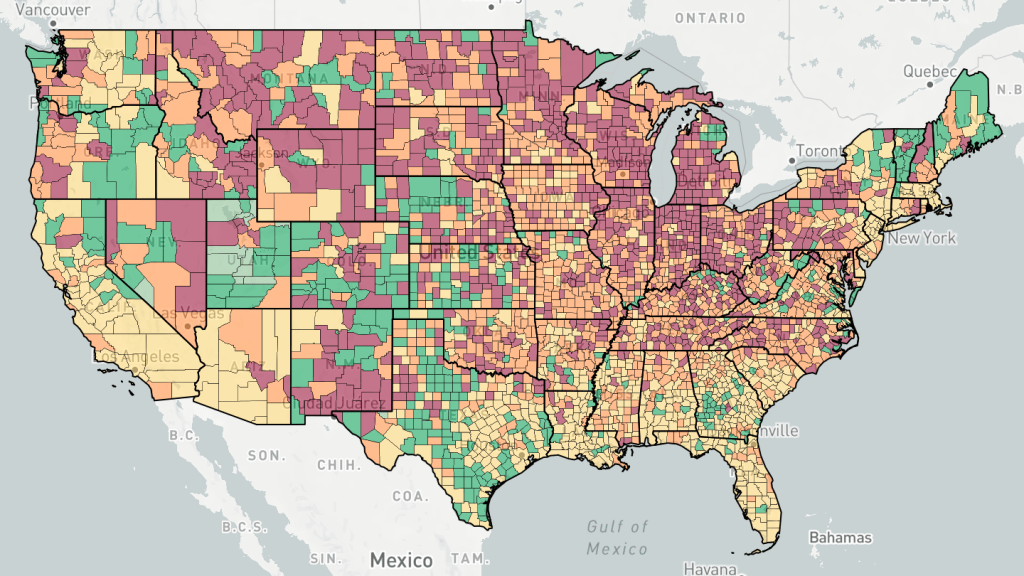
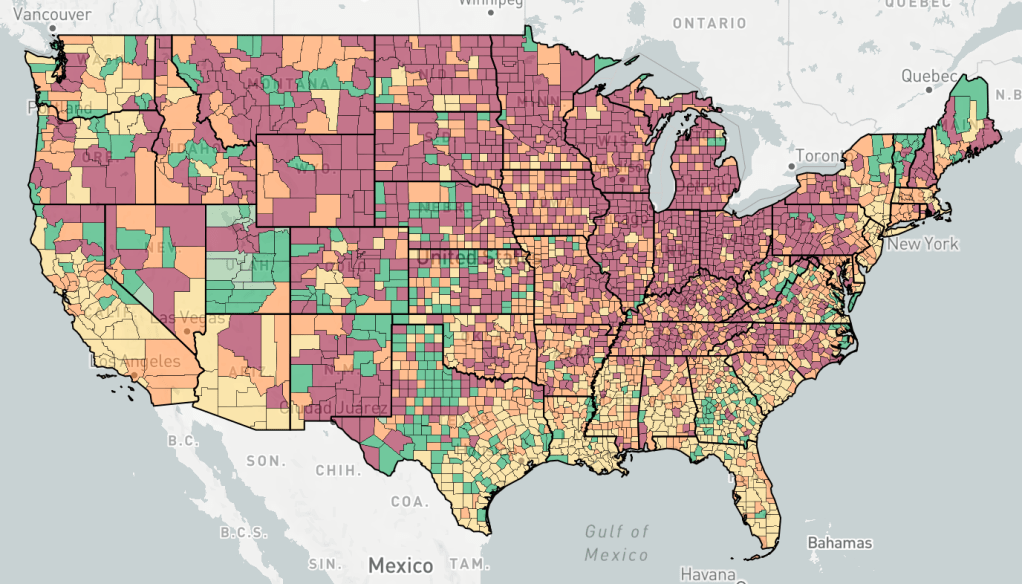
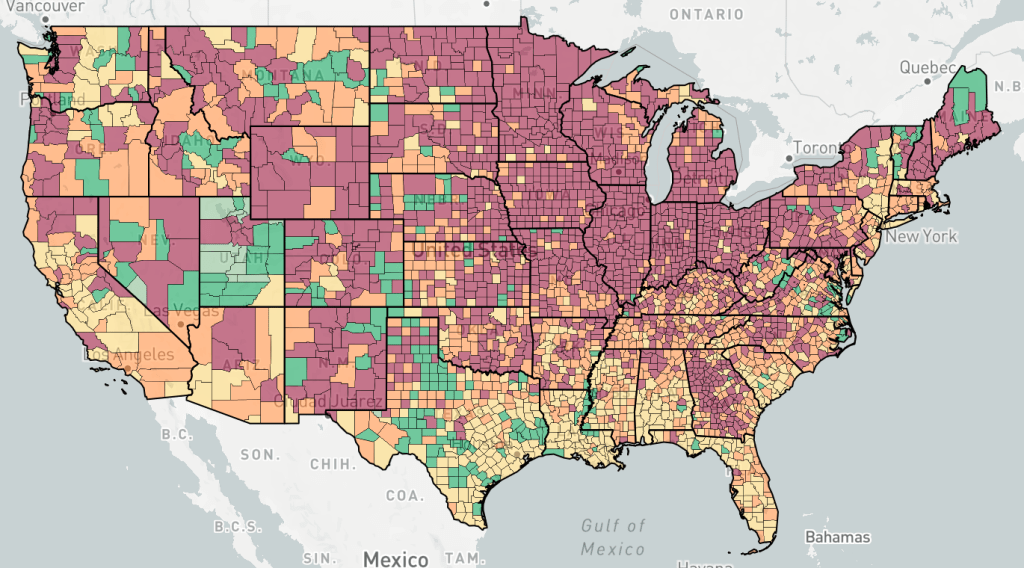
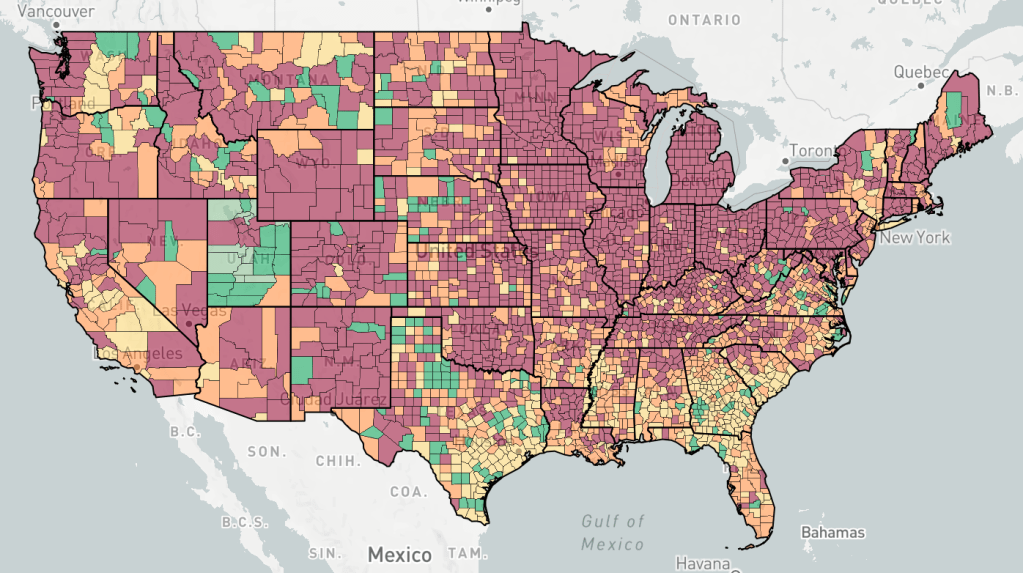
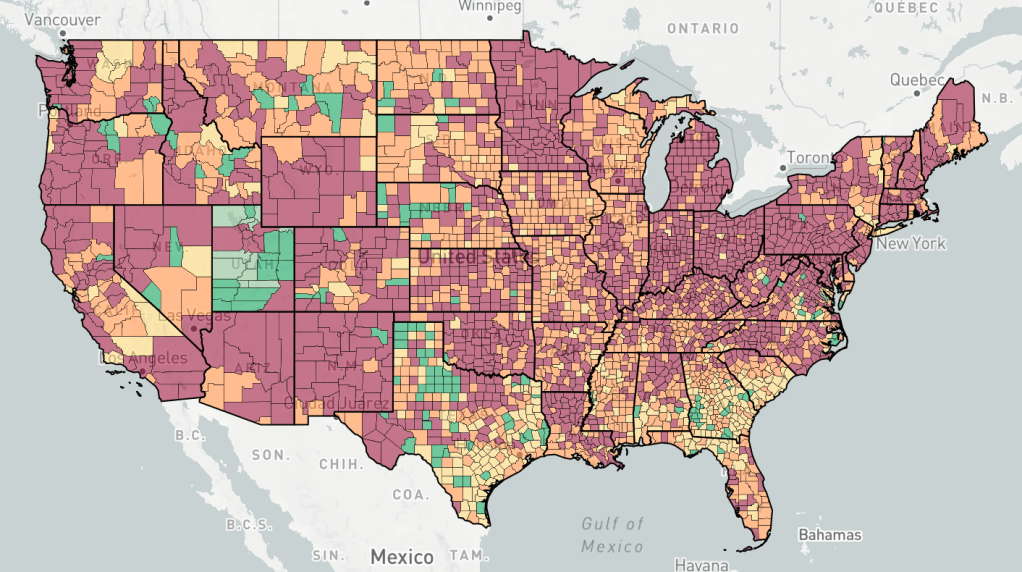
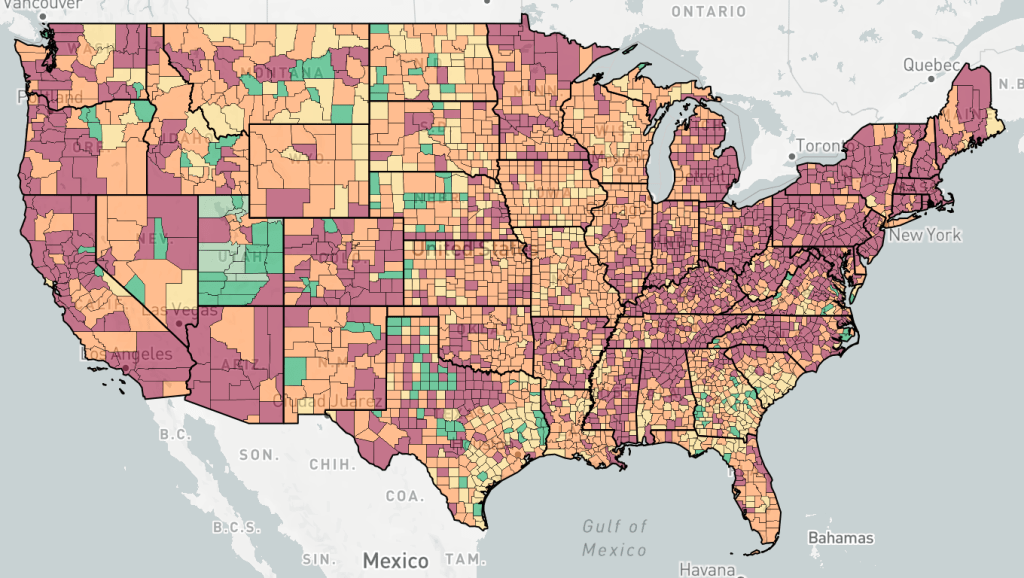
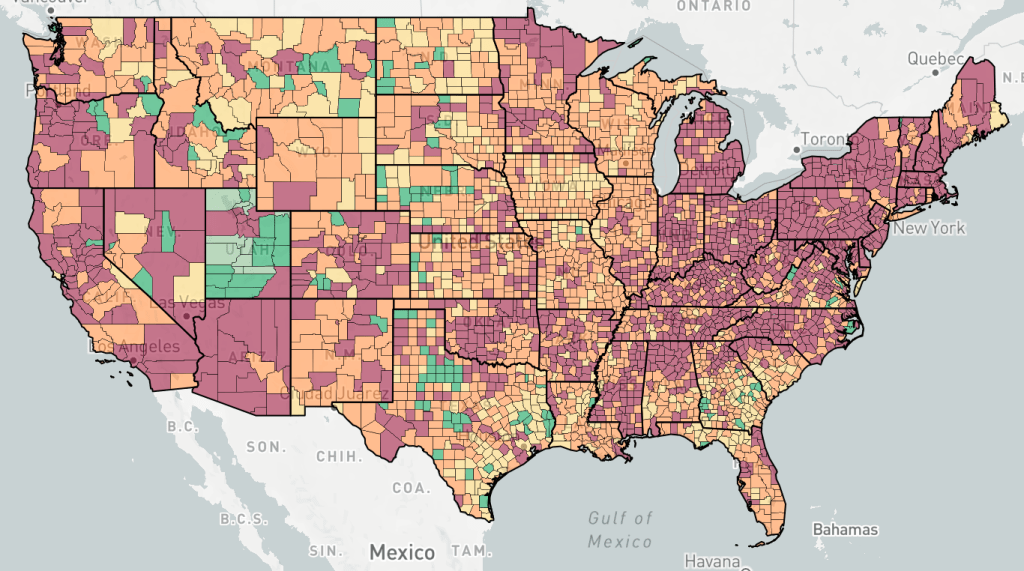
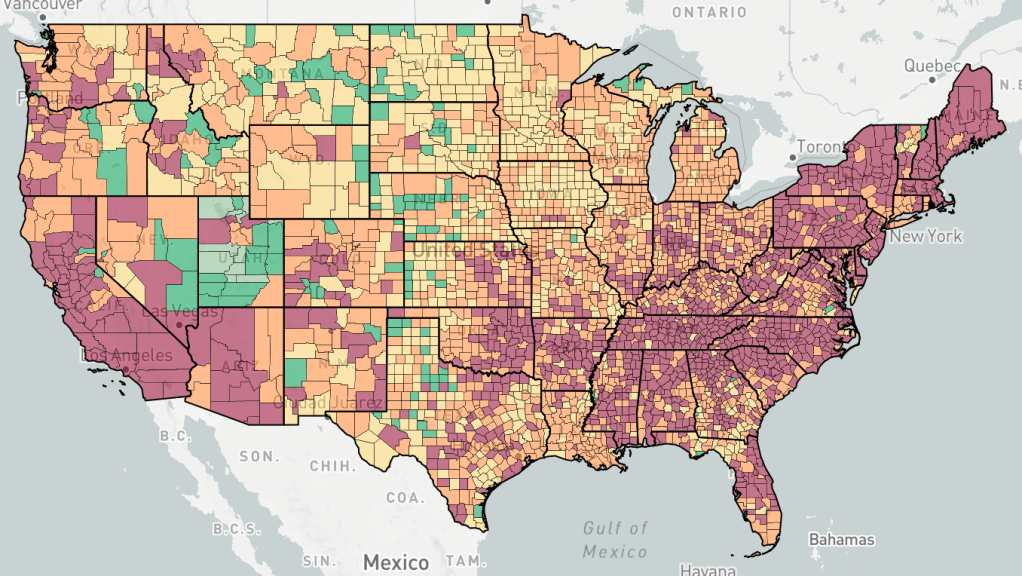
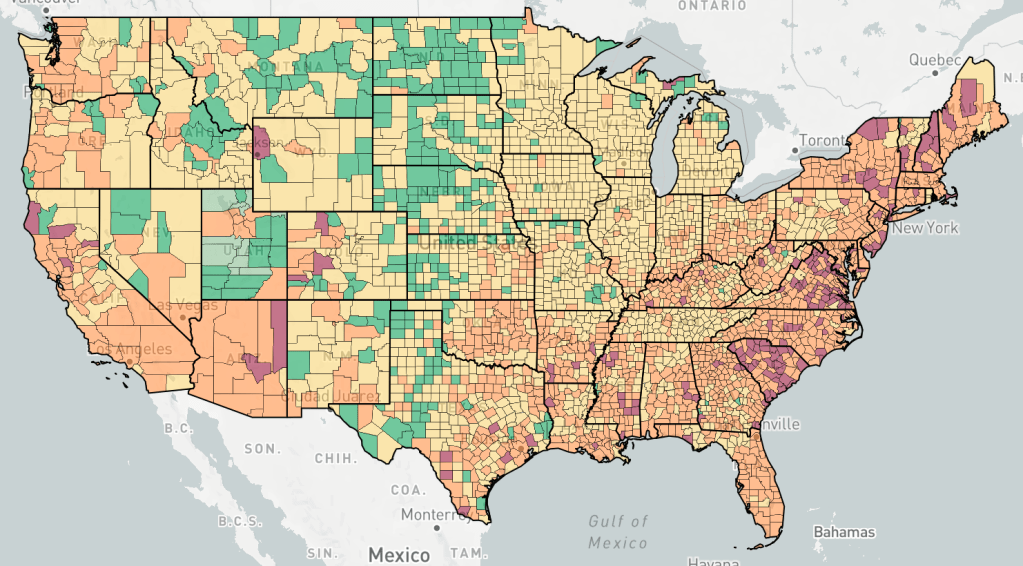
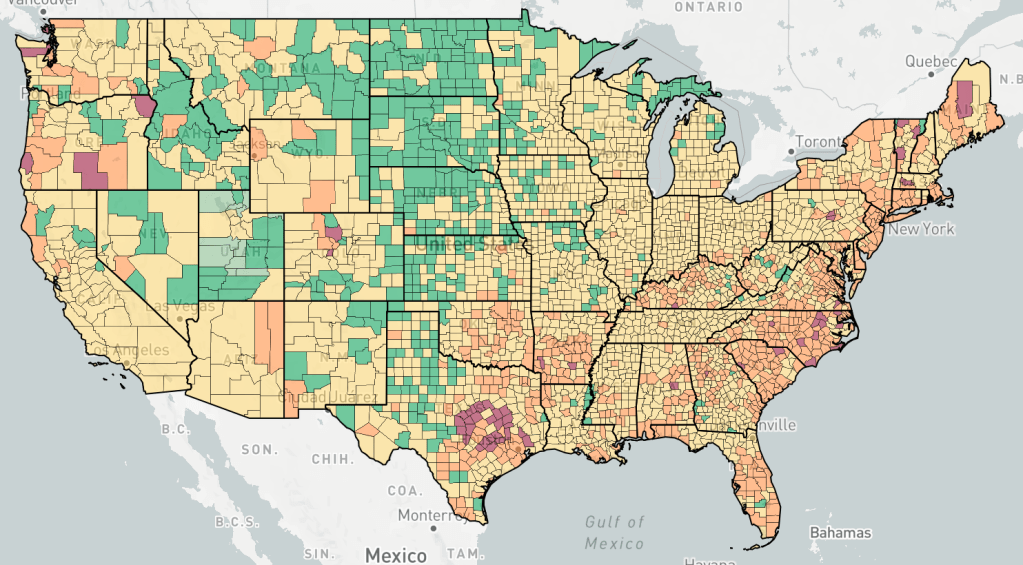
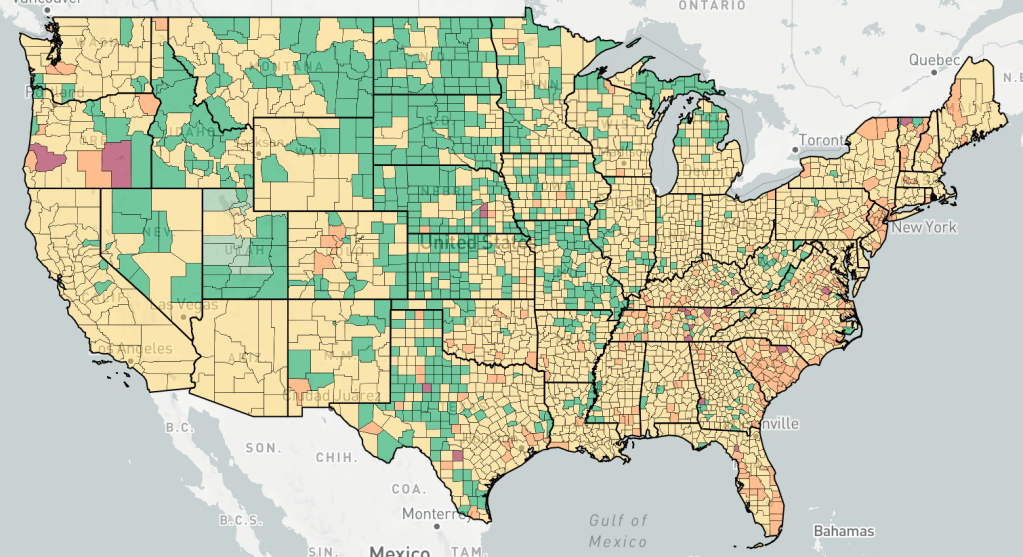
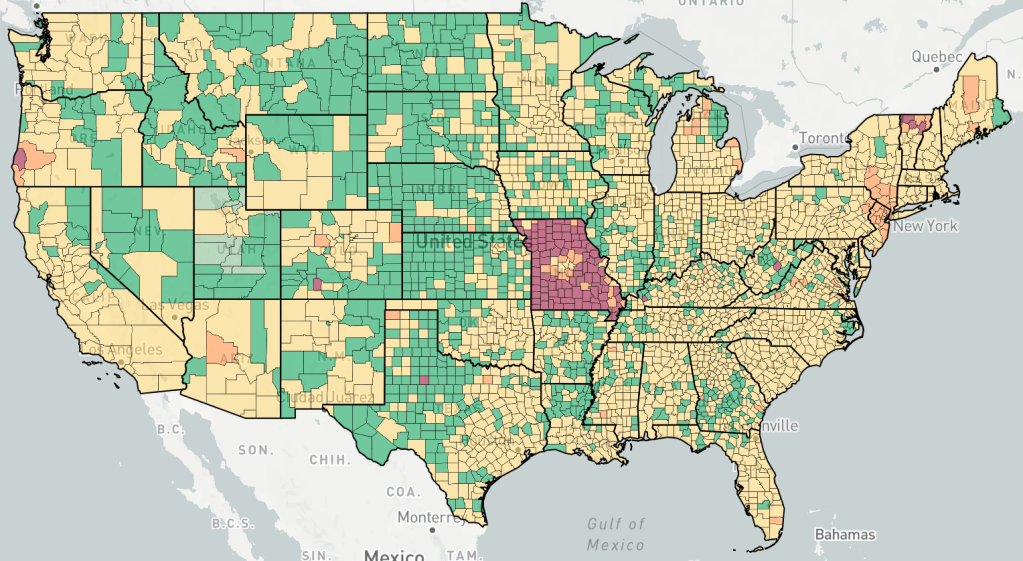
