This is a COVID update. I’ve been posting only every 2 weeks for a while, but this has been an interesting week, so I’m posting a little early.
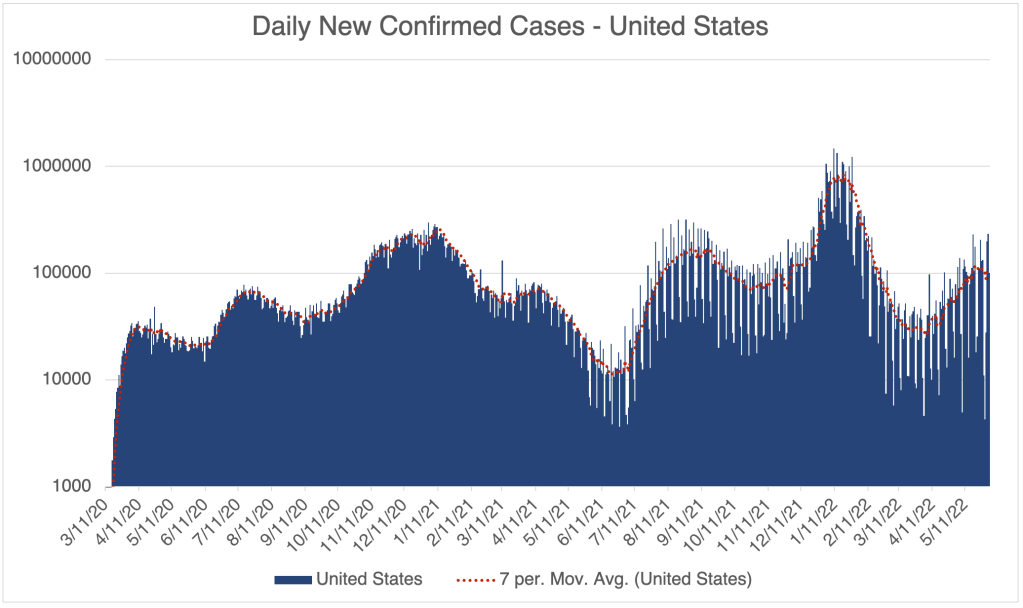
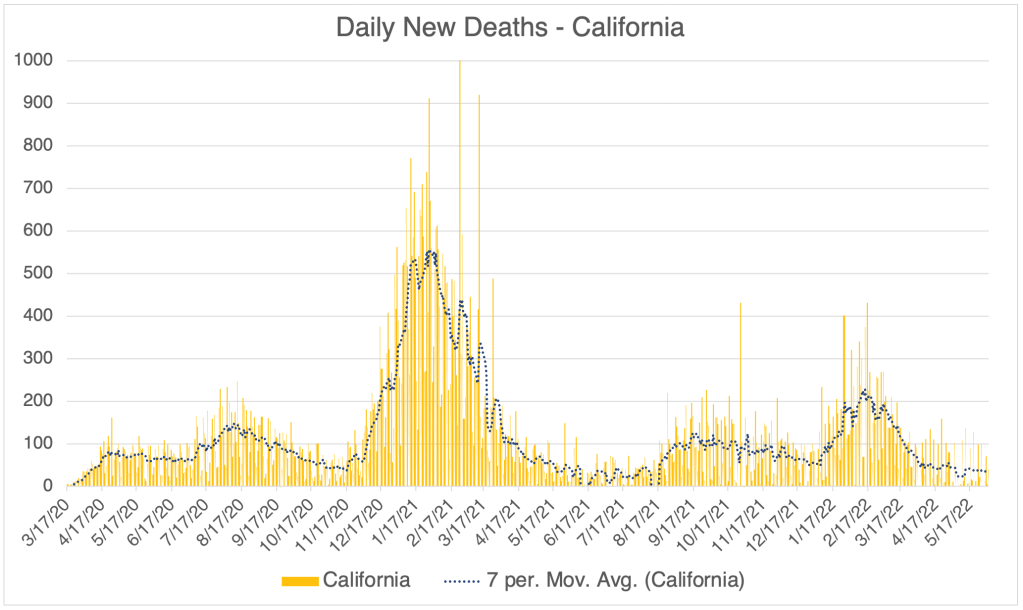
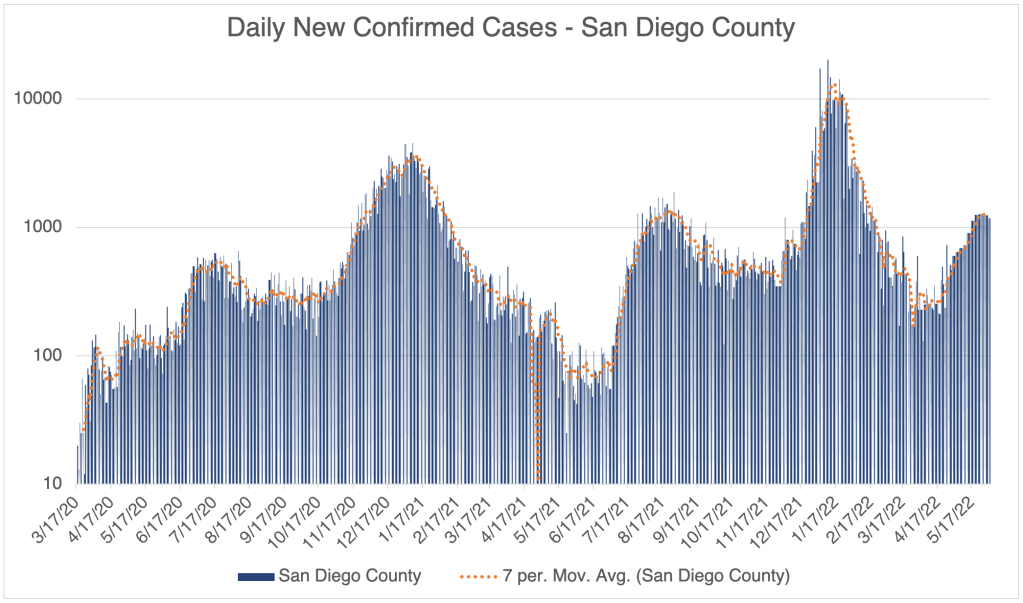
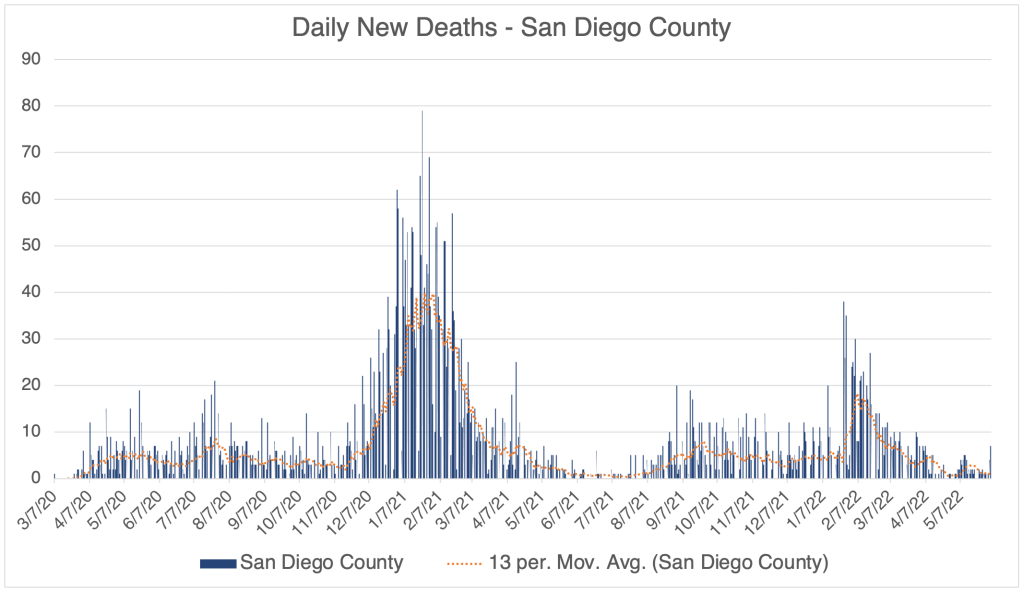
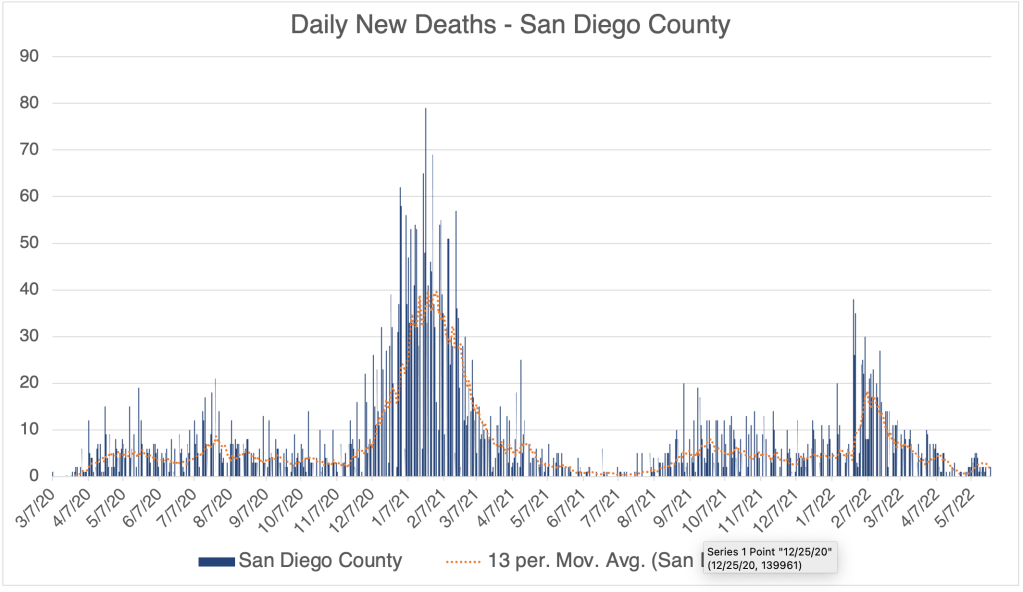
