This is a brief case update. I’ll also make some more comments on BA.2 related waves in Europe, a new paper suggesting that vaccine mRNA persists in the lymph nodes. Also, new evidence from the UK suggests that vaccines lose potency after 6 months and certain vaccinated individuals are more likely to be infected than unvaccinated people.
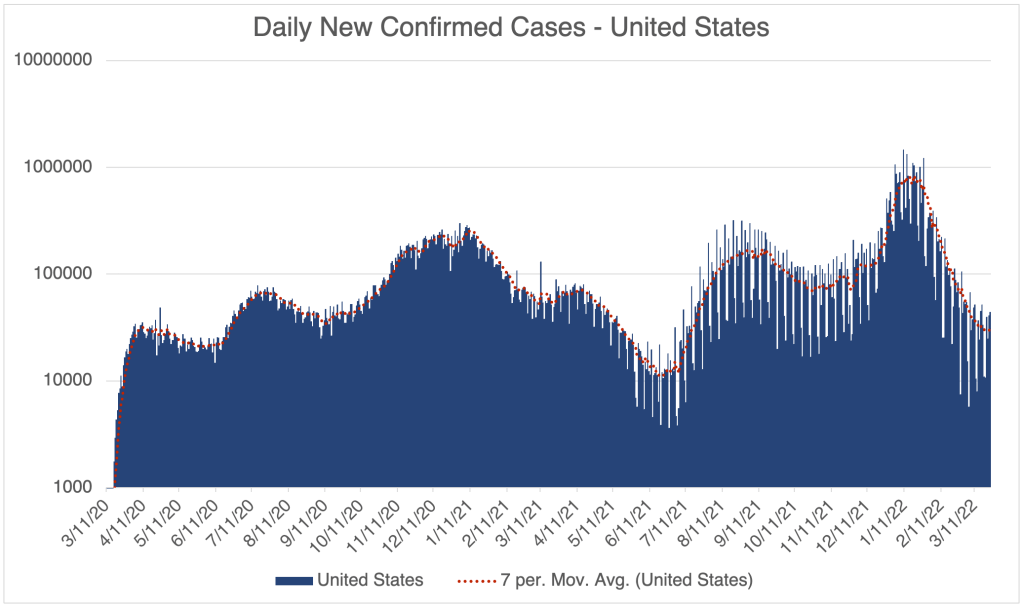
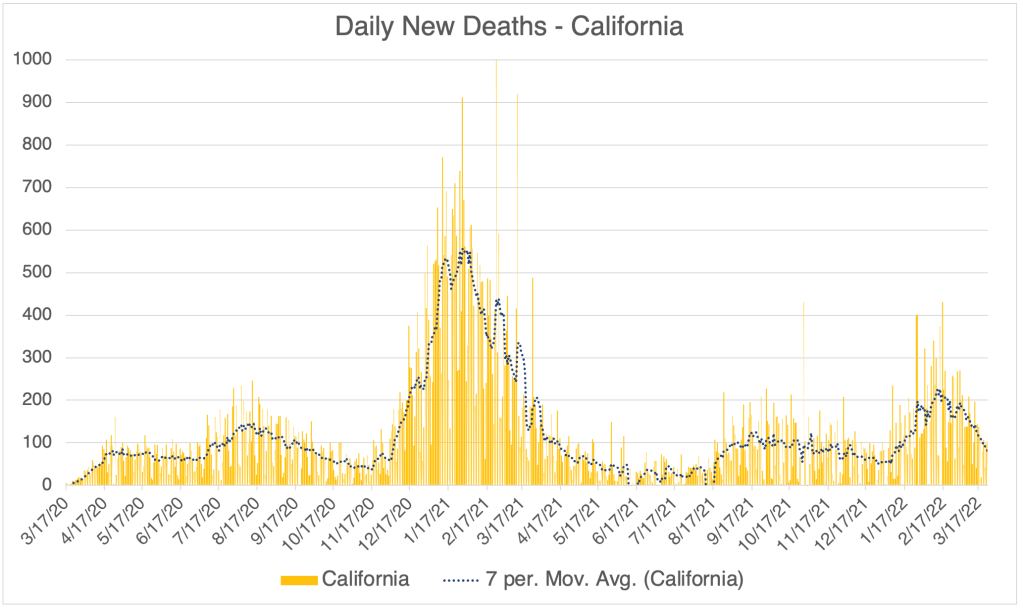
Cases continue to go down in the US, although the rate of decrease is slowing. As you’ll read below, some suspect that an Omicron variant, BA.2, may cause cases to rise in the US.



