Originally posted on April 22nd, 2020 on Facebook
Friends,
This is a little longer post, this time with lots of science. I’ll talk about new measures of the fatality rate, some of the new Antibody testing, and also about the new re-opening guidelines. As always, consult with your doctor when making health care decisions!
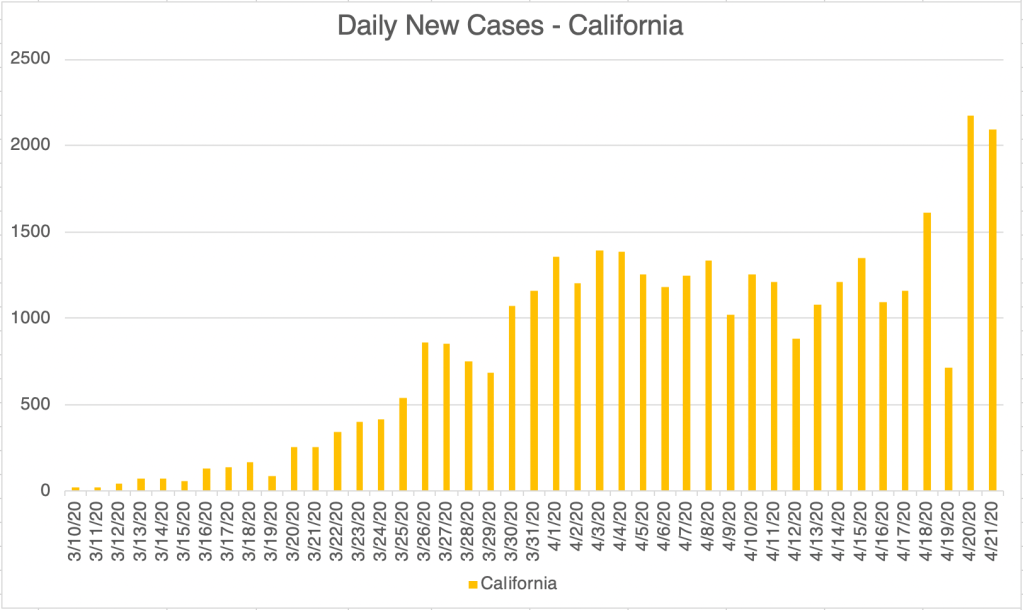
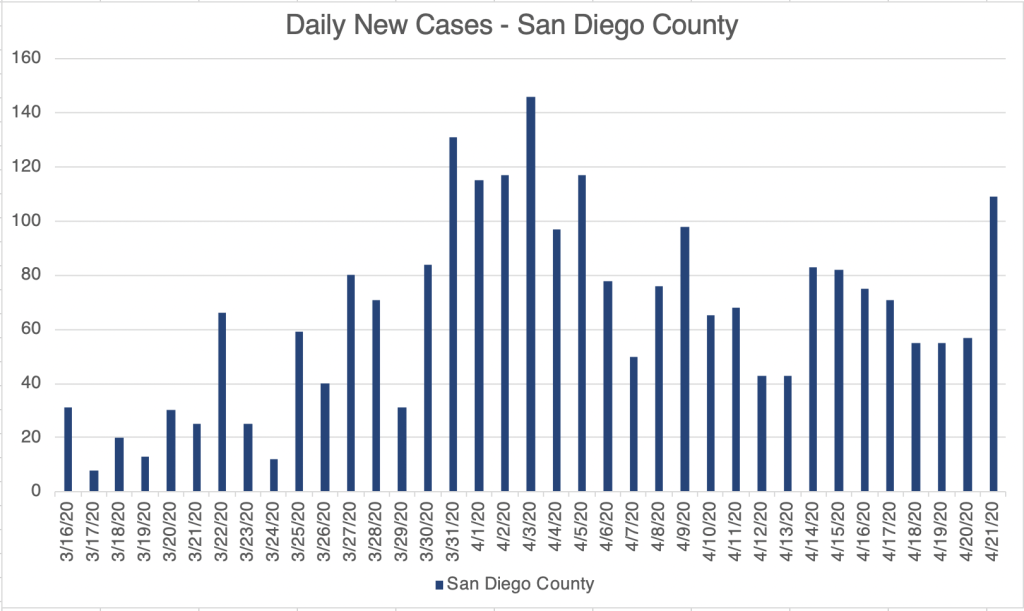
First, very briefly, I’ll just say that we have seen a big up-tick of cases in the last few days. I’m trying to be optimistic about this and assume for now that this is because of increased testing. The large labs have been purchasing new instruments of different types to broaden their offerings.
There have been a handful of studies trying to discern the number of asymptomatic cases. One recent study in New York tested all pregnant women coming in to deliver. It showed that at least in this sampling, there we about 7x more asymptomatic women testing positive for COVID than symptomatic women (Sutton et al, Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. April 13, 2020. NEJM, nejm.org). If this is roughly correct, then most confirmed cases numbers you see can be multiplied by 8 to get the real number of cases, as least until testing becomes more comprehensive. This also means the real fatality rate may be approximately 0.7%, about 5x higher than the typical flu.
