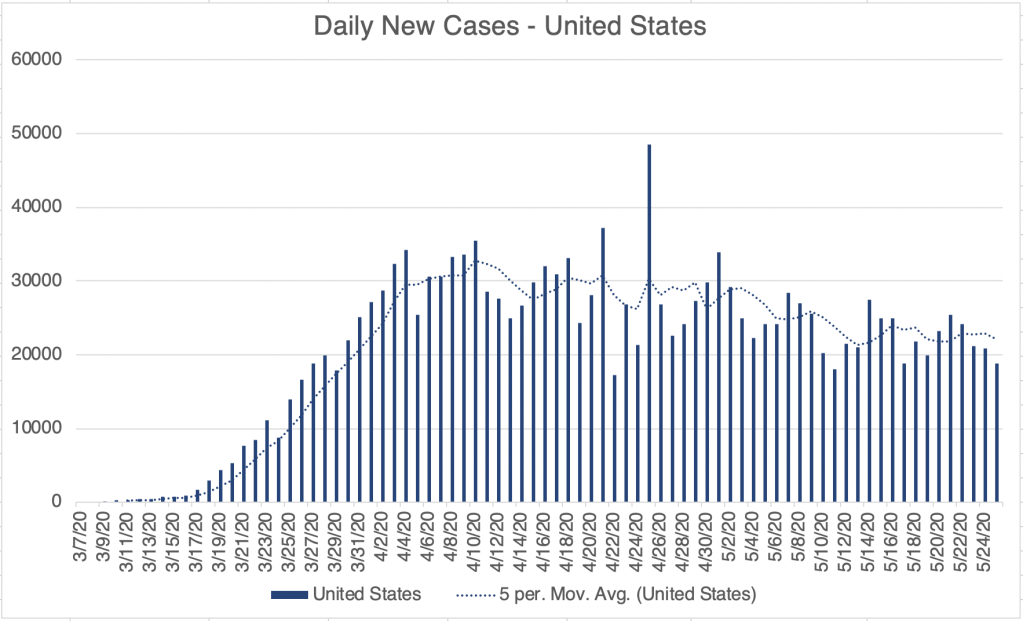
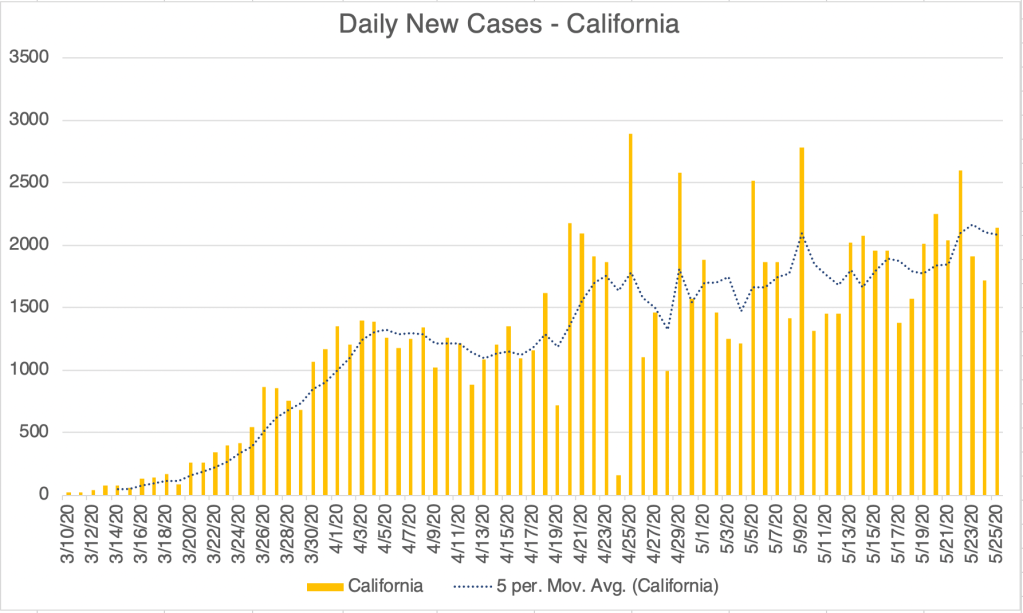
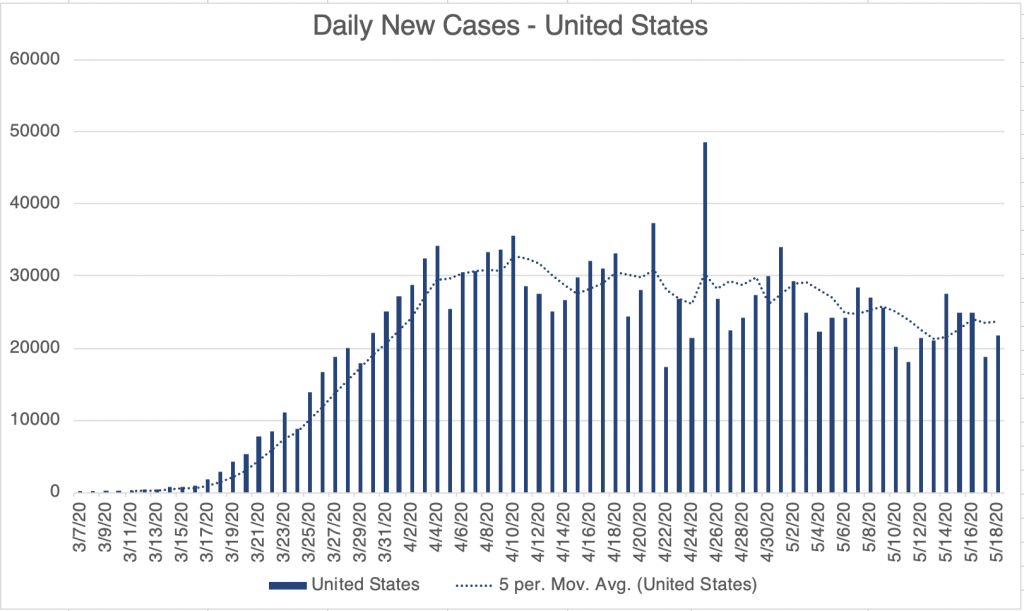
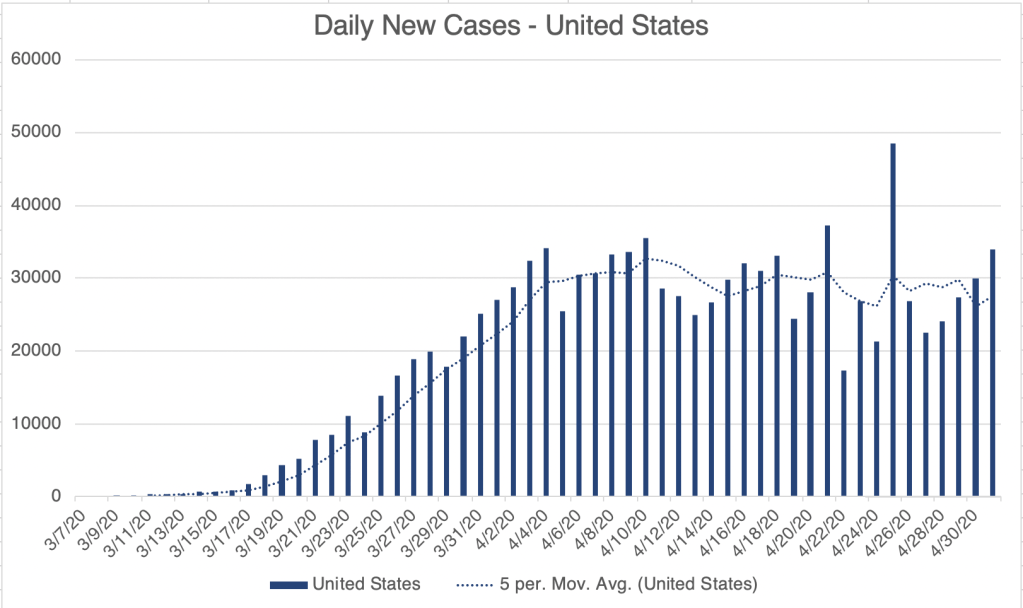
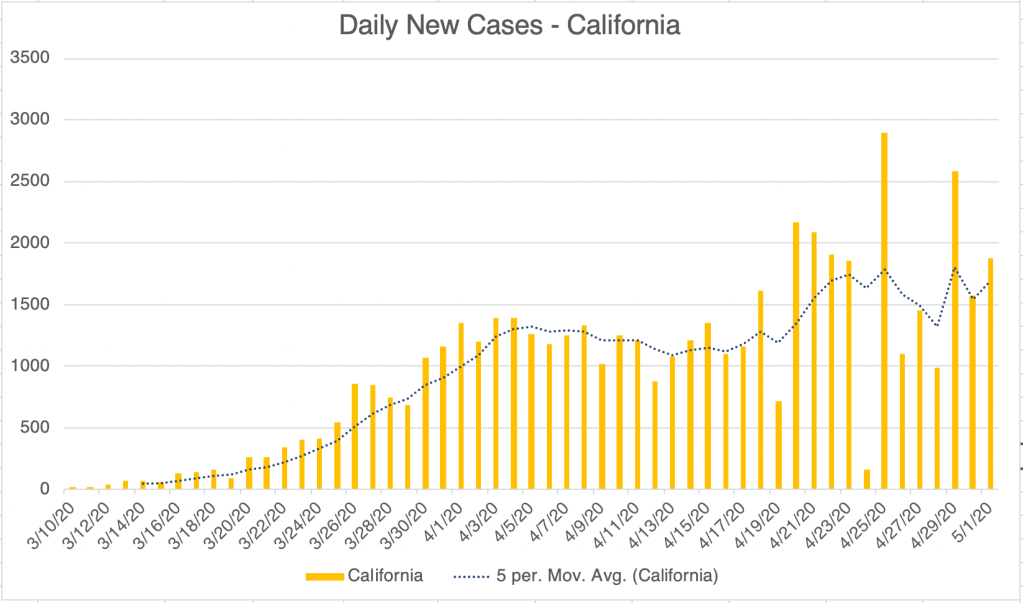
Today I have a weekly update on cases, followed by some speculation on what it means. As we’ve seen before, the United States has a slowly diminishing daily new case load for confirmed cases. Death rates for the US, perhaps a better measure than confirmed cases, are also slowly diminishing. Several sites seem to be accepting the data from Sutton et al (Universal Screening for SARS-CoV-2in Women Admitted for Delivery, NEJM, April 22, 2020) to estimate that actual cases is 8 times that of confirmed cases. California continues to have a slowly increasing caseload.
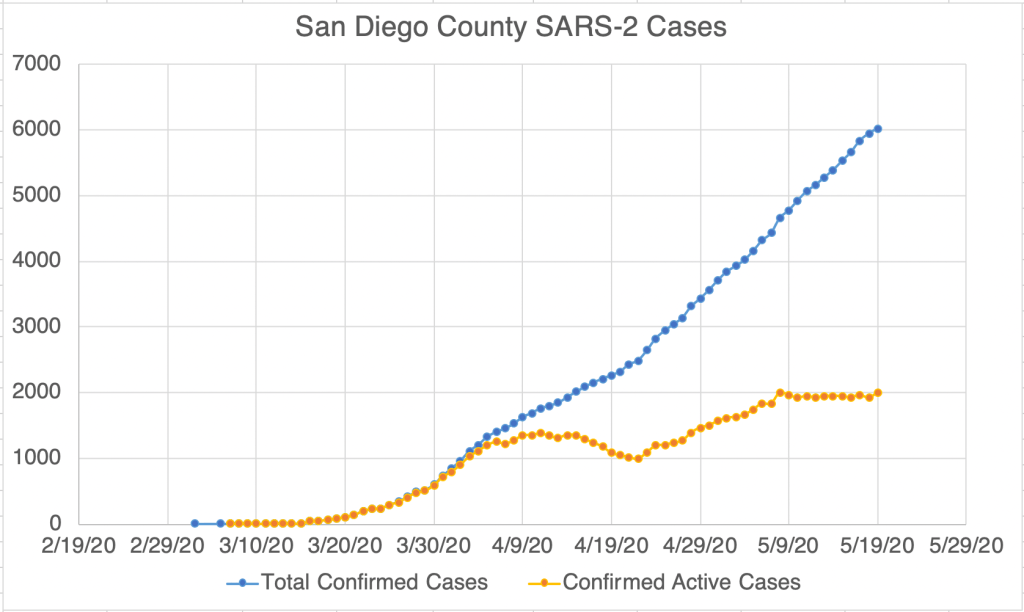
