Category Archives: All Articles
What is the Fatality Rate?, Antibody tests, Re-opening
Originally posted on April 22nd, 2020 on Facebook
Friends,
This is a little longer post, this time with lots of science. I’ll talk about new measures of the fatality rate, some of the new Antibody testing, and also about the new re-opening guidelines. As always, consult with your doctor when making health care decisions!
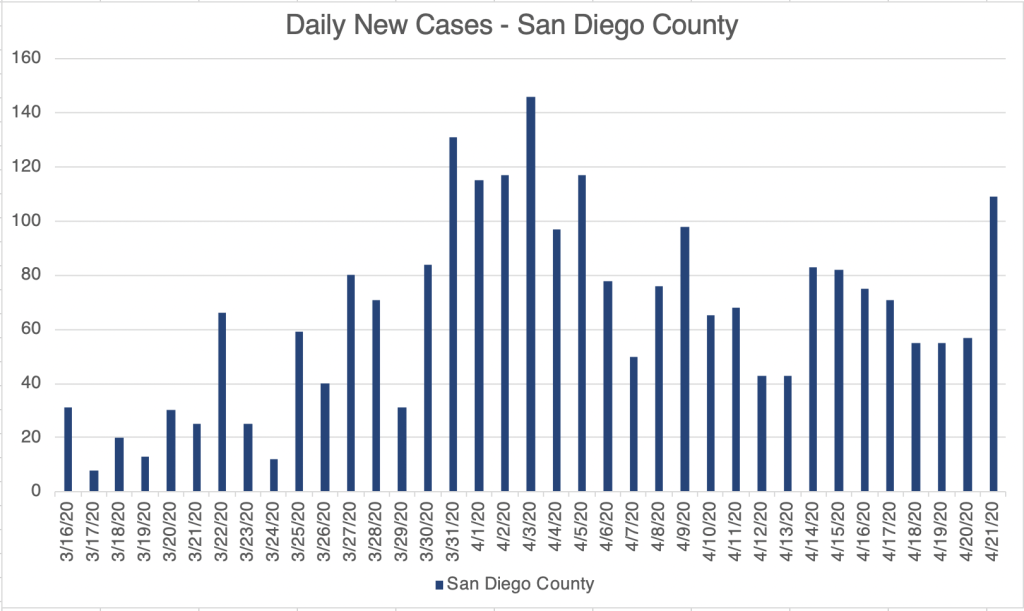
First, very briefly, I’ll just say that we have seen a big up-tick of cases in the last few days. I’m trying to be optimistic about this and assume for now that this is because of increased testing. The large labs have been purchasing new instruments of different types to broaden their offerings.
There have been a handful of studies trying to discern the number of asymptomatic cases. One recent study in New York tested all pregnant women coming in to deliver. It showed that at least in this sampling, there we about 7x more asymptomatic women testing positive for COVID than symptomatic women (Sutton et al, Universal Screening for SARS-CoV-2 in Women Admitted for Delivery. April 13, 2020. NEJM, nejm.org). If this is roughly correct, then most confirmed cases numbers you see can be multiplied by 8 to get the real number of cases, as least until testing becomes more comprehensive. This also means the real fatality rate may be approximately 0.7%, about 5x higher than the typical flu.
Some have suggested that the fatality rate for COVID is the same as the flu, but this is the low end of new estimates, and for now, my guess is that it is higher. I think 0.7% is a good estimate for now. The rate for the typical flu 0.14%. Keep in mind that the Ro value for SARS-2 is about 5.7, much higher than the flu at 1.28.
On to Antibody tests! There has been a lot of excitement recently about antibody tests, and I have promoted them in my posts as well. As many of you know, the PCR based tests look for viral RNA in nasal swabs and detect an active infection. They are very sensitive, but they are more expensive, and need to be performed at specialized sites. Because the virus mostly lives in the lungs, nasal swabs don’t always collect virus from an infected person, and the false negativity rate has been estimated to be around 29%, at least initially. This is very high.
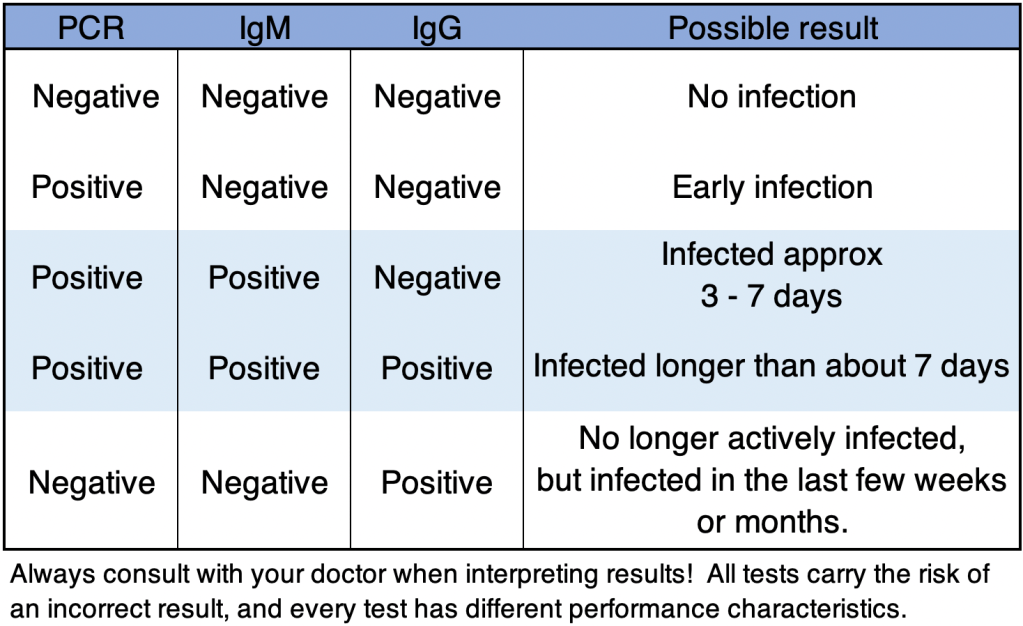
Antibody (Ab) tests detect an immune response by the patient by isolating antibody from the blood. Most detect 2 kinds of antibodies. IgM antibodies are produced during infection, and start appearing after about 3 days. IgG antibodies are produced later, at about 7 days, but continue to be produced for weeks to months after infection. The antibody tests are often less sensitive than the PCR tests, and they do not work during the first few days, since antibodies are not produced that early.
