Here’s a brief case update. I’ll also have a brief comment about vaccine mandates.
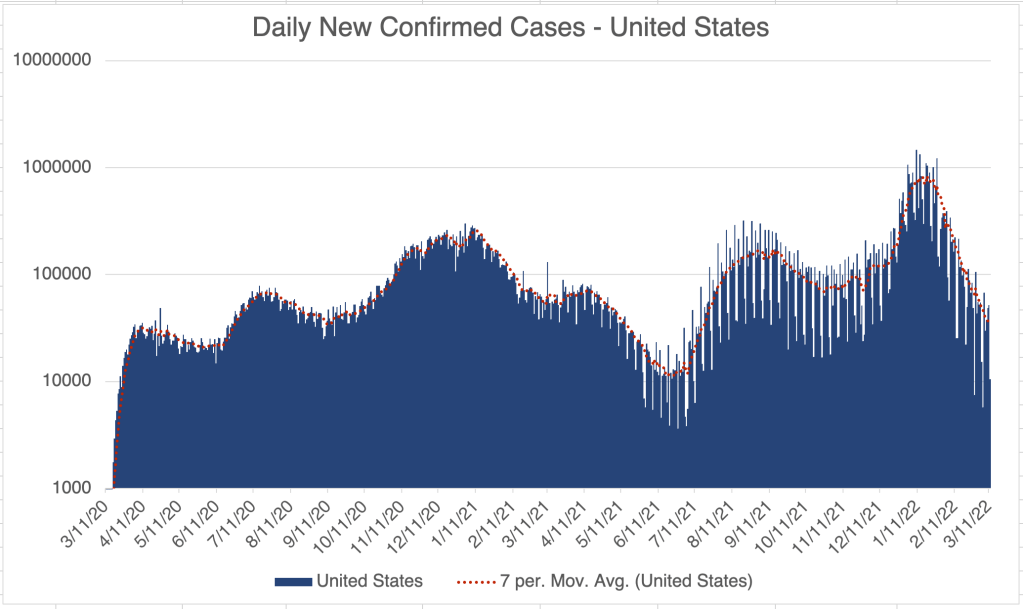
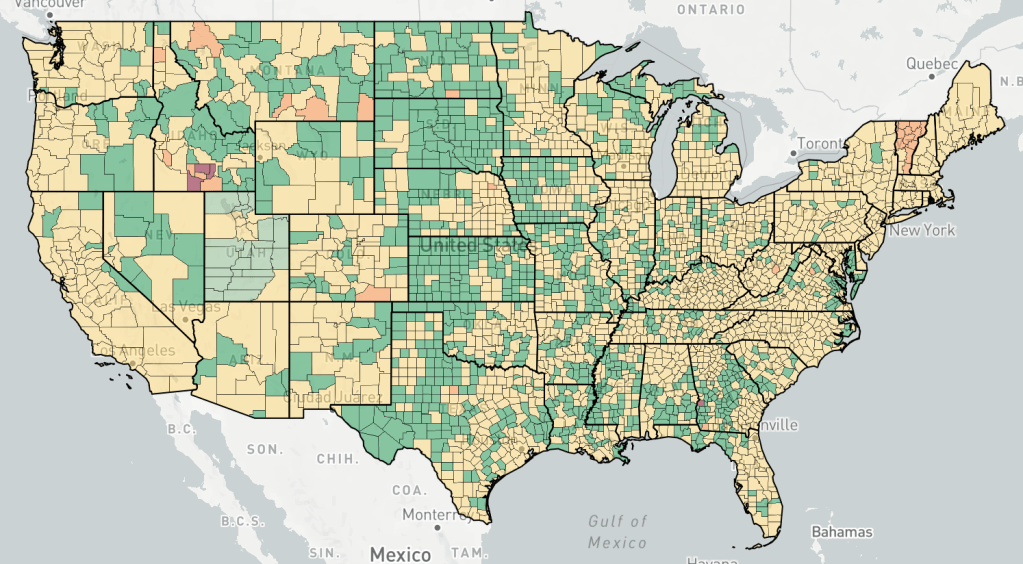
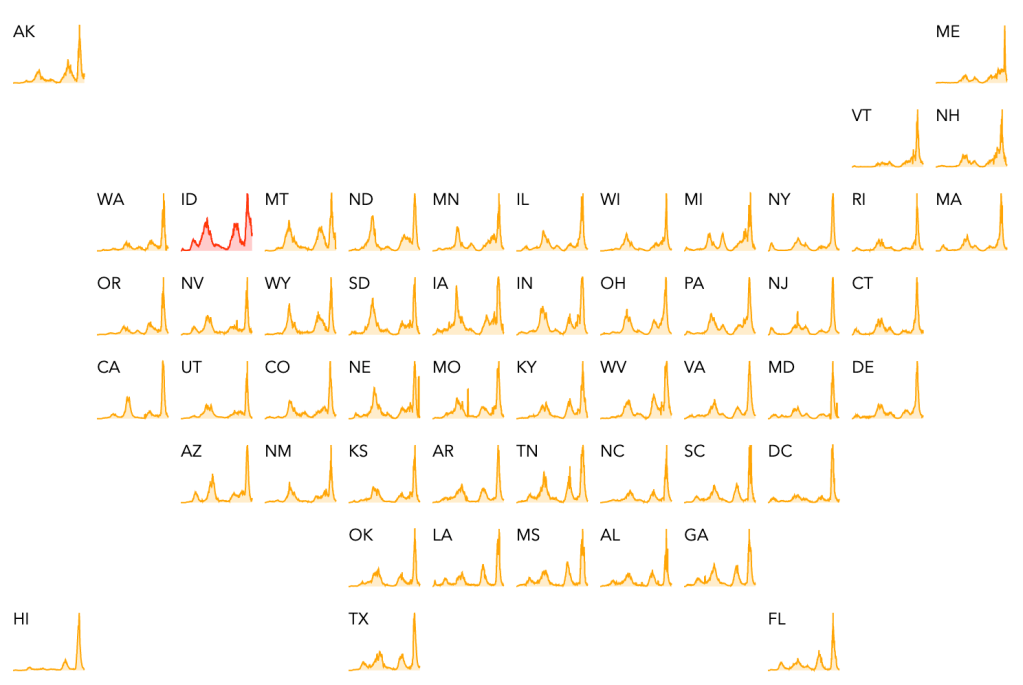
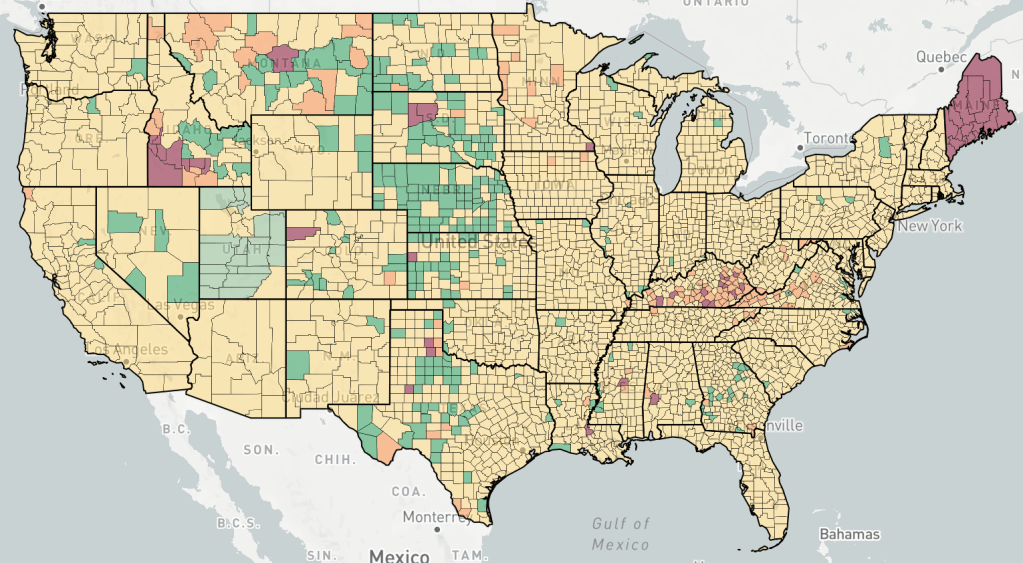
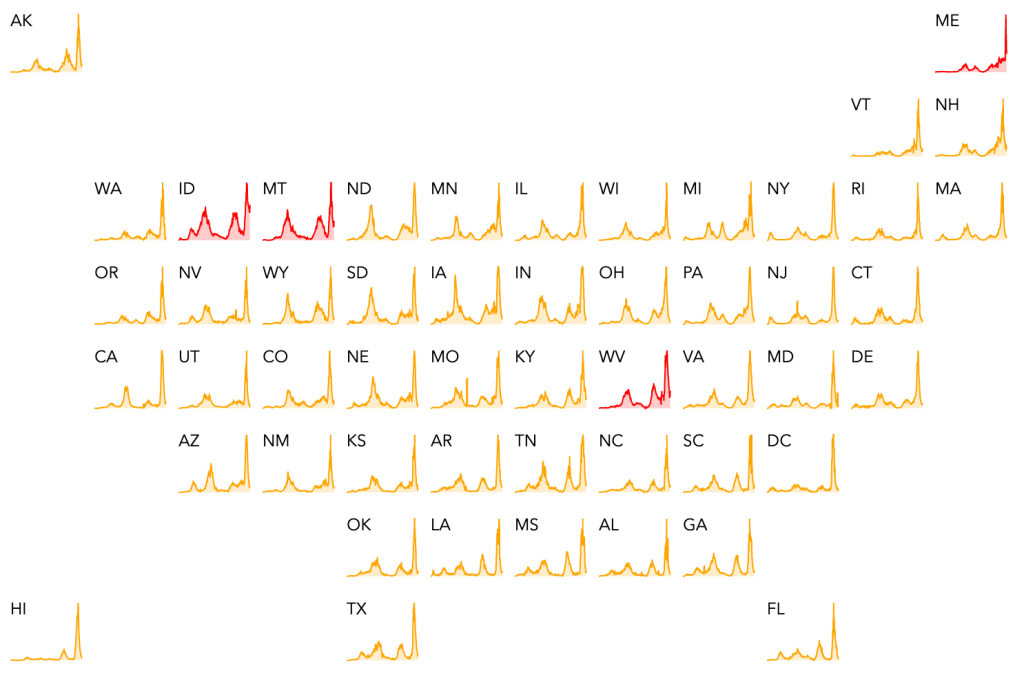
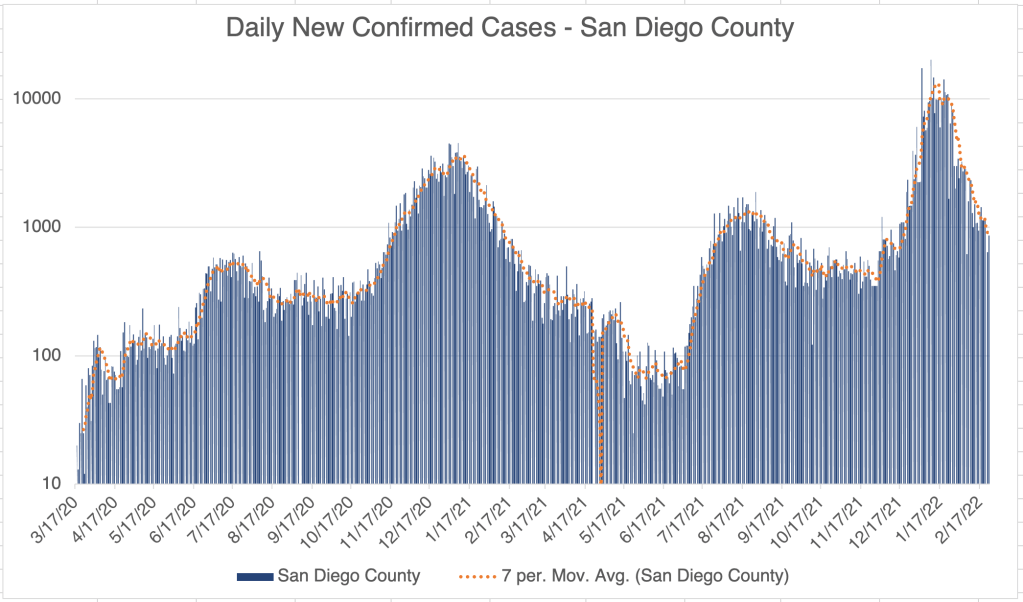
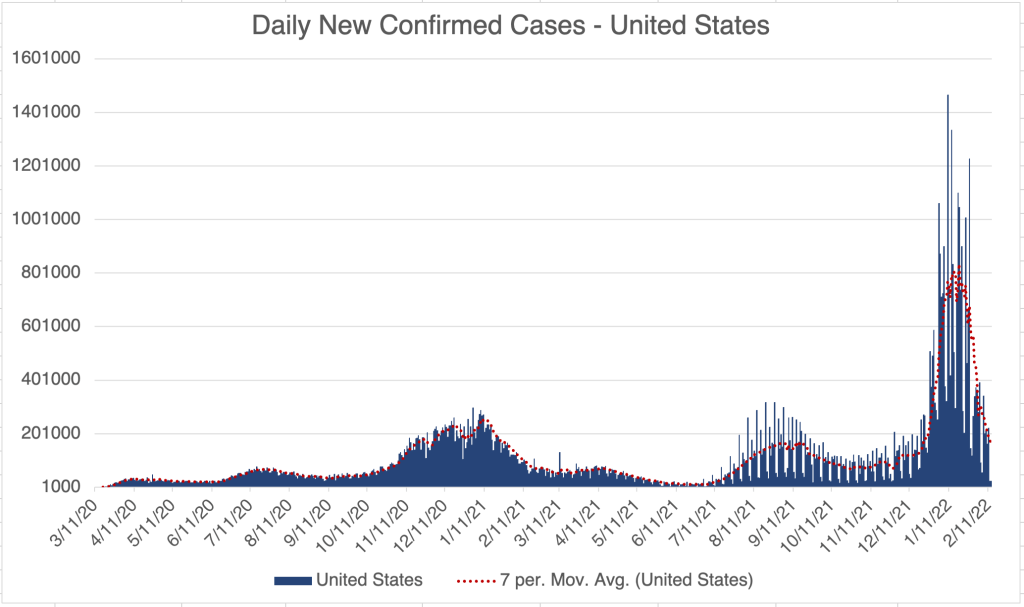
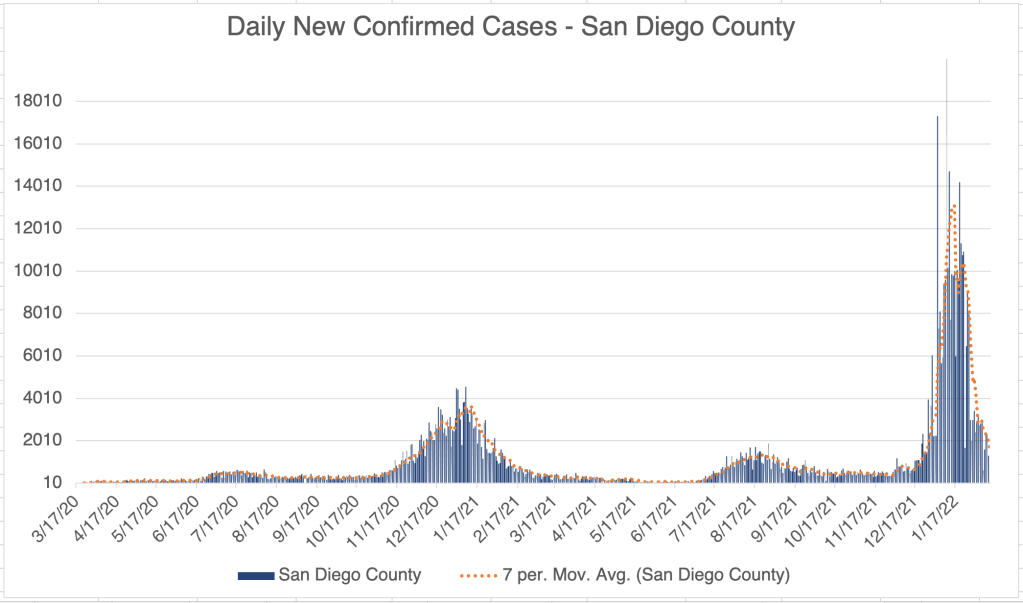
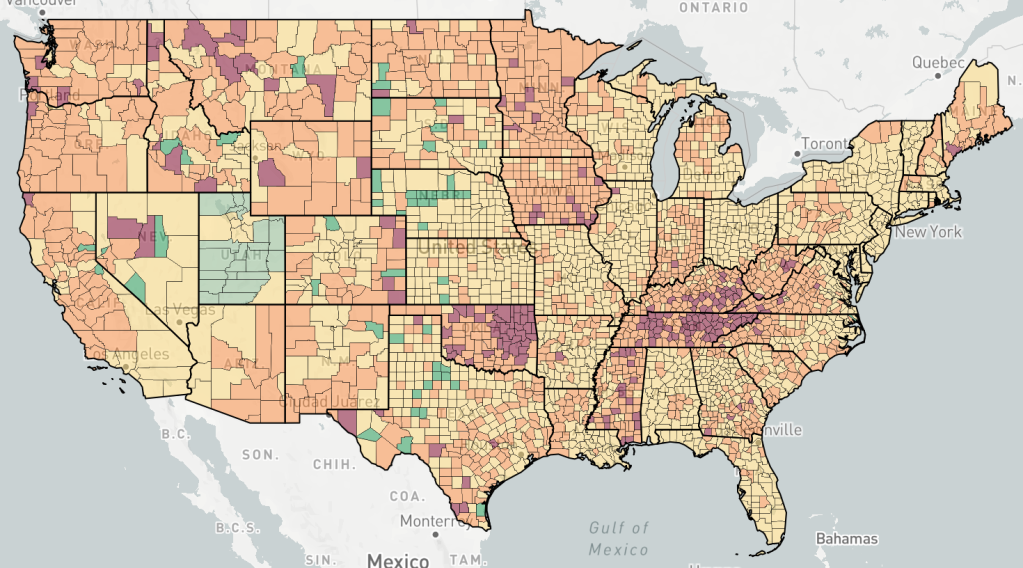
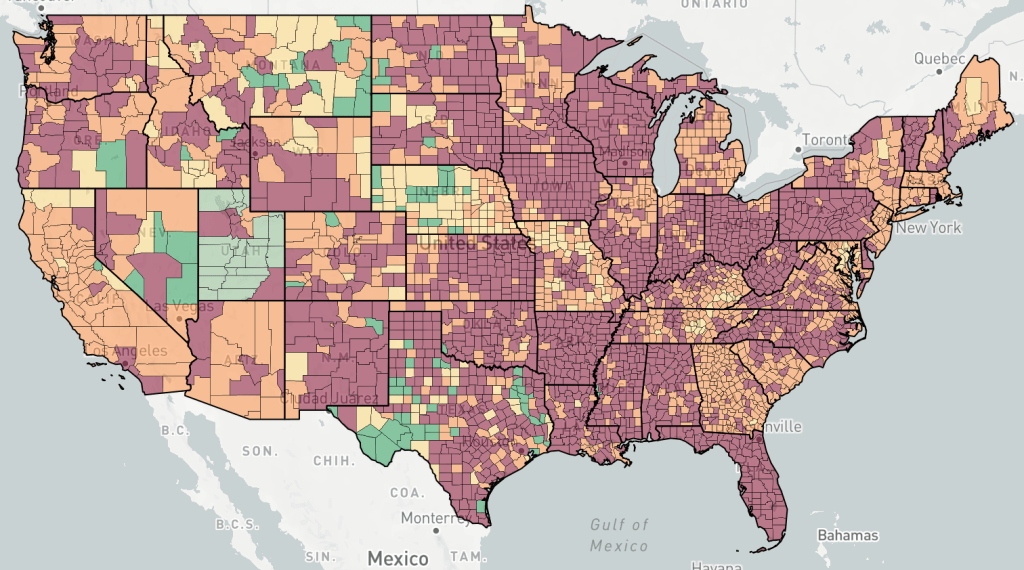
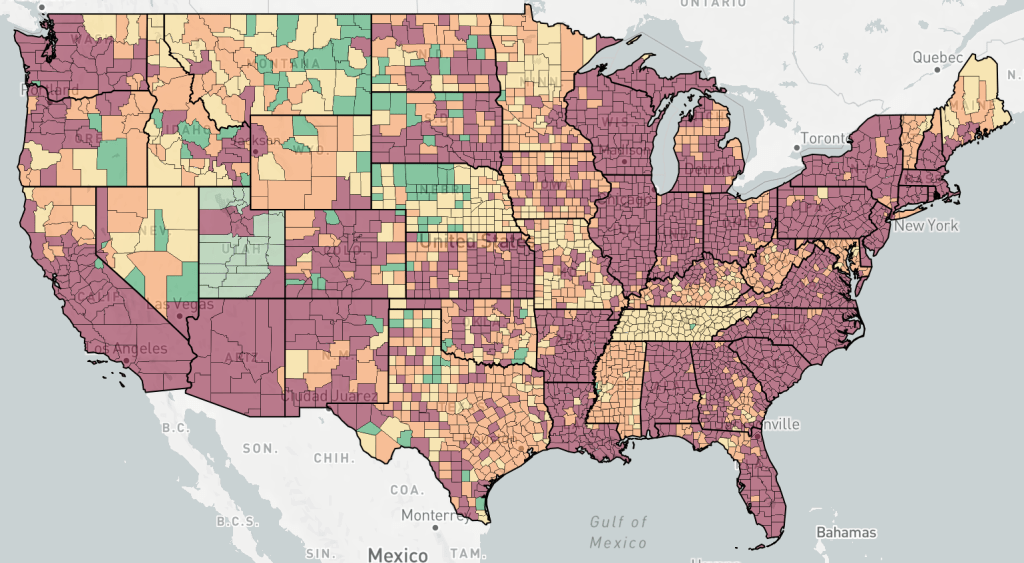
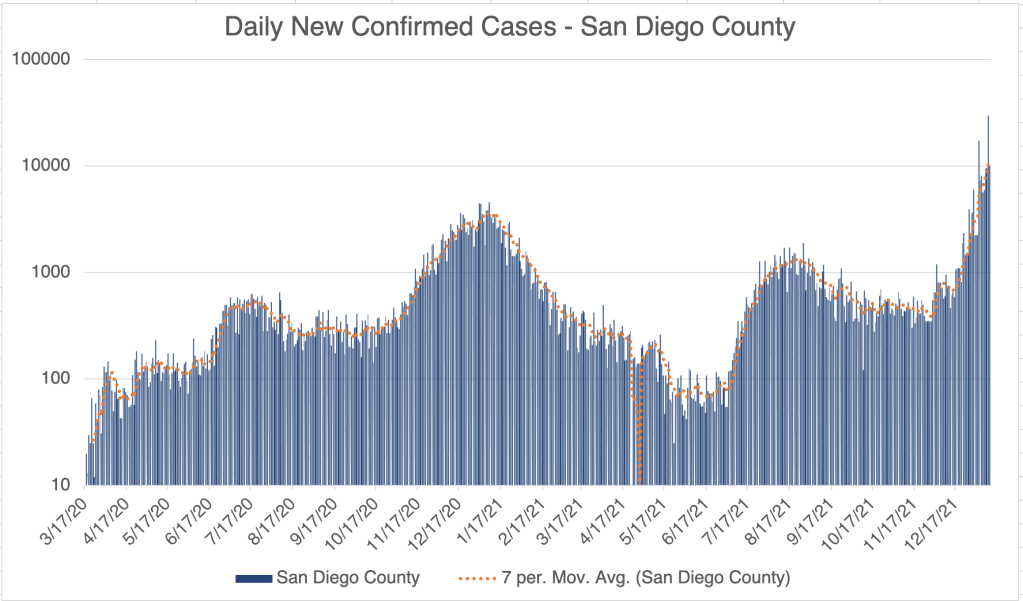
Cases continue to come down in the US, California and San Diego County. Cases in the US are now approaching being as low as they were in the Spring before Delta started. The only current outbreaks, according to endcoronavirus, is in the Twin Falls area in Idaho. Cases are dropping in San Diego County too, but unfortunately, not as fast as other places. LA and San Diego Counties are now #1 and #2 for new case numbers in the US.