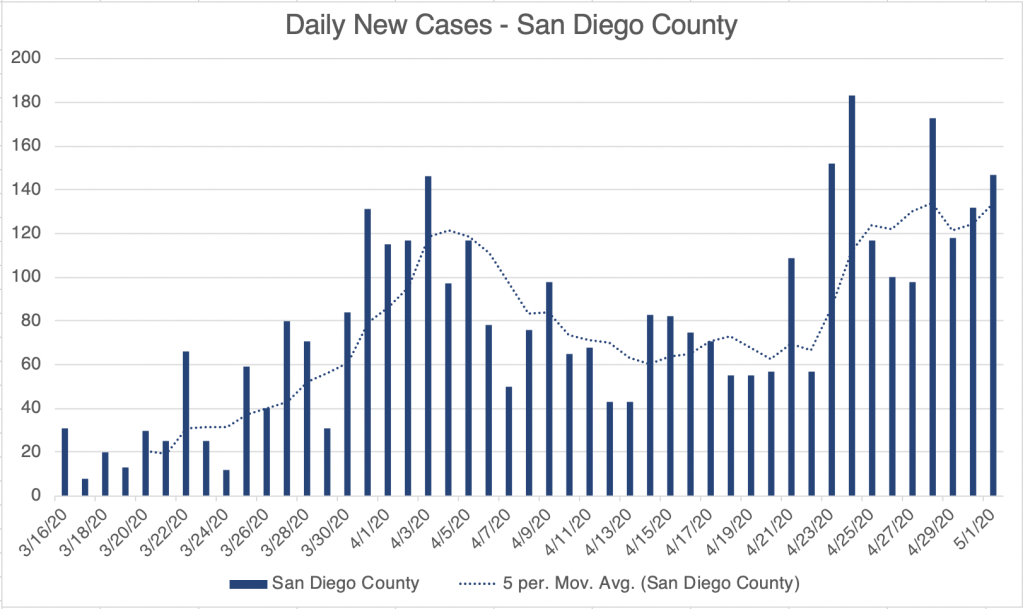
According to the John Hopkins University COVID site, LA County accounts for a full 48% of cases in California, with Sierra and Trinity Counties, in the East and North having just 1 case each. Cases are definitely centered in urban areas, mostly in Southern California. Daily death number in California appear to be perhaps flat. Interestingly, with all of these graphs, California daily deaths in particular, there is a clear weekend effect, with a weekly low in numbers on Sunday or Monday of each week. So when you look at the daily caseload for the US, with it’s jagged Sierra-like peaks, you’ll know it’s because health-care workers take the weekend off too, and reporting is being done during the week! San Diego’s numbers continue to be relatively flat.
