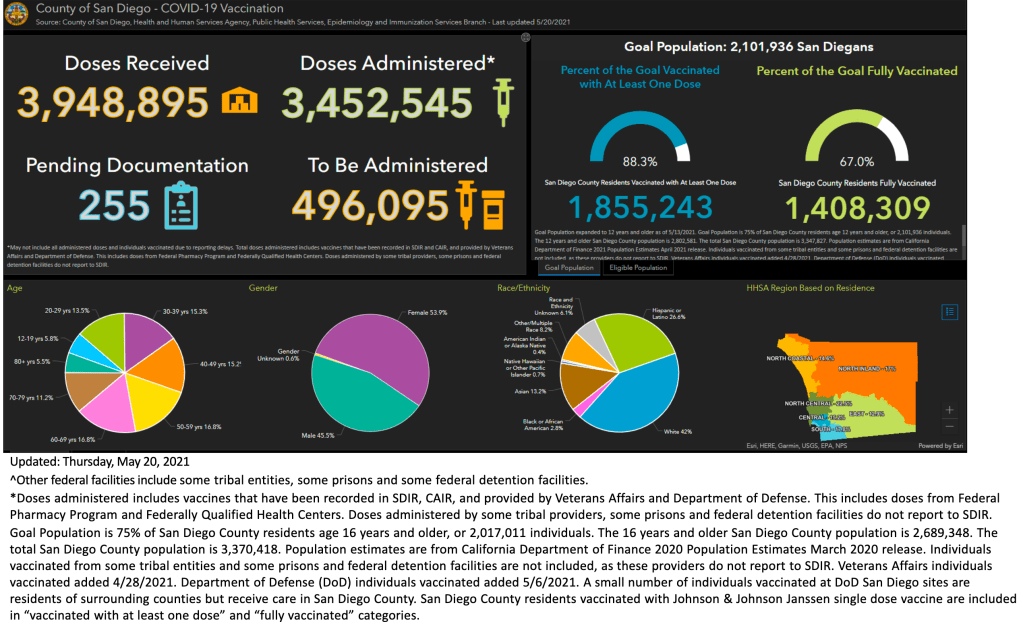
In San Diego County, 42% of the population has been fully vaccinated, and 55% have had at least 1 dose.
As you know, I’ve decided not to get the vaccine because of the ADE issue and because I’m reasonably confident that I can stay uninfected. So I’m committing to continue to wear a mask indoors until cases numbers are very low. And no, I’m not ready to define what “very low” means. But if you’re vaccinated, you should probably start considering yourself safe from the virus.
Should you get vaccinated? I still get a lot of questions about whether someone should get vaccinated. Again, I’m not a physician, so I’m not giving medical advice, I’m just giving you some information that you might find helpful.
First, let me say that my own misgivings about the vaccines have nothing to do with the new technology. Aside from persistent rumors, I haven’t yet seen any real evidence that vaccines have the following effects:
birth defects shedding viral particles (mRNA or Spike protein) into the environment re-coding of DNA
It is also theoretically very very unlikely that these things would happen. Biologically, mRNA is made in the nucleus, then goes out into the cell and is read by proteins that use it to make other proteins. It is designed to be very fragile, and quickly degrades, so that for a protein to be made constantly, mRNA encoding that protein must also be made constantly. The mRNA in the new vaccines goes into the cell, gets used to make some Spike protein, and then degrades. It does not persist in the body, and Spike protein production stops when it is gone.
Remember that it’s not your job to refute a claim. It’s the job of the person who makes the claim to provide evidence that it’s true. If they can’t provide evidence, you don’t need to do a bunch of homework.
I am not anti-vaccine! My concern with this vaccine is solely regarding the ADE issue, a phenomena peculiar to just a few viruses, including Dengue, HIV, Zika, SARS, MERS, and maybe SARS-2. If you’re concerned about the new technology, but want to get a vaccine, the J&J vaccine is your best bet.
Also, despite my misgivings, I still recommend the following people get vaccinated:
Anyone over 60 Anyone with 1 or more risk factors: obesity certain auto-immune diseases heart, lung or kidney condition respiratory condition such as asthma or COPD. Frequently working with the public Musicians who sing in indoor settings Medical personnel
People in these categories are very likely to benefit from the vaccine, despite the ADE issue.
If you’ve had the vaccine or had COVID and are concerned about ADE, remember that it will only become a factor if a significantly new strain arises (“SARS-3”). If this happens, then the procedure for you would be to be very careful initially, then get the “SARS-3” vaccine as soon as possible. The new vaccine will protect you from the new virus. In the future, vaccines against Coronaviruses will be produced even more quickly than this time.
Are vaccines safe? Last week, someone posted a few links regarding concerns about vaccine safety. One source I hope to look at soon is the Vaccine Adverse Event Reporting System run by the CDC. It lists any adverse reactions happening soon after a vaccination. Medical events listed include any event happening soon after a vaccination, and some are not vaccine related. Sorry, but I simply haven’t had time to study this site yet!
I will say this, however. All vaccines carry a risk. In almost all cases however, the risk is far, far lower than the risk presented by the disease they are designed to counter. While there have been many adverse reactions to the SARS-2 vaccine, most are very mild. Even deaths have occurred, but again they are very very rare. This is true with every vaccine!
We are almost out of the woods! Continued blessings on you and your family!
This is a late COVID update! I’ll also offer a correction on my April 20th post regarding vaccination numbers in San Diego County.