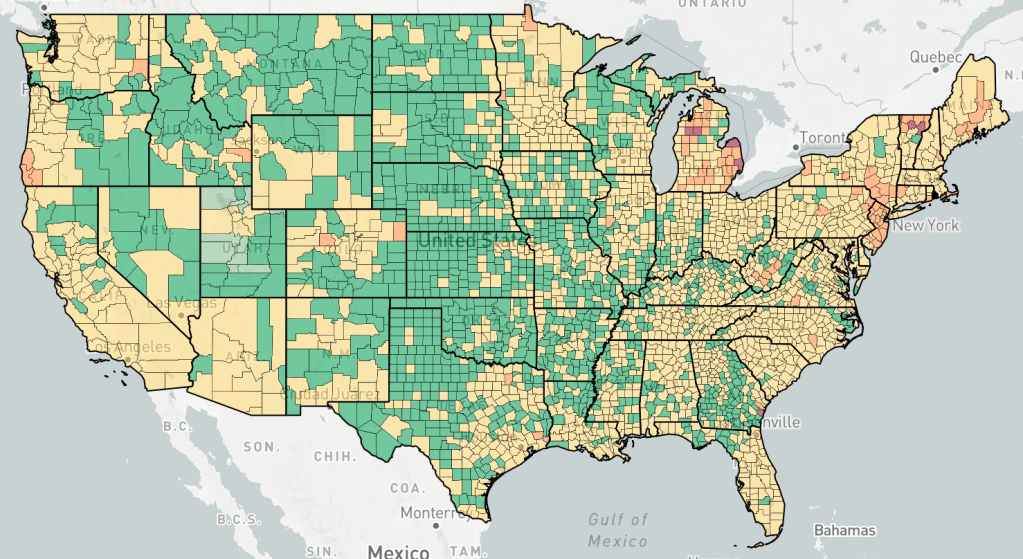
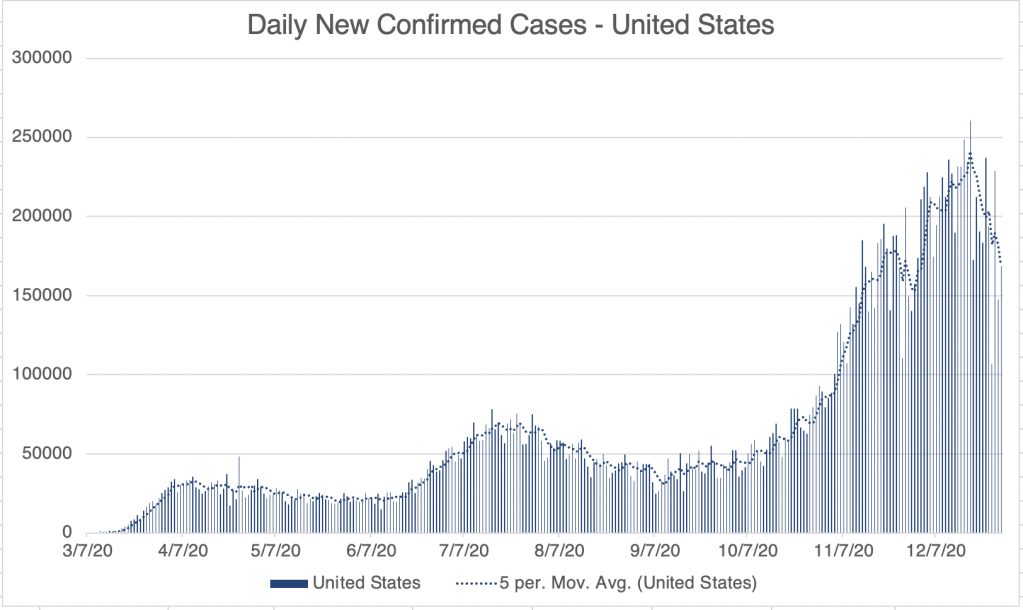
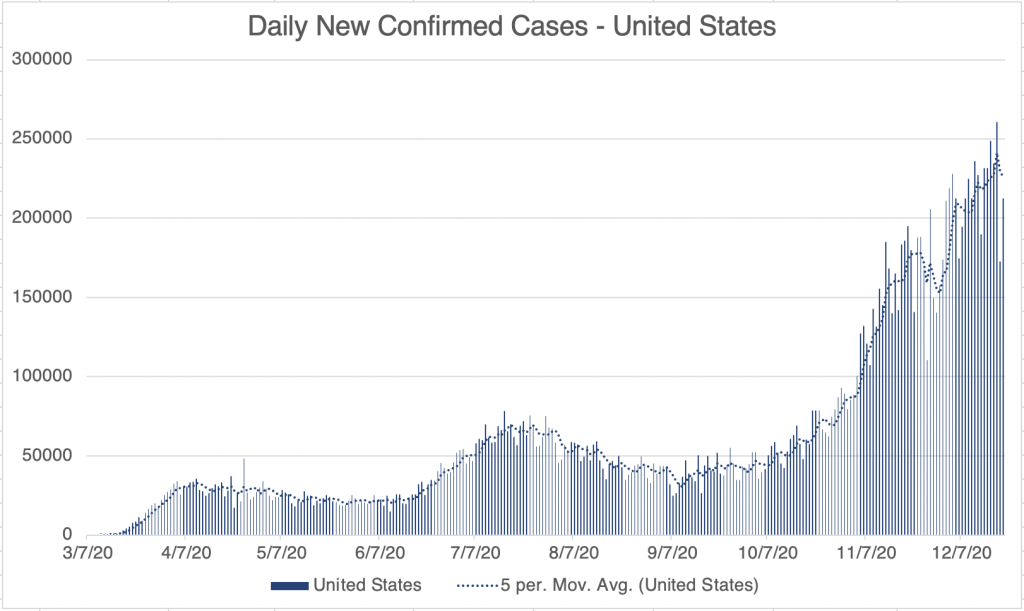
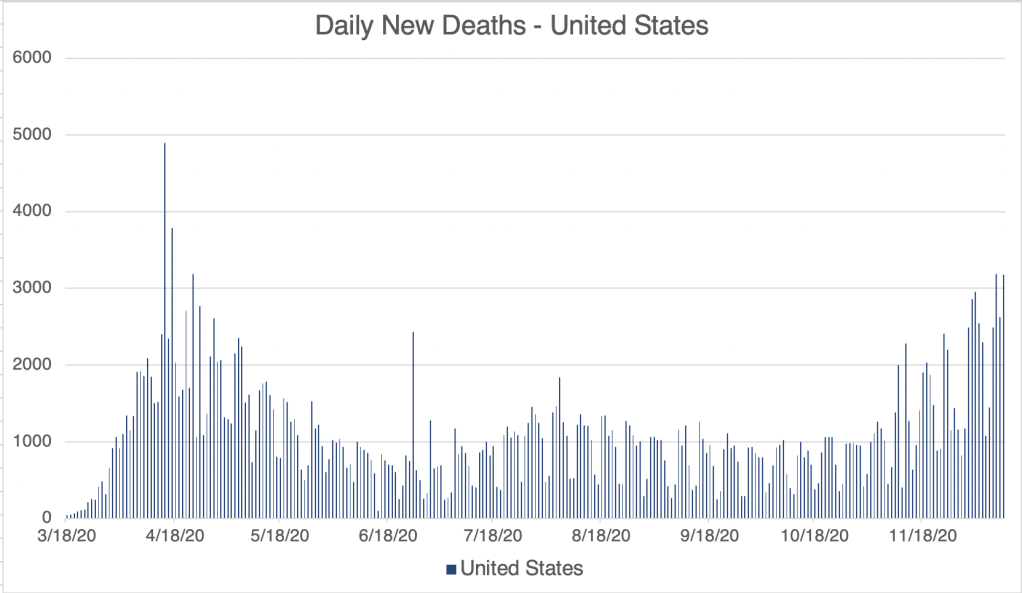
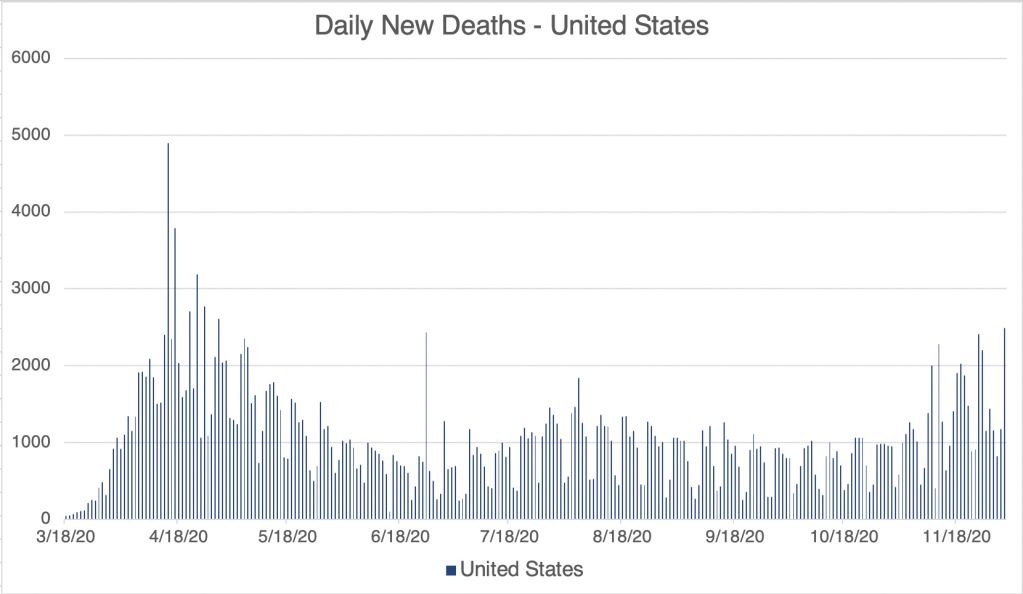
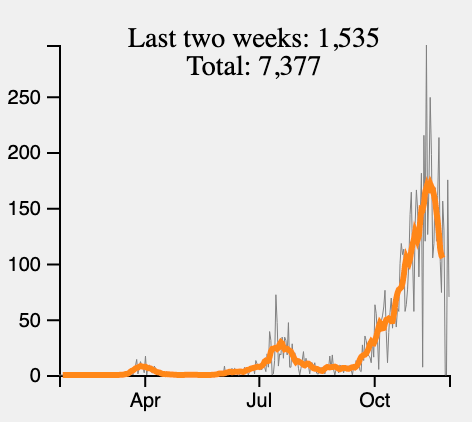
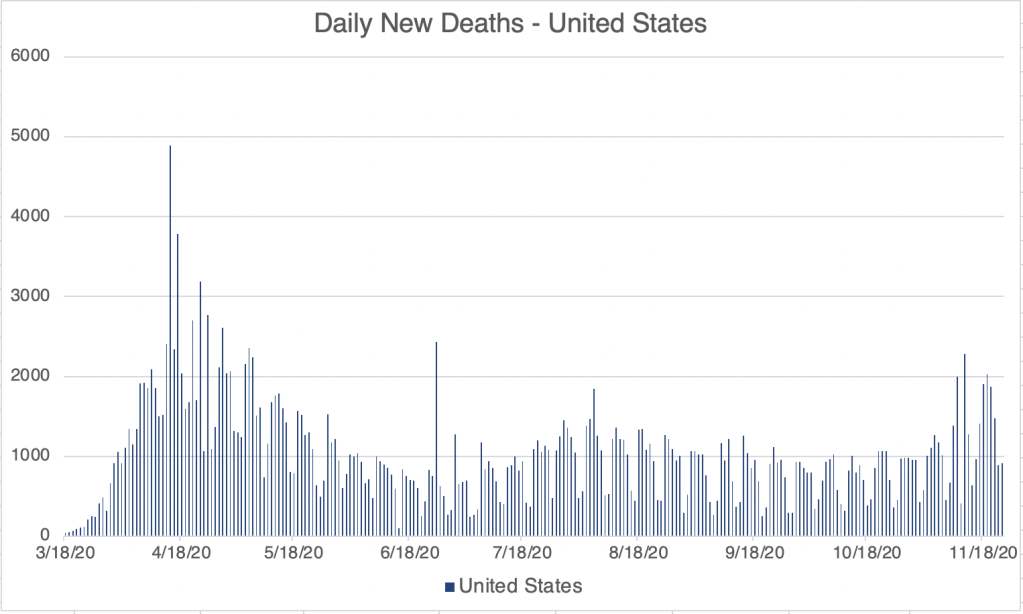
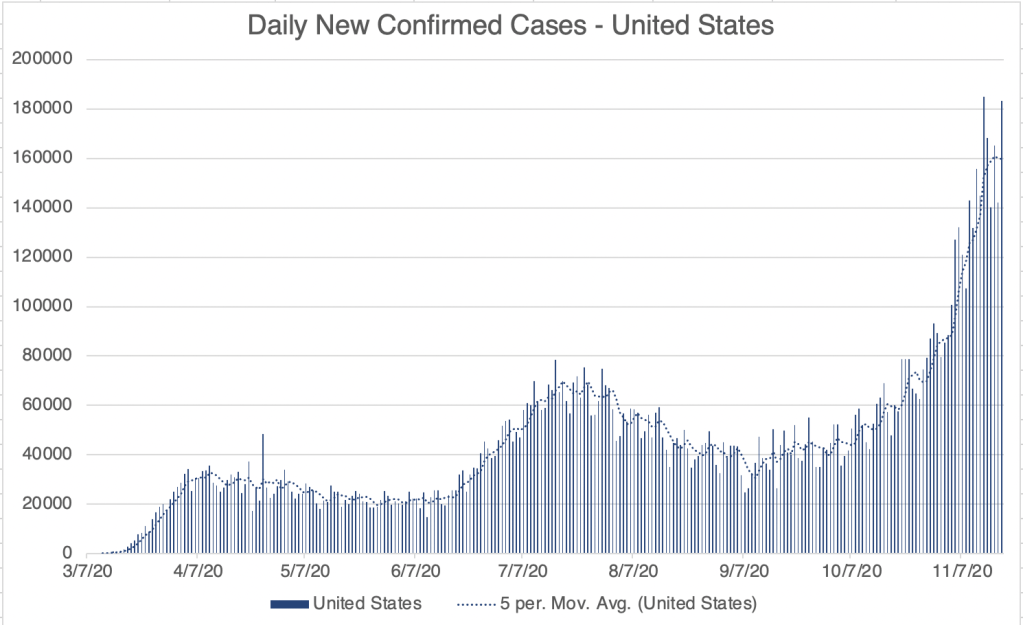
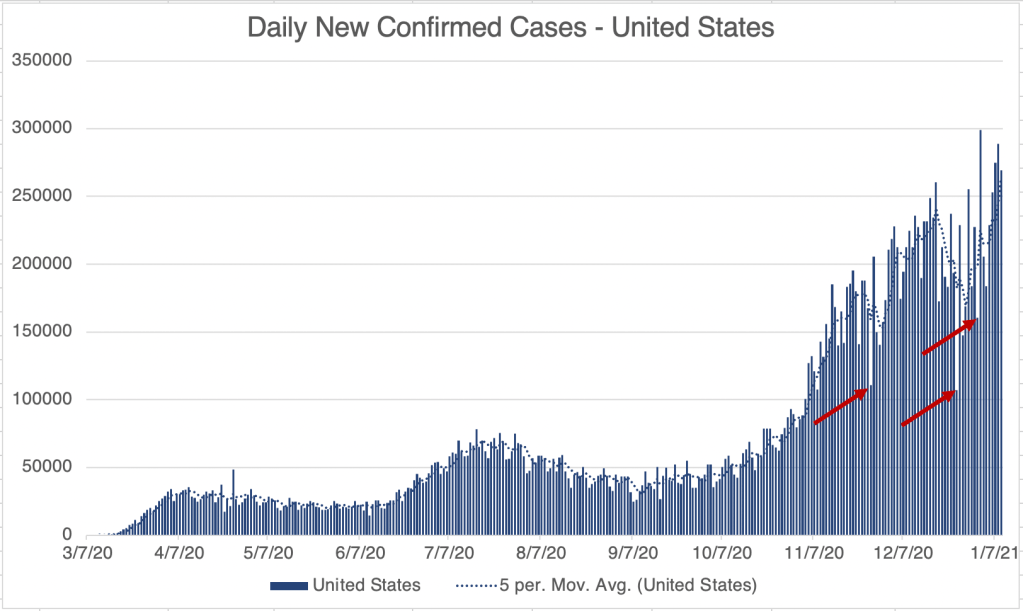
This is a case update. I’ll also briefly discuss some more new variants, and a testing equipment shortage. For the US, cases continue to increase. Day to day case rates have been very erratic for the past several weeks. This is partially because many testing facilities don’t report on holidays, so that there is an artificially low case number on holidays, and an artificially high case number the day after. The arrows in the case number graph for the US show Thanksgiving, Christmas, and New Years Day. Wave 3c, the wave starting after Christmas day, is still increasing in confirmed case numbers.