Data is collected from San Diego County Public Health at approximately 9:30 pm nightly.
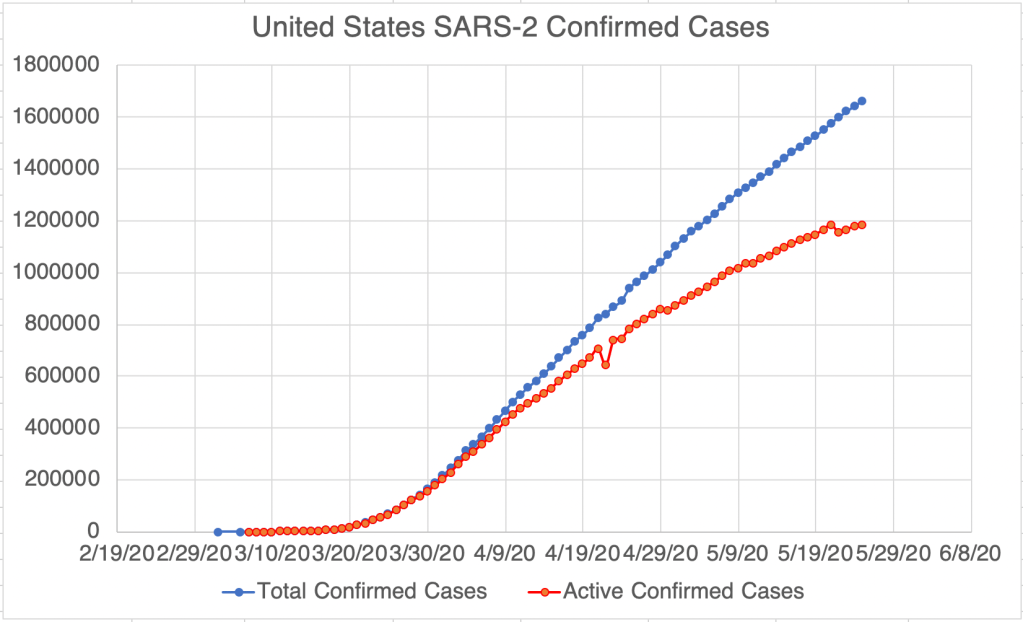
What we would like to see now is a lowering in the number of active cases. Unfortunately, this highlights a problem in all of this, how health departments define a “recovered” case. San Diego has just begun to report recovered cases. The reported numbers suggest that cases resolve in about 16 days after confirmation on average. For the US, reported recoveries suggest that patients recover in 50 days. California doesn’t report recoveries at all. Each entity defines a recovered case differently, so it will be difficult for us in the public to tell how many have recovered.
Data is collected from Johns Hopkins University at approximately 9:30 pm nightly. https://coronavirus.jhu.edu/map.html Reported recovered patients suggest recovery after 50 days after confirmation.Data is collected from San Diego Public Health at approximately 9:30 pm nightly. Active cases after 5/15 are based on data released by San Diego County. Points previous to 5/15 are calculated based on the assumption that recovery time after detection is 16 days. Reported recovered patients suggest recovery after 16 days after confirmation.
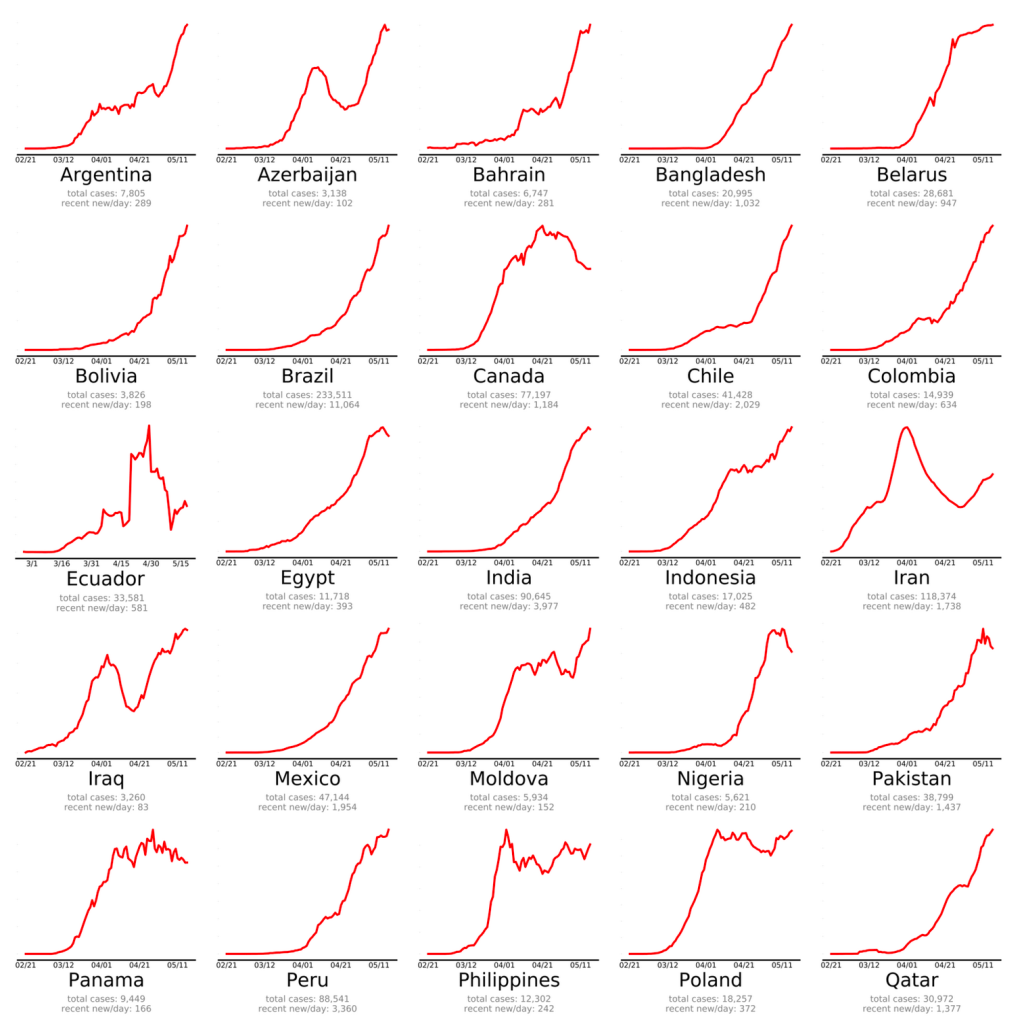
Reports from last week regarding the possible failure of lockdowns to bring numbers down are causing a lot of speculation on line as to the best way to improve. Many Western countries are struggling to reduce the number of new cases, and many countries are only now having their initial surge in cases (see my May 24th post).
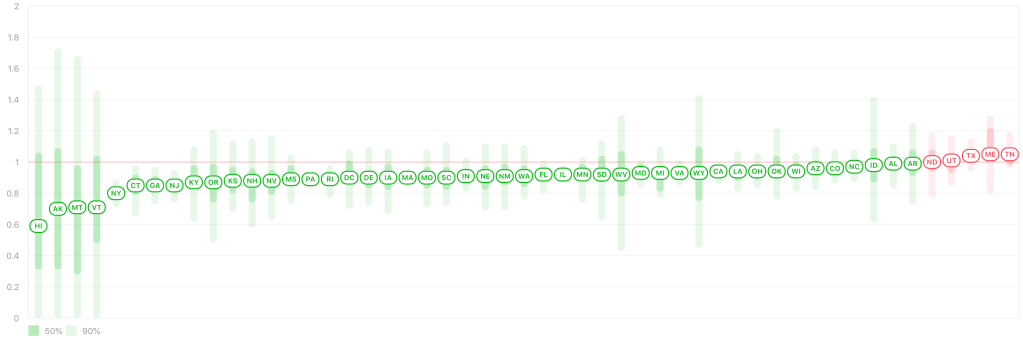
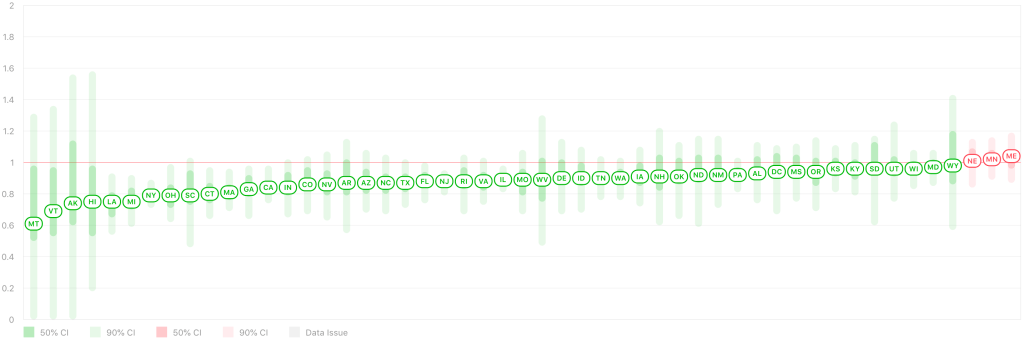
In the US, several states are creeping back toward an R0 of 1.0 after re-opening. We definitely want to stay below 1.0, as this indicates a slowly vanishing caseload. Texas was doing very well for a long time, but the R0 there is above 1.0 for the first time in quite a while. Cases are predominantly in urban areas, Houston, Dallas, and Austin.
A lot of studies are being done on the best approach. Japan is of particular interest because after an initial very small peak, they had a much larger peak starting in late March. They didn’t have the massive testing of So. Korea, nor did they have a strict lockdown. But they got things back under control quickly, and they have a very low daily caseload now, despite the VERY high population density of cities like Tokyo. So far, people are speculating that they are doing well because it’s culturally acceptable there to wear masks on a regular basis, and others are just calling it a mystery. I’m sure researchers will be taking a close look at Japan.
All the best to you and your family!
Don’t fear, but be smart,
Erik
Sutton et al (Universal Screening for SARS-CoV-2in Women Admitted for Delivery, NEJM, April 22, 2020):
Today I’m going to discuss the JP Morgan study on transmission (among other things), how the Moral Matrix effects how people see the fight against the virus, and the boom stage in many Southern Hemisphere countries.
JP Morgan has produced a study suggesting among other things that lockdowns are ineffective in fighting Coronavirus (see also a summary from Daily Mail). The reasoning for this is primarily that transmission is most common in households if a member becomes infected.
Frankly, when I think about anti-coronavirus efforts, I have tended to lump lockdowns and social distancing together, especially since many use these terms interchangeably. Notably, the study separates these 2 concepts and suggests that will social distancing (staying a distance away from people in public) may be valuable, lockdowns (staying in your home) is not.
You might say there have been 2 primary models for dealing with the pandemic in the last month after we’ve flattened the curve, but have not brought the numbers down, at least not in the US. I’ll call those models the Lockdown and the Re-opening models. Some want to continue the lockdowns to keep everyone safe from the virus, others want to re-open right away without restrictions. For several weeks, I have been gravitating toward a third Adaptive model. Of course, there can be many flavors of this model. Personally, I think masks, even bad ones, are far better than nothing, especially when worn by everyone, and can help us get back out of our houses and help us re-start the economy with reasonable safety. So I’m very open to the idea that the lockdowns have not been beneficial. Some of you will disagree.
The JP Morgan study is at odds with the endcoronavirus.org study, which recommends brief, very strict lockdowns. It could actually be that these 2 studies actually agree, depending on the time frame you’re talking about. I do think the lockdown was very helpful in the initial “boom” stage of the epidemic here in the US, but may have lost its usefulness later.
The Moral Matrix: ZDoggMD is a physician and medical YouTuber with a very silly screen name, but who posted VERY interesting video on how different people see the pandemic we are all facing. Using Jonathan Haidt’s work on the Moral Matrix, he talks about how different people’s moral framework shapes how we are viewing different efforts to address the issue. I was aware of Haidt’s work, but not had yet applied it to the pandemic in my mind. As someone who is sometimes exasperated with people who disagree with me (as they are with me I’m sure), this video is helping me remember to see their point of view. If you’re exasperated with your friends or family, I HIGHLY recommend you watch this video.
Upsurge in the Southern Hemisphere: Lastly, I just want to mention that many countries which have been relatively little effected until now, are now experiencing a big upsurge in cases. These countries include Russia, Brazil, and Mexico, and many are in the Southern Hemisphere, which is in the late Autumn months right now. Let’s hope they are able to get things under control quickly.
Don’t fear, but be smart!
Erik
PS. We went hiking in nearby Calaveras Park today for the first time in months, without our masks. There were a lot of people on the trail, and most were well behaved. When I can’t avoid someone on a narrow trail, I use an old SCUBA diving trick for ascending without getting the bends. Just close your mouth and blow slowly out of your nose as you pass someone. You’ll gently move any virus away from your nose! To maintain my friendliness, I greet people early, with plenty of time to start this little maneuver!
On Wednesday, San Diego County announced that the county will be moving further into California’s Step 2 re-opening plan. This means restaurants will be opening for modified seating with some other restrictions, and many more businesses will able to open as well. To sum, customers will still need to maintain 6 ft separation, and everyone will need to wears masks while shopping. Restaurant guests will need to wear masks while not at their table. Tables in restaurants will need to be moved so that seated customers are at least 6 ft apart. Tables that cannot be moved will need to have barriers between them. Restaurants can also expand outdoor seating!
I’m excited for this change, but it will be important for the public to follow these new guidelines. We want to keep making forward progress!
This is a case update for the previous week. As we’ve seen before, new cases in the US are slowly trending downward (currently around 21k confirmed cases per day), slowly trending upward in California (around 2k confirmed cases per day), and flat in San Diego County (around 125 confirmed cases per day). As we discussed from statistics last week (May 12th post), many of these are likely real cases, and not just because of additional testing.
Active cases after 5/15 are based on data released by San Diego County. Points previous to 5/15 are calculated based on the assumption that recovery time after detection is 16 days.
Rt Live reports that all but 2 states have an Rt value below 1.0, meaning that the virus is slowly disappearing in that state. You may notice if you look on that site, however, that several states, including California, still have slowly upward trending cases, even though they have an Rt value below 1.0. This appears to me to be a discrepancy. Possible explanations for this may be that the Rt Live’s algorithm is too generous and miscalculates Rt for some states, or that the Rt value needs to be much lower than 1 for a downward trend to be seen. We can certainly hope that we will see improvement in these states soon.
Some counties in California will be able to move further into Step 2 of re-opening (Step 2b?). Unfortunately for many of us, none of these counties are in Southern California!
My friend who works at San Diego County Public Health, Brit Colanter, has posted an update slide deck that the County has released, and will update regularly. The county is continuing to have more testing available to the public and is now releasing the number of recovered COVID patients. As of last night, total confirmed cases in SD is 5946, and current active cases is 1926. So more than half of our confirmed cases have recovered! That’s great news!
As we continue into recovery and more businesses open, please continue to wear masks in public, and continue to distance whenever possible! The CDC was slow to recommend masks, and it’s true that masks are not 100% effective, but if everyone is wearing masks that are 50% effective, this will go a long way toward minimizing transmission. See my May 5th post for more info and for mask designs! I’m a big fan of wearing masks in public, and it may be the key to opening more businesses.
The more we keep new cases low, the faster we can continue the re-opening process!
I have a variety of resources to share with you today.
Re-opening: First, after many states have started to re-open, Rt Live is showing that all but 3 states have an Rt value below 1. This means that for most states, each infected person is passing the virus to less than 1 other person, and the virus is slowly disappearing in that state. The states with an Rt above 1 are Minnesota, Maine, and Nebraska. After a poor initial response, I’m happy to say that New York State is doing very well now, and daily new cases are low in New York. In California, my home state, the number of new cases is flat, approximately 1700 cases per day since the middle of April.
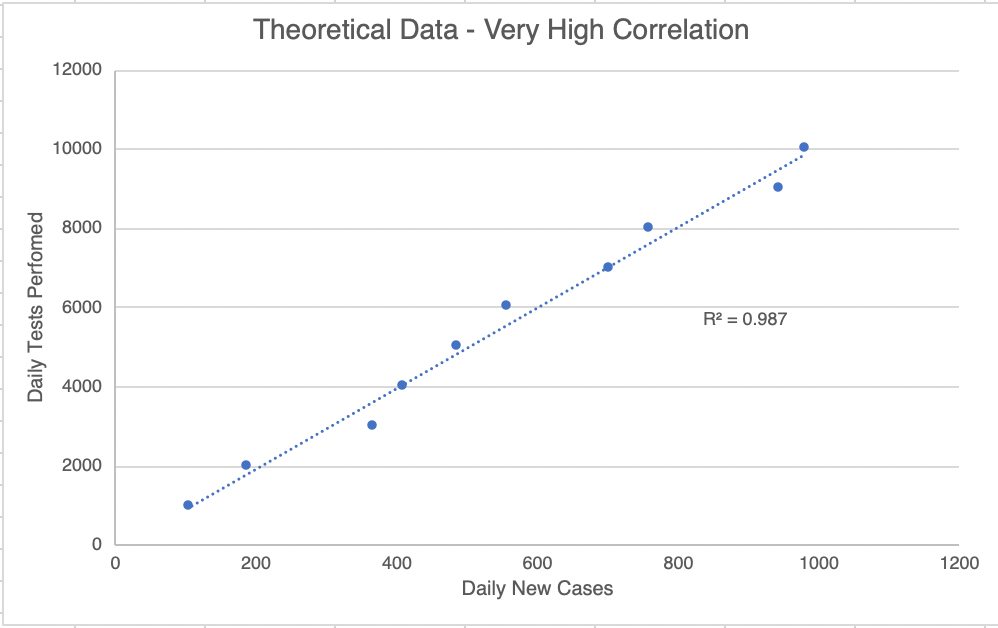
How many real new cases? This is going to be a little mathy! I told you I was going to start tracking the number of tests, and I have been doing that since April 27th. This will help us know how many of the new cases are just because of more testing, and how many are actual new cases. I’ve plotted the new cases against the new tests. For each day, a point comparing the new cases and new tests is shown. If new testing matters, then a day with a high number of tests will also have a high number of new cases. To find out if this pairing exists, we can do a statistical test called the R2 test (pronounced “R squared”, also called the correlation coefficient). This test creates a best fit line with the data and that creates an R2 value. This value is a measure of how well the 2 parameters (new tests and new cases) are correlated. I show a hypothetical graph in which the 2 sets of data are well correlated. A perfect correlation will have a score of 1.0, while a set of data with no correlation at all will get a score of 0.0. For scientists (at least the ones in diagnostics, like me) a correlation is considered “true” if the R2 value is above 0.95. You could also say that the correlation is 95% likely to be true.