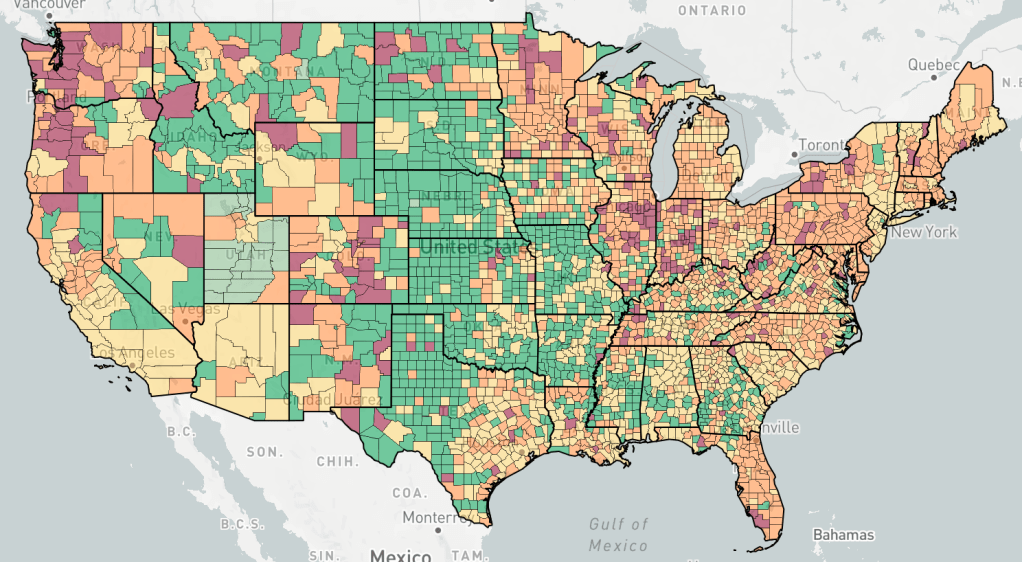
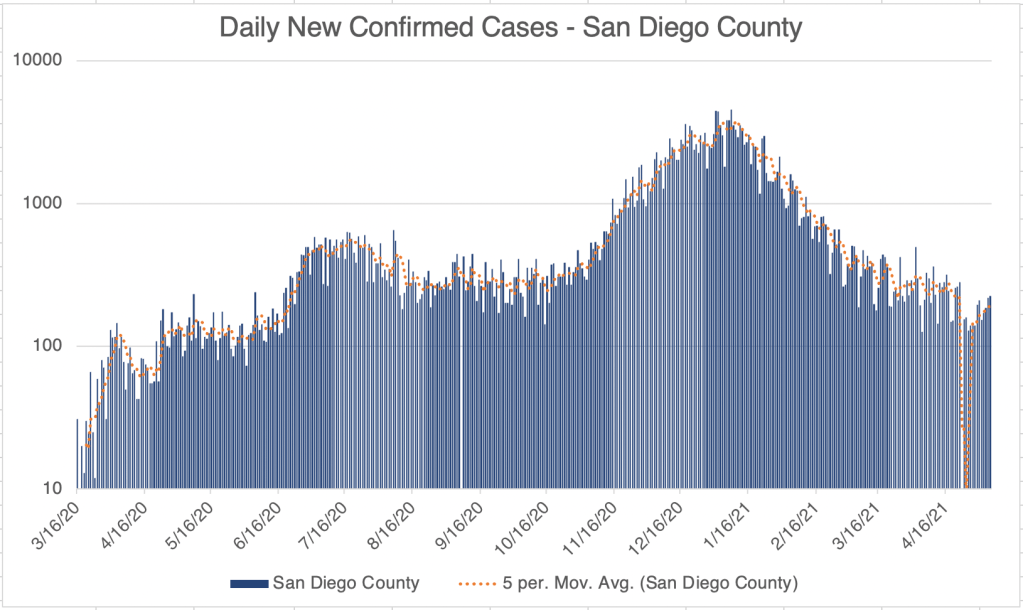
New case numbers continue to trend downward in the US, California and San Diego County. A few hot-spots persist in the Northwest, Colorado, and parts of the Rust Belt, but the situation in Michigan is improving.
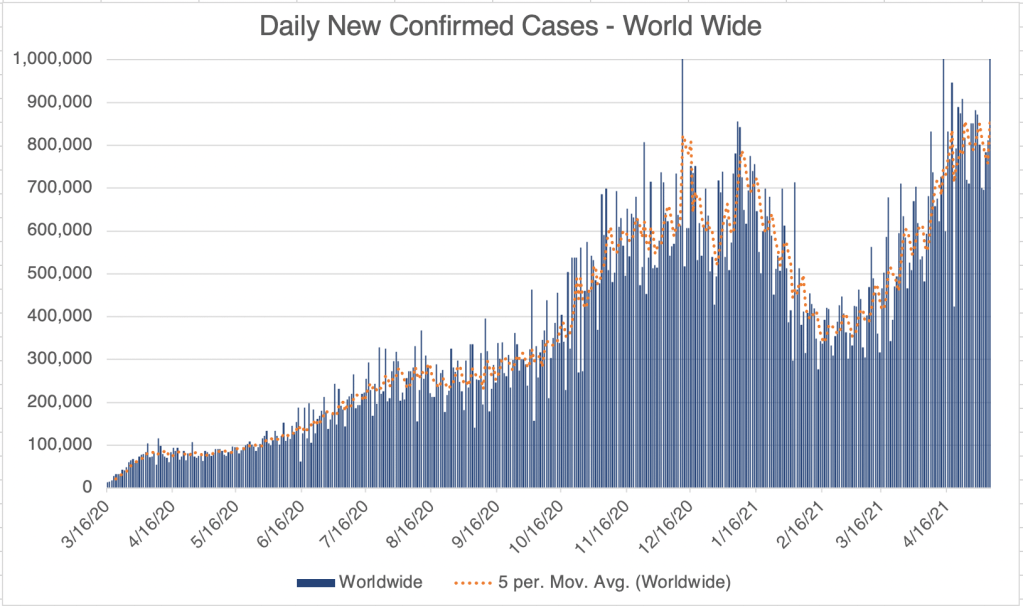
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Endcoronavirus County Level Map, May 7th, 2021Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site.
