This long post will be a summary of what we have learned so far about the Coronavirus, and I’ll make some predictions about what to expect next. Since I’ll be sharing so much information, I won’t give references for everything here. I also have to make the disclaimer that new studies are constantly being done, and some of the below information may need to be revised later. To make my standard disclaimer, I am not an epidemiologist or a physician. I have a Ph.D. in molecular biology, and my specialty is infectious disease testing. On much of the below, I have an informed but not expert opinion.
Coronaviruses: Coronaviruses are a large group of viruses unrelated to the flu. What we think of as the common cold, are actually member of several classes of viruses like Adenovirus, RSV viruses, Rhinovirus, and several Coronaviruses. Many Coronaviruses cause diseases no more virulent than the common cold. However, just like novel flus can cause extra trouble, so can novel Coronaviruses. The first SARS virus was much more lethal that the SARS-2 virus, but because SARS had a short incubation period and made almost every infected person sick, it was much easier to contain. The Middle East Respiratory Syndrome (MERS) Coronavirus infects a few people every year, and is very lethal, with a fatality rate of 34%, but it also has not made a global impact. The reason SARS-2 is so dangerous is that it’s VERY infectious (Ro of between 2.5 and 5.7) and has a VERY long incubation time (2-14 days), making it very hard to track. Plus, it’s at least 2x as deadly at the annual flu.
Name: The official name of the virus is SARS-2-CoV (for Severe Acute Respiratory Syndrome-2 CoronaVirus). The official name for the disease it causes is COVID-19 (for COronaVIrus Disease-2019). You may notice that the term SARS actually sounds a lot like a disease. You would be right. So why did they need a different disease name than SARS-2, or SARS-19? I don’t know.
Spread: Early reports were that SARS-2 mostly spread like a flu, with droplets spreading from coughing or sneezing. It became apparent later that the virus was also spread through aerosols by laughing, singing, shouting, or even just talking in close proximity for long periods. As further study was done, it appears that most infected people don’t infect anyone else. Rather, most infections come from “super-spreader” events, in which a single person infects a large group of people. This usually happens indoors (at least 19 times more likely) during activities like fitness classes, funerals, concerts, and choir practices. While outdoor activities aren’t completely immune to these events, they are much more rare.
Viral load upon exposure appears to be an important determinant of how severe a case will be. Basically, this means that if you’re infected by a “low dose” of virus, your disease is likely to be less severe. I have several physician friends who have stated that it seems to them that cases in the hospital are less severe than they used to be. One likely reason for this is that since more people are wearing masks in public than early on, those who are infected are being infected by a lower viral load.
Early studies demonstrated that viable virus can exist on objects for hours or days. However, it does not appear that a substantial number of people are being infected because they have touched a contaminated object.
The WHO made a confusing claim recently that asymptomatic people cannot spread the virus. While this is technically correct, they were not clear that “asymptomatic” is a technical medical term meaning someone who does not have, and will never have, symptoms. Another group is “pre-symptomatic”. These are people who currently don’t have symptoms, but will develop symptoms in a few days. As it turns out, pre-symptomatic people do spread virus, and are likely responsible for up to 80% of new cases. So yes, people without symptoms can and do pass the virus to others.
Risk Factors: Many believe that only old people are at risk. While it’s true that age is a dominant factor, other risk factors are important, and younger people have also experienced severe symptoms. Other risk factors include respiratory conditions like asthma or COPD, heart conditions, kidney conditions, liver disease, diabetes, obesity, auto-immune disease, use of NSAID anti-inflammatory medications, being immunocompromised (HIV infected, undergoing cancer treatment, under medication for a transplant), vitamin-D deficiency, type A blood (Type O appears to be protective), inadequate sleep.
Always check with your doctor before changing your medications. I have an auto-immune disease and take daily anti-inflammatories, but my doctor has advised me to continue taking these unless I experience COVID symptoms.
Make sure your doctor is aware if you have any of the above conditions.
Symptoms: Many people who have SARS-2 experience no symptoms, or experience mild flu symptoms. If you have ANY cold or flu symptoms, contact your doctor and see if you can be tested. If you live in San Diego County, and your doctor cannot offer you a test, call 2-1-1 to get a free test from SD County Public Health. If you have additional symptoms like shortness of breath (you just can’t seem to get enough air), loss of smell or taste, nausea or diarrhea, contact your health care provider or an urgent care immediately.
In severe cases, the virus can do wide spread and permanent damage to multiple organ systems. Early treatment is necessary to prevent the most severe symptoms.
Precautions: While lockdowns may have been effective in the US during the early stages of the pandemic, especially at a time when masks were hard to come by, recent evidence suggests that lockdowns provide only a moderate benefit over other means of control. Here’s what appears to be beneficial:
Masks: Masks are not all the same and some are better than others. Their main benefit is that they stop, reduce, or slow the travel of virus from infected people. This prevents surrounding people from infection, or lowers the viral load of exposure. Some, but not all, also prevent the wearer from inhaling airborne virus. N95 style masks without a valve are best if you can obtain one.

Social Distancing: Aerosolized virus can travel through the air. Staying 6 ft away from others helps prevent infection.
Handwashing:
Adequate sleep: Sleep is very important for a wide variety of body functions, including the immune system. Get 7 – 8 hours of sleep per night. A 26 minute power nap during the day is also beneficial if needed.
Vitamin D: Several studies have suggested that patients with the most severe cases of COVID also have the lowest levels of Vitamin D. Because of our often indoor lifestyle, most Americans are Vitamin D deficient to some degree. The best way of getting some Vitamin D is to make it yourself by going outside in shorts and a T-shirt for 30 minutes a day. This is because Vitamin D is manufactured in our skin in response to sunlight. If it’s not practical for you to do this, consider a Vitamin D supplement. Darker skinned people are more likely to be Vitamin D deficient in the US.
Home isolation: If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Tests are much more available that early in the pandemic, and you should be able to get a test by request. Also, if at all possible, isolate yourself from the rest of your family until you can be tested as negative. Many new infections are taking place among family members.
Testing: There are several kinds of tests, and they tell you different things.