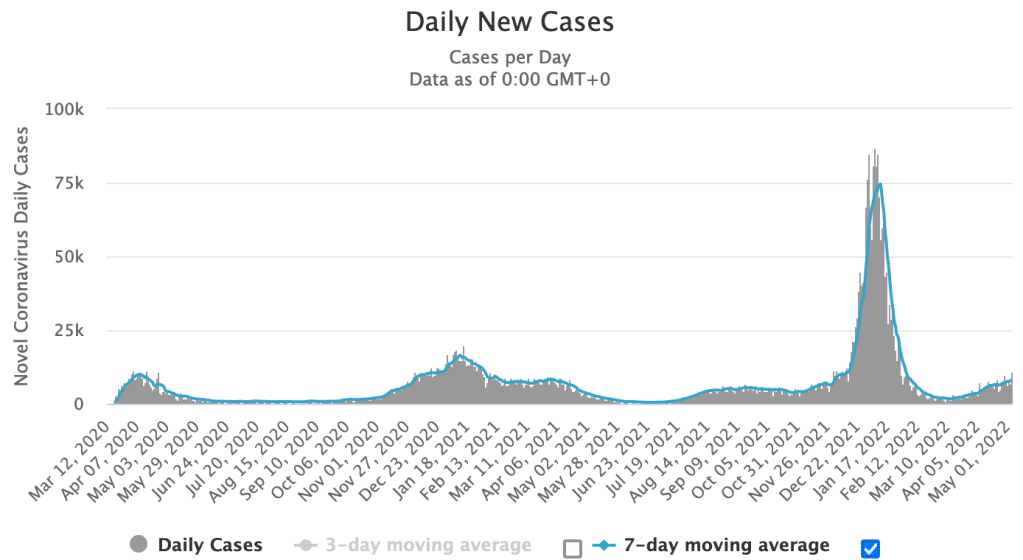
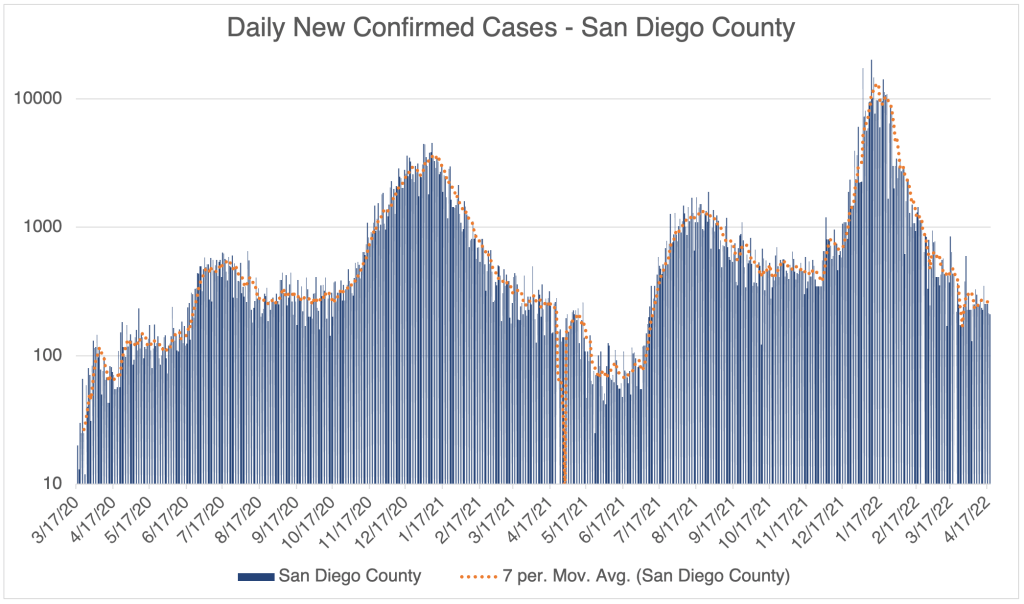
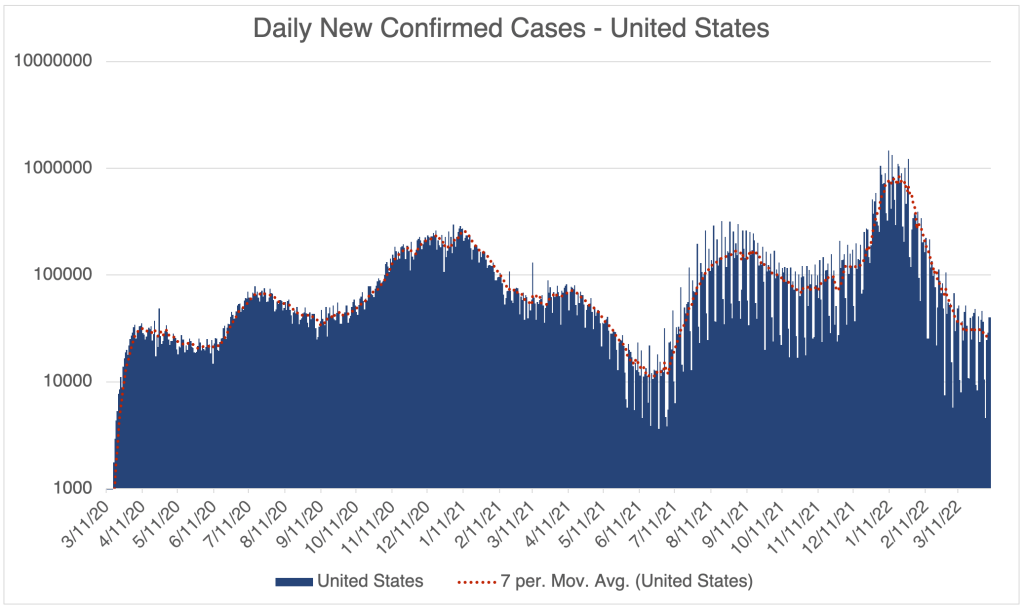
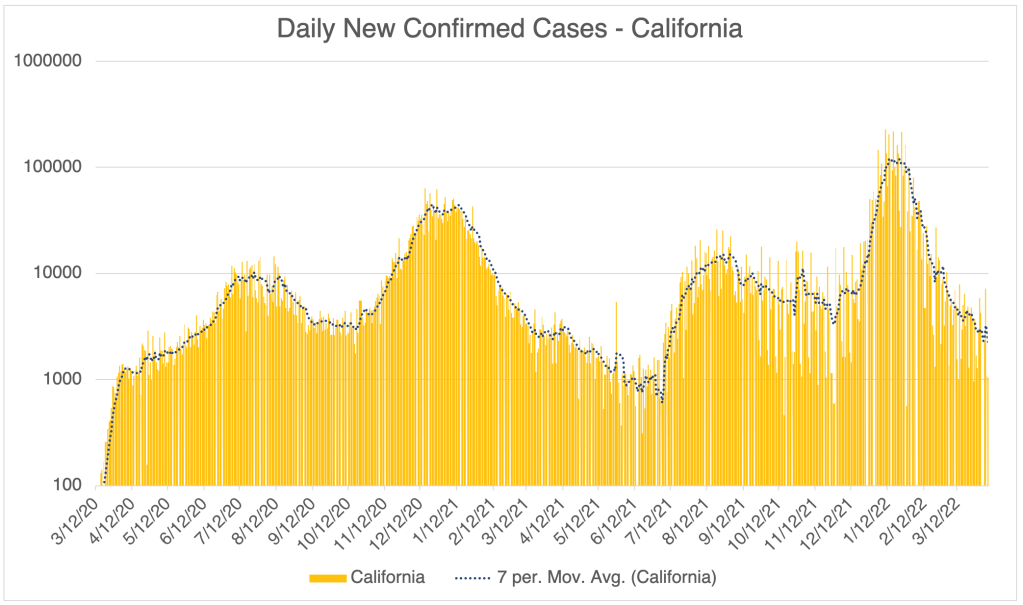
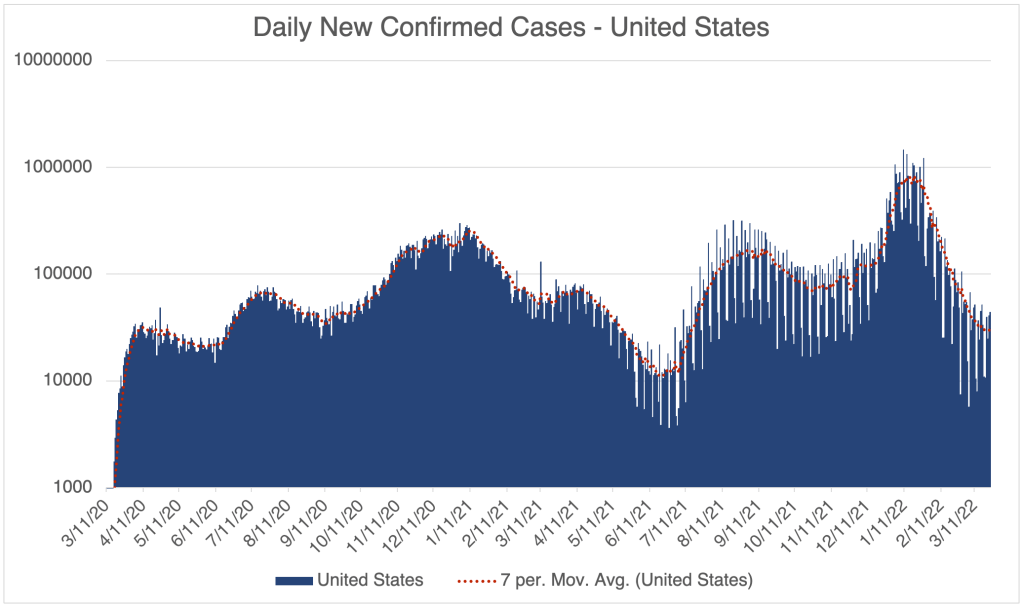
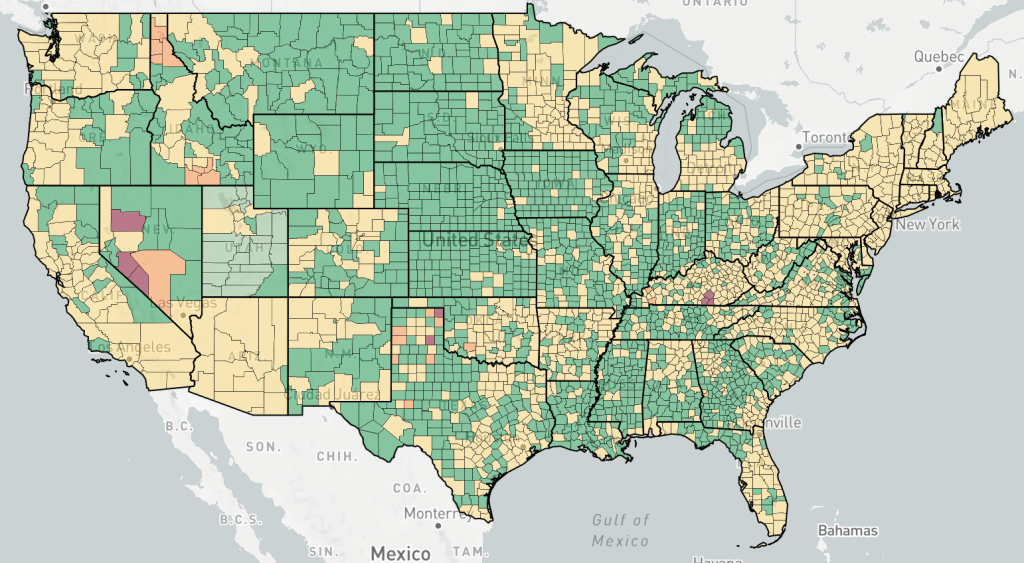
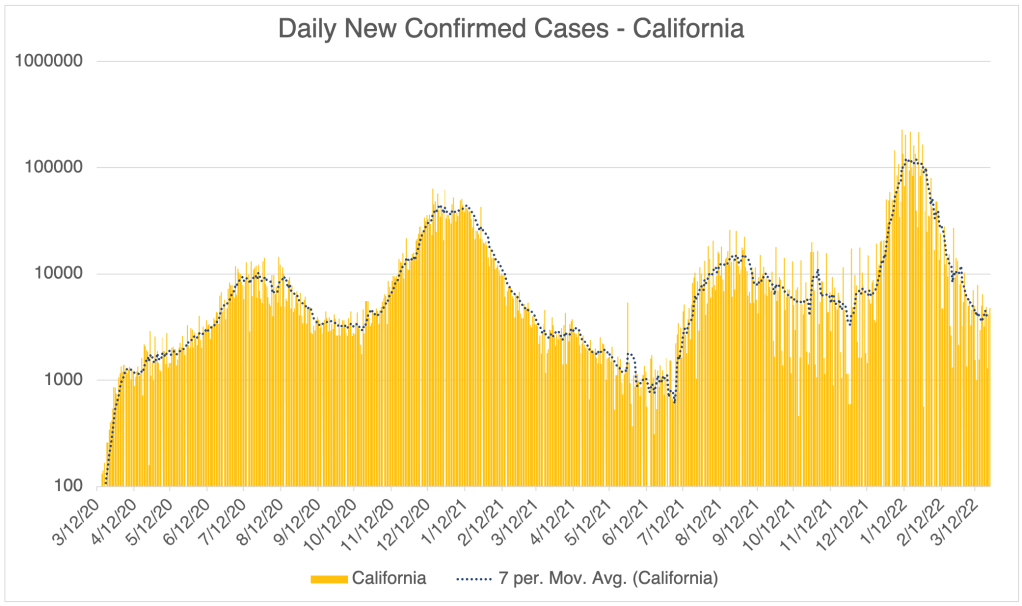
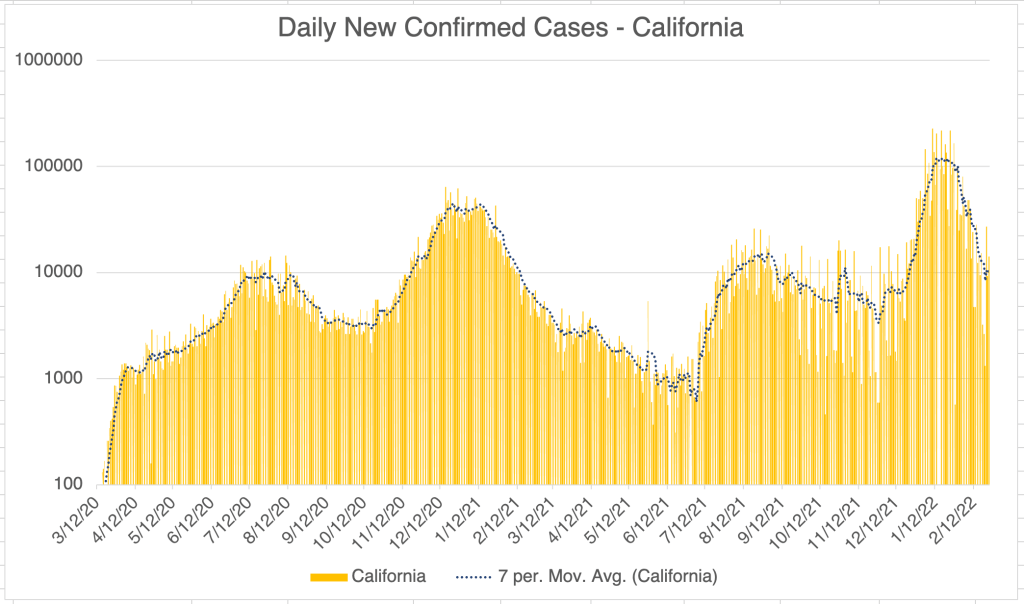
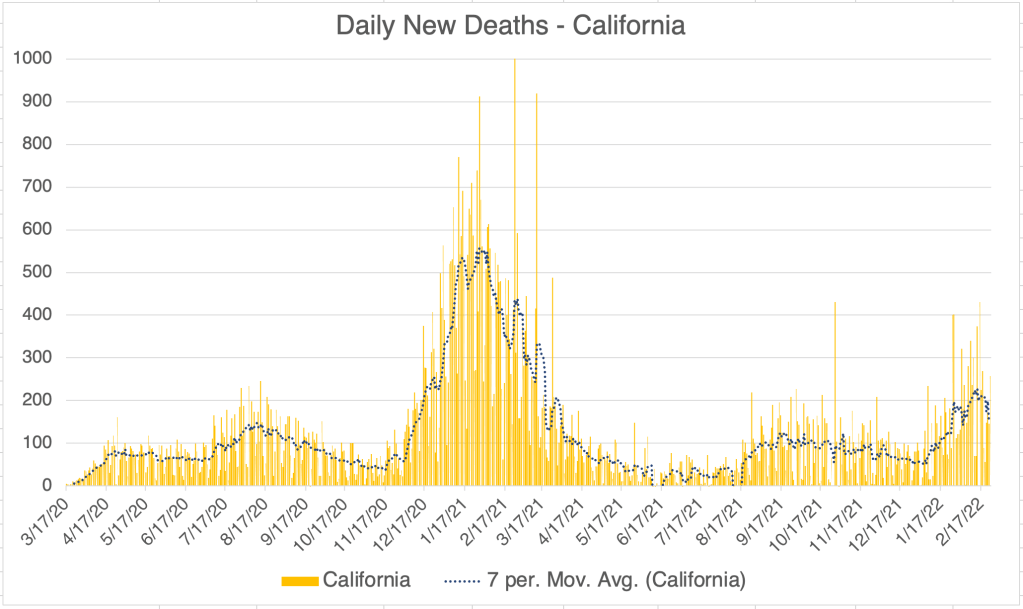