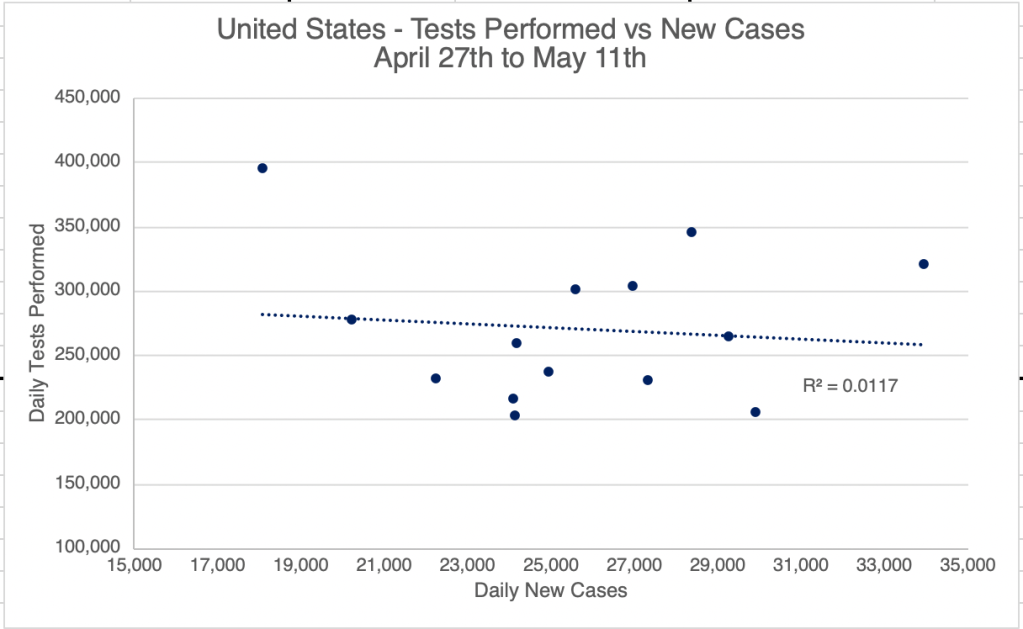
Now on to our data. I started plotting on April 27th. 5 days later, the graph for the United States got an R2 value of 0.6559. This suggests that new cases and new tests are 66% likely to be correlated for this time period. In real world terms, this probably means that some new cases are because of new testing, but some aren’t.
Interestingly, as of yesterday, a graph like this for the US gets an R2 value of just 0.0117. This is very low and suggests that there is now no correlation between new testing, and new cases. This means that new cases we see now are probably “real” new cases, and not just pre-existing ones that are just being found because of new testing. For California, the correlation between new cases and new testing was never very high. Right now, the R2 value is only 0.0039 for California, suggesting that most new cases discovered are “real” new cases. What this means going forward is that we probably have enough testing now to locate new cases. As we go forward, I expect we will start to see a steeper decline is new cases.
Good news! This good news comes with a warning, however! Those living in the West will easily understand a comparison to a brush fire. Right now, we are in the “containment” stage. We have the fire surrounded, and were at the beginning of the end, but if we walk away now, the fire will start to spread again. We need to stay on task and keep fighting the fire! I am all for re-opening, but we need to remain diligent. Wear a mask when you go out into public, and continue to keep your distance from others! If your workplace re-opens, you will probably want to wear a mask, wash your hands frequently, and sterilize your workspace often. I am probably going to start traveling for work again soon, and I’m very glad that everyone will be wearing a mask on the plane!
Endcorona.org compares responses: I discovered a new website the other day, endcorona.org, from the New England Complex Systems Institute. The group compares the responses and results from different countries. First, “green” countries responded very well, and were able to get the virus under control quickly. Aside from the good response, I also notice that most of these countries have relatively small populations. You may notice that China also appears on this list. Most experts agree that the data coming from China is not reliable, and they probably have many more cases than they are reporting. After intermediate cases in yellow are countries in red that need more action. This includes the US. If you’ve been reading my posts, you’ll recognize the “flat” curve of the US. Yes, we’ve flattened the curve, but we haven’t been able to knock down our case load yet. Other countries with similar flat curves include Canada, Finland, Indonesia, Panama, Poland, Sweden, and the UK. Other countries had low cases at first, but are now experiencing explosive growth in new cases, including Brazil, Mexico, and Russia.
After analyzing the responses of these countries, endcorona.org recommendations include the following, many of which you’ll recognize:
Lots of testing to identify new cases.
Isolating infected individuals, even from family members!
Strict lockdowns. The stricter the lockdown, the shorter it will be.
Travel restrictions, even within the same country.
Adequate health care capacity.
Safe practices for essential services.
Masks in public for everyone.
Viral spread: Erin Bromage, an Associate Professor of Biology at U Mass Dartmouth, has a very nice article on his blog describing how the virus spreads. It is well written for non-scientists and has lots of links to original research. The take home lesson is that the virus spreads particularly well in-doors. In addition, cough, sneezing, and to a lesser degree shouting, singing, and even talking are all risk factors in spreading virus.
Today I’m going to wade into the piranha filled waters of the vaccine discussion. I’m also going to talk about the issue of herd immunity, and my advice for re-opening. I’m not prepared for a discussion of the MRM vaccine that has been raging for the last several years, I’m going to discuss vaccines in general, and the hopes for a COVID vaccine in particular. I will say to start out, that I’m a big fan of vaccination in general, but each vaccine is different, and I may not be in favor of a particular vaccine.
Vaccines: I’m not an immunologist and I haven’t made vaccines myself, I’m just sharing with you what I’ve learned from an informed perspective over the last few months. When I first started sharing about COVID, I said something wrong, that it would take at least a few months to create a vaccine against COVID, which seemed like a long time to many. This was based on the time it takes to develop a flu vaccine every year. In the Spring and Summer, scientists find out that strains are likely to cause flu later that year, and they begin making a vaccine. This process takes several months. As it turns out, it’s only this fast for flu because there is a standard way to make a flu vaccine, they just need to know what strains will be likely to arise in the Winter. And sometimes they are wrong.