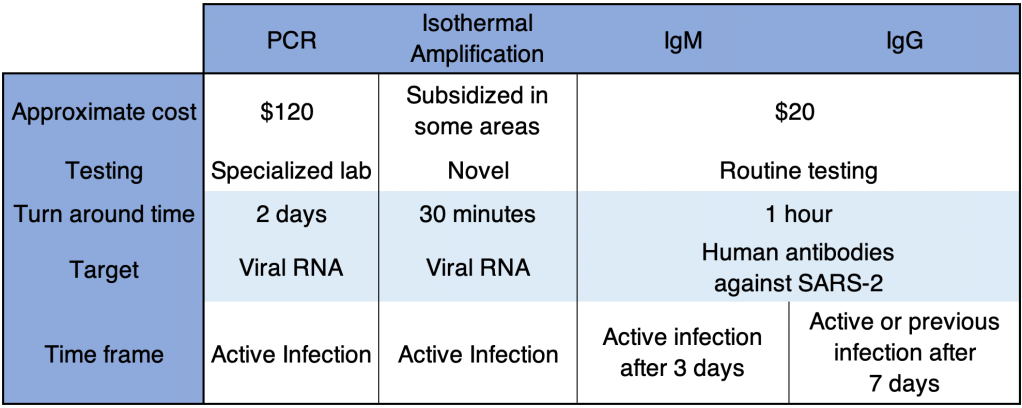
PCR: These tests use material collected from the nose and need to go to a specialized laboratory for processing. They are very sensitive and specific, and indicate whether the patient is currently infected. This is the most common kind of test.
Antibody: These tests detected antibody from a patient’s blood to see if the patient has been infected for at least a few days. IgG tests may also tell if a patient was infected weeks or months previous, but are no longer infected. Some patients do not mount an immune response that will provide long term antibody.
Isothermal amplification: The Abbott ID Now COVID tests uses this relatively new technology. These tests are similar to PCR and are both sensitive and very fast.