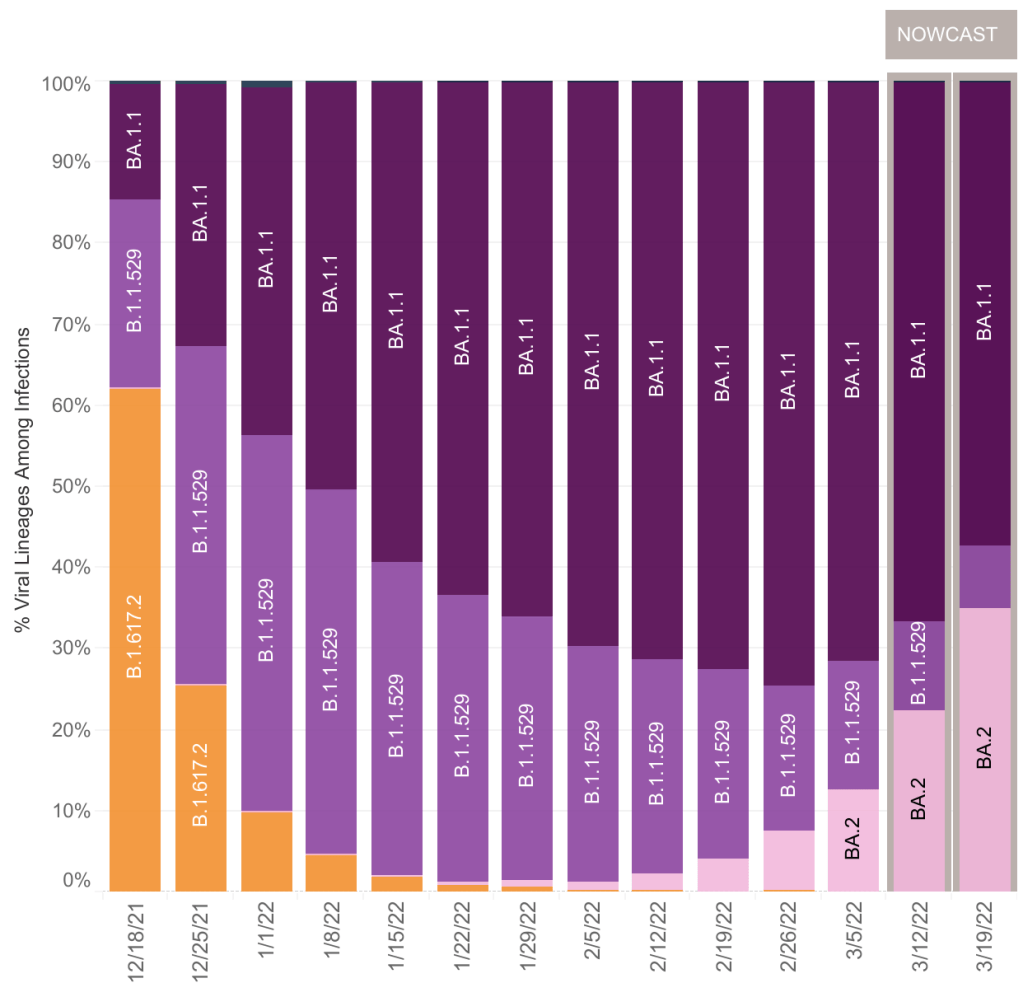
More on BA.2: I have commented on BA.2 before. This variant is a version of the Omicron variant, which is slightly more infectious than Omicron itself. It continues to follow the general trend of new variants being more infectious than older ones. Like the original Omicron, equal portions of B.1.1.529 and BA.1.1, BA.2 has a low fatality rate as compared to previous versions, including Delta.
