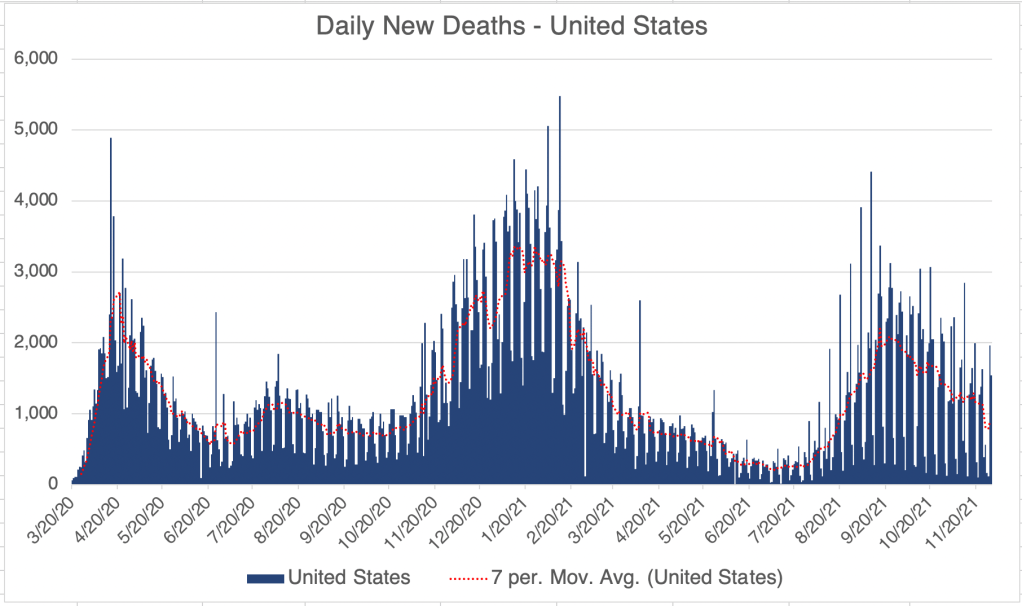
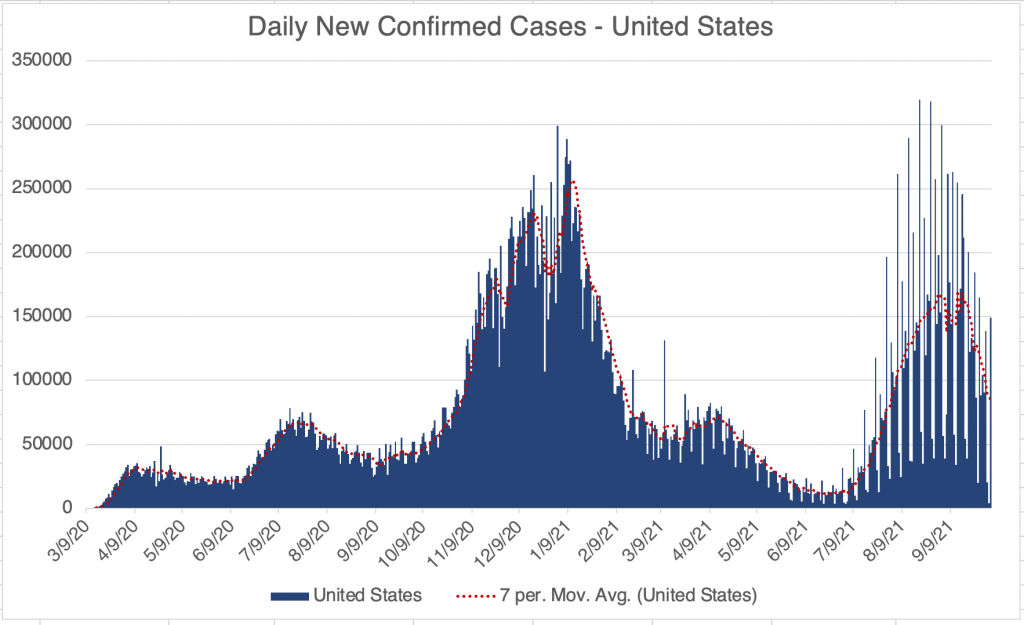
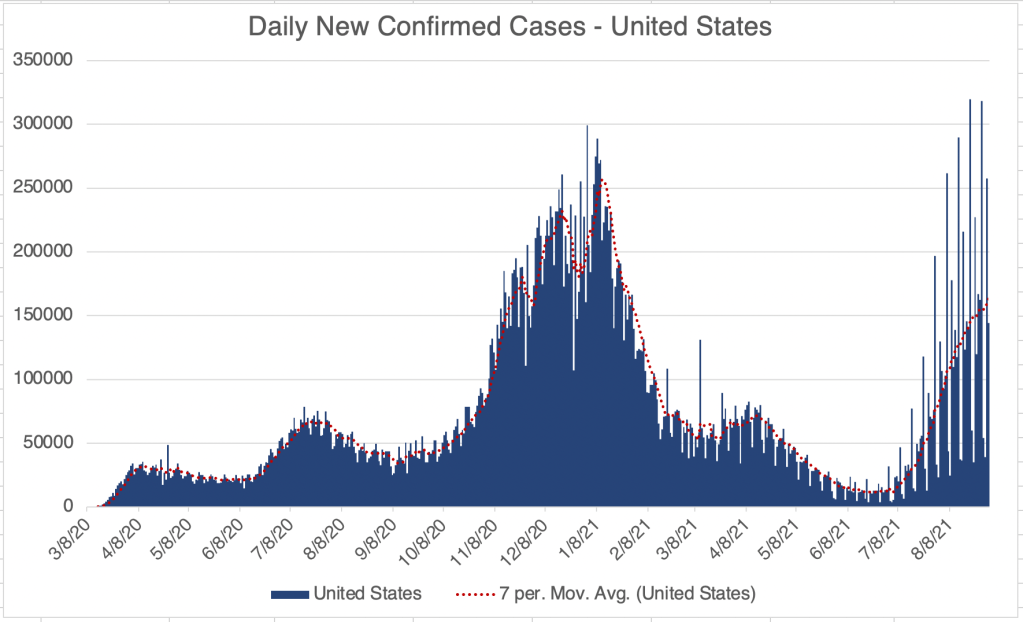
After 12 days of symptoms, I still have COVID. My symptoms are considered mild, but I’m still tired, have no appetite, and am frequently feverish, so writing a long post is not my favorite activity right now. I also have a small amount of viral pneumonia, but not enough to be treated for. For an update, I’ll just state for now that cases are coming down rapidly in the US right now. I may add a real update to this post later.
Aspiration by vaccinators: I did want to point out that I saw a very interesting video recently from John Campbell that is very instructive. He points out that vaccines are intended to be given in an “intra-muscular” fashion, meaning the injection is supposed to remain in the muscle it’s injected into. If this happens, the vaccine makes Spike protein just in that localized area, and your immune system finds it there and mounts a response. Unfortunately, if a vaccine is injected into a blood vessel, the vaccine can travel throughout the body, making adverse events much more likely. For the flu, this is still not a big risk because the flu proteins only really interact with respiratory cells. But for COVID, the Spike protein can interact with cells all over the body and cause various effects including inflammation.
There is a simple way to avoid injecting in to blood vessels. A vaccinator can simply push the needle in, then pull the plunger back slightly to make sure there is no blood, then inject (Demonstration of this process starts at 22:00 of the video). This eliminates the possibility of a blood vessel injection. Unfortunately, this procedure is standard practice in just a few countries like Denmark, S. Korea, and Japan. Most countries including the US, UK, Canada, and many others do not practice this. John Campbell is very pro-vaccine, but wishes aspiration was standard.
My doctor friends tell me blood vessel vaccine injections are very rare.
In the US, lots of people in the health care industry basically ignored adverse events due to COVID vaccination. This includes me for a time. The CDC is still not capturing all of the available data on adverse events. Many of these events could have been avoided with a small change in policy.
Vaccination has helped a lot of folks have milder COVID symptoms. It’s too bad that the lessons from adverse events were not absorbed sooner. If you get vaccinated or get a booster, see if you can get them to aspirate before they inject!