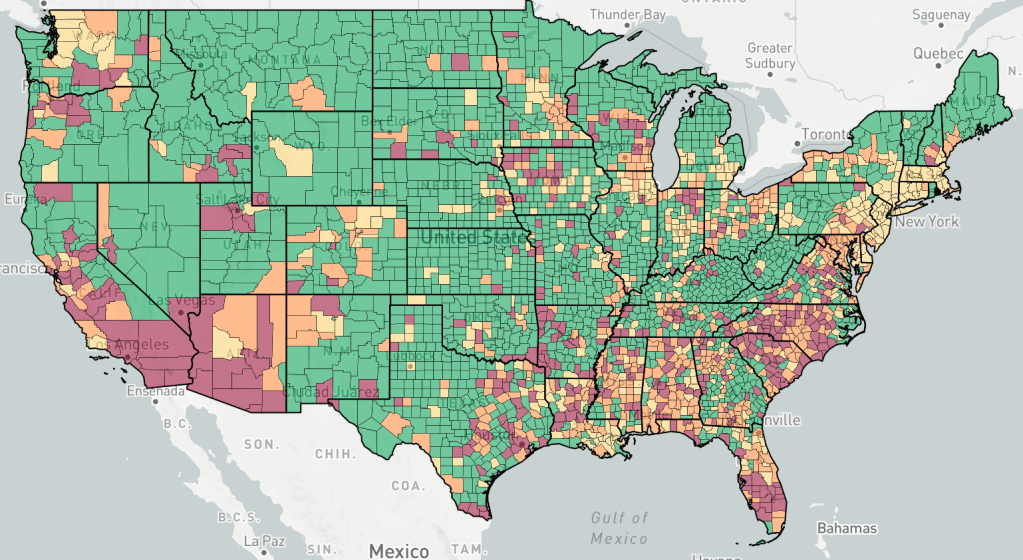
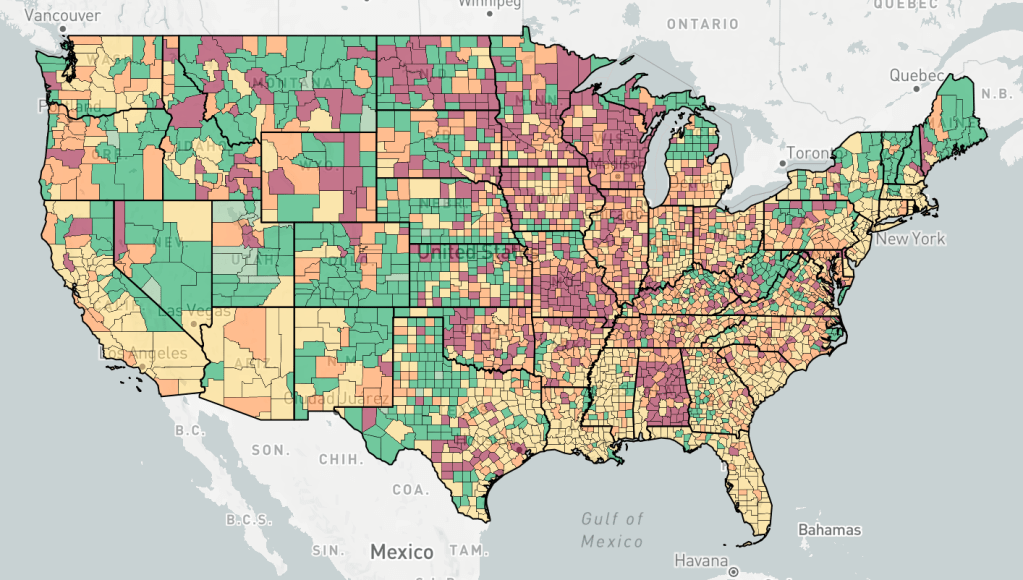
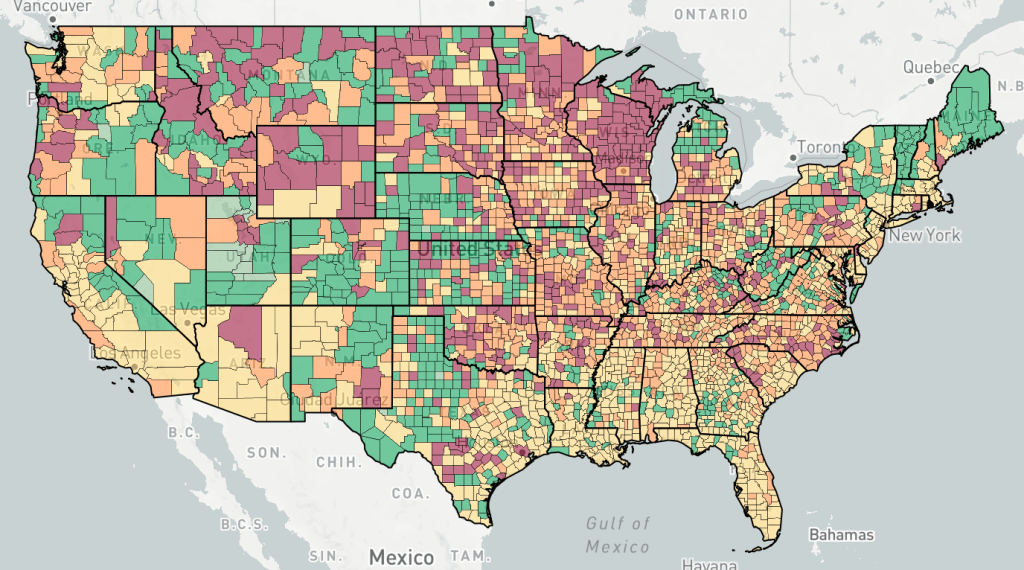
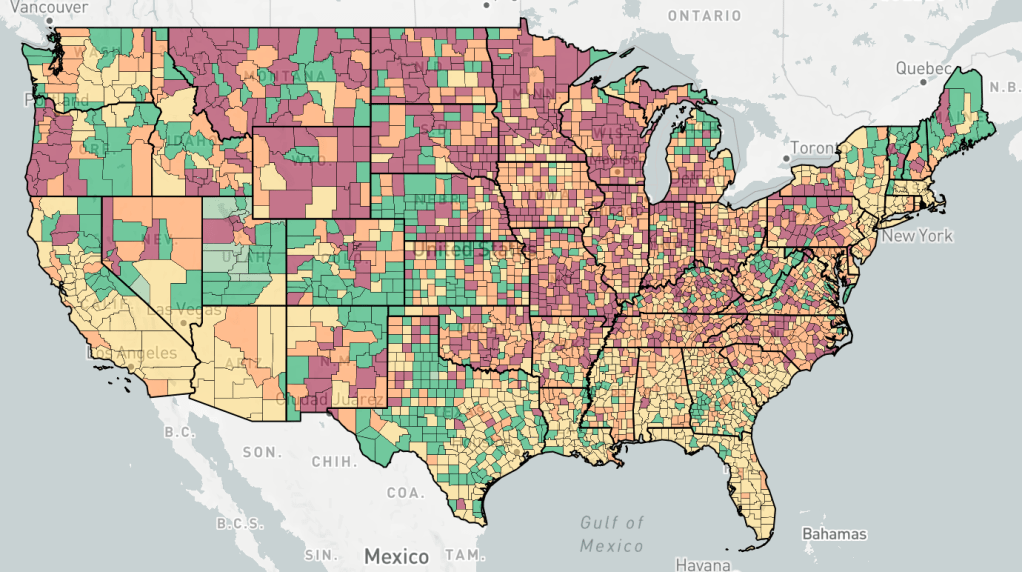
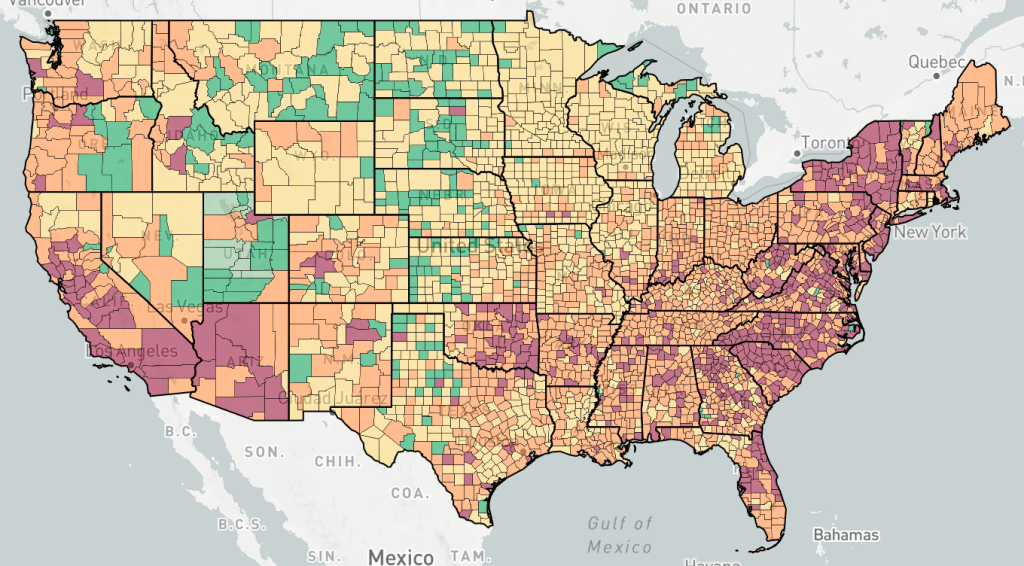
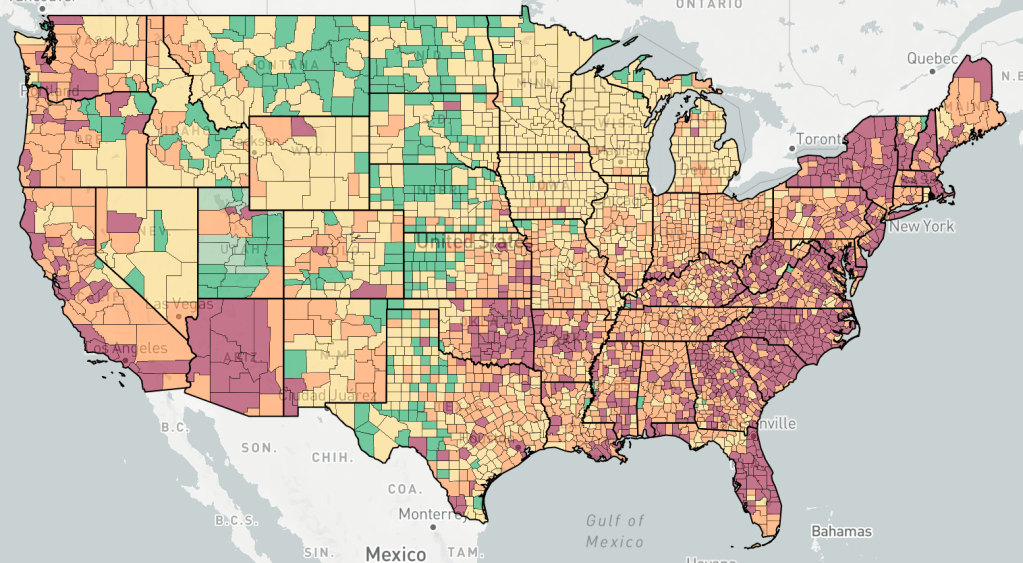
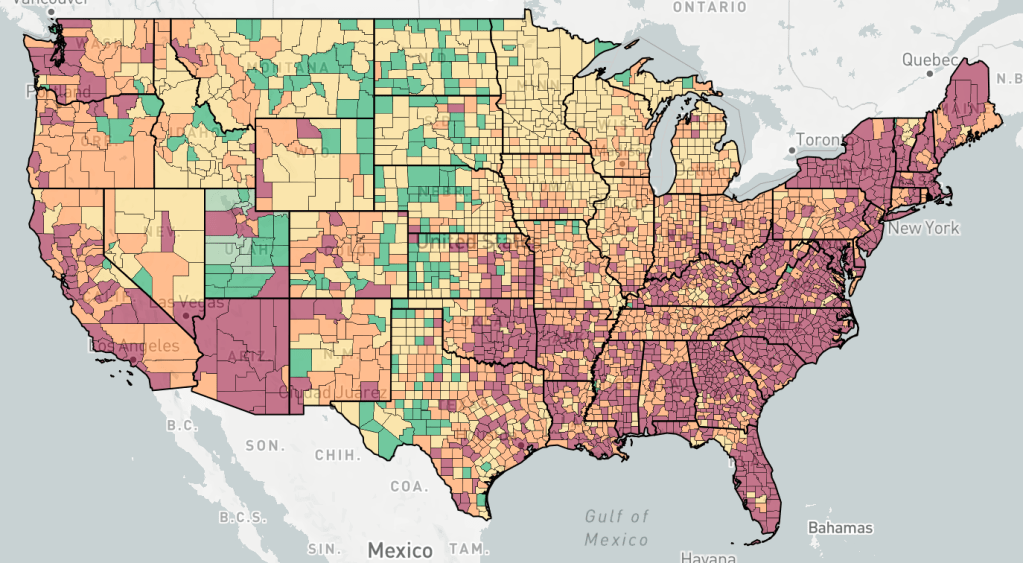
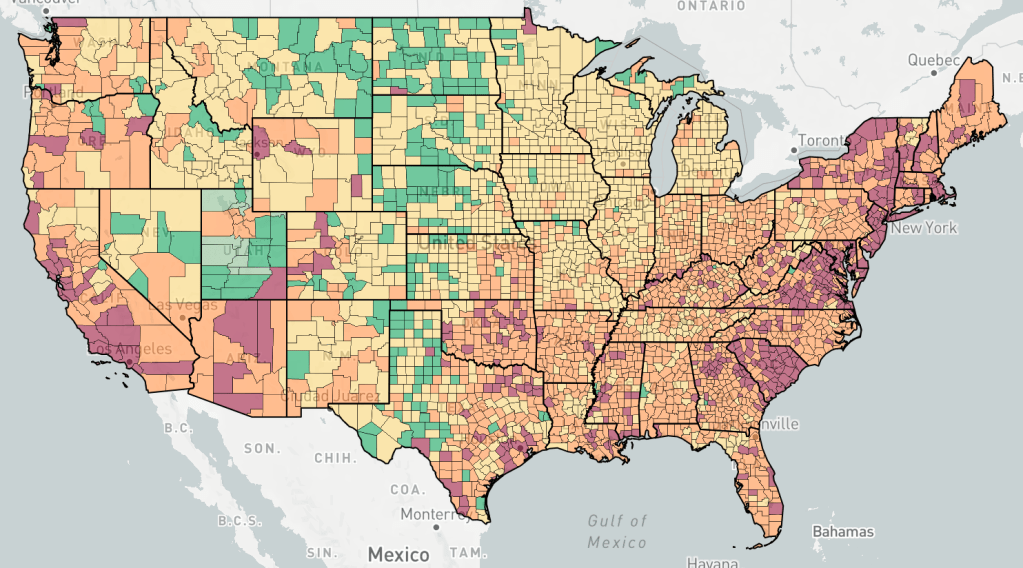
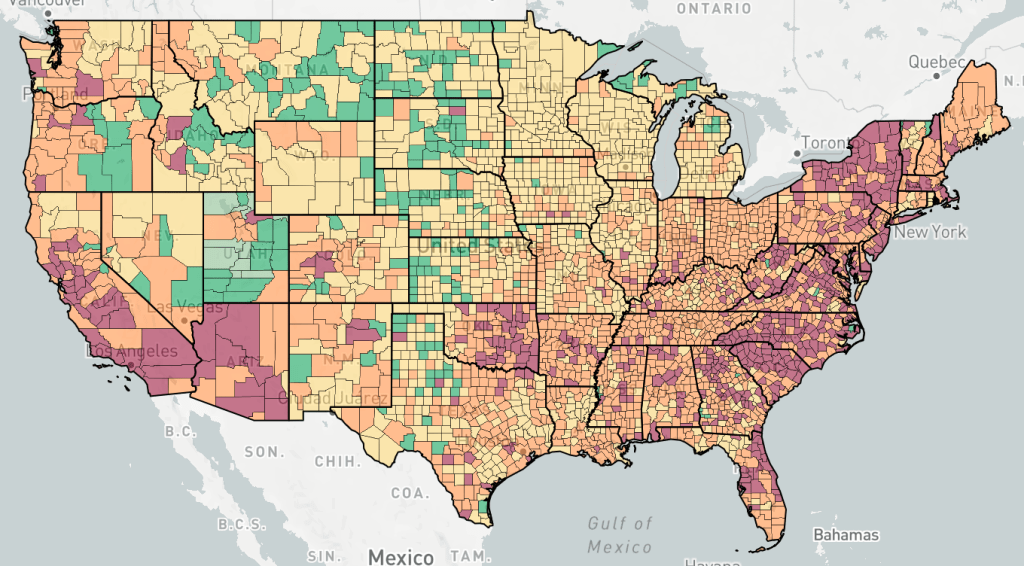