Some have suggested that the fatality rate for COVID is the same as the flu, but this is the low end of new estimates, and for now, my guess is that it is higher. I think 0.7% is a good estimate for now. The rate for the typical flu 0.14%. Keep in mind that the Ro value for SARS-2 is about 5.7, much higher than the flu at 1.28.
On to Antibody tests! There has been a lot of excitement recently about antibody tests, and I have promoted them in my posts as well. As many of you know, the PCR based tests look for viral RNA in nasal swabs and detect an active infection. They are very sensitive, but they are more expensive, and need to be performed at specialized sites. Because the virus mostly lives in the lungs, nasal swabs don’t always collect virus from an infected person, and the false negativity rate has been estimated to be around 29%, at least initially. This is very high.
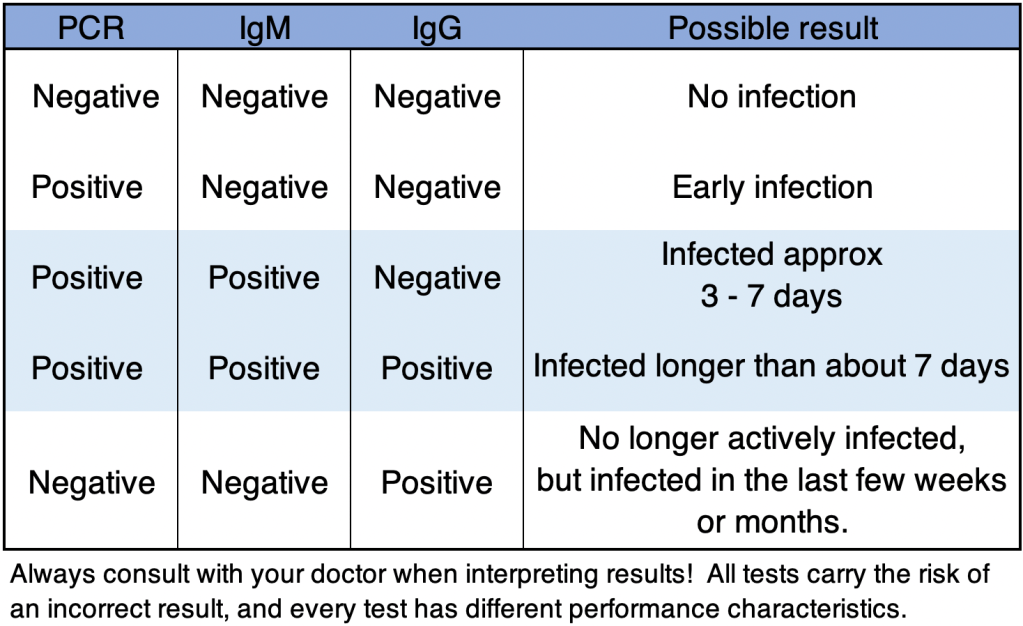
Antibody (Ab) tests detect an immune response by the patient by isolating antibody from the blood. Most detect 2 kinds of antibodies. IgM antibodies are produced during infection, and start appearing after about 3 days. IgG antibodies are produced later, at about 7 days, but continue to be produced for weeks to months after infection. The antibody tests are often less sensitive than the PCR tests, and they do not work during the first few days, since antibodies are not produced that early.
As you might guess, combining PCR and Antibody tests may give a good indicator if and even when an asymptomatic person was infected. Below is a table of possible interpretations of test results, assuming testing is accurate. Always confirm results and discuss with your doctor when making health care decisions! The FDA regulates testing in the US, and several tests have received Emergency Use Authorization (EUA) status. This is not FDA approval, but allows tests to be performed under emergency conditions. Several labs have started to perform antibody testing along with PCR. At first, Ab tests will be given in combination with PCR tests to see if health care workers have already been infected. If you want an antibody test, you’ll need to check with your doctor to see if you meet availability criteria. Many other companies have tried to offer tests without EUA status, including at home tests. Many of these tests have very high false negativity rates, and are basically no good! As of this writing, I would not use any at home test kit. Before taking any test, check with your doctor, or confirm with the FDA or CDC websites to see if a test has EUA status.
Re-opening: The federal government has released guidelines on the re-opening process. These are recommended guidelines, and most states are likely to adopt them, but the final decision will be up to the Governor of each state. I’ll provide the link below. In short, to enter the first phase of re-opening, states or counties must show a downward trajectory of cases and symptoms for 14 days, and must have certain hospital capacities and infectious disease surveillance procedures in place. Each additional phase can be entered if these conditions continue to be met for an additional 14 days. Some states or counties may already meet the criteria for phase 1, and some states plan to enter phase 1 on May 1st. Looking at the criteria, the guidelines seem reasonable to me, and I hope Governors will learn from the experiences of other countries and states while making these decisions.
Until next time, don’t fear, but be smart!
Erik
FDA Emergency Use Authorizations: