“Omicron” may sound like a killer robot, but it turns out, it’s OUR killer robot!
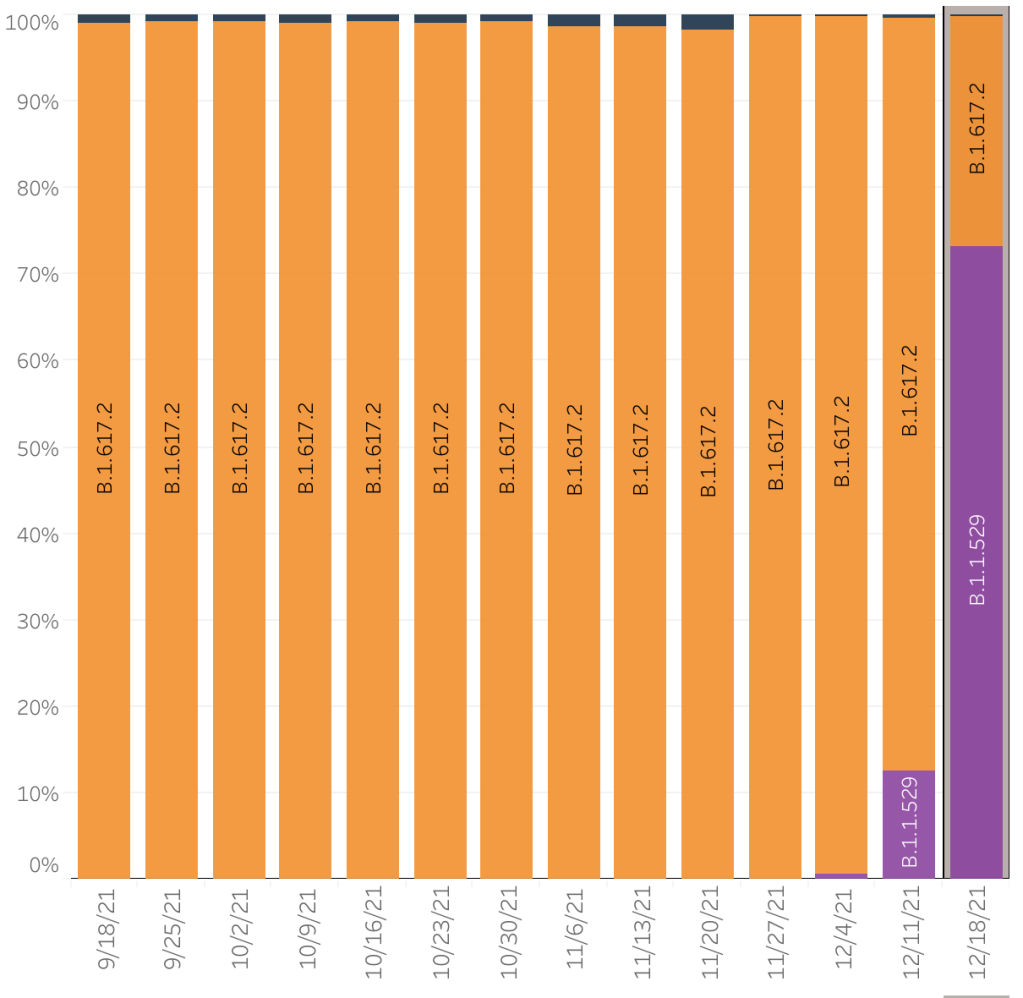
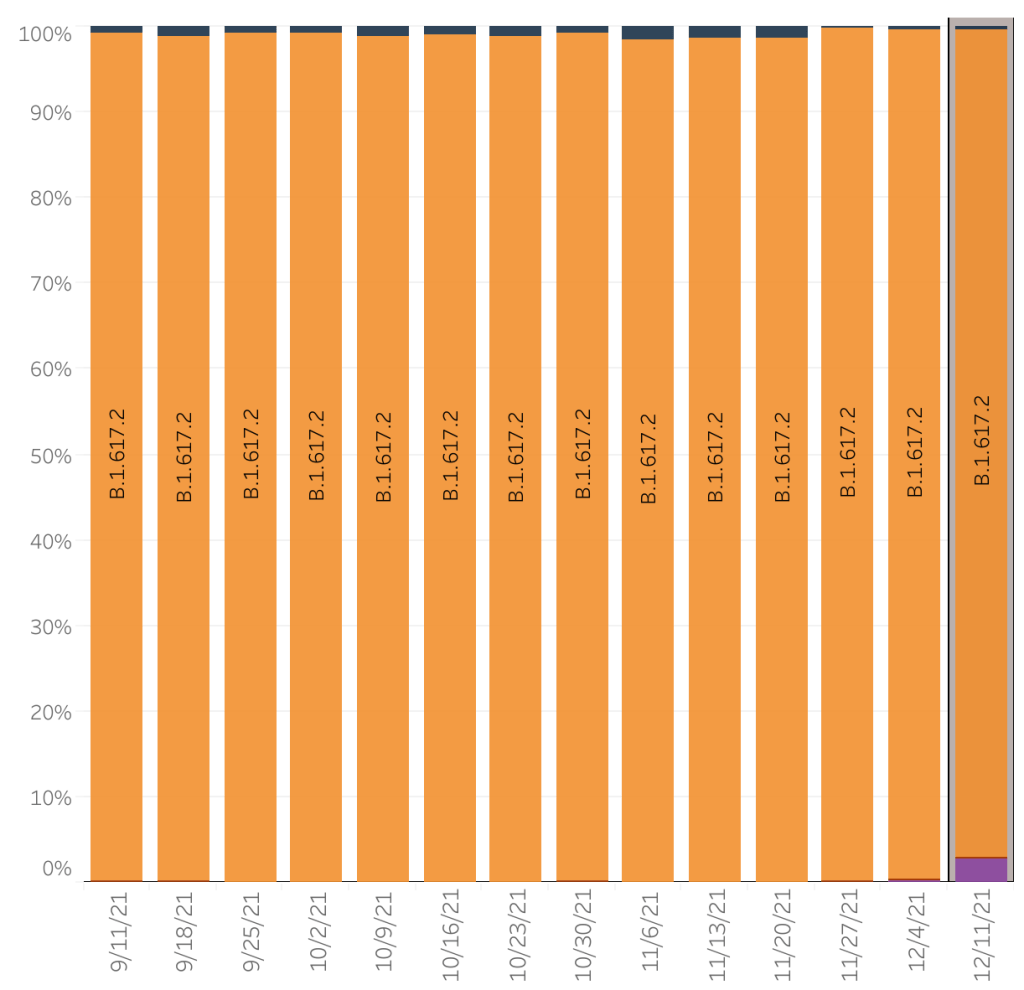
You’ll have to forgive my imprecise language this evening, but we have some potentially VERY good news, and I’m a little giddy. Last week I reported that 3% of the COVID cases in the US were because of the super infectious but mild disease causing Omicron variant. On Monday afternoon, the CDC updated their numbers from last week stating that 12% of the COVID was from Omicron. Today, they are reporting that for this week ending Sunday, a full 73% percent of COVID cases were from the Omicron variant! With only a doubling of cases in the last few days, that means at least 50% of Delta variant cases have been displaced by Omicron cases. This means that Omicron is displacing Delta. At the current rate of expansion, by Christmas, at least 95% of COVID in the US will be from Omicron, and nearly 100% by New Years! If we can keep Delta suppressed for at least 2 weeks, it will be eradicated from the US. This is so great!
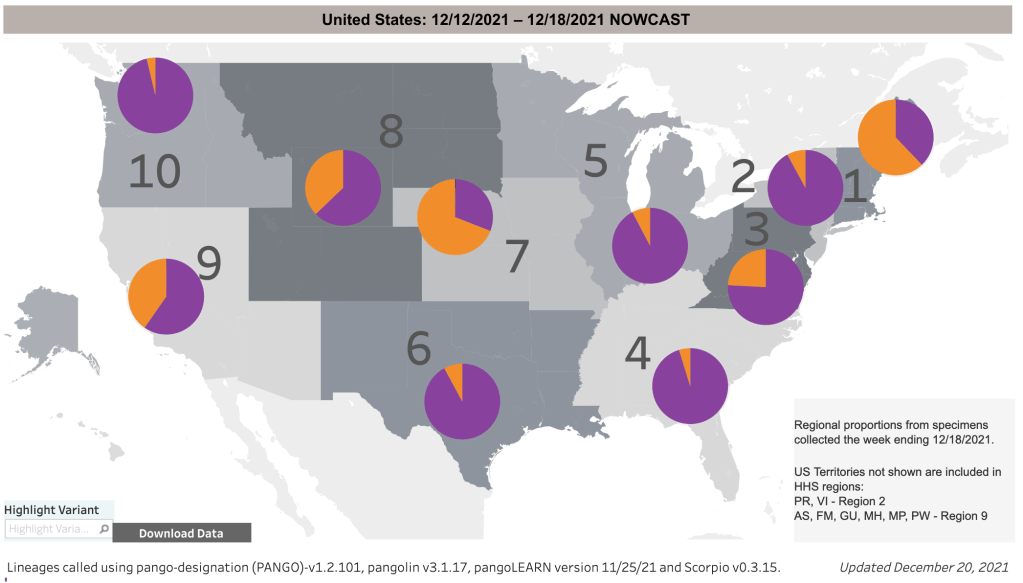
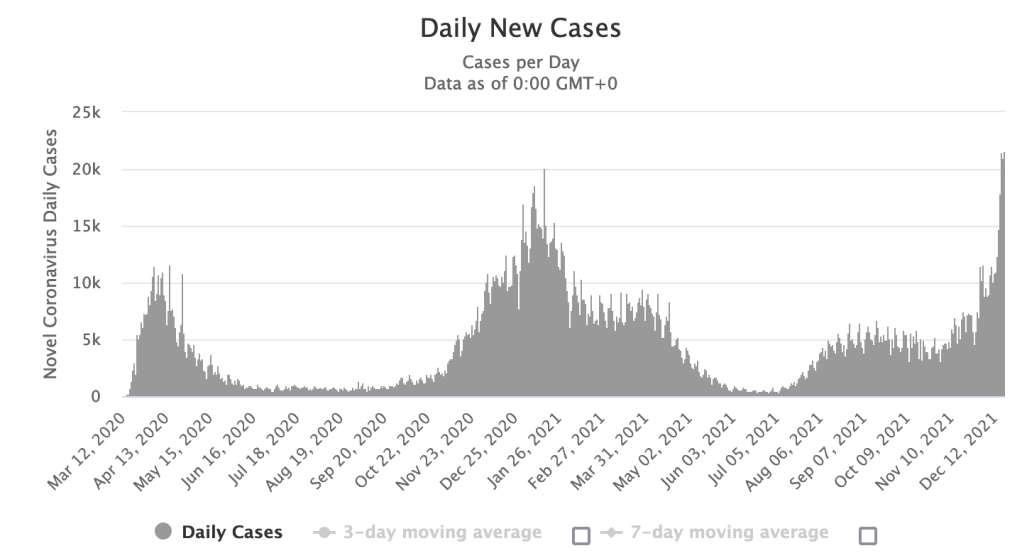
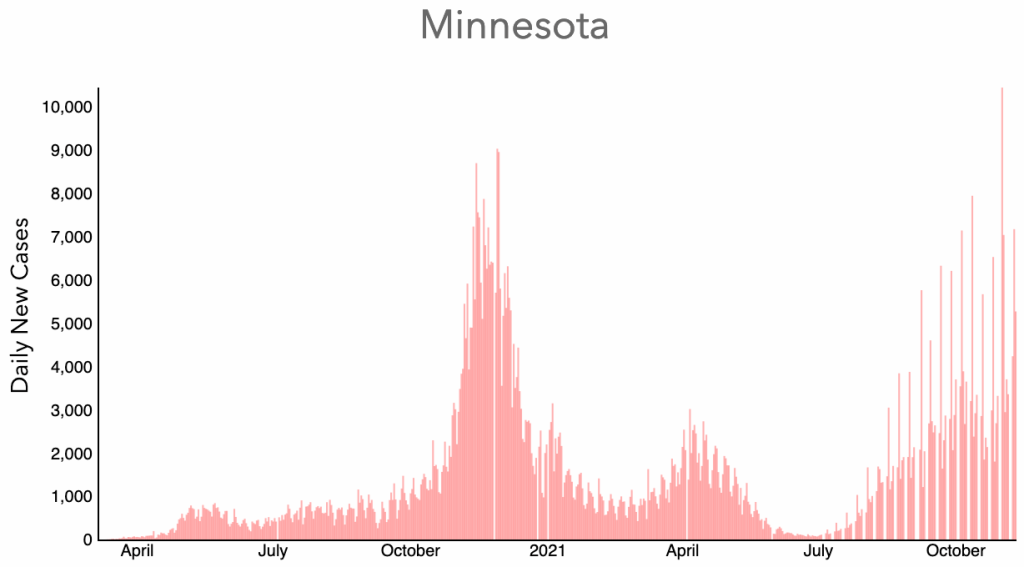
From the CDC page on Variant Proportions. Currently, 73% of COVID cases are from Omicron.From the CDC page on Variant Proportions. Currently, 60% of COVID cases in the Southwest are from Omicron.Daily new cases in New York State. Note the doubling of cases in the few days. But 90% of these cases are from Omicron, so Delta cases are roughly 25% of what they were a week ago, having been displaced by Omicron.
I have often been overly optimistic, but literally, if things go they way they’re going now, the Pandemic could virtually be over by New Years!
You know that cop at the beginning of all those movies who is about to retire and then gets killed in the first 10 minutes? Don’t be that guy. We’re almost out of the woods. Don’t go crazy and get COVID now. Keep it together for another few weeks, for crying out loud.
After I’ve settled down a but, I’ll be adding more information, links to my blog post, and a more sober assessment on this topic tomorrow, so check again then. For now, crack open a Diet Coke, in the seclusion of your own home or sensible outdoor gathering and celebrate!
This is case update. I’ll also give an Omicron update, and discuss the criteria that must be met if Omicron is to be a blessing rather than put us back to square one.