As you might guess, combining PCR and Antibody tests may give a good indicator if and even when an asymptomatic person was infected. Below is a table of possible interpretations of test results, assuming testing is accurate. Always confirm results and discuss with your doctor when making health care decisions! The FDA regulates testing in the US, and several tests have received Emergency Use Authorization (EUA) status. This is not FDA approval, but allows tests to be performed under emergency conditions. Several labs have started to perform antibody testing along with PCR. At first, Ab tests will be given in combination with PCR tests to see if health care workers have already been infected. If you want an antibody test, you’ll need to check with your doctor to see if you meet availability criteria. Many other companies have tried to offer tests without EUA status, including at home tests. Many of these tests have very high false negativity rates, and are basically no good! As of this writing, I would not use any at home test kit. Before taking any test, check with your doctor, or confirm with the FDA or CDC websites to see if a test has EUA status.
Re-opening: The federal government has released guidelines on the re-opening process. These are recommended guidelines, and most states are likely to adopt them, but the final decision will be up to the Governor of each state. I’ll provide the link below. In short, to enter the first phase of re-opening, states or counties must show a downward trajectory of cases and symptoms for 14 days, and must have certain hospital capacities and infectious disease surveillance procedures in place. Each additional phase can be entered if these conditions continue to be met for an additional 14 days. Some states or counties may already meet the criteria for phase 1, and some states plan to enter phase 1 on May 1st. Looking at the criteria, the guidelines seem reasonable to me, and I hope Governors will learn from the experiences of other countries and states while making these decisions.
Until next time, don’t fear, but be smart!
Erik
FDA Emergency Use Authorizations:

Rt Live
Originally posted April 20th, 2020 on Facebook
Friends,
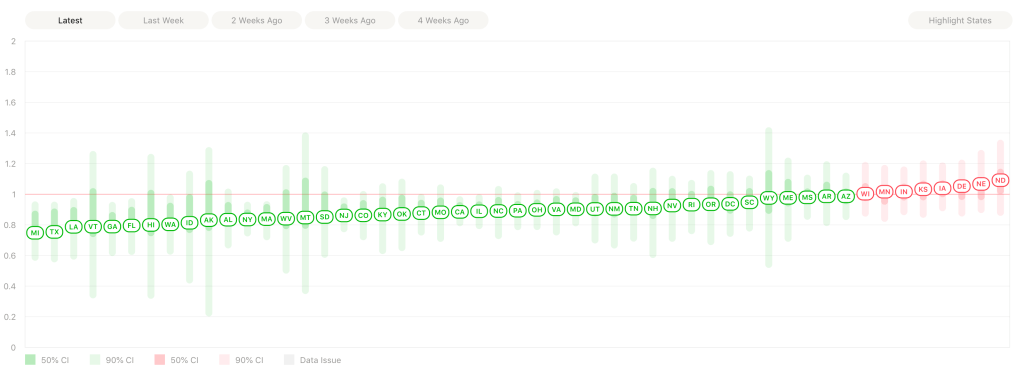
Mark Rasmussen sent me a link today that you’ll be interest in. It’s a new site that tracks the Effective Reproduction Number, Rt.
Ro, which we’ve talked about before, is a measure of infectiousness, and is the average number of people that a person would pass a virus to in it’s natural state, in a completely naïve population, and with no counter measures. For SARS-2, this number is 5.7. Rt is similar, but takes into account the measures we have taken to counter it. The Ro doesn’t change, but Rt does. The site shows the current Rt for every US state, and also shows a graph of Rt over time. Above 1.0 is bad, because that means each person is spreading the virus to at least 1 other person. Below 1.0 is good, and means the number of infected people is beginning to go down in that state. And yes, this is for confirmed cases only. There are more. We can only graph what we have information on.
The results are very interesting. For California, the state was below 1.0 for a few days, but as of April 20th, has climbed back up. This pattern is true of several states on the site, It appears many states started to climb as good news was coming out last weekend! Apparently people started feeling confident, and were less careful. An alternate explanation is that as testing is done on broader range of people, more cases are found.