The UK drops COVID restrictions: The Omicron wave has come and gone in the UK, and the country has basically dropped all COVID related restrictions. The US is a few weeks behind the UK, so we may be able to drop restrictions here soon too.
Omicron is milder, but I certainly haven’t had an easy time of it, so I wouldn’t recommend running out and getting your natural immunity by getting Omicron. If you haven’t had it yet, continue to wear your N95, KN95, or KF94 while indoors in public. Or even outdoors in groups. I probably got COVID outside but in close proximity to someone with COVID. The stuff that worked with previous versions doesn’t necessarily work with Omicron.
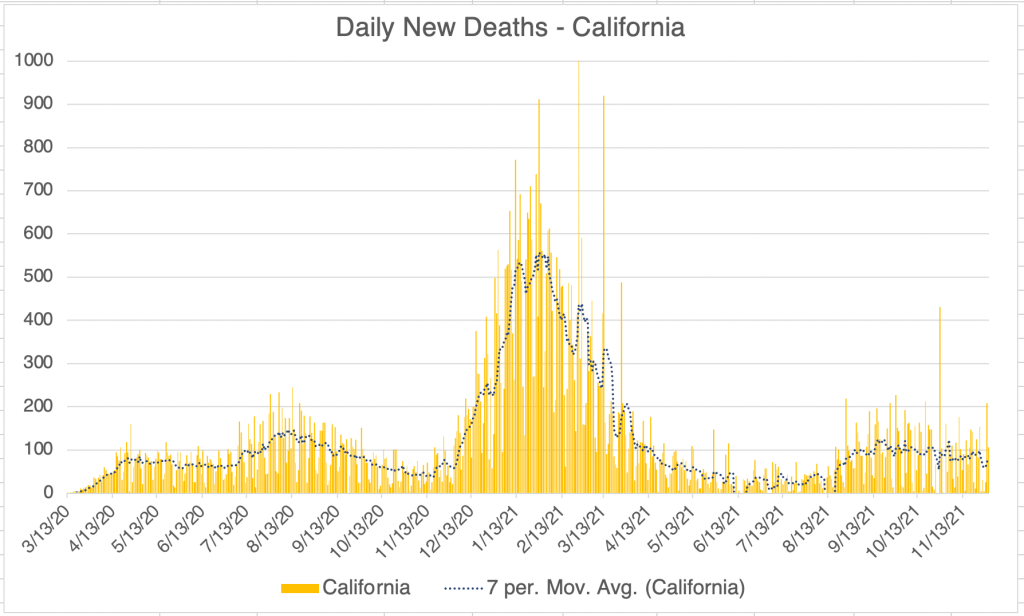
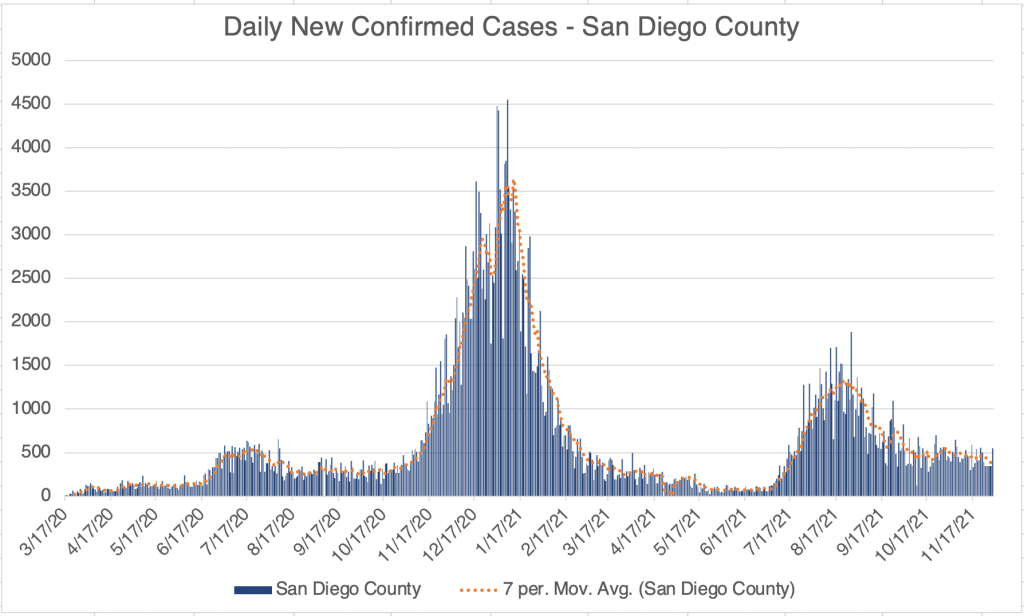
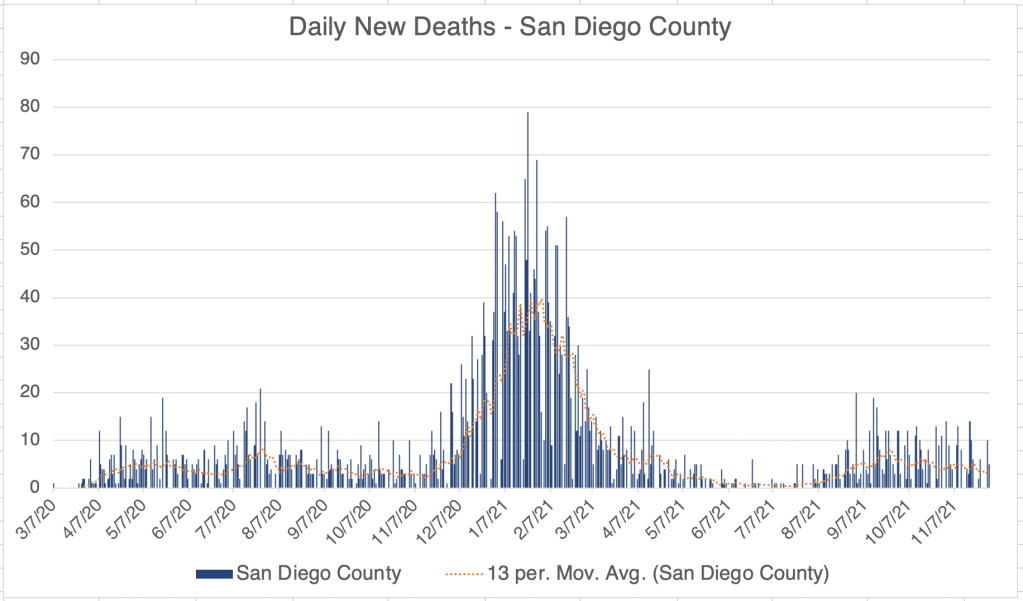
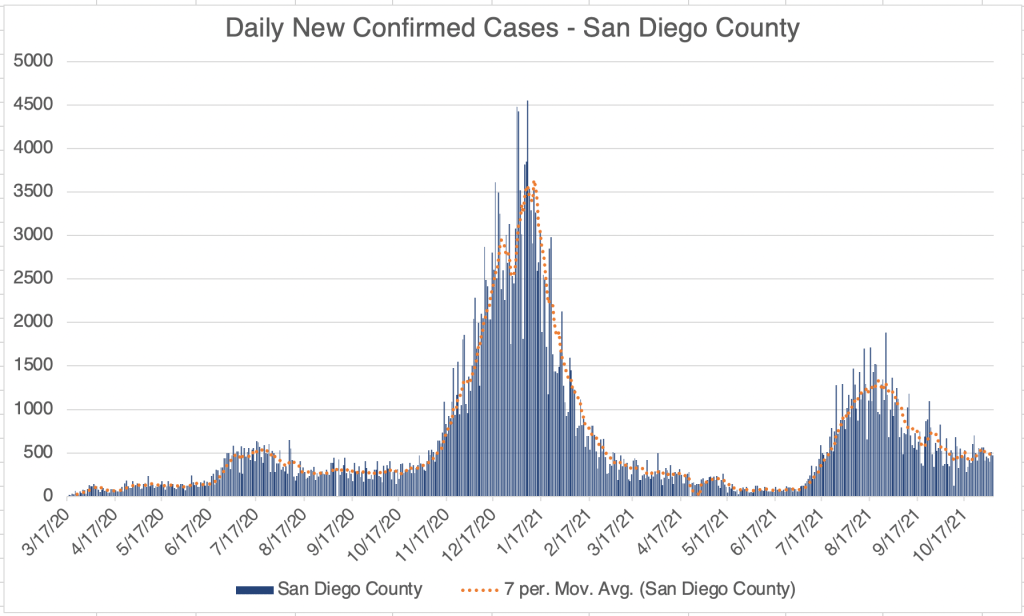
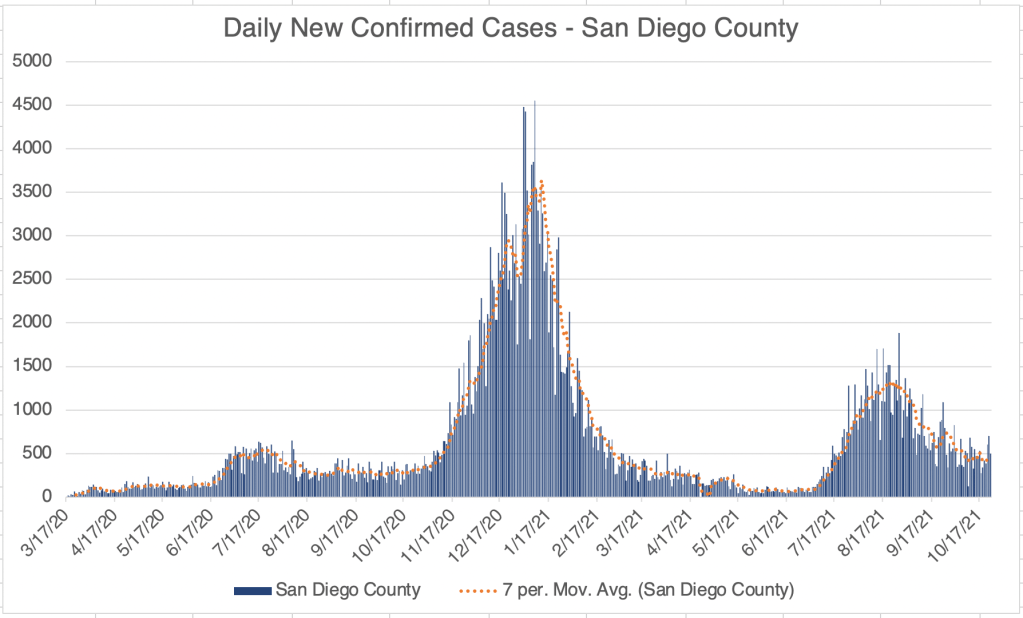
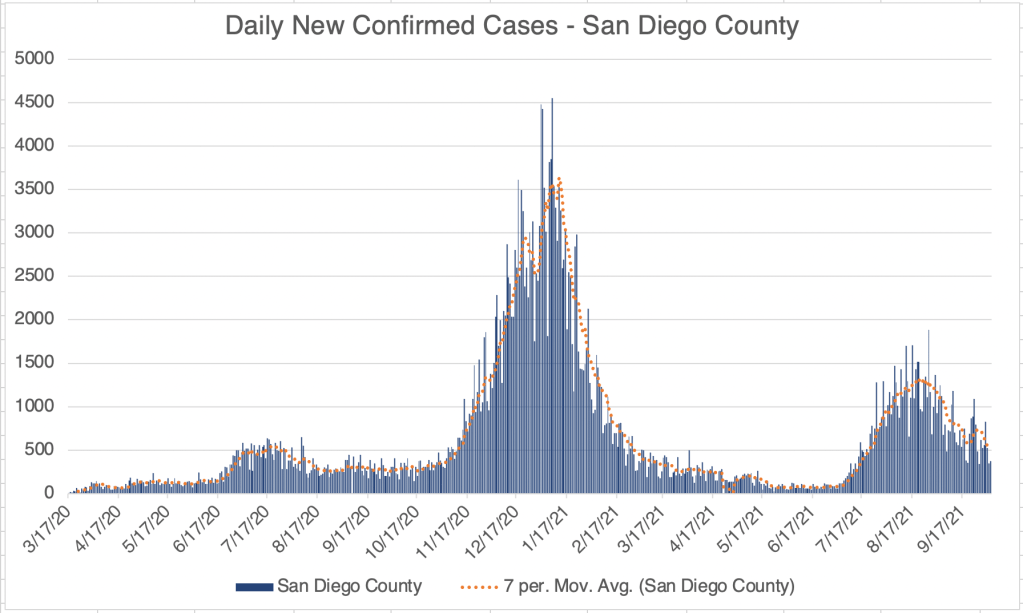
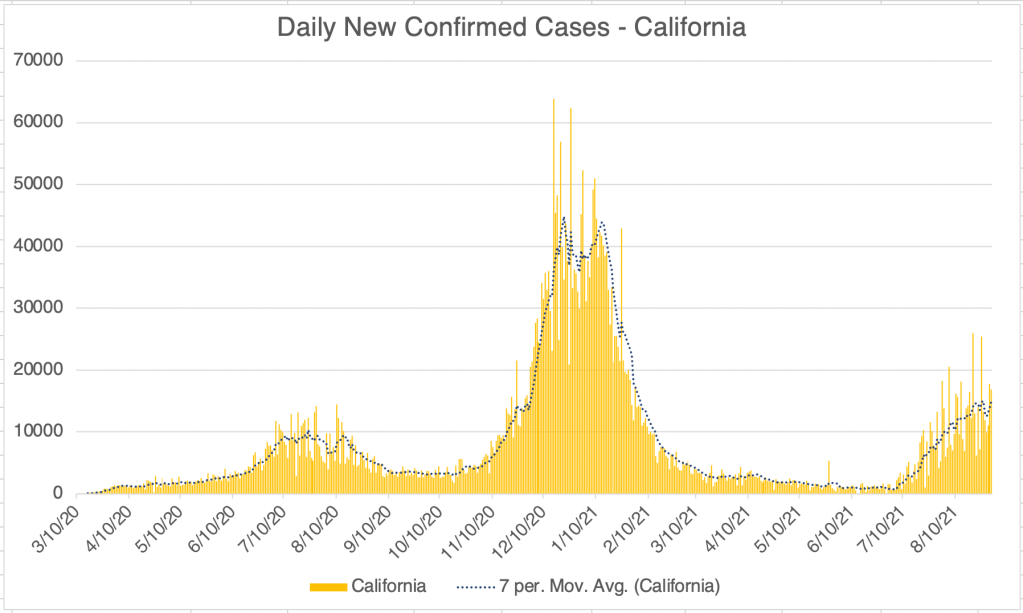
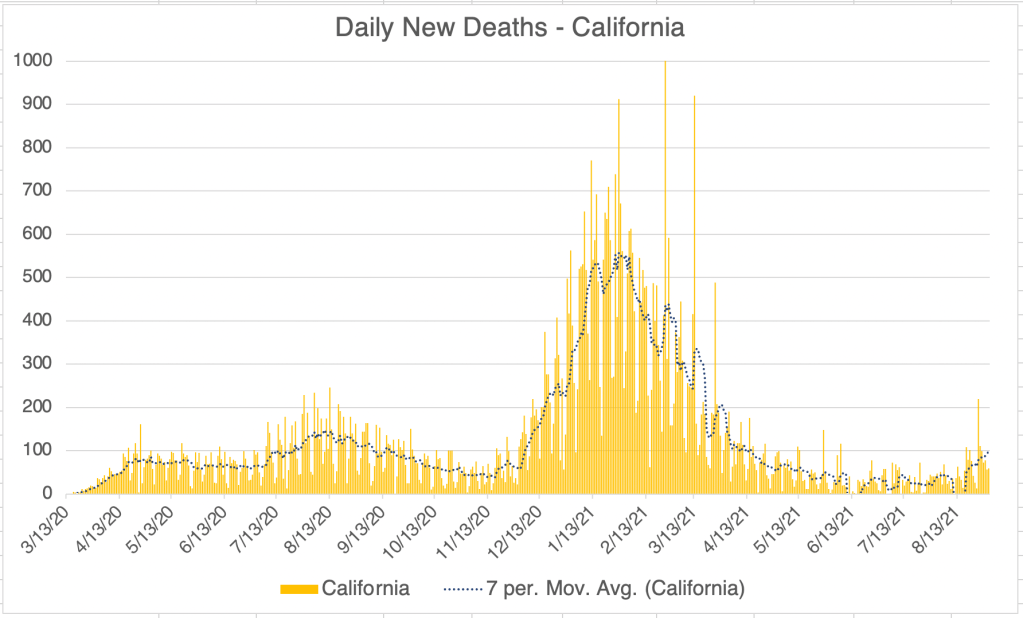
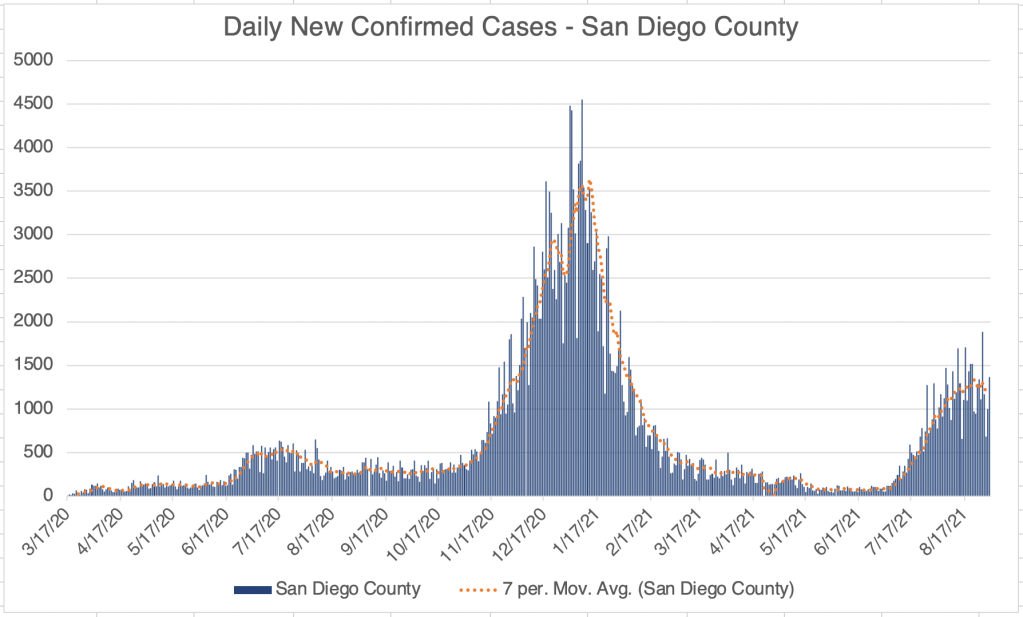
In California and San Diego County, cases are still stable, at a rate about as high as last Summer, but lower than the peak of Delta. Just hours ago, California Public Health and the CDC have announced that a patient with the Omicron variant has been detected in California. They had returned from South African on the 22nd, and the case was detected on the 29th.
_____________________________________ UPDATE: December 1st, 1:00 pm Just hours ago, California Public Health and the CDC have announced that a patient with the Omicron variant has been detected in California. They had returned from South African on the 22nd, and the case was detected on the 29th. _____________________________________ UPDATE: December 2nd, 2021 2 more cases of Omicron have been detected, in Minnesota and Colorado. The case in California and Colorado were in individuals who were fully vaccinated. All individuals have had mild symptoms so far.
Hours after reporting the above, another 5 cases of Omicron were reported in New York City. Suffice it to say, it’s now clear that Omicron is in the US and is already nation wide. I’m sure a lot more cases will be reported soon.
Most new cases of a new strain can only be reported after expensive and time consuming sequencing testing has been performed, so these results will come out more slowly than just a COVID detection.