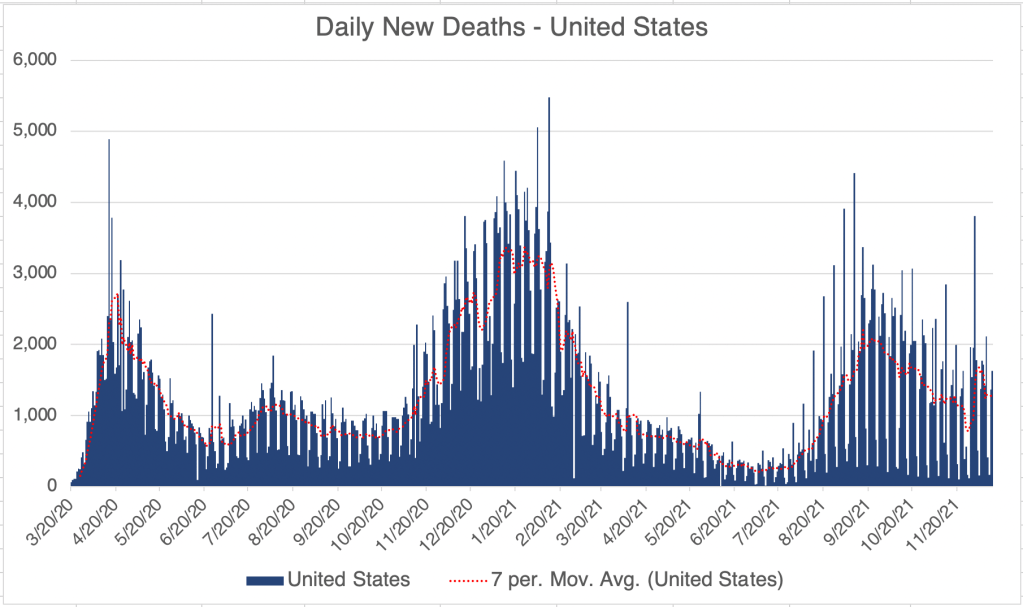
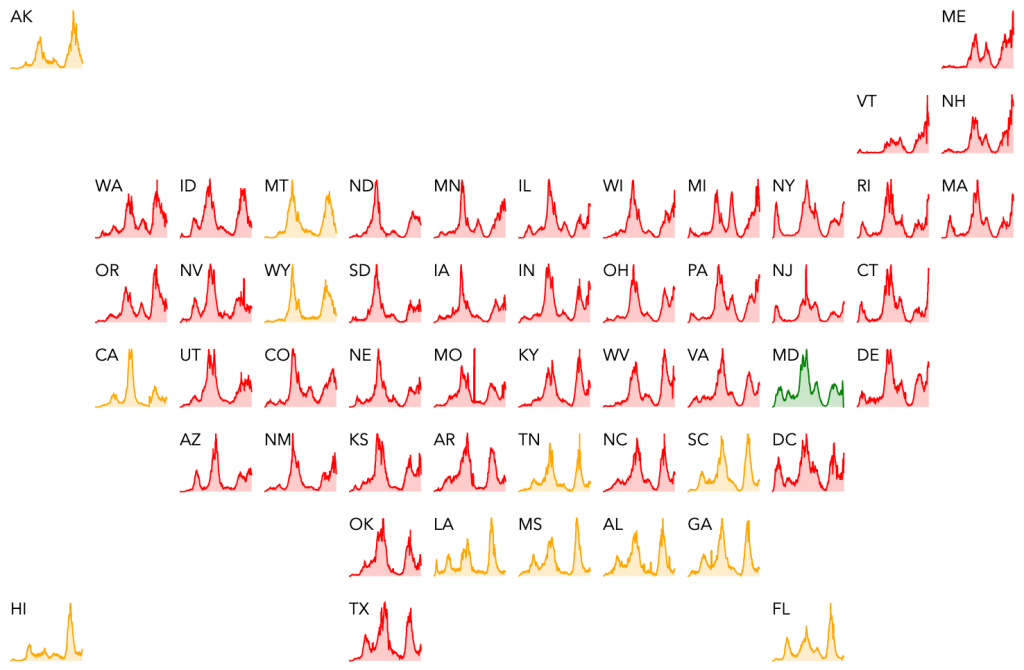
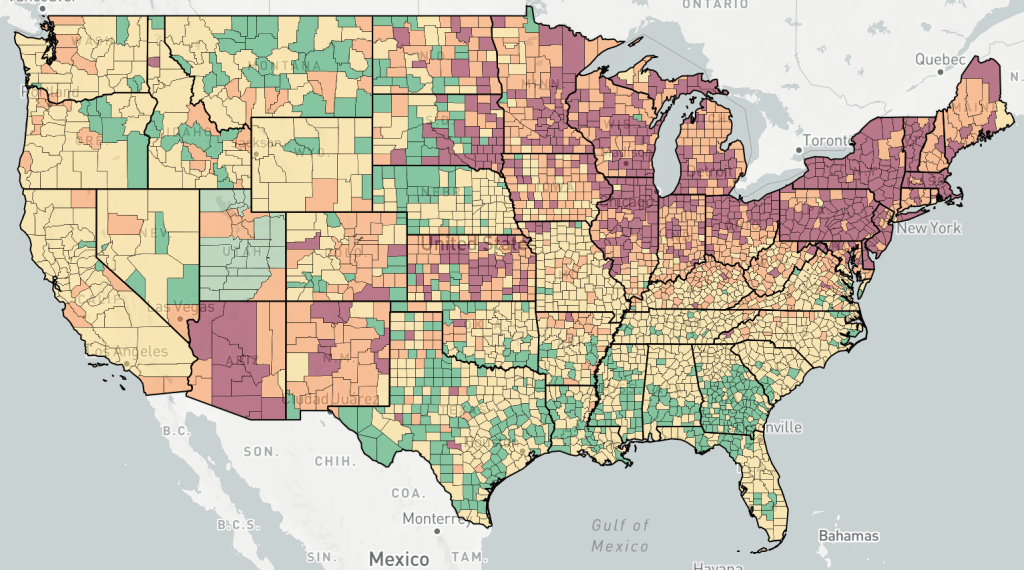
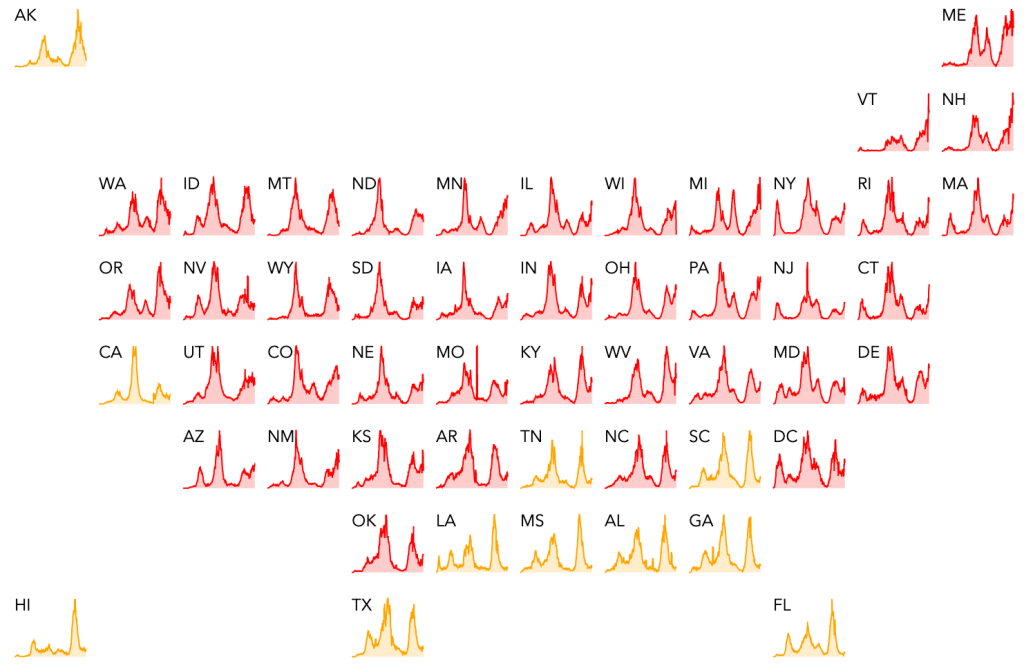
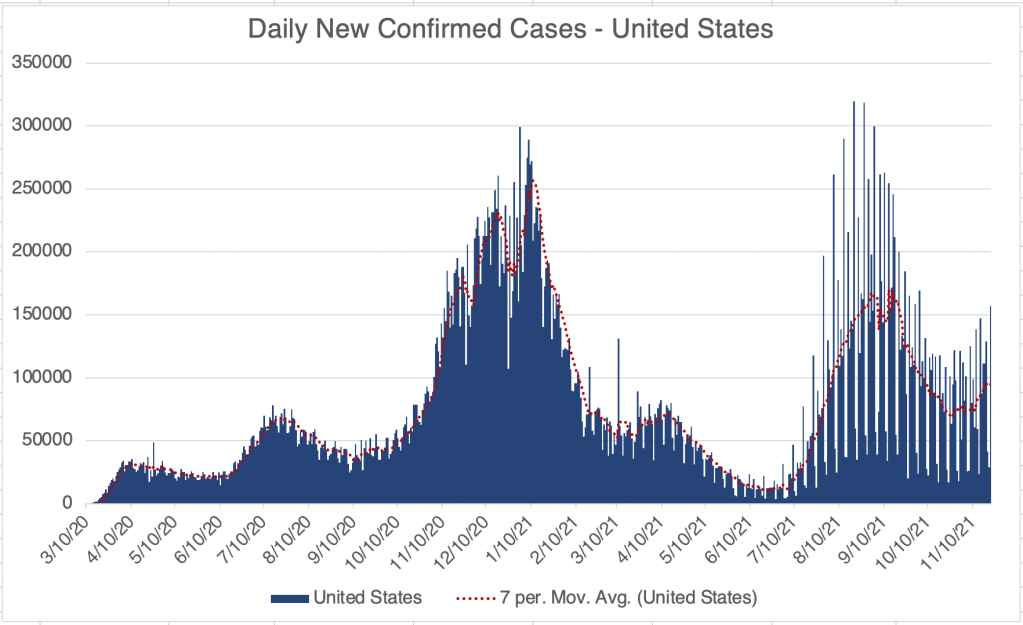
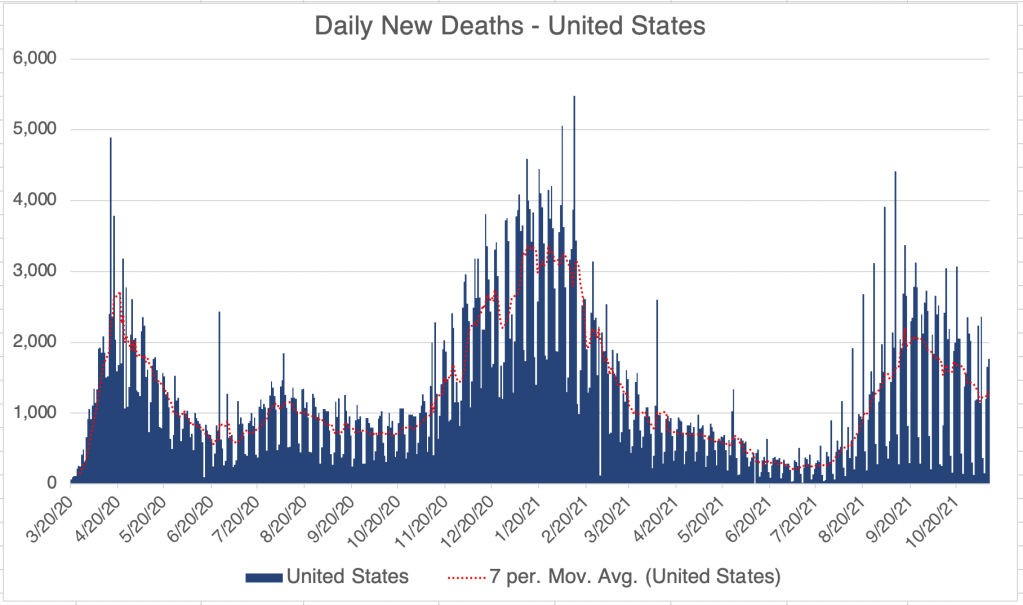
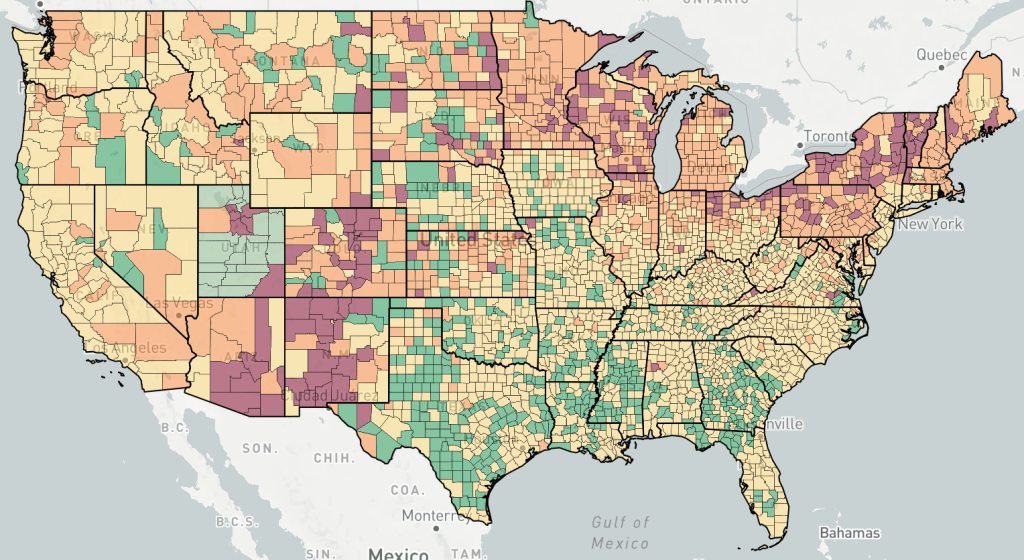
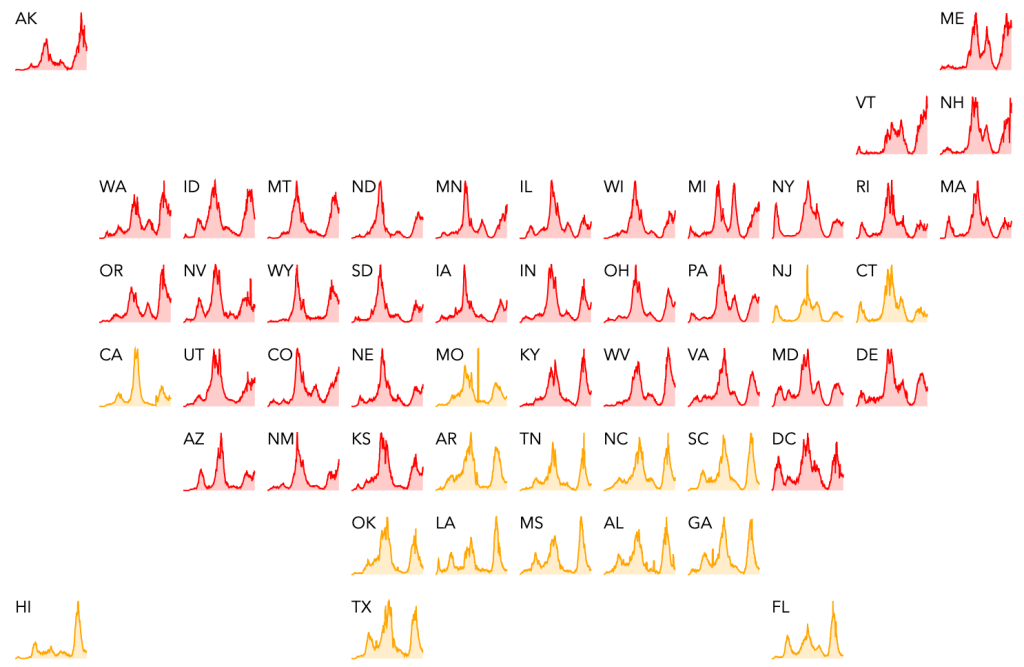
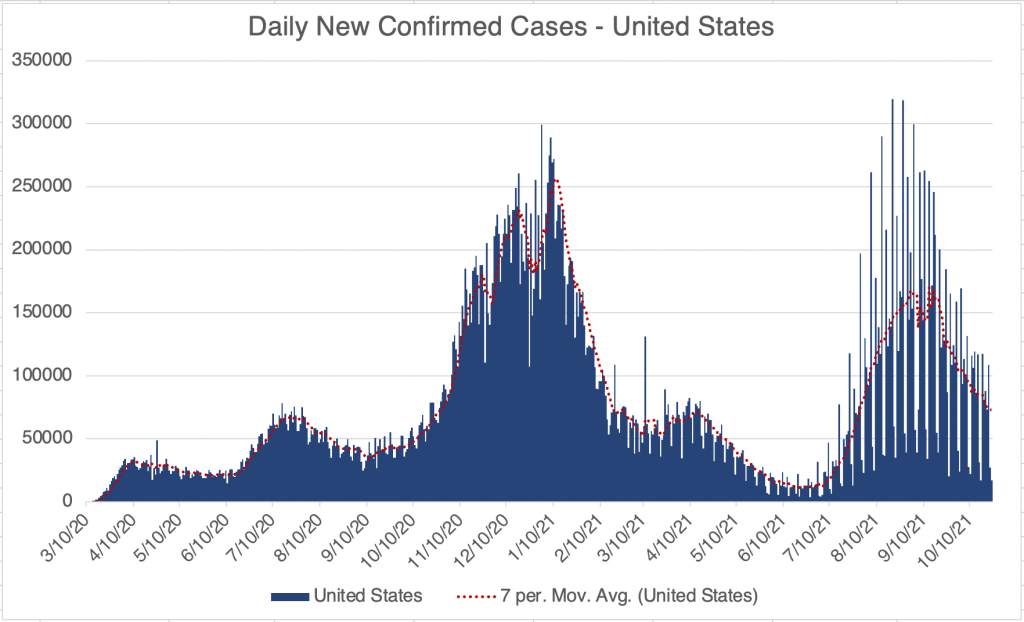
For the US, the Northeastern states are continuing to see increased cases in states like New York, Michigan, Pennsylvania, Ohio, and Illinois. This is at least partially because of colder temperatures leading to more people being indoors. Last year, the Winter wave spread from Northern states like Wisconsin, Michigan, and Minnesota. Just like last Winter, Cook County, the home of Chicago, has the most active cases in the US right now.