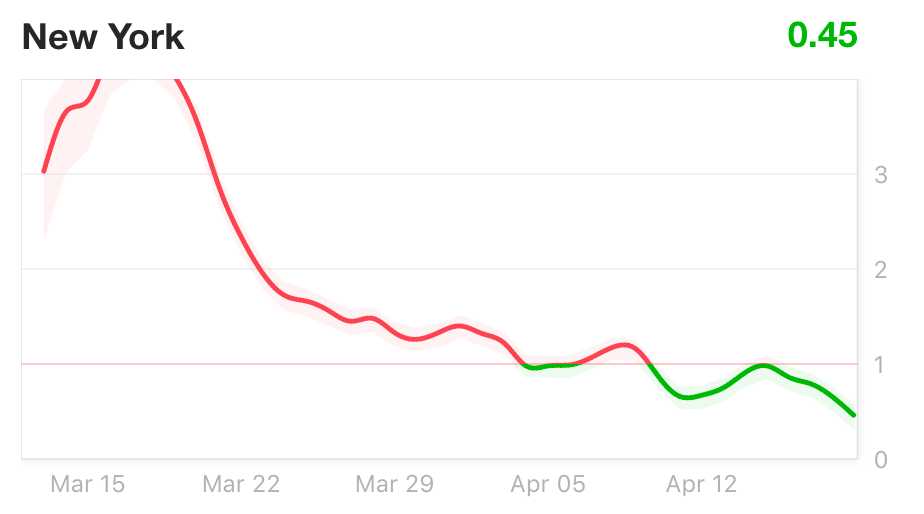
As we discussed before, New York state has had a very rough start, with more confirmed cases than any other state, and indeed more than any other country, except perhaps China. Recently, however, they’ve done much better, and have had an Ro below 1.0 since April 10th or so.
Using this site, you can see how your state is doing, and we can watch almost in real time, how the reopening process is affecting each state. This will really help us find the right approach.
Erik

When should we re-open? Opposite valid interests
Originally posted April 13th, 2020 on Facebook
Friends,
This will be a longer post, so buckle up!
While I certainly have political opinions, I’ve been trying to minimize them for the purposes of these posts, in order that more of you will be willing to read! Today, some of you may be able to figure out where I stand on some things, although I’ll still try to keep the controversy to a minimum. This last weekend, there were protests in many cities of the US asking for the economy to be opened up. Of course, most of these requests took the form of slogans shouted or written on signs, rather than specific policy proposals. I’m very sympathetic to the need of many to get back to work so they can provide for their families, pay the rent, etc. I also share the frustration that much of the information provided by the media and government agencies is untrustworthy or incomplete. This is why I write these posts!
I want to reiterate the differences between the typical flu and the SARS-2 virus:
The R0 value (a measure of infectiousness, see my April 13th post) for the flu is 1.28. For SARS-2, it’s 5.7, 4.5 times higher!
The incubation time for the flu is 2-4 days, for SARS-2, it’s 2-14 days, and asymptomatic people are often contagious!
Yes, the fatality rate for both is impossible to know. And it’s probably over-estimated for both, since we don’t know the number of infected people with mild to moderate symptoms for either disease. But estimates are that the fatality rate for the typical flu is 0.14%. The current rate for COVID-19 in the US is 5.36% (deaths/confirmed cases), 38 times higher.
In short, SARS-2 is not the typical flu.
We have to concede that in an event like this one, there are many valid interests that are in some ways are opposed to each other. People at risk want to stay safe. Doctors and nurses want to treat their patients, but also face constant exposure of themselves and their families to the virus. Those in government do not want to expose their constituents to unnecessary risk. On the other hand, many have lost their jobs and need to get back to work. Mental health workers worry that their patients cannot withstand prolonged isolation and stress. Employers wonder if they have to lay off more people or close their businesses. All of these are real concerns, and they can’t be dismissed.
It will be difficult moving forward to strike a balance between these competing interests, and no solution will be perfect. We need to understand that most are doing their very best to manage a very difficult situation. There is lots of blame to go around, but remember that the nature of the virus has never been completely clear. For myself, I gave a talk at my church on March 13th (Posted here on March 18th). During the previous week, I was trying to determine if the virus was spread by droplet transmission (coughing and sneezing), or by aerosol transmission (shouting, laughing, singing, even talking). At the time, most outlets including the CDC said it was only spread by droplet transmission, but a few scientists were warning that it may be aerosol. Should I really be giving a talk on virus safety to room full of people? It appeared at the time that it would be OK, so I moved forward. Luckily for me, the decision was made to cancel gatherings, and my talk was recorded for the web. As it turned out, the SARS-2 virus is much more infectious that originally thought (see my post from April 13th), so add me to the list of people who were wrong! Thank God I didn’t have a crowd in the room during my talk!
Again, I am not an epidemiologist, I am a molecular biologist specializing in infectious disease. But in my informed opinion, reopening the economy without great care is a mistake. A similar experiment has already been done. On March 11th, California Governor Gavin Newsom banned large gatherings including sporting events, church services, and university classes. On the same day, New York Mayor Bill De Blasio was encouraging people to eat out and enjoy themselves. As of this writing (April 19th), California has 31,000 confirmed cases, and New York City alone has 138,000, more than all but 6 countries (yes, I’m including China, the Chinese Communist Party is almost certainly heavily under-reporting their case load)1. For a time, New York hospitals were overwhelmed, and bodies were being temporarily buried on Hart Island. This is the possible consequence of going back to normal too quickly! If you choose to gather in large groups during this time (for example at protests in downtown San Diego), I would strongly encourage you to take extra care to isolate yourself from those at risk or those who may come in contact with them.