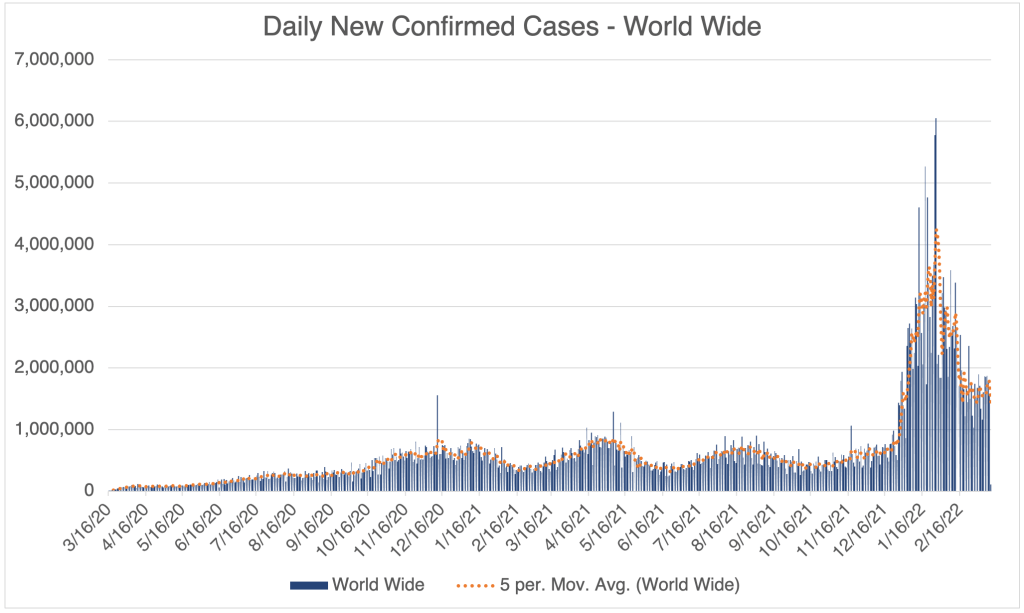
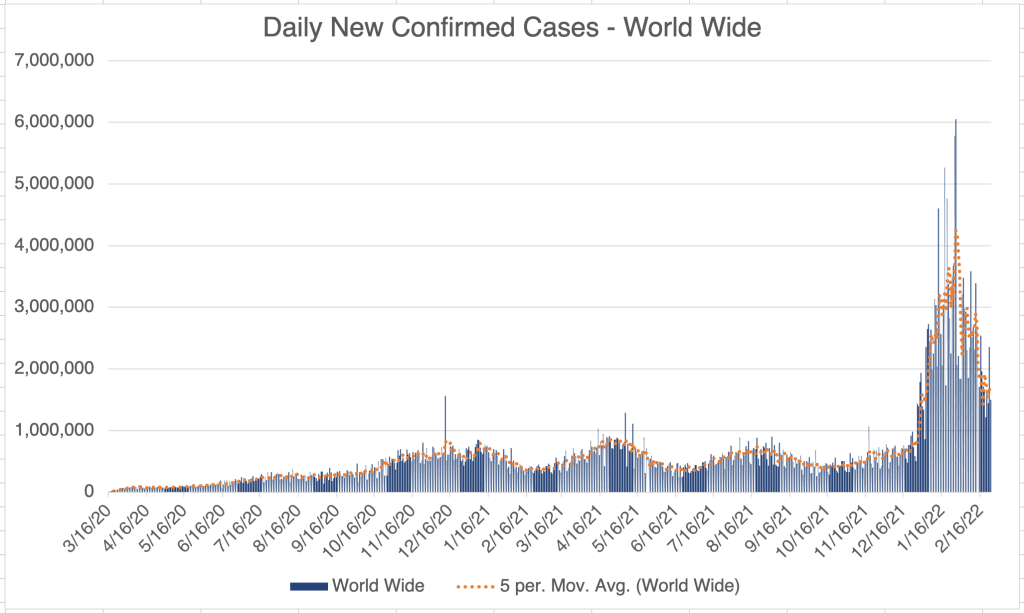
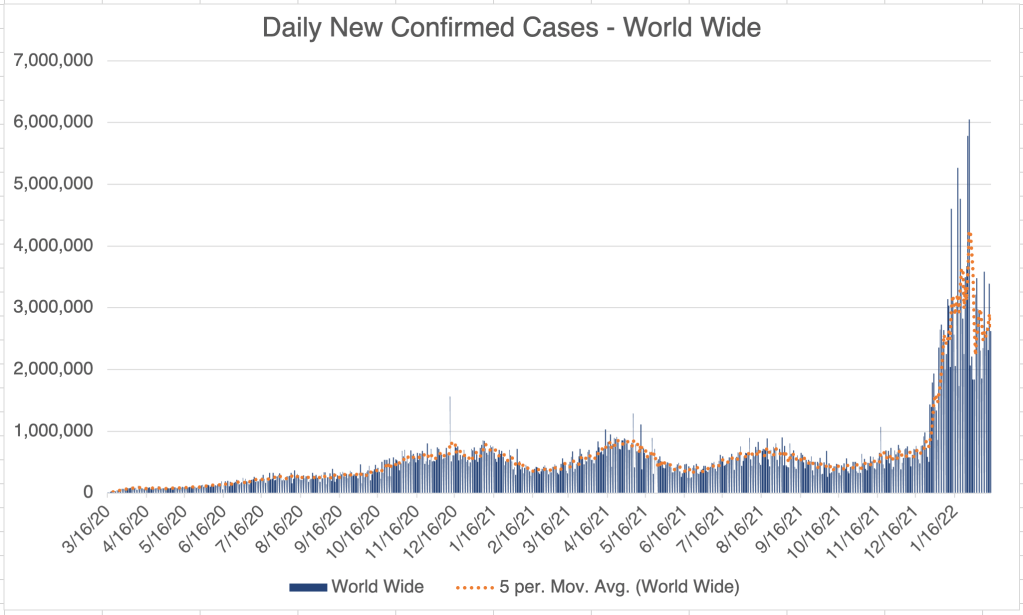
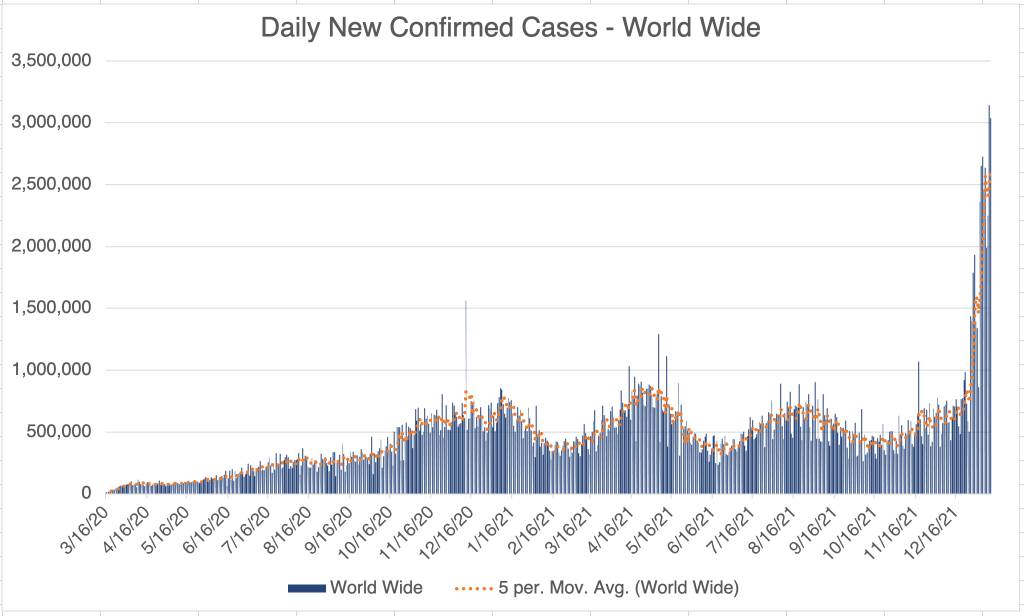
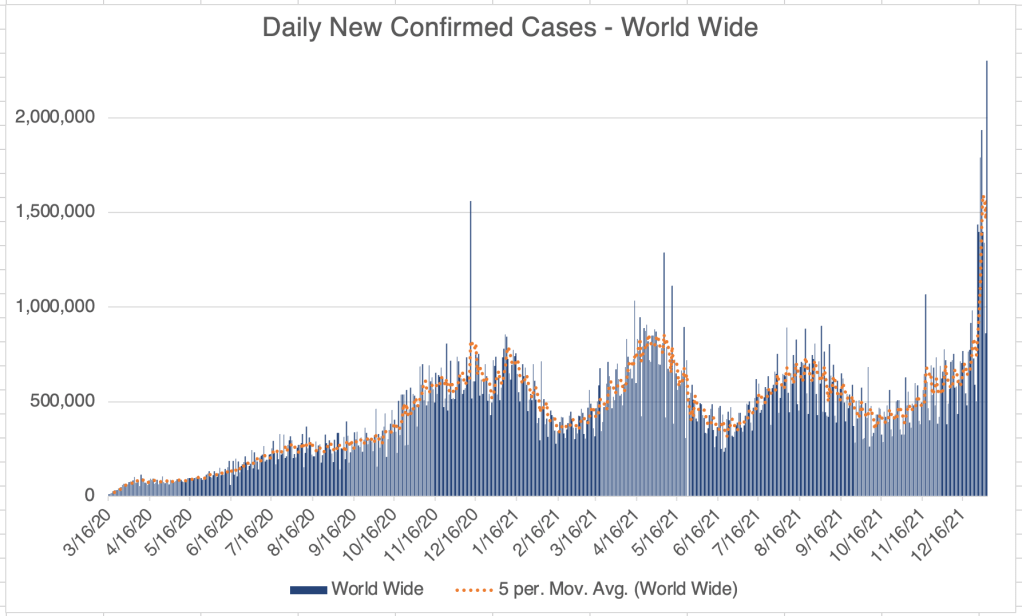
World wide, the US is now in 8th place for countries with the most new COVID cases in the last month. This is a welcome change, since the US has spent large majority of the pandemic in 1st place. Ironically, the country in first place right now is South Korea, which has been doing well for the majority of the pandemic, serving as an example for other countries to follow. The majority of cases country wide have happened in the last month, due to the super infectious but less virulent Omicron variant.
Vaccine mandates still enforced: In January 2022, the Supreme Court struck down the vaccine and testing mandate for all but a few health care workers. Mandates for federal workers are still working their way through the courts. In spite of this, some companies and municipalities are still enforcing the mandates. They often cite vaccine mandates, but the vaccine mandates still do not officially exist, having been struck down. So these entities are enforcing mandates entirely on a voluntary basis, and of their own volition. These entities do not acknowledge the now well known data that natural immunity is better than vaccine mediated immunity at preventing infection and the spread of SARS-2.
As you may have noticed, I’ve been tapering off the frequency of my updates as the pandemic recedes. As things continue to improve, I will post more infrequently.
I have a brief case update today. I’ll also do some more complaining about the CDC, with some vindication from other sources. I’ve complained about them a lot before, so if you’re not interested in more complaints, you can skip the last part of the post.
Cases are still coming down in the US, California, and San Diego County. Cases are about as high in the US now as they were in November, before the Omicron variant appeared. They are still not as low as they were in late June and early July, when the vaccines had been released to everyone, but Delta had not yet ruined the party. Things are improving greatly, and I’m enjoying going out with my new hard won immunity, but the pandemic isn’t over quite yet.
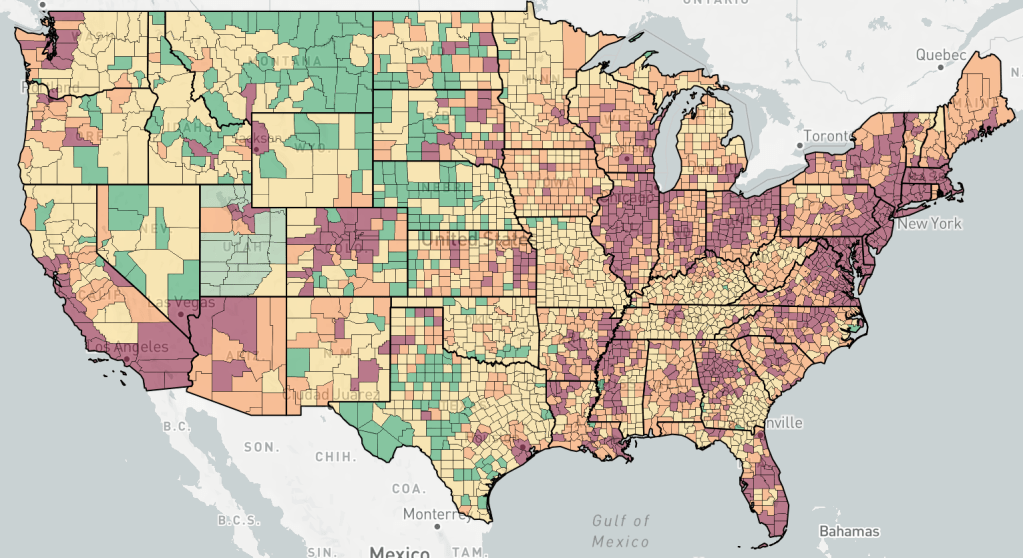
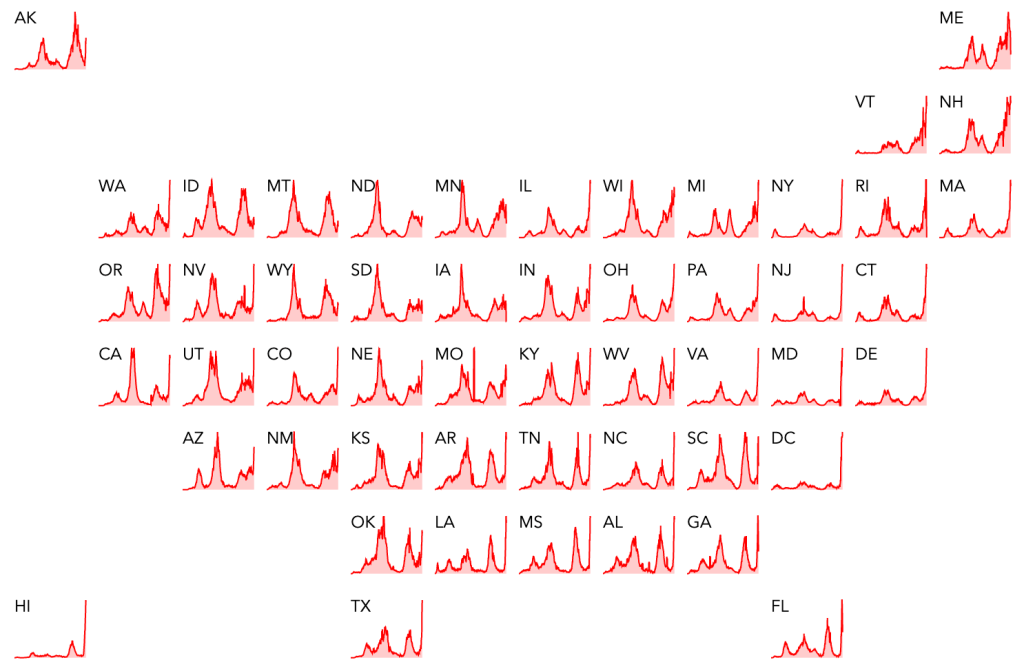
A brief look at endcoronavirus state and county level maps shows that Maine is having an outbreak right now. Looking at a higher resolution graph, the outbreak is actually already over, and cases are dropping again. This may be a real outbreak, but it may also reflect reporting practices in Maine.
Trouble at the CDC: If you’ve been reading my posts, you know that I regard the CDC as one of the main villains of the US response to the pandemic. I don’t have enough data to say that they intentionally under performed, and most pundits I’ve heard chalk this up to simple incompetence. Early on, they basically agreed with whatever the WHO said, even though is was clear that the WHO was repeating Chinese government talking points. Later, I assumed that their slow release of information was because they were just very careful, waiting until there was certainty before releasing information that was already nearly obvious to everyone.
Later, however, things took a dark twist. As useful papers began to come in from other countries like Japan, South Korea, the UK, Israel, South Africa, Sweden and Denmark; Morbidity and Mortality Weekly (MMWR) and Emerging Infectious Diseases (EID), the CDC’s own journals, produced very few useful papers on the pandemic. This despite the fact that the CDCs mission, it’s only job, and supported by 11,000 employees, is to produce information and guidance on the prevention of infectious disease. They don’t even have to implement or enforce their recommendations. The federal and state governments do that.
Then OSHA produced it’s official vaccine mandate. On the FAQ page, OSHA waived the requirement that employers must report adverse events from the COVID vaccination of it’s employees. They explicitly state that “OSHA does not wish to have any appearance of discouraging workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers’ vaccination efforts.” Yes, as of today, February 25, 2022, this ridiculous and damning statement is still on their website. Many have been suspicious that the CDC has not been diligent in collecting data for the Vaccine Adverse Event Reporting System (VAERS), but it was hard to prove it. The statement from OSHA confirmed that the CDC was intentionally blinding itself to data that would help answer questions about the vaccines.
While the vaccines have certainly been helpful in reducing COVID severity and deaths for many, it is suspected that thousands have died directly from the toxic effects of the Spike protein in the vaccine, and many thousands have suffered long term negative health effects. Only recently did a CDC paper admit that natural immunity was better than vaccine mediated immunity, even though that has been known for months, thanks to an Israeli paper.
The New York Times has been supportive of the CDC for much of the pandemic. However, on February 20th, 2022, the Times published an article claiming that the CDC has been withholding information from the public. Better late than never, I suppose. Data withheld includes hospitalization rates for various categories including vaccinated individuals, and the effectiveness of boosters for those younger than 50. Unfortunately, the author says that this is likely only a fraction of the information the CDC has been sitting on like an egg. When asked why so much information had been withheld, a spokesperson said it was because they feared the data would be misinterpreted. This from 11,000 people we pay to communicate to the public.
The United States is the third most populace country in the world, and we have 53 separate approaches to pandemic. The CDC has or could have had a wealth of data that could provide science based guidance to the world. Unfortunately, it appears to me that they have mostly been motivated to sell vaccines, rather than to serve their central function.
FDA corruption: In the meantime, Project Veritas released 2 videos featuring an FDA official revealing corrupt relationships between the FDA and the pharmaceutical companies. These relationships influenced regulation of COVID treatments.
What should be done about the CDC: In general, I’m not for abolishing things willy nilly. I will say, however, that the CDC needs top to bottom review and serious reform. The Director as well as much of senior leadership should be fired. Will any of this happen? Not for the foreseeable future. The CDC is empowered by Congress and overseen by the Executive Branch. Members of Congress are typically motivated by political considerations more than by producing sensible policy. I know I’m stating the obvious. Only when Congress changes will reforms happen. I will also point out that members of all political parties are prone to being absorbed into the Washington Hive. So vote carefully in primary elections! Do your best to select honest people to Congress, and don’t forget to vote local too.
This week I’ll have a case update, then discuss variant BA.2, and Dr. Fauci’s announcement about the end of the Pandemic.
Cases in the US, California, and San Diego County are all still going down sharply. Cases are now at the same level as in mid-December. According to Endcoronavirus, most states have decreasing cases.