Omicron update: Information on Omicron infection continues to come in from South Africa, and now from the UK and Denmark. In South Africa, most new cases are now from Omicron, but fatalities are only 4% of what they were during the Delta wave there. In the UK, it is estimated that fully 50% of new cases are from Omicron. At this point, there are 1 million new Omicron cases every day. Omicron is proving to be explosively infectious. John Campbell says the US is about 3 weeks behind the UK, and we’ll see 1 million new cases of Omicron per day by the first week of January.
Surveillance is very good in Denmark, and a lot of isolated strains are being sequenced. It appears in Danish data that previous vaccination or infection status has almost no bearing on whether someone is infected by Omicron, so we can’t expect vaccines to prevent infection. However, it does appear that previous infection or vaccination reduces the chance of hospitalization or death from Omicron.
Commentators warn that because of its very high infectiousness, nearly everyone will be infected with Omicron at some point. However, the fatality rate is very low compared to other strains, although not zero. In order to reduce your symptoms, continue to supplement with Vitamin D, Vitamin C, and Zn. Costco carries a supplement with all 3 in the same pill! If you’re in a Northern state, you can also make Vitamin D by having an extended snowball fight with your kids on a sunny day. Don’t throw at the face, or it’ll be a short fight.
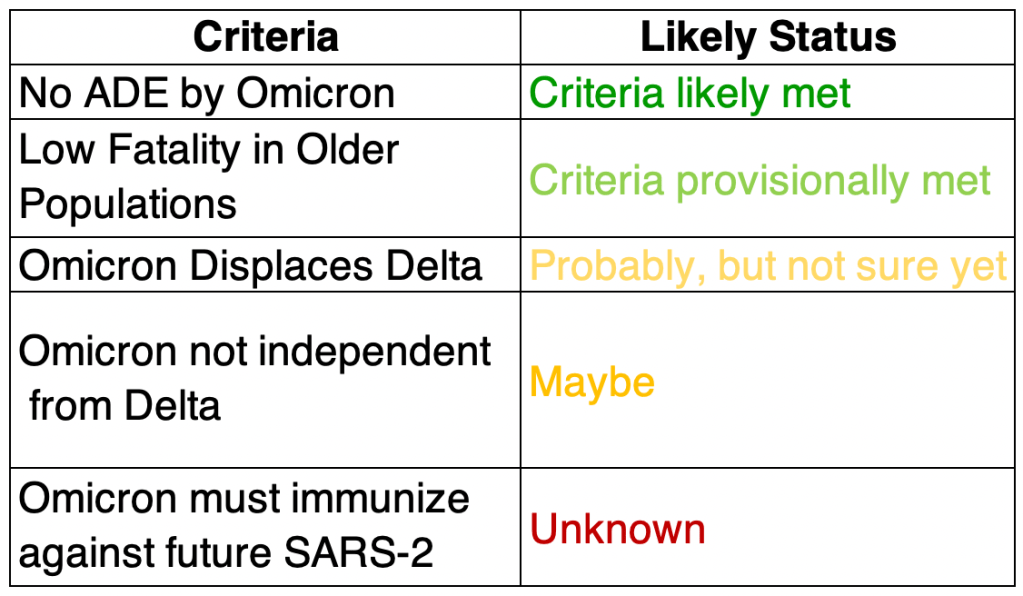
Will Omicron be a blessing?: Several commentators like John Campbell, Chris Martenson, and Mobeen Syad are feeling optimistic that Omicron really may represent the end of the pandemic. Here’s what needs to be in place for this to be a reality, and how the data stands right now. As a reminder, I am not an epidemiologist, I’m a molecular biologist. This is my informed but not expert opinion.
Omicron must not use the ADE pathway to produce more severe cases: Looking at the available data so far, while Omicron may preferentially infect those who have been previously infected, cases are still mild, and fatality rates very low. So for now, this criteria is met.
Low fatality in older populations: South Africa has a relatively young population, so reports of mild symptoms may not carry over to countries with older populations. At this point, it appears preliminarily in the UK that fatality rates are lower than with Delta, so I’m going to say this criteria is met with some caution.
The next 3 are related, but not exactly the same.
Displace Delta: Delta is currently the most common strain in the world, and almost 100% of COVID in the US right now. Omicron must displace Delta as the dominant strain. Binding of a more infectious SARS-2 strain to cells will prevent others from binding instead, so this criteria will likely be met.
Omicron must not circulate independently from Delta: Related to the above, if Omicron is very different from Delta, it may act as a completely different virus. There’s a chance that Omicron may displace Delta on the short term but still allow Delta to persist. Right now, most guess that Omicron will not be independent from Delta, but we’re not sure yet.