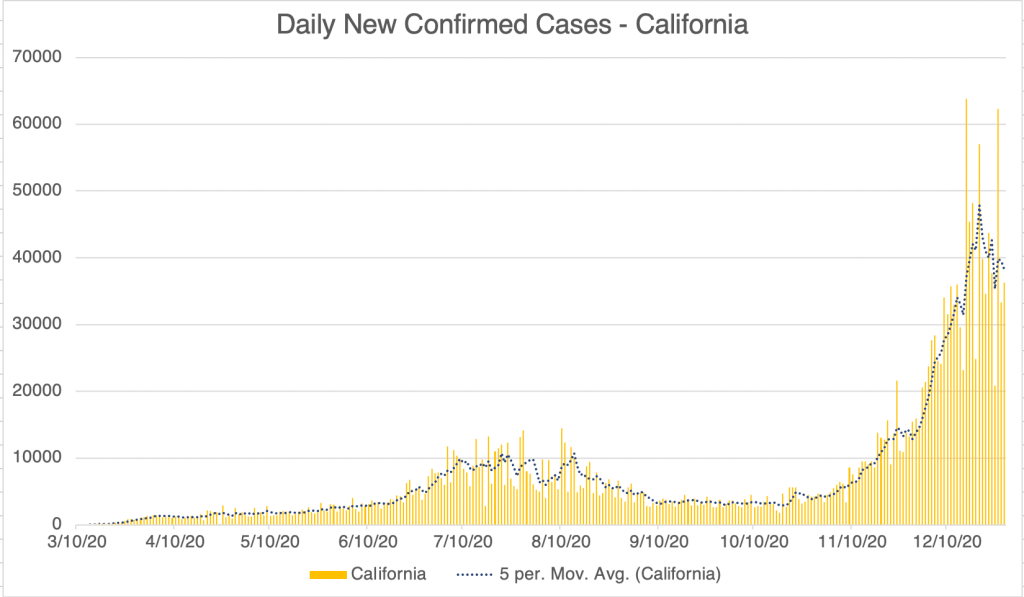
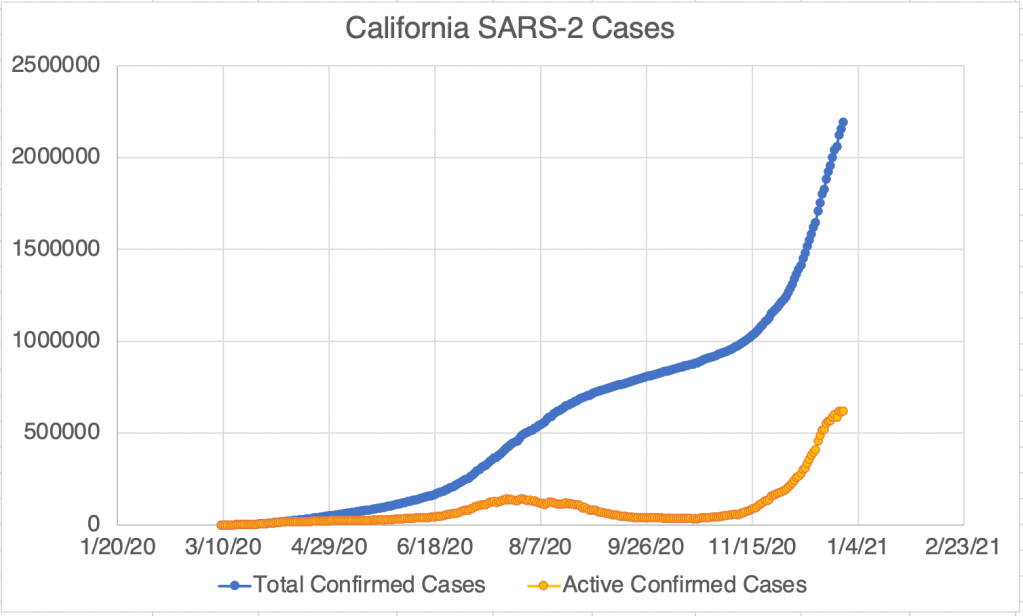
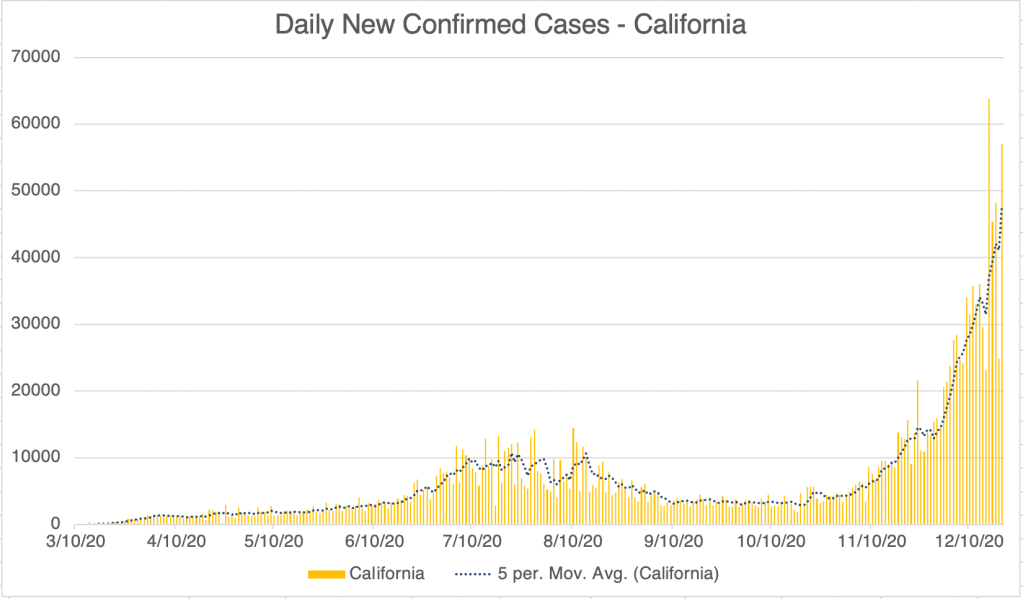
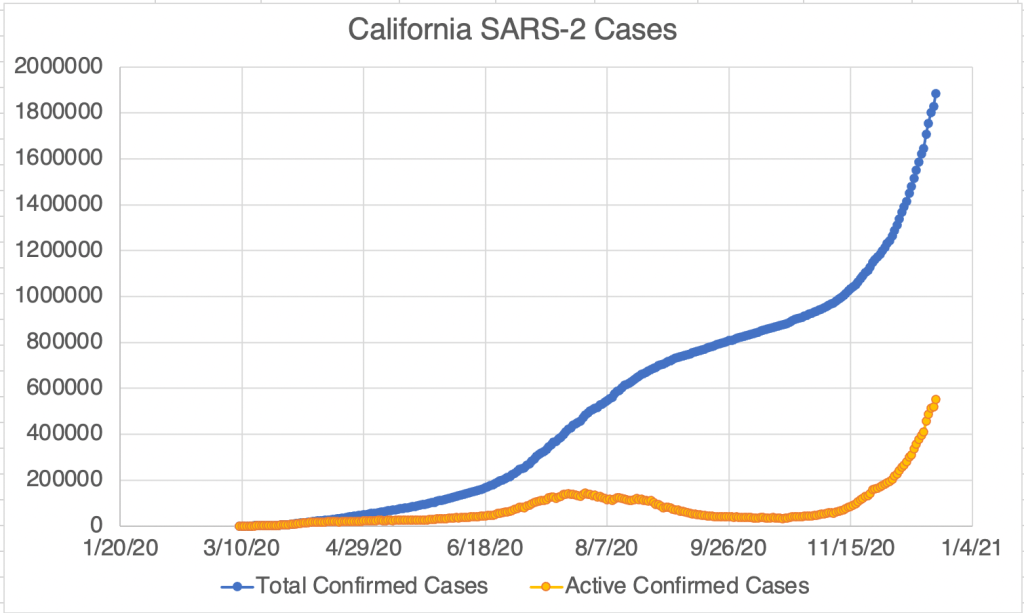
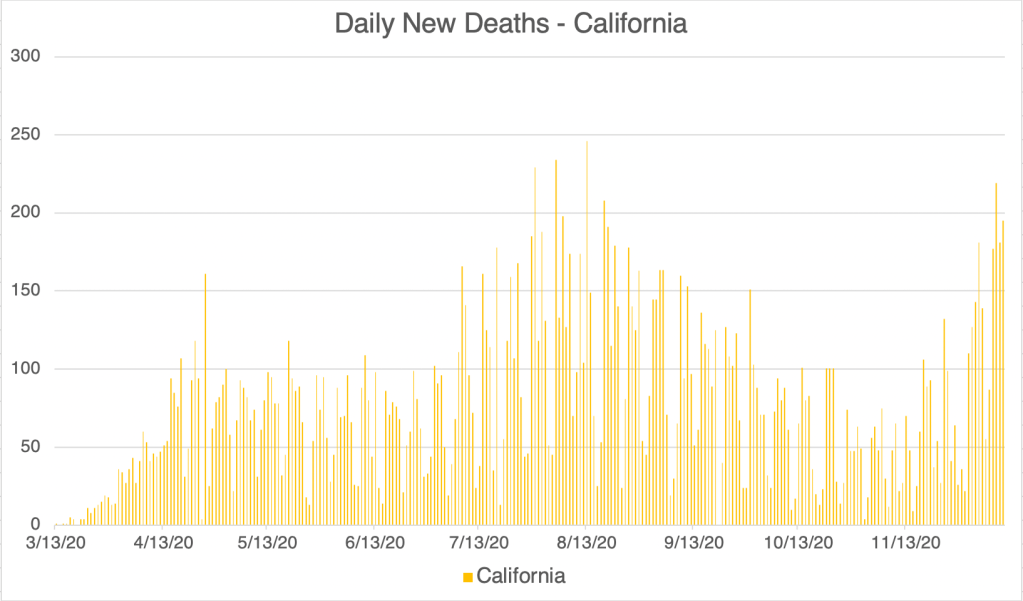
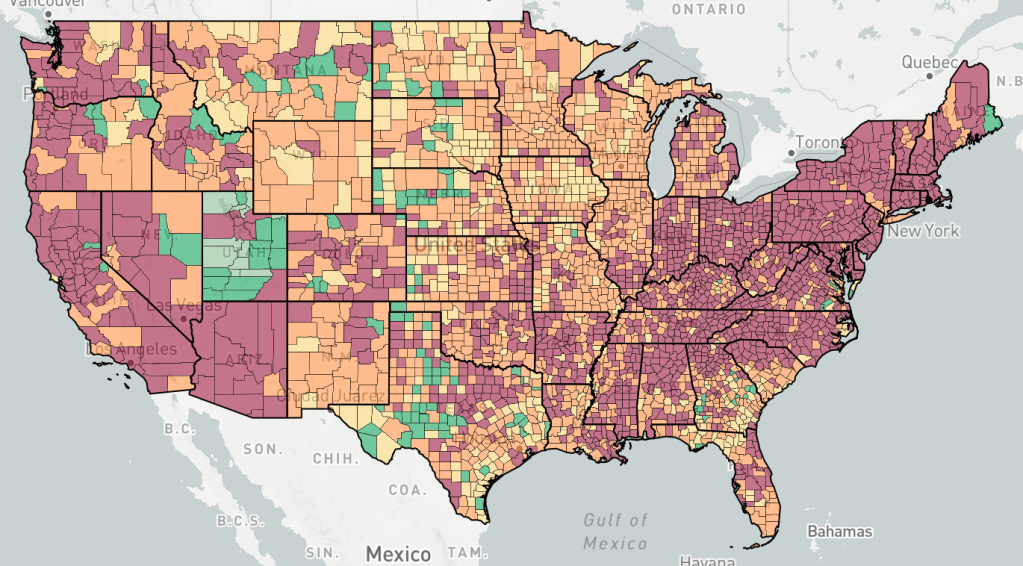
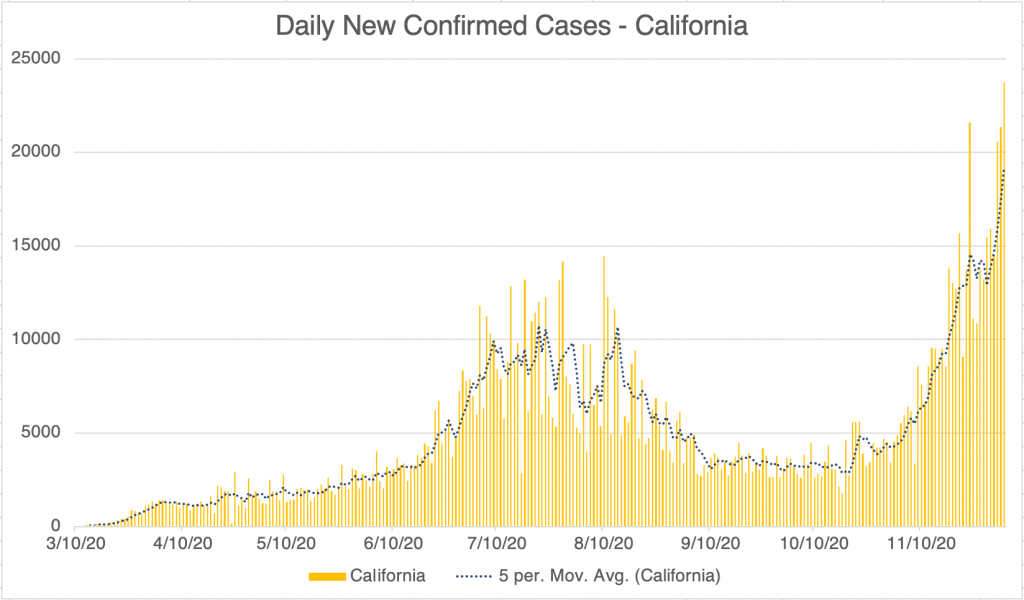
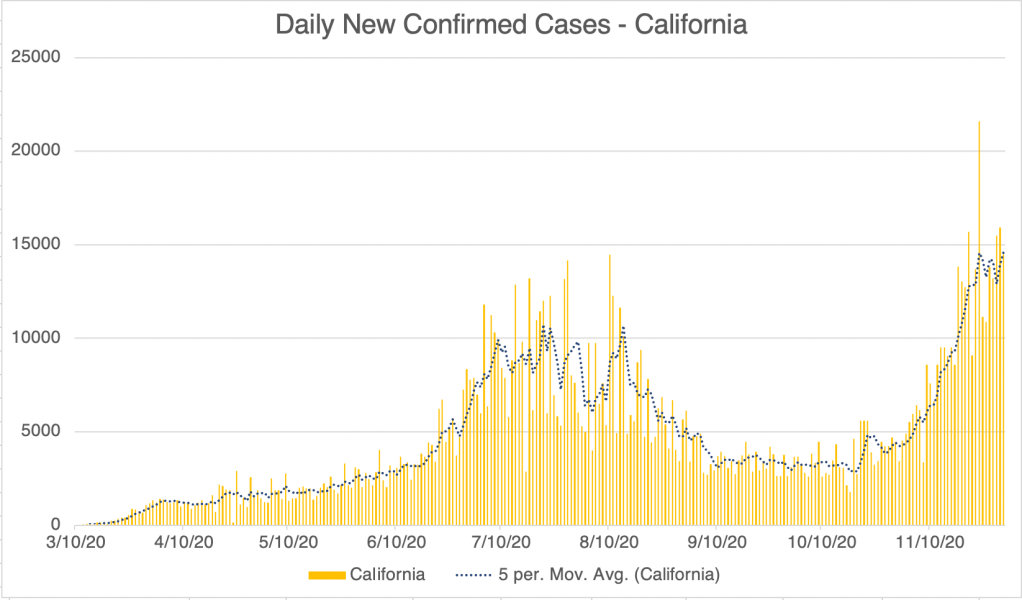
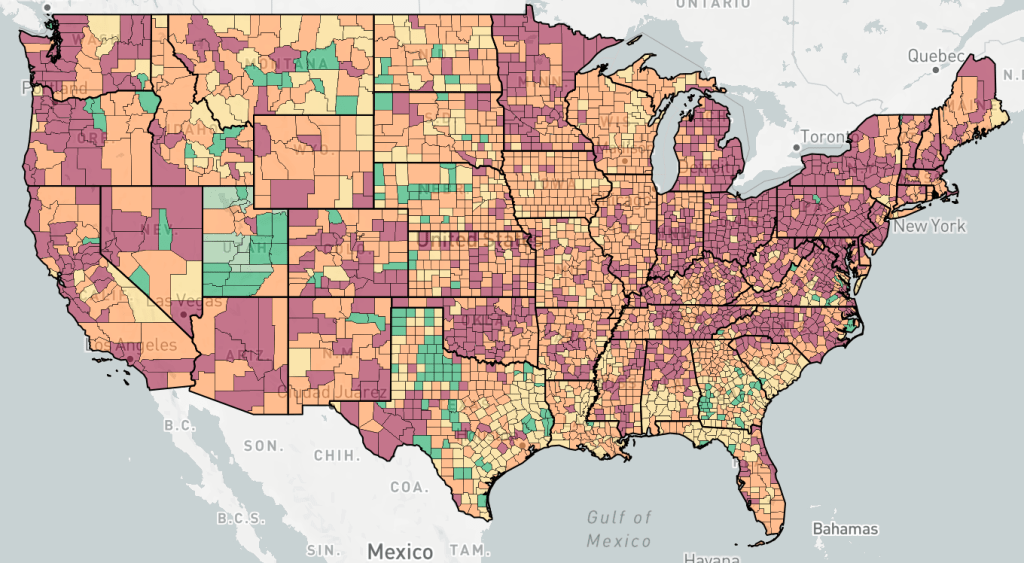
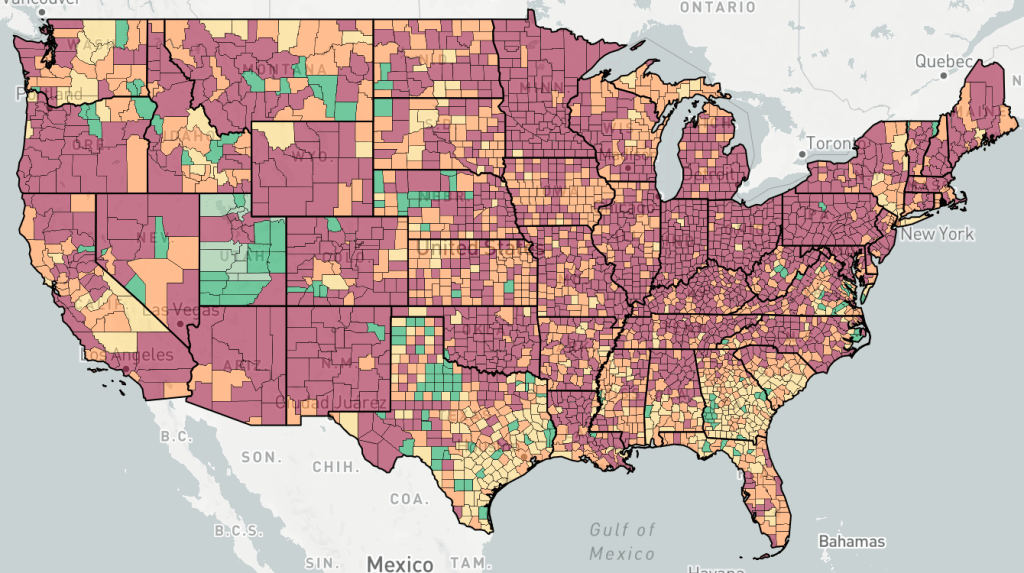