Variant BA.2: This new variant is now increasing slightly over the original Omicron. This is no reason to be concerned, however, since BA.2 is just a slightly more infectious version of Omicron. Antibodies against Omicron are expected to be effective against BA.2, so this does not represent a new variant that will cause case numbers to rise.
Dr. Fauci announces the end of the Pandemic: In an article in Financial Times, Dr. Fauci stated that he expects that the pandemic phase of COVID will be over in the next few months. I agree, with the exception that I think a reasonable time frame is more like weeks than months.
He also stated that he thinks boosters will continue to be necessary to keep the virus at bay. On this I have to disagree. The vaccines had a minimal impact on new infections due to Omicron, although they probably had a positive impact on disease severity. Given that the new cases are now very low, and the unknown but real danger from adverse reactions, I think there is now almost no reason to get a vaccine booster. For vaccines to continue to be useful, we need a more current version, against something like Delta or Omicron. I don’t expect we’ll be getting that.
Many scientists, including those I respect, think the virus will become endemic, meaning it will continue to circulate at a low level in different forms basically forever. With some trepidation and perhaps over-optimism, I think Omicron will eventually peter out and SARS-2 will be over. We’ll see if that happens.
Just a brief case update today. New cases are still dropping fast in the US, California, and San Diego County. Cases are now about as many as their were just before Christmas when the Omicron wave was just starting in the US.
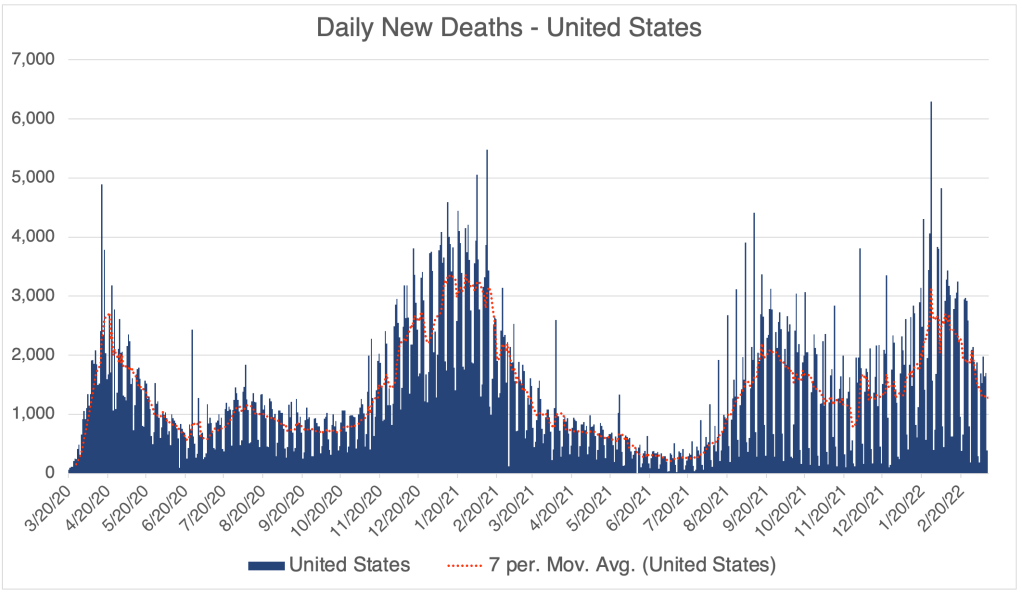
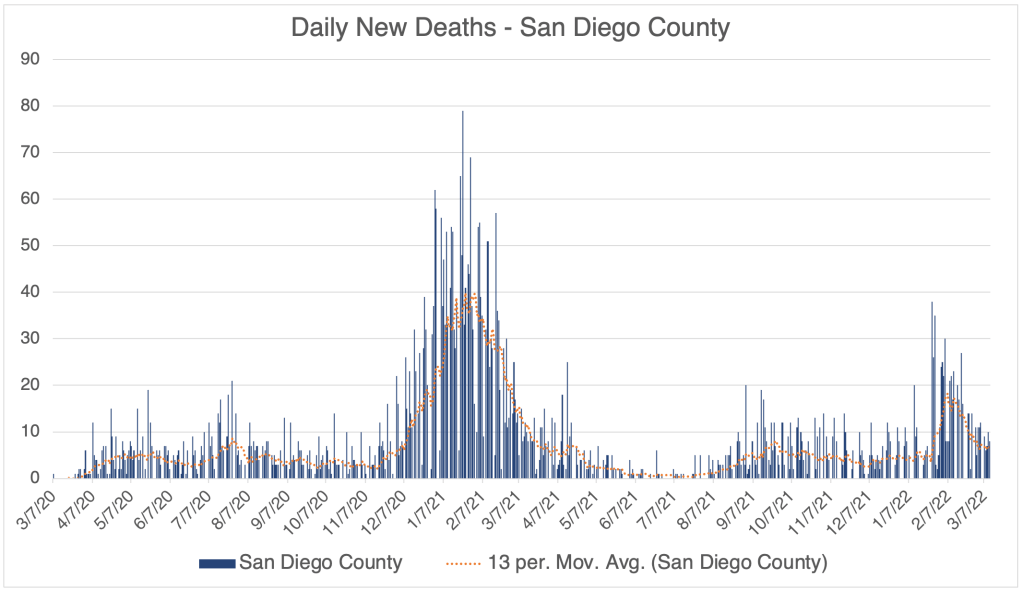
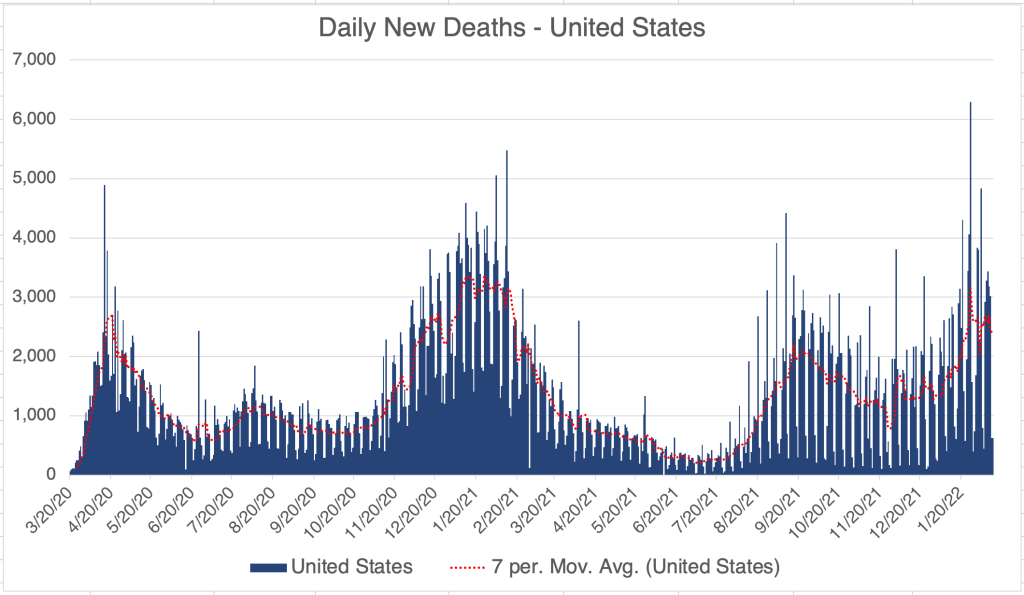
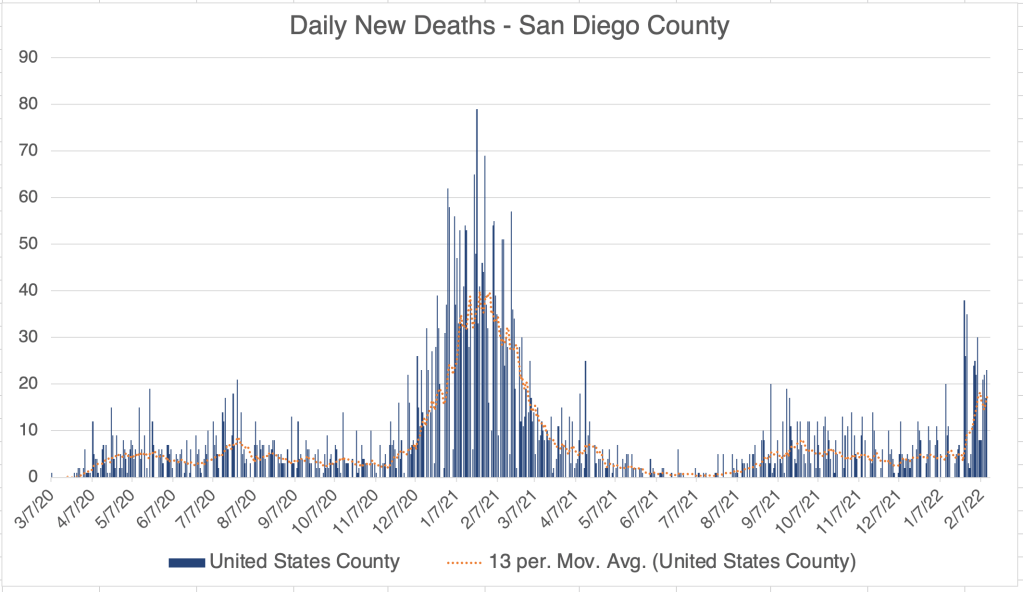
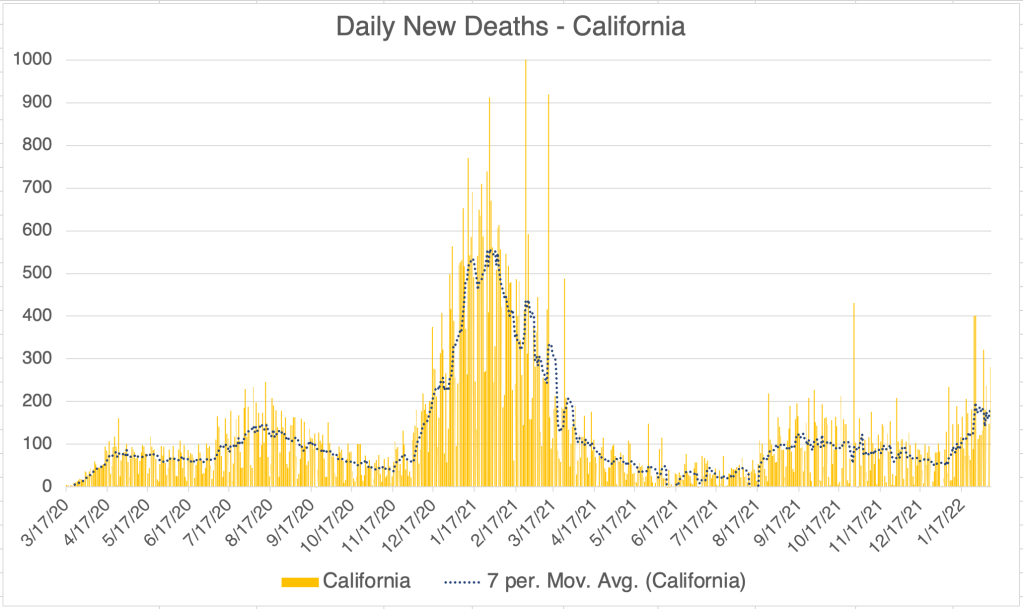
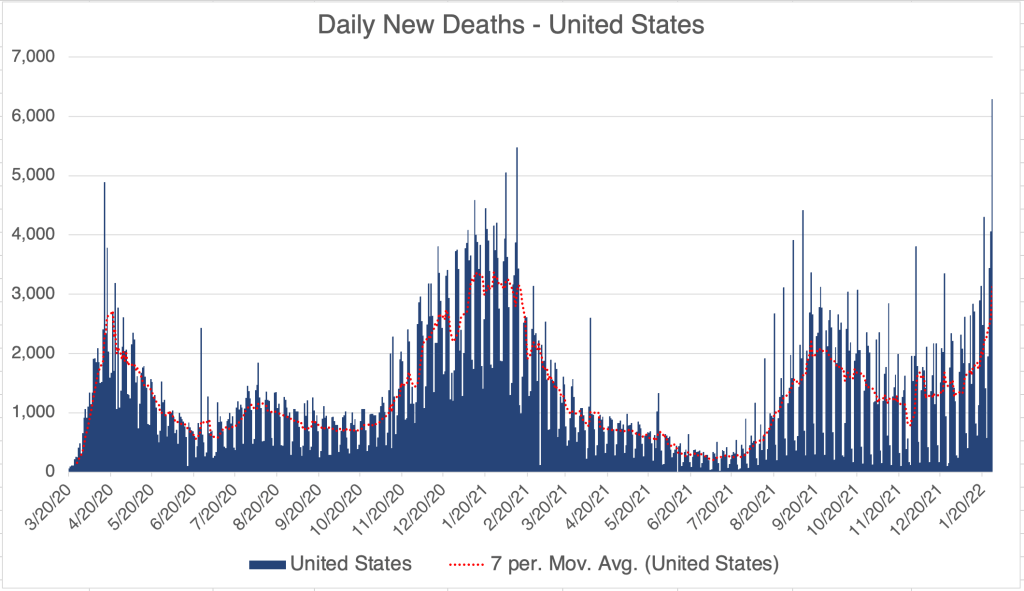
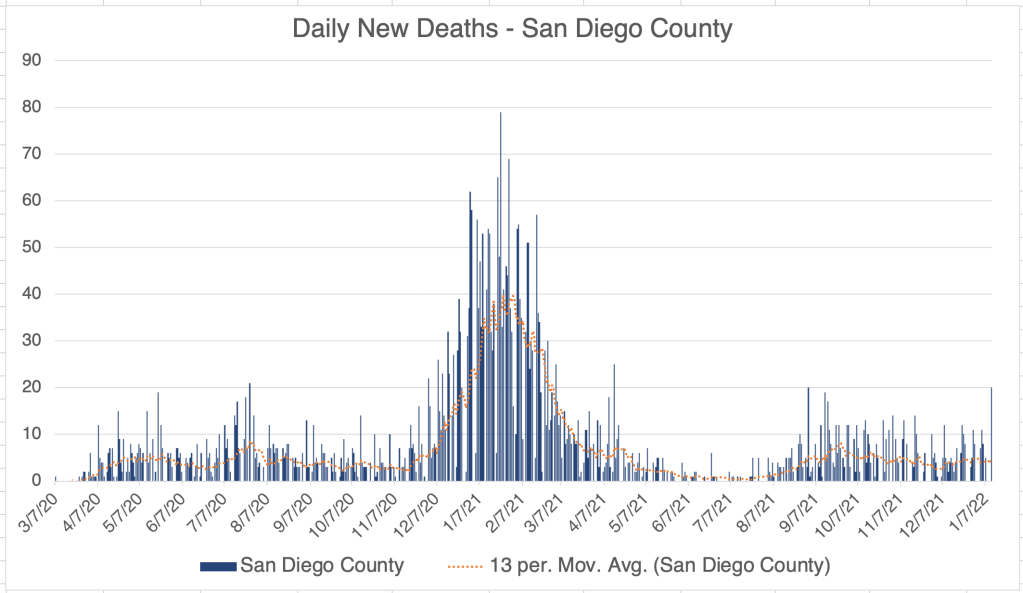
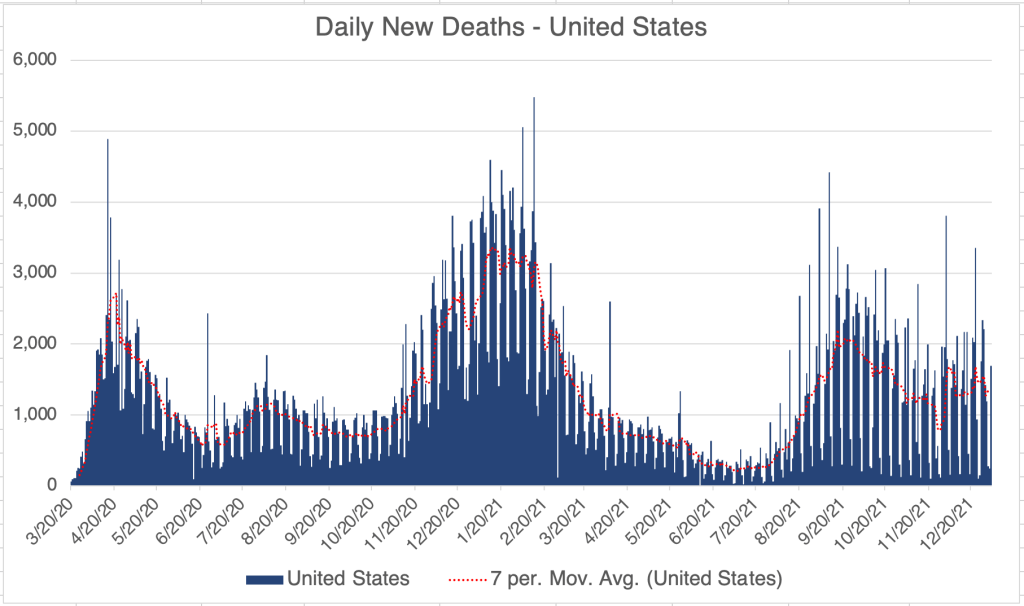
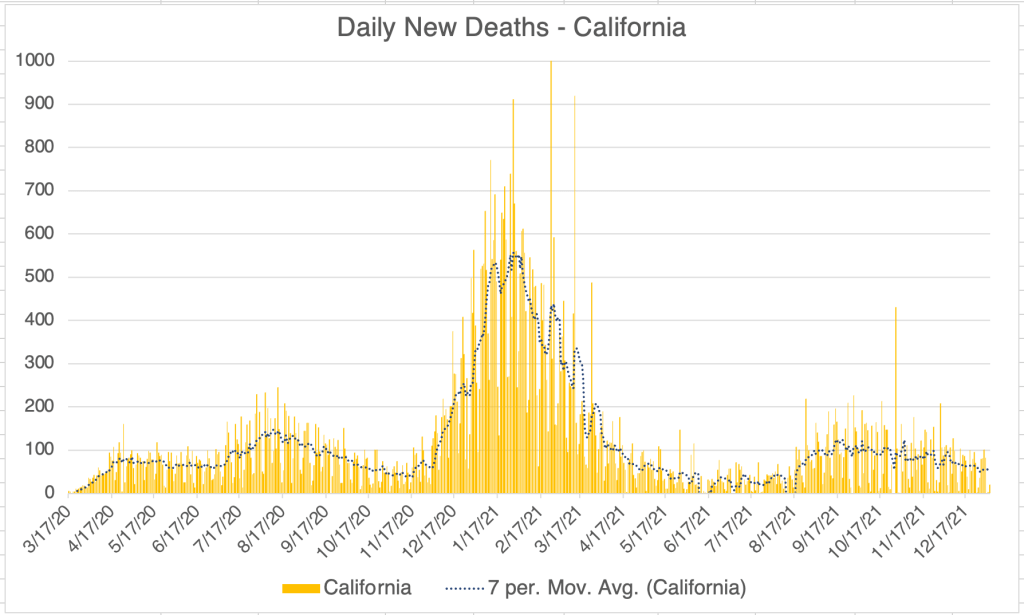
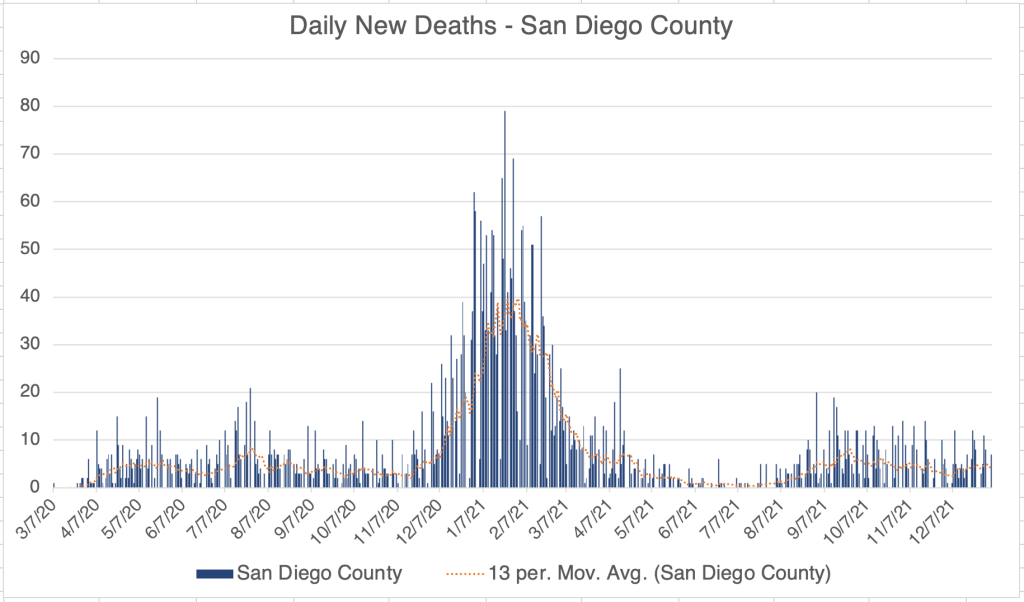
The great news is, deaths appear to have peaked in the US 2 weeks ago, and were indeed very low, about as many as last Winter when the cases were far fewer than in the Omicron wave. A little math says that Omicron is roughly a quarter as deadly as the Alpha variant from last Winter.
Another plug for data: Last week I asked for folks to answer the following questions:
1) Have you ever had COVID? If so, when?
2) Have you been vaccinated? When?
3) Have you had COVID multiple times? If so when? What were your symptoms like each time? Were you hospitalized? If so for how long?
4) Is there anything else you’d like to share?