I’m going to stop reporting individual new cases, since the point has been made that Omicron is in the US. _____________________________________
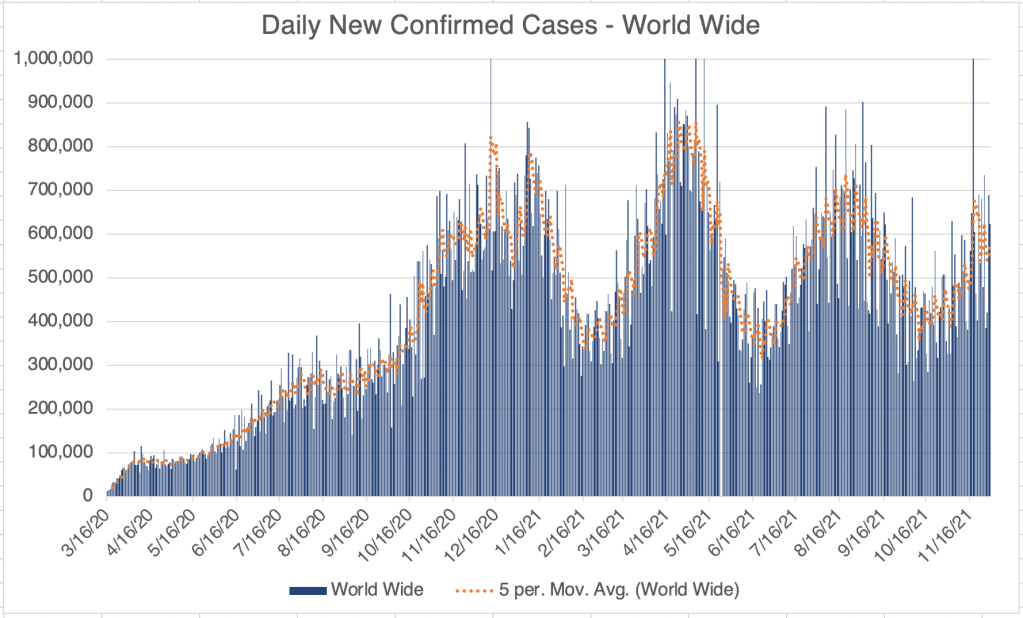
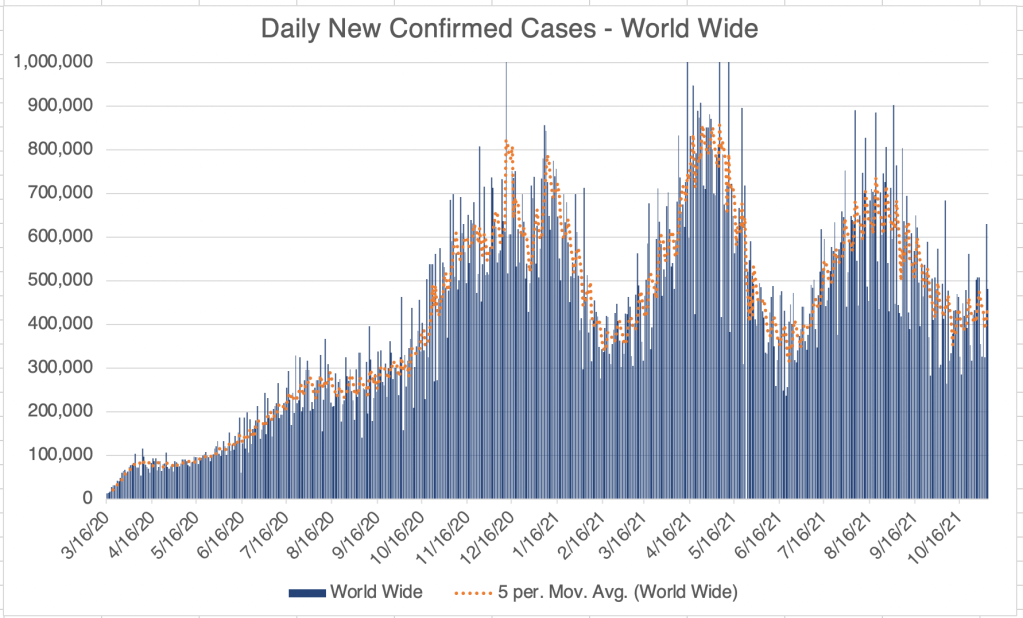
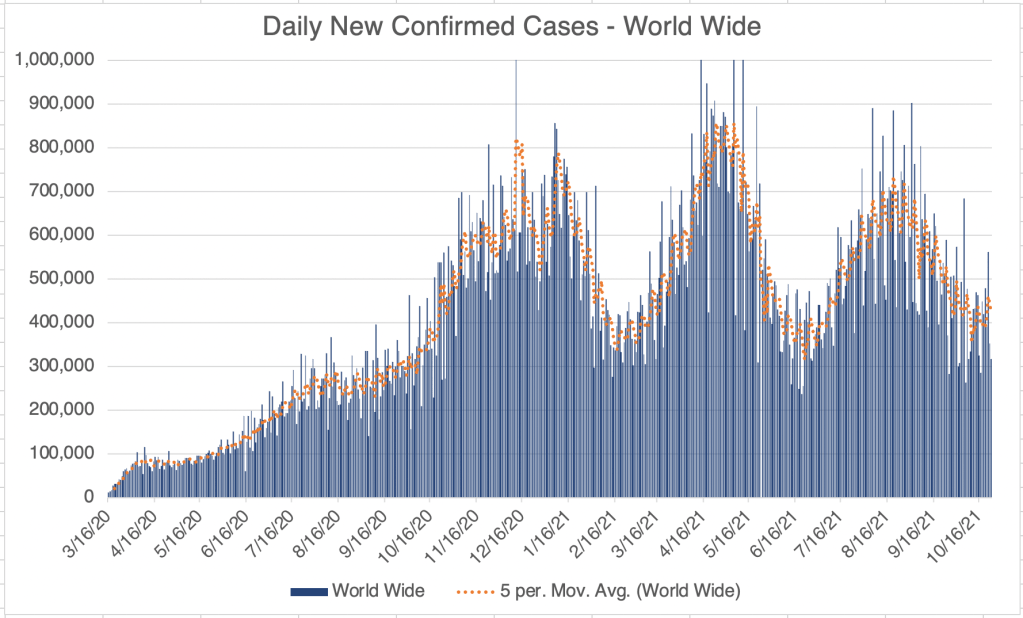
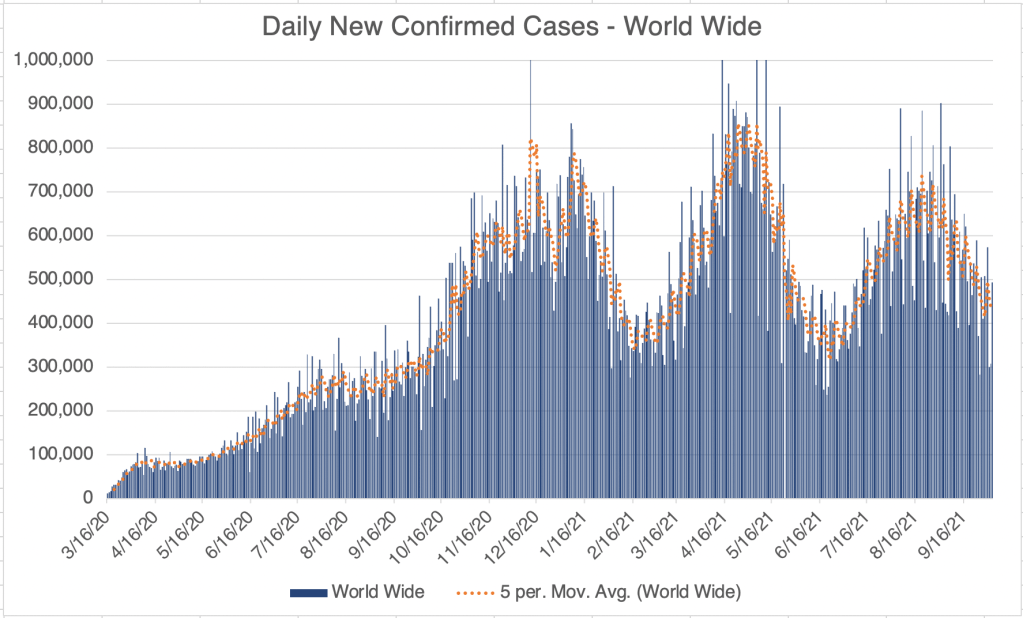
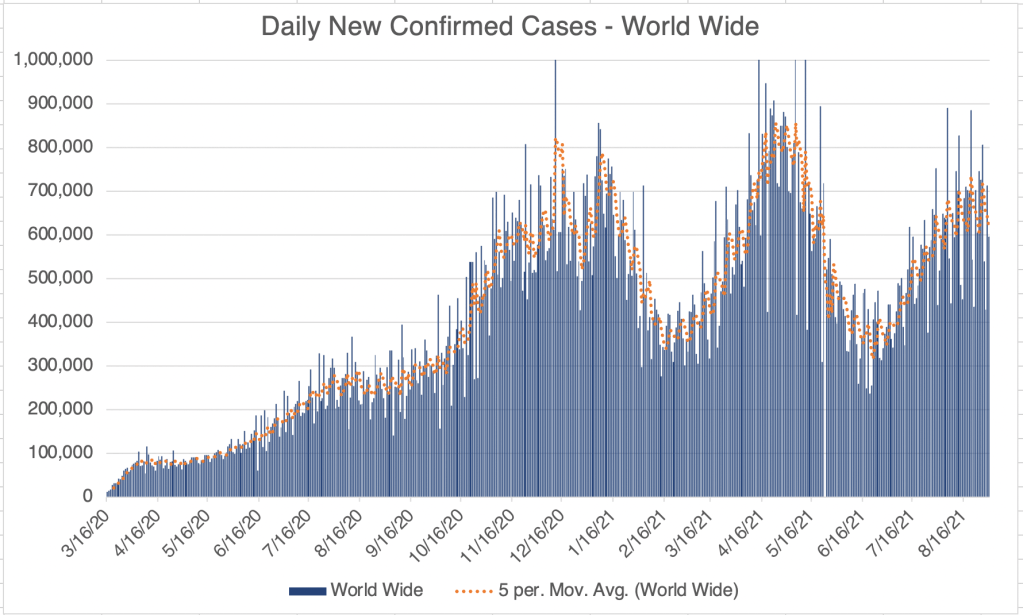
World wide, cases are climbing at the moment, with big increases in several European countries. Several countries have reported the detection of the Omicron variant, but so far only a few cases in each country are due to Omicron, so the big increase in cases may be due to Delta and the onset of Winter.
Vaccine against Omicron: So far, Delta is still the majority of cases world wide. Even in South Africa, only about 20% of the COVID cases are suspected to be due to the Omicron variant as of this writing. But because of the large number of mutations in the Omicron variant, scientists are concerned that the current batch of vaccines will not work against Omicron.
I saw an interview with Albert Bourla, the CEO of Pfizer. He stated that Pfizer could have a vaccine against Omicron ready for distribution in 100 days. Interestingly, Bourla also said in the interview that they had designed a vaccine against Delta, but they hadn’t released it because the original vaccine worked well against Delta. I was very discouraged by this comment. Many countries, including Israel, have been reporting that the vaccines have only been about 40-50% effective against Delta, and even the CDC admitted in July that 15% of COVID deaths have been in vaccinated individuals. I seems the me that the vaccines against the Wuhan strain have not worked well against Delta, and that vaccines against Delta should have been released. The comment seems to be evidence that Pfizer is not fully absorbing data on vaccine effectiveness from around the world.
Is COVID endemic?: I had hoped that once the vaccines came out, we would be able to generate enough immunity (natural and vaccine related) against COVID that it would go away. With 2 major variants that can evade the vaccine already out (Delta and Omicron), I’m becoming more convinced that COVID is indeed endemic at this point, meaning that it will continue to mutate, circulate, and be part of the fabric of life from here on out.
My personal strategy has been to avoid infection and vaccination until it all blows over. I’m becoming convinced that this will not work. So should I get vaccinated now? I’m concerned that Omicron might trigger the ADE pathway and cause worse symptoms for those with immunity to SARS-2. For this reason, I’m going to continue to keep myself SARS-2 free until more is known. Regardless of vaccination status, I encourage you to take some extra precautions until more is known about Omicron. Concern is good, panic is bad.
A glimmer of hope: As stated in Monday’s post, South African Doctor Angelique Coetzee has stated that her COVID patients have had very mild COVID symptoms. Her patients are mostly young people. If symptoms from Omicron are mild in older patients, and the new variant is very infectious, that there is a small chance that it will present a safe and effective way to provide immunity to lots of people. Of course, we will need to wait a few weeks to see.
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.”
This is a case update. I’ll also talk about the newly release v@¢¢¡ne mandate from OSHA, whether you should get a booster, and the question of whether v@¢¢¡nes lead to new SARS variants.
New cases in the US, California, and San Diego County are all fluctuating right now. It’s hard to say if this represents the beginning of a new wave. Most of us are feeling like the pandemic is basically over, but I will point out that in the post-Delta trough, we still have as many new cases per day as we did at the peak of last Summer’s wave. Minnesota, Colorado, New Mexico, and Arizona are all experiencing increases in cases right now.
V@¢¢!ne mandate finally drops: In September, the President said he wanted government agencies to produce a mandate for v@¢¢¡nation. Just this week, OSHA issued an Emergency Temporary Standard. This is official form of the v@¢¢¡ne mandate we’ve been waiting for. The mandate conforms to the news you’ve heard, all employers with more than 100 employees must get v@¢¢¡nation status from all employees, and those who are not v@¢¢¡nated must be tested weekly. The testing option means that the standard does NOT require that everyone be v@¢¢¡nated. Enforcement will begin January 4th, 2022.
As we saw last week, the CDC has known since July that a significant number of hospitalizations and deaths have occurred in fully v@¢¢¡nated individuals. In addition to this, a recent Lancet paper from Singanayagam et al suggests that the transmission of Delta is less from v@¢¢inated individuals, but is still very significant. In light of this, I think all employees, regardless of v@¢¢¡nation status, should be tested regularly, although it would be impossible to test everyone every week. Ignoring the transmission threat from v@¢¢inated individuals is likely to lead to trouble. Everyone exposed to someone who tested positive for COVID should also be tested.
I saw a truly amazing thing on an OSHA FAQ page regarding v@¢¢ination. I checked it again just now to make sure it was still there. Under the item “Are adverse reactions to the COVID-19 v@¢¢¡ne recordable on the OSHA recordkeeping log?” The answer reads:
DOL and OSHA, as well as other federal agencies, are working diligently to encourage COVID-19 vaccinations. OSHA does not wish to have any appearance of discouraging workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers’ vaccination efforts. As a result, OSHA will not enforce 29 CFR 1904’s recording requirements to require any employers to record worker side effects from COVID-19 vaccination at least through May 2022. We will reevaluate the agency’s position at that time to determine the best course of action moving forward.
In effect, an official government page is saying, we are asking you to ignore health information in order to get people to do what we want. Some of you may be wondering why so many people are willing to ignore official calls to get v@¢¢¡nated, or are suspicious of government in general. This is why. This also answers the question as to why it is so difficult to get clear information on adverse events. The government appears to have an official policy of ignoring these events.
I’ll say again what I’ve said many times, I am not anti-v@¢¢¡ne. I think many people with risk factors including age, obesity, respiratory or cardiac issues, those who work closely with the public, etc. should get v@¢¢¡nated. However, I am against a v@¢¢¡ne mandate. I am not v@¢¢¡nated, mostly because of the ADE issue, and because I think I can avoid being infected.
I will also state what is obvious to many, but not to some that are making policy. Lying or hiding information from the public will make people mistrust you. You can sometimes force people to comply, but you cannot, even in principle, force people to trust you. Trust must be earned. Once you lose it, it is very difficult to get back.
This rule can be applied to any area of life. Remember this if you’re a husband, wife, parent, child, pastor, politician, consultant, leader of a company, employee, or anything else where trust is required. Trust is earned, and once broken, is very hard to get back.
Should you get a booster?: Several people in the past few weeks have asked me if they should get a booster. Right now, unfortunately, my best answer is “I don’t know”. A booster may improve your immune response to the originally Wuhan strain of the SARS-2 virus, but the Spike protein from the v@¢¢¡ne is likely toxic on it’s own. In addition, the paper from Japan I wrote about some time ago suggests that another booster of the current variety is unlikely to provide complete protection against Delta. Instead they recommend a Delta derived booster.
Anyone who has had COVID or has been v@¢¢¡nated should get a Delta v@¢¢¡ne as soon as it is available to protect from any ADE related effects. Several companies are currently working on v@¢¢¡nes against Delta.
Does the v@¢¢¡ne create variants?:A nobel prize winning scientist is claiming that v@¢¢¡nation creates SARS variants. I absolutely agree that v@¢¢¡nation creates selection pressures that can force viruses to gain new forms to avoid neutralization. However, the very same can be said for natural immunity. Both natural immunity and v@¢¢¡nation create selection pressures that can lead to new viral variants. This is true of all viruses and other invading agents. In spite of this, our bodies are designed to use the immune system to fight off infection, and immunity has had a tremendous benefit, despite the selection pressure it poses. ADE is a rare exception to this rule. Our immune systems work much more quickly than viruses can adapt to them, which is why they are so effective at preventing infectious disease.
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.” _______________________________________
For California and San Diego County, however, there is a persistent higher case number, and the numbers for last week may even reflect a very slight increase in new cases.
The very large wave from last Fall and Winter started in October. We may be seeing the very beginnings of a Fall wave. Hopefully our Summer Delta wave will have provided some extra immunity.