I am less sympathetic to those who want to get back to normal just so they can go to Disneyland or to their favorite restaurant. As we reopen the economy, we have to do so carefully. Theaters, restaurants, and amusement parks are among the last things that should be reopened.
We will need have adequate testing and hospital capacity to handle the additional case load. Each area will be different in this regard, and New York City should not be treated the same as Ennis, Montana. We will also need to have grace for one another, as well-intentioned mistakes will be made along the way. Ideally, we should also have contact tracing, contacting those potentially exposed to an infected person. This practice, along with aggressive testing, was used very effectively in Taiwan, So. Korea, and Singapore, to minimize caseload. Unfortunately, we are not yet able to do contact tracing in the US.
While I am very sympathetic to individual rights, and am in general for small government, we may need to voluntarily lay down certain rights for a time in order to protect each other. Pray for our leaders, regardless of party, and take care of each other!
I’ll have another post soon on the topic of antibody testing.
Don’t fear, but be smart!
Erik

1 Editor’s note: As of the date of posting, the statistics here were correct. As of July 7, 2020, however, the situation has reversed. New York State as 398k confirmed cases, California has 284k confirmed cases. New York state daily cases are trending downward, while California daily cases have been trending upward.
Case Update: April 13th
Originally posted April 13th, 2020, on Facebook
Friends!
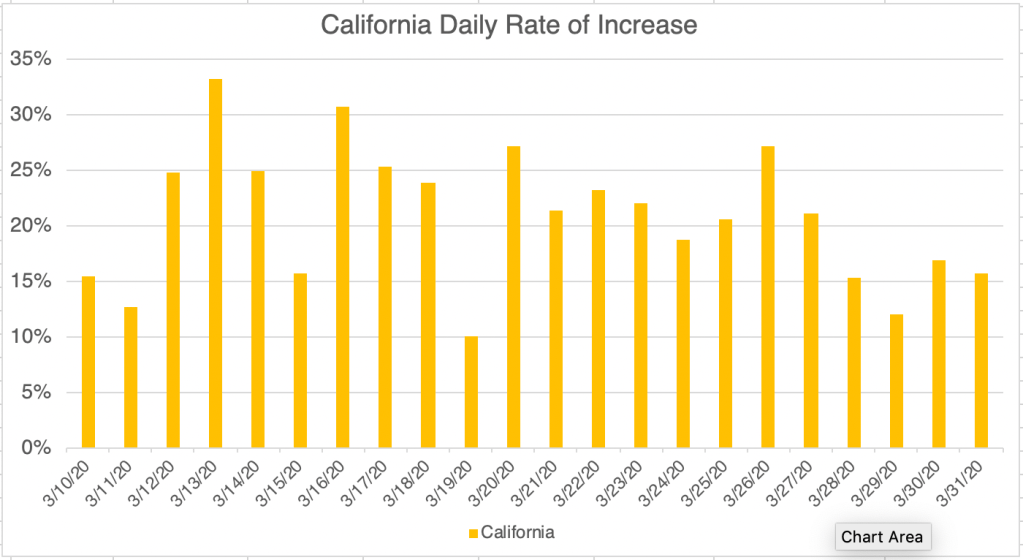
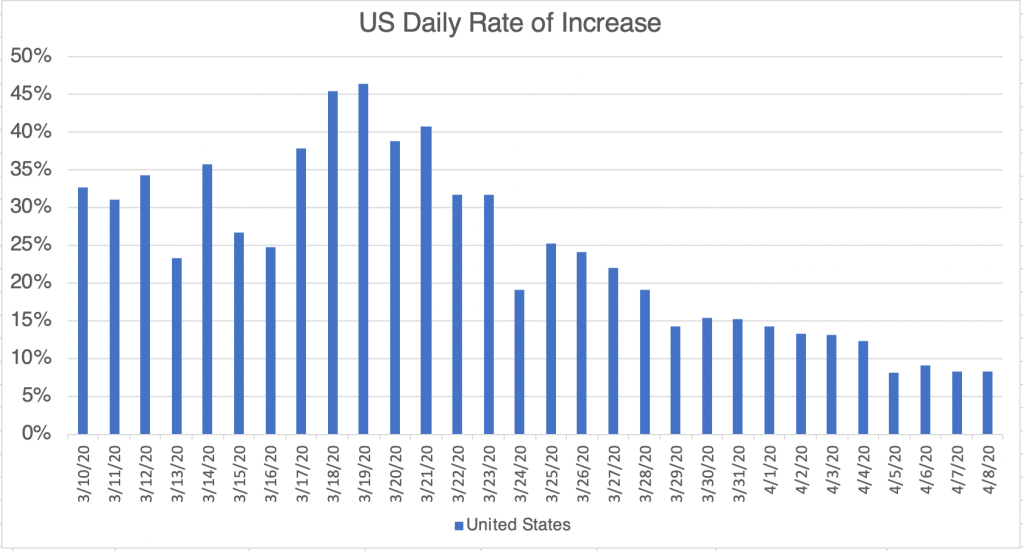
I have another good news/bad news post for you today. First the good news. Yesterday, 8pm on April 12th, the rate of new infections for the world, the US, California, and San Diego County, were all below 5%! Our efforts are paying off!