Obviously, a lot of people don’t want to go public with this information. You can post below or direct message me. I want to get an idea of how vaccination and previous infection produced protection for future infection. When you were infected will tell me what SARS-2 variant you had, and whether that variant protected you from future versions.
So far, I’ve only gotten about 30 responses, too few to be useful. If you want chime in, please do so! Thanks!
Just as the Pandemic seems to ending with a bang, so my personal COVID story ended dramatically. But first, the case update for this week.
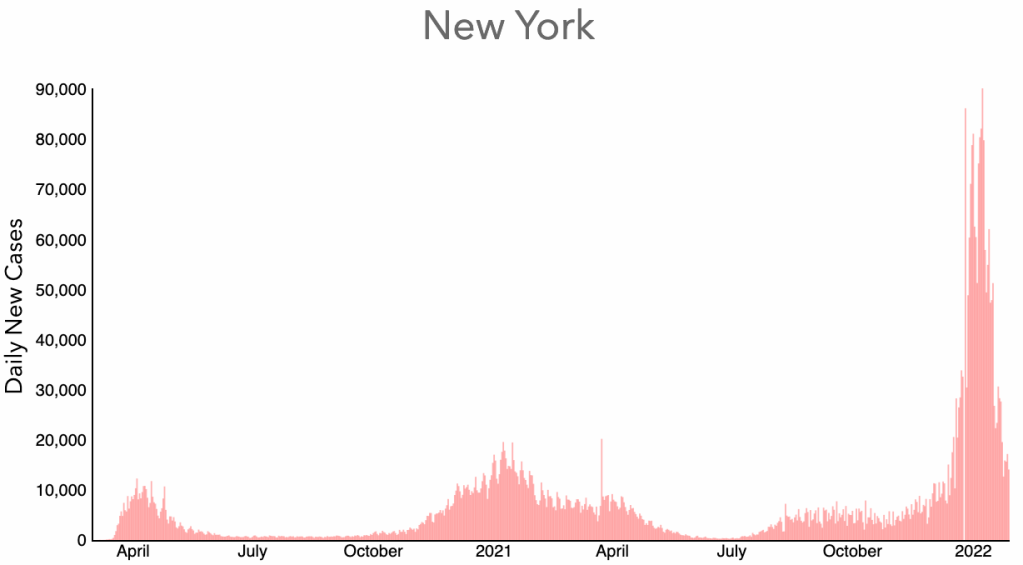
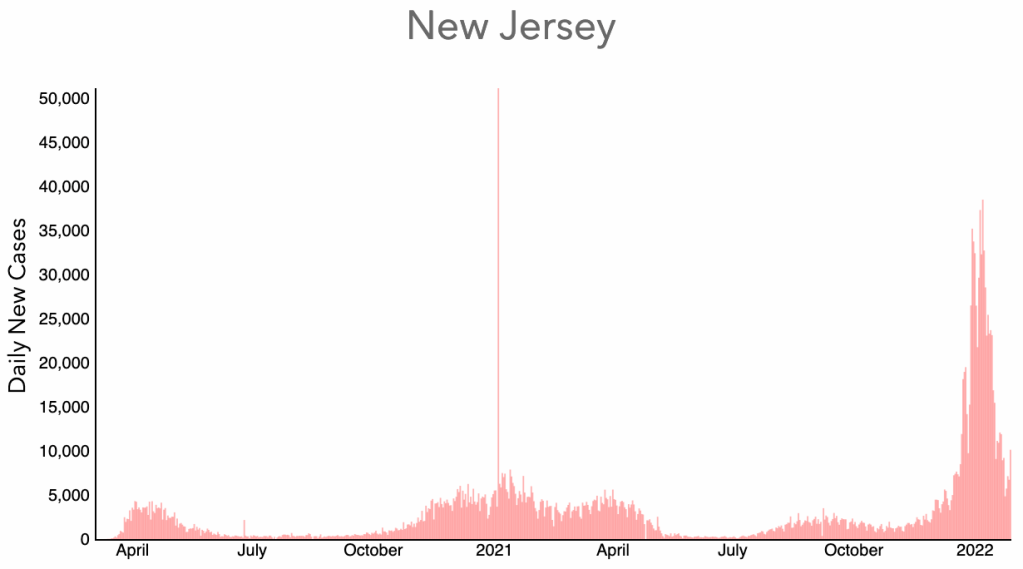
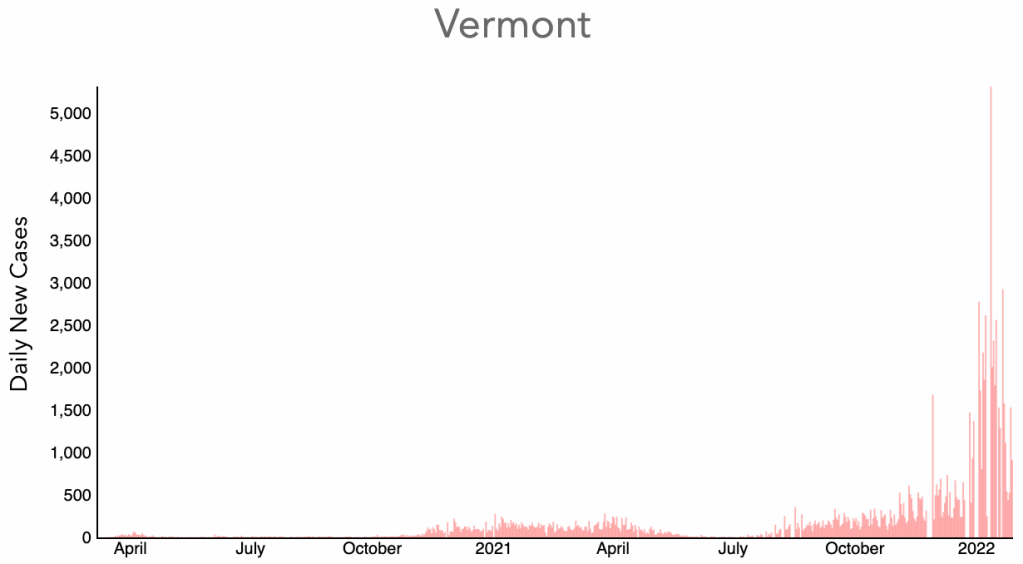
The US, California, and San Diego County are all well past the peak of Omicron cases, and cases are dropping rapidly. In some Northeastern states like New York, New Jersey, and Vermont, the Omicron wave is already nearly over.
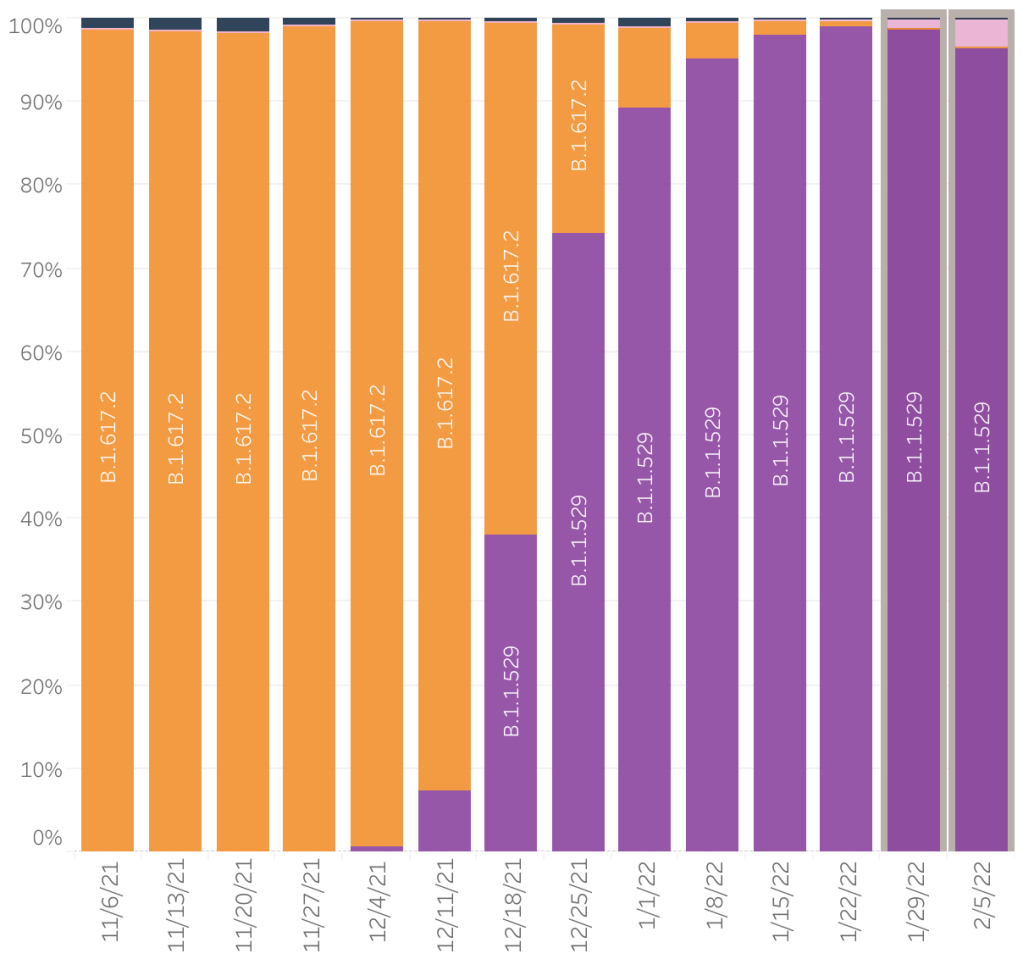
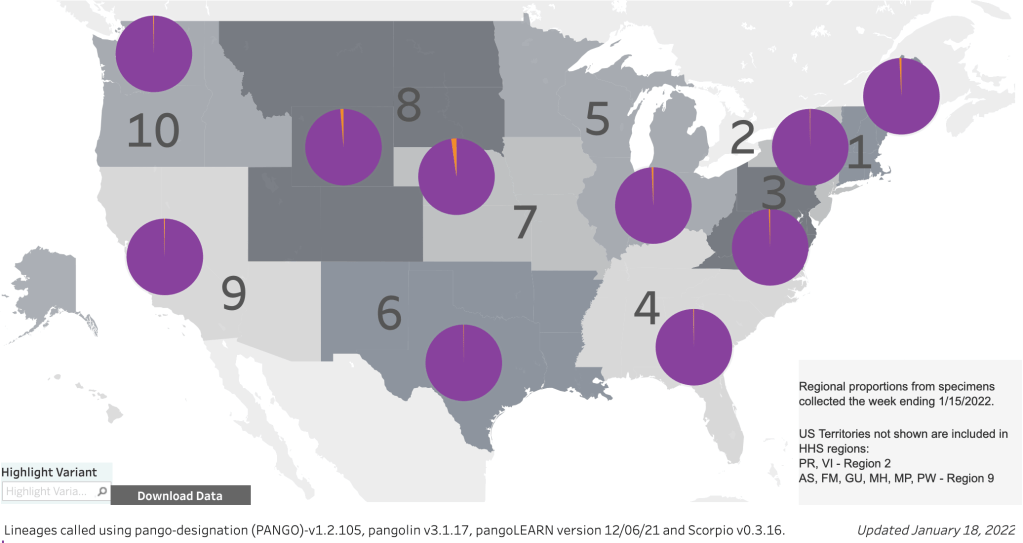
According to the CDCs variant proportion site, Omicron is now 99.9% of new cases. I will not report on this again, since this has now become uninteresting. There have been reports of a new subcategory of Omicron, BA.2, which is even more infectious than Omicron, but just as mild.
The end of my COVID story: I tested Positive for COVID on Friday the 14th, and finally tested Negative this Thursday morning, the 27th, almost exactly 2 weeks later. COVID actually got worse for me during course of the 2 weeks, with me getting more fatigued as time passed. Thursday night and yesterday were particularly bad, with extreme fatigue, sleeplessness, dehydration, uncontrollable shaking, and finally mental incoherence on Thursday night and Friday. Finally last night I was able to sleep for 11 hours and I finally feel like I’m recovering. I ate a full breakfast this morning and am actually doing some chores around the house.
I really only have 1 co-morbidity, celiac disease, an auto-immune disease. Unfortunately, I’ve never seen research on how auto-immune diseases interact with COVID or vaccination. It may be safe to assume for now that my auto-immune disease put me at greater risk from an immune system intensive disorder, but I don’t know for sure. While most of my COVID symptoms were indeed very mild, I was very surprised by the severity of my fatigue, which had multiple other negative effects. I sought medical attention twice, but they were never nearly as concerned as I was.
The “Final” Verdict on Antibody Dependent Enhancement: As most of you know, ADE has been a major concern of mine from almost the beginning. I’m finally willing to give an assessment of how ADE impacted the pandemic. There were a smattering of cases in previously infected people who may have had more severe cases because of possible ADE, but not more than a smattering. It’s also becoming well acknowledged that Omicron infected everyone regardless of vaccination status and may have even preferentially infected vaccinated people. I know MANY people who are double vaxxed and boosted who got Omicron.
All that being said, I never saw any evidence that conclusively suggested that ADE was causing more severe symptoms because of natural or vaccine mediated immunity. In fact, even during Omicron, during which ADE was most likely to be operating, those with previous immunity clearly fared better than those without. Because I think Omicron is the death rattle of the pandemic, I’m willing to say that ADE never became the threat I was concerned about. For this reason, IF I didn’t already have natural immunity because of Omicron, I might actually get vaccinated IF I could find someone who would aspirate before injecting!
I never saw any paper that dealt with the issue of ADE, not even a little. Those that mentioned it did so only in passing.
Don’t go looking for Omicron: Lastly, I’ll just say that while most of my friends had an undramatic time with Omicron, I did not. If you haven’t gotten Omicron yet, don’t go out looking for natural immunity from an Omicron infection. For me, it was no fun at all, and not worth the lost time and anxiety, even though I’m glad to now have hard earned natural immunity. The vaccines may not actually help you against Omicron infection, but they do seem to help you have an easier time of Omicron. Also, if you haven’t gotten Omicron yet, I recommend taking precautions and wearing an N95, KN95, or KF94 when in public.
Precautions against Delta are not adequate for Omicron, so kick it up another notch if you haven’t had Omicron yet.
After 12 days of symptoms, I still have COVID. My symptoms are considered mild, but I’m still tired, have no appetite, and am frequently feverish, so writing a long post is not my favorite activity right now. I also have a small amount of viral pneumonia, but not enough to be treated for. For an update, I’ll just state for now that cases are coming down rapidly in the US right now. I may add a real update to this post later.
Aspiration by vaccinators: I did want to point out that I saw a very interesting video recently from John Campbell that is very instructive. He points out that vaccines are intended to be given in an “intra-muscular” fashion, meaning the injection is supposed to remain in the muscle it’s injected into. If this happens, the vaccine makes Spike protein just in that localized area, and your immune system finds it there and mounts a response. Unfortunately, if a vaccine is injected into a blood vessel, the vaccine can travel throughout the body, making adverse events much more likely. For the flu, this is still not a big risk because the flu proteins only really interact with respiratory cells. But for COVID, the Spike protein can interact with cells all over the body and cause various effects including inflammation.
There is a simple way to avoid injecting in to blood vessels. A vaccinator can simply push the needle in, then pull the plunger back slightly to make sure there is no blood, then inject (Demonstration of this process starts at 22:00 of the video). This eliminates the possibility of a blood vessel injection. Unfortunately, this procedure is standard practice in just a few countries like Denmark, S. Korea, and Japan. Most countries including the US, UK, Canada, and many others do not practice this. John Campbell is very pro-vaccine, but wishes aspiration was standard.
My doctor friends tell me blood vessel vaccine injections are very rare.
In the US, lots of people in the health care industry basically ignored adverse events due to COVID vaccination. This includes me for a time. The CDC is still not capturing all of the available data on adverse events. Many of these events could have been avoided with a small change in policy.
Vaccination has helped a lot of folks have milder COVID symptoms. It’s too bad that the lessons from adverse events were not absorbed sooner. If you get vaccinated or get a booster, see if you can get them to aspirate before they inject!
The UK drops COVID restrictions: The Omicron wave has come and gone in the UK, and the country has basically dropped all COVID related restrictions. The US is a few weeks behind the UK, so we may be able to drop restrictions here soon too.
Omicron is milder, but I certainly haven’t had an easy time of it, so I wouldn’t recommend running out and getting your natural immunity by getting Omicron. If you haven’t had it yet, continue to wear your N95, KN95, or KF94 while indoors in public. Or even outdoors in groups. I probably got COVID outside but in close proximity to someone with COVID. The stuff that worked with previous versions doesn’t necessarily work with Omicron.
This is a case update. I’ll also give an update on the state of Omicron in the US, and show some data from a great new paper from California. I’ll also comment on the new mask guidance by the CDC.
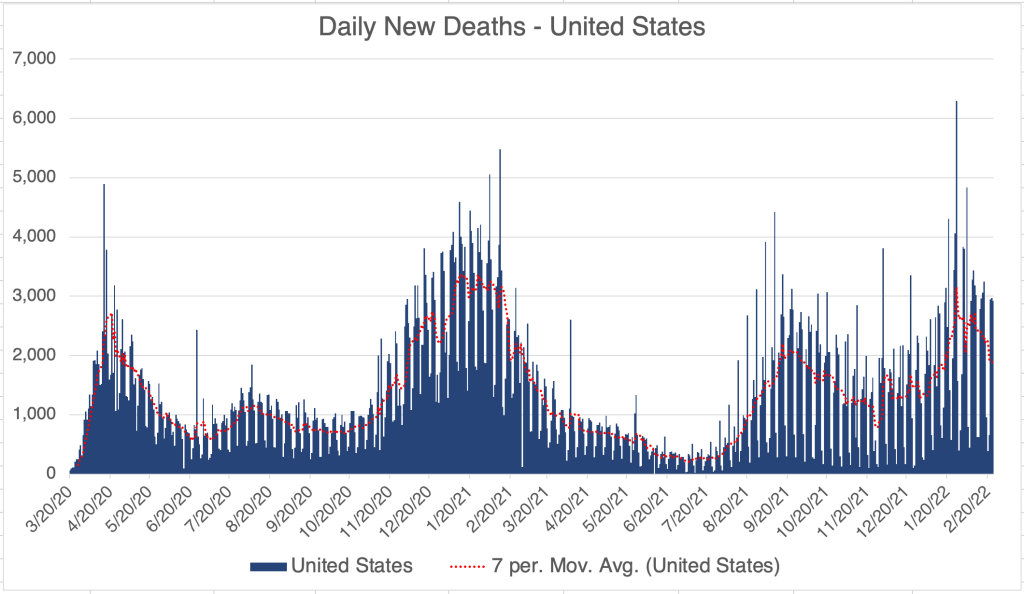
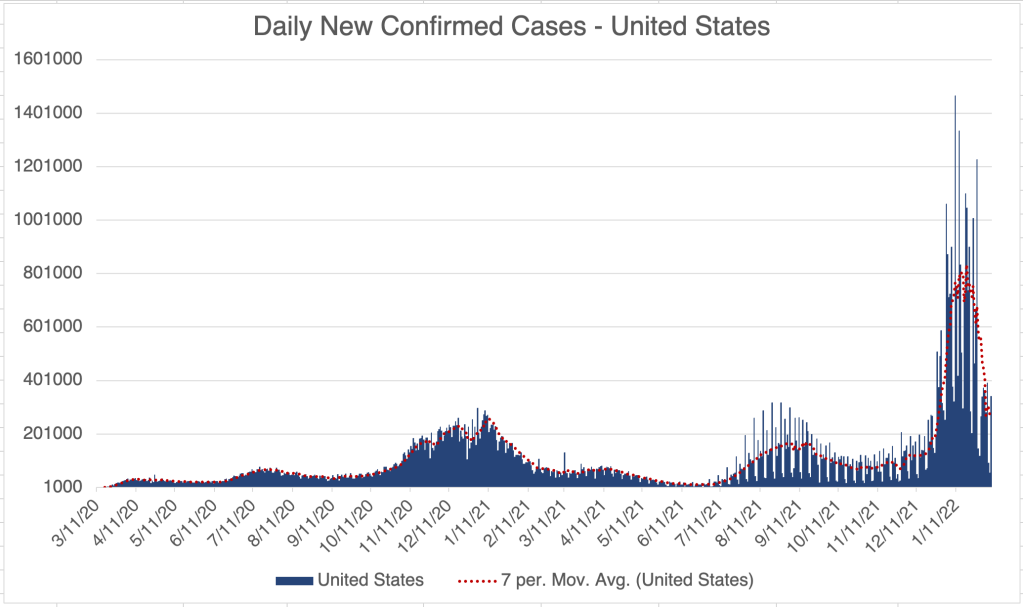
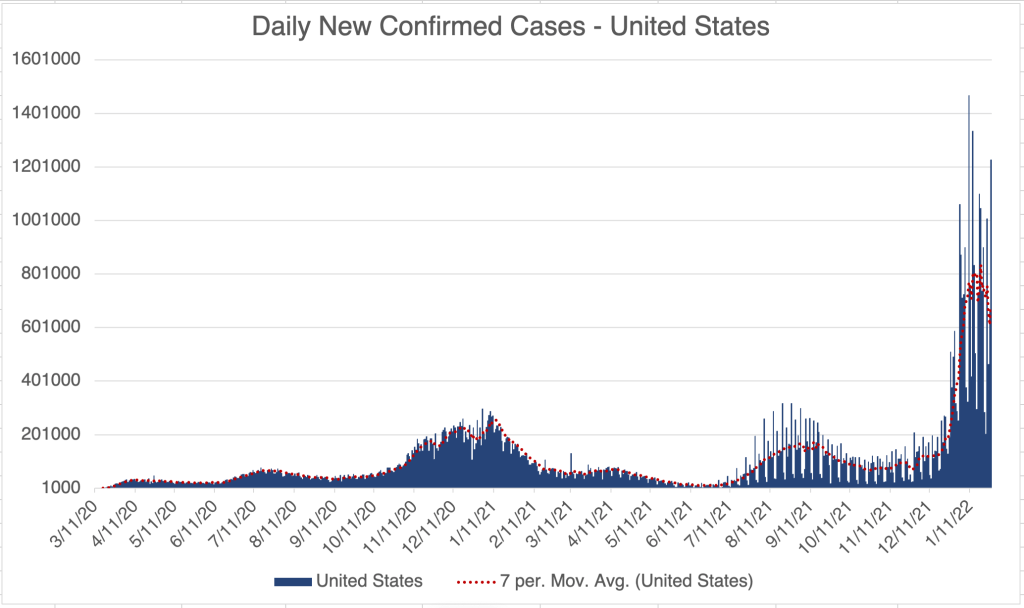
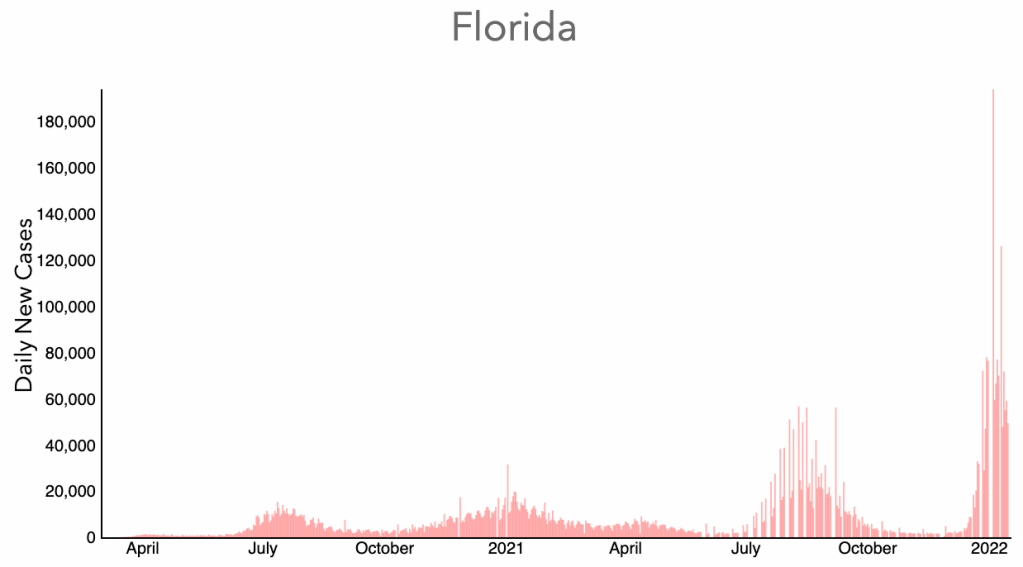
New cases have apparently peaked in the US over the past week, reaching a high of 1.5 million cases in 1 day. Cases are now declining for the US as a whole, driven by declines in several Eastern states like New York, New Jersey, and Florida. Cases have not yet declined in most US states, although many may be peaking right now as new cases have slowed. So far, deaths are only slightly up for the US. Hospitalizations appear to have peaked as well.