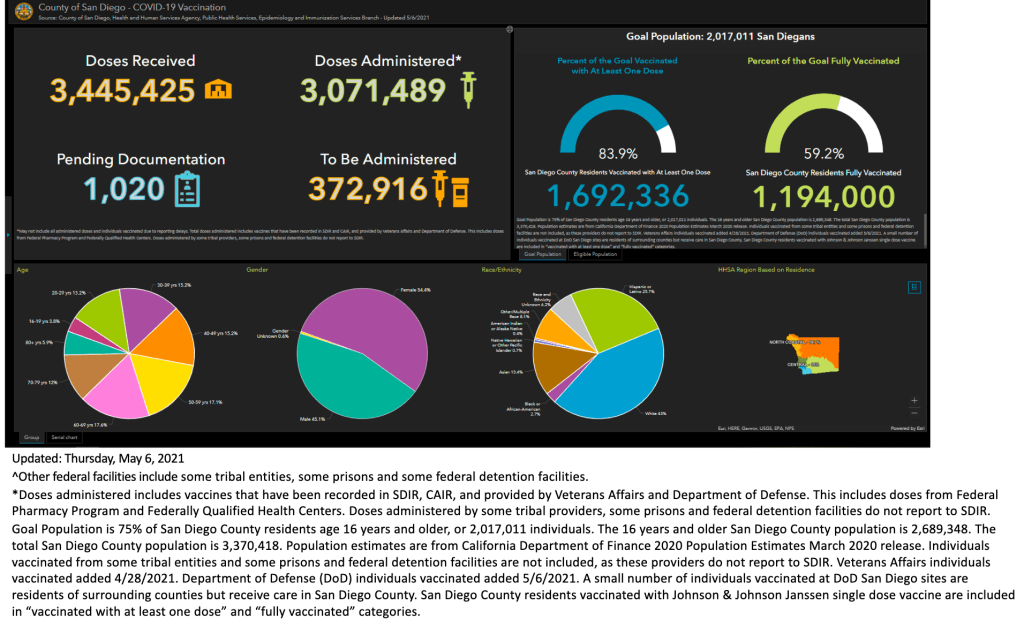
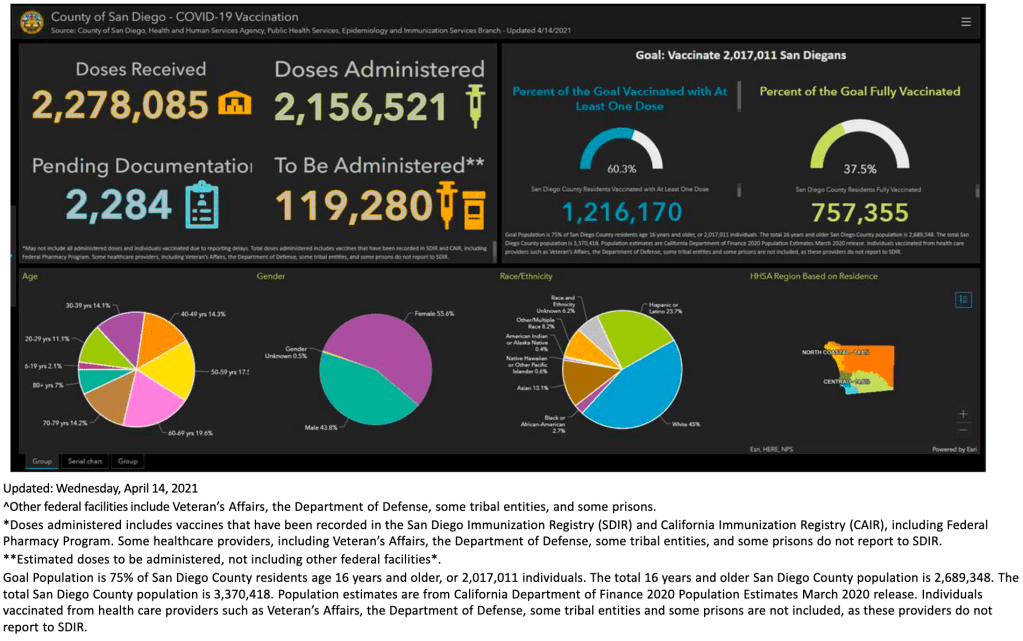
I was overly optimistic in my April 20th report of vaccination in San Diego County, because I didn’t read the fine print! On their press briefing slide deck, they report the percentage of people with either 1 or both doses of vaccine. As it turns out, however, this is not of the total County population, but only of their target of 75% of residents over 16! Yesterday, they reported that 83.9% of the target population has received 1 dose, and 59.2% has been fully vaccinated. This actually corresponds to roughly 50% and 35% respectively of the estimated 3.3 million SD County residents.
This is a case update. I’ll also discuss vaccination in San Diego County and herd immunity in general.