Unfortunately, however, there isn’t just one way to make a vaccine. There are many different ways, and it can be different for every virus or bacteria. So for every new infectious disease, a vaccine must be developed from scratch, testing all these different methods. The process can take from 2 to sometimes as long as 30 years! Some scientists have said that Dr. Fauci’s prediction of a vaccine by next Summer is actually very optimistic! In my informed, but not expert opinion, we should not count on a vaccine for this current COVID-19 crisis. However, the vaccine work being done will likely help with future outbreaks. At least part of Dr. Fauci’s optimism is that a lot of red tape is being cut to speed the process, and that’s good, but less development time will also mean more risk for the final product.
Herd immunity: I have heard many people promoting the idea that herd immunity will help us get out of the crisis. Even some governments have been promoting this idea. Herd immunity is a useful discussion for diseases for which there is a vaccine, but in my opinion, it is not something we should be striving for now with COVID. We shouldn’t put a bunch of people in danger to keep fewer different people out of danger. Herd immunity requires a lot of people to be immune, and that number is different for every virus. I’ve heard the numbers 50 – 70% for COVID thrown around. That’s a majority of the population! Why would we risk exposing the majority to the virus to save the minority? To be crass, it’s kind of like saying that once the pool is full of bodies, no one else will drown.
Reopening: More states continue to begin the reopening process. I actually strongly support this, as long as people continue to take care as they interact in public! Even California has entered Phase 1 (CA calls it Stage 2) today, Friday May 8. The stages CA will use, as well, as the announcement for the May 8th reopening were announced by Twitter by the Governor. Not my favorite method of making an official announcement, but there it is. Re-openings have a much higher chance of being successful if we continue to take care! Continue to wear masks in public, and continue to distance when appropriate (see my May 5th post). I’m hopeful that we can advance quickly through the stages if people continue to take precautions. Also, it will be important for us to continue to expand testing, and for businesses to take advantage of expanded testing by screening employees as appropriate. Some municipalities are starting to have drive through testing, including parts of San Diego (you must still have an appointment to be tested). Check with your health care provider or public health department to see if and how you can be tested. Keep watching how other states are doing! We can learn a lot by observing what methods are working, and what methods are not! I predict that outbreaks will occur in places that become relaxed too soon.
2nd Wave: Again, I’m not an epidemiologist, and the following is an informed guess, not an expert assessment. In my informed opinion, we will have second wave in the Fall or Winter, and history suggests it may be more severe than the first wave. But I’m still optimistic. Why? Because I think that with expanded testing, we will be able to test far more broadly this Fall than we could in March and April. This will help us identify and quarantine infected people rapidly, and will help us control the spread much better than in the first wave. For the 2nd wave to go well, we will need to stay diligent!
The messaging on masks has been very confusing. For several weeks, the CDC said the public doesn’t need masks, then finally, the surgeon general was demonstrating how to make a mask out of a T-shirt. I’m convinced that the CDC was so slow to recommend masks simply because they have been so hard to come by. But the delay in recommending masks has caused a lot of confusion.
______________________________________ Section added 2/22/21: Masks have produced a lot of controversy, but I am a big fan of mask wearing indoors. This does several things, it usually prevents infection if you’re wearing an N95 or KN95. However, studies suggest that even if you get infected, a masks will help you have a lower initial viral load on exposure, greatly reducing your symptoms! I personally always wear a mask indoors, and I rarely eat indoors right now.
Outdoors are a different story. Unless you are in a tightly clustered large group of people, you probably do not need to wear a mask outdoors! Some municipalities encourage or require mask wearing outside, but this is usually unnecessary. I am not saying you should ignore local requirements! I’m just saying that when you are going for a walk, a hike or a bike ride, a mask is not necessary. _______________________________________
First, let’s talk about the words you’re hearing now!
Cloth Face Covering: A “cloth face covering” (I’ll say CFC for short here) is not technically a mask as the CDC defines it, and is not considering Personal Protective Equipment (PPE) from a medical perspective. This a t-shirt, bandana, buff, or anything else that can be used to cover your nose and mouth. The virus can still get both into your nose or mouth, or leave your body through these coverings, but it’s much better than nothing. A lot of people who are trying to be responsible, but can’t find a mask to buy, are using these coverings. If you hear someone saying they don’t work, they mean that they aren’t completely effective, but they are much better than nothing! Even if you sneeze, a face covering will capture larger droplets, slow the velocity of the sneeze, and help protect those around you. If all you have is a CFC, you should still wear it when you go out!
According to Fischer et al, gator style masks may be even worse than wearing nothing at all, since they may break up droplets into a smaller size that stays in the atmosphere longer! So avoid a neck-gator style mask!
A surgical style face mask.
Face mask: A “face mask” is a filtering mask that covers the nose and mouth, but does not seal around the nose and mouth. This includes the blue surgical mask that you see a lot of today. These masks are designed to prevent material from medical worker’s face and nose from getting to a patient during a procedure, while still allowing somewhat normal breathing. They filter incoming air to some degree, but there are large gaps at the sides of the mask, so there are not very effective at preventing infection by SARS-2. Coughing, sneezing and singing will still expel air from the sides while wearing these masks! They aren’t completely effective, but they are certainly better than nothing, and will prevent transmission through simple talking. If you have one, please wear it!
UPDATE: Now that KN95 masks and some N95s are available (see below), I can no longer recommend wearing these masks.
Respirator: These masks seal against the sides of the face cover at least the nose and mouth. They are designed to filter the air and prevent particles from entering the nose and mouth. N95s prevent 95% of viruses from getting through and are the preferred mask for medical workers in most situations right now. Unfortunately, they have been in very short supply since the beginning of the pandemic, so the public is being asked not to purchase these for now. Doctors tells me that N95s are not adequate protection while performing certain procedures on COVID patients! One told me a story about 14 medical workers being infected by a single patient during a procedure! This work requires a Powered Air-Purifying Respirator (PAPR). These masks cover the entire face and also blow air into the mask, pushing virus out.
An N95 with a valve.
If you have an N95 with a valve in the front, these masks will still vent air when you cough or sneeze, so be aware that it will not protect others from virus coming from you! N95s with no valve are the best choice for protecting both you and those around you. Again, hold off on purchasing these until there are in greater abundance.
An N95 with no valve.
I see a lot of very nice looking fitted masks with a little round filter in the front. These filter out large particles like dust or large droplets, but not necessarily small virus particles. While much better than nothing, these are not necessarily N95 masks! Read the product information carefully when buying these masks.
KN95 Masks: A new style of mask is being sold in the US now, labeled KN95. These masks are made in China and designed to filter out 95% of viral particles, like N95s. However, they are certified by a Chinese agency, and not by the FDA or CDC. They have been allowed to be sold in the US on an emergency basis. Users say they fit more loosely than N95 masks.
KN95 mask.