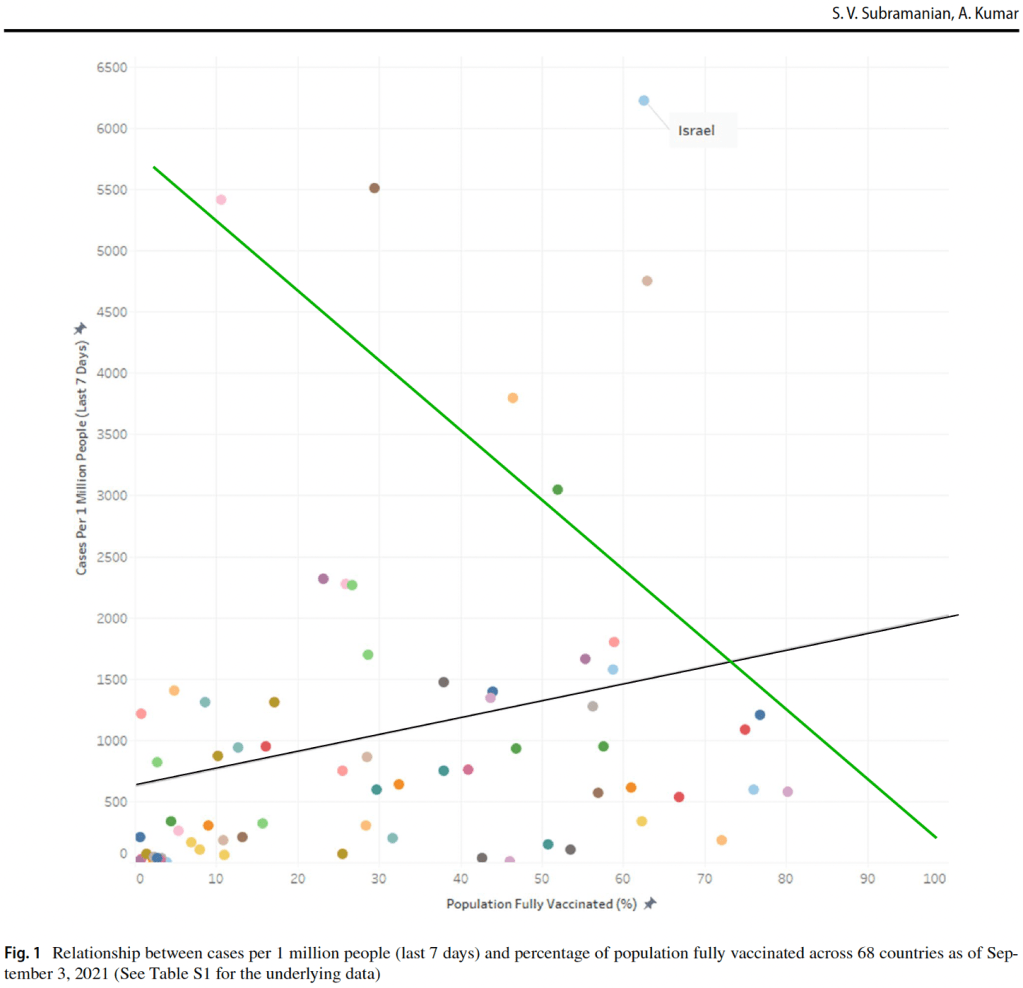
V@¢¢!nation and new cases: A paper came out in September regarding the correlation between v@¢¢!nation rates and new cases. The study compares data in 68 countries and 2947 US counties that had 2nd v@¢¢!ne doses available.
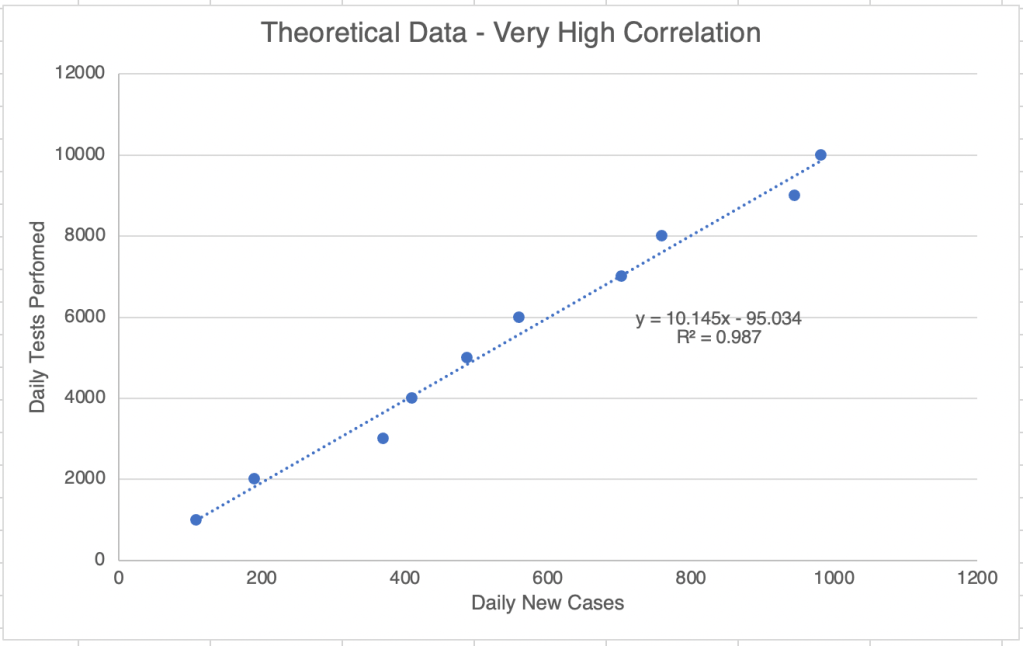
The most interesting figure features a piece of data called a “linear regression”. This kind of data compares 2 variables and shows visually if they are related. In the below hypothetical example, the 2 variables, the number of tests in a day and the number of confirmed cases in a day, shows a high correlation between these 2 things. Notice that the line plotting the relationship between data points goes from bottom left of top right as the values of each variable increase.
A linear regression plot with hypothetical data. Good correlation gives an R squared value between 0.95 and 1. If the variables are negatively correlated, the R squared value will be between -0.95 and -1.
The paper shows a linear regression plot with the percent of the population that is fully v@¢¢!nated on the x-axis, and the per capita confirmed case rate on the y-axis. If v@¢¢!nation strongly protects individuals from infection, new cases would go down as v@¢¢!nation went up. In this case, the plot line would go from top left to bottom right (the green line). Instead, it appears that there is little correlation between percent v@¢¢!nation and cases, producing the black line.
V@¢¢!nation vs cases produces black line, showing little correlation between the 2 variables. The green line was added by me and shows hypothetical data that would show strong correlation. From Subramanian et al.
They also have a box plot with US counties showing the new per capita case loads arising from counties with various levels of v@¢¢!nation. While counties with high v@¢¢¡nation rates do have fewer cases, the impact is not as profound as might be expected, and the difference between counties above 50% v@¢¢!nation rate is likely not statistically significant.
Box plots showing v@¢¢¡nation vs per capita cases in US counties. V@¢¢¡nation rates are groups in blocks for this view. Notice that very little difference exists between counties above 50%. From Subramanian et al.
It should be noted that this study was performed in September with data mostly from August. This is during the Delta wave in the US and many Western countries. The Delta variant may be different enough from the original Wuhan strain to enable the Delta virus to avoid neutralization by Wuhan induced immunization.
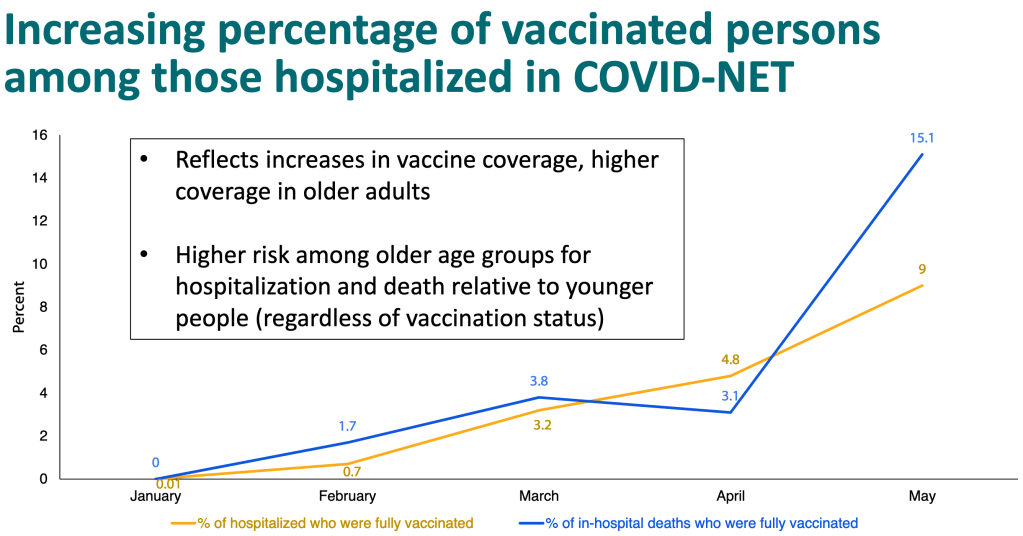
It has long been rumored that v@¢¢!nation does not prevent infection, and this paper seems to support this view. In spite of this, most scientists, including me, still hold that v@¢¢!nation does reduce the chance of hospitalization and death in infected patients. This is still true. However, a power point published by the CDC shows that this protection is diminishing as well. In January, hospitalization and death among v@¢¢!nated individuals was essentially 0%, but now 9% of hospitalizations are among v@¢¢!nated people, and 15% of deaths.
Why is this happening? There are likely multiple factors. Certainly, the Delta variant is not the same virus as the Wuhan strain. The different Spike protein makes it more infectious, and may not be recognized by an antibody against, the Wuhan strain. It may even be triggering the Antibody Dependent Enhancement (ADE) pathway in some patients. Also, it is becoming clear that v@¢¢!ne mediated immunity has been going down over time, necessitating a booster. The paper from Liu et al argued that given the differences in Delta, a booster against Delta would be much more effective than another booster against the Wuhan strain.
V@¢¢!ne mandates: I still believe that v@¢¢!nation is a good choice for some with risk factors like age, obesity, diabetes, or respiratory problems. However, I remain against v@¢¢!ne mandates because they do not take into account the medical history of individuals, the data that natural immunity is significantly better than v@¢¢!ne mediated immunity, and also the potential danger of ADE. In addition to these scientific reasons, I have also felt an increasing orneriness on my own part. Orneriness is not a good reason to make scientific or medical decisions, but policy makers should realize that it is a powerful reason for many.
For myself, I have chosen to not be v@¢¢!nated, but to remain careful to not be infected. I continue to wear a mask indoors when there is poor ventilation.
President Biden mandated v@¢¢!nation for federal agencies soon after taking office. He announced in September that he would seek v@¢¢!nation mandates for private companies with more than 100 employees. While many assume that a mandate for private companies is in effect now, as of this writing, no such mandate for private companies actually exists, either by law or by executive order. Companies that have enacted v@¢¢!ne mandates as of now have done so voluntarily.
________________________________________________ Update: November 5th, 2021
The official vaccine mandate was released on November 4th 2021 and is scheduled to be enforced starting on January 4th 2022. Details are on my November 5th post. ________________________________________________
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.” _______________________________________
This is a case update. I’ll also discuss a new video from Project Veritas featuring interviews from employees of Pfizer.
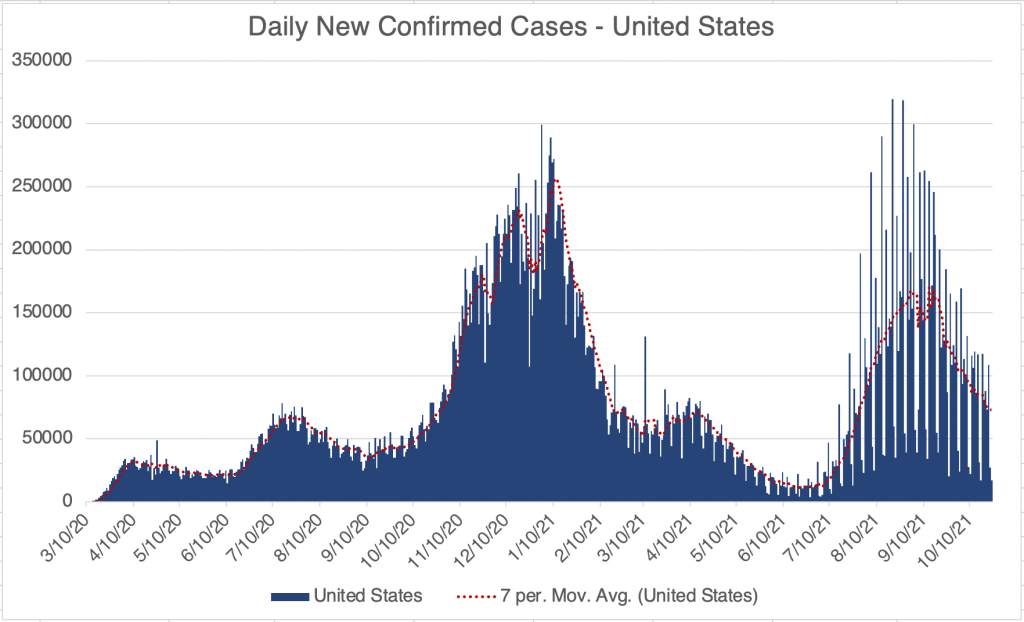
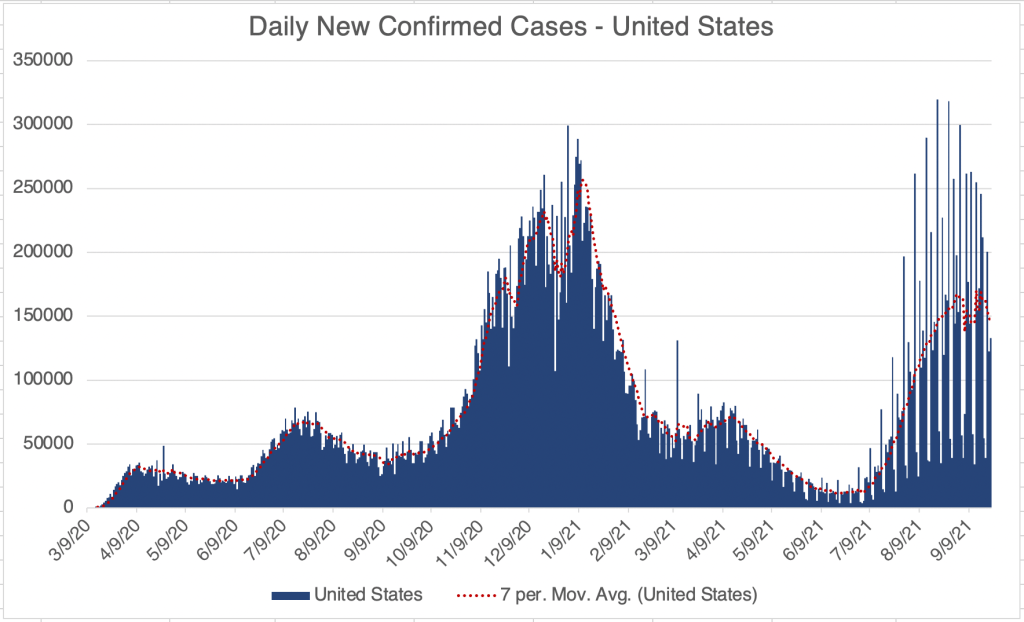
The Delta wave continues to wane in the US, with cases overall continuing to go down sharply. This is great news, but I have to caution that last year’s Fall/Winter wave started in October, so there is a chance we will see a new wave starting in the Northern states. In fact, cases are starting to increase right now in Minnesota, Wisconsin, Michigan, and Maine, while they are going down in the Southern states.
Cases are also going down in California and San Diego, although there was a spike in cases last week. Since both regions saw the same spike, it suggests that the event causing the spike may have taken place in Southern California, but this is only speculation.
Pfizer employees discuss immunity: I always hate making politically charged posts, but this is another occasion when I must. Project Veritas posted another video just yesterday. In it, 3 scientists at Pfizer discuss the v@¢¢!nes, saying among other things that natural immunity is actually better protection against the virus than v@¢¢!ne mediated immunity. This is in agreement with the data from Israel published as a pre-print a few weeks ago.
As I’ve stated many times, for at risk people, a v@¢¢!ne is very likely to be of benefit. I have recommended that at risk people get v@¢¢!nated. If you’ve already had COVID, 1 dose of v@¢¢!ne is likely to provide extra benefit. However, if you’ve had COVID, your natural immunity is likely to provide better protection than “full v@¢¢ination”.