If you have cold or flu symptoms, contact your doctor immediately and see if you can get a test. Testing is much more available than it was early in the pandemic. San Diego County is encouraging anyone who wants a test to be tested.
Treatments: Treatment for COVID is complicated and not all patients can be treated in the same way. Additionally, treatments are evolving rapidly, and your doctor many not treat you in the ways listed below.
Ventilators: Some doctors now state that ventilators carry risks that may be unacceptable for COVID patients. Many doctors now favor a nasal cannula, using ventilators only as a last resort if breathing is labored.
Hydroxychloroquine, Azithromycin, Zinc: Several doctors from several countries have reported success with this combination. Studies on the effects of these drugs have as yet still been non-conclusive. Some positive studies suggest that Zinc is the main virus fighter of the treatment, with Hydroxychloroquine allowing better penetration of Zinc into cells. Unfortunately, the debate on the efficacy of this regimen has taken on a strongly political tone, which almost always interferes with the scientific process. Now pundits, as well as scientists, weigh in on this regimen. I’m still holding a “wait and see” posture with this treatment.
MATH+: This regimen uses Methylprednisolone (an anti-inflammatory), Vitamin C, Thymine, and Heparin, as well as optional other treatments including Vitamin D and Zinc. Early reports suggest success with this treatment.
Vaccines: Each spring, scientists learn which flu is likely to be prominent by the following Fall. They make some guesses and create a vaccine for the flu season. The manufacture process takes a few months. But it’s only this short because they already know how to