Omicron infection must immunize against future SARS-2: Since Omicron appears to infect those with immunity to Delta, it may be that it is different enough that it will not provide immunity to Delta or other SARS-2 strains. This criteria is not strictly necessary if Omicron completely displaces other SARS-2 strains (see 3 above), but it would be really nice to have some protection against future strains.
These are my criteria for whether Omicron is likely to end the pandemic. If all criteria are met, we may see a large reduction in COVID cases world wide in the coming months. I am not an epidemiologist, I am a molecular biologist. This is my informed but not expert opinion.
As of right now, I’m actually feeling optimistic about chances that Omicron will end the pandemic! It’s still too early to tell for sure. For myself, I continue to take precautions until more is known. Keep in mind that Delta is still almost all of the SARS-2 virus in the US right now, so it’s not time to run out and get your natural immunity to Omicron. Also, when Omicron hits hard in the US, a lot of people will be at home sick at once, so expect some economic disruption, and be prepared for colleagues to not be at work.
This is a case update. I’ll also discuss the first pre-print paper on Omicron, from a lab in South Africa.
Cases are rising in the US and cases in the Northeast are rising sharply at the moment. While the Omicron variant is now present in 19 states, most new cases are still from the Delta variant, and Omicron cases in the US are still very low.
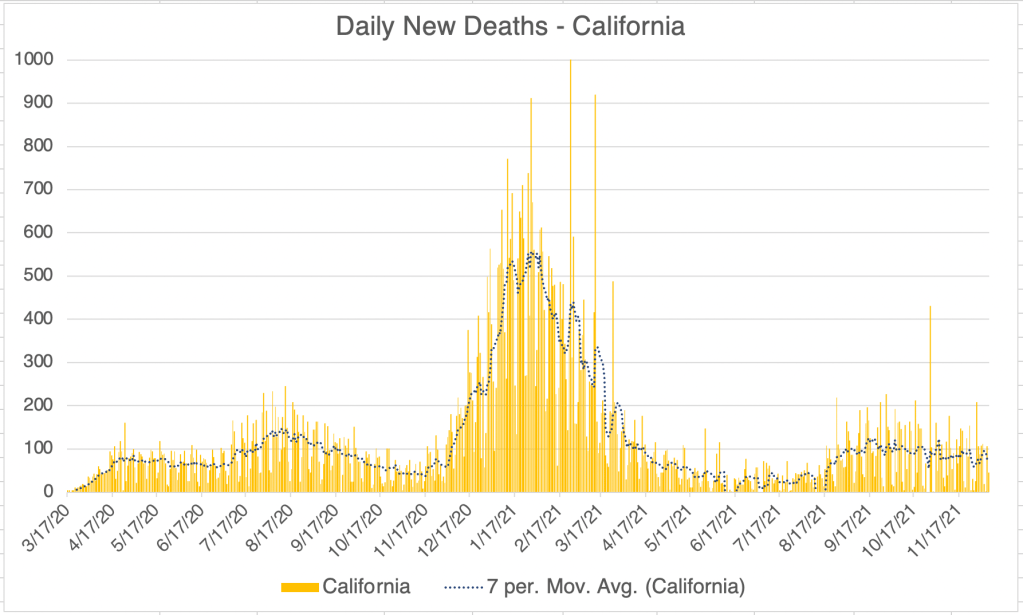
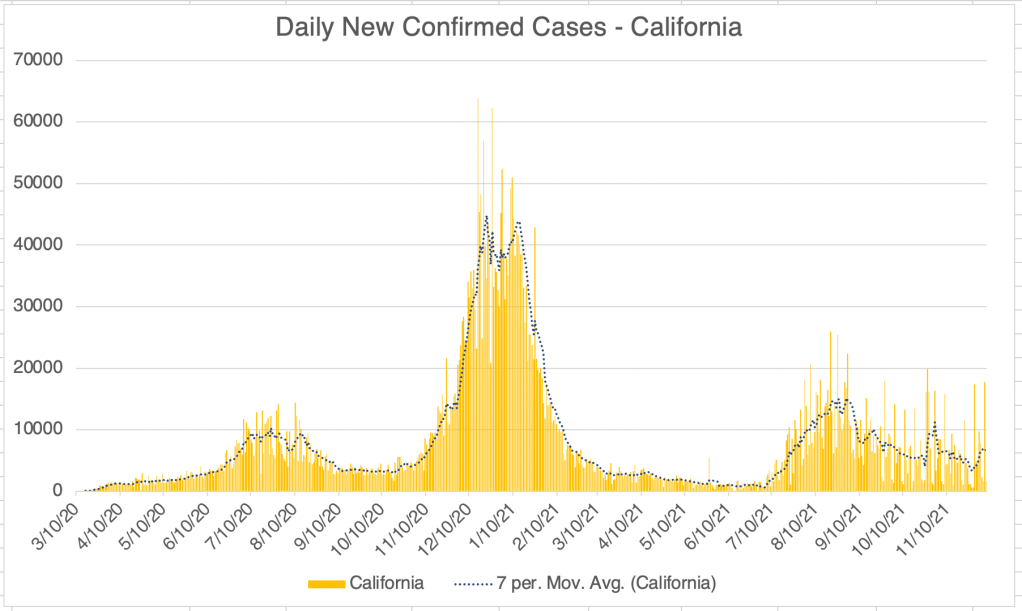
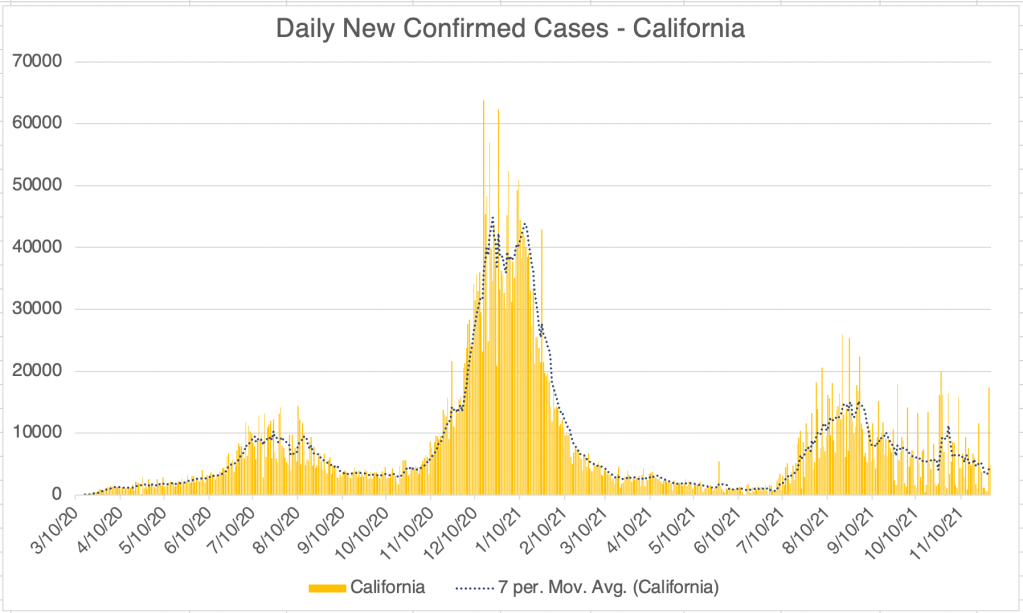
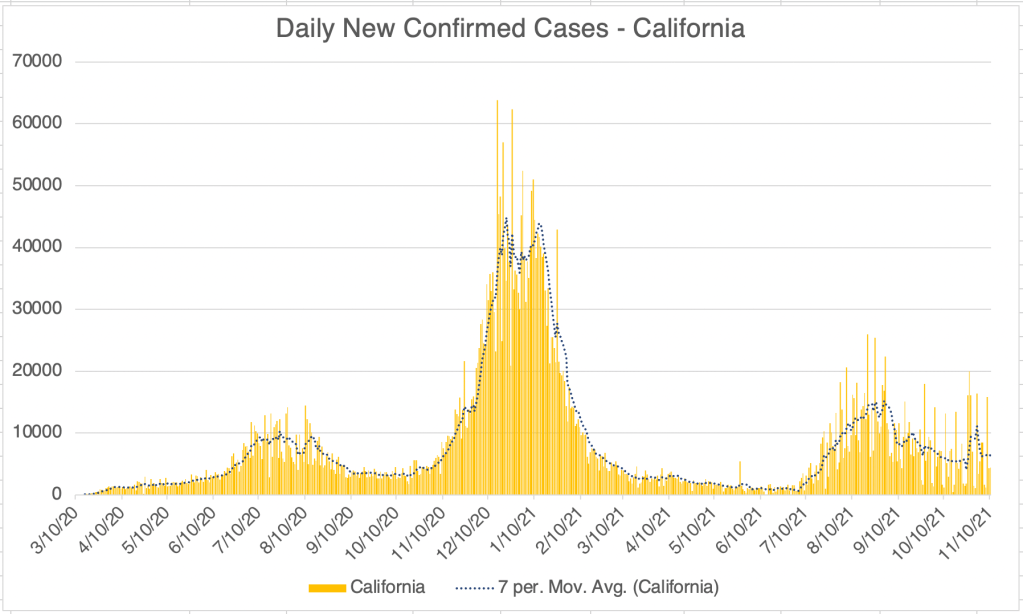
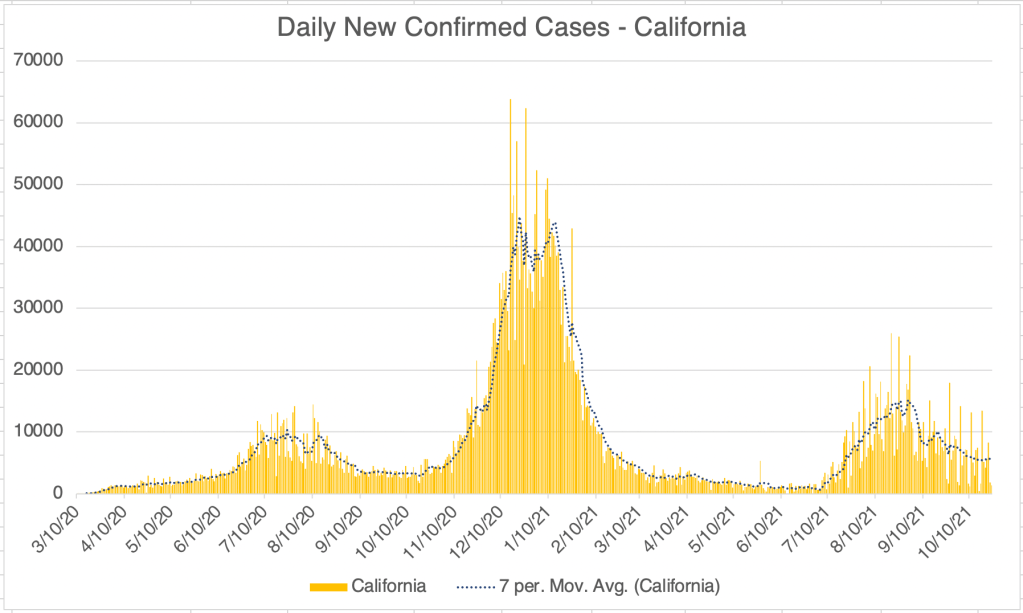
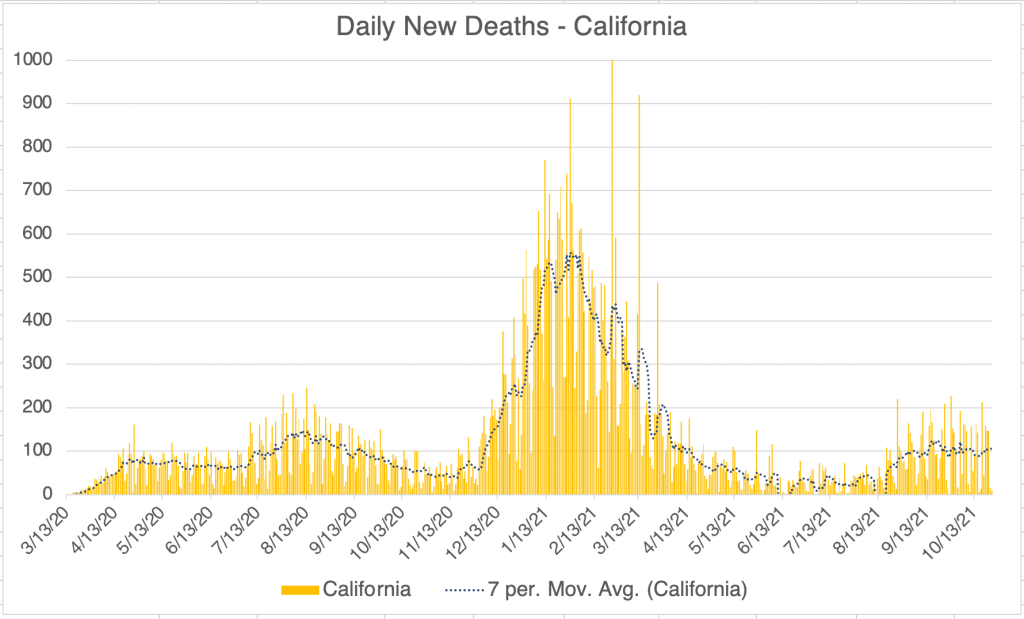
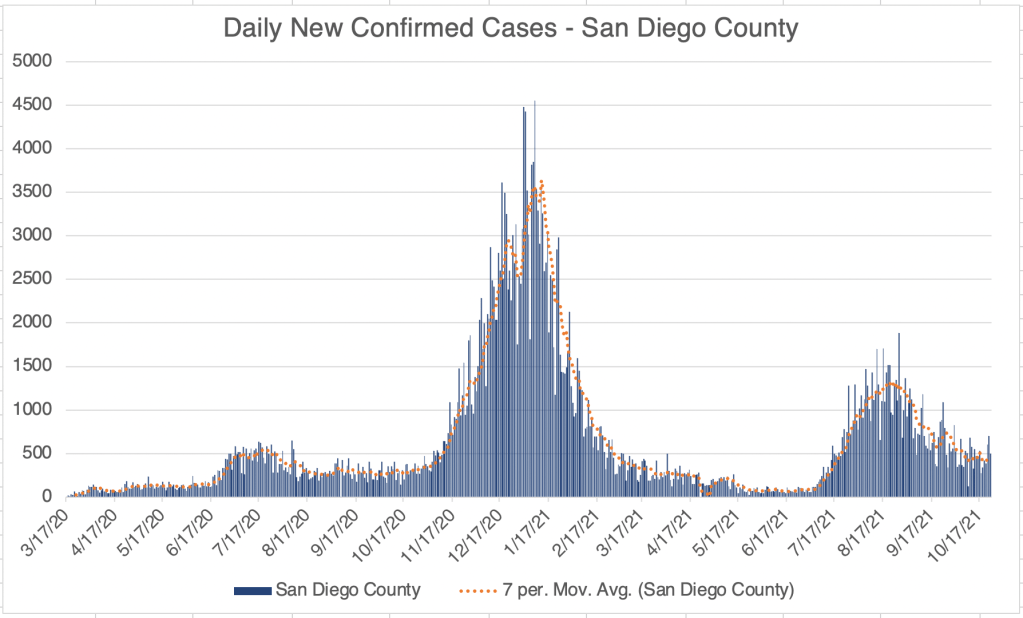
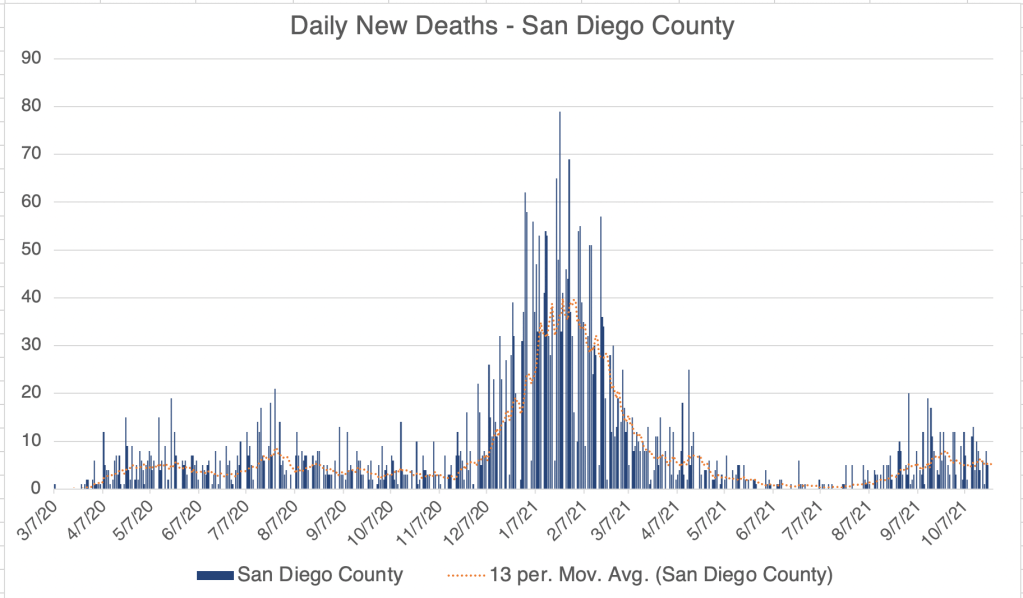
California is still not showing an increase in cases due to the Winter season, although the persistent number of cases after the Delta wave is still quite high, almost as high as last Summer’s wave.
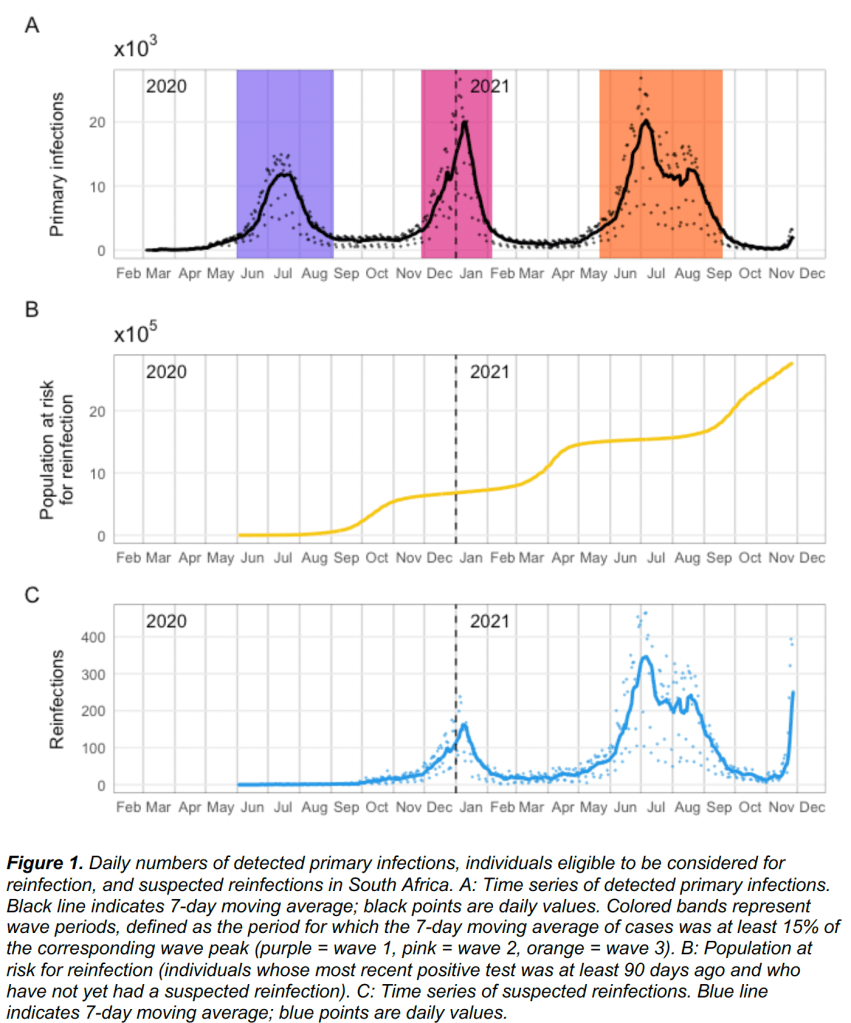
Omicron causes increased co-infection: A pre-print paper has been released from a lab in South Africa, Pulliam et al. The paper looks at Omicron infections and also previous history with other SARS-2 variants. Since vaccination is relatively low in South Africa, the ability of vaccination to prevent infection by Omicron is not accessed.
The big take away from the paper is that while previous infection with a Wuhan strain prevented infection with Beta or Delta variants, it does not prevent infection with Omicron, at least according to this study! In fact, Omicron may be using the ADE pathway to reinfect patients, as risk of infection with Omicron appears to go up if a person has had a previous version.
The paper does not directly address whether vaccination will prevent infection with Omicron, but at this point, it seems unlikely. Unfortunately, the paper also does not discuss case severity in Omicron patients. A previous report from Dr Angelique Coetzee suggested that symptoms from Omicron are mild.
This data suggests that getting one of the current vaccinations will NOT help to prevent infection with Omicron. If you have not been vaccinated at this point, I suggest you NOT get vaccinated now, but instead take precautions until we find out how severe infection with Omicron will be. Of course, I am a molecular biologist, not a physician. Consult with your physician when making medical decisions.