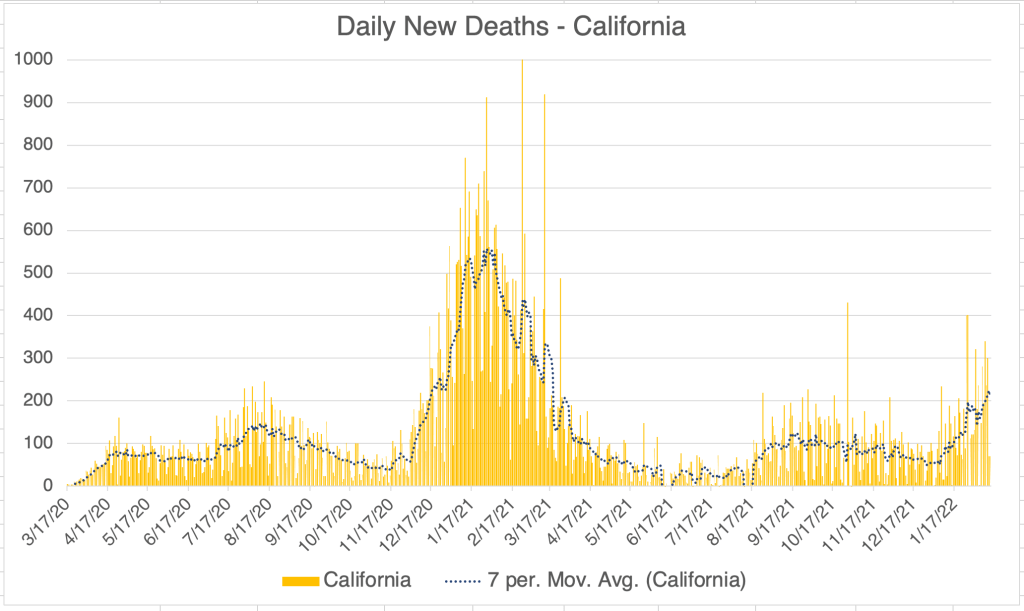
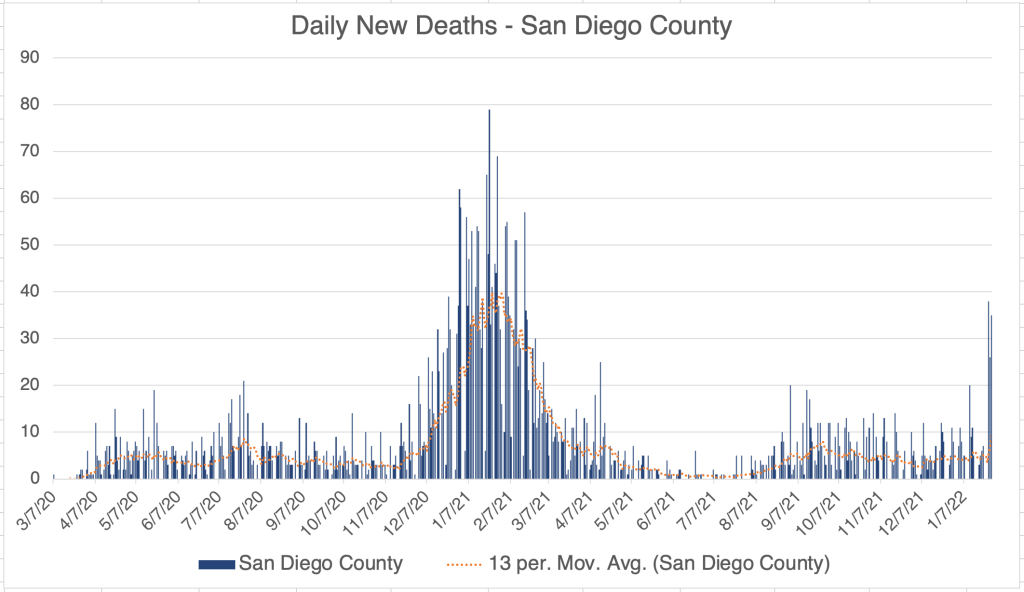
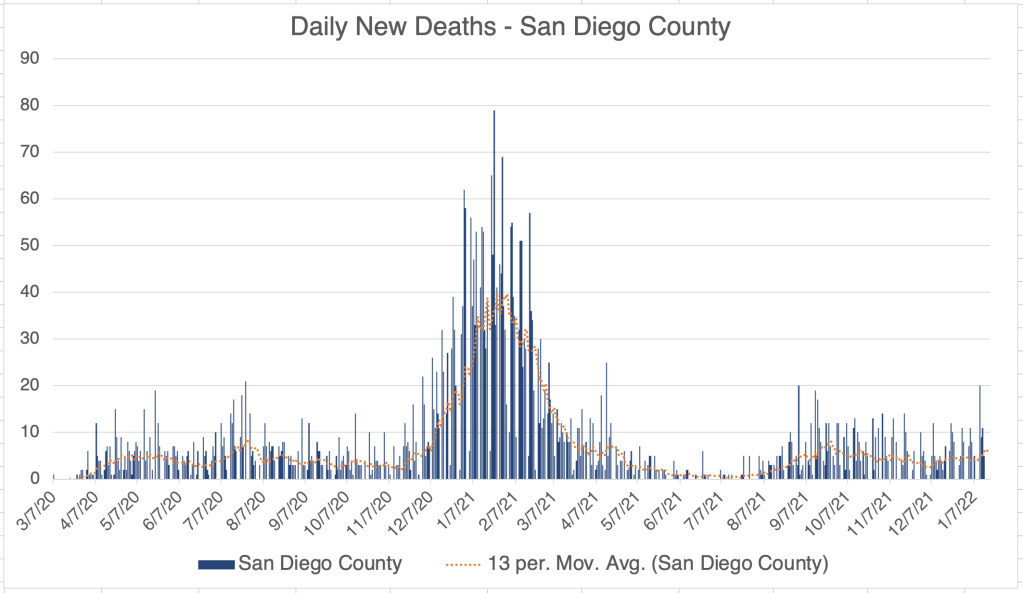
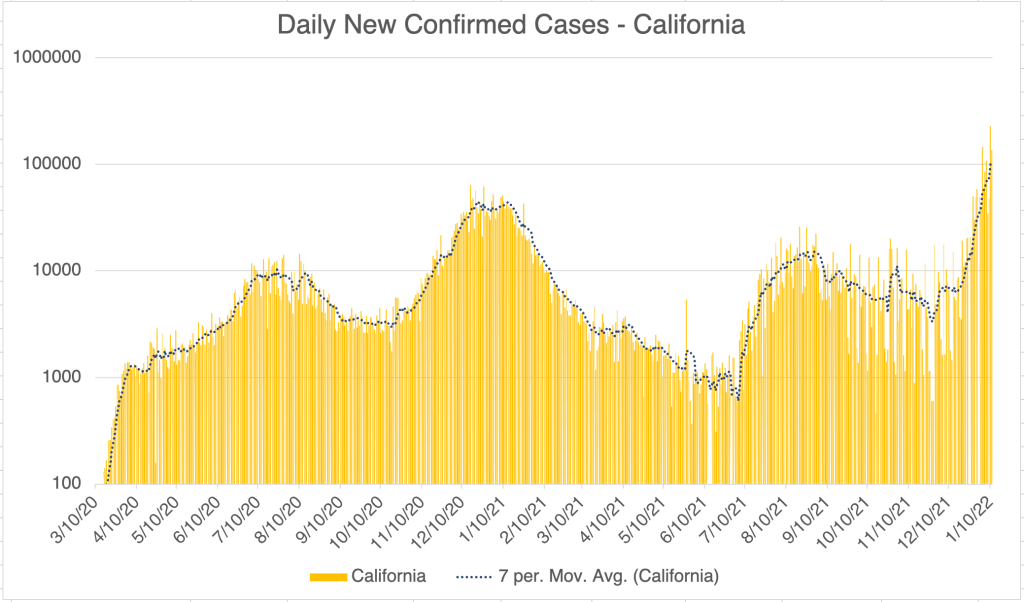
California and San Diego County new cases appears to be still going up, but new cases have slowed, and I suspect will start declining soon, maybe this week. Again, deaths have not yet started to increase. Deaths usually follow cases by between 2 and 4 weeks.
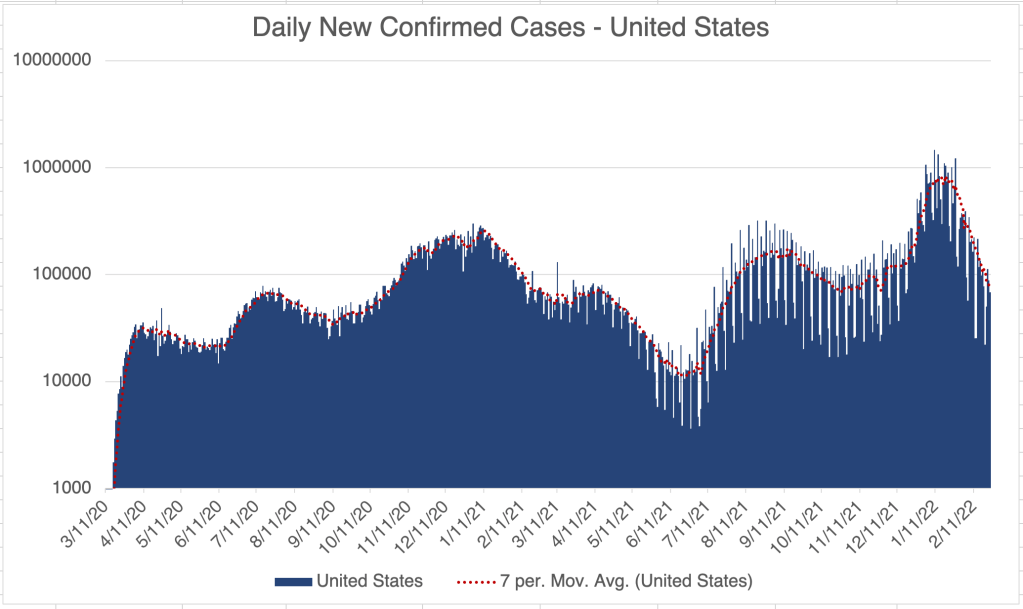
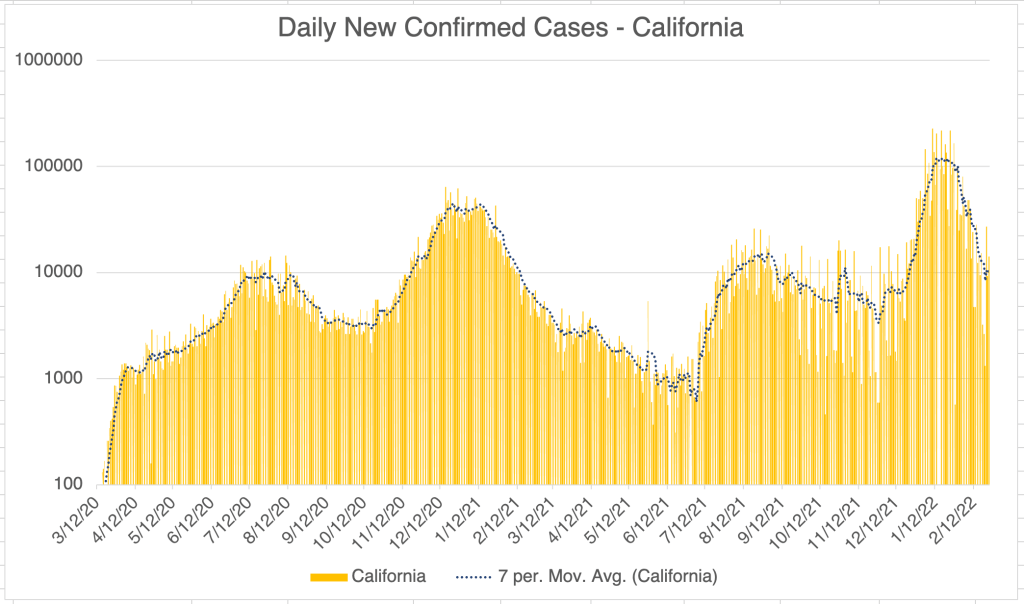
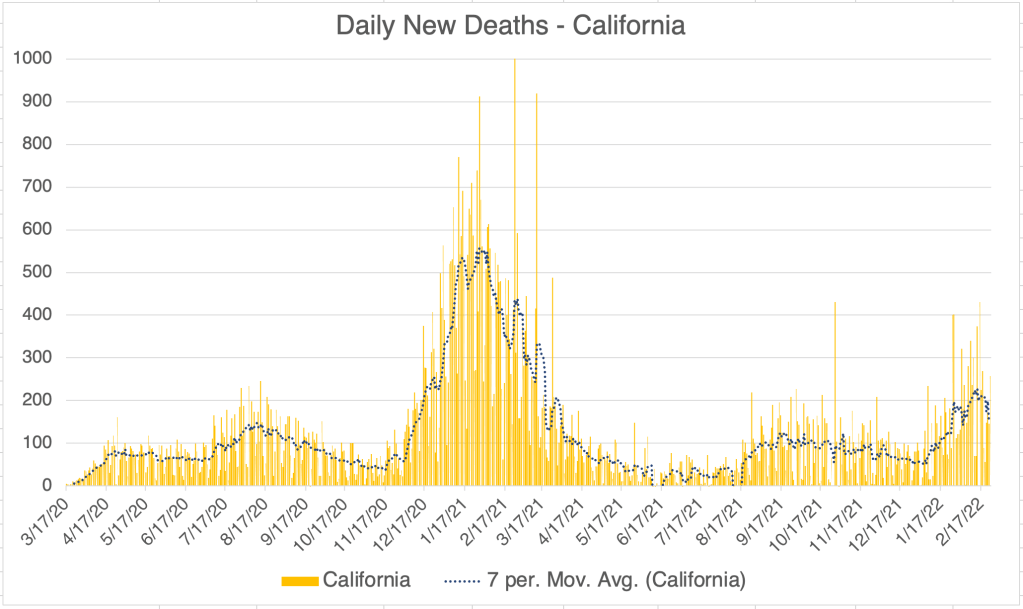
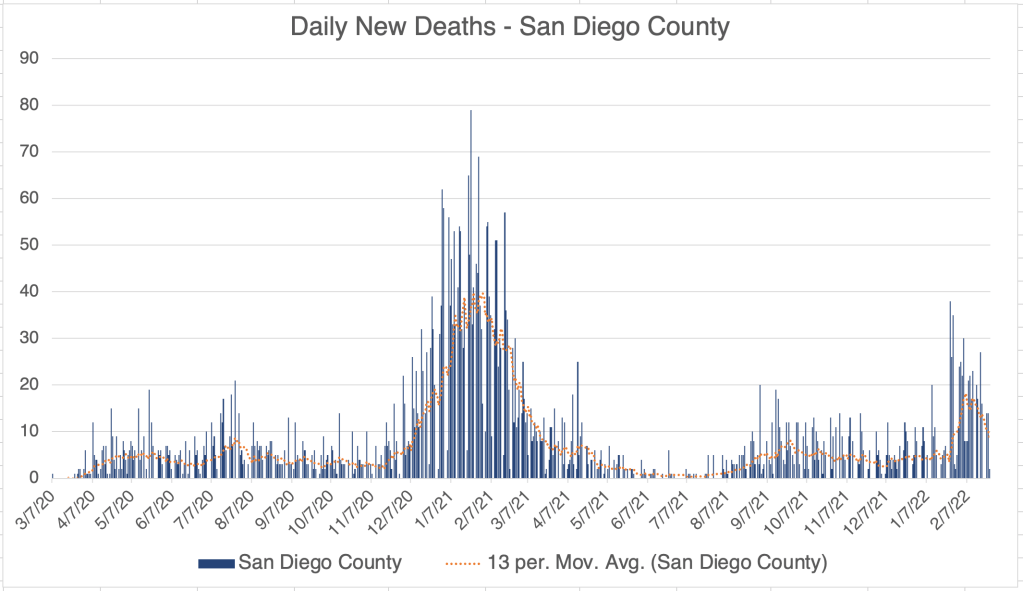
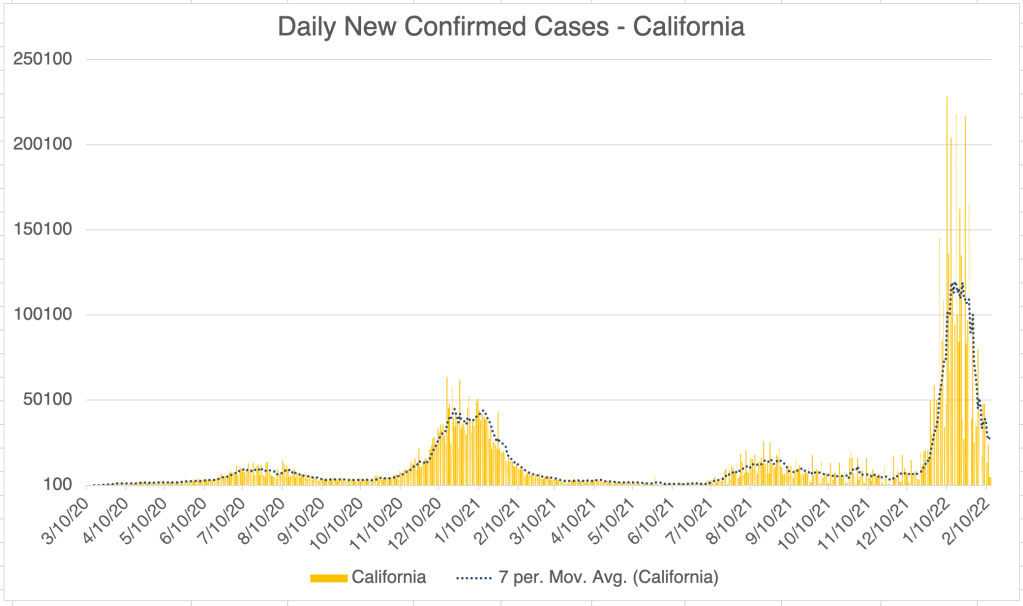
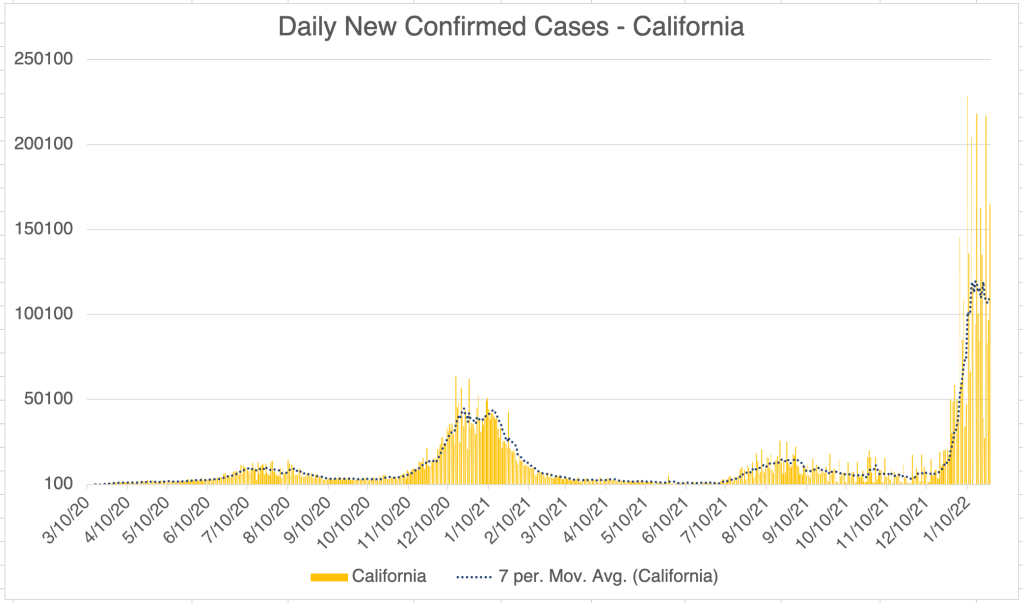
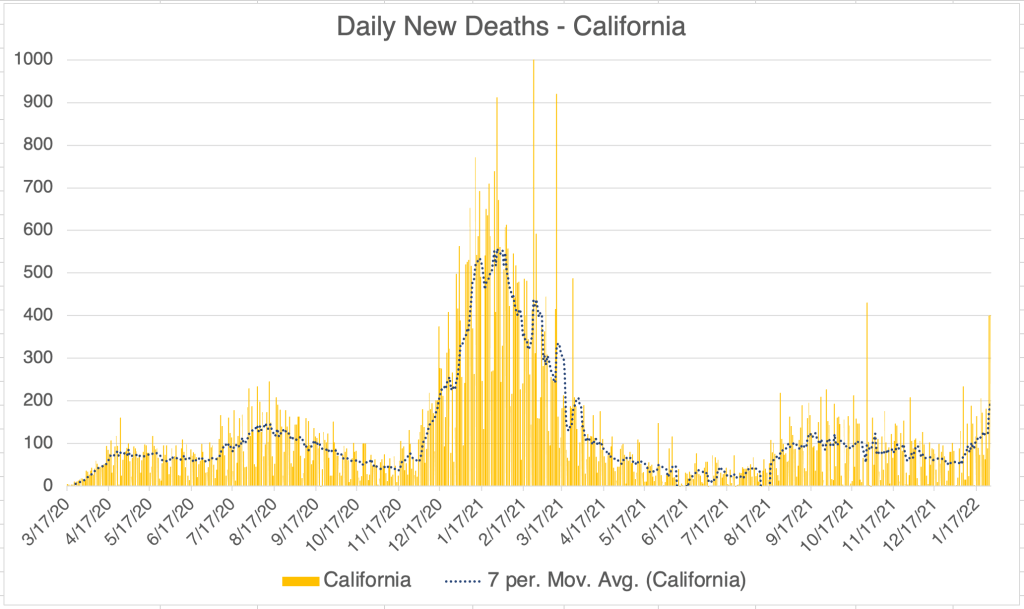
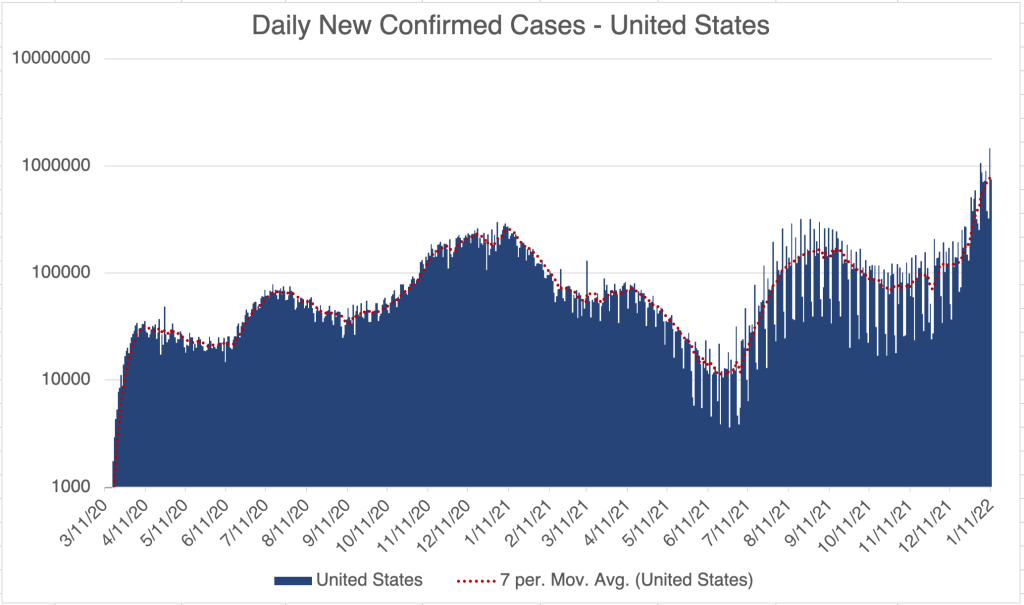
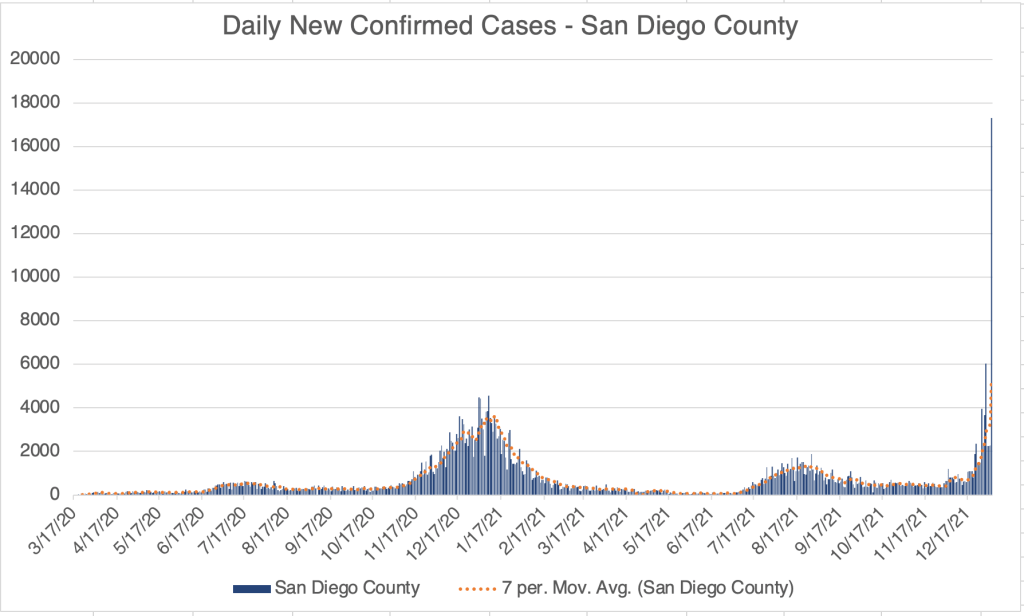
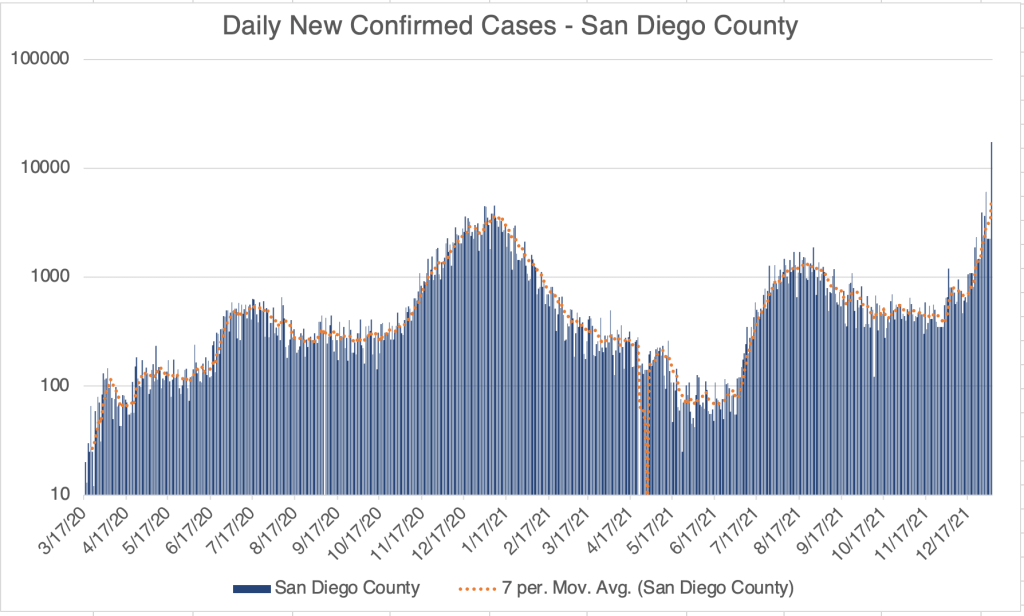
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
Omicron Update: Omicron infections now represent 99.6% of infections in the US. Omicron has now almost completely eliminated Delta in the US. It continues to appear that Omicron represents the end of the pandemic, although it will go out with a bang!
I finally got COVID!: Last Friday I tested positive for COVID! I almost certainly got it while in a “gray area” situation that had some risk, but might have been OK with a previous variant. Most symptoms have been very mild, but I was super achy for a day. I’m still not feeling strong and I nap a lot. No loss of taste and smell, or shortness of breath, but I did have a fever during my achy day. As of yesterday, I still test positive, so my body is still fighting.
Omicron much milder than Delta, but evades vaccines much more: As I’ve stated before, it’s a little scandalous how few useful papers have come out of the US this last year. But a UC Berkley lab has a great new paper in pre-print right now. They had the foresight to collect data for a time period in December when both Delta and Omicron were present in the population. The paper is a little opaque because much of the information is in dense tables, with less than useful headings (SGTF = Omicron, non-SGTF = Delta) but has some great information nonetheless.
Table S10 is the most interesting to me. I’ve turned some of the data into graphs to make the meaning more clear. The table compares the number of infections by Delta or Omicron in unvaccinated persons, those with differing levels of vaccination, and with documented previous infection (natural immunity). Vaccination definitely helps prevent infection by the Delta variant, but Delta still infects vaccinated individuals. This may be because vaccine efficacy goes down over time, the Delta variant is too different to be completely stopped by the Wuhan based vaccines, or some combination of both.
Graph is by me, from data in Lewnard et al, Table S10. Cases with Natural Immunity were multiplied by 6 to normalize for the number of documented infected individuals in the population. In San Diego County, there are roughly 500,000 documented COVID-19 cases, out of a population of approximately 3 million in the county.Graph is by me, from data in Lewnard et al, Table S10. Cases with Natural Immunity were multiplied by 6 to normalize for the number of documented infected individuals in the population. In San Diego County, there are roughly 500,000 documented COVID-19 cases, out of a population of approximately 3 million in the county.