make a flu vaccine. Development of a brand new type of vaccine takes between 4 and 30 years! There are many methods to make a vaccine, and scientists must try many of them before finding one that works. Then they must try the vaccine on patients and make sure they are relatively safe. Every vaccine carries some risk of side effects.
Early estimates for a Coronavirus vaccine were around 18 months. My guess is that this is too optimistic. Personally, I wouldn’t count on a vaccine for at least a few years. In addition, some studies have suggested that Coronavirus vaccines in particular may cause side effects that may make vaccine development challenging. My standard practice for my family is to wait on new drugs for a few years before using them myself. While I pro-vaccine in general, I would personally recommend waiting for a few years before getting a Coronavirus vaccine.
Herd Immunity: Some are promoting herd immunity as a way to move through the crisis faster. The idea of herd immunity was popularized in pre-pandemic discussions on vaccines, promoting the idea that the more people are vaccinated, the more protection for those who can’t be. This is a good idea when a vaccine is available, but not when there is no vaccine. Putting many people in harm’s way to protect fewer others is not wise and is not standard medical practice.
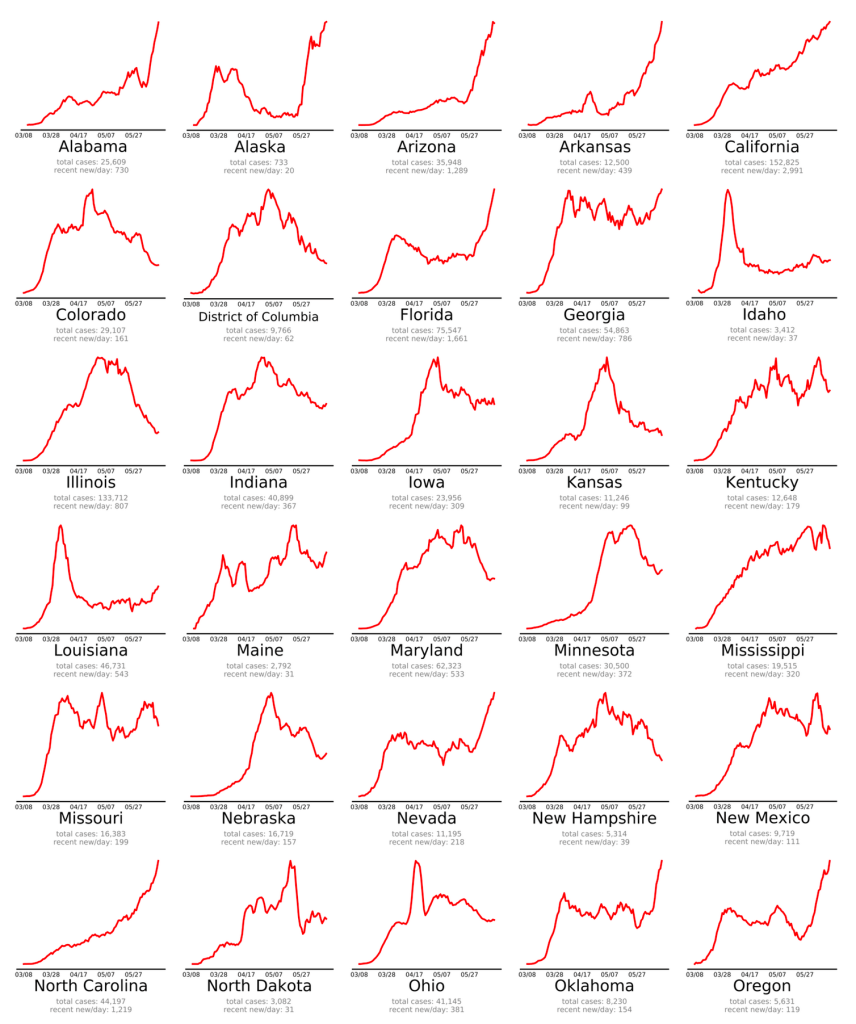
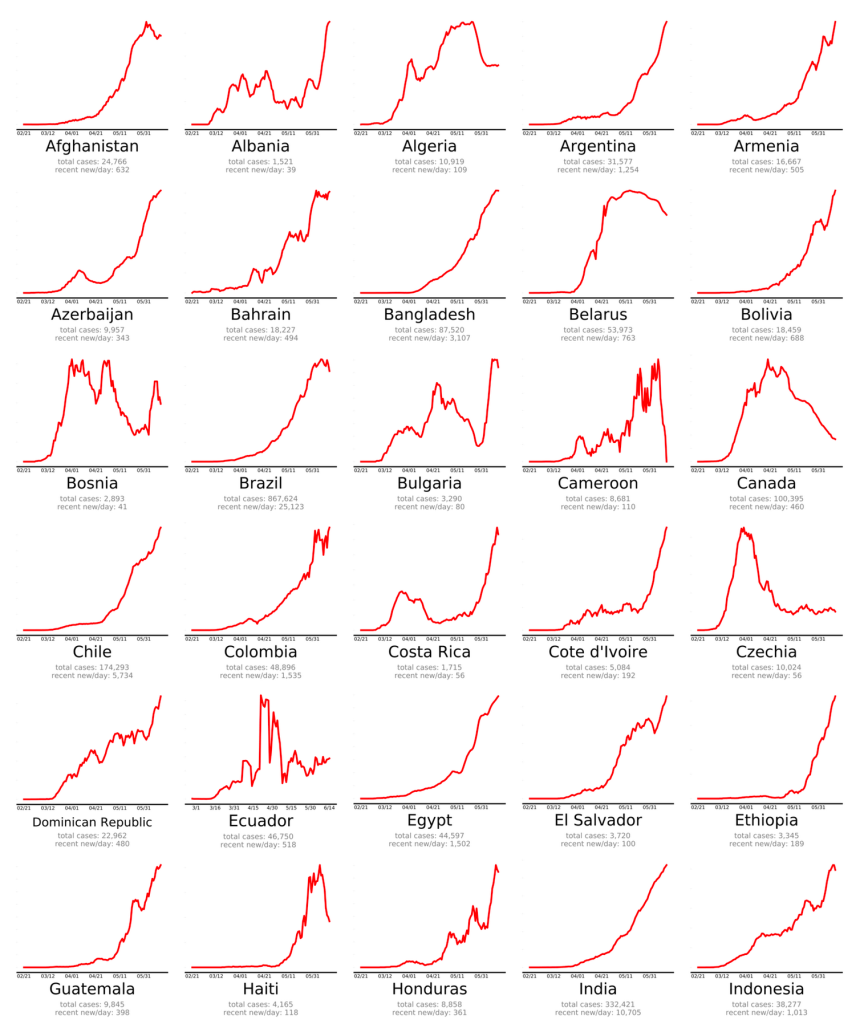
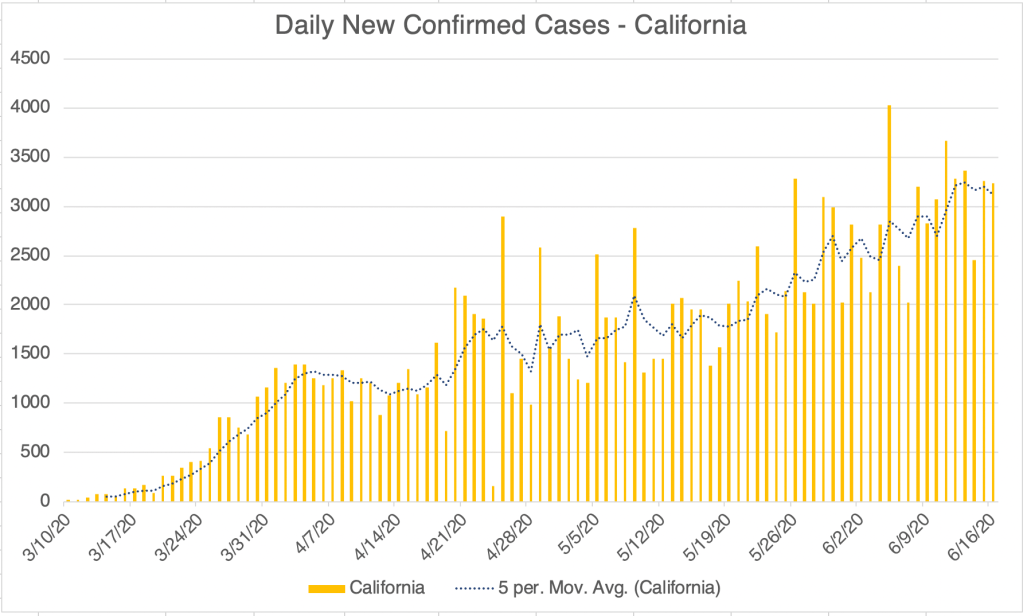
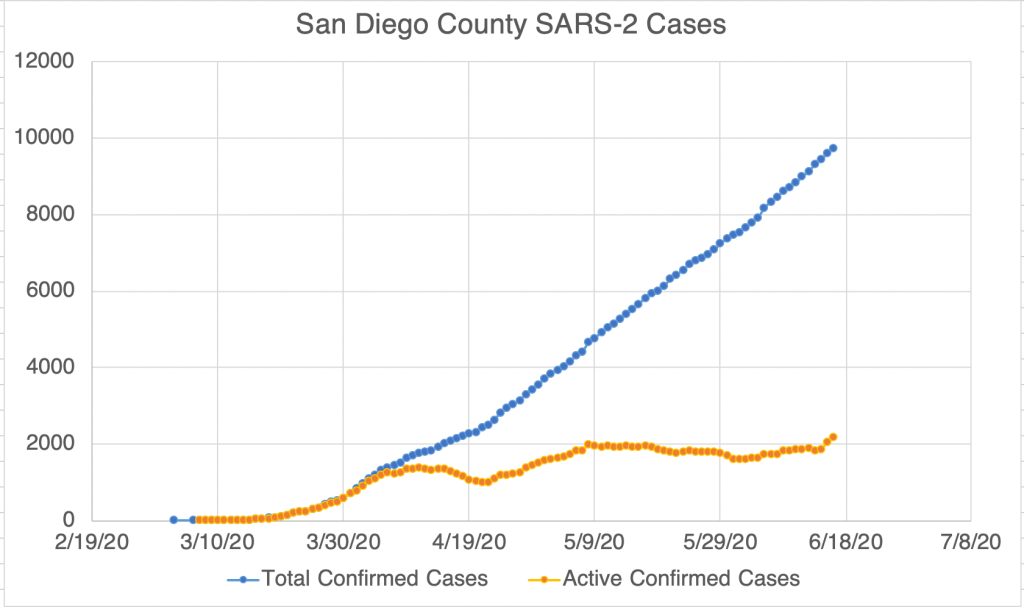
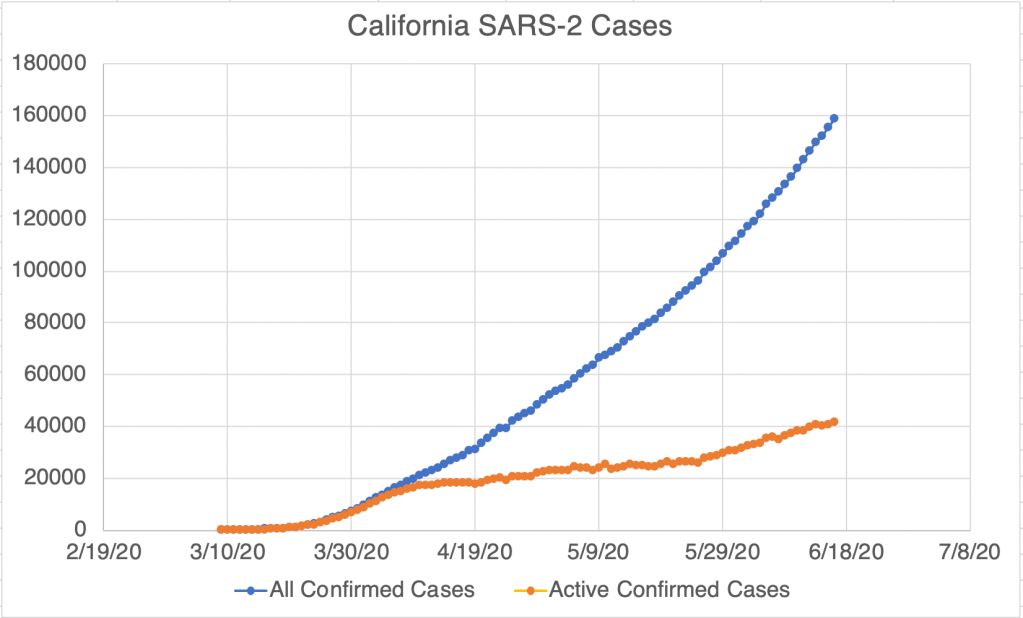
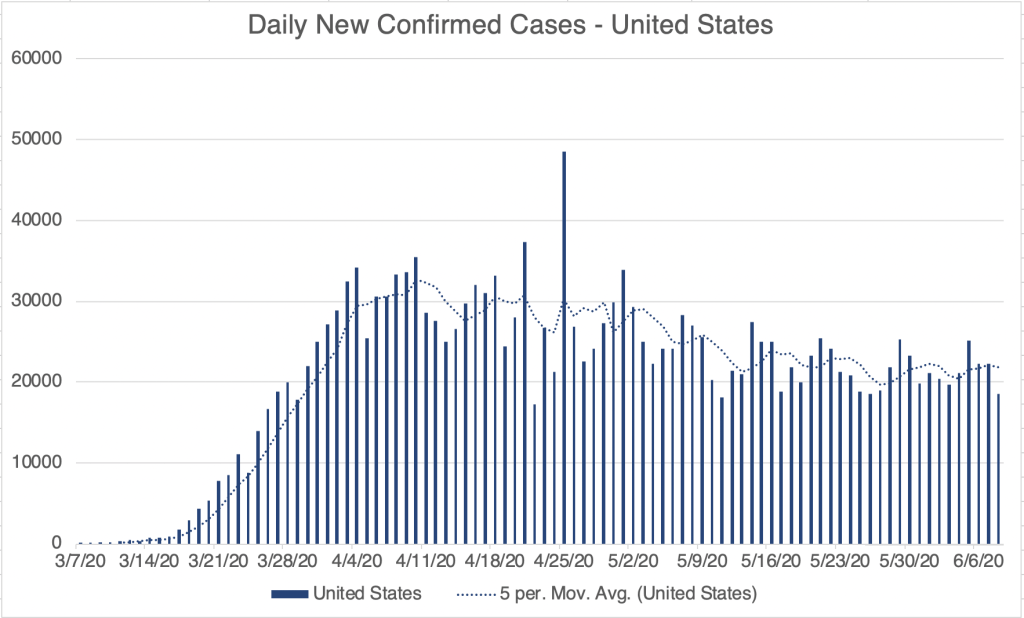
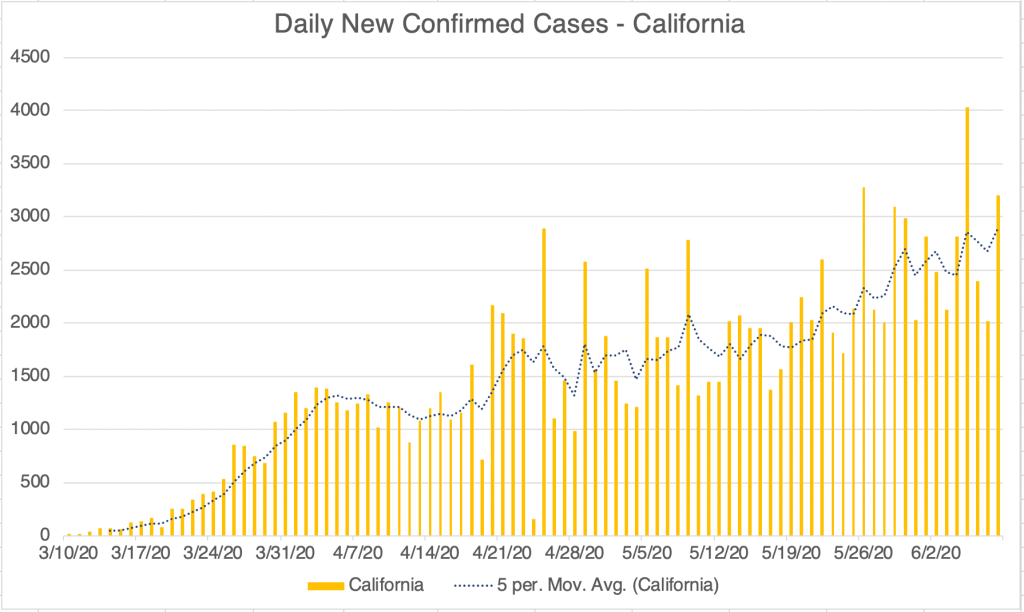
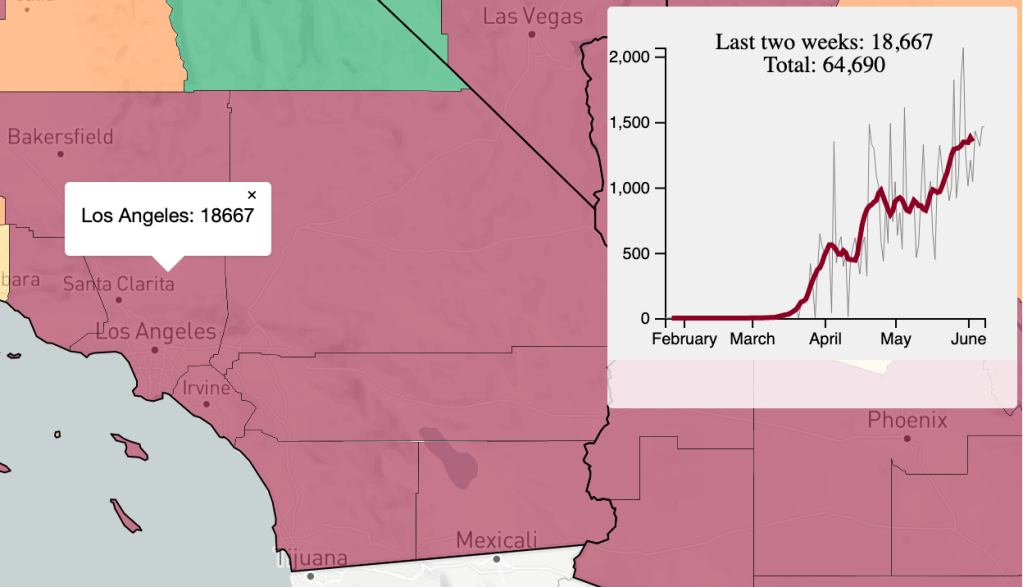
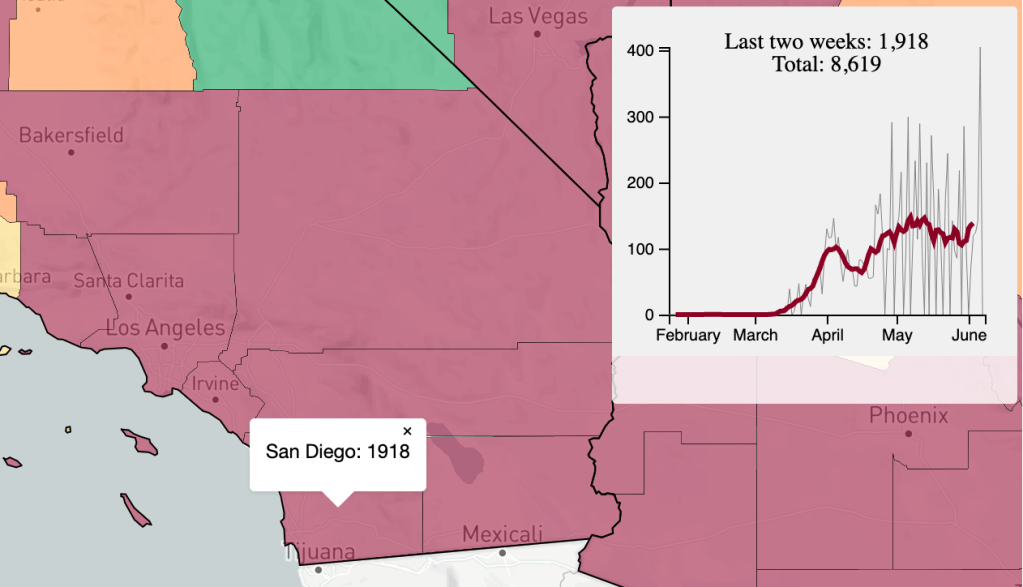