From Pulliam et al, the new South Africa paper. Case numbers from the initial wave, and Beta, Delta and new Omicron waves are shown in figure 1A. The Omicron wave is on the far right and does not have a highlight color band. In figure 1C, reinfections are shown. Notice the reinfections are very high for Omicron in proportion to infection numbers.
Monoclonal antibodies: Monoclonal antibodies are a common and effective treatment against SARS-2. They work similar to your own antibodies, but are often used early in disease before a person’s own immune system has yet been able to produce an immune response.
Medically useful antibodies can be obtained from a variety of sources, even purified from another person who has already had a disease. Monoclonal antibodies are made by first purifying immune B-cells from an infected animal or person, growing many copies of this cell in a lab, then purifying out the desired antibodies. These antibodies can then be injected into a patient to give them a boost in immune response.
And no, getting antibodies created from animal cells will not make you grow a tail or get beady little eyes.
If you get COVID, don’t hesitate to accept monoclonal antibodies if they are offered to you. They do not contain any vaccine components, nor do they involve any of the questionable ethical issues surrounding vaccines that are of concern to some.
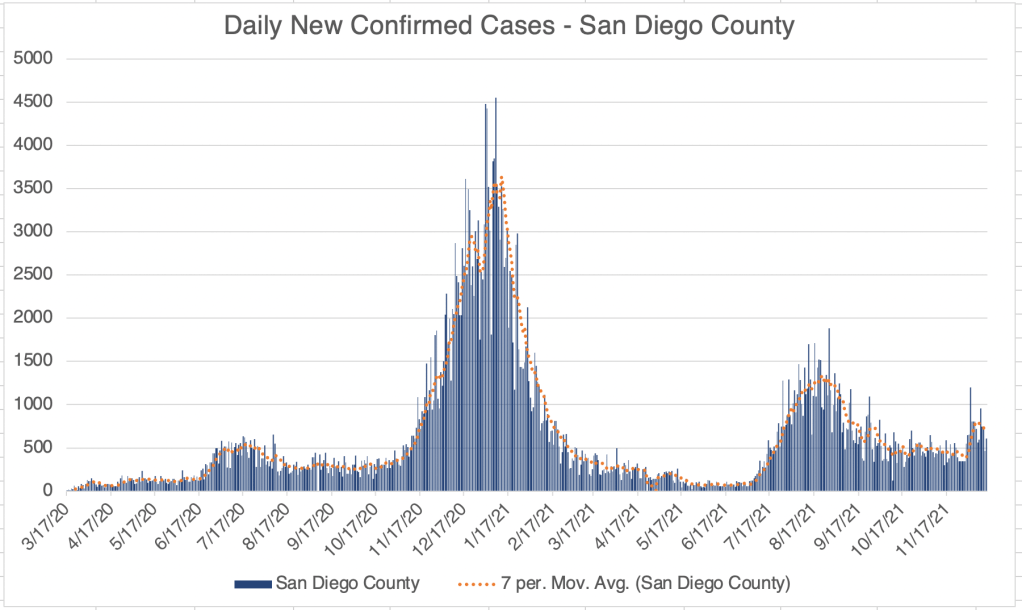
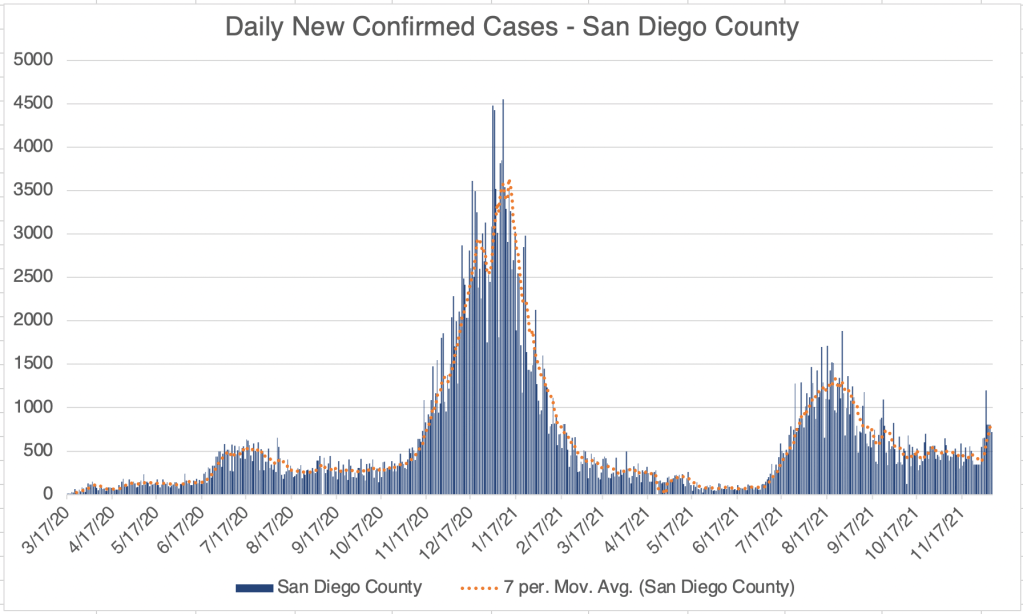
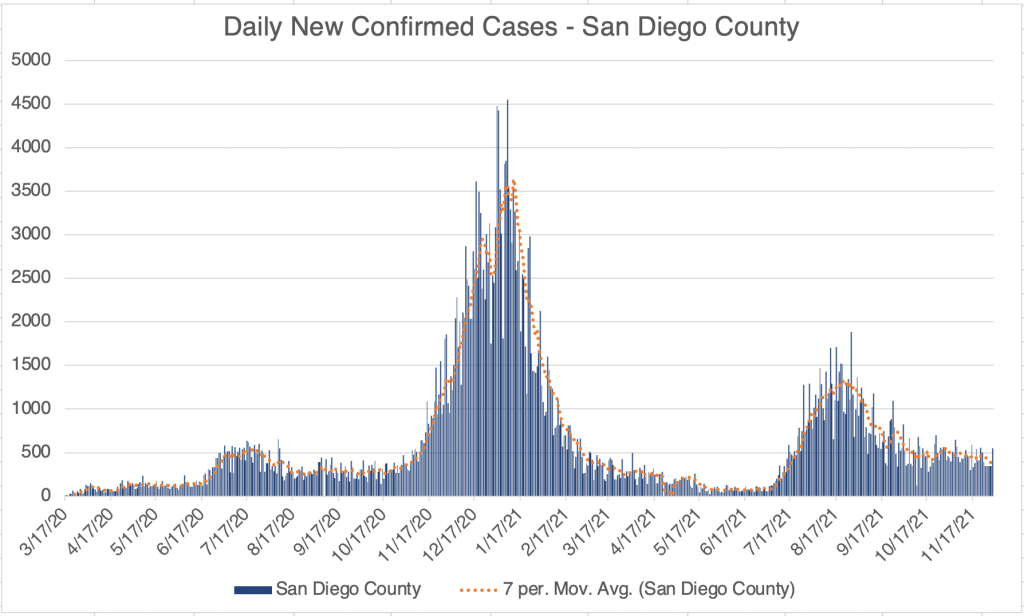
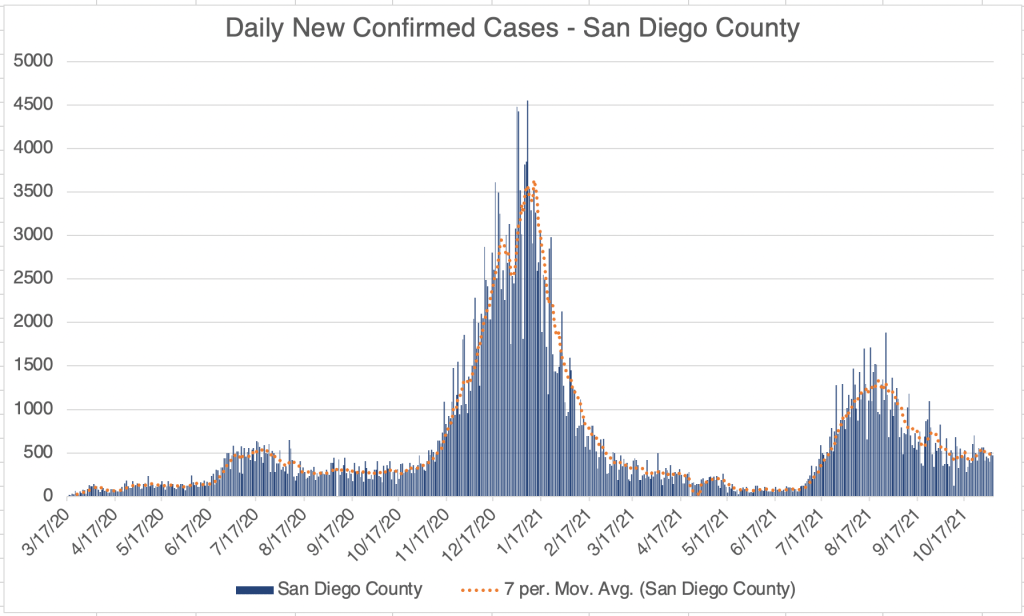
In California and San Diego County, cases are still stable, at a rate about as high as last Summer, but lower than the peak of Delta. Just hours ago, California Public Health and the CDC have announced that a patient with the Omicron variant has been detected in California. They had returned from South African on the 22nd, and the case was detected on the 29th.
_____________________________________ UPDATE: December 1st, 1:00 pm Just hours ago, California Public Health and the CDC have announced that a patient with the Omicron variant has been detected in California. They had returned from South African on the 22nd, and the case was detected on the 29th. _____________________________________ UPDATE: December 2nd, 2021 2 more cases of Omicron have been detected, in Minnesota and Colorado. The case in California and Colorado were in individuals who were fully vaccinated. All individuals have had mild symptoms so far.
Hours after reporting the above, another 5 cases of Omicron were reported in New York City. Suffice it to say, it’s now clear that Omicron is in the US and is already nation wide. I’m sure a lot more cases will be reported soon.
Most new cases of a new strain can only be reported after expensive and time consuming sequencing testing has been performed, so these results will come out more slowly than just a COVID detection.
I’m going to stop reporting individual new cases, since the point has been made that Omicron is in the US. _____________________________________
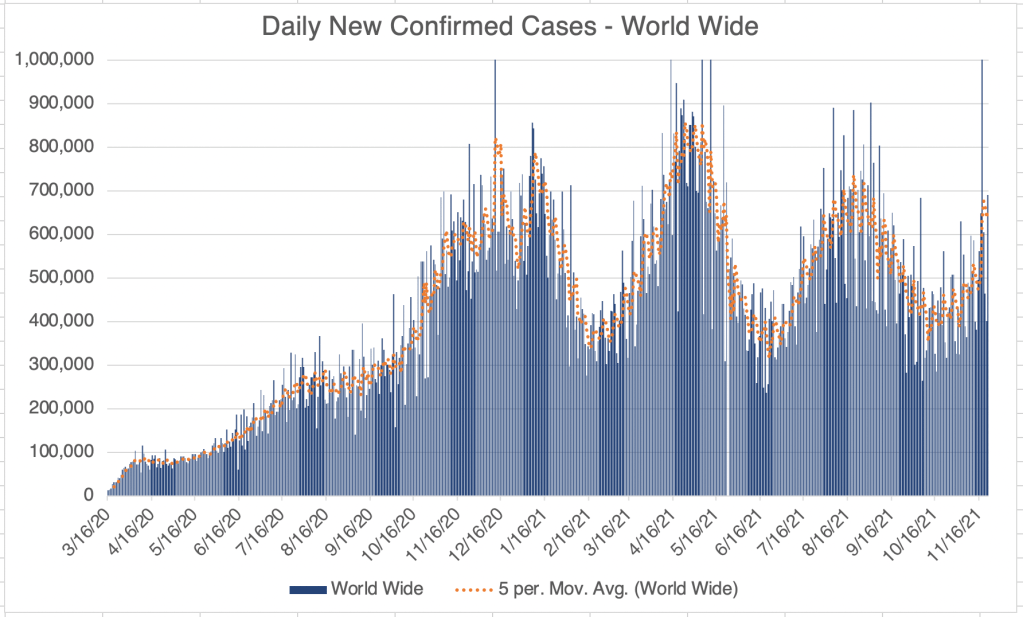
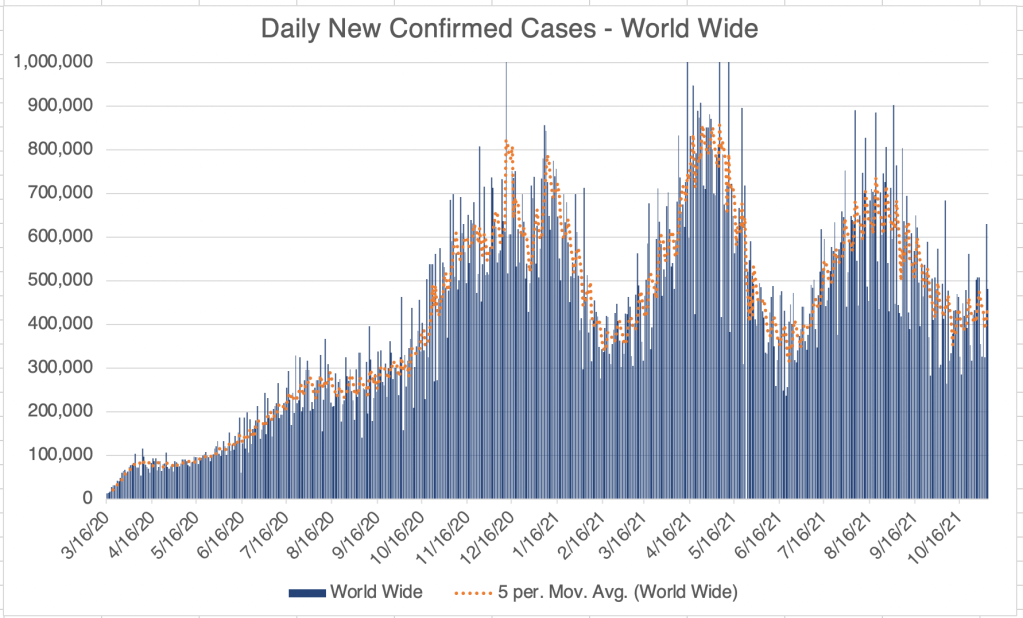
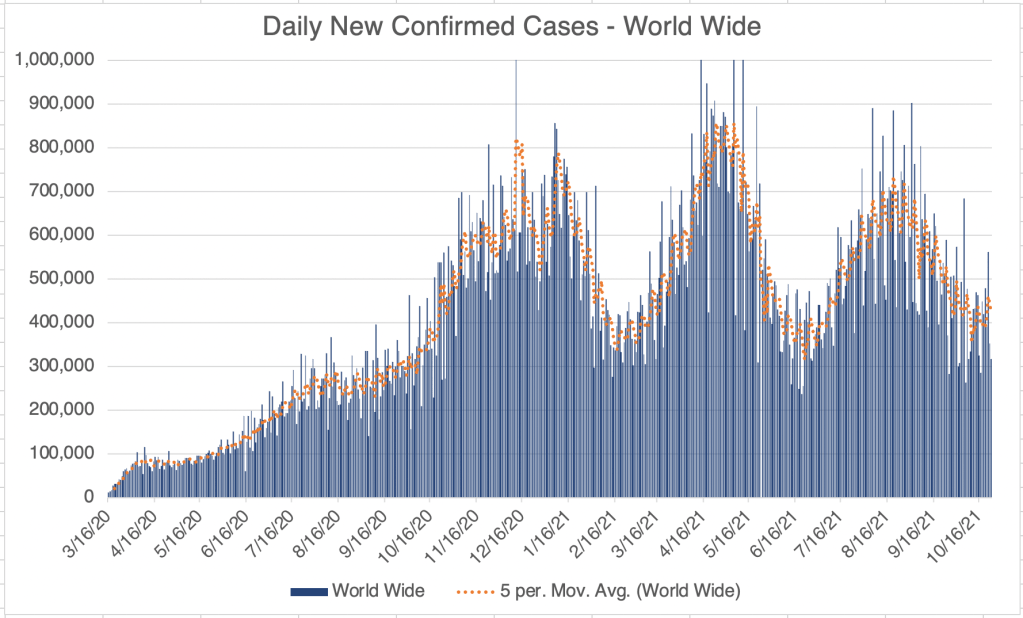
World wide, cases are climbing at the moment, with big increases in several European countries. Several countries have reported the detection of the Omicron variant, but so far only a few cases in each country are due to Omicron, so the big increase in cases may be due to Delta and the onset of Winter.