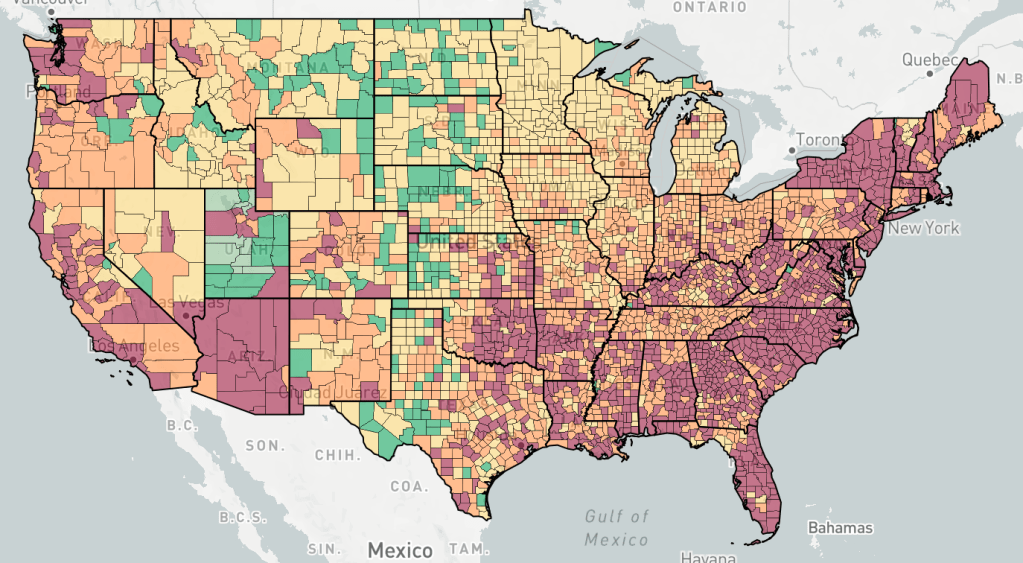
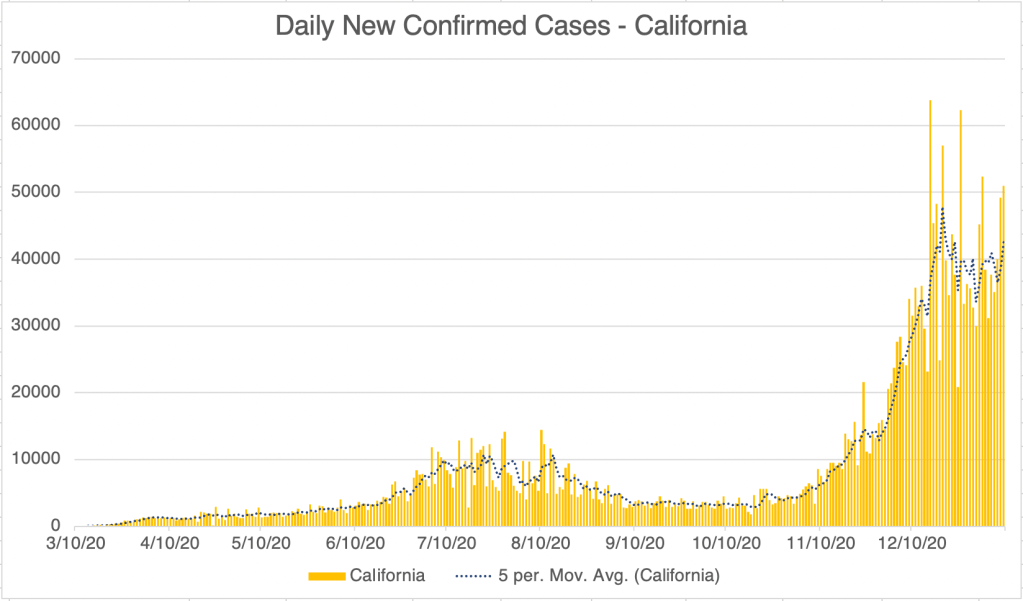
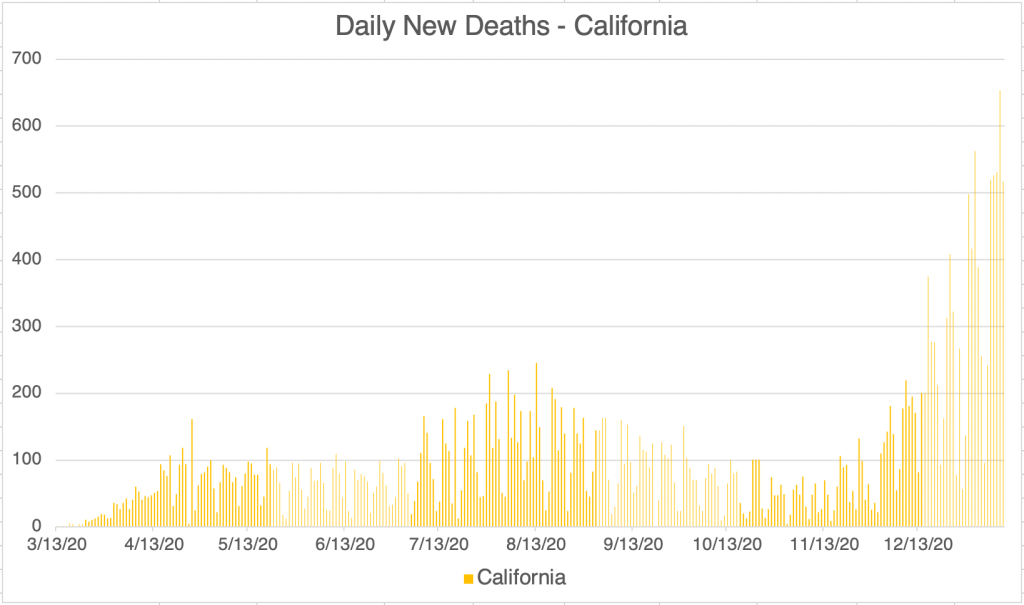
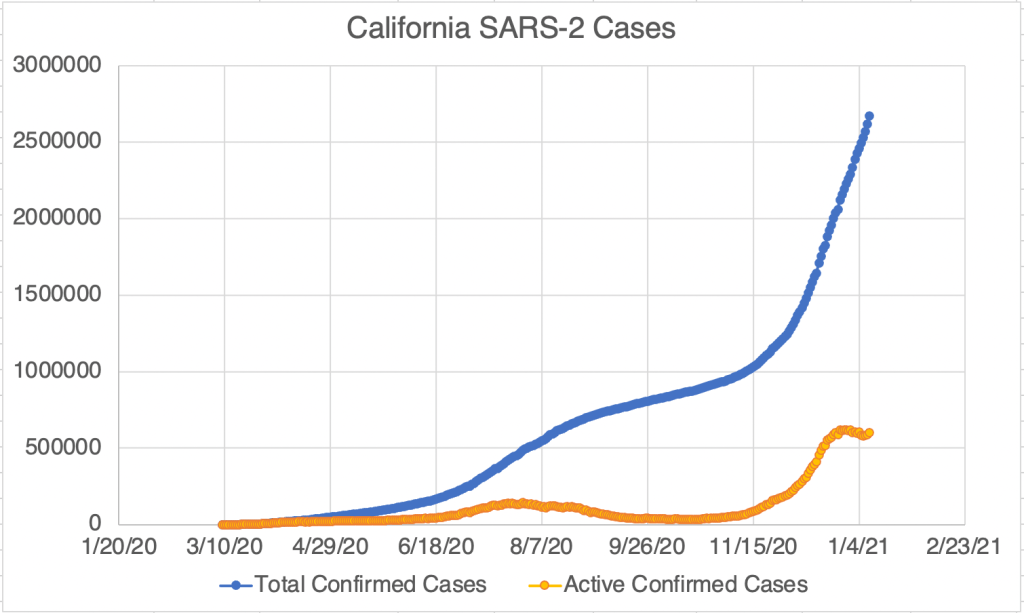
New cases continue to be focused in the East and Southwest. In particular, new case numbers have plateaued in California, but numbers are still quite high, with 4 of the top 5 counties being in California.