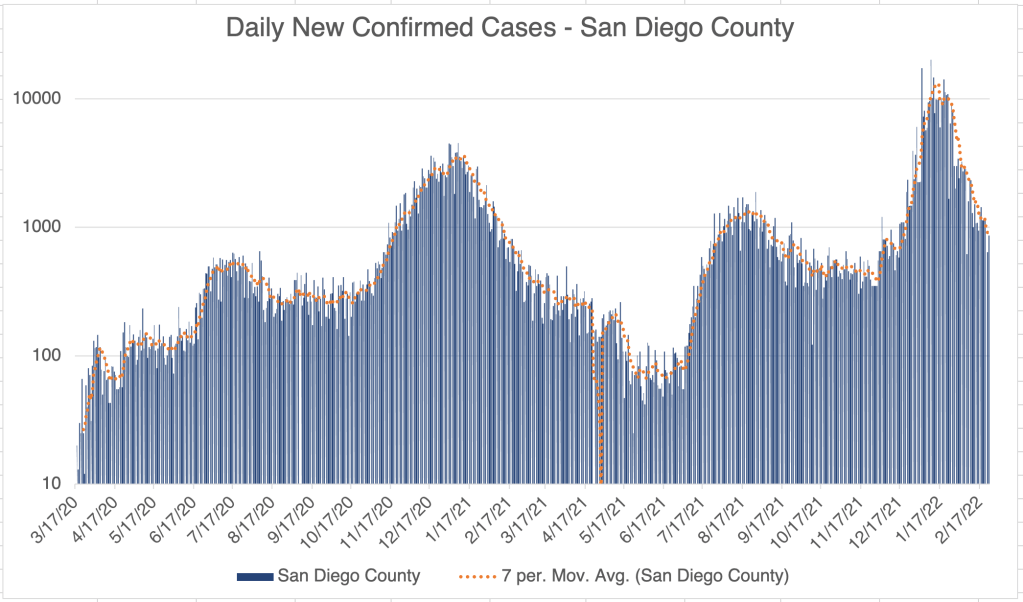
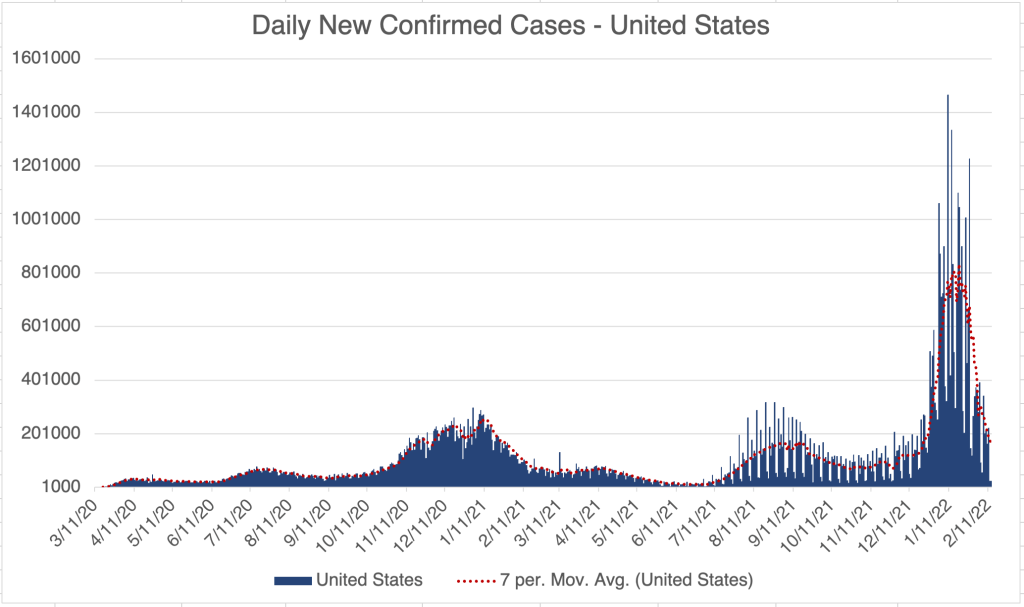
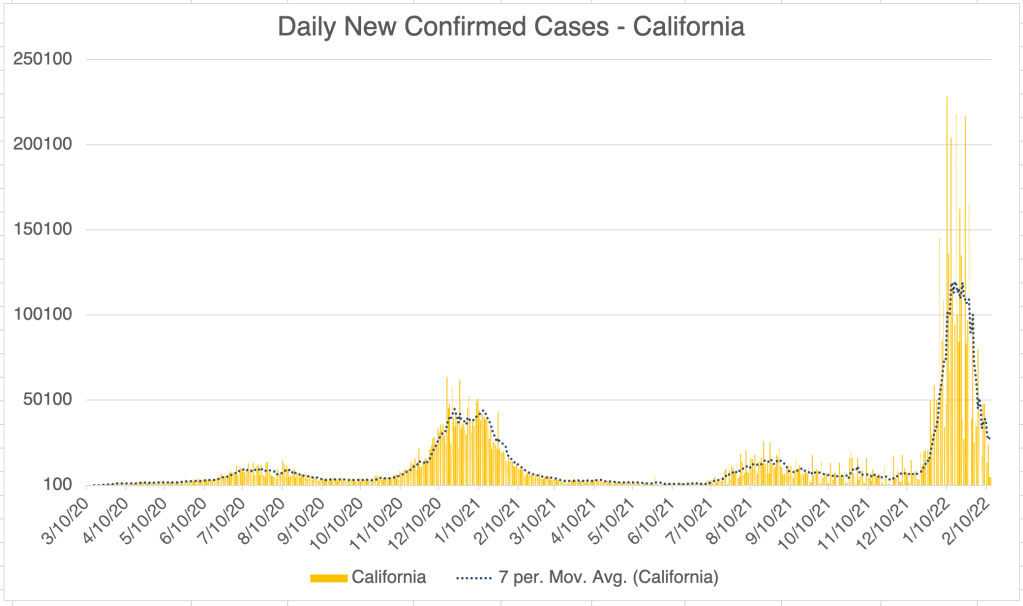
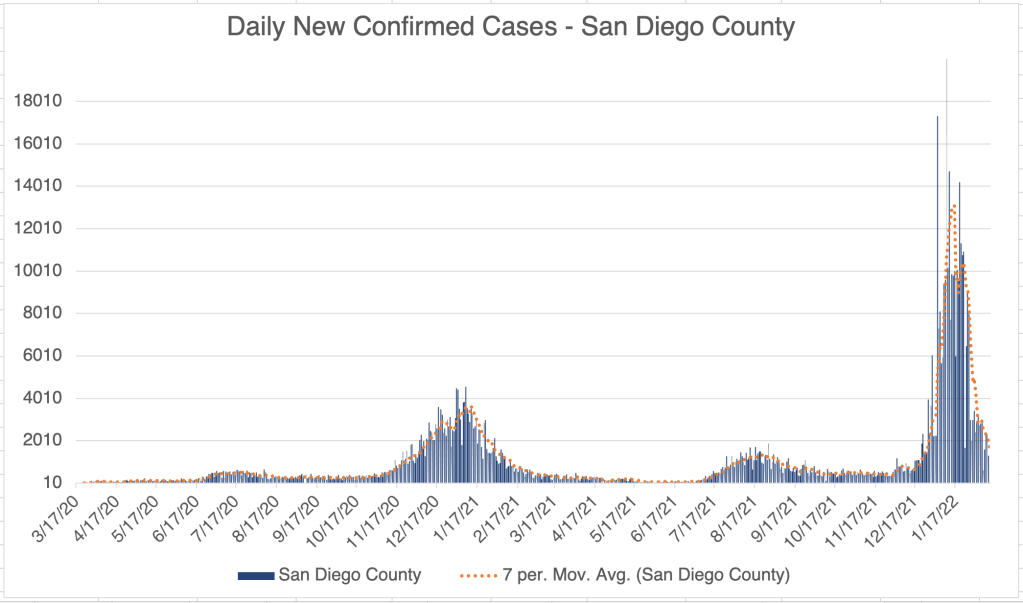
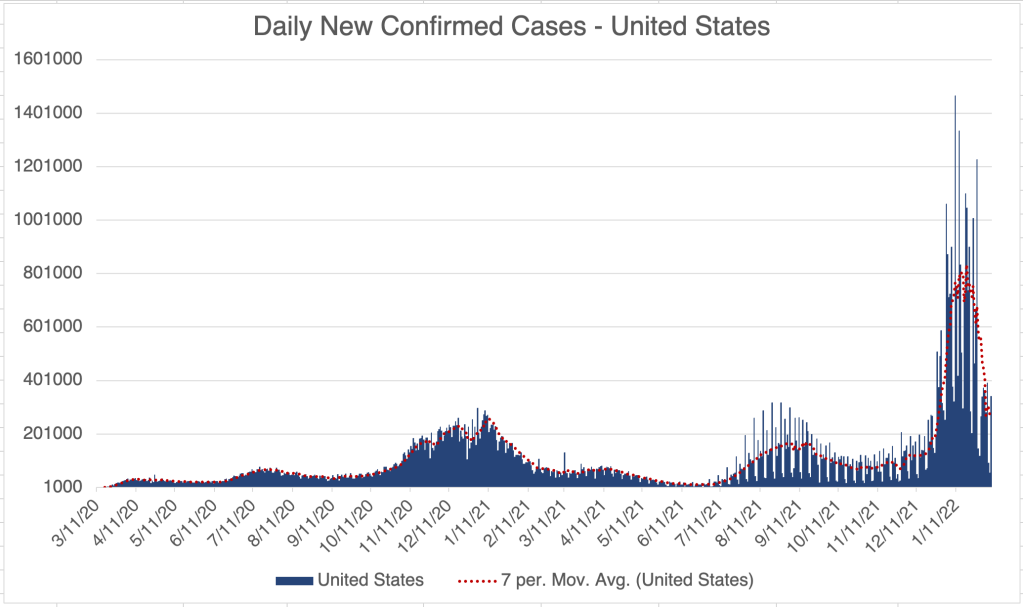
New case numbers for the US, California, and San Diego County show that the second Omicron wave, I’ll call it the BA.2 wave, has peaked, and numbers are now dropping sharply.