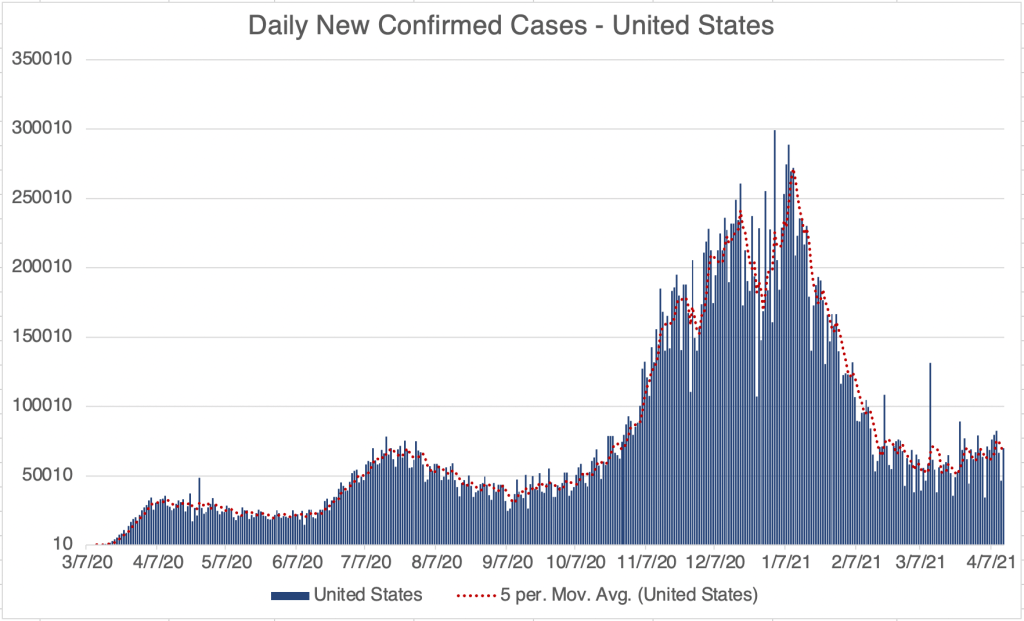
New cases may have plateaued in the US, but new outbreaks are apparent in some states. Michigan was the standout state for new cases, but endcoronavirus now suggests outbreaks across the Rust Belt, Northeast, Northwest, Colorado, and Florida. In most counties, actual numbers are small, but are obviously much larger in urban areas. If we are in a 4th wave, it appears to be much smaller than Wave 3, probably impacted by increased vaccination.
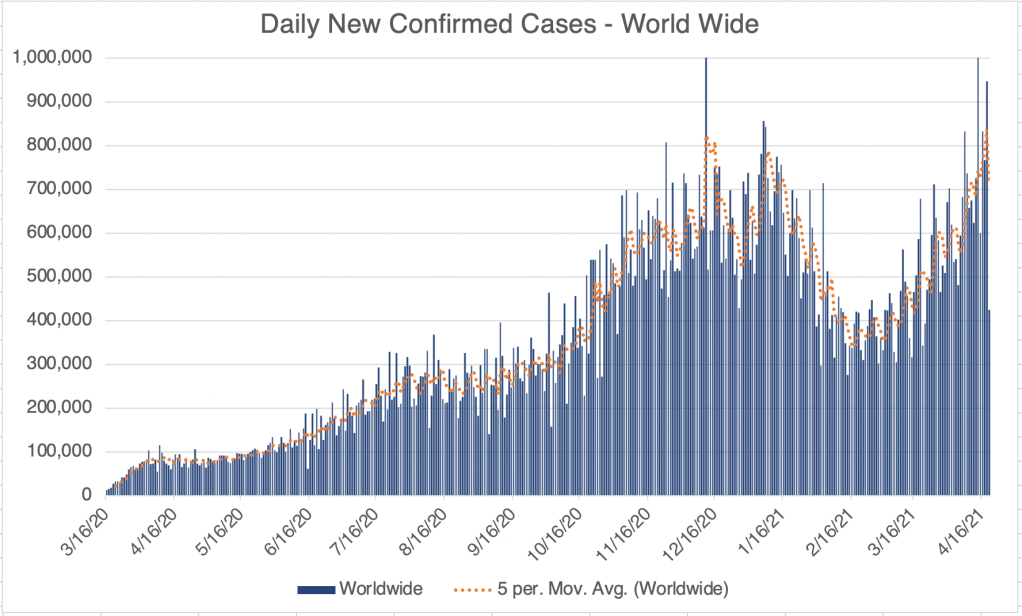
Internationally, new cases are very high worldwide. The new high cases numbers are likely impacted by the new variants such as B.1.1.7 (the UK variant) which is more infectious than the original Wuhan strain, and now dominates in many countries. Brazil and India are particularly hard hit. Canada’s current wave is as high as their Winter wave, but the numbers there are in general much lower than for the US.
Vaccination in San Diego County: According to the County, about 37% of County residents are now fully vaccinated, with 60% having had at least 1 dose. Vaccination is now available to anyone 16 and up who wants to be vaccinated. If you want to be vaccinated, you can find a location on their website.
Herd Immunity: First, just a reminder that I am not an epidemiologist. Early in the pandemic, many recommended herd immunity as a way out of the pandemic. At the time, I argued that exposing a lot of people to a disease to protect people from a disease was counter productive. Now that we have a vaccine, herd immunity is a viable option for moving forward. For a population, herd immunity can be effective, although the percentage of people who need to have immunity to reach this is dependent on the disease and usually surprisingly high. On an individual basis, if you’re concerned about catching the virus, it’s far better to just get vaccinated at this point than to worry about if we’ve reached herd immunity.
This is a case update. I’ll also talk briefly about ADE and it’s impact on the current pandemic and the potential impact on the next SARS virus, if one ever happens.