They also make the claim that v@¢¢!nation benefit drops over time because the antibodies gained from v@¢¢!nation drop off over time. I would also point out that another cause may be that new variants may diverge from the original Wuhan strain enough to makes v@¢¢!nes less effective, but this point is not addressed in this video.
One person even states “I mean, I still feel like I work for an evil corporation.” I want to make a comment about this. It’s easy for us to blame big corporations for some of the decisions they make, since most of us aren’t in that position. I worked for Quest Diagnostics, a large medical testing company. The vast majority of the people who worked there believed in the mission of providing high quality information to our client doctors and patients. However, as with any large organization, there were those who were focused on profit, at times over the interests of the clients. Most often this came in the form of passing over projects that would help patients, but would not bring in a lot of income. They would argue something like “We aren’t a charity. We need to bring in money to survive as a business.” This is of course partially true. Director Spike Lee once commented in an interview that the most interesting conflicts are those in which both sides are correct.
Of course, a company or an individual can cross a line after which their actions become unambiguously wrong. This often happens because they’ve made well intentioned compromises until they have lost their moral sensitivity. But I want you to remember something important. The Presidents and CEO of companies work most directly for the board of directors. The board of directors works most directly for the shareholders. In our modern investment environment, which includes mutual funds, many of the shareholders don’t even know they are part owners of a company! As far as they know, they just own a mutual fund. As far as their mutual fund goes, they only care if it’s making them money, since they don’t know what companies they hold, or what their business practices are! So the CEOs are ultimately working for people for whom profit is the only concern. Folks, those people are you and me!
Yes, companies that behave unethically should be held accountable. If Pfizer has misled the public, then they should be held accountable. But we can’t forget that anyone who holds a mutual fund that includes Pfizer has a voice in this as well. I will tell you that I am talking to myself as well. I currently have no idea what companies are in the mutual funds that I own. We should all take the time an find out what companies we hold the most stock in, and consider finding out what they are doing. You can then contact your mutual fund company and make suggestions about what they can communicate to these companies, or consider selling funds with stocks you don’t like. The small choices we make every day do have an impact.
V@¢¢!ne mandates: V@¢¢!nes will certainly benefit at-risk individuals. In addition, it is clear that countries with large v@¢¢!nation programs have had lower fatality rates during the Delta wave than other countries. However, I am not v@¢¢inated, and am firmly against v@¢¢!ne mandates. It is especially counter productive for hospitals and other organizations to be letting go of highly trained people who have chosen not to be v@¢¢!nated. I hope this new information will bring some balance to the current discussion.
This is a case update. With some trepidation, I’ll also discuss the new video by Project Veritas concerning vaccines.
It appears that the US has reached the peak of the Delta Variant, with cases clearly starting to come down. On the other hand, as numbers start to come down in the South, we may already be starting to see increasing cases in the North, as Wisconsin, Pennsylvania, Ohio, and Iowa are experiencing increased cases right now. If last year was any pattern, we may see large case numbers in the North as people start to spend more time indoors.
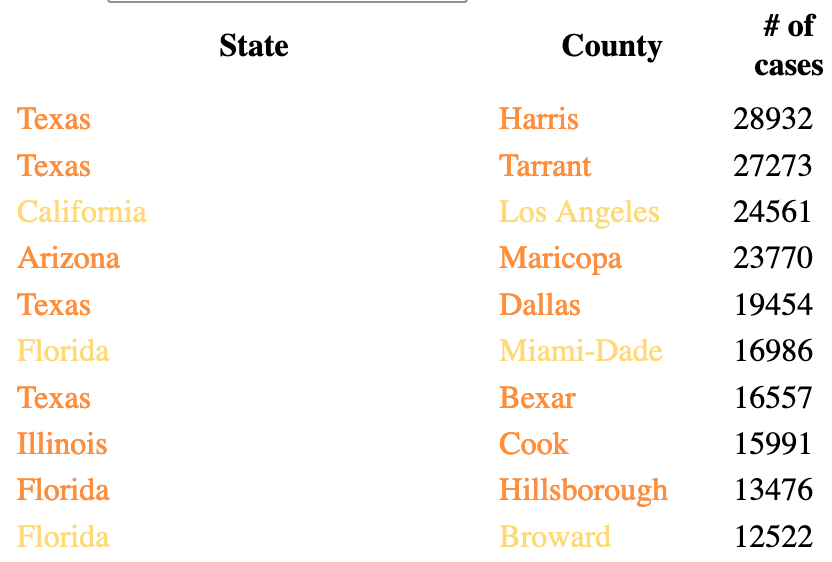
California and San Diego County are continuing to improve. LA County has “achieved” something in the last week, improving enough to give up the spot as the county with the most cases since last Winter. 2 counties in Texas, Harris (Houston) and Tarrant (Fort Worth), have had more cases in the last 2 weeks than LA County.
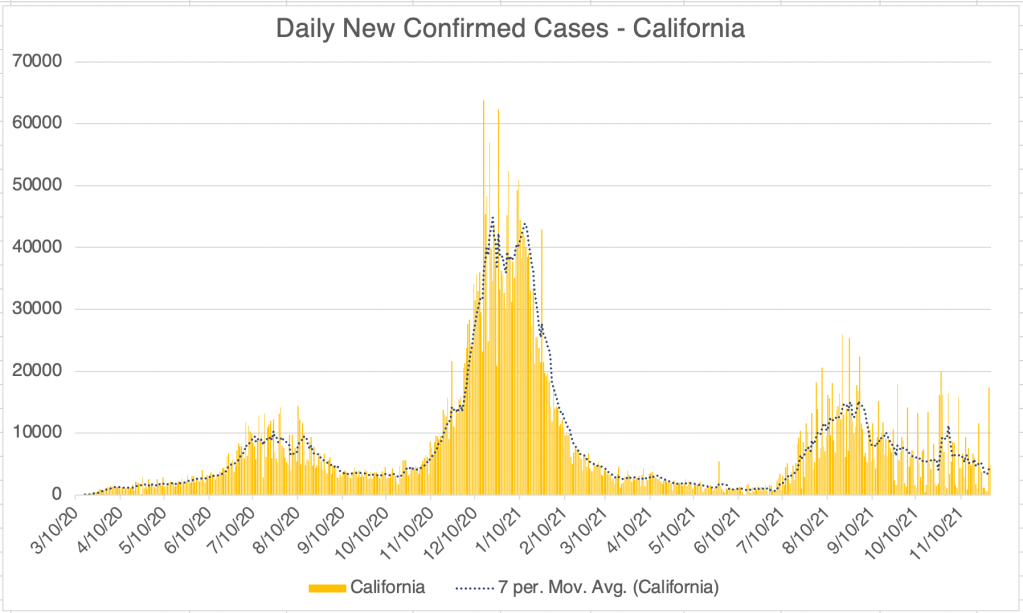
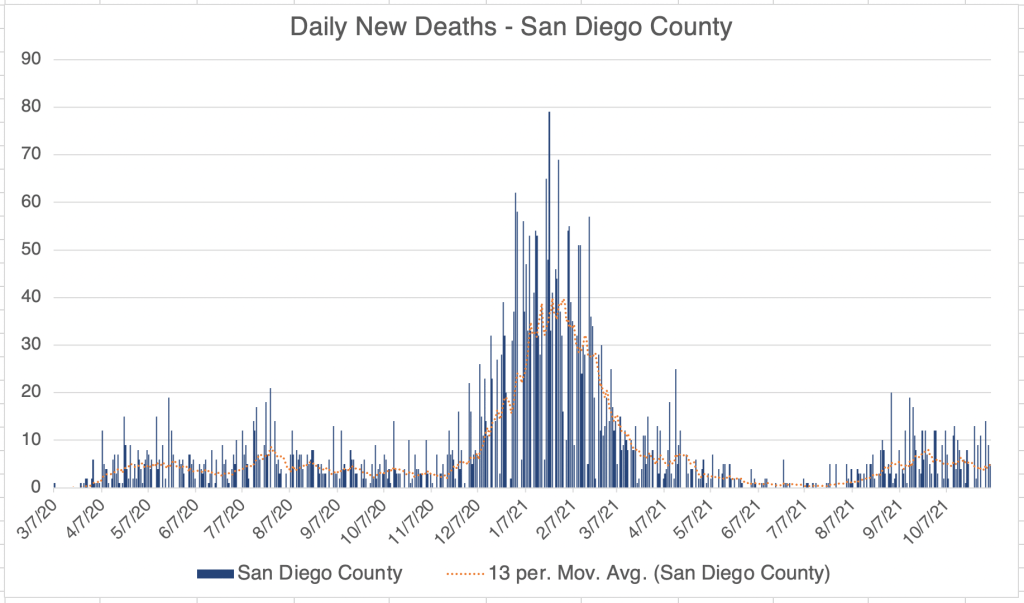
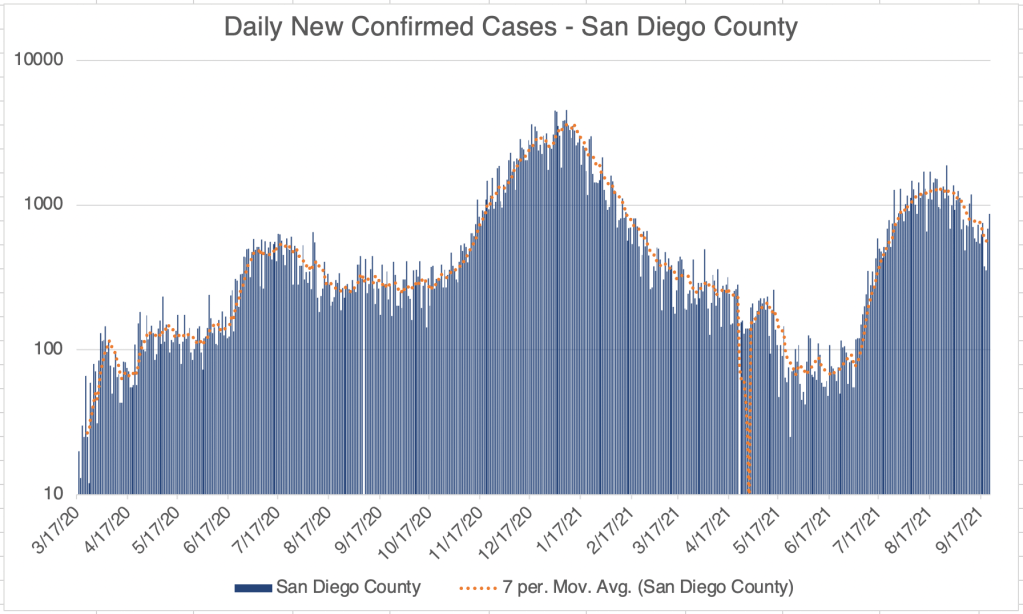
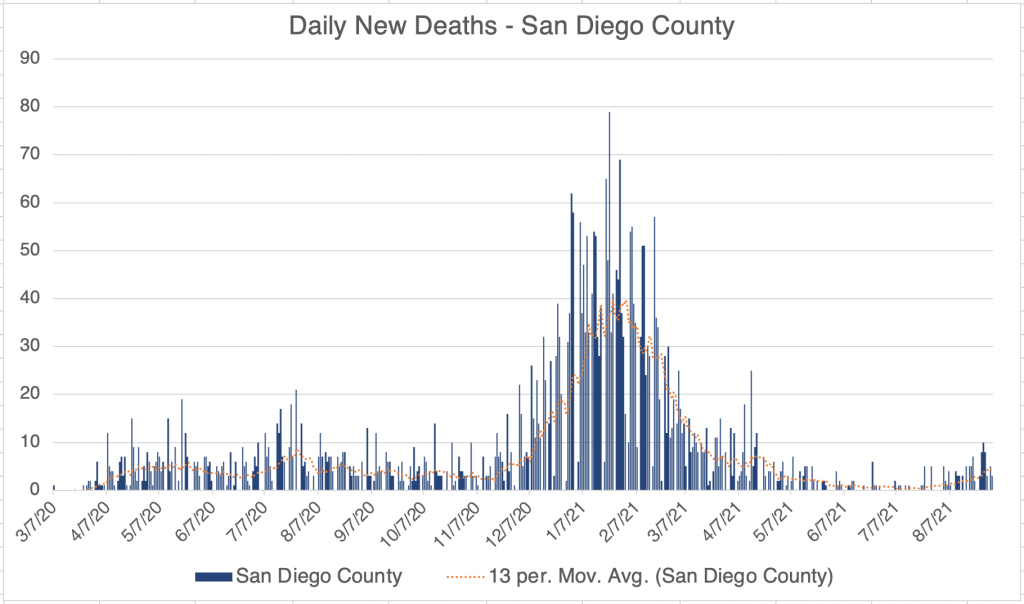
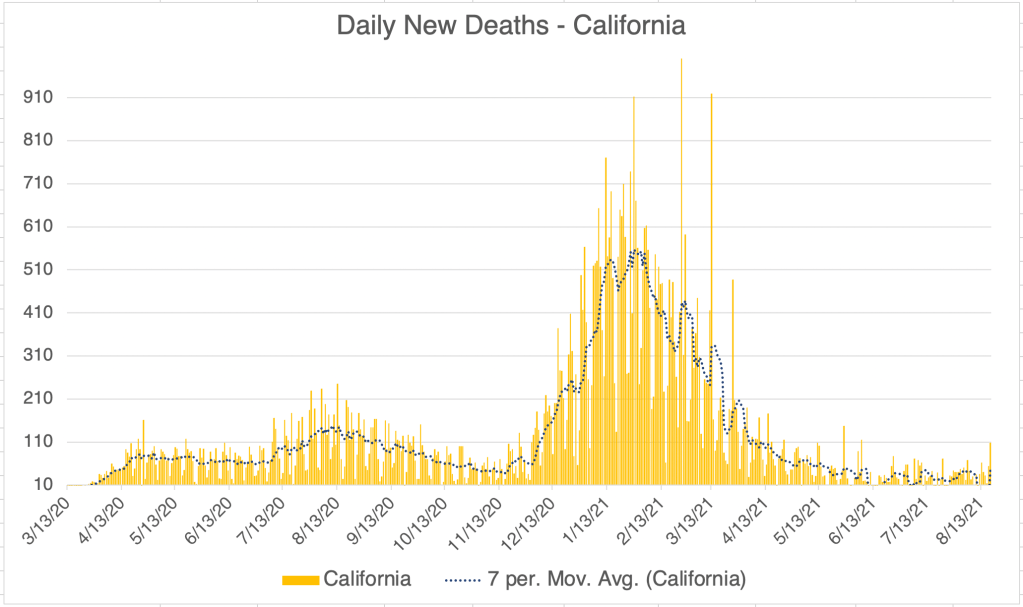
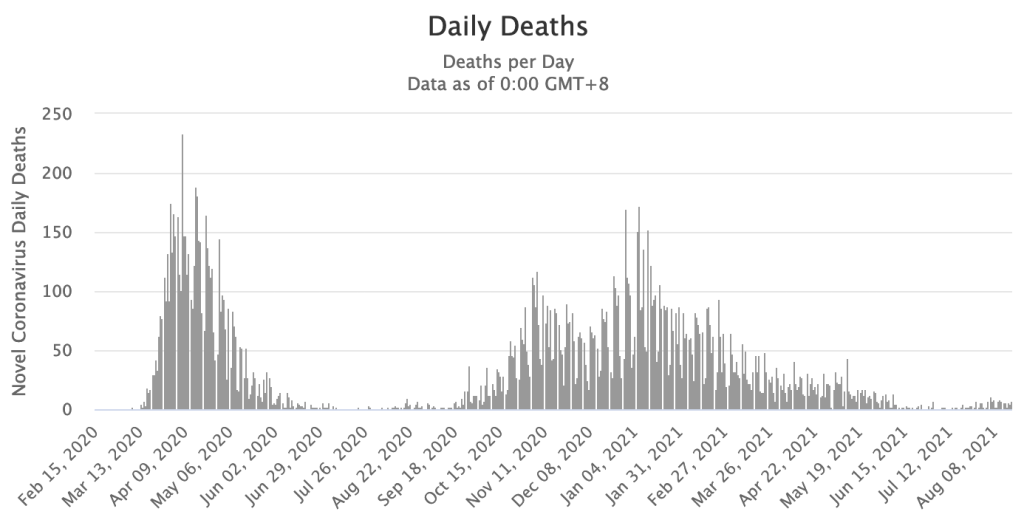
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
Project Veritas released a video of a taped conversation between medical workers at a medical center in Phoenix. In it, the workers use, shall we say, colorful and scientifically imprecise language to suggest that the COVID vaccines are not performing as expected.