Some of you may wonder if this is a Sunday Effect, a lowering of new case numbers just because it’s a Sunday, and there may fewer people performing tests that day. While it’s certainly true that there have been fewer new cases on Sunday, I noticed that in past weeks, a Sunday drop has often been followed by a lower rate for the entire next week. Last week for example, the rate was below 10% on Sunday, a big drop, but remained low for the entire next week. If this trend holds, then we may have rates near 5% for the entire next week.
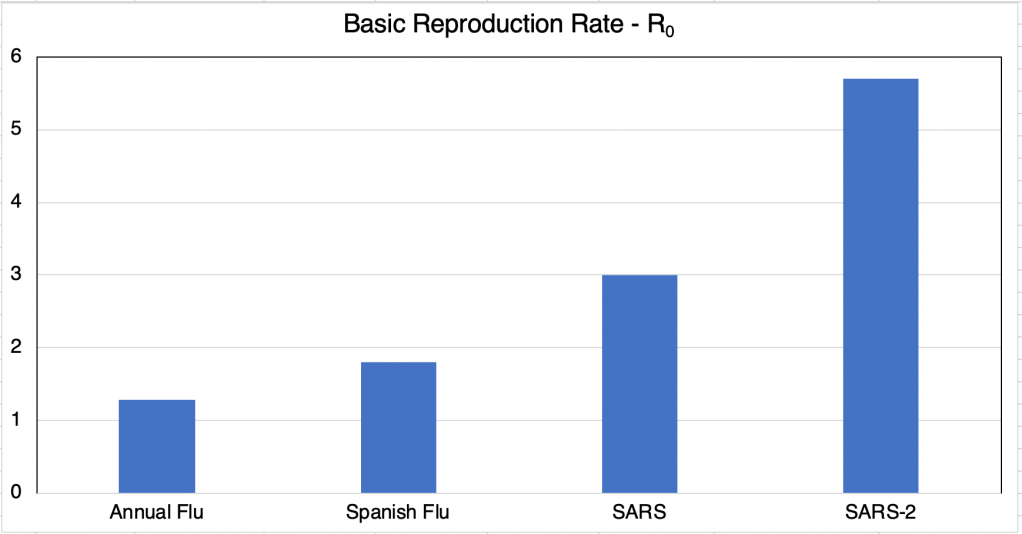
The bad news isn’t really new, but rather a new study of the Basic Reproductive Number (R0). This number is a measure of infectiousness and is an attempt to calculate the average number of people that an infected person will pass the virus to. For a typical flu, this number is 1.28. For the first SARS virus in 2002, it was around 3. As recently revealed in a pre-publication paper [Sanche et al. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. July 2020, pre-print captured April 13th, 2020. Em. Inf. Dis. 6(7)], the actual R0 value is 5.7, twice as high as originally thought, and 4.5 times more infectious than the typical flu.
Early on, there was a lot of discussion on whether this virus was spread by droplet transmission (coughing and sneezing) or by aerosol transmission (singing, laughing, shouting, even just talking). The new paper, along with several stories in the news, suggests that SARS-2 is indeed spread at least to some degree by aerosol transmission.
So here’s the take away from this post. We are doing better, but we’ll have to be very careful how we “go back to normal”. The virus has the potential of springing back to life if we just go back to normal right away. If people are to go back to work anytime in the next few weeks, we will need to remain diligent, yes, possibly wearing masks at work, and do wider spread testing to find infected people. Stay tuned on this evolving situation!
Don’t fear, but be smart!
Erik
PS Pre-published journal articles have not yet received final approval and may change before publication!
Case Update: April 9, When can we go back to normal?
Originally posted April 9th, 2020 on Facebook
Friends,
You may have heard lots of positive news in the press in the last few days about new lower rates of new infections in the US. If you saw my posts on March 30th and April 1st, you know that I was enthusiastic about some good news a little earlier than was warranted. So I wanted to wait a few days to see if the current positive trends would hold.