Omicron is far more infectious in general, and also is far more infectious in vaccinated individuals. In fact, more people in this study were infected by Omicron if they had 2 doses of the Pfizer or Moderna vaccines. Since a majority of Southern Californians are vaccinated, it this does not necessarily mean that vaccination made it more likely to be infected by Omicron, but it’s a striking result. Yes, Antibody Dependent Enhancement may play a role in this result, although the exact reasons are likely a complicated combination of factors.
Another interesting result is that infections are far lower among those with previous infections. For the graphs I include, I’ve even normalized this number for the proportion of people who have been infected by multiplying the given number by 6 (see graph for details). In spite of this, infections are FAR lower in those previously infected. This is consistent with the data from Israel suggesting that natural immunity is far better than vaccination at preventing future infection.
Most European countries and Israel include previous infection in immunity requirements. The US still does not accept previous infection as prove of immunity. As we continue to argue about vaccine mandates, it would be wise to include previous infection as proof of immunity.
Better super late than never I suppose: After many months of treating all masks as essentially equal, the CDC released new guidelines regarding masks that points out that simple cloth masks are not as effective as medical grade respirators like N95s, KN95s, and KF94s. They still don’t go far enough in my opinion, since they still promote surgical masks as effective. Blue surgical masks are loose fitting on the side and allow air to enter and exit without being filtered. If you wear a mask, wear a medical grade respirator, not a blue surgical mask.
I believe we are a few weeks away from the end of the pandemic! As for me, I’m really looking forward to eating indoors at a restaurant again!
I know a lot of this post is dense and complicated. Your questions will help me be more clear.
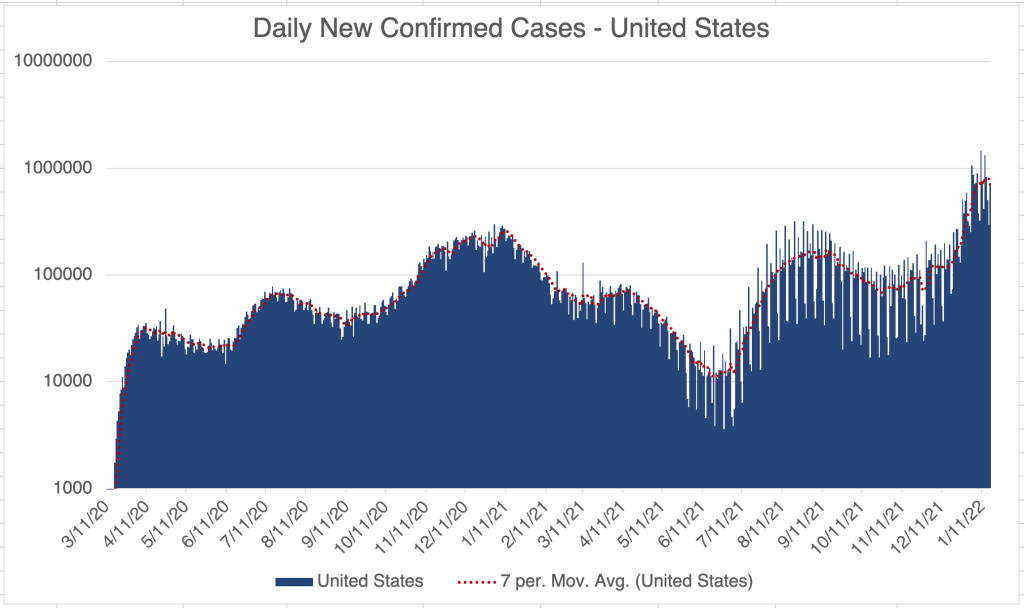
This is a case update. Cases continue be super high in the US. Over the past 2 years, the Sunday numbers are always the lowest of the week, but they also usually predict what will happen to the number in the following week. If you look closely at the case graph for the US, you can easily see the weekend dips in numbers. For this Sunday’s number, the rise in cases is much lower relative to the previous week than the number for the 26th. Because of this, I expect new case numbers in the US to peak this week or next.
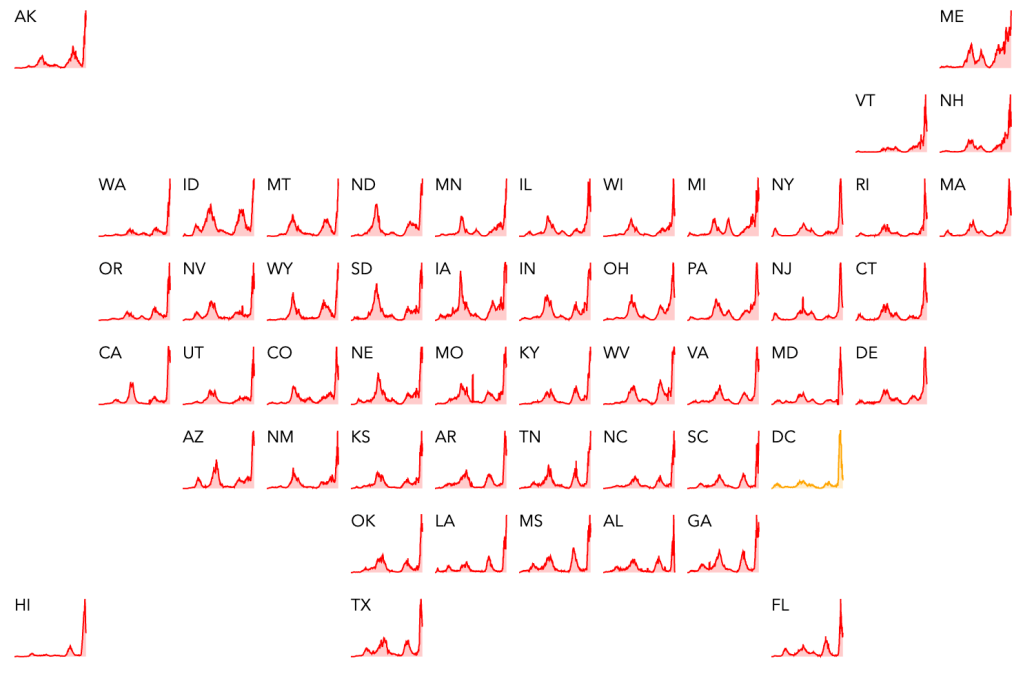
All that being said, cases are still extremely high in every state in the US right now, and still rising. Only Washington DC appears to be seeing a drop in cases right now. Deaths have not yet started to increase in the US. Deaths have tended to increase between 2 and 5 weeks after the start of a peak, so it’s still too early to know how high they will be.
California and San Diego County are of course also experiencing extremely high numbers of cases right now. LA County again has the highest number of cases in the US, with a staggering 384,000 active cases right now.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
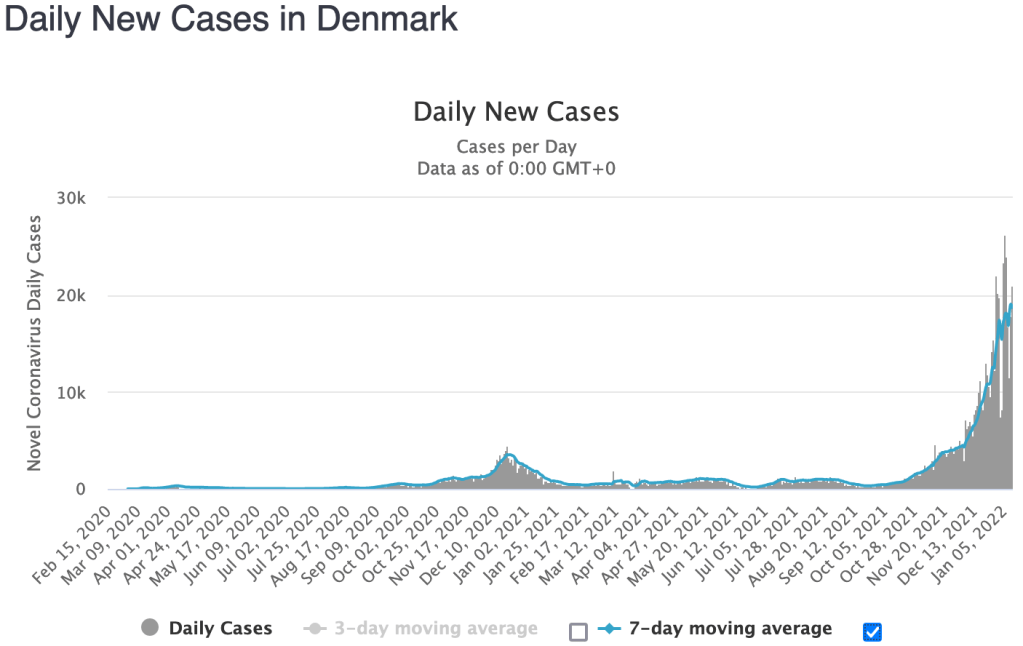
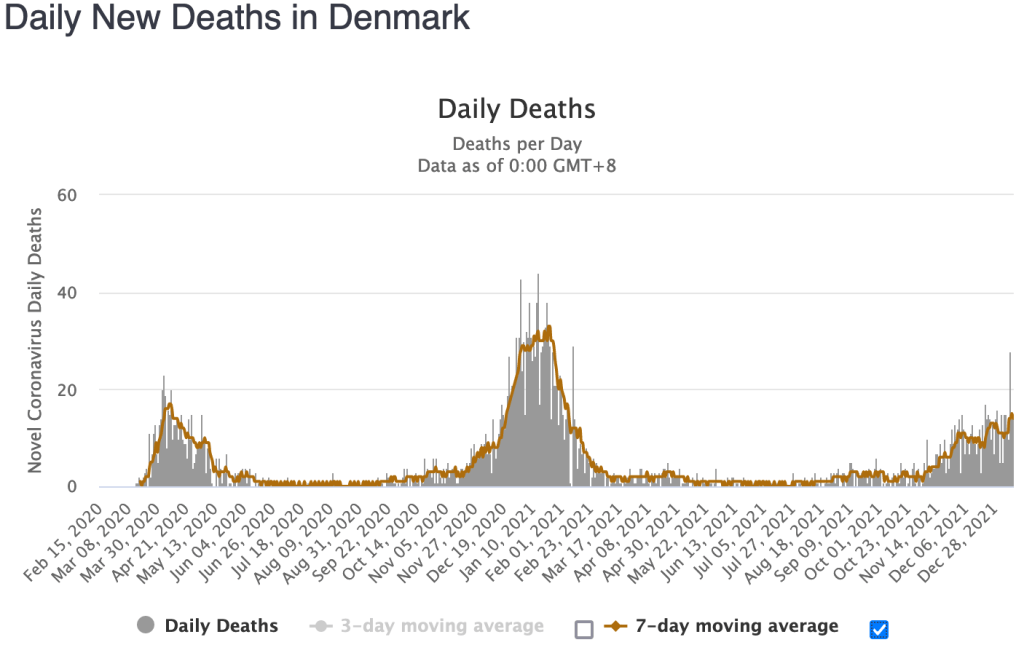
In Denmark, which has a lot of testing and virus surveillance, deaths are up but at a very moderate rate. At the peak of last year’s Winter surge, the COVID fatality rate was 0.94% (deaths/confirmed cases). For the Omicron wave in Denmark, the rate has been only 0.053%. This rate is very small, but it’s still not zero, so if you have COVID risk factors, continue to take precautions.