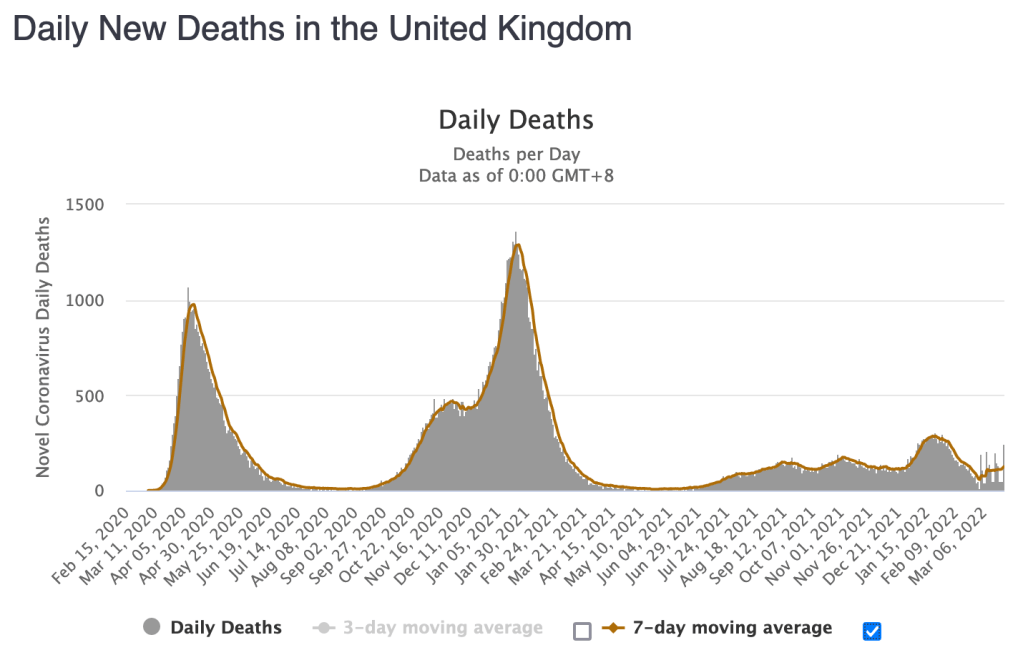
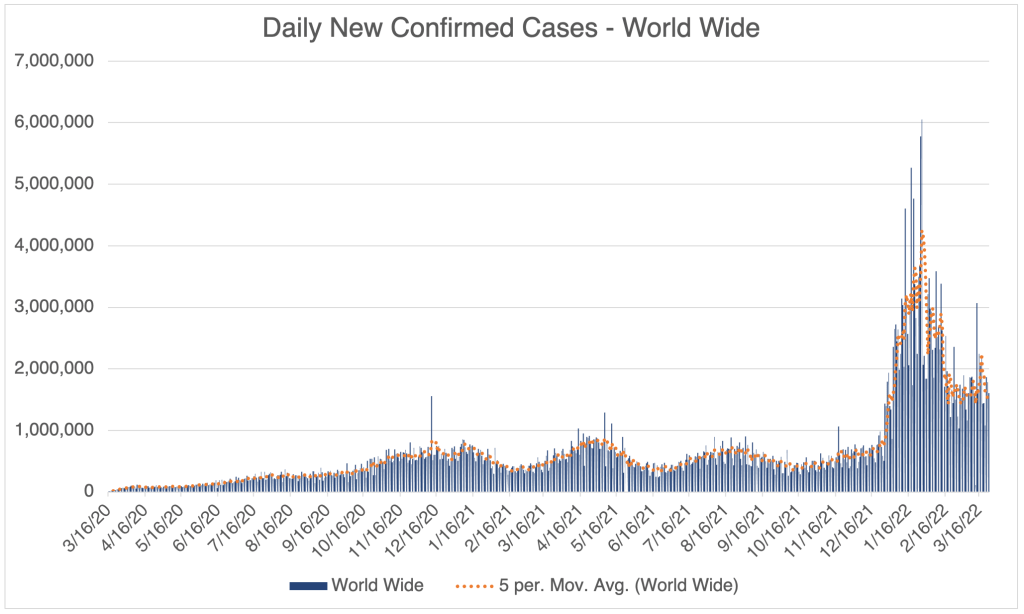
I originally held that BA.2 is not particularly interesting because of its similarity to the first Omicron strains. This still may be true, but some countries like the UK and the Netherlands have seen significant new peaks after BA.2 became prominent. BA.2 is likely contributing to rising cases globally.