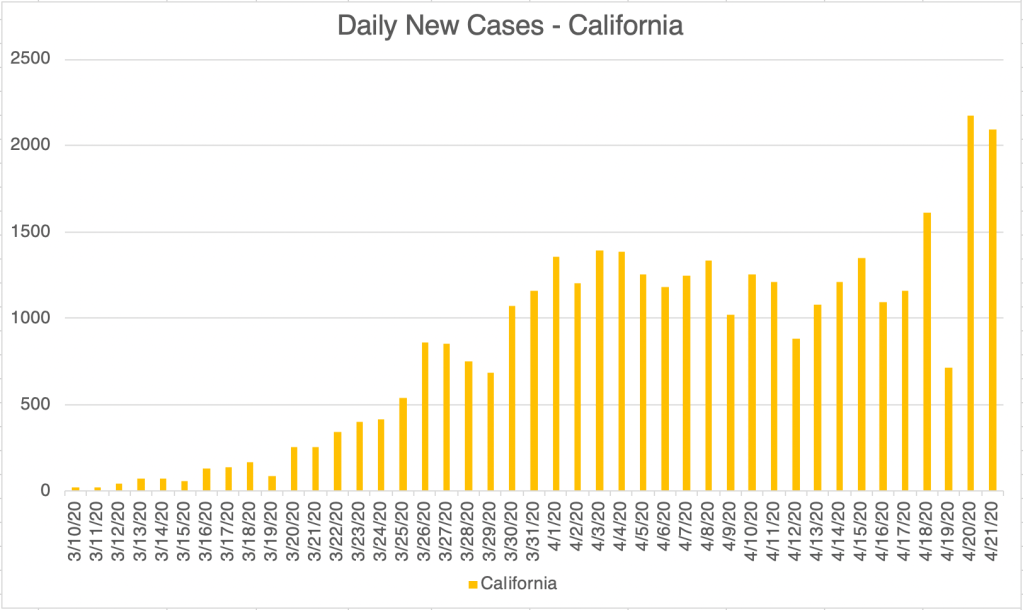
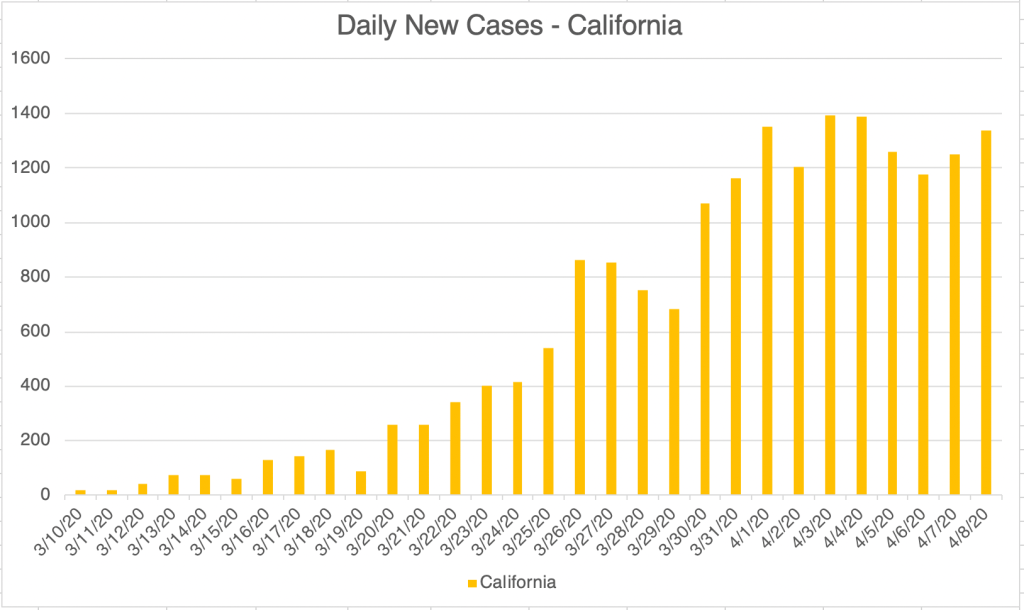
All that being said, I do have good news for you today! For the World, the US, California, and San Diego County, the rate of new cases as been below 10% every day since Sunday, April 5th! That’s great news. The actual daily new cases has been trending basically flat in the US since Sunday, and in California since April 1st. So the news is definitely good! There is even better news if you live in San Diego County. Daily new cases actually appear to have peaked on April 3rd, and are actually down since then.
Some in the media are discussing an end to our isolation, but I have to say that it is still very important that we continue to practice social distancing for a while longer. Our efforts are working, but we still have a lot of work to do!
My brother asked me when I thought it would be safe to go back to normal. I’ll preface my opinion by saying that I am not an epidemiologist. My opinion on this is informed, but I’m not an expert. In my opinion, we can go back to normal when:
- Our daily new cases are very low, a few a day.
- We can be reasonably certain that we know where every sick person is located, and that they are isolated.
- That we have enough testing capacity that we can test those who have been potentially exposed, not just confirming cases that appear to be COVID-19 cases by symptoms.
You can see that we have quite a ways to go to achieve these 3 criteria. So it’s important that we remain diligent! It is highly likely that we will experience a second wave of infections if we try to go back to normal too early.
A local physician told me last week, April 1st that wait times for testing was 12 days. Yesterday, Wednesday, April 8th, he said that results were coming back in just 2 days. So with new cases falling, we are able to test much faster. This will eventually give us capacity to test for exposure! I don’t know if public health officials are considering this yet.
So be encouraged, but be diligent! Your efforts are paying off!
Don’t fear, but be smart!
Erik



Hugs, not Drugs: Oxytocin and Stress Reduction
Originally posted on April 7th, 2020
Friends,
I still have some science for you today, but from a little different angle. Many of you know that we make a hormone, Oxytocin, that makes us feel good and is produced when we make physical contact with the people that we love, spouses, family, friends, etc. I was listening to a podcast the other day, in which a scientist was talking about how many of us are experiencing extra stress these days either because of isolation, or perhaps because of overexposure to some of those same loved ones! 😬
This scientist recommended 2 things: First, a 20 second hug every 2 hours! This produces Oxytocin, lowers Cortisol, the stress hormone, and makes us feel better. Your teenagers may think it’s totally weird, but I think they may secretly like it!