Cases in the US continue to rise slightly. Outbreaks continue in Michigan, with some new cases also in the Greater New York Metro area and the Texas panhandle. Why is Michigan having such a hard time? Frankly, I’m a little mystified, especially since Michigan has been in strict lock-down through much of the pandemic. It’s now well known that the viral load upon infection has a large impact on the severity of COVID symptoms. Those who get a low viral load upon exposure have lower symptoms. I will speculate and say that perhaps some states with very strict lock-downs caused people to interact in ways that encouraged larger viral loads upon infection, like being with groups of people in private homes. Again, I’m just speculating. This may also explain the large and sustained number of cases in LA county this Fall and Winter.
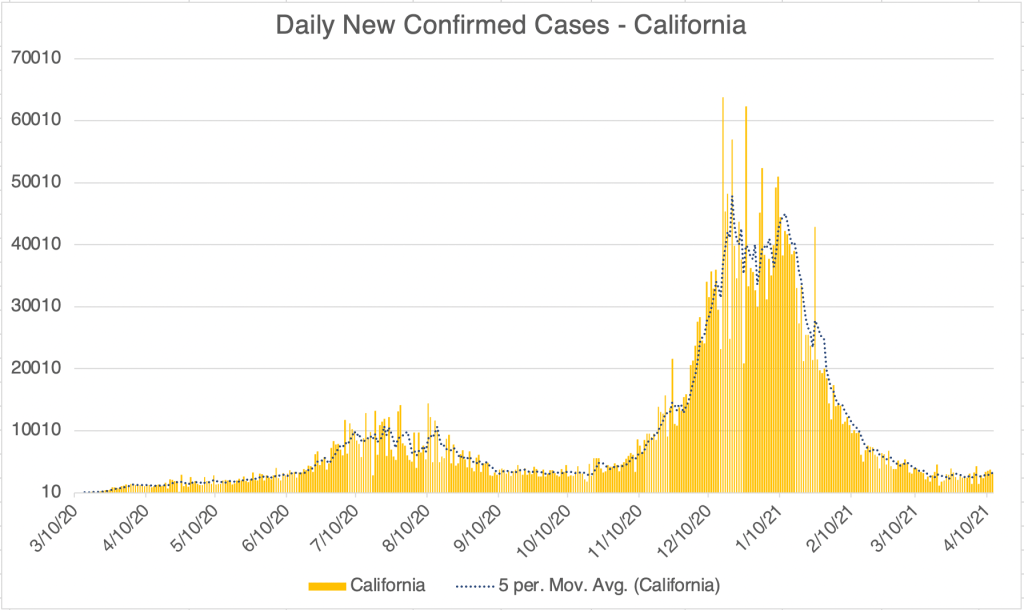
California and San Diego County both have come to an equilibrium, with approximately 3000 and 200 new cases a day respectively. Neither appears to have experienced an Easter related bump in cases. The new lower caseload in the US is likely related to vaccination and natural immunity, and is likely to become lower still as we head into Spring and Summer.
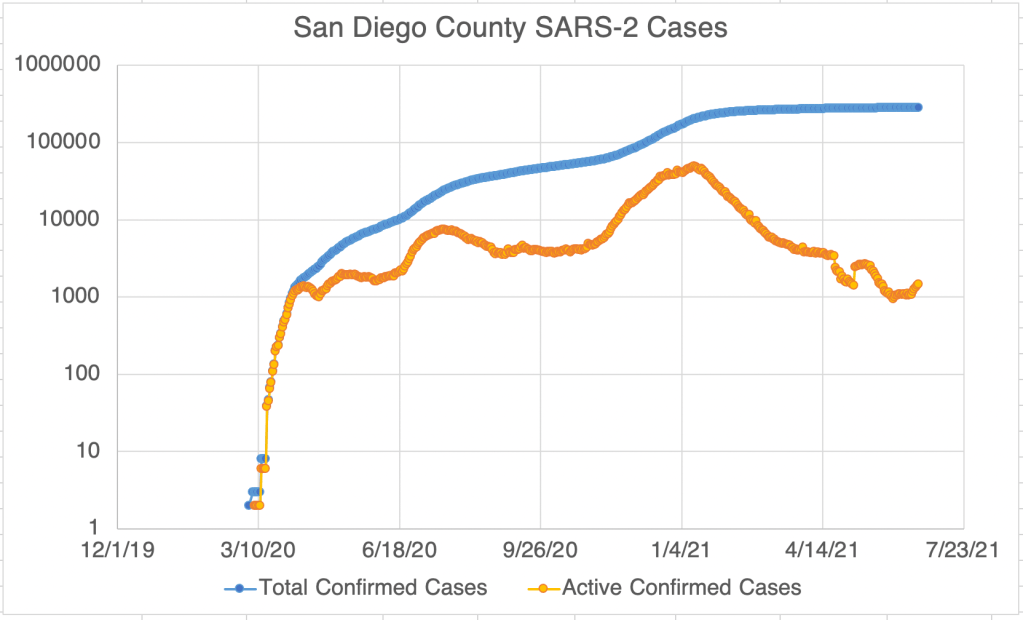
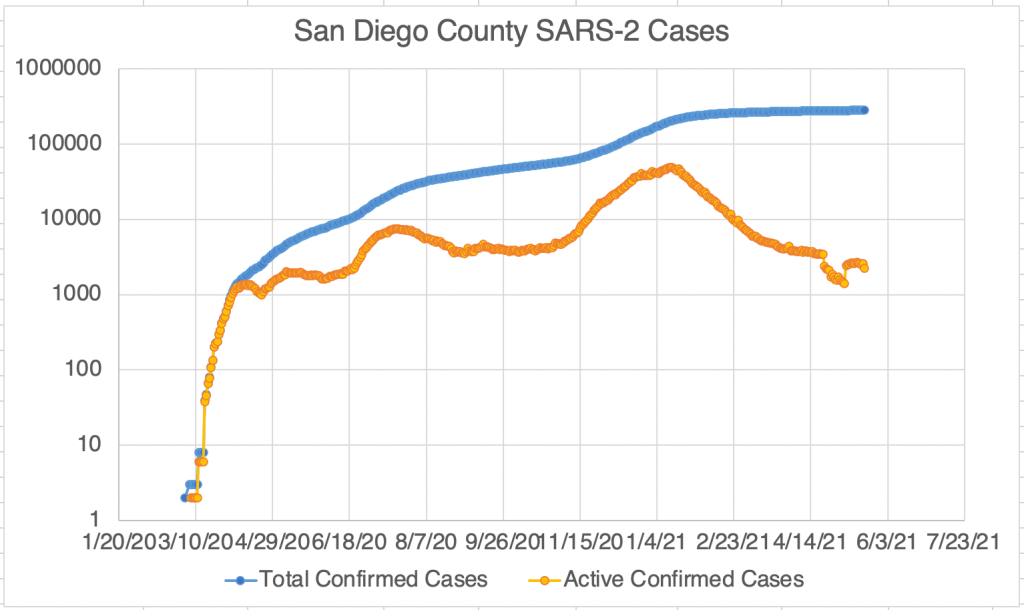
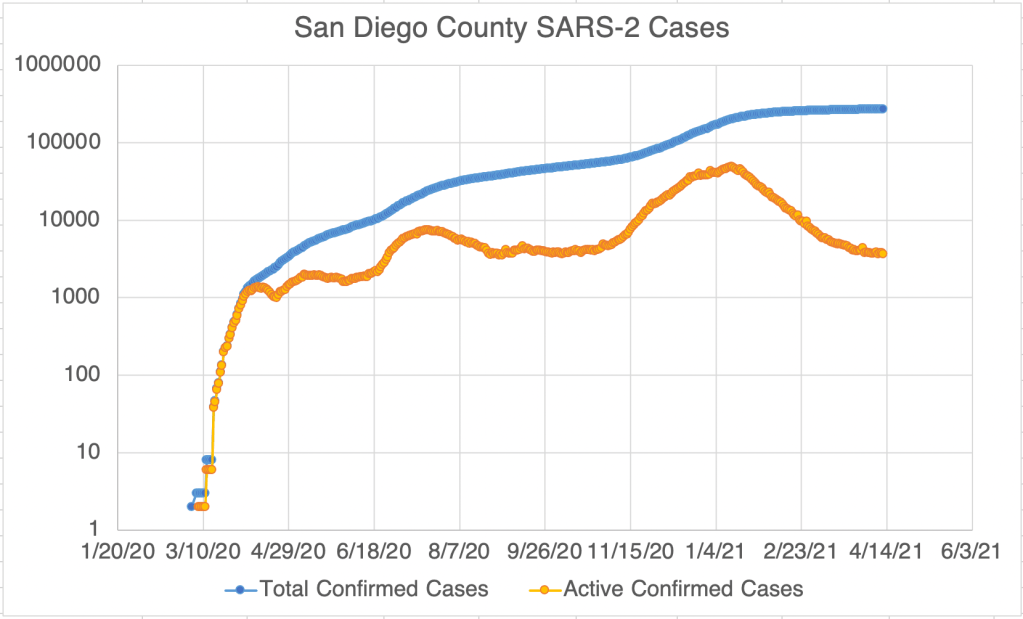
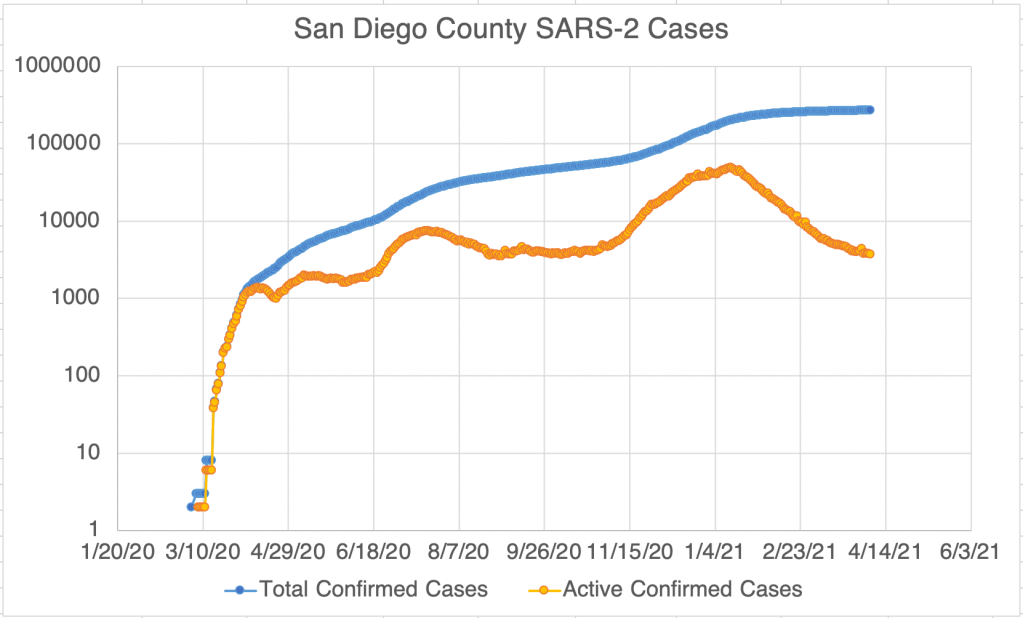
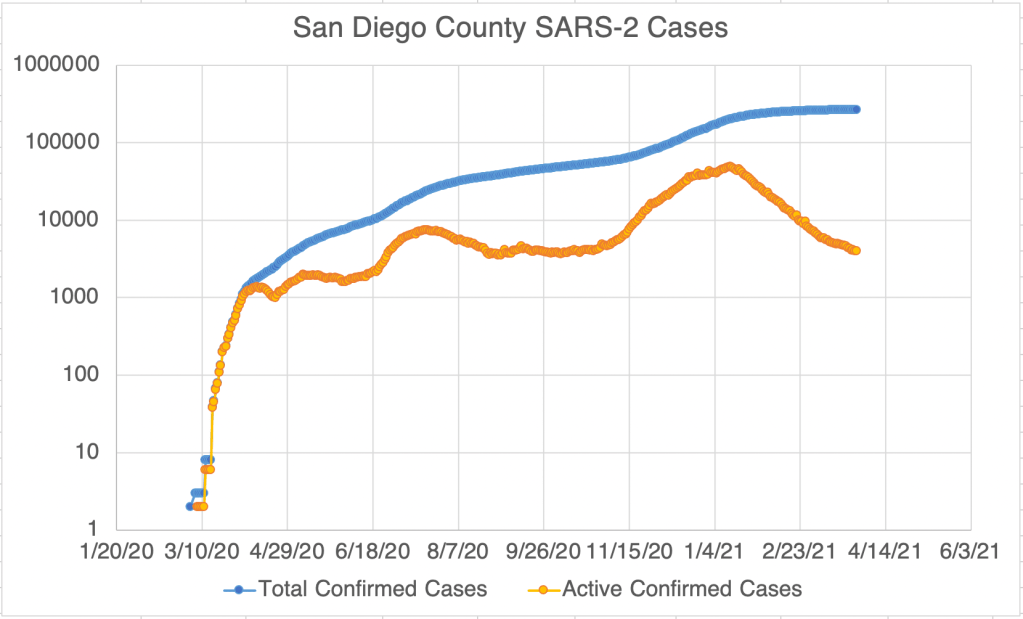
Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. “Active Confirmed Cases” numbers are reported by San Diego County. Because our new active case numbers are getting low, I’ve switched to a logarithmic view. This emphasizes small values and makes them easier to see. Notice that the case number on the left now go up 10 fold with each higher line on the graph.
Internationally, the caseload continues to increase, almost to Winter peak numbers.