There is a lot to say about this! First, let me say that available data is still insufficient to say with any certainty how many adverse effects there are, and of what kind. I will speculate here, so keep in mind that I am mostly guessing, since I don’t have sufficient information to know exactly what’s going on.
Anecdotal evidence is based on the experiences of a few people, often relayed as a story or rumor. This kind of evidence is an important pointer that something may be going on, but very often, it is insufficient to understand the situation with any clarity or as a foundation for policy. At best, anecdotal evidence gives researchers the motivation to conduct a careful study of a situation so there can be more understanding. At worst, they can cause rumors to overwhelm careful thinking, and lead to wrong conclusions in the minds of many. This kind of evidence must be taken with a grain of salt, with final judgement reserved until more information is available.
My own thinking on adverse events has evolved a lot since the vaccines came out. All vaccines carry risks, with a few adverse events happening with even routine vaccines like the flu. On balance, vaccines have been extremely beneficial to individuals and society as a whole, effectively ending diseases like smallpox and polio. So when rumors of adverse reactions to the COVID vaccines first started coming out, I initially dismissed them as the standard rare event.
But then came the suggestion that the Spike protein itself was responsible for the vaccine’s toxicity. While still not proven, this idea makes sense to me because it could explain the wide variety of reported adverse events. Increased inflammation aggravates the part of your body that is already under stress. The Spike protein causes inflammation, so it’s no wonder that the vaccine causes strange and varying symptoms in some individuals. As someone with an auto immune disease, inflammation is a big deal for me.
Unfortunately, the vaccines cannot work without producing the Spike protein, because the protein is needed to produce a working immune response. The Spike protein is an unavoidable risk.
The recent Project Veritas video is a remarkable piece of anecdotal evidence. It does not provide scientific or statistical evidence, but it does demonstrate that more information on adverse events is desperately needed.
The most disturbing part of the video to me is the claim that adverse events are not being reported to the CDC VAERS system simply because the forms take too much time to fill out! If true, this is frankly typical of a program from the CDC. Since long before the pandemic started, the CDC has sought to keep tight control of information and guidance regarding the spread of infectious disease and related matters. Legitimately, they try very hard to be accurate. During a pandemic, however, information changes too quickly for this approach to be effective. They are so careful to publish only accurate information, that information is often hopelessly out of date. Ironically, in an effort to always be right, the CDC has usually been wrong. Nothing illustrates this better than the mixed messaging on masks. Now almost everyone is hopelessly confused on this issue.
When there is a large vacuum of information, people will attempt to fill it with speculation. People from the federal government often complain about misinformation, but the CDC has contributed to it by leaving a huge hole for people to fill with guesses.
A form that takes 30 minutes to fill out is useless if no-one has the time to fill it out. In response to the video, the CDC should immediately re-make the form, making it take only 5 minutes or even 30 seconds to fill out. Yes, they will be missing some information from each patient, but they’re getting nothing on them right now, so it will still be an improvement. Instead of making the necessary changes, the CDC will probably just call the video misinformation, and try to send it behind the Digital Curtain.
A note on the VAERS system: the system is meant to capture all data that may point to a vaccine producing a pattern of adverse reactions. Any negative medical event that happens within a few days after a vaccination is recorded. This even includes events that are unlikely to be attached to the vaccination. The hope is that patterns may be recognized by immunologists that will point to a problem with a vaccine. For example, if you notice that a lot of people report hitting their head after a vaccination, this may suggest dizziness or disorientation.
