I’m going to share a brief update, and then give you some information on how my treatments work! In my private discussions with some of you, there is some curiosity about radiation, chemo, and the immunotherapy that I’m using to get well. So I thought I’d give some details on those things.
I also want to say before I start, that I’ve also learned from several of you that you are going through your own journeys with major health problems right now, including cancer. Know that I am praying for you! May God take care of you just as He has been taking care of me!
Update:
My first infusion was October 3rd. The nurse told us that the worst days were 4-10 days after infusion and she was right! I was miserable and wiped out the following Tuesday!
I’m doing much better now, and enjoying the break. My next infusion is this week, on the 24th. I’m half way done with radiation treatments on my primary tumor, and my last radiation is on November 8th. So my last 2 infusions will happen after radiation is over. So this next one will likely be the worst, but the last 2 infusions are likely to be easier than the first 2!
My last infusion is on December 5th, and I’m looking forward to feeling much better in December. Hopefully by Christmas, I’ll basically be back to normal.
My pain is low enough now that I’ve started to work myself down from the opioids, which is lowering some of the negative side effects from an already low dose. The doctors are pleased at this news! I’m also able to eat more, so I’m working on gaining some weight.
We are so thankful for the support of friends and neighbors that we continue to get. Your prayers have been an important part of my progress, so keep it up!
Radiation:
Radiation is a common cancer treatment because it’s less invasive than surgery, but it’s still quite effective at killing cancer cells. It works by damaging the DNA of cancer cells, leading to the self-destruction of the cells.
X-ray radiation is the most common. An emitter looks like a giant microscope and moves around the patient, firing hundreds of X-ray beams in sub-lethal doses. Only the tumor receives a lethal dose of X-rays. The CT scan measurements are exact and treatment plans are done by a physicist for each patient. In fact, a physicist and doctor need to be present and approve how the machine is lined up with the tumor every day before they start the radiation treatment!

Inside the instrument, an electron beam is created by a cathode ray tube, much like the ones that used to be in the old tube televisions. The electron beam strikes a tungsten plate The electron beam is absorbed by the plate and transformed into X-rays that are emitted by the tungsten plate. These X-rays then pass through a lead aperture that shapes the beam into just the right configuration for the shape of the tumor at that angle. This aperture is made of lead “leaves” that actually move to shape the beam as the emitter moves around the patient. Yes, I can actually see the aperture changing shape as the emitter moves around me!
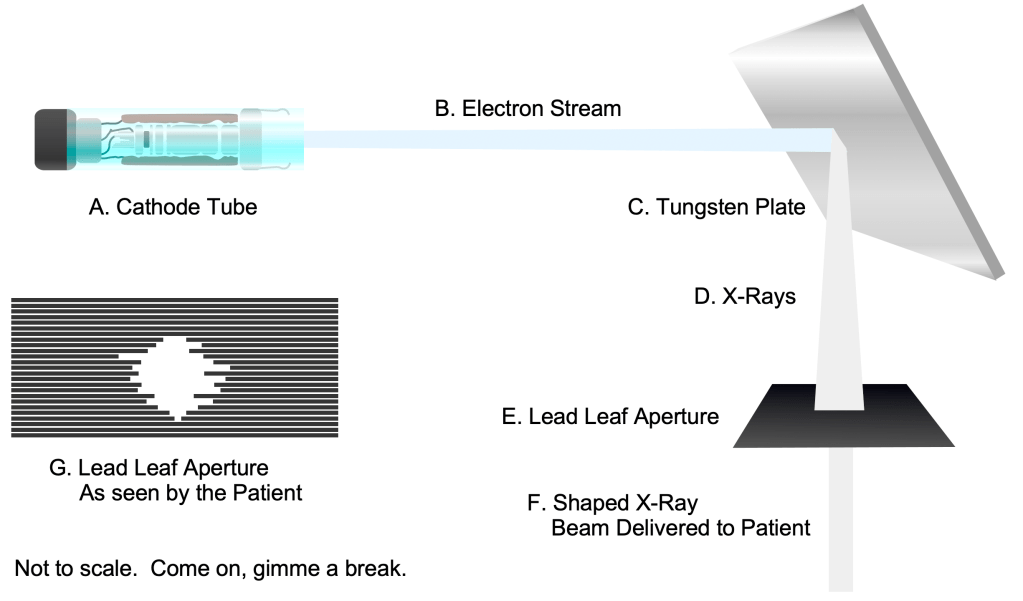
These X-rays then pass through a lead aperture (E) that shapes the beam into just the right configuration (F) for the shape for the tumor at that angle. This aperture is made of lead “leaves” (G) that actually move to shape the beam as the emitter moves around the patient.
Yes, there is a risk that the X-rays themselves will cause a new cancer tumor to form, but the likelihood is that if one does, it will take many years for the new tumor to cause a problem, after the patient will have passed away from natural causes.
Proton beam radiation is much less common and much more expensive than X-ray treatment. Protons can more easily be concentrated on the tumor and are less likely to cause a new tumor. For these reasons, proton therapy is more commonly used on younger patients, to avoid the likelihood of producing a new tumor within the patient’s lifetime.
Chemotherapy:
Normal human cells have many molecular checks to their growth, making sure the cells don’t get out of control. Cancer cells have mutations that turn off these checkpoints. This is why cancer cells grow rapidly and can become dangerous. Chemotherapy agents selectively kill cells that are growing rapidly. Since cancer cells are growing very rapidly, chemotherapy agents kill them first. Unfortunately, some normal cells in the body grow faster than others, like hair, gut, and blood cells. This is why patients can lose hair, experience nausea and digestive problems, and suffer from low blood cell counts, or even become immunocompromised.
The good news is, on balance, chemotherapy is usually very effective at killing cancer cells, and many people have been saved through the use of these agents.
As I said in my first 1st update, Next Generation Sequencing (NGS) testing can help doctors know if a patient will need to use certain chemotherapy agents. My tumors don’t happen to be particularly interesting in this regard, so I’m just getting a “normal” first try set of chemotherapy agents. NGS has definitely increased the survivability of cancer by helping chemotherapy work on the first try!
Immunotherapy:
The PD-1 protein exists on the surface of certain T and B cells of the immune system. They work to inhibit the function of these cells in most conditions, making them tolerate “self” cells in the human body, helping to prevent autoimmunity. If a person has cancer, “turning off” these proteins can make these T and B cells no longer recognize cancer cells as “self”, and attack them! Immunotherapy agents like Keytruda inhibit the PD-1 protein, causing the immune system to attack some tumor types, like the cancer I have, non-small cell lung cancer.
Prayer requests:
I’m doing much better eating, and my goal is to maintain my weight through the next round of chemo, and to gain some after that. Pray that I will be able to eat enough calories for that! Thanks!
Don’t fear, but be smart!
Erik
If you want to subscribe to these posts, click on the “Subscribe” link on the lower right corner of this page. The link will also appear if you start scrolling up from somewhere in the middle of the page.