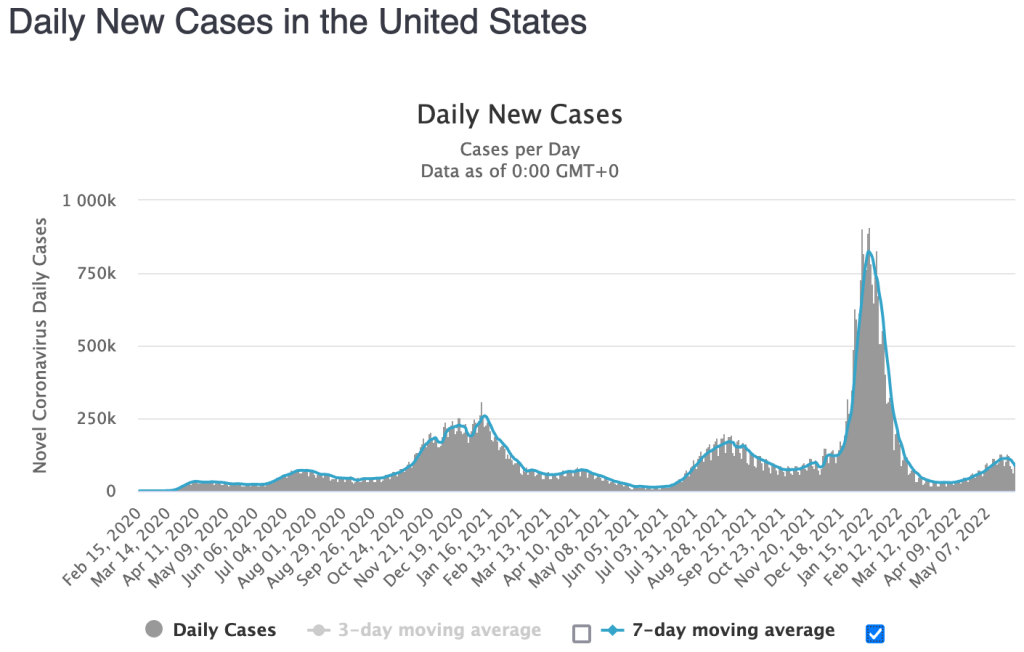
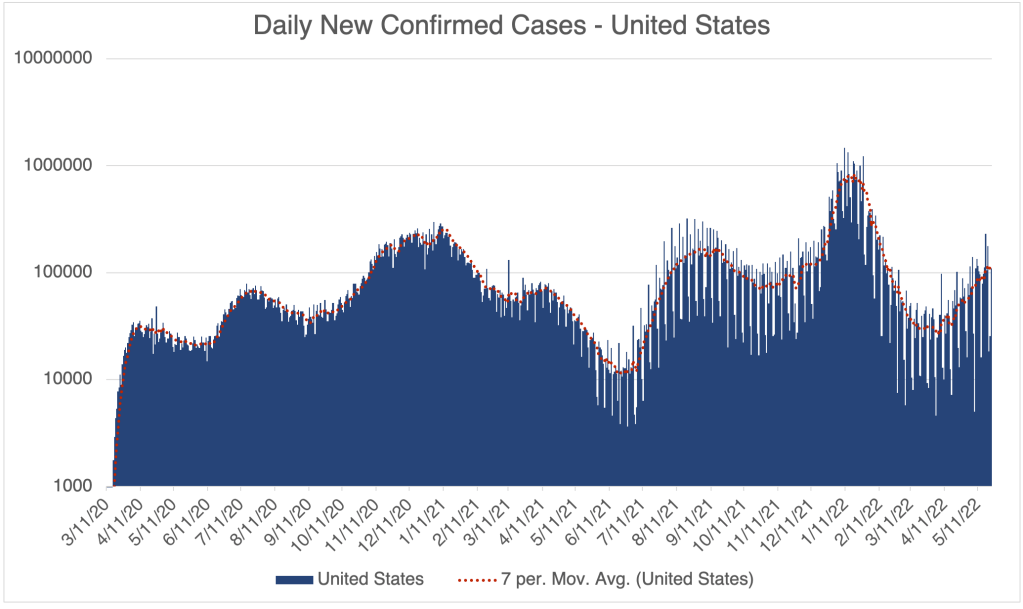
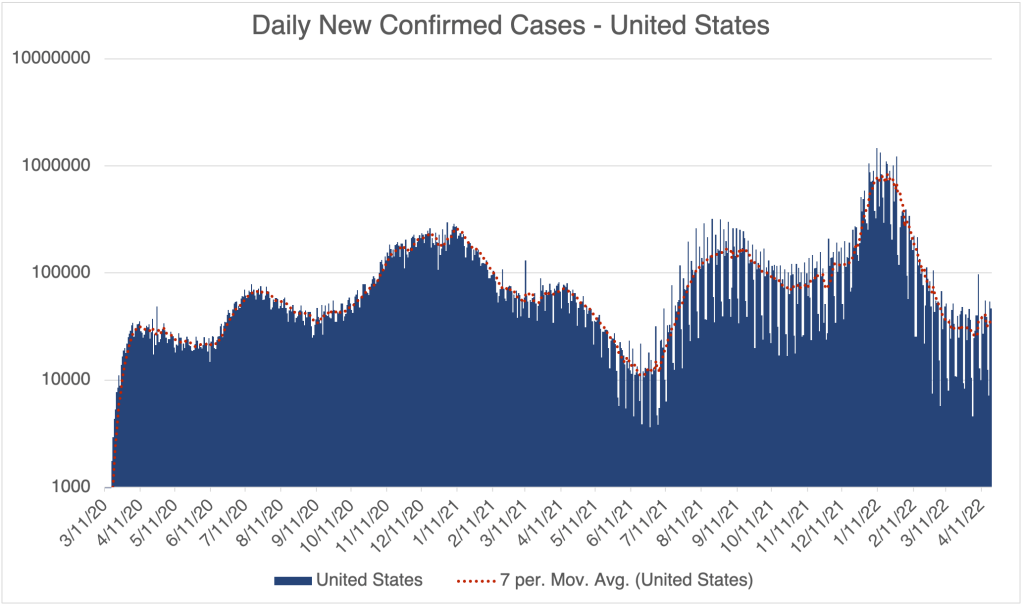
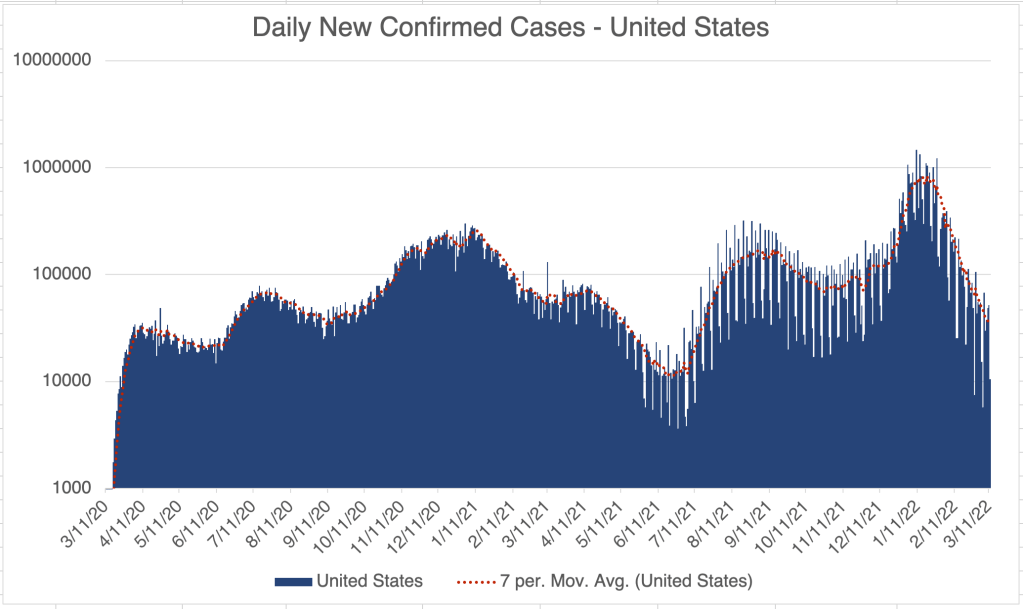
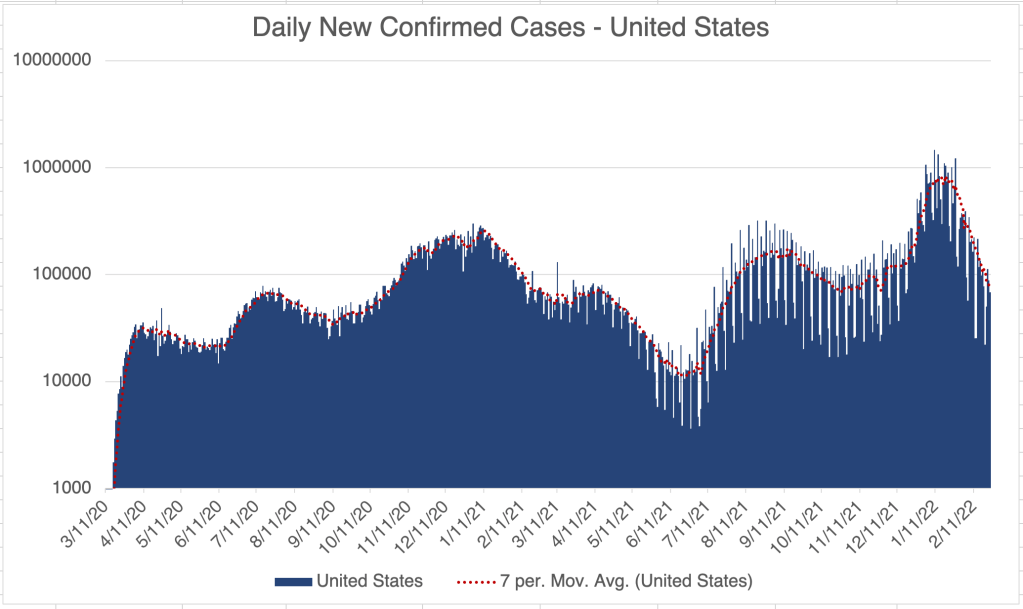
For some reason, my numbers are a little erratic for the last week for the US. This is likely because of irregular reporting by places that Johns Hopkins gets information from, so I’ll also show the US data from Worldometer.
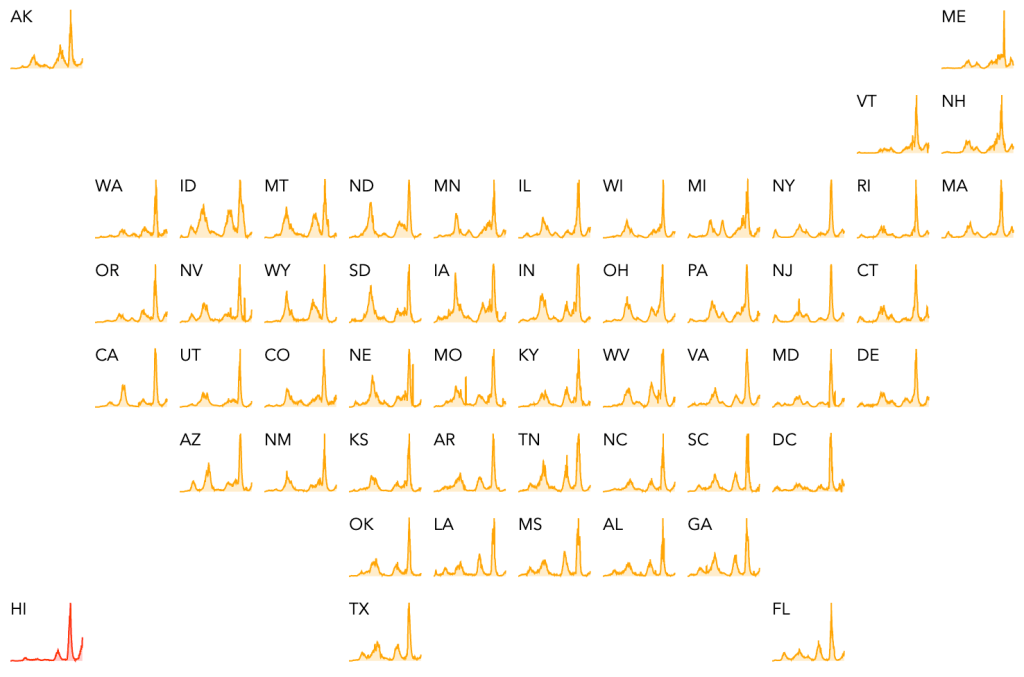
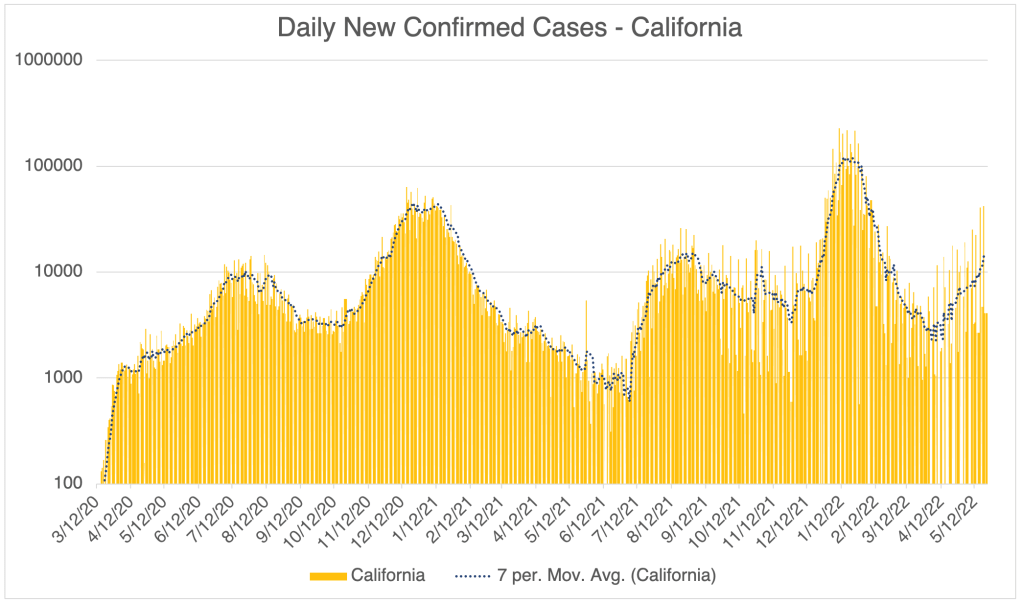
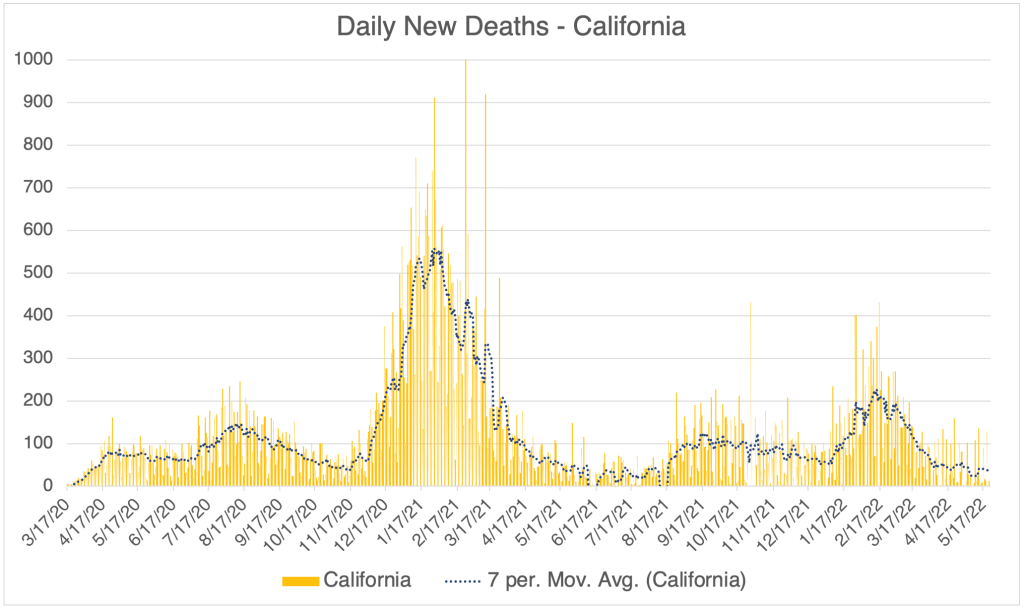