Because of this practice not all adverse reactions are vaccine related. Careful study of cases by a scientist may be required to notice patterns. The data is not presented in a user friendly fashion!
Of course, the usefulness of this system is limited if a systematic problem, like a long form, is preventing events from being reported!
Vaccine rumors: I still get questions about vaccine rumors like the following:
The vaccines will re-write your DNA The vaccines will keep women from getting pregnant. The vaccines will make you shed Spike protein into the environment
When addressing questions like this, I always ask “What evidence do you have that this is happening.” Almost always, it’s just something they heard. I can’t disprove that any of these things are happening. Trying would take an enormous amount of time. I can say, however, that I haven’t seen any evidence that they are. This doesn’t mean they aren’t happening! But if there isn’t any evidence for them, we don’t have to spend time and emotional energy worrying about them.
If you have any evidence, aside from persistent rumors, that any of above things or things like them are happening, please let me know. If you see an article or blog post that argues for any of the above, they should contain actual data that supports these ideas, not just speculation.
This is a case update. I’ll also discuss the potential for a Fall peak, new branding for the approved Pfizer vaccine, and whether you should get a vaccine shot if you’ve had COVID.
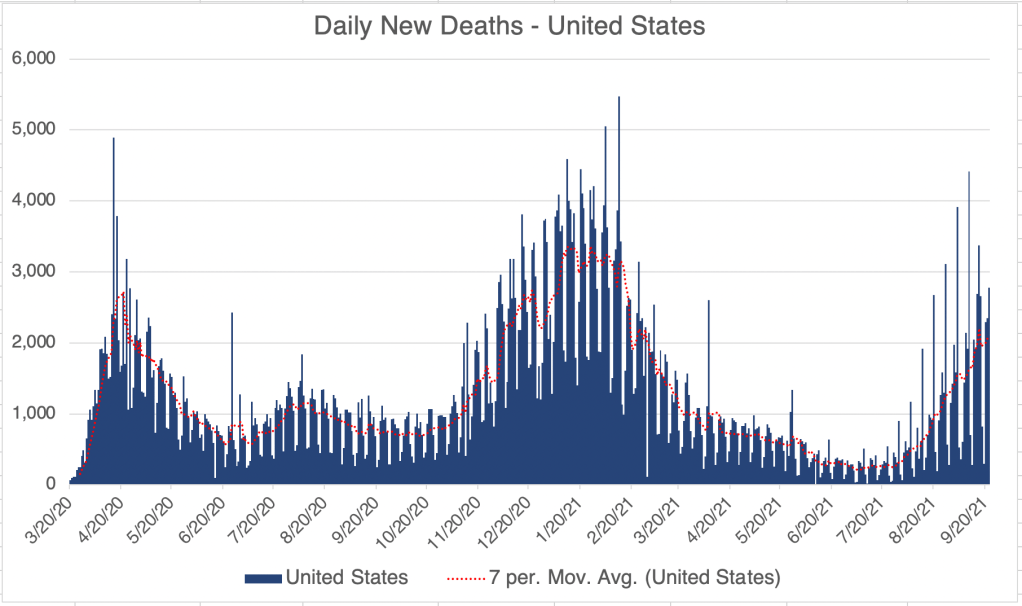
In the US, cases continue to rise, but the rise is slowing. Numbers from this last weekend suggest we may be seeing a peak in cases, but it’s too early to say. Deaths from the Delta peak are increasing also, but are proportionately less than for previous peaks.
We are starting to see fewer cases in the South. Last year, the Summer peak was centered in the warmer states, California to Florida, and then we had a very large wave starting in the North starting in October. With cases still high at the start of September, we may see another large surge of cases in the North as we head into Fall.
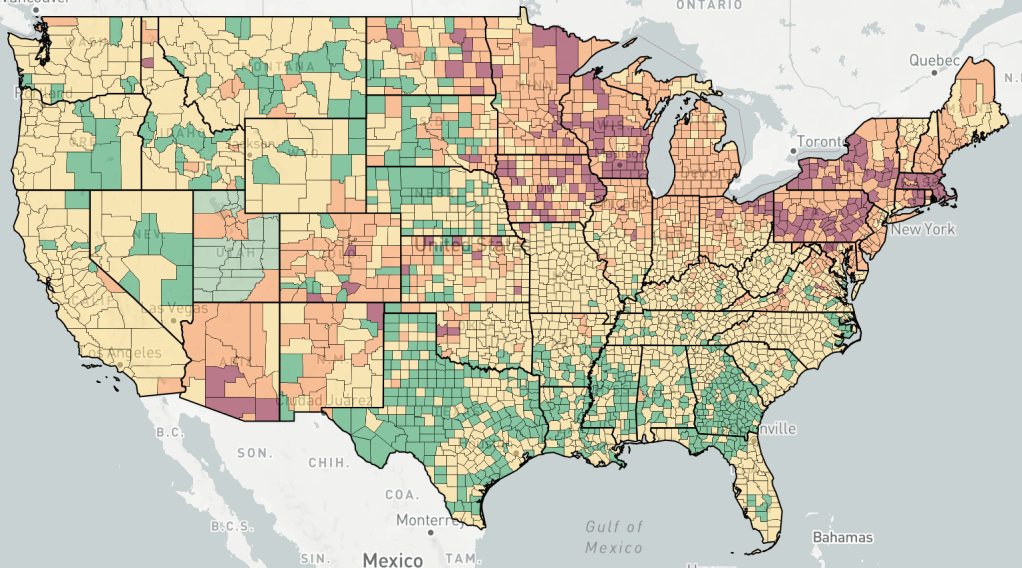
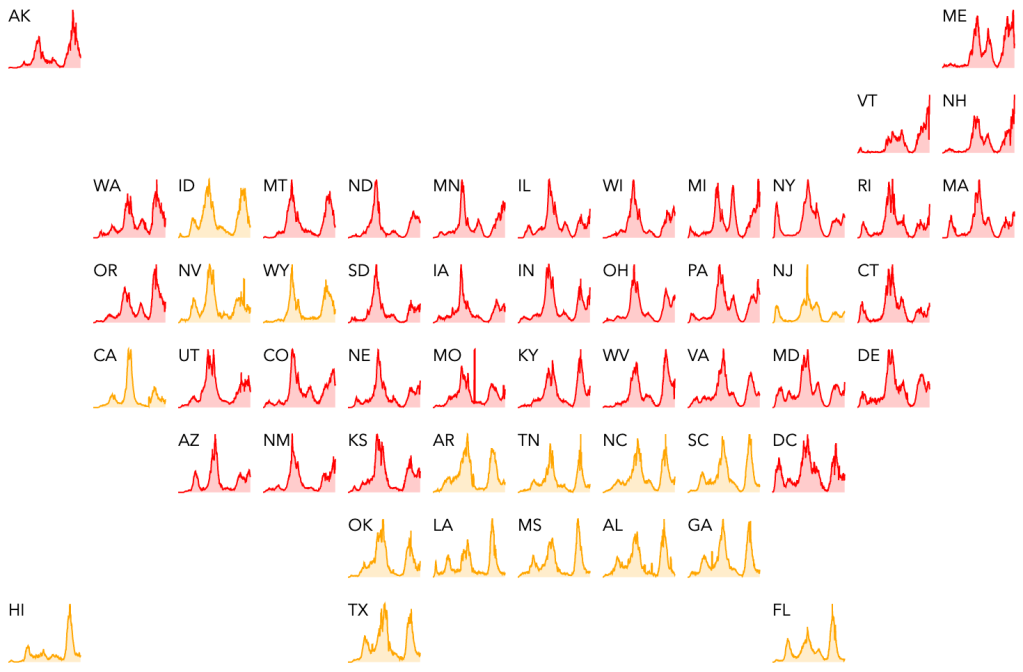
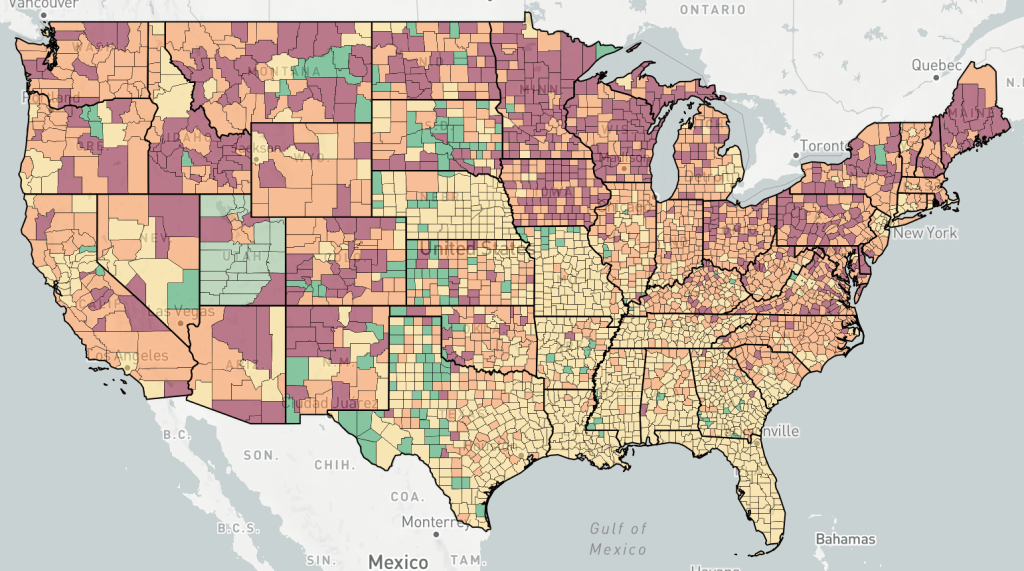
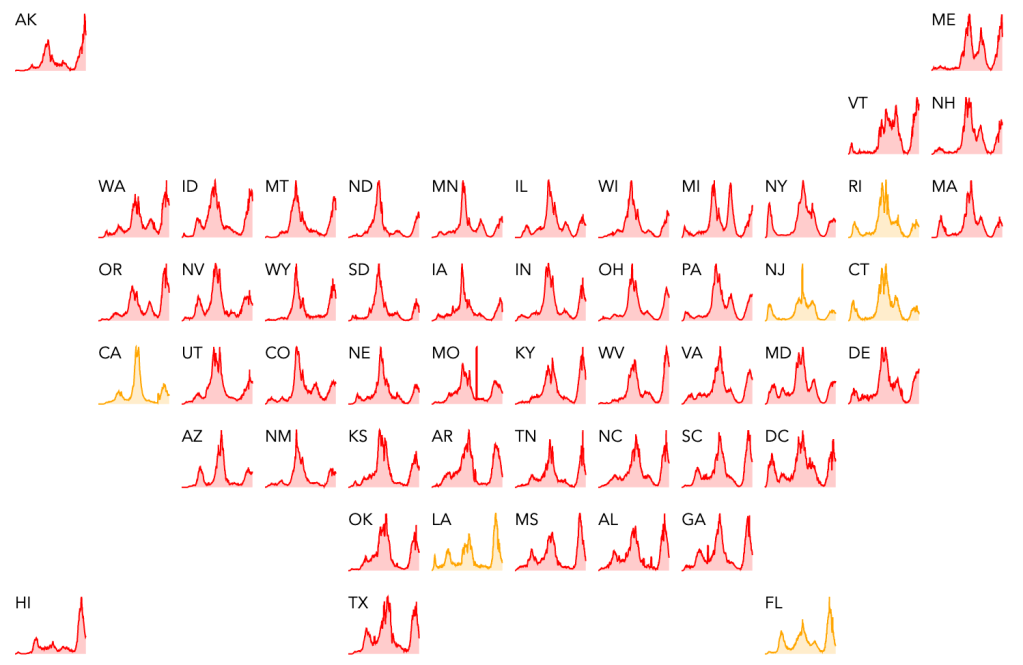
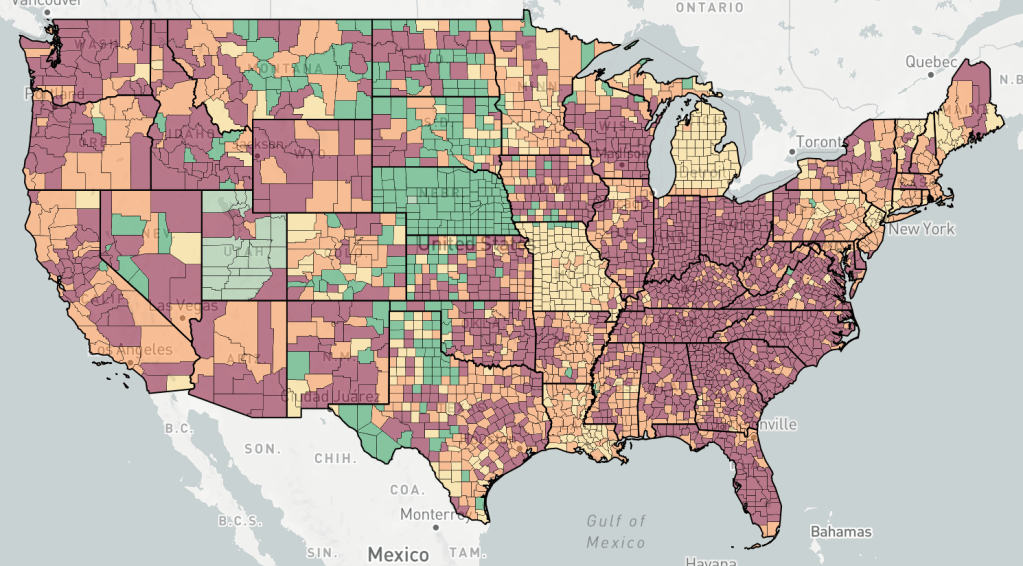
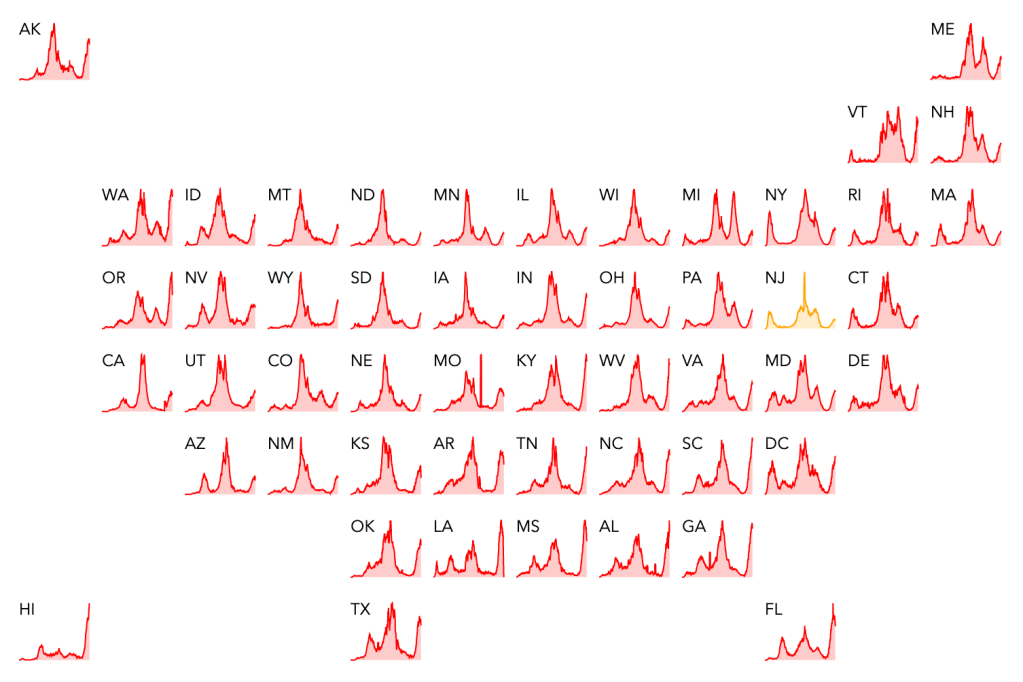
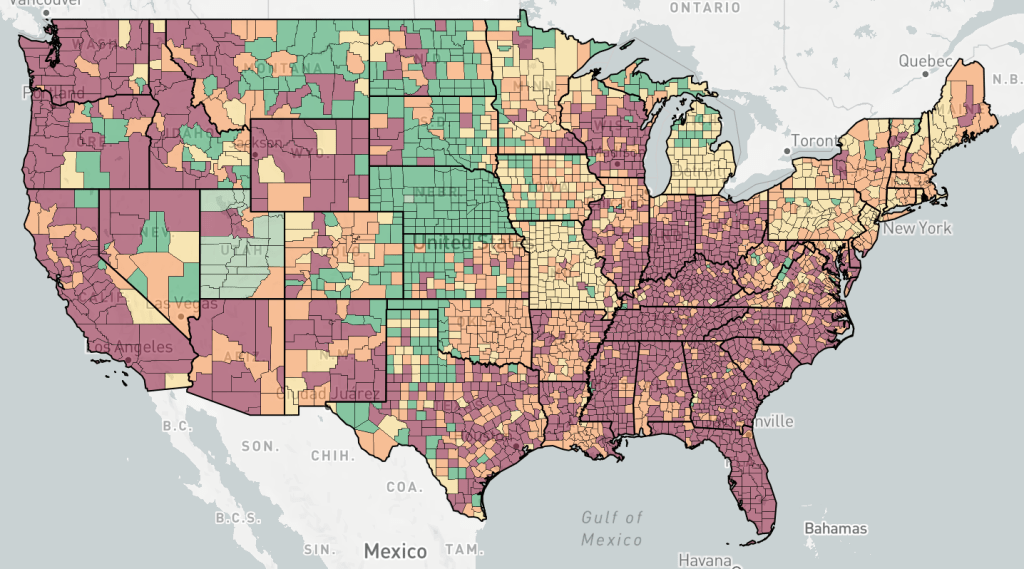
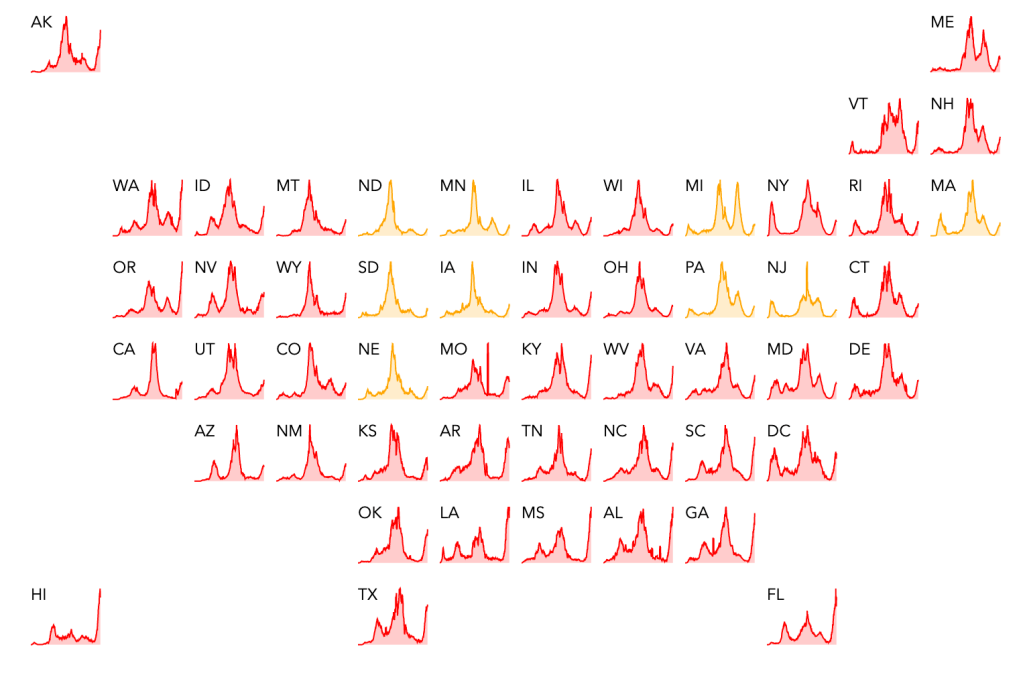
Endcoronavirus County Level Map, August 31st, 2021. New cases slowly receding in the South and growing in the North. Michigan, Missouri, Nebraska still appear to not have strong outbreaks as of now, likely because of large case numbers during the UK variant wave in the Spring of 2021.Endcoronavirus State Level Map, August 31st, 2021
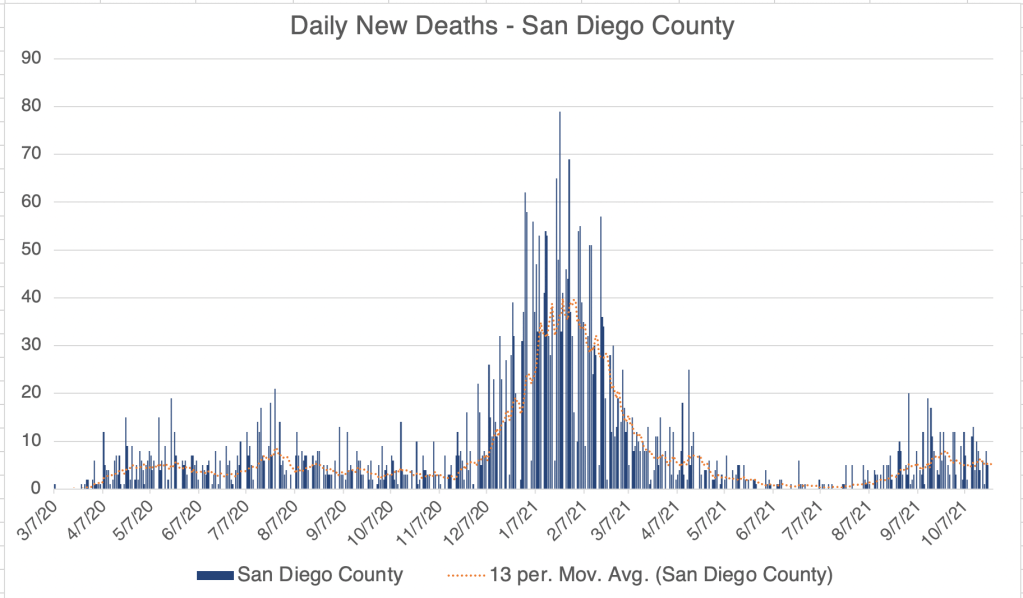
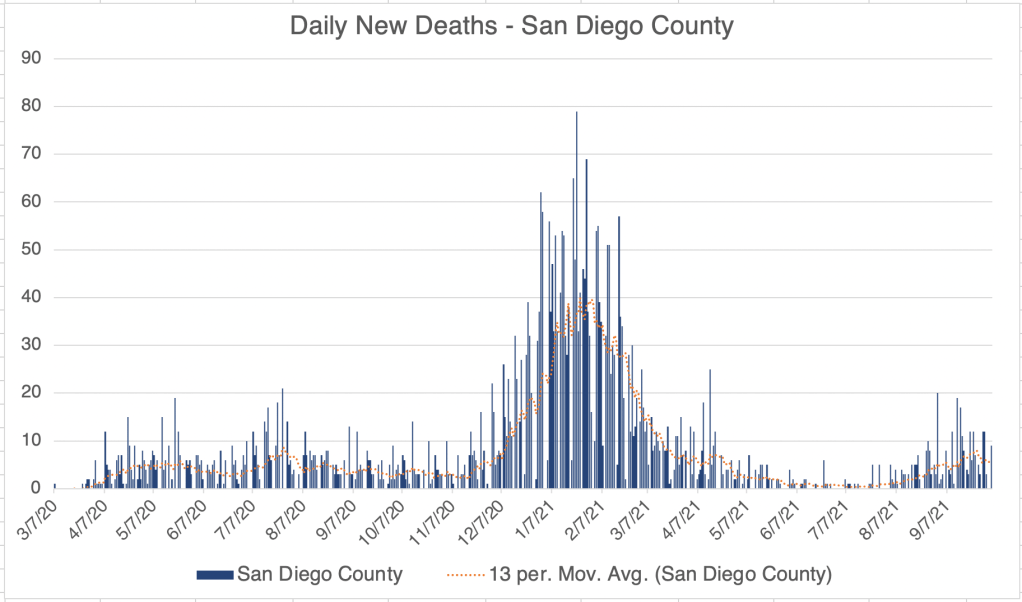
New cases continue to fall in California and San Diego. Tentatively, it even looks like deaths are falling as well.
The Pfizer vaccine recently received FDA approval. The confusing part, is that legally speaking, the approved vaccine is not the same legal entity as the Emergency Authorized vaccine. The Pfizer vaccine we’re used to is called “Pfizer-BioNTech COVID‑19 Vaccine”. The FDA approved one is called “COMIRNATY (COVID-19 Vaccine, mRNA)”. I’m not a legal expert at all, but my understanding from watching some legal analysis is that the original vaccine is still only EUA authorized, and has some liability protection for Pfizer. However, Pfizer does not have liability protection for the COMIRNATY vaccine. According to the approval letter from the FDA, the formulations of the 2 vaccines are the “same formulation” and “can be used interchangeably”.
So why the name change? An analyst I watched said that Pfizer would like to continue to use the original vaccine under the new approval, but avoid liability. So those getting the vaccine now would still be getting the vaccine with liability protection for Pfizer. If you want to get a 3rd shot, you may want to wait until the legally approved COMIRNATY vaccine is available. Again, I am not a legal expert, so my analysis may be wrong on this.
If all this is true, you may regard this as a dirty trick by Pfizer. I try not to be cynical about things that I have only a vague understanding of, but if you thought that, I couldn’t disagree with you.