Second, he also said that we also get a shot of Oxytocin when we meet an old friend, or simply make eye contact with someone we care about. So when interacting with friends on line, seek to de-emphasize Facebook (yes, I get the irony), email, and phone calls, and emphasize FaceTime, Zoom, or some other tech that allows eye contact! This is especially important for those who are isolated during these times!
I checked all this with Dr. Scott Bunner, a psychiatrist friend of mine, and he said the hugging thing is pretty well known. He hadn’t heard of the eye-contact thing, but that it made sense to him.
So give grandma a FaceTime call! If you’re in the position to do so safely, help an elderly person get set up for Zoom! It will help us all get through this!
Don’t fear, but be smart!
Erik
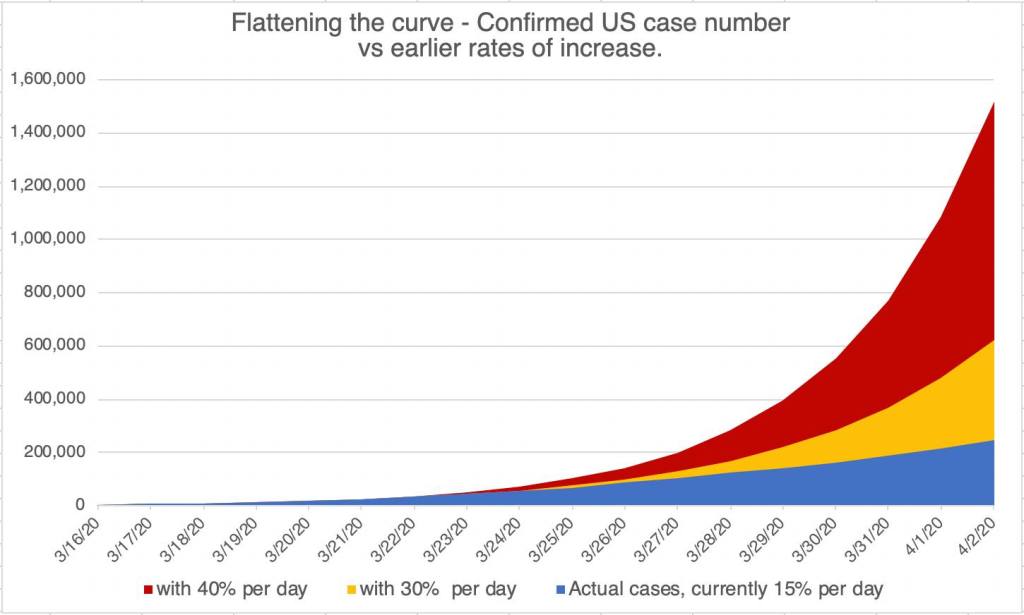
Are We Flattening the Curve?
Originally posted April 3rd, 2020 on Facebook
Friends,
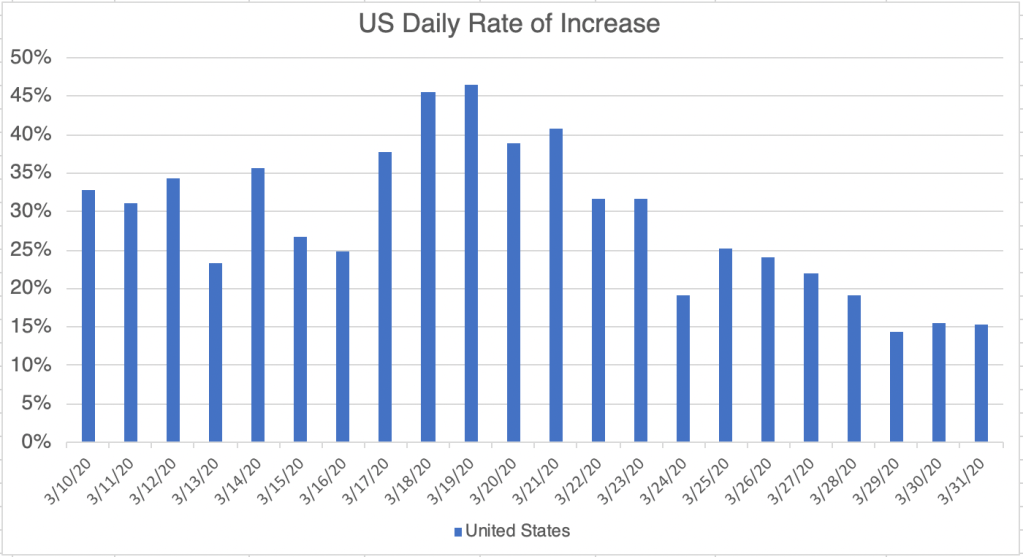
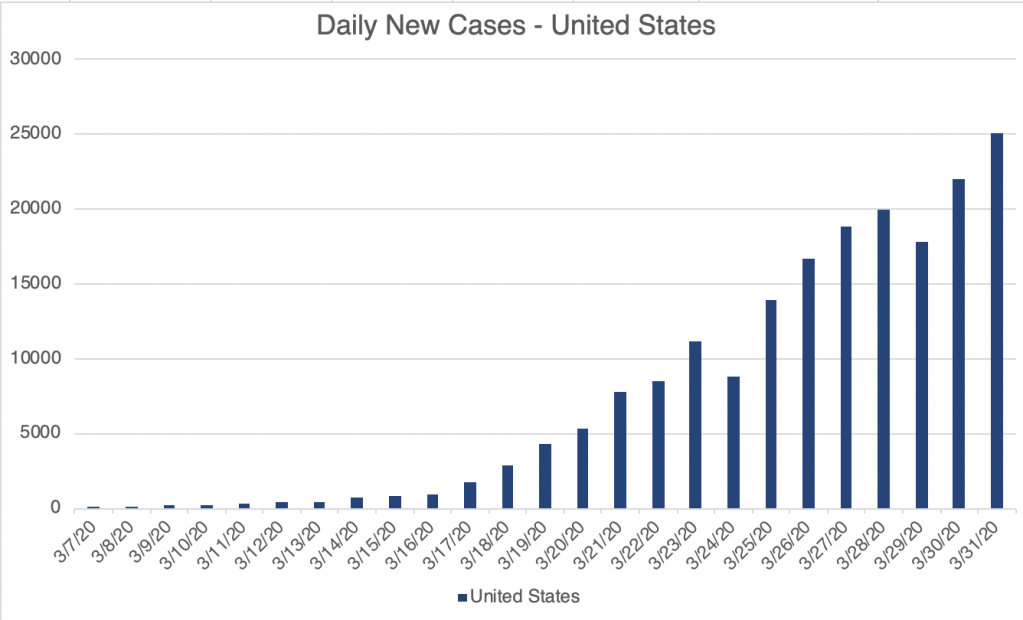
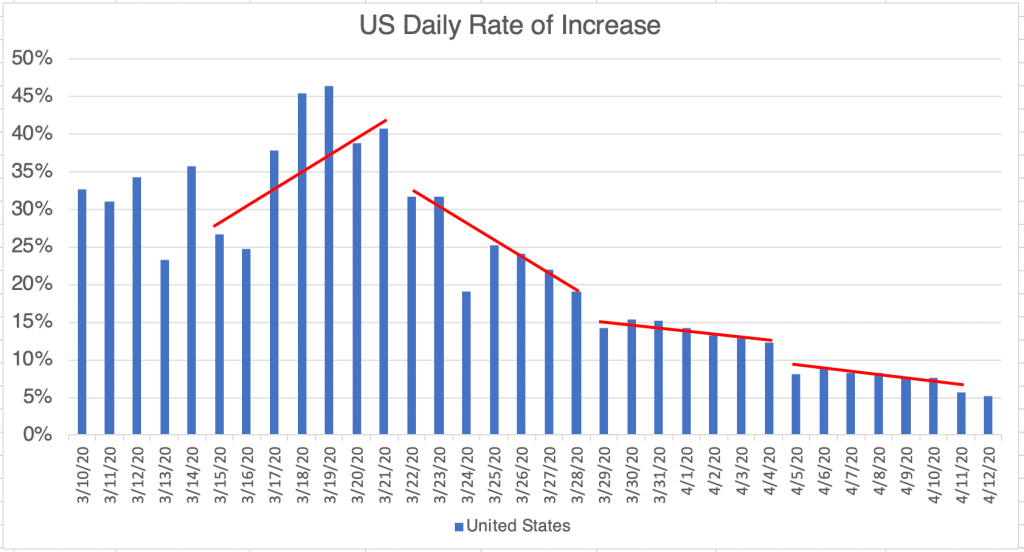
Is our isolation helping? In mid-March, the rate of increase of new confirmed cases was around 40%. Yesterday it was around 15%. I made this graph of what the case load in the U.S. MIGHT have been if we were not in our homes.
It may seem like you’re wasting your time, but you are helping! Many people AREN’T sick today because of our efforts. So keep it up!
Don’t fear, but be smart,
Erik
Thanks!
Originally posted April 3rd, 2020
Of course, the medical community deserves a lot of thanks for the long hours, and extra exposure during this time!
But I also want to thank grocery store workers, truck drivers, take out restaurant staff, and others who are keeping us fed and well during this time.
Thank you!
Erik
Case Update: April 1st
Originally posted April 1st, 2020