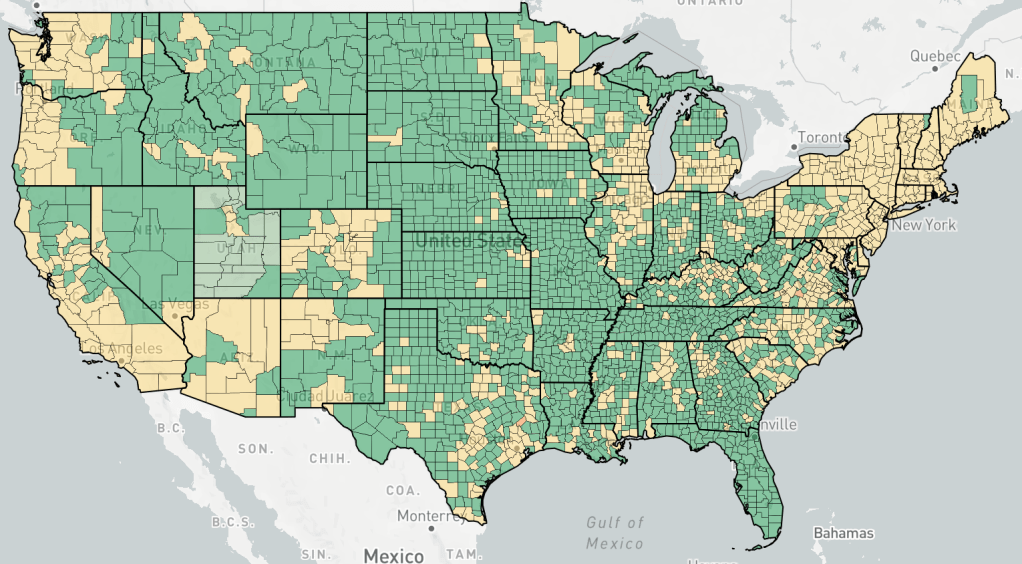
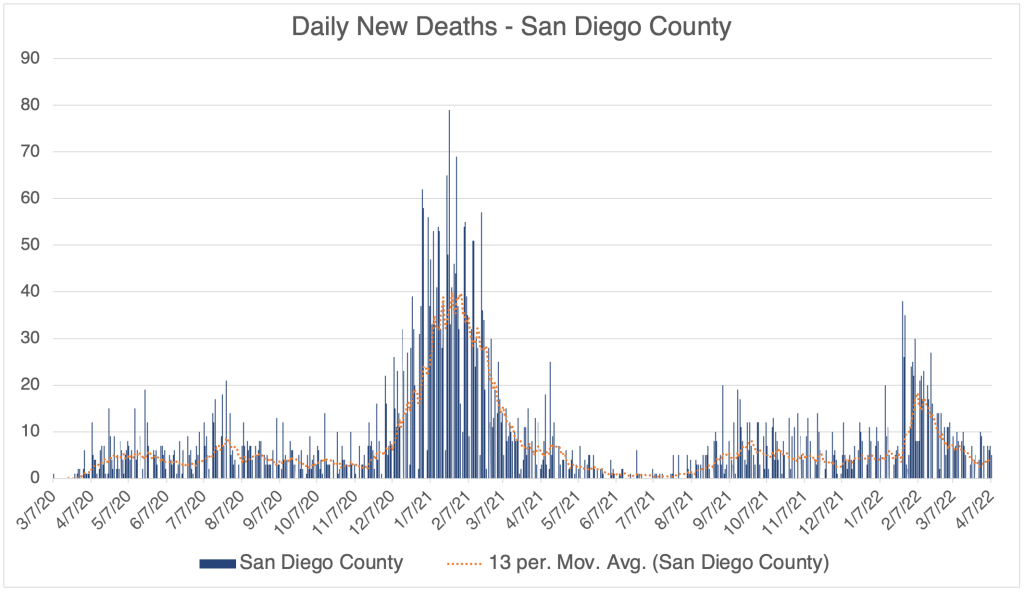
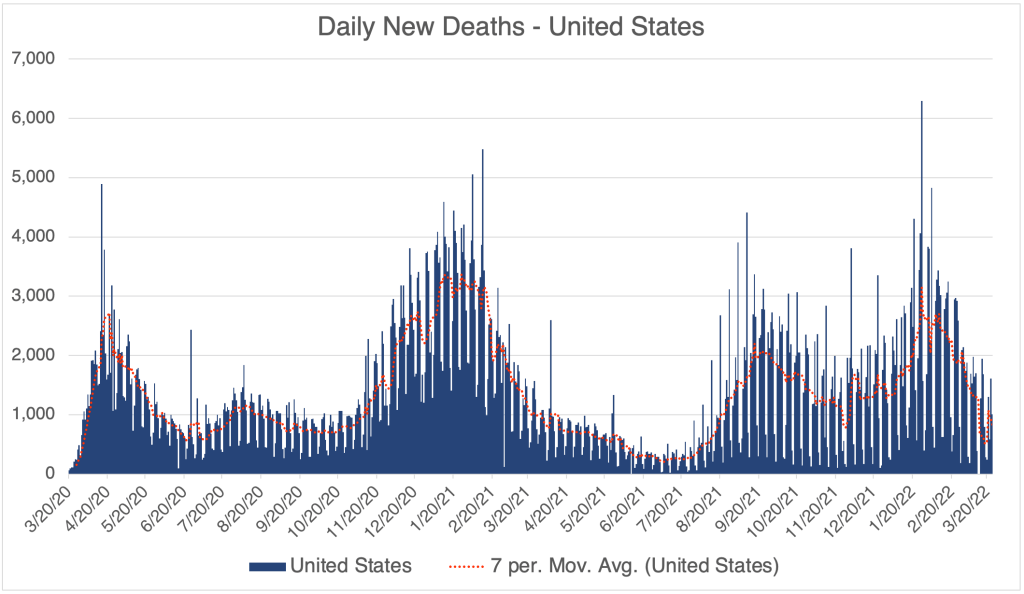
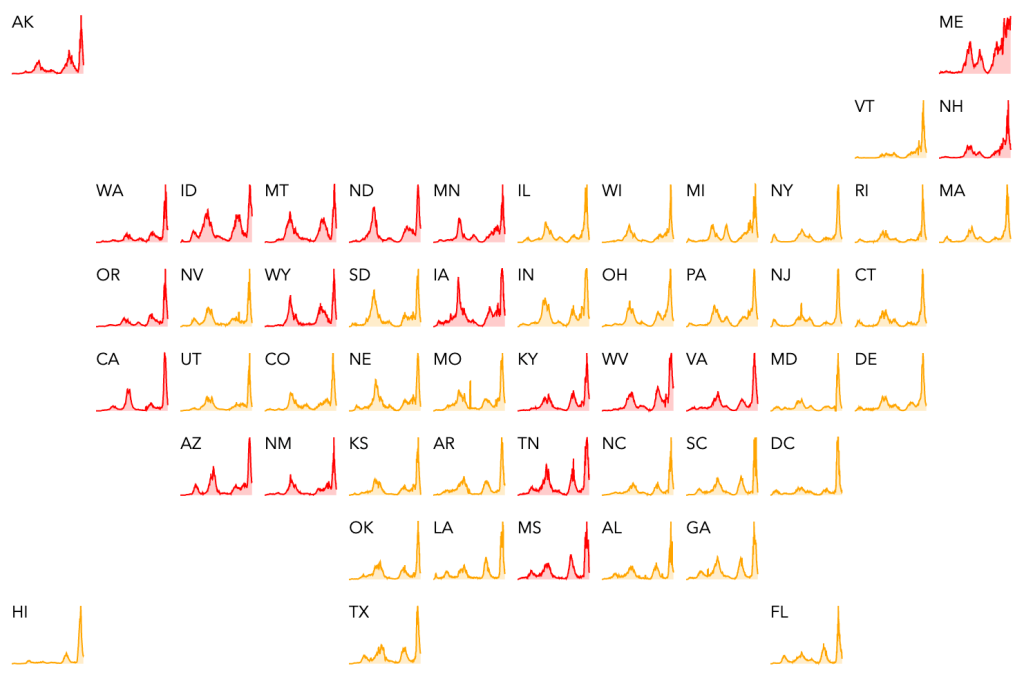
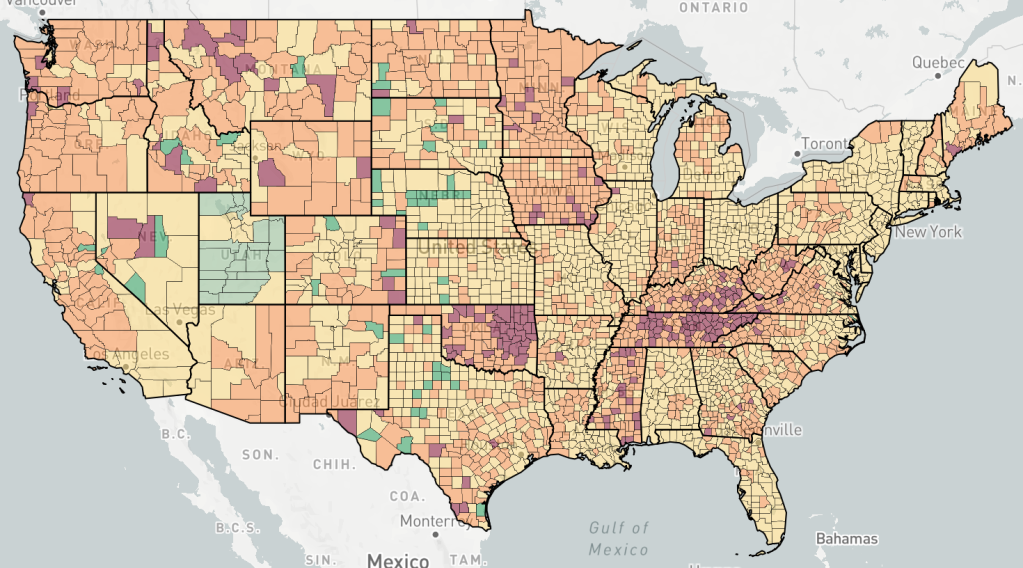
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.From Worldometer, Daily New Cases, United States.From Worldometer, Daily New Cases, United States.Endcoronavirus County Level Map, June 2nd, 2022Endcoronavirus State Level Map, June 3rd, 2022Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.From the CDC page on Variant Proportions.Hospitalizations, from the CDC website.