Right now in the US, BA.2 is increasing in prevalence, and is currently 1/3 of SARS-2 found in the US. It’s similarity to previous Omicron versions means that it is displacing B.1.1.529 and BA.1.1, just like Omicron displaced Delta before it. We now have 0% Delta in the US.
Currently, new case numbers in the US are still going down, although the rate of decrease is slowing. John Campbell, a physician and COVID commentator in the UK, argues that a new peak in the US due to BA.2 is inevitable, and he may be right. But we aren’t seeing it yet. We may see it the next few weeks. Campbell also argues that “cases”, the number of infections recognized by the NHS, is much lower than actual infections. This is certainly true, but we can’t know how many infections there are, since they aren’t reported. This was almost certainly true in the US as well during the Omicron wave.
Does BA.2 significantly change the picture? I still say no, since the fatality rate with BA.2 is still very low, perhaps even lower than with other Omicrons. We may or may not see a significant BA.2 wave, depending on how many Americans already have resistance to BA.2. If you had Delta or Omicron, you almost certainly won’t get BA.2. Vaccination is only partially effective against Omicron variants.
Most people in my area, northern San Diego County, are basically going back to normal. This is warranted for most. If you have risk factors like age, obesity, or respiratory issues, you will want to remain vigilant and consider a booster. I do not recommend a booster for those without risk factors, and certainly not for those with natural immunity. Talk to your doctor when making medical decisions.
mRNA and Spike Protein Persist in Lymph System for up to 8 weeks: The Journal Cell just published a paper (Röltgen et al) which argues that mRNA and spike protein are present in vaccinated individuals for up to 8 weeks after vaccination. Cell is the third most highly respected journal in cell and molecular biology.
The cells in your body are surrounded by a fluid called “interstitial fluid”. This fluid carries nutrients from nearby blood vessels to your cells, and also carries waste back to the blood vessels. The lymph system is a one-way circulatory system that carries excess interstitial fluid from the extremities of your body back to veins near your arm pits. On the way, they pass through the lymph nodes, a biological filter and part of your immune system that checks for invading particles.
The Röltgen et al paper suggests that vaccine mRNAs from the interstitial fluid collect in the lymph nodes and can persist there for many weeks. They continue to produce spike protein during this time. Remember that vaccines are intended to be given in an intra-muscular manner, meaning that they are intended to be injected to a muscle and stay there. This paper shows that they are able to migrate to the lymph nodes.
The paper does not discuss the medical importance for this in terms of adverse events. Given the relative rarity of adverse events, I would guess that the presence of vaccine mRNA does not produce adverse events, and that these events are caused by vaccine injection into a vein. Again, the data is not conclusive on this, so this is just my guess at this point.
mRNA technology note: At this point, I have no evidence to suggest that the problem with the new vaccines is the mRNA technology. In my estimation, the likely reason the new vaccines lead to adverse events is that they produce the SARS-2 Spike protein which likely causes inflammation throughout the body. This may only be in vaccine recipients who receive a vaccination in a vein rather than an intra-muscular injection. If you choose to get a vaccination or booster, ask the health care provider to aspirate before injection.