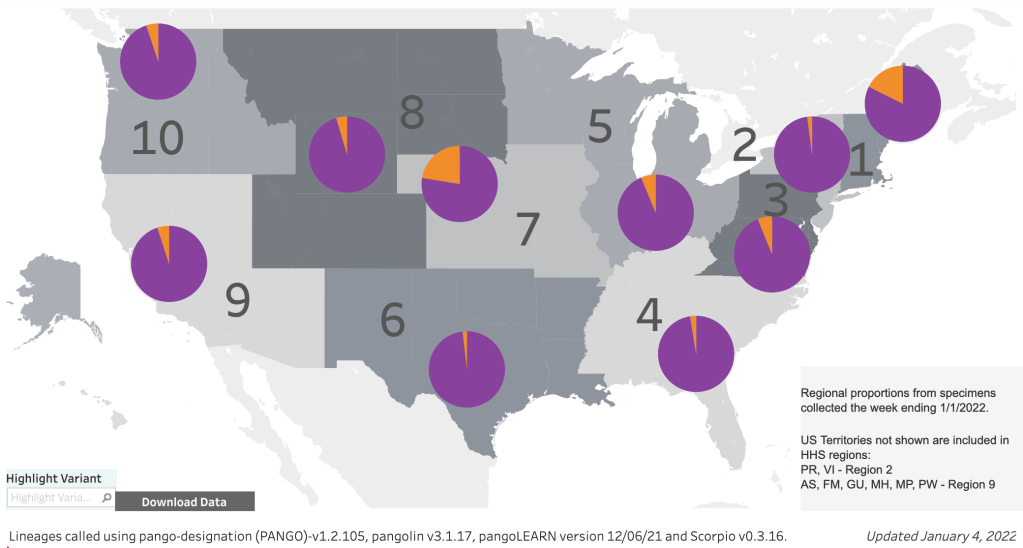
Omicron Update: The CDC recently released an update on variant proportions. Omicron is now 98% of SARS-2 cases for both the US and the Southwest region This is great news.
Omicron infections are proving to be very mild in most patients. That being said, there are a tremendous number of cases right now. I have lots of friends and family who have had COVID in the last 2 weeks, and several businesses near me have had closures or reduced hours because of under staffing. Additionally, hospitalizations are way up, and doctors and nurses are pretty exhausted taking care of all the sick people.
Managing COVID right now: Hospitalizations are way up, and lots of people are getting tested, either in a health care setting or with home rapid test a drug store. For this reason, tests are now in short supply everywhere. If you don’t need a test to go back to work or school, please consider NOT testing yourself just to satisfy your curiosity. If you do need to test yourself, please don’t test yourself every day, and try to reduce the number of tests you use. Since current tests are based on the Wuhan strain, there are lots of false negatives right now, especially with the rapid tests, since Omicron is the dominant strain. So a negative test is not very meaningful if you have symptoms. Most people’s Omicron symptoms last between 2 and 5 days.
Although Omicron causes less severe disease in general, there are a huge number of cases right now and some are still severe. If you don’t think you need medical attention, and are just experiencing cold-like symptoms, consider NOT going to the hospital for a test or to be treated. Please keep space open for those with more severe symptoms. However, if you have one of the classic COVID symptoms, like shortness of breath, don’t hesitate to check in with your doctor.Please don’t assume your vaccination, even with booster, will prevent you from getting COVID right now. Many fully vaccinated and boosted people are getting COVID right now because the Omicron variant is so different from the Wuhan strain used to make the vaccines.
Also, I still usually wear a mask indoors. If you choose to wear a mask, wear an N95, KN95, or KF94. Don’t imagine that a blue surgical mask, cloth mask, or neck gator is going to prevent infection. These masks are ineffective against Omicron. Effective medical grade masks are easily available at stores and online right now.
Remember to supplement with Vitamin C, Zinc, and especially Vitamin D! This is for everyone, to prepare your body should you get infected, or if you have Omicron right now.
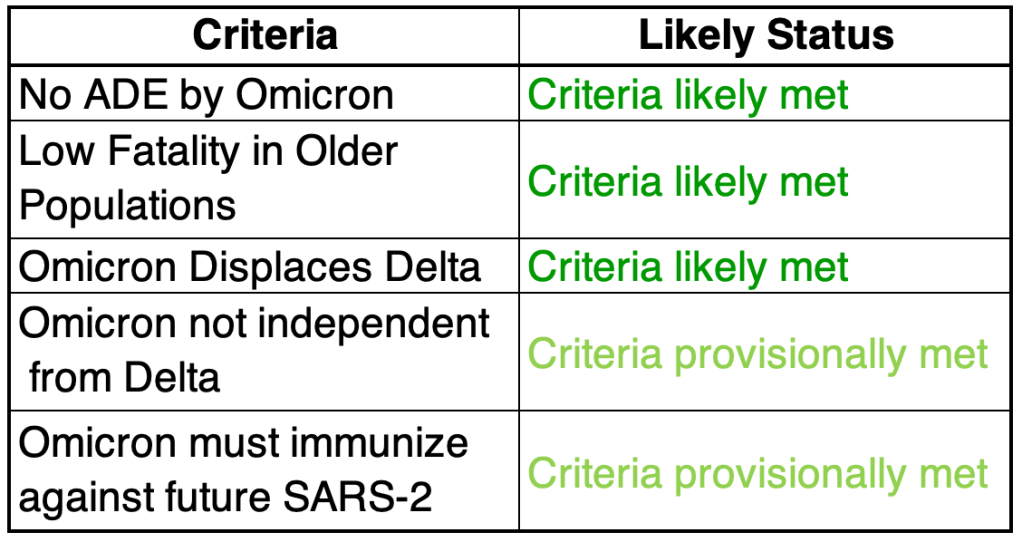
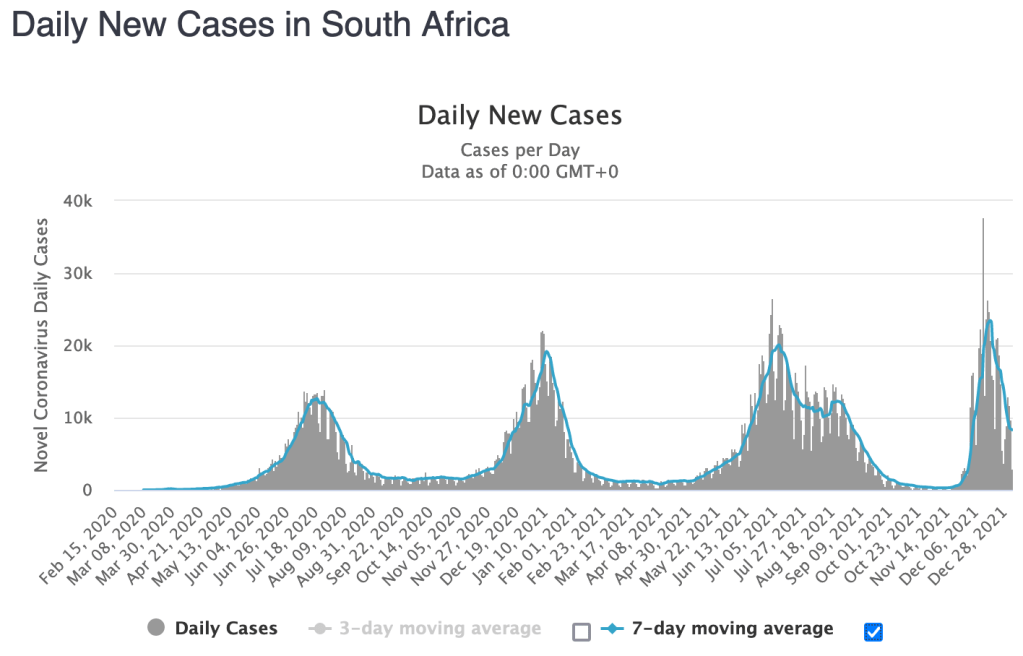
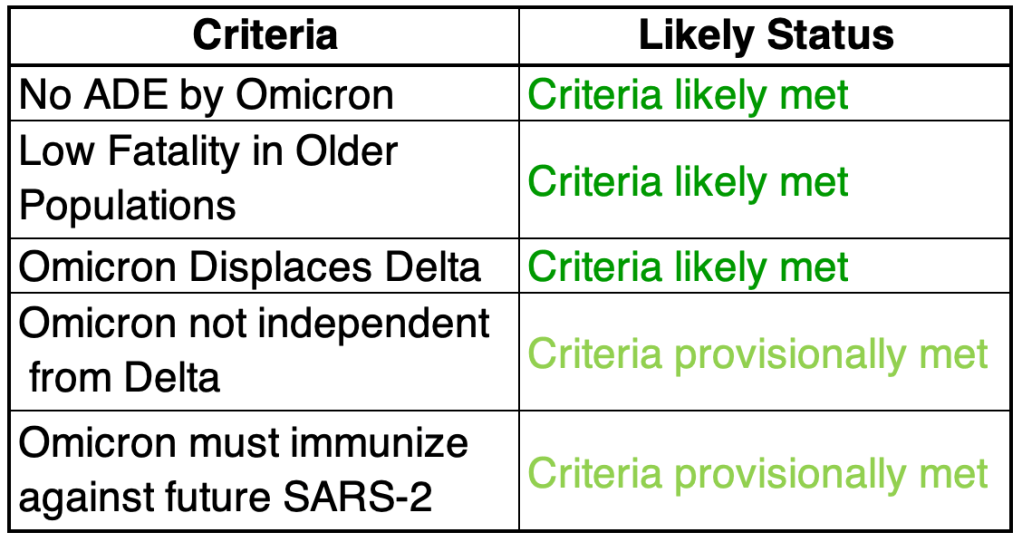
Omicron scorecard: Here’s my “scorecard” for this week. The new data from South Africa suggests that Omicron infection is “back compatible” with Delta, preventing Delta infection. This is great news and suggests Omicron infection will prevent future infections from other variants. As a reminder, I am not an epidemiologist, I’m a molecular biologist. This is my informed but not expert opinion.
1) Omicron must not use the ADE pathway to produce more severe cases: Looking at the available data so far, Omicron may preferentially infect those who have been previously infected, but cases are still mild, and fatality rates very low. So for now, this criteria is met.
2) Low fatality in older populations: South Africa has a relatively young population, so reports of mild symptoms may not carry over to countries with older populations. The UK data from this week suggests that Omicron deaths will be low, even in older populations. We are seeing a slight drop in deaths already.
3) Displace Delta: Delta has a much higher case fatality rate in the US than Omicron appears to have. For Omicron to end the pandemic, it must displace Delta from the COVID population of strains. Data from the US and UK suggest this is happening!
4) Omicron must not circulate independently from Delta: Related to the above, if Omicron is very different from Delta, it may act as a completely different virus. There’s a chance that Omicron may displace Delta on the short term but still allow Delta to persist. Since Omicron is displacing Delta, it looks like this criteria may be met, but we won’t know for sure until we can see if Delta pops back up after the Omicron wave is over.
5) Omicron infection must immunize against future SARS-2: Since Omicron appears to infect those with immunity to Delta, it may be that it is different enough that it will not provide immunity to Delta or other SARS-2 strains. This criteria is not strictly necessary if Omicron completely displaces other SARS-2 strains (see 3 above), but it would be really nice to have some protection against future strains. We won’t know for sure about this one until a new version of COVID arises. The new data from Denmark suggests this criteria is met!
I believe that the Pandemic is almost over, but there’s one big final push! Continue use your head, but be encouraged!
This is a case update. I’ll also give an update to the Omicron wave we are experiencing.
On Monday, the new case numbers were approximately 3 times the single day case number from last Winter, with over a million new cases in 1 day. Cases are skyrocketing in many states across the country, in particular in the Northeast where Omicron cases are tremendously high. Of course, the very high 1 day number is partially due to the lower rate of reporting over the holiday weekend. I’m switching back to a logarithmic format for some of my graphs because the new high numbers make my linear graphs a little meaningless.
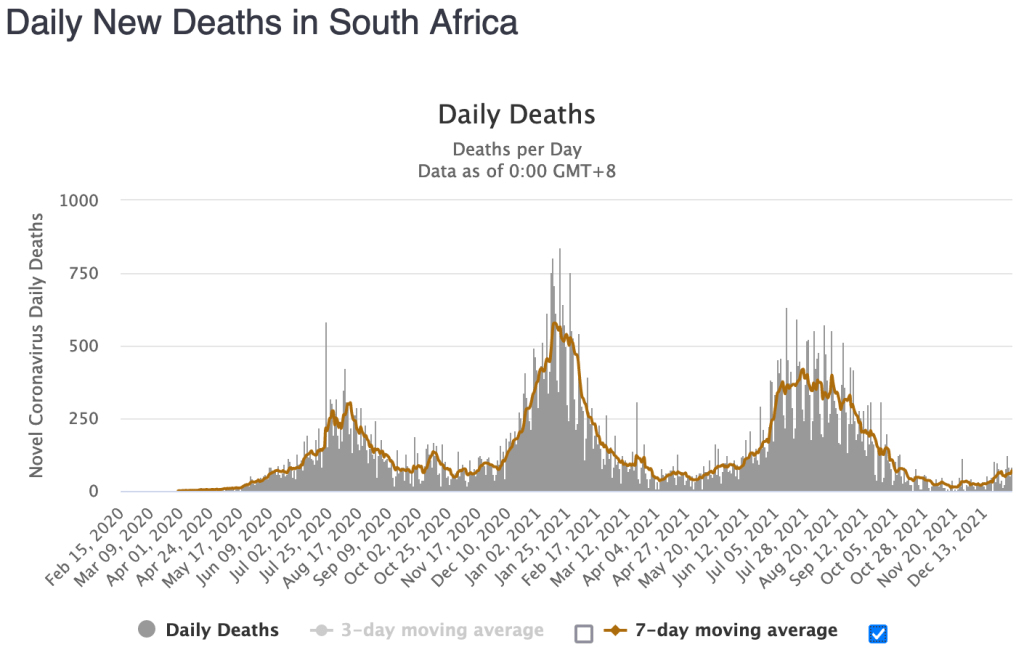
Deaths have not yet started to rise in response to new Omicron wave, at least here in the US. Deaths tend to follow cases by between 2 and 5 weeks, although this time frame will be shorter for Omicron because both incubation time and disease duration are shorter for Omicron. In South Africa, where the Omicron wave is almost over, deaths are up very modestly during the Omicron wave.
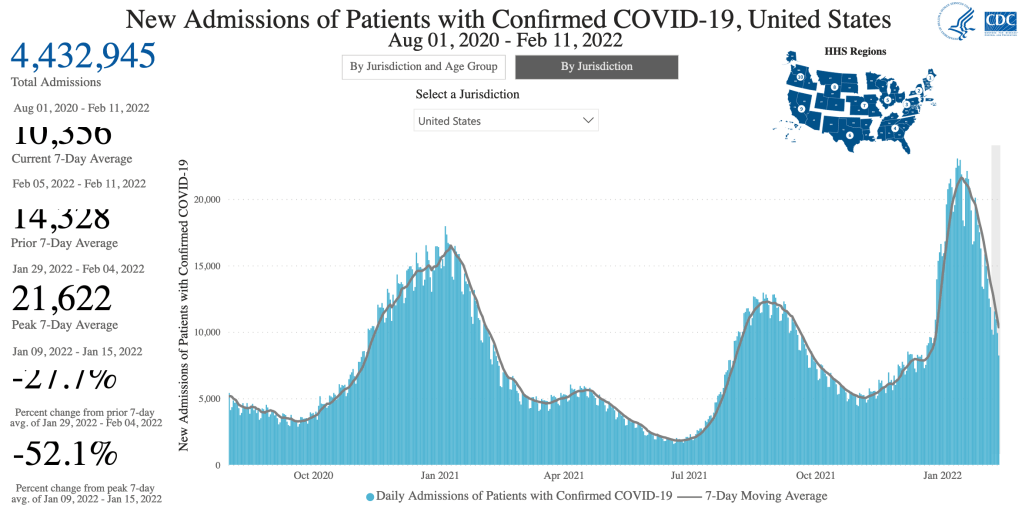
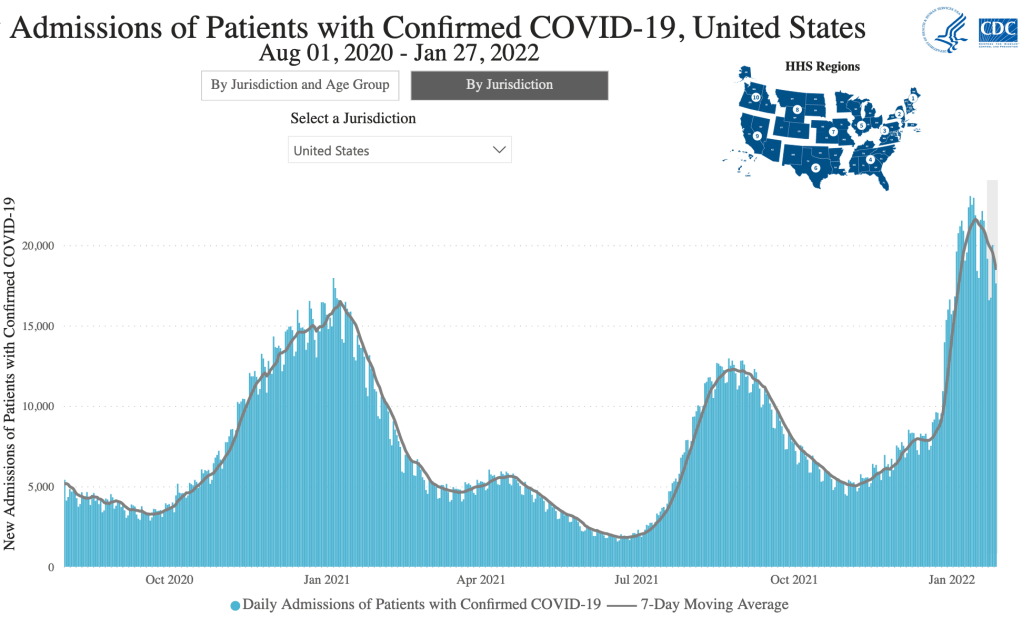
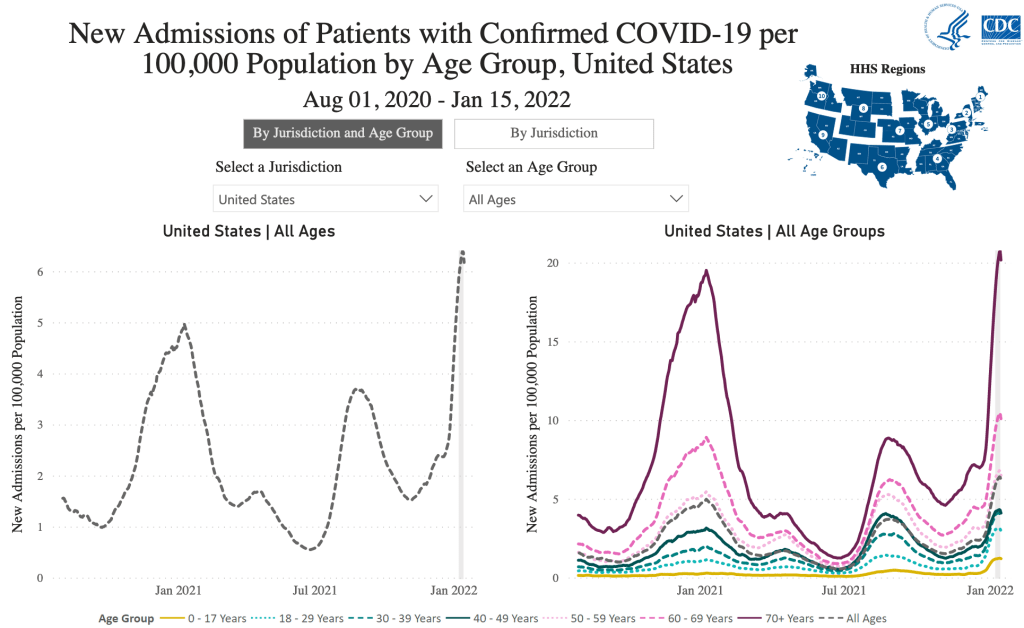
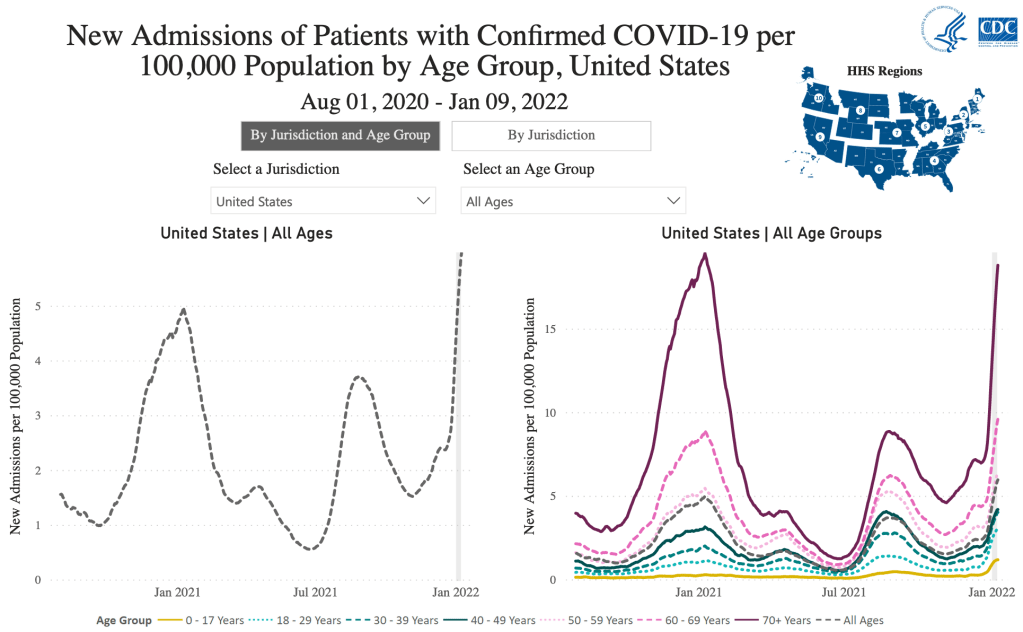
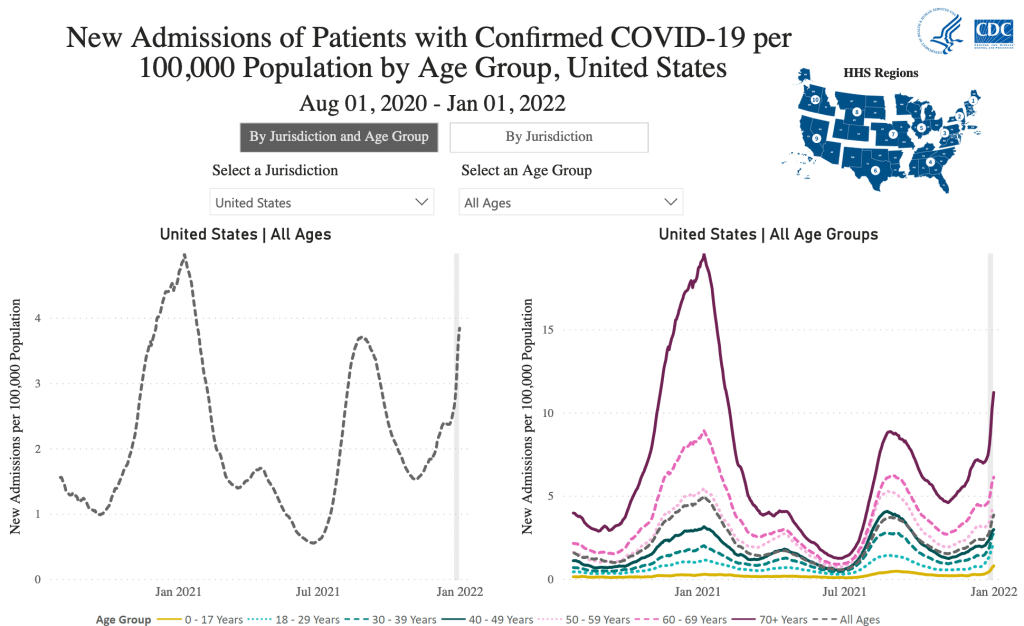
Hospitalizations in the US are up, but notice from the CDC graph that this is explicitly “Patients with Confirmed COVID-19”. Since all patients are screened for COVID, even those who were admitted for non-COVID reasons may be registered as a COVID admission. John Campbell has stated that about half of recent hospital COVID patients are “incidental”, meaning they were admitted for something else. For most Omicron patients, the symptoms are like a cold. Is is certain that many who have Omicron are not entering the medical system and are not seen in the new case numbers.