Vaccine against Omicron: So far, Delta is still the majority of cases world wide. Even in South Africa, only about 20% of the COVID cases are suspected to be due to the Omicron variant as of this writing. But because of the large number of mutations in the Omicron variant, scientists are concerned that the current batch of vaccines will not work against Omicron.
I saw an interview with Albert Bourla, the CEO of Pfizer. He stated that Pfizer could have a vaccine against Omicron ready for distribution in 100 days. Interestingly, Bourla also said in the interview that they had designed a vaccine against Delta, but they hadn’t released it because the original vaccine worked well against Delta. I was very discouraged by this comment. Many countries, including Israel, have been reporting that the vaccines have only been about 40-50% effective against Delta, and even the CDC admitted in July that 15% of COVID deaths have been in vaccinated individuals. I seems the me that the vaccines against the Wuhan strain have not worked well against Delta, and that vaccines against Delta should have been released. The comment seems to be evidence that Pfizer is not fully absorbing data on vaccine effectiveness from around the world.
Is COVID endemic?: I had hoped that once the vaccines came out, we would be able to generate enough immunity (natural and vaccine related) against COVID that it would go away. With 2 major variants that can evade the vaccine already out (Delta and Omicron), I’m becoming more convinced that COVID is indeed endemic at this point, meaning that it will continue to mutate, circulate, and be part of the fabric of life from here on out.
My personal strategy has been to avoid infection and vaccination until it all blows over. I’m becoming convinced that this will not work. So should I get vaccinated now? I’m concerned that Omicron might trigger the ADE pathway and cause worse symptoms for those with immunity to SARS-2. For this reason, I’m going to continue to keep myself SARS-2 free until more is known. Regardless of vaccination status, I encourage you to take some extra precautions until more is known about Omicron. Concern is good, panic is bad.
A glimmer of hope: As stated in Monday’s post, South African Doctor Angelique Coetzee has stated that her COVID patients have had very mild COVID symptoms. Her patients are mostly young people. If symptoms from Omicron are mild in older patients, and the new variant is very infectious, that there is a small chance that it will present a safe and effective way to provide immunity to lots of people. Of course, we will need to wait a few weeks to see.
Unfortunately, I have some concerning news on the COVID front. The WHO has identified a new variant, currently called B.1.1.529. The variant likely first arose in South Africa, but has already spread to several countries in Southern Africa as well as at least Hong Kong and Israel. It has an estimated 32 mutations in the Spike protein alone. The new variant has been assigned the Greek letter Omicron (O).
Omicron is currently estimated to be 500% (6x) more infectious than Delta. For reference, Delta was just 60% more infectious than Alpha. Because of the many mutations in the Spike protein, the new variant may evade current vaccinations.
Since Omicron is so new, there isn’t yet information on fatality rate. Historically, new viruses in a group tend to be more infectious and less pathogenic (disease causing) than previous versions.
Most outlets will never talk about Antibody Dependent Enhancement, but a new variant with a very different Spike protein has the potential to trigger the ADE pathway. I might recommend that you take more precautions until more is known.
The President has suggested that anyone who hasn’t been vaccinated should do so now. I disagree. Because of the possibility of ADE, vaccination may even be worse for you than not being vaccinated. Until we know more, take additional precautions regardless of vaccination status.
My precautions are: 1) Wear an N95, KN95, or KF94 mask indoors in public. These masks are rated to filter out 95% of viral particles. In my opinion, surgical masks and especially neck gators are nearly worthless in these settings. 2) Keep 6 ft away from others. (I basically ignore this one if other precautions are in place, especially on an airplane!) 3) Avoid indoor gatherings, especially ones in which singing or shouting is likely. 4) Outdoor gatherings are fine, even without masks, if everyone maintains a distance. I have hosted several outdoor gatherings. 5) While many restaurants are open for limited indoor seating, I personally am still not comfortable eating indoors at a restaurant. I enjoy eating outdoors at restaurants, however. 6) I never take my mask off on the plane, and find an isolate spot in the airport to eat or drink on layovers. 7) If you find you can’t do any of the above, try to produce as much ventilation for yourself as possible. Sit next an an open window, choose larger rather than smaller indoor areas, or use a number 10 Honeywell air filter in your home or office. You can even make a virus filter out of a box fan and a number 10 filter.
Because Omicron is new, and may trigger the Antibody Dependent Enhancement pathway, vaccination may be either worthless or even detrimental. We’ll just have to see. Even vaccinated people should be more careful until we know more.
This story is early and evolving, and will let you know when I have substantial information to share.
__________________________________________ Updated November 29th, 2021:
There is a little more news about the Omicron Variant. South African Doctor Angelique Coetzee was the first Doctor to alert health care authorities about the new variant. She says that symptoms are more mild than for previous versions, causing severe fatigue for a new days, but no cough and no loss of smell and taste. She cautions that most of her patients are relatively young and healthy, so she can’t yet say how symptoms will be for older patients.
Worse or Better?: With a huge number of mutations (34 in the Spike protein alone) the Omicron variant has the potential to be much worse than previous versions, because it may trigger the Antibody Dependent Pathway and make infections worse for those who have already had COVID. It is also likely to at least partially elude vaccination, putting us back to square one in terms of vaccination efforts. Omicron is also 6x more infectious than Delta.
The Omicron variant has 53 mutations relative to the original Wuhan strain. 34 of these are in the Spike protein. Delta has only 9 mutations in the Spike protein. Photo is from the Stanford University Variants Genome Viewer.
On the other hand, there is currently a chance that Omicron may be a blessing in disguise. IF symptoms are truly mild, and the fatality rate from Omicron is very low, the variant may spread very quickly and infect large populations with a mild disease, giving them safe immunity.
So at this point, there is a broad range of potential outcomes. I know many of you are “over it” and are living life normally at this point. However, I urge some increased caution at this moment, until we know more about the new variant. It will probably take a few weeks before we know how things will go.
At this point, I do not recommend strict lockdowns as practiced last year. Last years lockdowns did not prevent the spread of SARS-2, and had many more negative impacts. I recommend instead protecting your self from infections by taking the precautions listed above.
The United States and several other governments have put restrictions in place for travel to South Africa. The South African government is complaining that they are being punished for being transparent about the virus. I have mixed thinking about this. South Africa is to be greatly commended for being open and sharing information about Omicron, unlike the Chinese government when this all started. However, I do think it is warranted to be cautious regarding travel. We should take a pause while we access the situation.
I predict, however, that as countries sequence virus detected in patients, they will soon discover that Omicron is already wide spread. It may already be too late for travel restrictions to have a big impact. The new variant has already been detected in Israel, Hong Kong, the UK, the Netherlands, Portugal, and many other European countries. Given the extreme contagiousness of the new variant, it is likely already wide spread. ______________________________________________ UPDATE: December 1st, 1:00 pm Just hours ago, California Public Health and the CDC have announced that a patient with the Omicron variant has been detected in California. They had returned from South African on the 22nd, and the case was detected on the 29th. ______________________________________________ UPDATE: December 2nd, 2021 2 more cases of Omicron have been detected, in Minnesota and Colorado. The case in California and Colorado were in individuals who were fully vaccinated. All individuals so far have had mild symptoms. ______________________________________________
This is a case update. I’ll also discuss data suggesting that the v@¢¢¡nes are having a mixed effect.
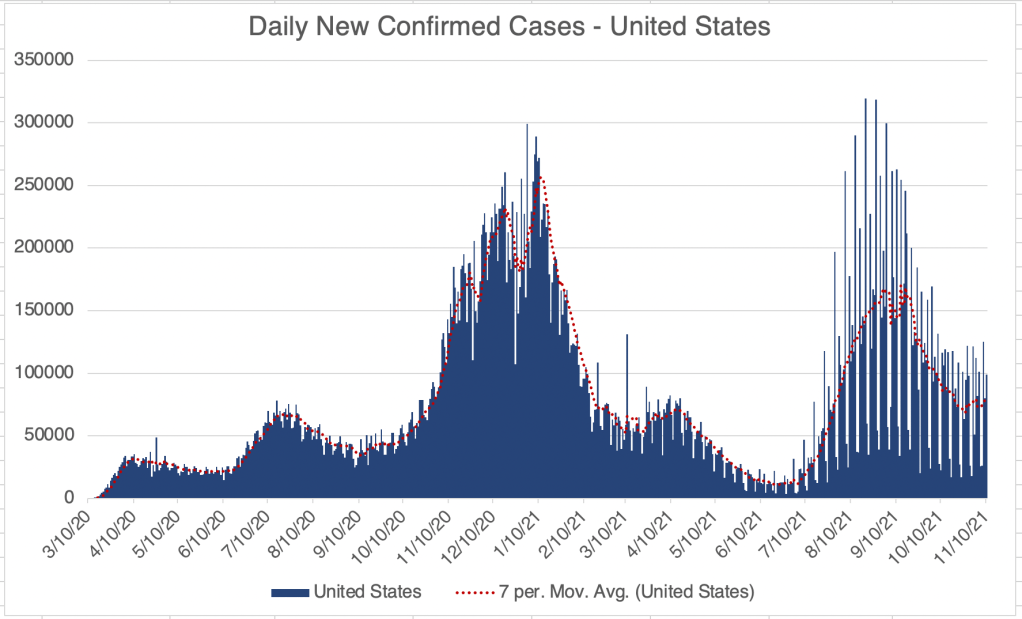
For the US, new case numbers have begun to creep back up. Several states like Vermont, Minnesota, Colorado, and West Virginia are experiencing increased cases right now. This is likely at least partly because colder weather is forcing more people inside. Several states are still enjoying decreasing case numbers after the Summer Delta wave, like Oregon, Washington, Alaska, and the Southern states.
Last year’s Fall wave started in October, so it’s good news that a new wave may just be starting now, but keep in mind that new case numbers are just as high now as they were at the peak of last Summer’s wave.
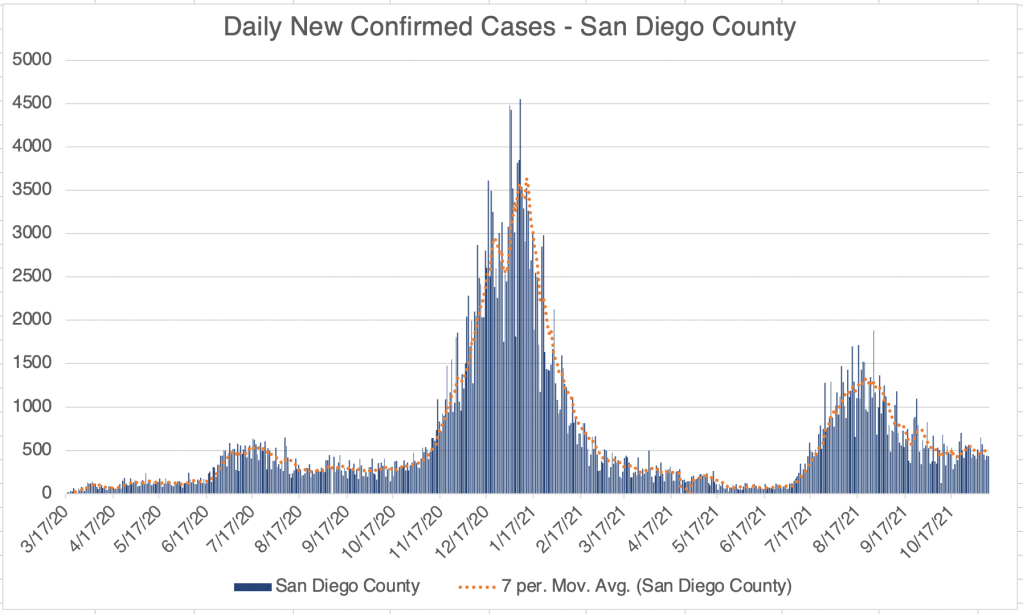
In California and San Diego County, new case numbers are persistent, at around 5000 and 500 new daily cases respectively. The higher persistent number likely reflects the higher infectiousness of the Delta variant.