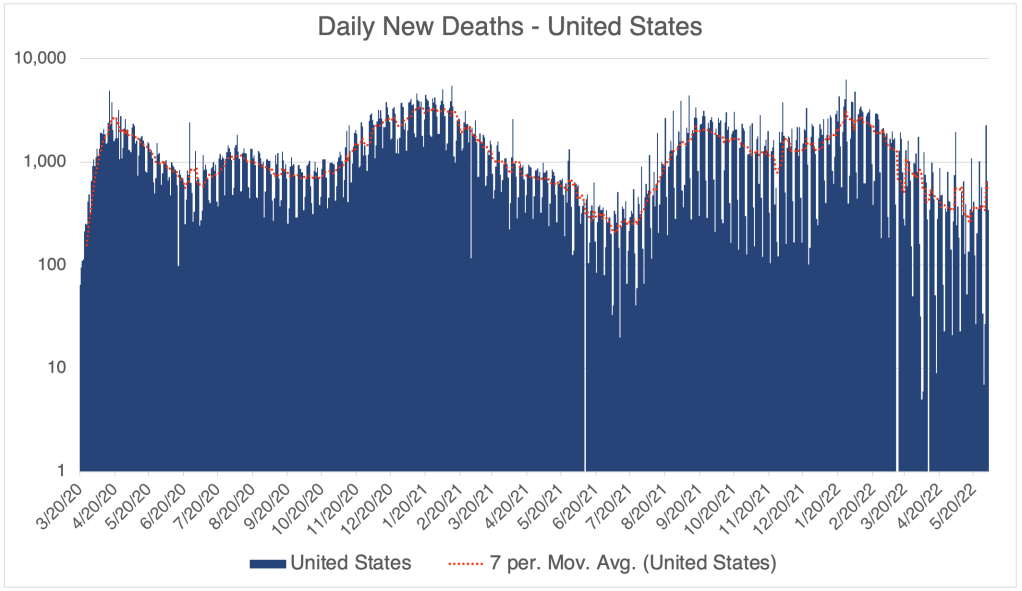
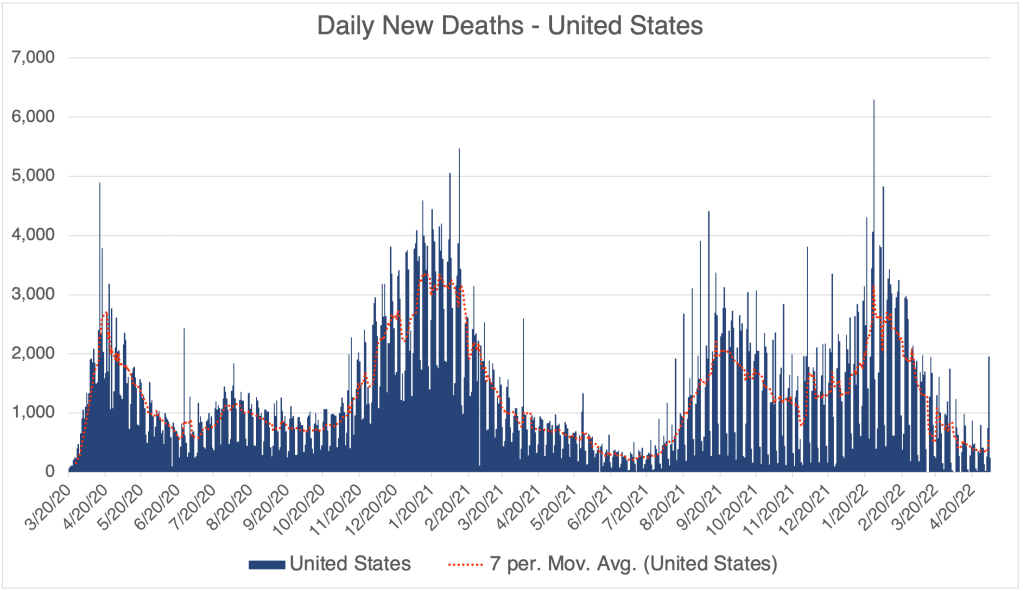
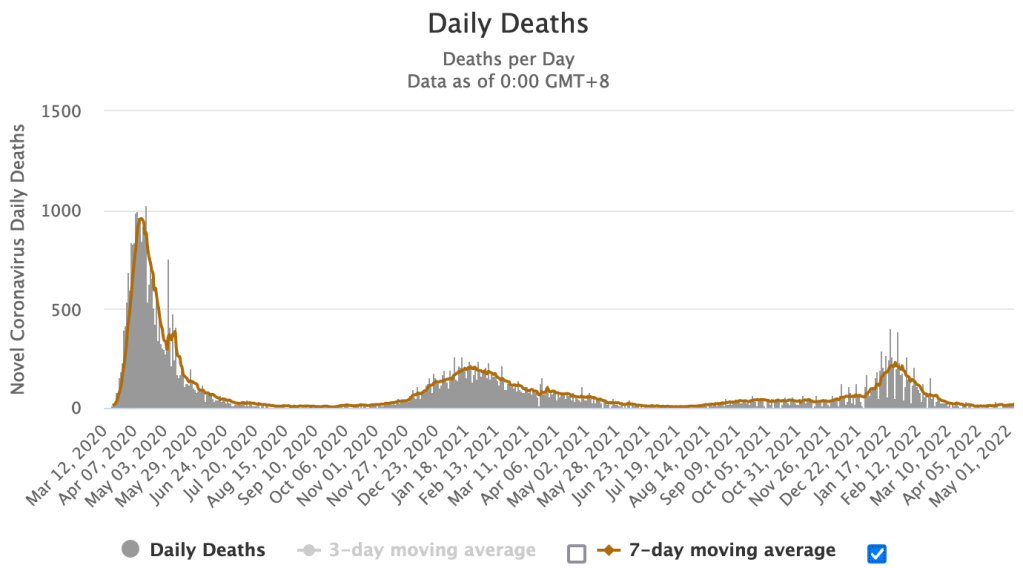
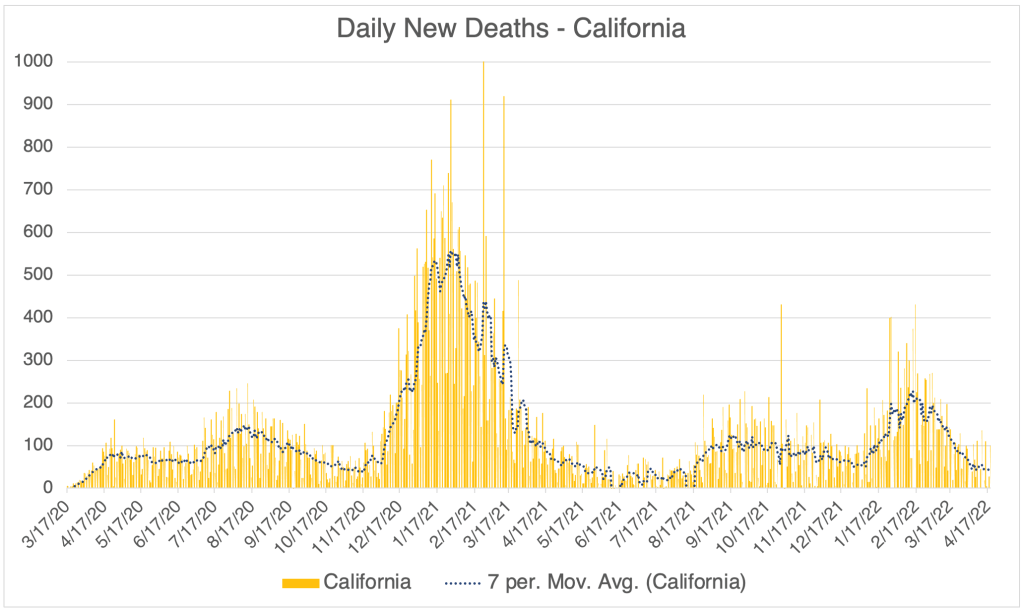
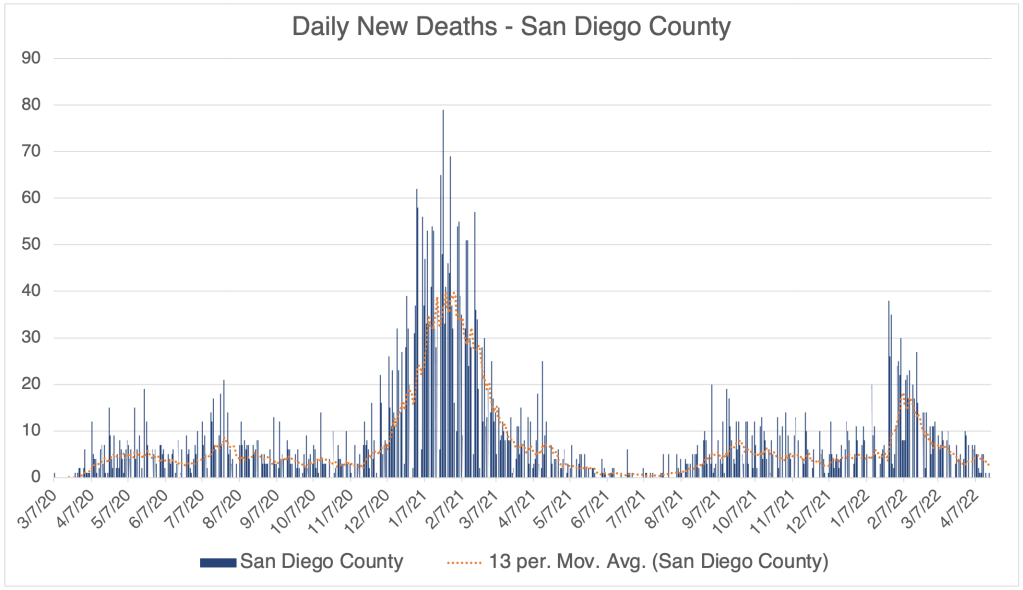
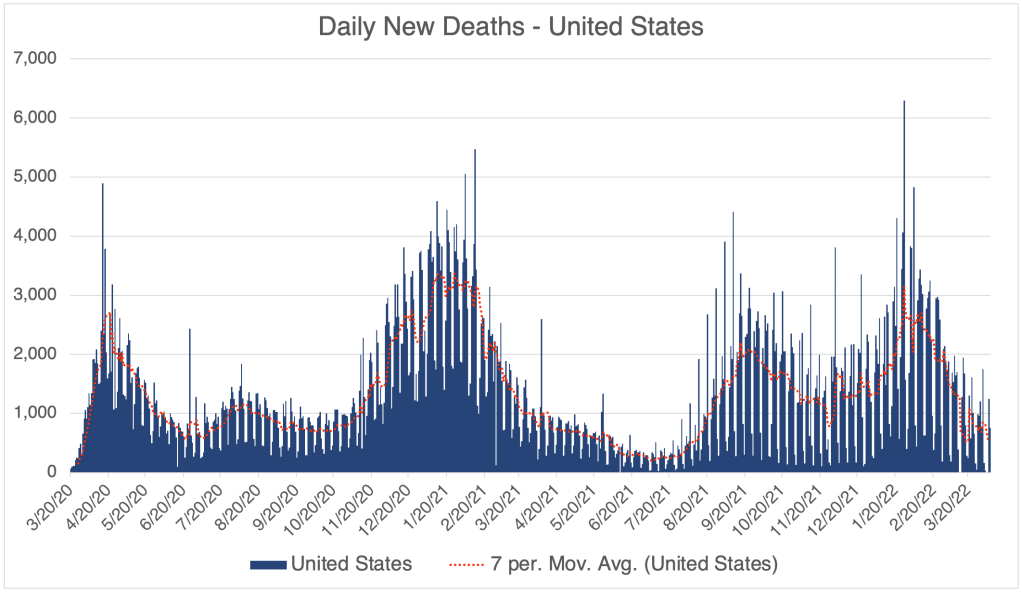
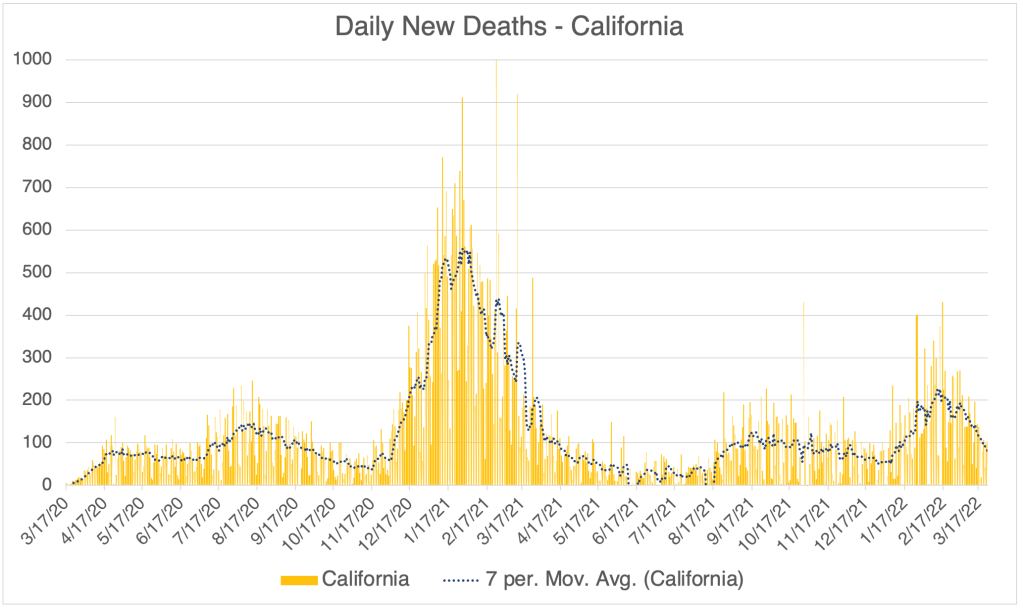
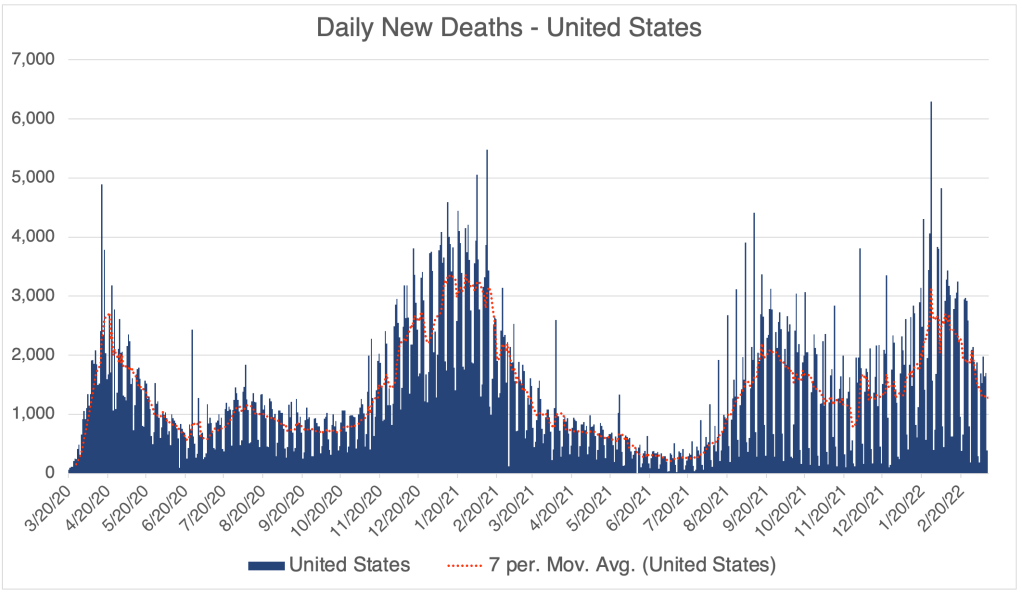
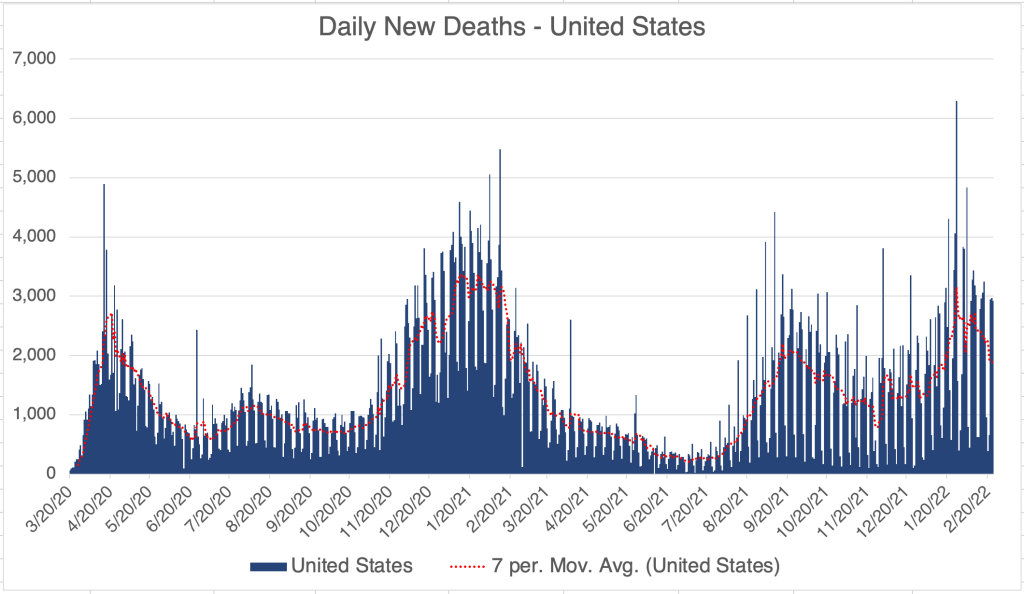
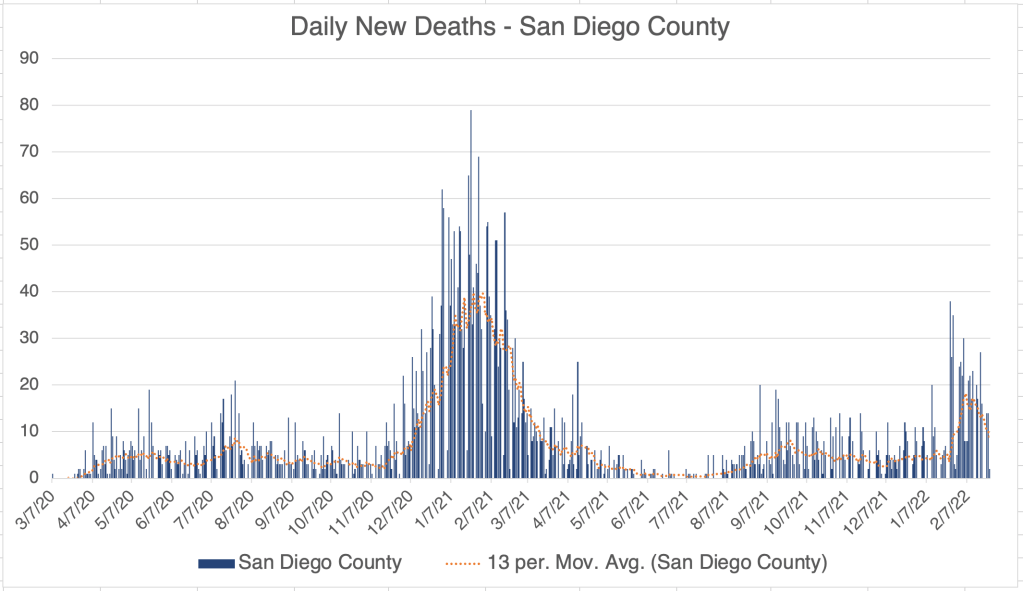
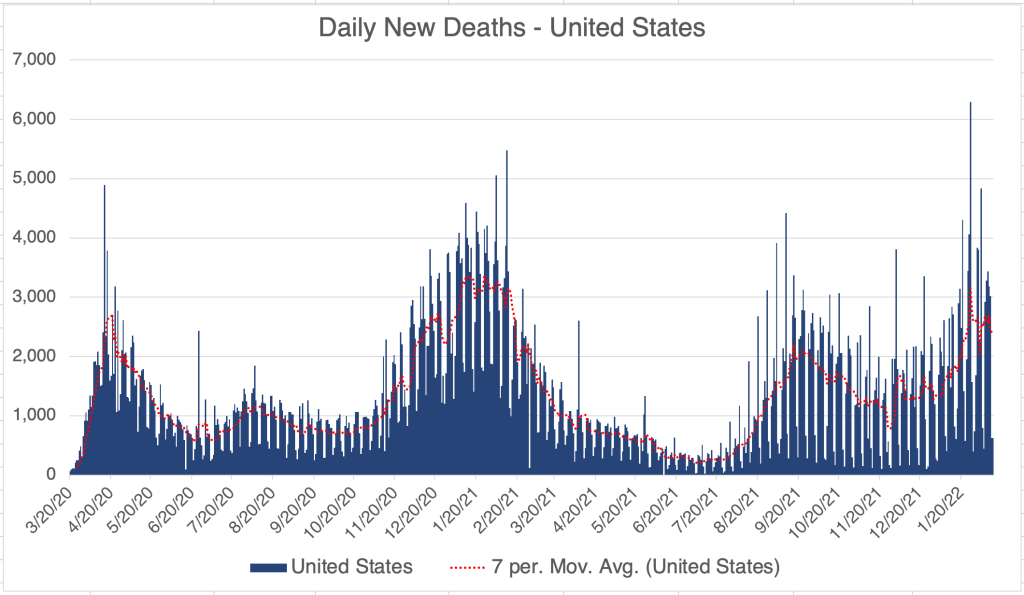
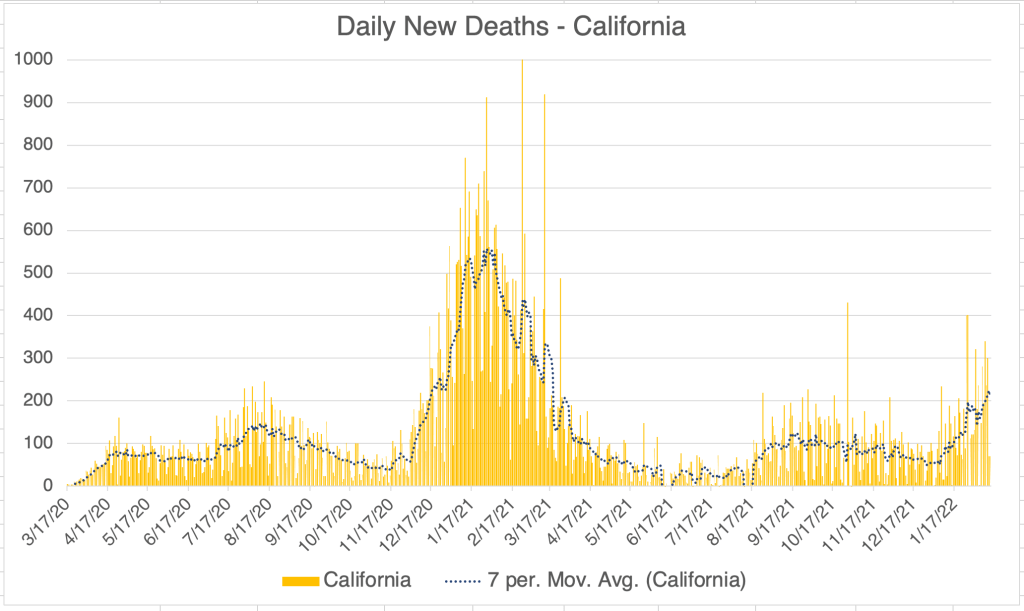
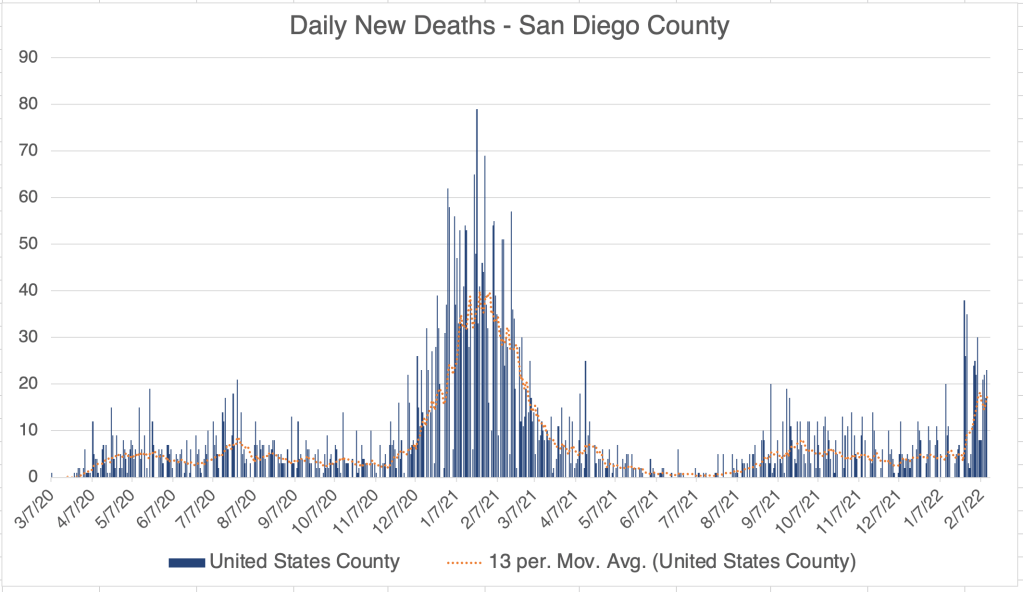
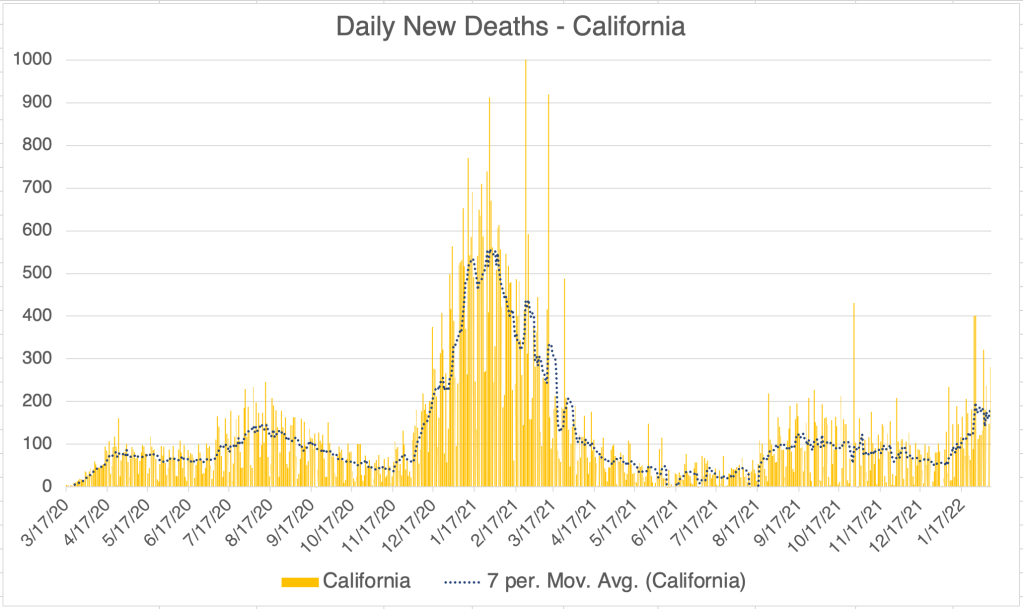
Anyway, new case numbers for all three regions are coming down now, and deaths have still not started to come up, despite us being 6 weeks into the BA.2 peak. John Campbell has also pointed out that new deaths have not tracked with new cases, so the BA.2 Omicrons seems to be less pathogenic than previous versions.
And yes, since cases are less severe and over-the-counter testing is available, infections are likely much higher than official reporting suggests.
Still not quite over: Since I had Omicron in January, and current strains are still in the Omicron family, I am not concerned about getting COVID again right now. So the Pandemic is essentially over for me, but people are still getting COVID.
I was with a buddy this week who was very fatigued and miserable, just like I was, but he didn’t have any life threatening symptoms, just like me. So just a word of encouragement for those who have COVID now or will get it in the coming weeks. You can be really miserable and not be dying! You generally only need to go to the hospital if your blood oxygen is low. Different sources have a different definition of “low”, some say below 90 and some say below 95. Feel free to chime in on this if you’re a health care worker! Get yourself a high quality pulse oximeter so you can reassure yourself if your oxygen is normal! Some medical networks also have a messaging system where you can ask your doctor COVID questions without going in.