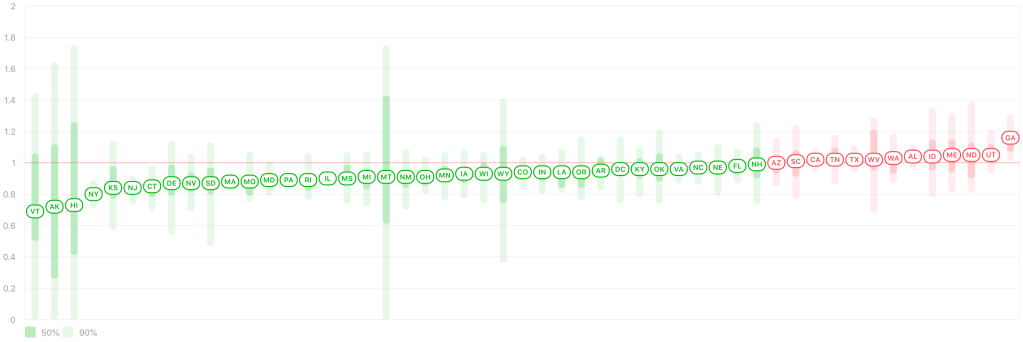
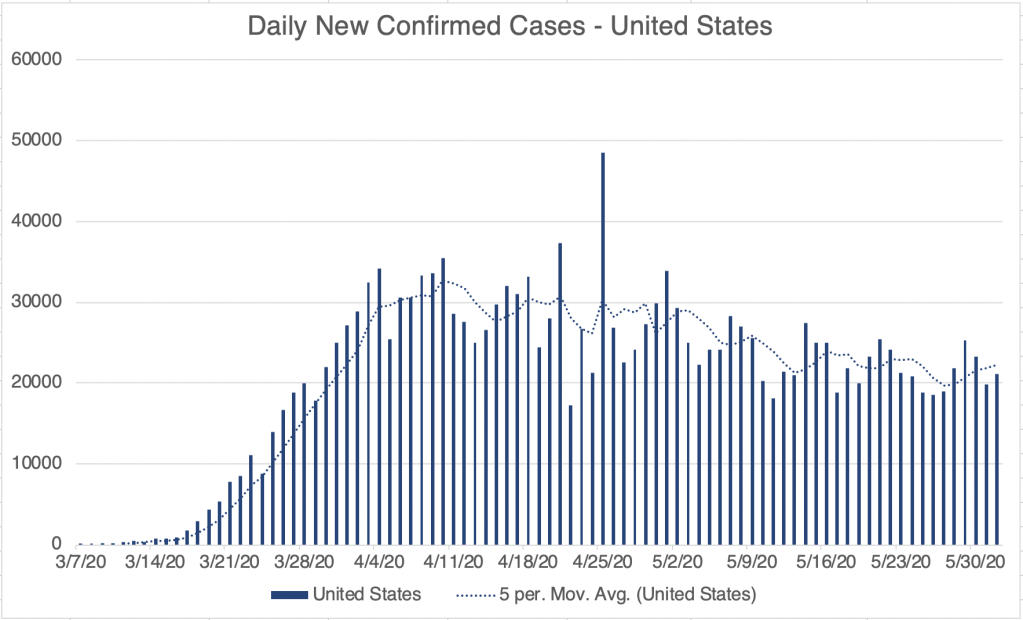
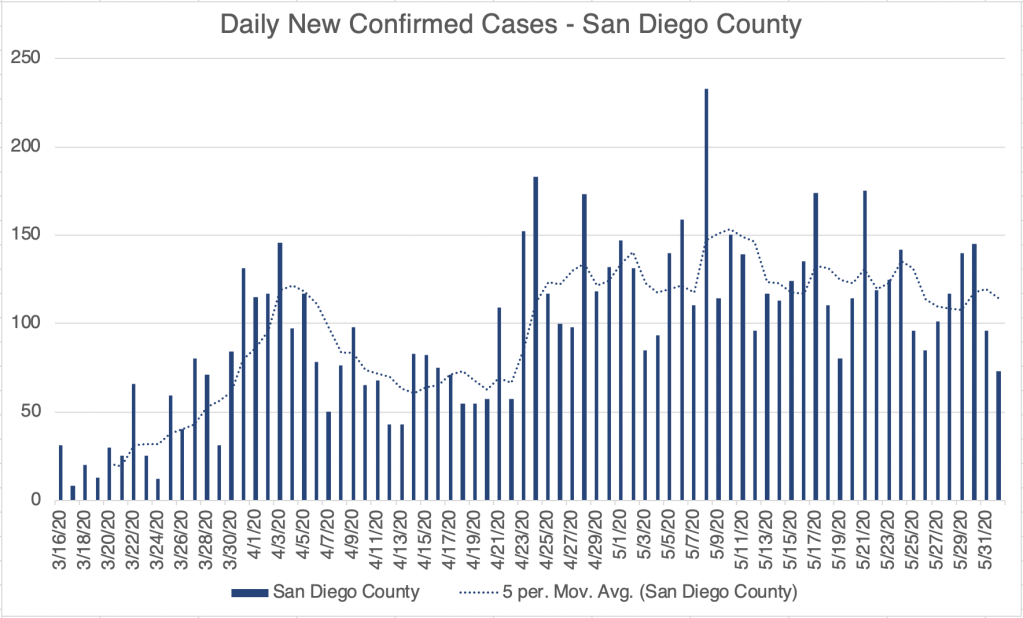
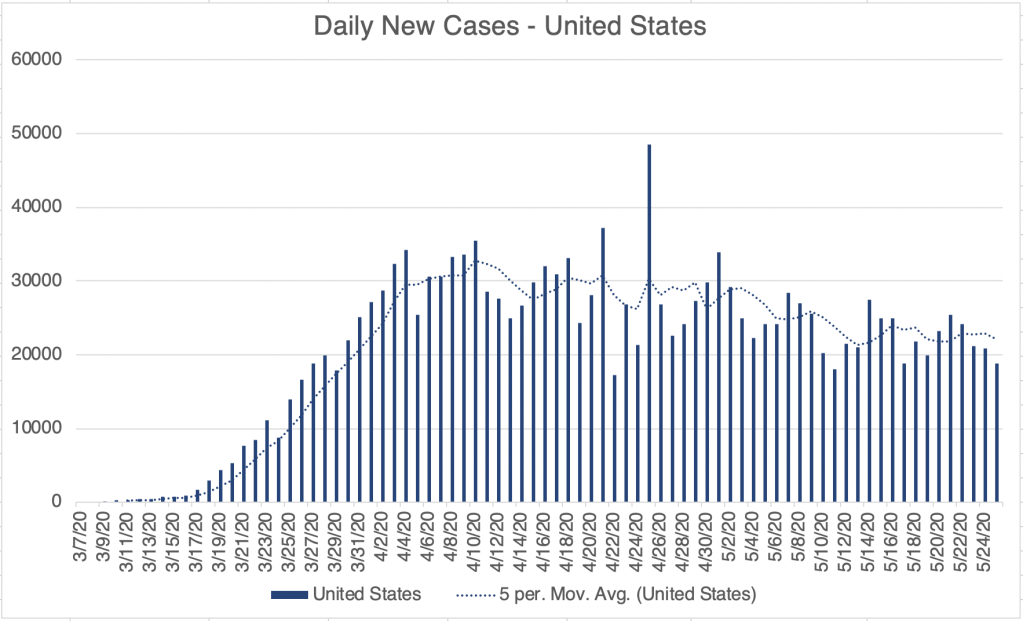
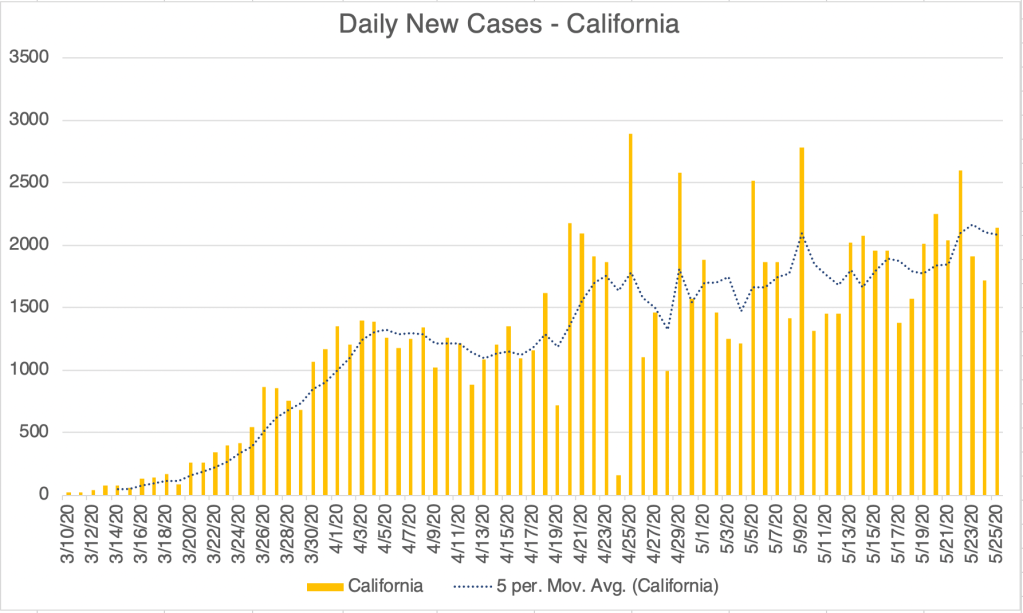
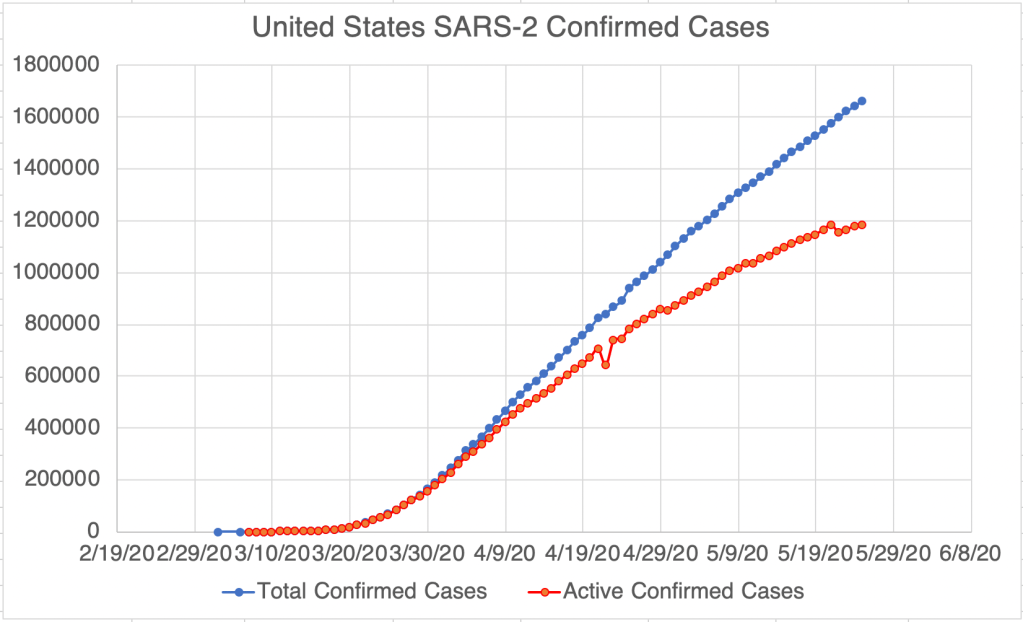
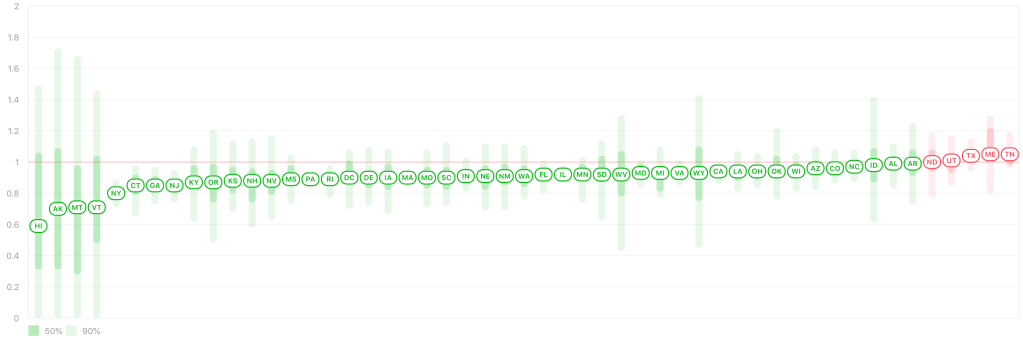
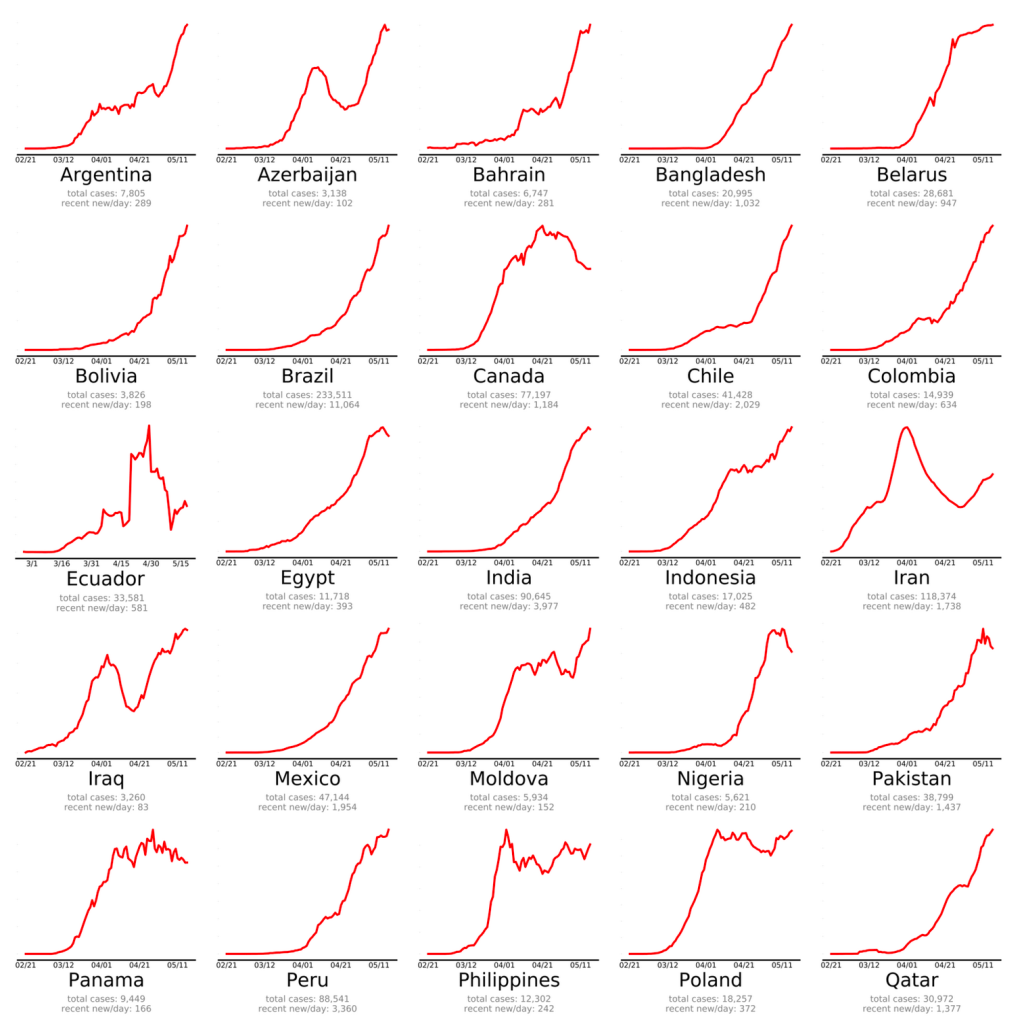
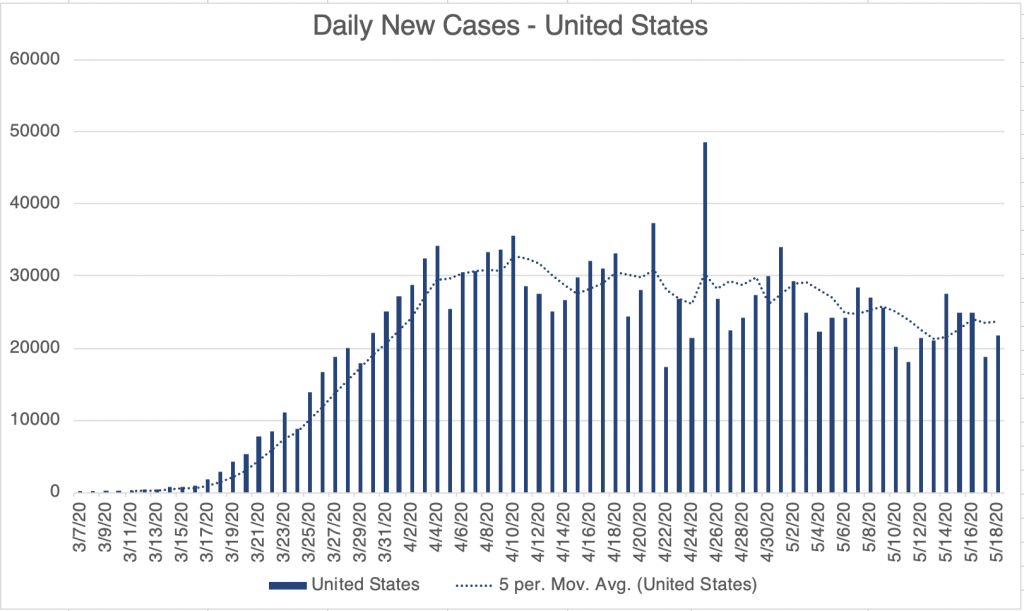
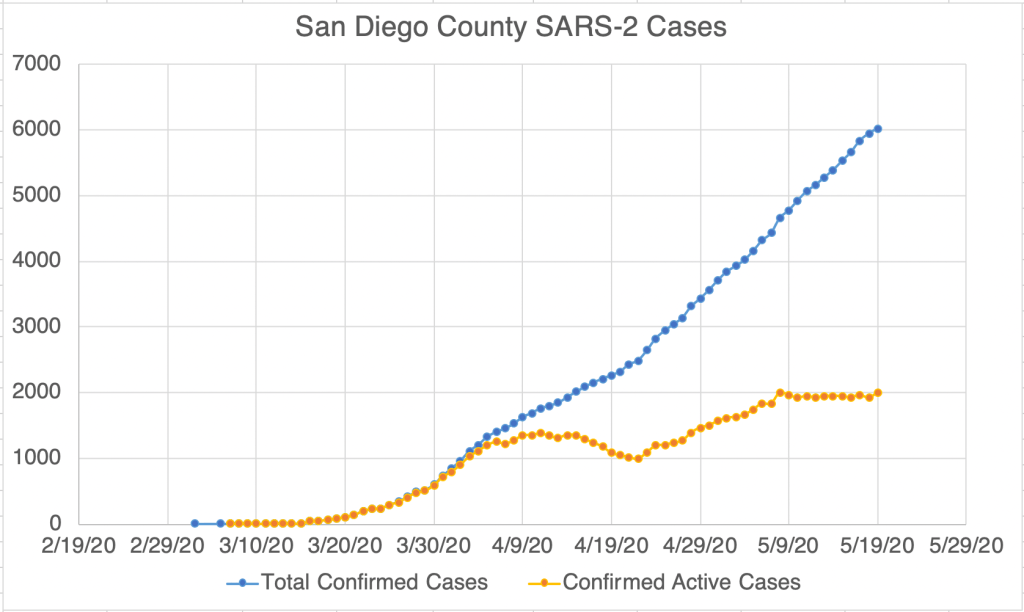
The Future: Of course, it’s impossible to know what will happen next. My initial prediction was that the first wave would be over by July, and at this point, this doesn’t look likely. New confirmed cases have started to rise or rise faster in the 3 areas I monitor most closely, the US, California, and San Diego County, and cases are rising fast in some countries previously unaffected, especially Brazil, Russia, and India. So I’m starting to think we may not be out of the first wave before the Fall season.
In addition, RNA viruses, such as Coronavirus, can mutate very quickly because the proteins used to copy their genomes are very error prone. This means that a virus may change to a new form that can re-infect a person who has already had a previous version. Some reports suggest that this may already be happening with SARS-2. Some good news is that on the very long term (years), novel viruses tend to evolve to be less virulent, because it’s not in the “interest” of the virus to make the host very sick. The message is, we may need to adapt to a new reality for the next few months or years. We can’t really afford to be “locked down” anymore, but mask wearing and elbow bumps may be a part of the landscape for some time.
Don’t fear, but be smart,
Erik