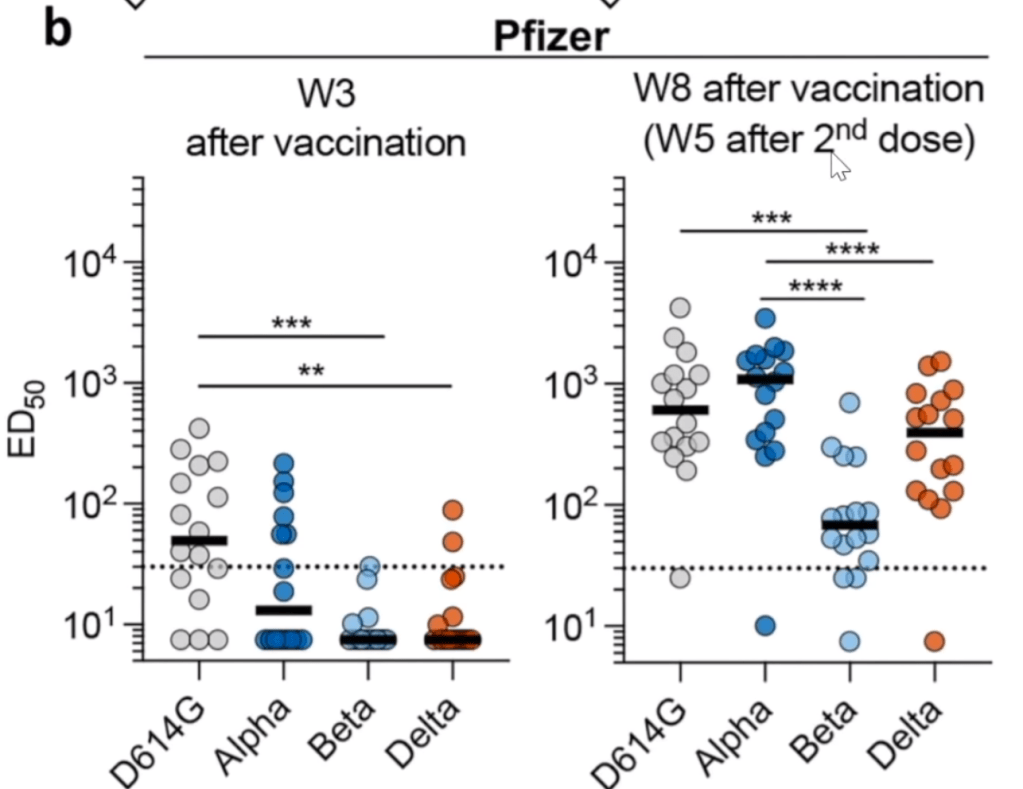
2nd shot improves protection against Delta, even for those with natural immunity. In a video by Dr. Roger Seheult, he argues that another shot greatly improves the immune response to the Delta variant. This follows both for those with only a single shot of the Pfizer vaccine, or with natural immunity. All this to say, if you’ve had COVID, 1 shot of a vaccine will help protect you from a breakthrough infection from the Delta Variant.
From Planas et al, 2021. Data suggests boosted binding of antibodies to Delta Variant after natural immunity (COVID infection) and 1 shot of the Astra Zeneca or Pfizer vaccine.From Planas et al, 2021. Data suggests boosted binding of antibodies to Delta Variant after 2 shots of Pfizer vaccine.
This post is detailed, but adds an important new set of facts regarding the Delta Variant, the current vaccines, and prospects for a new booster shot.
You may have heard commentators in the last few days talking about the reduced efficacy of the current set of vaccines. There has also been a lot of discussion about a study from Israel about relatively high numbers of Delta COVID cases among vaccinated individuals.
First a little background on antibodies. Your immune system is making a random set of new antibodies all the time. In an ingenious mechanism, your immune cells “mix and match” pieces of a gene in your immune cells, producing the ability to make a zillion (scientific language for a whole lot) of different antibodies. Your body is basically making different “keys” that can fit into the “lock” of some new protein.
When you get an infection, several different antibodies may bind to the invading agent, on different regions, so you may be protected by several different “keys”. When this happens, a bunch of different things happen, including the manufacture of Memory B cells which makes just the antibody that binds to a particular protein. These cells get activated if you get re-invaded by something with that protein. All this to say, if you’ve had COVID, or been vaccinated, your body will have B cells with antibodies on them that bind to different parts of the Spike protein.
Before I say anything else, I want to repeat that I have not been vaccinated, but have recommended that high risk individuals get vaccinated! I’ve also pointed out many times in the past few weeks that countries with large vaccination programs have lower death rates due to Delta than other countries!
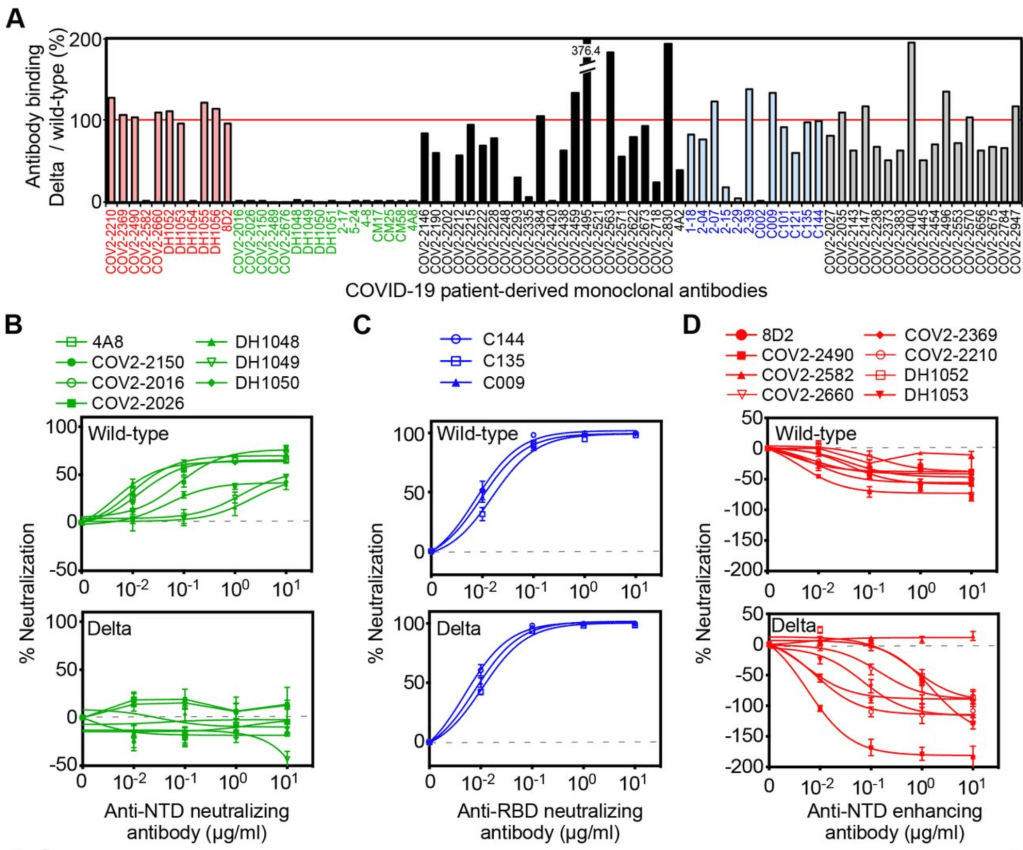
Literally 30 minutes after Thursday’s post on vaccine myths, a doctor friend of mine sent me a pre-print paper from a lab in Japan. Please note, this is a pre-print paper and has not yet finished peer review! The paper describes experiments using antibodies derived from patients infected with the Wuhan strain, as well as with the Delta Variant. They then studied binding of these antibodies to artificial viruses. The paper argues that Delta variant viruses are less neutralized by vaccines against “wild-type” or Wuhan strain vaccines. While the “wild-type” antibodies against Wuhan can neutralize a region of the Delta Spike protein called the Receptor Binding Domain (RBD) (Figure 1C), other antibodies binding to another region of Delta Spike protein actually enhance infectivity. Figure 1D from the paper shows negative levels of “neutralization” for antibodies that bind the N-terminal domain of the Spike protein. The paper calls this “enhanced”. Yes, this is the ADE I’ve been talking about.
They suggest that with rapid changes in COVID variants, a new version of Delta is going to be able to use the ADE pathway in the near future, when Wuhan era antibodies will no longer be able to neutralize a mutated Delta strain.
To sum that all up in simpler language, it basically says that Delta is more infectious because it is partially using the ADE method of infection. Future versions may be less prone to be neutralized by Wuhan antibodies, making them fully enhanced. If this happens, we may have more severe disease in those who get infected with this new enhanced Delta.
They conclude by saying a booster against the Wuhan strain will not be effective in improving protection from Delta, and that a new vaccine against Delta will be required.
The material in the paper may help to explain why we have been seeing lowering levels of vaccine effectiveness in some countries.
Just to be very clear, they are not saying that this new enhanced Delta exists now, just that it may exist in the future.
I will pay close attention to this issue. If you have already been vaccinated or had COVID, a new Delta vaccine will be your best defense against possible ADE arising from a possible enhanced Delta.
If an enhanced Delta arises, and you have had Wuhan COVID or a Wuhan vaccine, and you haven’t had Delta, then you may be at greater risk for severe disease.
If you have had COVID since July 2021, you are likely already immune to the Delta variant, and this will not be an issue for you.
I am fully aware this complicated. Also, the CDC has rarely if ever discussed this possibility, so unfortunately, most of the people you talk to about this will not believe it. I am sharing this with you so you can make wise decisions for you and your family.
Some companies are already working on Delta versions of the vaccine. If you have had the current vaccines, or had COVID, you should get the Delta vaccines as soon as they are available.
Of course, discuss your medical history with your doctor before making medical decisions.
Another note on misinformation:My post from last Thursday generated a lot of discussion regarding censorship and misinformation. I argued strongly that the dangers of misinformation do not outweigh the benefits of free speech. Many of you are pro-vaccine and others are suspicious of the vaccine. I would simply urge this:
1) If you use the words “misinformation” and “disinformation” in a post or in a discussion, please come ready with evidence to support whatever claim your making! Don’t just throw out this word, support it!
I recently saw a video with a pro-vaccine medical person saying “we just need to keep pounding this information into people”. That is the wrong approach. With someone who is not yet convinced to get a vaccine, “pounding” away on them is just going to raise their defenses and exasperate you. Instead, gently show them your reasons for believing what you do! Explain to them what the data means. You may not convince them, but you may move them toward being more open to your view.
2) If someone makes a claim that sounds unfounded or that you don’t trust, don’t just tell them they’re wrong or make a counter claim, ask them to provide evidence, or where they got their information. You don’t have to do their homework for them! If they can’t produce any evidence, you are under no obligation to counter it. I’ve saved myself A LOT of work with this approach. It’s OK that they just heard it somewhere IF their source is reliable and has evidence themselves. You can still ask them to provide you with a link or something to that person’s statement. However, “I just heard it somewhere” is not evidence.
Part of the reason I’m not so worried about “misinformation” for myself is because of my regular use of suggestion #2.
This is a case update. I’ll also briefly discuss the future of the pandemic.
Numbers continue to rise in the US, but are definitely slowing in their increase. New cases are most prominent in the West and Southeast. New deaths are rising, but much more slowly than for other waves.
For California and San Diego, it looks like we have crested the wave and new cases are starting to head down. In both of these regions, new deaths are not really increasing at all. This supports the pattern that in vaccinated areas, large numbers of new cases due to the Delta Variant are not followed by large numbers new deaths. I mentioned a few weeks ago that deaths can trail new cases by as much as 4 weeks, but we are now 6 weeks into the Delta Wave in California and San Diego without seeing a significant rise in new deaths.
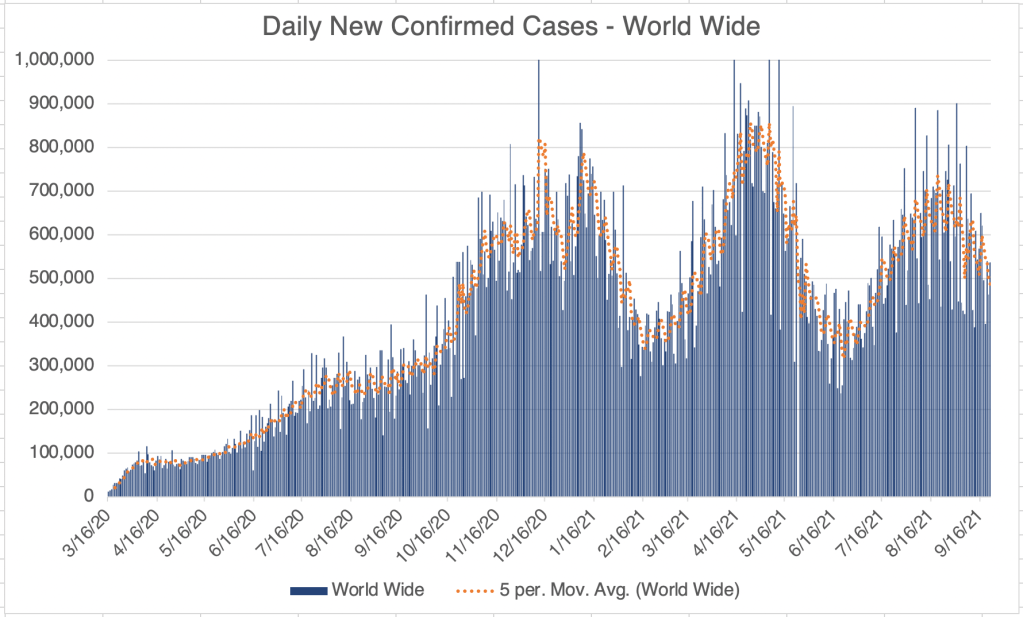
Internationally, new cases appear to perhaps have peaked world wide, but it will take some time to see if cases start to go down. As stated above, countries with vaccination programs are experiencing almost no new deaths due to Delta Variant. Numbers for the Netherlands are striking, and other countries like the UK, Sweden, Japan, and South Korea show a similar pattern.
Several sources I listen to are now saying that SARS-2 is now or will be endemic. For some background, an epidemic is an outbreak of a disease in a small area or region. Avian influenza and the first SARS outbreaks were epidemics, since they didn’t leave Asia. A Pandemic is an outbreak in a large area including several continents. A disease becomes endemic when it becomes a constant feature of life in an area. I would include malaria, seasonal flu, and HIV in the list of endemic diseases. Interestingly, Wikipedia still considers HIV to be a pandemic.
I have resisted calling COVID endemic. I don’t think it fits the criteria at this point. While there have been several new variants that have caused additional waves of cases, they are all at least partially impacted by the available vaccines, and presumably by natural immunity as well. While this is the case, I still think it is possible that we can eradicate the virus from the world at some point.When might SARS-2 become endemic? For me, that would happen if either new variants arose that were not mitigated by natural or vaccine driven immunity, or if immunity in vaccinated or naturally immune people ceased to be effective in preventing new infection. Both of these would allow SARS-2 to continue to circulate indefinitely.
Some have argued that vaccine mediated immunity is not as long lived as hoped. This may be why there have been many “breakthrough” cases in the last few weeks. However, Youtuber Dr. Zubin Damania suggests that while protected from new infection wanes over months, vaccine protection against severe disease is persistent, at least against the Delta Variant. This may explain our current pattern of low deaths despite high cases in vaccinated regions.
So is COVID endemic? I still say no, and hope it can be eradicated. However, some municipalities, including Norway and the state of Iowa, have declared that is endemic and will be a permanent feature of the world. If I decide that the data shows that SARS-2 is endemic, then that is the day that I will get vaccinated. ‘Cuz I do want to go back to normal life someday, but I don’t want to actually get COVID. Obviously, many vaccinated and unvaccinated folks have decided to go back to living normally, despite official calls to maintain vigilance.
Vaccination mandates: I have not been in favor of requiring vaccination in order to return to work, fly on commercial aircraft, or other activities. While I am all for precautions and continue to wear a KN95 indoors while in public, healthcare is a personal choice and should not be coerced. Some have even claimed that it is illegal to coerce a measure that does not have FDA clearance. While vaccination is a good choice for many, it does have liabilities that have made many resistant to vaccination. This should be honored.
I know several people in the healthcare industry who have not wanted to be vaccinated, and have quit or been fired from technical or nursing jobs. While an argument could be made that those working with patients should be vaccinated, it seems misguided to be letting go of nursing staff when there has been a long standing nursing shortage.