ADE and the next SARS virus: I wanted to explain a little more about my continued concerns about ADE. As the pandemic progresses and we have numerous variants circulating around the world and the US, ADE does not appear to have had an impact on the current situation. This is certainly good news. If it did have an impact, we would be seeing additional deaths from the new variants, which we do not.
My continued concern comes because ADE impacts our ability to fight the NEXT virus. SARS viruses (SARS, MERS, SARS-2) have the ability to easily infect the immune systems of those previously infected with closely related but different strain of the virus. If a future strain of SARS comes out, let’s call it SARS-3 for now, ADE may become a big deal. I stress that this is only theoretical at this point. SARS was moderately infectious, but also very pathogenic, giving all known patients severe symptoms and killing 10%. It was actually less dangerous globally, since outbreaks tended to be detected early and quickly snuffed out. SARS-2 is highly infectious, but much less pathogenic. It’s greater global impact came from it’s very high infectiousness and very long incubation time, being passed even from pre-symptomatic patients. The tendency of all viruses is to become more infectious and less pathogenic over time, a pattern followed by SARS and SARS-2. If we have a SARS-3 someday, it will likely be even more infectious than SARS-2, but less pathogenic. On the other hand, MERS is more pathogenic than SARS, so this pattern doesn’t always follow. The next time another SARS coronavirus breaks out, we will need to be very careful initially until we understand the parameters of the new virus.
So what do you do if you had COVID or had a COVID vaccine if a SARS-3 comes out? If that happens, vaccine production will likely be much faster than this time. Be very careful with the virus initially, and get the new vaccine as soon as it is available to you, because you may be at greater risk for severe symptoms. I know some of this is confusing and counter-intuitive! Feel free to ask questions below!