Friends,
I have to moderate my enthusiastic post from a few days ago some good news/bad news information. The good news is, for both the US and California, the rate of new cases is still trending down and is now below 20% for both regions. Unfortunately, even with the lower rate, the total number of new cases is still increasing after a short pause. It is definitely increasing at a slower rate, and that’s good, but increasing nonetheless.
Some have asked, how are these number affected by the new testing? It’s hard to say. The US is definitely doing more testing, and bringing more on line all the time, but our testing is still not adequate to capture all the information we need. There are still certainly a lot of cases we don’t know about, especially among asymptomatic and pre-symptomatic people. So even if you don’t have symptoms, it’s still important to keep your distance from others.
Others have asked about the new drug treatments that President has been enthusiastic about. Keep in mind that the medical field is highly regulated, and scientists and regulators are very slow to say a piece of equipment, test, or drug works until rigorous testing has been completed. So is the President right in saying these new drugs show promise, or is Dr. Fauci right in saying we don’t know yet. Well, they both are. The President is being hopeful, citing trials by physicians in other countries and in the US, and Dr. Fauci is expressing caution that the drugs have not been rigorously tested. Both things are true. The FDA recently approved the use of these drugs in trials here, and physicians in the US are always allowed by their credentials to use drugs off label. So testing is being done, and hopefully, we’ll have something that can be used widely soon.
Stay safe, my friends!
Erik