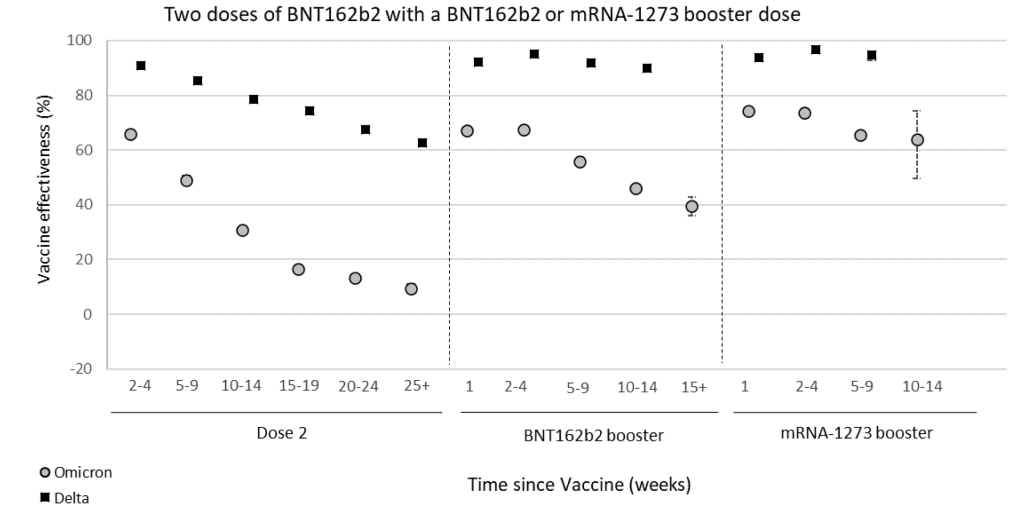
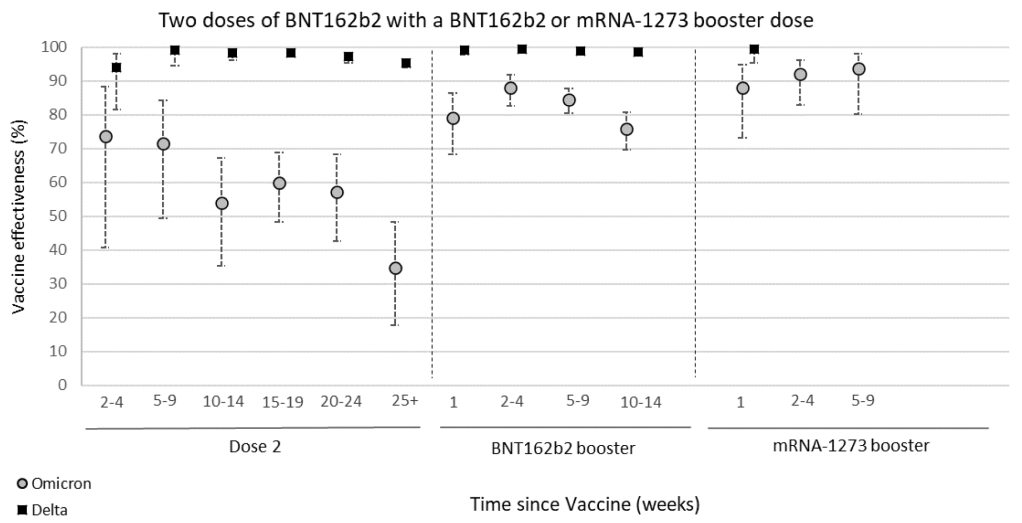
Certain vaccinated individuals are more likely to be infected by Omicron than the unvaccinated: A UK surveillance report shows that vaccine effectiveness against symptomatic Omicron infection goes from around 65% effective soon after 2 doses of vaccine, to around 5% 6 months later. Protection from hospitalization goes down to just 35% after 6 months. These findings suggest that to maintain full protection against Omicron, a vaccinated person will need to get a booster every 3 to 6 months.