This is a case update. I’ll also add something to last week’s discussion of the South Africa variant and vaccines, and also talk briefly about autoimmune disease.
Last week, cases in the US looked like they were rising, but this week, it’s more ambiguous. New cases in the US are the same or maybe even a little lower than last week, so I can’t point to a clear trend right now. A spike in new cases persists in the Eastern Michigan at the moment, as well as higher new cases in several other Eastern states.
New confirmed cases are also slightly up from last week in California and San Diego County. If we have a bump in cases because of Easter, it will start to show up on Wednesday or Thursday.
Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. “Active Confirmed Cases” numbers are reported by San Diego County. Because our new active case numbers are getting low, I’ve switched to a logarithmic view. This emphasizes small values and makes them easier to see. Notice that the case number on the left now go up 10 fold with each higher line on the graph.
Update, Vaccines and the SA Variant: Last week I discussed the effectiveness of several vaccines on the South Africa variant (B.1.351). I said that the Astra-Zeneca vaccine works poorly against the vaccine and that the Pfizer and Moderna vaccine were still poorly understood. New data from a small study Pfizer released in early April suggests that their vaccine is effective against the SA variant, though the study is too small to say how much. The Moderna vaccine is not particularly effective against the SA variant, but they are testing a booster against the SA variant right now. The Johnson and Johnson vaccine is 75% effective in the US, and 57% effective in South African patients (as reported by J&J).