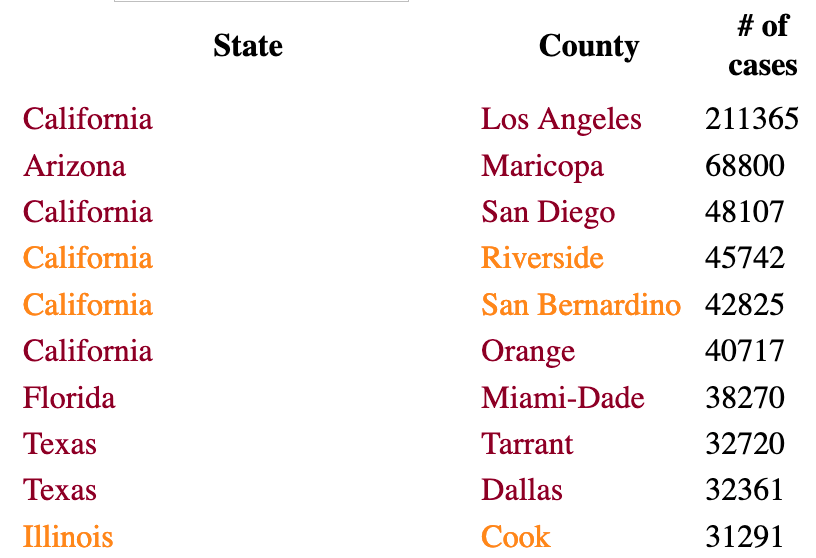
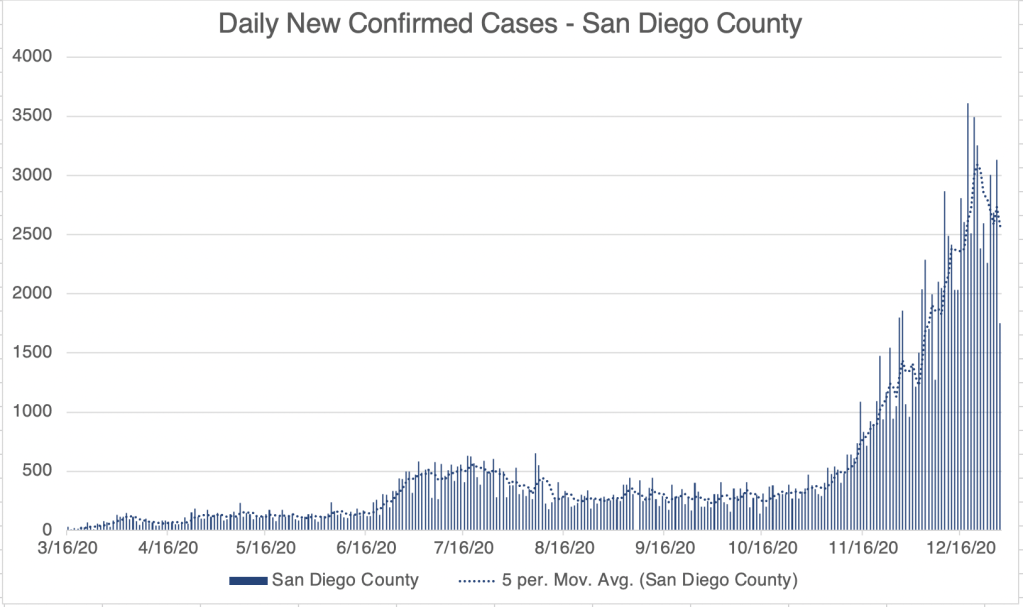
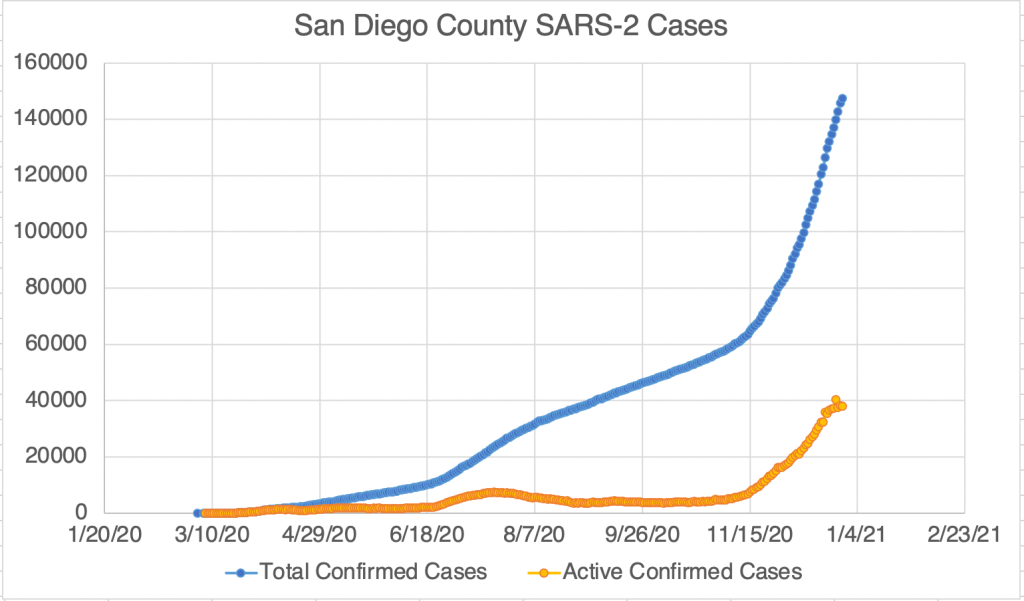
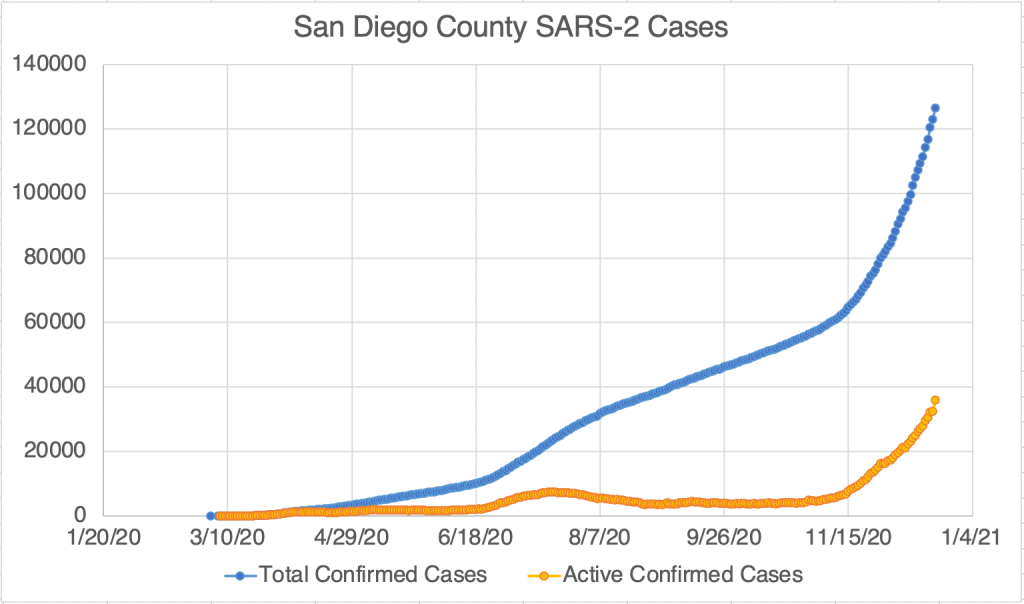
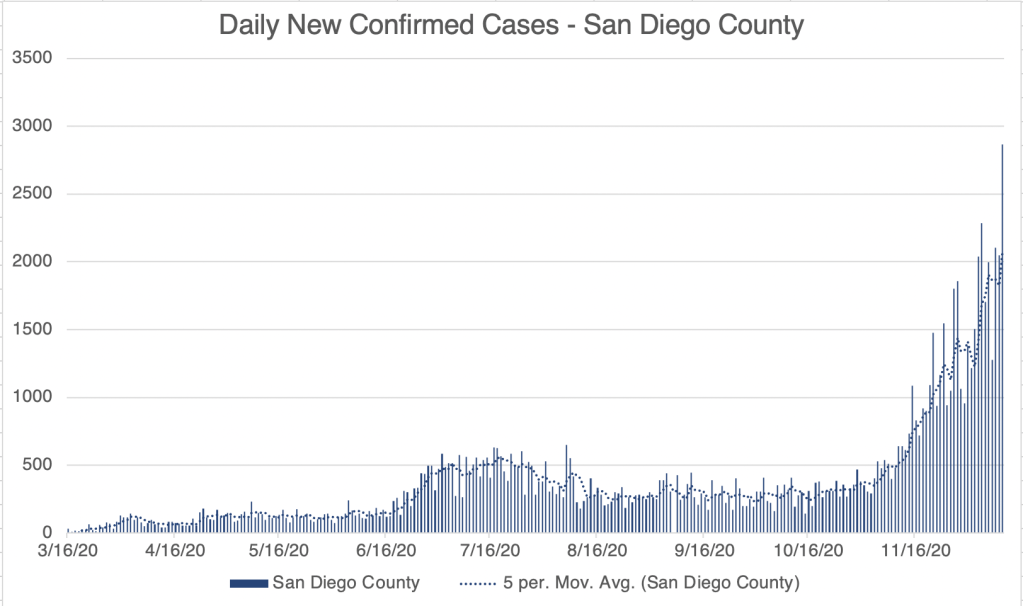
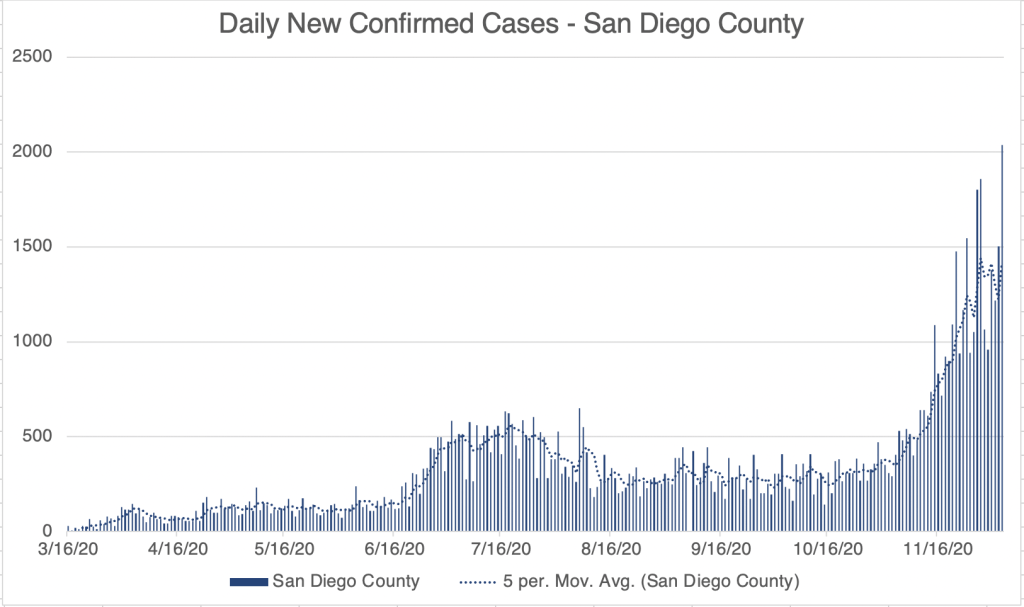
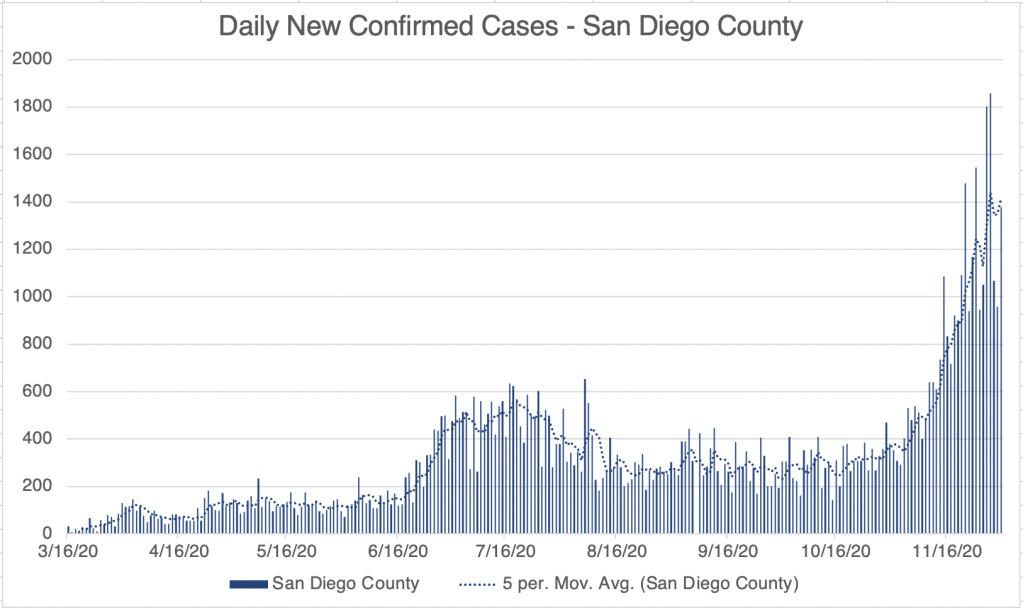
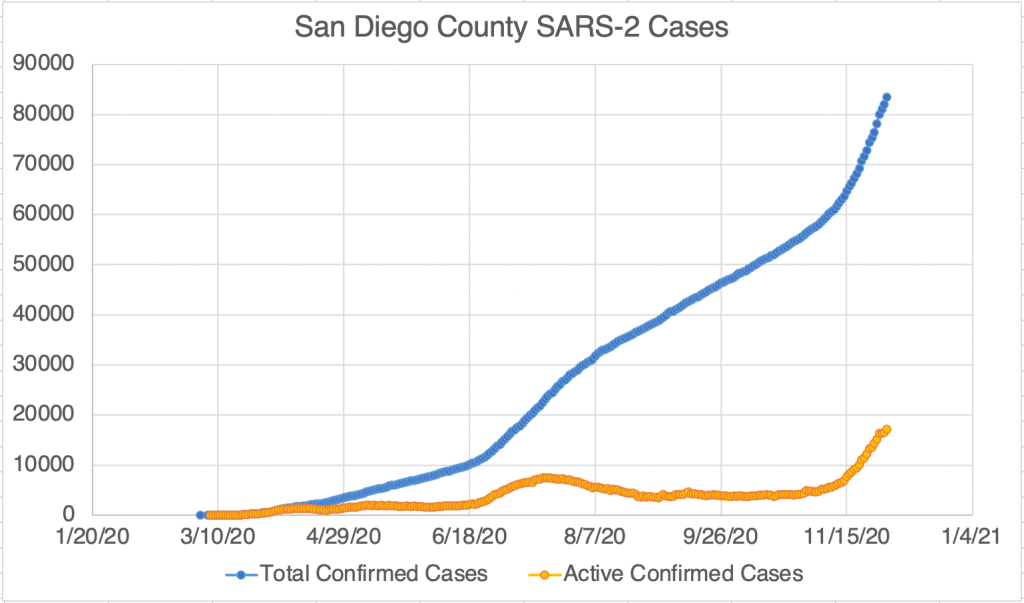
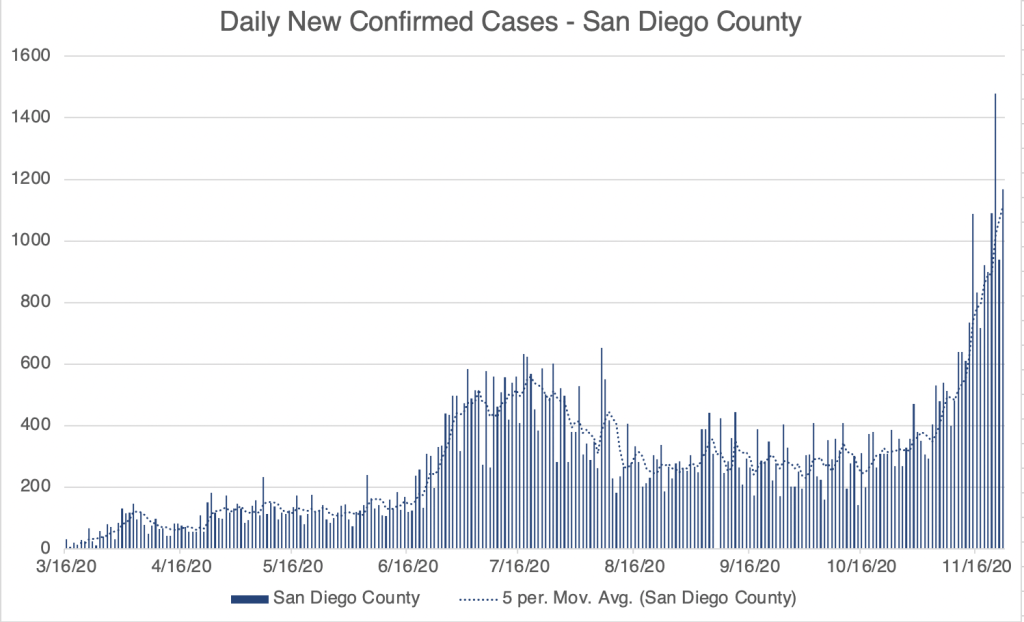
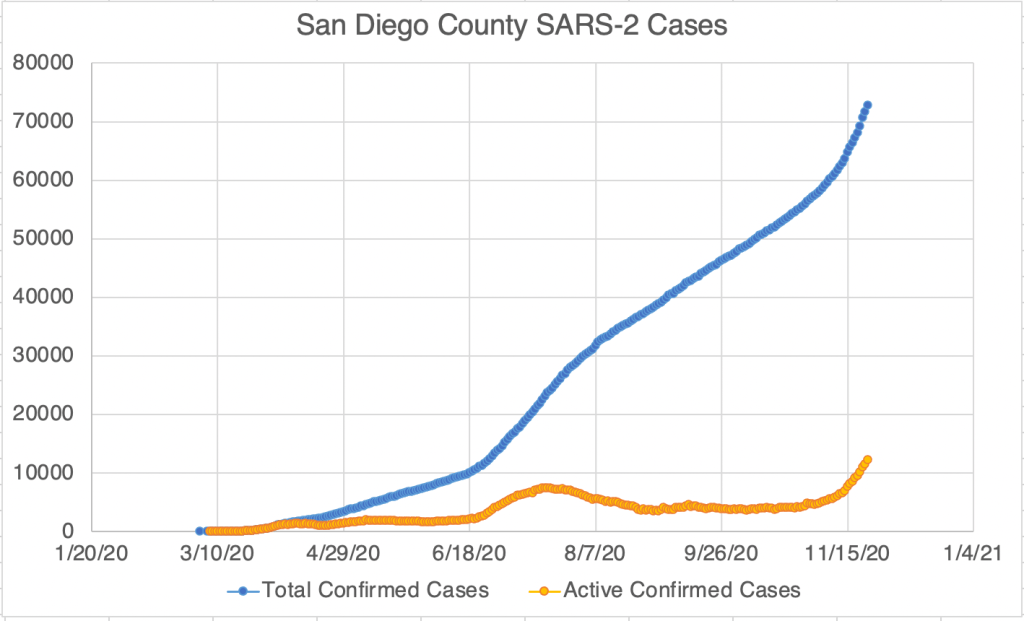
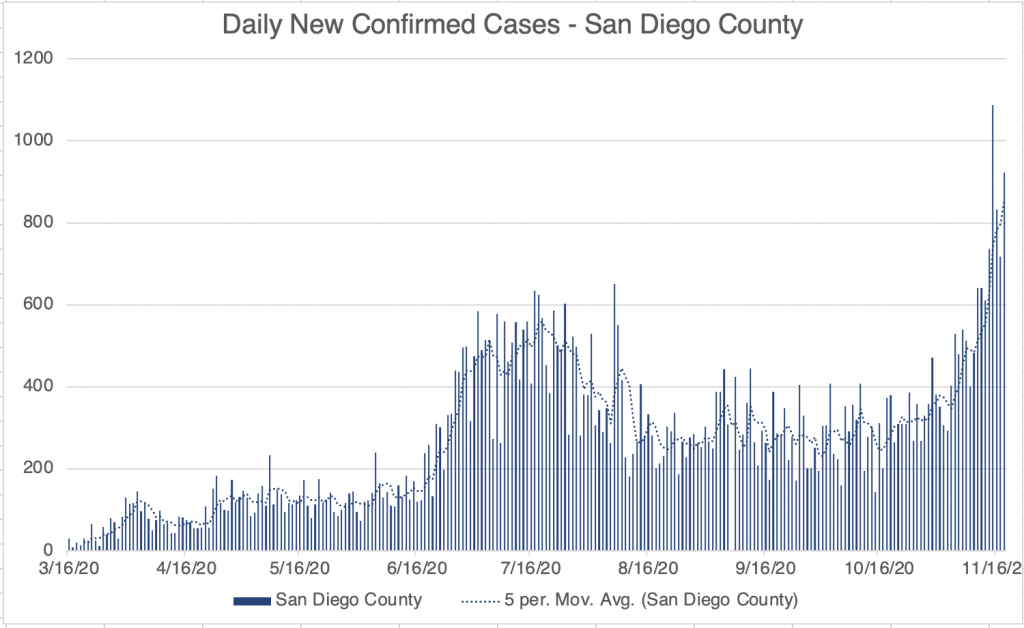
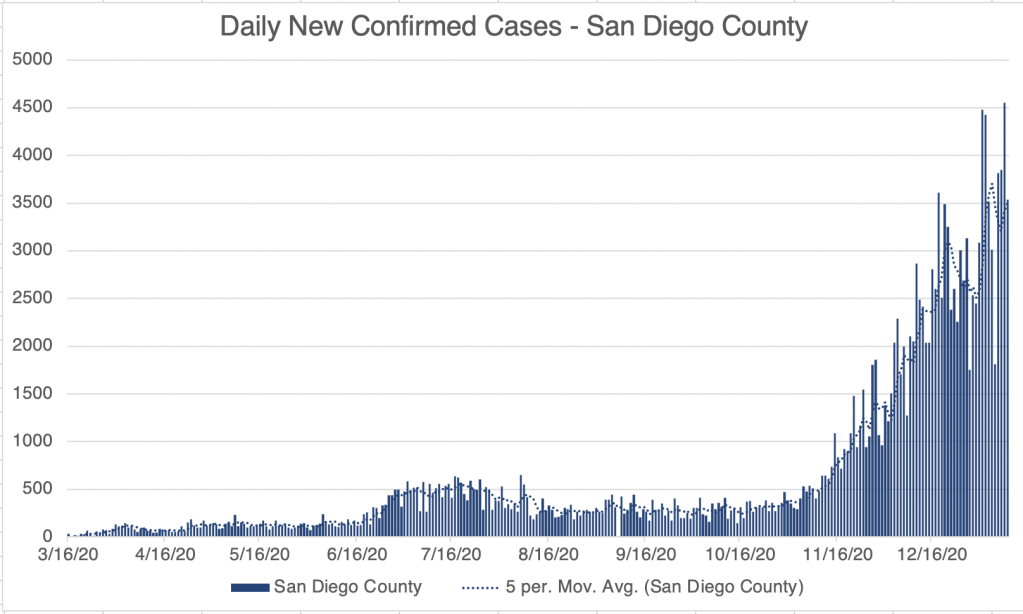
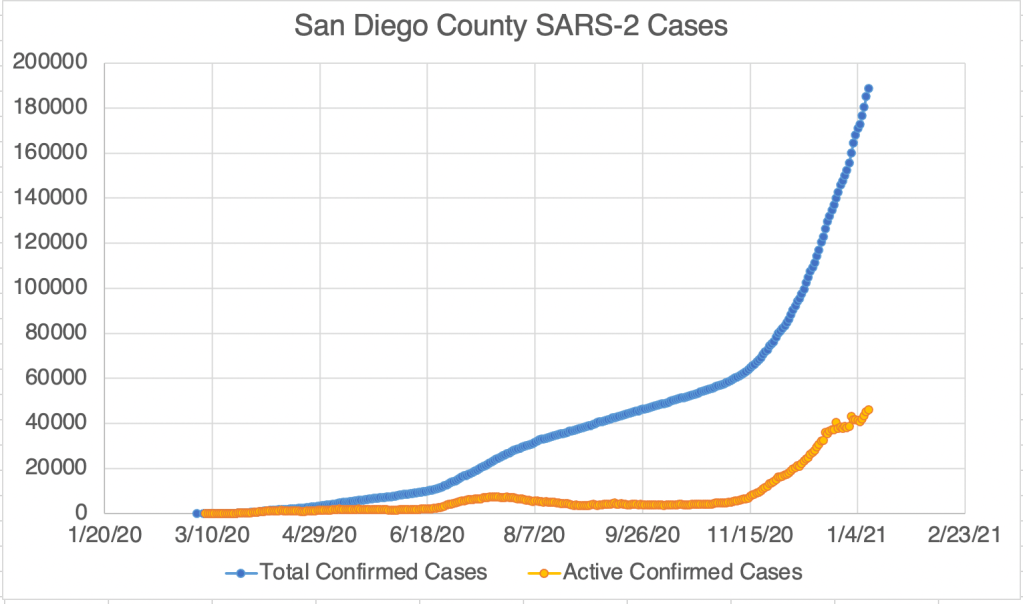
New confirmed cased numbers are continuing to increase in San Diego County, with no clear separation between Fall, Thanksgiving, and Christmas waves.
More new variants? I mentioned the new UK variant a few weeks ago. Since then, I’ve heard reports of new variants also arising in South Africa and Colorado. I don’t have much information on those yet, but the more people who are infected, the more likely a new strain will arise.
Equipment shortage. For those outside the medical community, just a little inside knowledge. The crisis has revealed many of the items that are limiting in our efforts to combat the virus. For the medical testing industry, many common materials have been very difficult to obtain, leading to long wait times for testing. There is a short supply of testing instruments, detection kits, RNA extraction machines, extraction kits, plastic plates used to contain testing reactions, and even plastic tips used to move small volumes of liquid in the lab. If you place an order of tips today, they may not arrive until April or May! This is part of the reason testing has been so slow and new labs difficult to start. I’m told that part of the issue is that there are only a few factories in the world that make medical plastics, and they are all overwhelmed. As a country, we’ll have to rethink our supply chain now and in the future.
Don’t fear, but be smart!
Erik