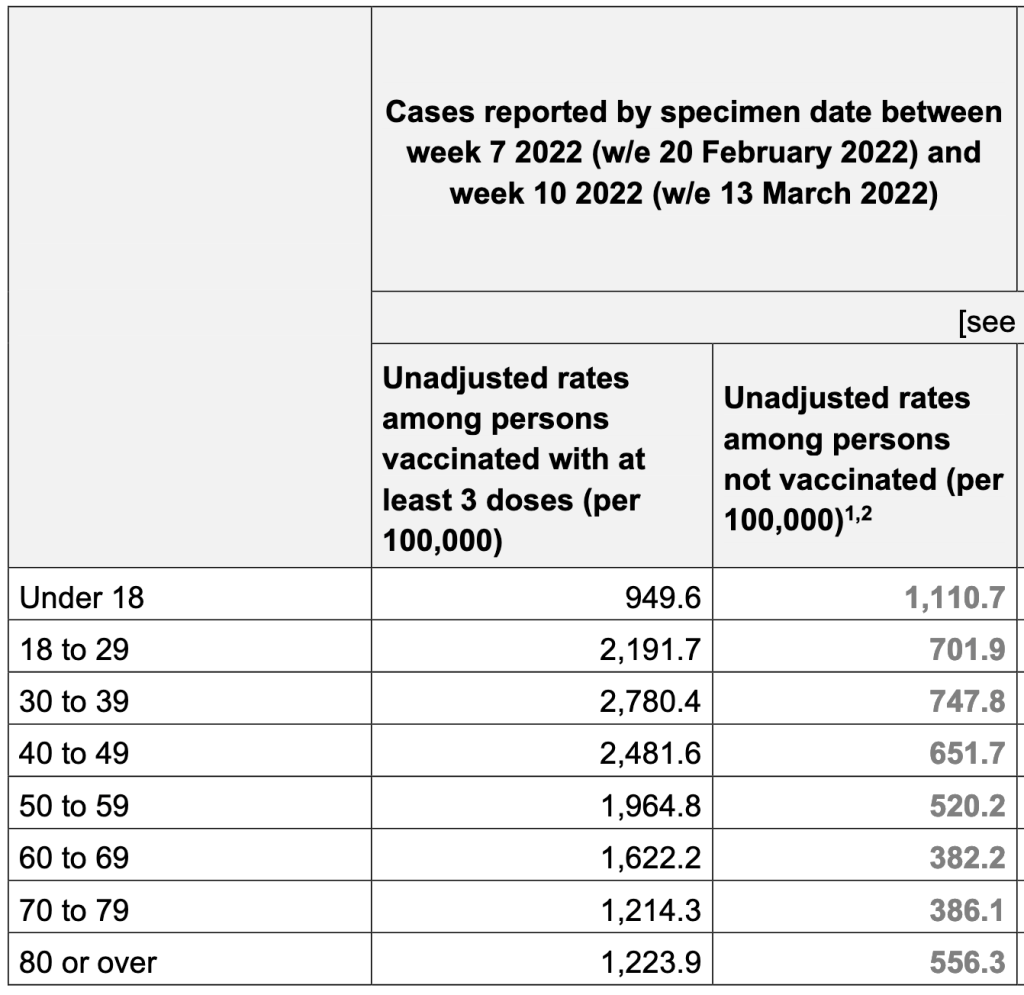
In another finding from the report, people with 3 doses of vaccine are 3x more likely to be infected with Omicron than unvaccinated individuals. This is the clearest evidence yet that Omicron may be using Antibody Dependent Enhancement (ADE) to infect people. The Lewnard et al paper from a few months ago has a similar finding. For both studies, a certain number of vaccine doses are more likely to increase the chance of infection. If viruses are using the ADE pathway, this effect would be explained more by the timing than by the number of doses per se. For ADE to work, a person needs to have a mediocre immune response to an agent, not a strong or weak one. Since we know vaccine mediated immunity goes down over time, then a person becomes more likely to be reinfected as their immune response goes from strong to mediocre.
So should you get a booster? Again, if you have risk factors like age, obesity or respiratory problems, you might want to get a booster every 3 – 6 months. Otherwise, you may choose instead to just take extra precautions as Omicron cases continue to fall in the US. If you choose to get a booster, ask them to aspirate before injection. Talk to your doctor when making medical decisions.
I know this is all very complicated. Your questions will help me make this more clear.
Don’t fear, but be smart,
Erik

5 thoughts on “Case Update, March 25, 2022; BA.2 cases in Europe, Persistence of Vaccine mRNA in Lymph Nodes, Higher Omicron Infection in Vaccinated individuals in UK”