Auto-Immune Disease and COVID: It appears that those with auto-immune diseases, like me (celiac disease), may suffer more severe symptoms from COVID. There is some suggestion that this may be because of consistent use of NSAID medications to counteract inflammation. Most doctors will suggest remaining on anti-inflammatories unless COVID symptoms appear. Check with your doctor before changing any medications. I am continuing to take my NSAID medications. By the way, Ibuprofen (Advil) is an NSAID, so if you’re taking an NSAID regularly, take Tylenol instead of Advil for routine pain so as to not double up on NSAIDs.
Unfortunately, there aren’t really studies yet to determine if auto-immune sufferers are at greater risk from getting the vaccine. In my non-expert but informed opinion, the risk of SARS-2 infection for auto-immune sufferers is likely higher than the risk of a reaction from the vaccine. Since the COVID vaccines only present the Spike protein to the immune system, they’re likely no more risky than any other vaccination. If you tolerate other vaccinations well, you’ll likely tolerate this one too. My recommendation would be for auto-immune sufferers to get the vaccine. Of course, check with your doctor first. If you choose to get the vaccine, I strongly suggest getting it at a medical facility that can monitor you rather than in a mass vaccination center.
Don’t fear, but be smart, Erik
PS. FB doesn’t like it when I discuss vaccines! They often add a note about vaccines when I discuss it, referencing info from the WHO. While comments FB has added recently are accurate, I generally don’t regard the WHO as a good source of information about COVID, since they are overly influenced by certain political entities and have occasionally been very wrong. The CDC is better, but it often very slow to present new information.
This is a COVID new case update. I’ll also discuss new cases world wide, and discuss a new video from immunologist Shane Crotty with lots of important information on vaccines and variants.
In the US, we’re starting to see an increase in new case numbers in several states, Michigan and New York in particular. This may be because of the relaxing of requirements by many municipalities, but may also be because of some of the new variants arriving in the US. More on the new variants below.
New case numbers have stabilized in California and San Diego County with around 2000 new cases a day in California and 300 in San Diego. We have yet to see a clear uptick in cases in those 2 regions, but we may see this soon.
Graph is by me, from data collected from Johns Hopkins University COVID site.Graph is by me, from data collected from Johns Hopkins University COVID site. “Active Confirmed Cases” numbers have been calculated based on the assumption that patients confirmed to have SARS-2 virus at least 17 days ago have recovered. Recently, however, this would produce an active case number that is too low to make sense in comparison to San Diego. This graph estimates 17 to days to recover in January, but gradually moves to 22 days for mid-March. I’ve lost confidence that I can make an Active Case plot that is accurate, so this will probably be the last time I post this for California. Let me know if you think it’s still useful.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. “Active Confirmed Cases” numbers are reported by San Diego County. Because our new active case numbers are getting low, I’ve switched to a logarithmic view. This emphasizes small values and makes them easier to see. Notice that the case number on the left now go up 10 fold with each higher line on the graph.
Internationally, the US and UK are doing better than average at the moment, but many countries scattered all over the world, with concentrations in Eastern Europe and South America, are seeing new surges in cases. The US and UK are both vaccinating heavily right now, with vaccine rollouts moving slowly in continental Europe, so vaccination may play heavily in this pattern. Also several new variants of the SARS-2 virus are more infectious than the original strain and likely factor in these new surges.
Important new video with Dr. Shane Crotty: MedCram has posted a new video interview with Dr. Shane Crotty, an immunologist in San Diego. His work looks into immune system responses to vaccination as well as native infection. He has several very interesting points to make about SARS-2 immunity and vaccines. First, he says that those infected with SARS-2 do have significant lasting immunity for many months, although it does go down a bit over time. Different people can respond very differently, however, and reinfection is possible in some.
Regarding vaccines, he said that those who have been infected have a good but not great immune response, but it is significantly boosted by a single vaccine dose, gaining an immune response higher than those vaccinated alone. So there is a good reason to be vaccinated if you have already been infected. Of course, if you’ve been infected, you may choose to wait until at-risk people have been vaccinated before you get a vaccine booster.
As for variants, he says there are 2 broad categories of variants, those similar to the UK variant (now commonly called B.1.1.7), and those similar to the South Africa variant (B.1.351). Both new strains are more infectious than the original Wuhan strain. The big difference between them is that those who have had SAR-2 are immunized against the UK strain, but not the South Africa strain. Also, the Astra-Zeneca vaccine does not protect well against the South African strain, and the Pfizer and Moderna vaccines appear to be less effective as well. The good news is, the Johnson and Johnson and Novavax vaccines do appear to protect against the South Africa strain. This suggests that although the South Africa strain is different, it isn’t so radically different that we have nothing to fight it with.
_____________________________ Update, April 6th A new small study from Pfizer suggests that their vaccine does work on the South Africa variant. The patient number in this trial is small, so they still don’t know exactly how effective it is. _____________________________
Soberingly, the South Africa strain has reached the US, so if we see a surge in the next few weeks, this strain may be at least partially responsible.
Impact on ADE? If you’ve read my posts on ADE, then you know that the danger from ADE may come when a different strain arises. With the South Africa strain arriving in the US, we may be able to see if ADE will have an impact with SARS-2 in the next few weeks and months. So far, new death numbers have come down with Wave 3, and there is no apparent impact from ADE on case severity. I will certainly be watching to see if this changes.