There are lots of studies showing the effectiveness of these masks, and unfortunately I don’t have one ultimate study to share with you. Suay, a clothing company in LA, did a study suggesting that normal blue shop towels (like Tool Box Shop Towels or Zep Industrial Towels) do a much better job at filtering than cotton, and are a cheap and available alternative to an N95 when sewn into a mask. My sister-in-law Penny is part of a team that makes masks for the local hospitals in Bozeman. These are homemade masks with a pocket for a HEPA filter. She’s sending me some, and I’m going to add a Shop Towel to mine! Both designs are posted below.
Here’s a few tips for wearing your mask:
Your CFC or mask must cover your mouth and nose. Leaving your nose hanging out, or simply wearing it as a chin mask is not adequate!
When adjusting your mask assume both your hands and the mask are contaminated. Wash your hands before AND after adjusting.
30 min of UV light effectively kills SARS-2 virus. In the bright sunlight, it may only take a few minutes. I sterilize my mask by leaving it in the sun for a half hour after a shopping trip. If you have a cloth face covering or mask, machine washing is a better choice.
In addition to preventing infection, masks appear to reduce the viral load in newly infected patients, leading to less severe symptoms! So even if you get infected while wearing a mask, your symptoms are likely to be less severe!
As we think about re-opening the economy, face coverings, even the bandana type, will really help keep new infections low. So wear a mask when you go out in public! Any improvements will hasten the day when businesses can re-open. I am awaiting data to see what the infection rate is at businesses in which employees wear masks. Hopefully, this data will come out soon.
Cochrane Report on the Effectiveness of Masks: Jefferson et al released a meta-study through Cochrane Reviews on the effectiveness of medical masks (surgical masks) and medical respirators (N95) in public settings. A meta-study is a study in which the authors gather information from published articles and try to draw conclusions from a large body of data. They do not gather a new set of data.
The Jefferson et al study reviewed 78 different studies, including data from pre-COVID flu outbreaks. Their conclusions are sobering. First, the authors suggest that there is virtually no benefit to wearing a medical surgical mask over not wearing a mask in most settings. If you’ve been reading my blog for long, you will know that this conclusion does not surprise me. Blue surgical masks have large gaps in the sides and do not filter air leaving the mouth and nose. They were designed to prevent droplets from a medical worker from contacting a patient, not to prevent transmission of aerosol based agents. This is a problem, since most mask wearing people in public during the pandemic were wearing surgical masks. These people thought they were protected from aerosols, but they were not.
The study also concludes, however, that N95 masks didn’t perform much better. In fact, for lab tested COVID, the difference was statistically insignificant, meaning that the difference between wearing N95s or surgical masks was so small, it could not be proven to be a real difference statistically.
I have to point out that the Jefferson meta-study points out that many of the studies they reviewed had various failings that may have made them unreliable. Much of the data was collected through self-reporting of participants, which is a source of inaccuracy, and participants were often non-random, making application to the general population difficult. So some of the conclusions may have suffered from these kinds of errors.
As you know, I’ve been a proponent of wearing N95, KN95, or KF94 masks when indoors during the pandemic. Unfortunately, N95s are tight and intolerable for most people for long periods, so most people didn’t want to wear them at all. Those that did were not careful to make sure the mask fits properly, making the mask ineffective. This is part of the reason I wore a KF94 (Korean) during the later stages of the pandemic when I had choices.
So have I been wrong this whole time? Well, yes and no. I wore a KN95 in all kinds of environments while traveling during the pandemic. When I finally got COVID in January of 2021, I was not wearing my mask, working in a “gray area” environment with people that I later found out had COVID. I was technically indoors, but the room had a lot of ventilation, so I thought I would be OK. Obviously, I was incorrect. All this to say, I think my KN95 was effective for much of the pandemic. On the other hand, I am a scientist in the infectious disease field, and have had a lot of experience wearing and fitting these masks to myself, so I am not a typical user. It may certainly be that my experience does not translate to non-scientists.
If you still have not had COVID and are not high risk, I might say that the current version has an extremely low fatality rate, and it may now be worth the risk to say good-bye to the mask. I know the large majority of you have done this already.
If you are at high risk, I still think an N95, KN95, or KF94 can be effective for you. In order for it to be effective, however, you need to make sure it is properly fitted, making sure you don’t have gaps between your nose and cheek. The mask should filter the air coming into your nose and mouth.
Since I had COVID last January, I no longer wear a KN94, and enjoy eating indoors in restaurants again. I’ve basically been back to normal for a long time.
Dr. Visay Prasad has an excellent video describing some of the details of the meta-study. He is an epidemiologist from UCSF. ____________________________________
The number of news cases has been erratic in the last week, but at least in the US, it continues to trend downward. I’ve started collecting the number of new cases in the US and California, and while I’m not sure how to integrate that data into my Excel spreadsheet yet, I can tell you that more tests definitely mean more new confirmed cases. So some of the erratic graphs were seen are definitely because of more testing. In the long run, I expect to see new cases come down drastically as we continue to increase testing.
Rt.live is showing that 45 of 50 states have an Rt value below 1 yesterday. This is great news, as it shows that in most states, the virus is slowly disappearing. I’m watching with great interest to see how the states that have started re-opening do. Keep up the great work! We are having an impact!
Also included is a very interesting video I ran across, Simulating an Epidemic, showing a non-scientific computer model of possible epidemic outcomes given different approaches. Keep in mind, this model is NOT attempting to show what will happen in the COVID epidemic, just some theoretical things that might happen given different approaches. He does NOT attempt to prove that any of these things are what’s happening.
The most interesting parts for me were when he compared 2 methods that have been used in different places. At 6:00 minutes, he talks about the Detect and Isolate method, which I favor. This is were you find an infected person and quickly quarantine them until they have recovered. He argues that this is the most effective method in an epidemic like the current one. We haven’t been able to do this, really, because of our lack of testing in the beginning. My fervent hope is that if we get a second wave in the Fall or Winter, we will be ready for this approach.
At 16:50, he talks about a method that I think we are kind of using, the shelter in place, but with trips to central locations. He says that without other measures, these locations become a source of new infections. This is probably not happening as badly in real life because so many are wearing masks to the store!
Friends, For those of you living in San Diego County, there is a lot of news on the evolving situation in San Diego and California.
First, San Diego County reports that the county has met 4 of the 5 criteria for entering Phase 1 of re-opening. We have had down-trending new symptoms and cases for the last 14 days. However, to meet the last criterion, the County needs to have more testing, PPE, and hospital capacity available in the county. Let’s hope this happens soon!
Also, after a brief beach opening for walking, swimming, and surfing, Gavin Newsome has closed all beaches and state parks effective today, May 1st.
Brit Colanter just shared some info from San Diego County Public Health. San Diego will be scaling up contact tracing soon! This is the practice of informing those who have been in contact with sick individuals. This technique has been very helpful in some of the more successful countries, So. Korea, Taiwan, and others. It will help us get back to normal more quickly!