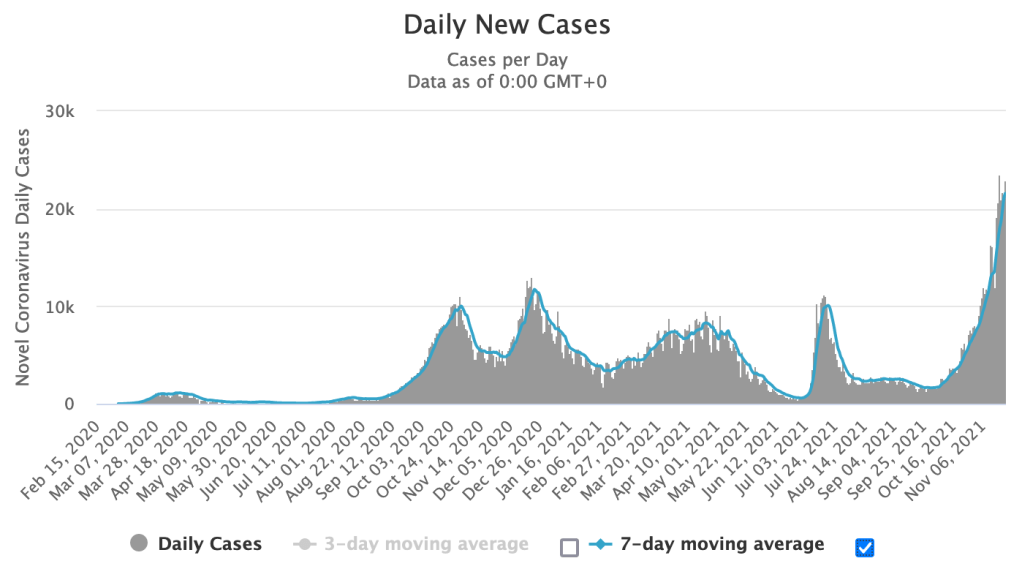
Internationally, several European countries like Germany, the Netherlands, Hungary, and Czechia are experiencing increasing numbers of cases right now.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Daily new cases from Germany, November 23rd, 2021.Daily new cases from the Netherlands, November 23rd, 2021.Daily new cases from Czechia, November 23rd, 2021.
V@¢¢¡ne effectiveness: A pile of new papers have come out regarding v@¢¢¡ne effectiveness. A few weeks ago, I discussed Subramanian et al which claimed that v@¢¢¡nation rates are not correlated to case numbers internationally. New papers from Britain, Germany, and even a story on msn.com are claiming that v@¢¢¡ne effectiveness is becoming reduced.
The British paper states something I’ve suspected for a long time, that most SARS-2 transmission takes place in households, explaining why lockdowns are not an effective means of controlling COVID. They also claim that v@¢¢¡nation status is nearly irrelevant in a household setting, because of long term exposure to family members.
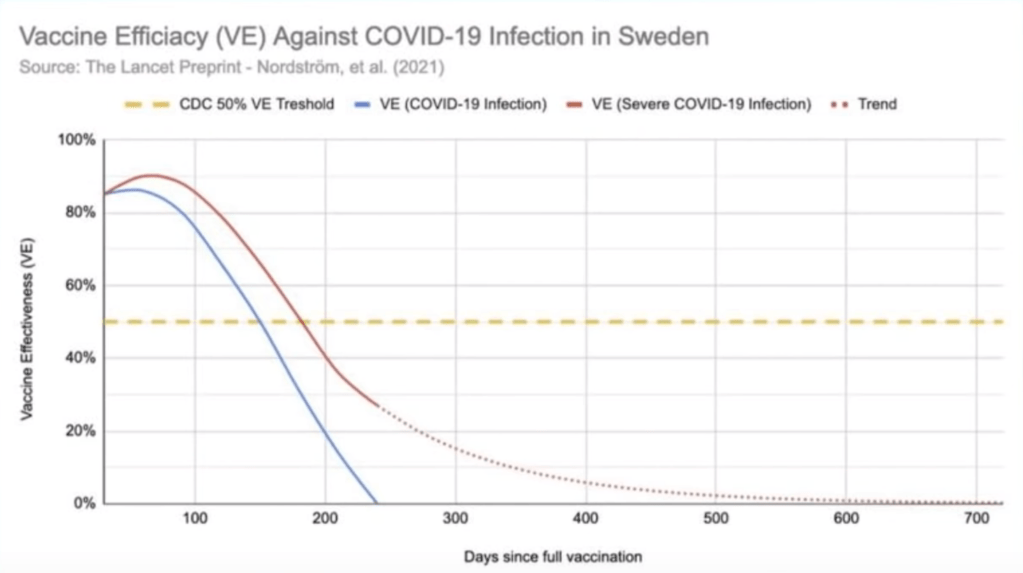
A Swedish paper (Nordström et al) suggested that v@¢¢¡ne effectiveness is reduced over time, especially for elderly men and those with co-morbidities. Effectiveness against severe symptoms begin to be reduced after about 9 months.
Disturbingly, some have suggested that v@¢¢¡nation is doing more harm than good. A set of British data claims that v@¢¢¡nated individuals are dying at twice the rate of the unv@¢¢¡nated.
A German analysis of national data comparing German states is claiming similarly that excess mortality is actually due to v@¢¢¡nation.
Meanwhile, in the US, the CDC is claiming that v@¢¢¡nation greatly reduces the chances of hospitalization and death, although not to zero. The agency currently claims that the unv@¢¢¡nated are 5.8 times more likely to become infected and 14 times more likely to die than v@¢¢¡nated individuals.
What are we to make of all this? Is the v@¢¢¡ne really making people sicker? Are things different in the US and Europe? It’s hard to know right now. We are in a period when v@¢¢¡ne effectiveness may be going down right now, so we may be getting mixed signals because we’re seeing this in real time. The Delta variant is certainly exacerbating the issue, eluding antibodies developed against the Wuhan strain. We also have to consider that we may be seeing the effect of Antibody Dependent Enhancement (ADE), which may cause greater symptoms in those already infected with a related strain.
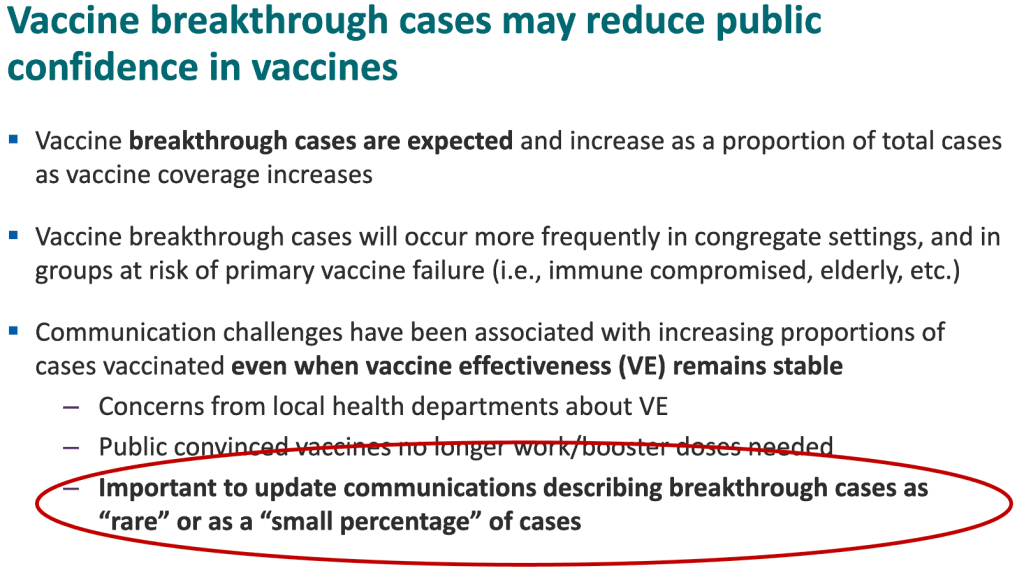
The present confusing situation is a great example of why it’s so crucial to accumulate as much data as we can, and to be as objective as possible about the results. US agencies are still openly admitting that they have as a goal to promote vaccination (see slide 2),
From CDC powerpoint, July 29, 2021, slide 2. Red oval is mine.
I cannot stress strenuously enough that if we work from incomplete or faulty data, we have no hope but to come to faulty conclusions and bad solutions. If you have a hole in your gas tank, it doesn’t matter how much gas you put in it. You will still have no gas. You have to deal with the real problem first.
The CDC has one and only one job. To produce data and guidance on how to fight disease. But the very sad fact is that I don’t trust the CDC to produce truthful and/or complete data. This is why we are relying on papers from foreign sources like Britain, Israel, and Japan to inform us on how to approach COVID. With all the cases here, and 53 different approaches to the virus, we should have the best and most complete data set for figuring out what to do. But politics continues to make this impossible. I hope this will change.
As discussed in the paper by Liu et al, boosters against the Wuhan strain will likely not offer long term protection against the Delta strain. Instead, those who have been v@¢¢¡nated should get a v@¢¢¡ne against the Delta strain as soon as it is available.
Most people with severe symptoms are Vitamin D deficient. If you aren’t already, remember to be supplementing with Vitamin D, Vitamin C, and Zinc in order to reduce symptoms and viral load if you should be infected. Most Americans, especially those with darker skin, are Vitamin D deficient, since we spend so much time in doors. Alternatively, make your own by spending 30 minutes outside per day in shorts and a T-shirt!
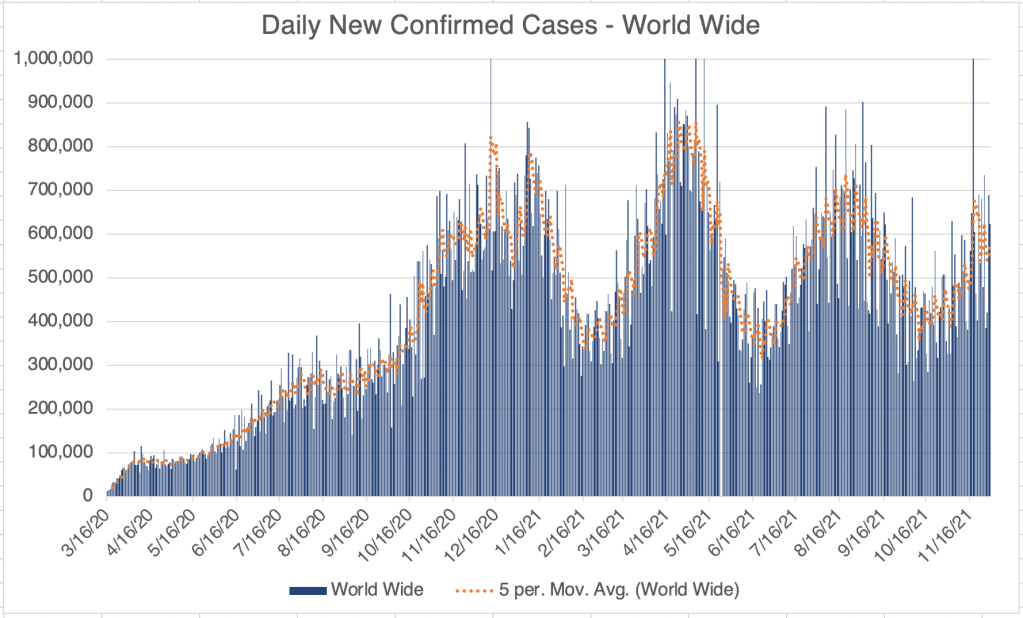
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.”
This is a brief case update. For the US, California, and San Diego County, new cases have reached a persistent level. While cases are not going down in these regions, I will point out that last year at this time, we were beginning a big Fall/Winter wave. As of right now, we are not seeing cases rise, but stay steady. So in spite of stable cases, we are not seeing a new Fall wave either. I take this as good news overall.
This is a case update. I’ll also talk about the newly release v@¢¢¡ne mandate from OSHA, whether you should get a booster, and the question of whether v@¢¢¡nes lead to new SARS variants.
New cases in the US, California, and San Diego County are all fluctuating right now. It’s hard to say if this represents the beginning of a new wave. Most of us are feeling like the pandemic is basically over, but I will point out that in the post-Delta trough, we still have as many new cases per day as we did at the peak of last Summer’s wave. Minnesota, Colorado, New Mexico, and Arizona are all experiencing increases in cases right now.
V@¢¢!ne mandate finally drops: In September, the President said he wanted government agencies to produce a mandate for v@¢¢¡nation. Just this week, OSHA issued an Emergency Temporary Standard. This is official form of the v@¢¢¡ne mandate we’ve been waiting for. The mandate conforms to the news you’ve heard, all employers with more than 100 employees must get v@¢¢¡nation status from all employees, and those who are not v@¢¢¡nated must be tested weekly. The testing option means that the standard does NOT require that everyone be v@¢¢¡nated. Enforcement will begin January 4th, 2022.
As we saw last week, the CDC has known since July that a significant number of hospitalizations and deaths have occurred in fully v@¢¢¡nated individuals. In addition to this, a recent Lancet paper from Singanayagam et al suggests that the transmission of Delta is less from v@¢¢inated individuals, but is still very significant. In light of this, I think all employees, regardless of v@¢¢¡nation status, should be tested regularly, although it would be impossible to test everyone every week. Ignoring the transmission threat from v@¢¢inated individuals is likely to lead to trouble. Everyone exposed to someone who tested positive for COVID should also be tested.
I saw a truly amazing thing on an OSHA FAQ page regarding v@¢¢ination. I checked it again just now to make sure it was still there. Under the item “Are adverse reactions to the COVID-19 v@¢¢¡ne recordable on the OSHA recordkeeping log?” The answer reads:
DOL and OSHA, as well as other federal agencies, are working diligently to encourage COVID-19 vaccinations. OSHA does not wish to have any appearance of discouraging workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers’ vaccination efforts. As a result, OSHA will not enforce 29 CFR 1904’s recording requirements to require any employers to record worker side effects from COVID-19 vaccination at least through May 2022. We will reevaluate the agency’s position at that time to determine the best course of action moving forward.
In effect, an official government page is saying, we are asking you to ignore health information in order to get people to do what we want. Some of you may be wondering why so many people are willing to ignore official calls to get v@¢¢¡nated, or are suspicious of government in general. This is why. This also answers the question as to why it is so difficult to get clear information on adverse events. The government appears to have an official policy of ignoring these events.
I’ll say again what I’ve said many times, I am not anti-v@¢¢¡ne. I think many people with risk factors including age, obesity, respiratory or cardiac issues, those who work closely with the public, etc. should get v@¢¢¡nated. However, I am against a v@¢¢¡ne mandate. I am not v@¢¢¡nated, mostly because of the ADE issue, and because I think I can avoid being infected.
I will also state what is obvious to many, but not to some that are making policy. Lying or hiding information from the public will make people mistrust you. You can sometimes force people to comply, but you cannot, even in principle, force people to trust you. Trust must be earned. Once you lose it, it is very difficult to get back.
This rule can be applied to any area of life. Remember this if you’re a husband, wife, parent, child, pastor, politician, consultant, leader of a company, employee, or anything else where trust is required. Trust is earned, and once broken, is very hard to get back.
Should you get a booster?: Several people in the past few weeks have asked me if they should get a booster. Right now, unfortunately, my best answer is “I don’t know”. A booster may improve your immune response to the originally Wuhan strain of the SARS-2 virus, but the Spike protein from the v@¢¢¡ne is likely toxic on it’s own. In addition, the paper from Japan I wrote about some time ago suggests that another booster of the current variety is unlikely to provide complete protection against Delta. Instead they recommend a Delta derived booster.