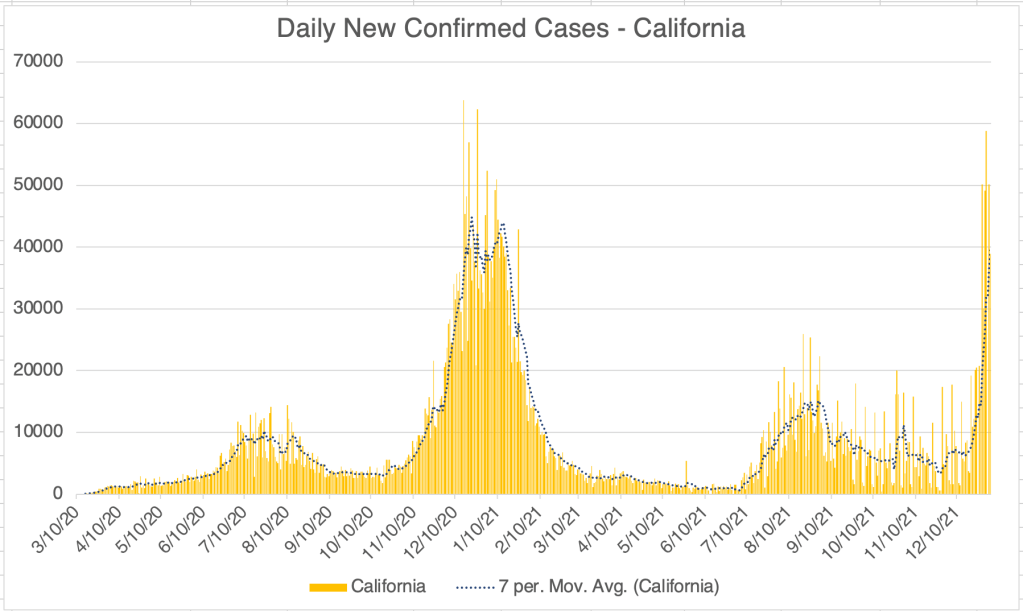
California and San Diego County are likewise experiencing very high numbers, although the case numbers in California are only just as high as last Winter, not higher.
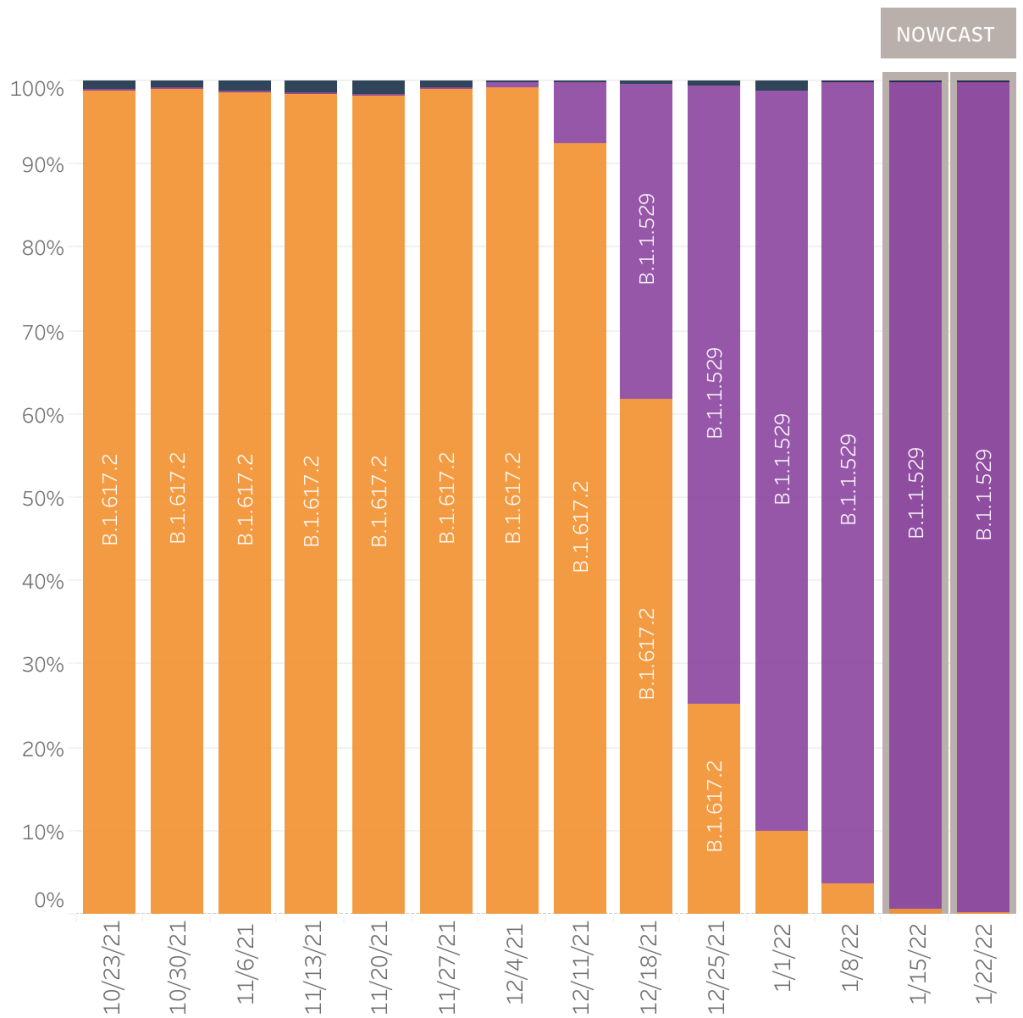
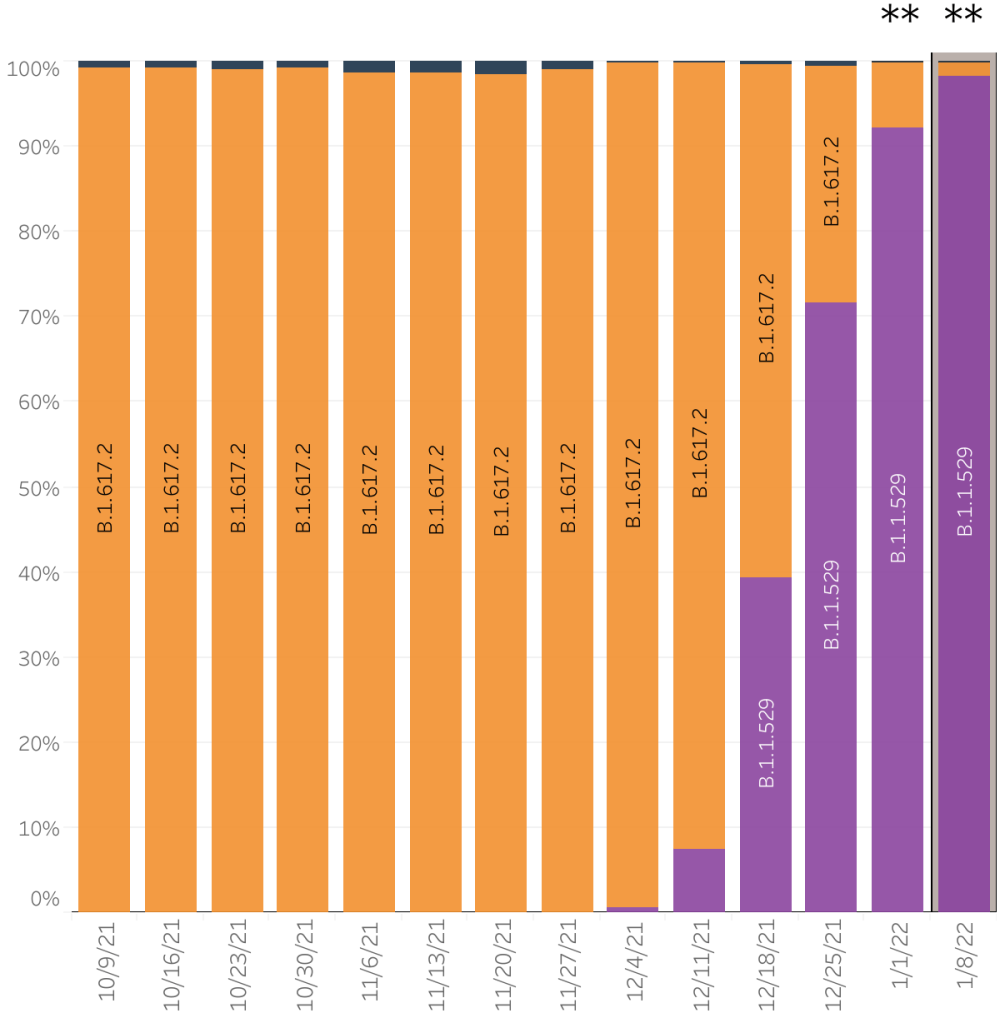
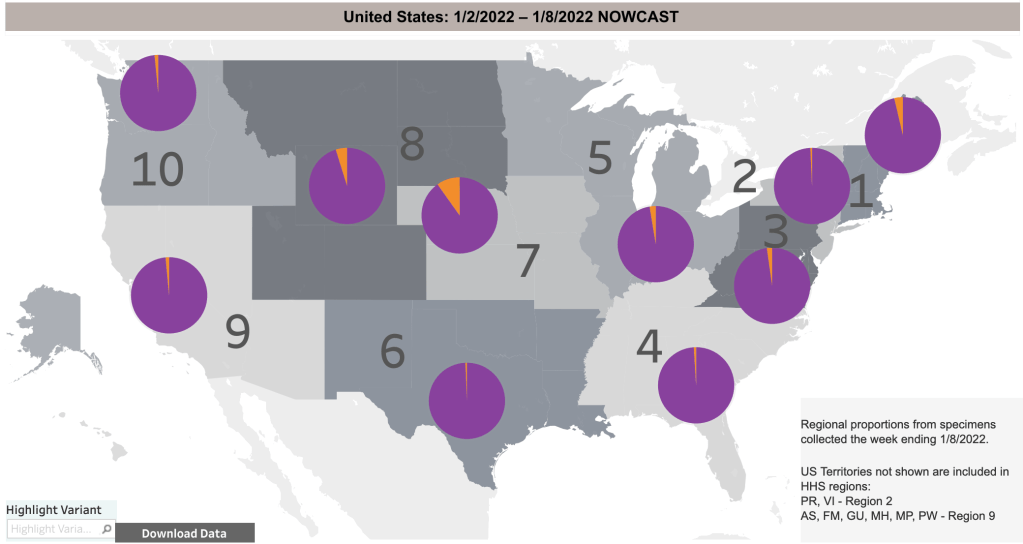
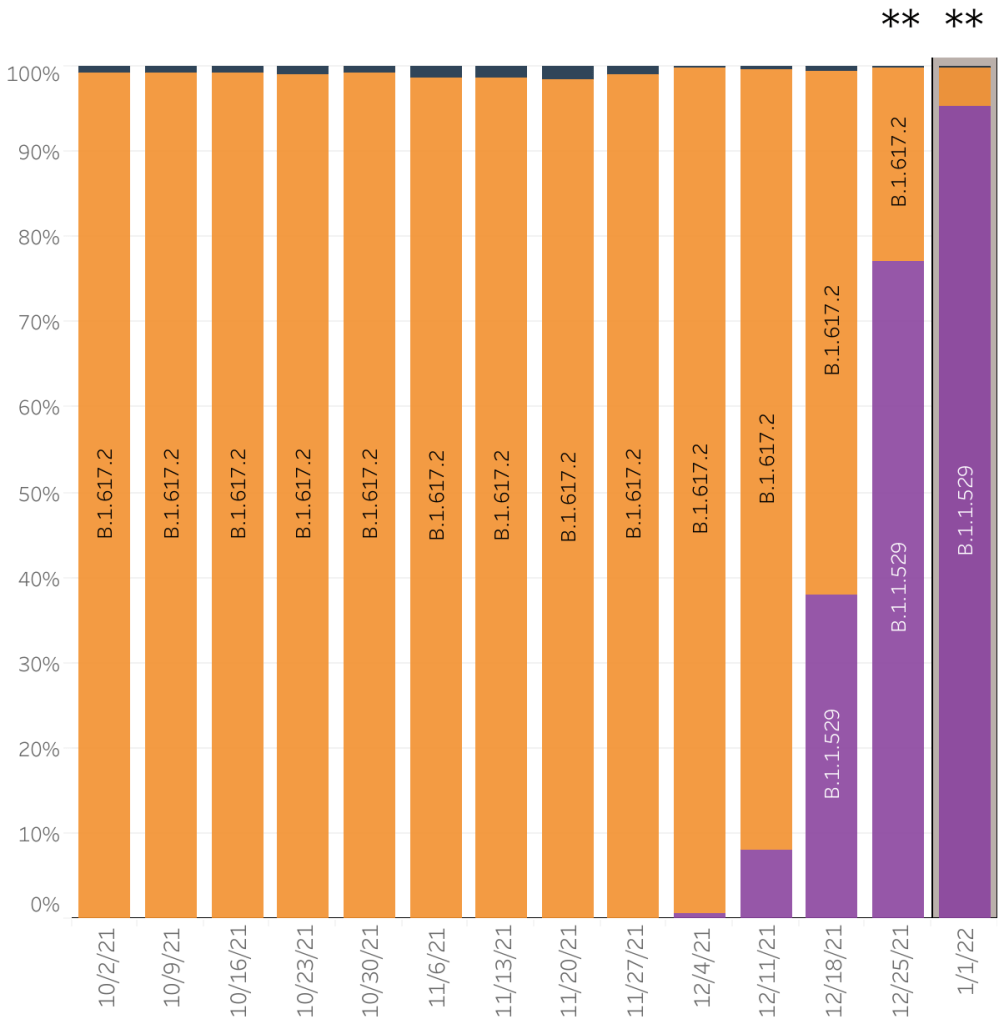
Omicron update: The CDC updated their page on variant proportions again just this morning. The estimate for the week ending 1/1/2022 is 95.7% Omicron, and just 4.6% Delta. The estimate for last week was upgraded from 58% to 77%. Remember that the last 2 weeks of data include “Nowcast” numbers based on computer modeling, and computer modeled numbers are only as good as the algorithm and the data that go into them.
The very high proportion of Omicron cases is very good news. Omicron is much less pathogenic (disease causing) than Delta. Most experience mild cold-like symptoms, and few experience fever, loss of taste and smell, inflammatory events, or blood clots.
My wife and I both experienced mild cold-like symptoms last week, and I think we both had Omicron. My symptoms were mild, even for a cold.
In addition, new data suggests that Omicron is in fact displacing Delta, and even that Omicron immunity protects against Delta infection. This is all fantastic and suggests that Omicron is in fact ending the Pandemic! Just a little cautionary note. I have a close friend who got COVID over the weekend, and she says it was Delta. No, I don’t know how she knows it was Delta. Her symptoms were severe, but not enough to be hospitalized. She was very sick for a few days, but is on the mend. So Delta is still lurking about.
Should you get a booster?: I’m going to say something you definitely won’t hear on the news right now. A study from Denmark suggests that the vaccines are about 55% effective against Omicron, and that effectiveness wanes quickly afterward. Given the possibility of an adverse reaction from the vaccines, mostly because of the Spike protein itself, my opinion is that vaccines are not an effective measure for Omicron infection. In a cost/benefit analysis, the costs of a booster outweigh the benefits. If you are in an at risk group, I would advise instead simply taking precautions like mask wearing indoors and avoiding indoor gatherings. If you wear a mask, use a medical grade mask like an N95, KN95, or KF94. Blue surgical masks, neck gators, and cloth masks are ineffective in protecting against infection. Of course, always consult your doctor when making medical decisions. I am a molecular biologist, not a physician, or an epidemiologist. This is my informed but not expert opinion.
Also, remember to keep supplementing Vitamin C, Zinc, and especially Vitamin D! Data keep rolling in that Vitamin D deficiency is heavily correlated to severe COVID symptoms!
Testing: I know several people with clear Omicron-like symptoms who were negative for COVID after using an at home rapid test. Is it clear that these tests are doing a poor job detecting the Omicron variant. If you need to know if you have COVID, you’ll need to get a PCR based test. Even those are missing some cases right now, but they are much more sensitive for Omicron than the rapid tests.
What if we get another variant?: Variants have had a huge impact these year. The vaccines were working great until the Delta variant appeared and messed everything up. Then Omicron showed up and changed everything again, this time for the better. Viruses tend to become more infectious and less pathogenic over time, and Omicron certainly fits that pattern. I’ve been asked “what if we have another variant?” The potential exists for another variant to come along and ruin the party like Delta did, but more likely, it will be less pathogenic than Omicron, especially since it will probably be most related to Omicron. So I’m not worried about new variants for the time being.
Omicron scorecard: Here’s my “scorecard” for this week. The new data from South Africa suggests that Omicron infection is “back compatible” with Delta, preventing Delta infection. This is great news and suggests Omicron infection will prevent future infections from other variants. As a reminder, I am not an epidemiologist, I’m a molecular biologist. This is my informed but not expert opinion.
1) Omicron must not use the ADE pathway to produce more severe cases: Looking at the available data so far, Omicron may preferentially infect those who have been previously infected, but cases are still mild, and fatality rates very low. So for now, this criteria is met.
2) Low fatality in older populations: South Africa has a relatively young population, so reports of mild symptoms may not carry over to countries with older populations. The UK data suggests that Omicron deaths will be low, even in older populations.
3) Displace Delta: Delta has a much higher case fatality rate in the US than Omicron appears to have. For Omicron to end the pandemic, it must displace Delta from the COVID population of strains. Data from the US and UK suggest this is happening!
4) Omicron must not circulate independently from Delta: Related to the above, if Omicron is very different from Delta, it may act as a completely different virus. There’s a chance that Omicron may displace Delta on the short term but still allow Delta to persist. Since Omicron is displacing Delta, it looks like this criteria may be met, but we won’t know for sure until we can see if Delta pops back up after the Omicron wave is over.
5) Omicron infection must immunize against future SARS-2: Since Omicron appears to infect those with immunity to Delta, it may be that it is different enough that it will not provide immunity to Delta or other SARS-2 strains. This criteria is not strictly necessary if Omicron completely displaces other SARS-2 strains (see 3 above), but it would be really nice to have some protection against future strains. We won’t know for sure about this one until a new version of COVID arises. The new data from Denmark suggests this criteria is met!