Anyone who has had COVID or has been v@¢¢¡nated should get a Delta v@¢¢¡ne as soon as it is available to protect from any ADE related effects. Several companies are currently working on v@¢¢¡nes against Delta.
Does the v@¢¢¡ne create variants?:A nobel prize winning scientist is claiming that v@¢¢¡nation creates SARS variants. I absolutely agree that v@¢¢¡nation creates selection pressures that can force viruses to gain new forms to avoid neutralization. However, the very same can be said for natural immunity. Both natural immunity and v@¢¢¡nation create selection pressures that can lead to new viral variants. This is true of all viruses and other invading agents. In spite of this, our bodies are designed to use the immune system to fight off infection, and immunity has had a tremendous benefit, despite the selection pressure it poses. ADE is a rare exception to this rule. Our immune systems work much more quickly than viruses can adapt to them, which is why they are so effective at preventing infectious disease.
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.” _______________________________________
For California and San Diego County, however, there is a persistent higher case number, and the numbers for last week may even reflect a very slight increase in new cases.
The very large wave from last Fall and Winter started in October. We may be seeing the very beginnings of a Fall wave. Hopefully our Summer Delta wave will have provided some extra immunity.
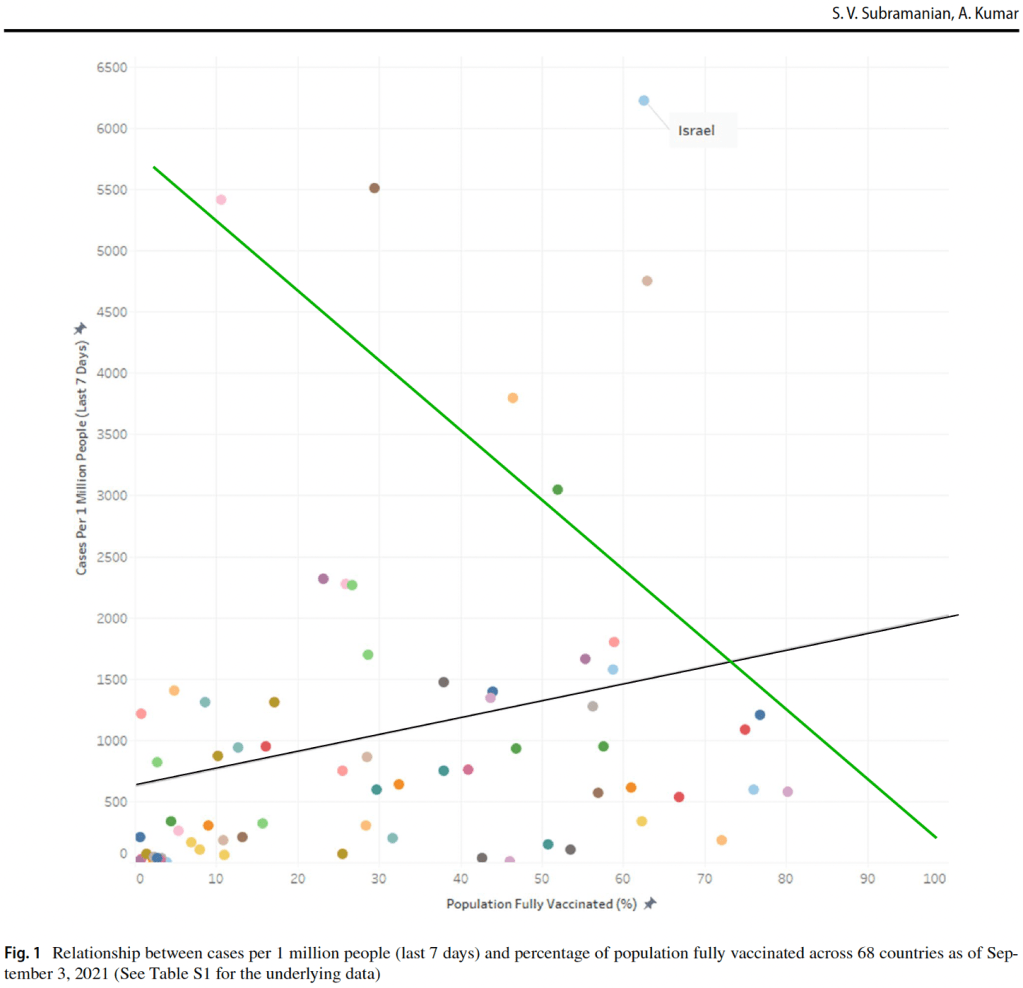
V@¢¢!nation and new cases: A paper came out in September regarding the correlation between v@¢¢!nation rates and new cases. The study compares data in 68 countries and 2947 US counties that had 2nd v@¢¢!ne doses available.
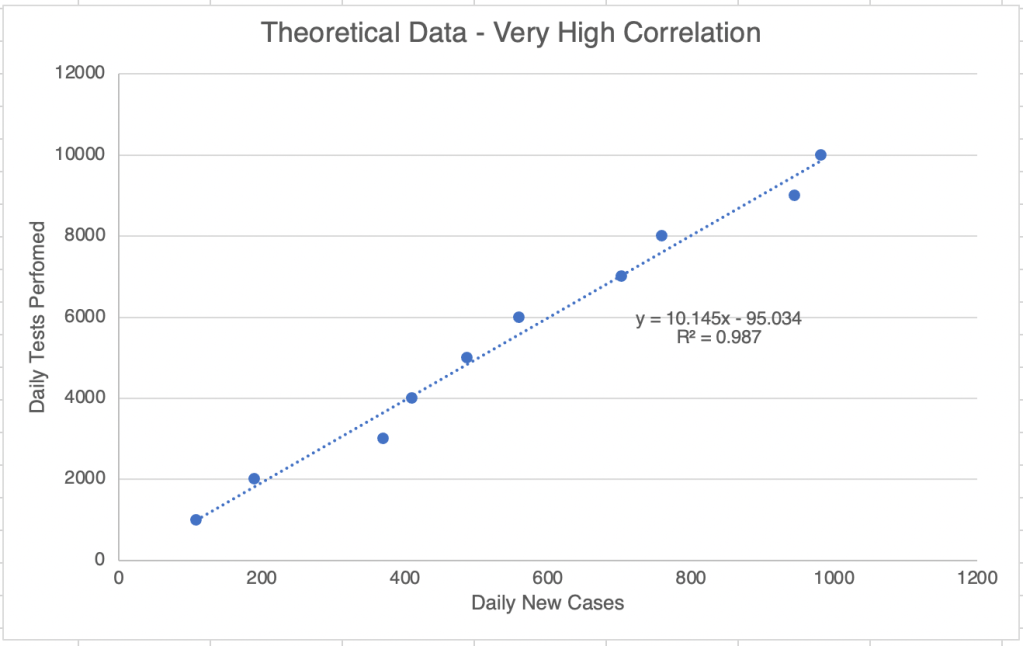
The most interesting figure features a piece of data called a “linear regression”. This kind of data compares 2 variables and shows visually if they are related. In the below hypothetical example, the 2 variables, the number of tests in a day and the number of confirmed cases in a day, shows a high correlation between these 2 things. Notice that the line plotting the relationship between data points goes from bottom left of top right as the values of each variable increase.
A linear regression plot with hypothetical data. Good correlation gives an R squared value between 0.95 and 1. If the variables are negatively correlated, the R squared value will be between -0.95 and -1.
The paper shows a linear regression plot with the percent of the population that is fully v@¢¢!nated on the x-axis, and the per capita confirmed case rate on the y-axis. If v@¢¢!nation strongly protects individuals from infection, new cases would go down as v@¢¢!nation went up. In this case, the plot line would go from top left to bottom right (the green line). Instead, it appears that there is little correlation between percent v@¢¢!nation and cases, producing the black line.
V@¢¢!nation vs cases produces black line, showing little correlation between the 2 variables. The green line was added by me and shows hypothetical data that would show strong correlation. From Subramanian et al.
They also have a box plot with US counties showing the new per capita case loads arising from counties with various levels of v@¢¢!nation. While counties with high v@¢¢¡nation rates do have fewer cases, the impact is not as profound as might be expected, and the difference between counties above 50% v@¢¢!nation rate is likely not statistically significant.
Box plots showing v@¢¢¡nation vs per capita cases in US counties. V@¢¢¡nation rates are groups in blocks for this view. Notice that very little difference exists between counties above 50%. From Subramanian et al.
It should be noted that this study was performed in September with data mostly from August. This is during the Delta wave in the US and many Western countries. The Delta variant may be different enough from the original Wuhan strain to enable the Delta virus to avoid neutralization by Wuhan induced immunization.
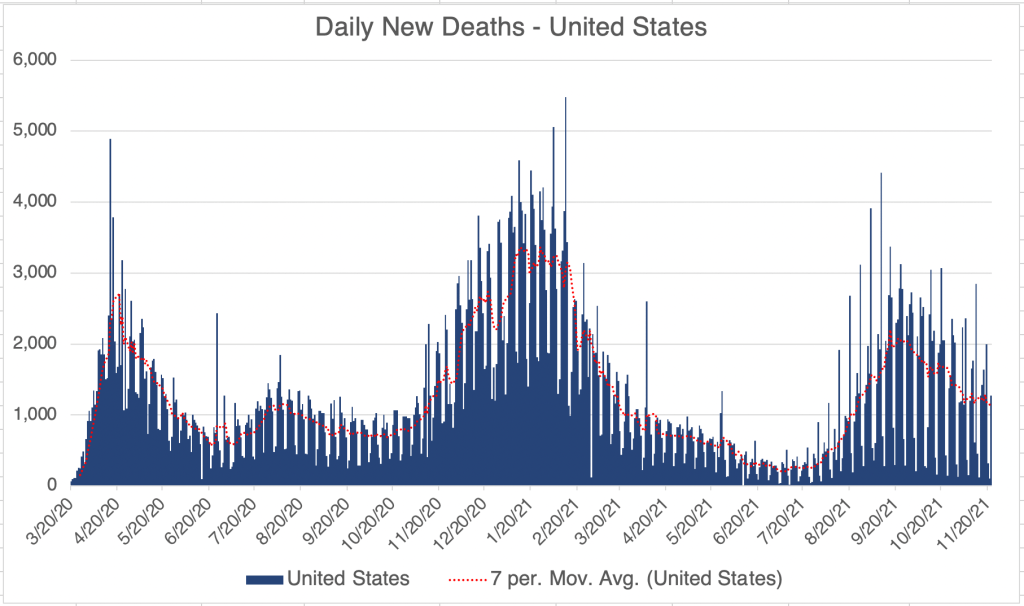
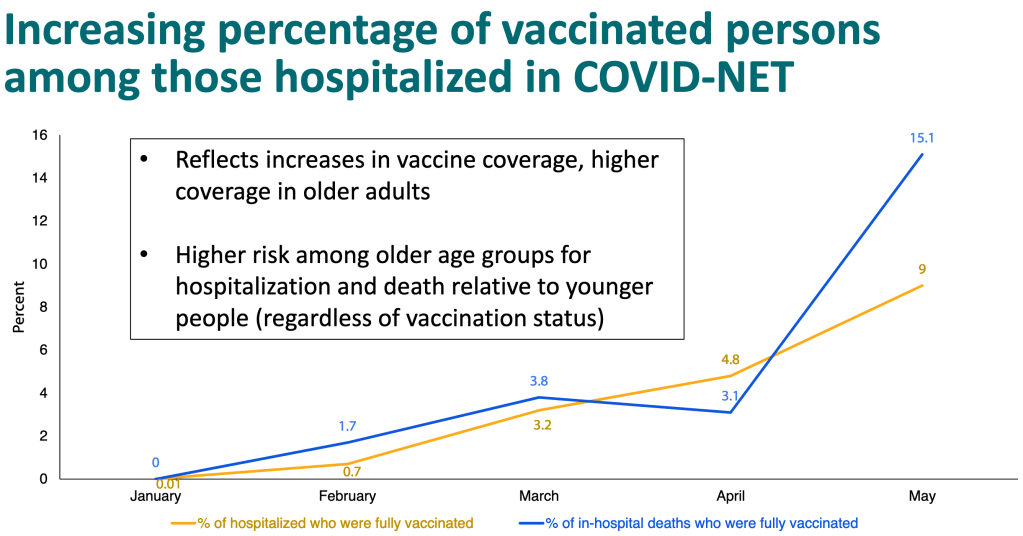
It has long been rumored that v@¢¢!nation does not prevent infection, and this paper seems to support this view. In spite of this, most scientists, including me, still hold that v@¢¢!nation does reduce the chance of hospitalization and death in infected patients. This is still true. However, a power point published by the CDC shows that this protection is diminishing as well. In January, hospitalization and death among v@¢¢!nated individuals was essentially 0%, but now 9% of hospitalizations are among v@¢¢!nated people, and 15% of deaths.
Why is this happening? There are likely multiple factors. Certainly, the Delta variant is not the same virus as the Wuhan strain. The different Spike protein makes it more infectious, and may not be recognized by an antibody against, the Wuhan strain. It may even be triggering the Antibody Dependent Enhancement (ADE) pathway in some patients. Also, it is becoming clear that v@¢¢!ne mediated immunity has been going down over time, necessitating a booster. The paper from Liu et al argued that given the differences in Delta, a booster against Delta would be much more effective than another booster against the Wuhan strain.
V@¢¢!ne mandates: I still believe that v@¢¢!nation is a good choice for some with risk factors like age, obesity, diabetes, or respiratory problems. However, I remain against v@¢¢!ne mandates because they do not take into account the medical history of individuals, the data that natural immunity is significantly better than v@¢¢!ne mediated immunity, and also the potential danger of ADE. In addition to these scientific reasons, I have also felt an increasing orneriness on my own part. Orneriness is not a good reason to make scientific or medical decisions, but policy makers should realize that it is a powerful reason for many.
For myself, I have chosen to not be v@¢¢!nated, but to remain careful to not be infected. I continue to wear a mask indoors when there is poor ventilation.
President Biden mandated v@¢¢!nation for federal agencies soon after taking office. He announced in September that he would seek v@¢¢!nation mandates for private companies with more than 100 employees. While many assume that a mandate for private companies is in effect now, as of this writing, no such mandate for private companies actually exists, either by law or by executive order. Companies that have enacted v@¢¢!ne mandates as of now have done so voluntarily.
________________________________________________ Update: November 5th, 2021
The official vaccine mandate was released on November 4th 2021 and is scheduled to be enforced starting on January 4th 2022. Details are on my November 5th post. ________________________________________________
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.” _______________________________________