Also, if you haven’t had COVID recently, supplement with Vitamin C, Vitamin D, and Zinc. A physician friend of mine says he has had patients who’ve had both Delta and Omicron, so “recently” means since December.
Don’t fear, but be smart! Erik
_________________________ June 5th, 2022 Post Script: Mark Foreman sent me a paper he found describing 47 cases in Denmark in which people who had been infected with Omicron BA.1 were also infected with BA.2 just a few months later. The cases were all in young, unvaccinated people who had had mild symptoms from their BA.1 infections.
Since BA.1 and BA.2 are so similar, I find this a little baffling, but my being baffled doesn’t discount the data. The data must speak for itself. One possibility suggested by the mild symptoms is that the patients had a low dose exposure to BA.1, so had mild symptoms, and perhaps only mounted a medium immune response to BA.1, allowing infection by BA.2. This is just a guess of course.
In all cases, the BA.2 infections in this group produced mild symptoms.
A very interesting paper that will perhaps give more insight into how our immune systems interact with this disease!
This is a case update. I’ll also talk briefly about new Omicron variants, BA.4 and BA.5, and also the new Monkeypox virus, and several cases of hepatitis in children.
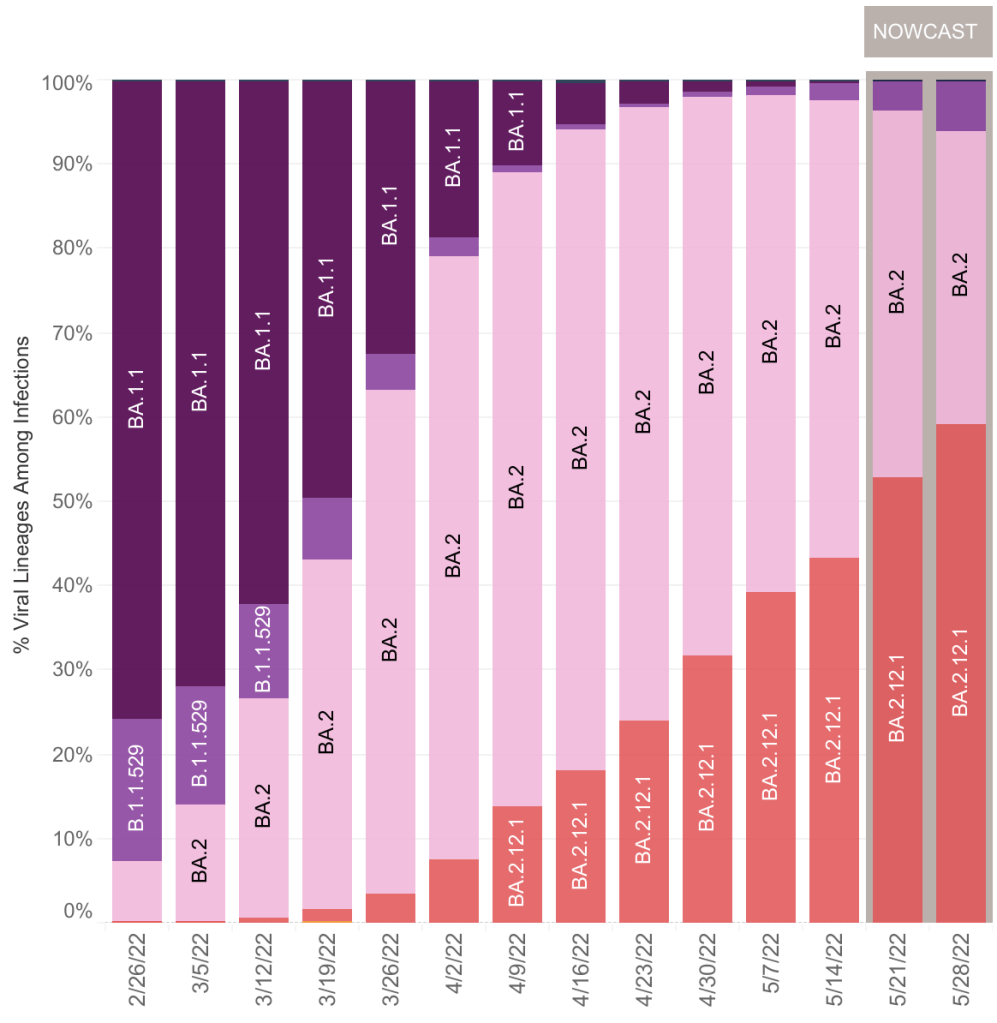
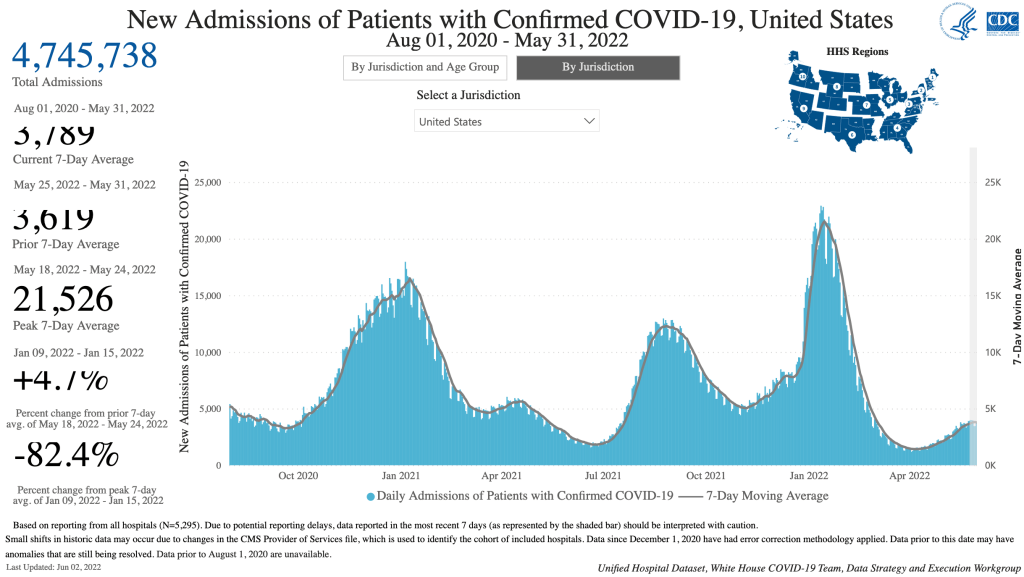
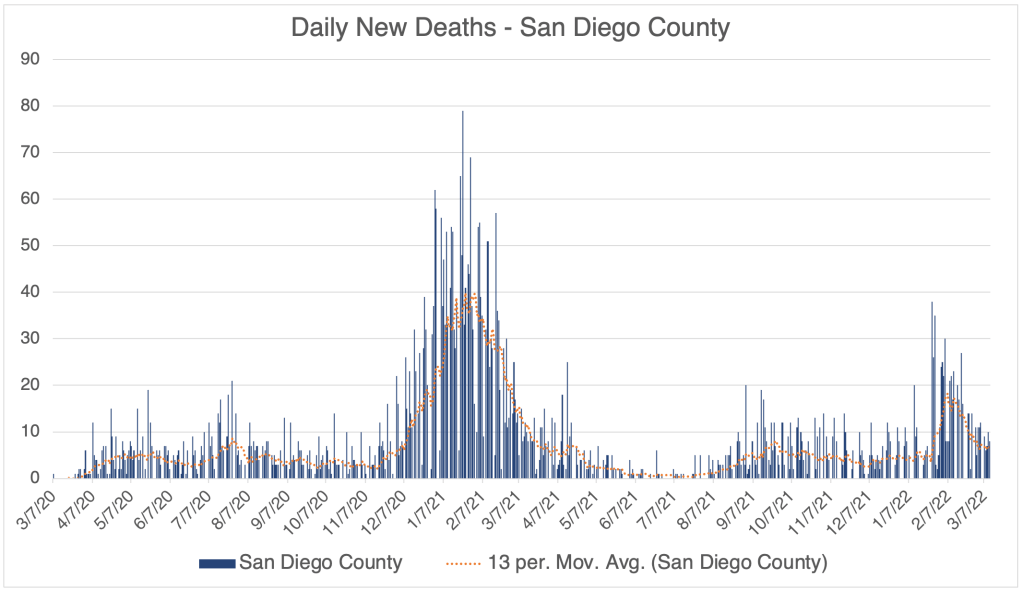
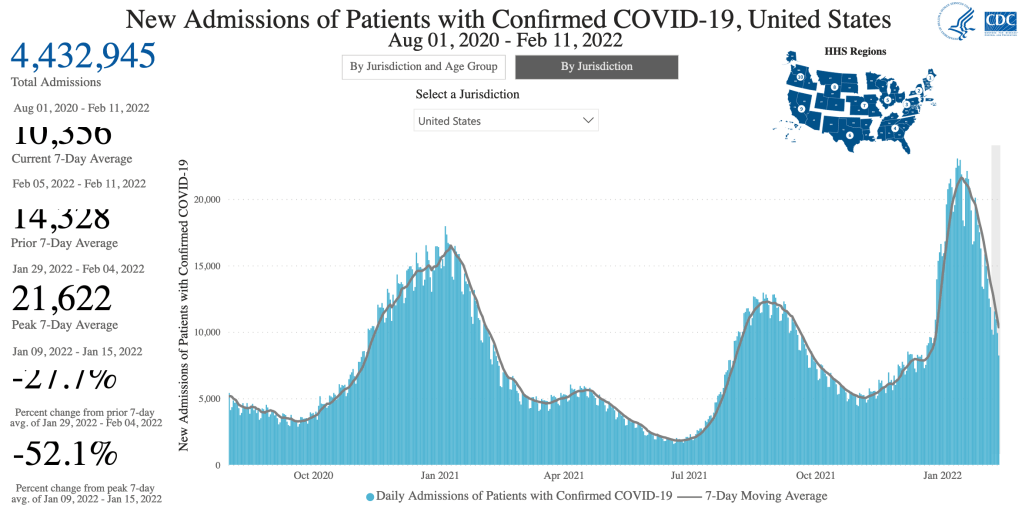
New confirmed cases are still increasing due to the new Omicron BA.2 and BA.2.12.1 variants, which are now nearly 100% of cases in the US. Hospitalizations are also up in the US. However, new daily deaths are still not rising in the US or California, with only a temporary blip in San Diego County. I have often cautioned that deaths trail cases by 2-5 weeks, but for the first Omicron wave in December and January, deaths trailed cases by just 1 week. Since we still aren’t seeing an increase in deaths after 6 weeks, this suggests that the BA.2 variants are not as deadly as even the BA.1 Omicron variants.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Hospitalizations, from the CDC website.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. San Diego County now only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
I’ll also point out that I continue to have friends who are getting COVID right now, meaning they are getting one of the BA.2 variants. While some feel bad, none are going to the hospital, and none are becoming a “confirmed case” by getting tested in a medical setting. If this is true on large scale, then we have lots of infections, maybe even most of them, that are not showing up in the “confirmed case” data.
BA.4 and BA.5: I’ve heard some news about some more new Omicron variants BA.4 and BA.5. So far, these variants have not come to the US and have not had a large impact on the pandemic.
Monkeypox virus: There have been several clusters of Monkeypox cases in Europe, and just a few cases in Canada and the US, about 120 cases in total. Monkeypox is a pox virus similar to Smallpox. It is much less much deadly than Smallpox, but can cause death. It is endemic (widespread and likely permanent) in Africa but does not usually cause serious outbreaks in non-African countries. It is only moderately infectious, spread by contact and also by respiratory droplets. It is not spread in aerosol form. Asymptomatic people do not generally transmit the disease.
Those vaccinated against smallpox will still have some immunity against monkeypox. Pox viruses do not mutate quickly.
All this to say, most infectious disease experts do NOT think that Monkeypox poses a serious health risk to most people, and that it does NOT pose a potential pandemic risk. Why am I covering this then? Because it’s in the news, and I wanted to clear up any anxiety about the virus. It will mostly likely not become a big issue in the US.
As a side note, I do NOT intend to cover new infectious diseases forever when the pandemic is over, but may occasionally cover items of special concern.
Mystery hepatitis in children: The suffix “-itis” refers to swelling or inflammation in the body. The term “hepatitis” refers to swelling or inflammation of the liver. There are several Hepatitis viruses, (A, B, C, D, and E) but these viruses are not related to each other, and having hepatitis does not necessarily mean that you have one of these viruses. It can be caused by other things.
A few weeks ago, hundreds of children in countries all over the world had sudden onset hepatitis. So far, 11 children have died and medical care was necessary for many, including liver transplants. None of the children had an infection of a Hepatitis virus.
Testing showed that many but not all patients were infected with an Adenovirus upon examination. Adenovirus infections are very common, and usually have no symptoms, so are often not addressed medically. Some adenoviruses can cause common cold like symptoms.
So far, 20 individuals tested have had a history of COVID infection, and most individuals were NOT vaccinated against COVID, so at this point, a connection to COVID or a COVID vaccine seems unlikely.
All this to say, the cause of these cases is still unknown, but many in the medical community are currently speculating that they are related to Adenovirus type 41. At this point, there is no reason for general concern about hepatitis in children, but I will certainly let you know if this changes.
If you or your child experience any of the following, especially in combination, seek medical attention immediately, at least a phone call to your doctor:
Nausea Abdominal pain Vomiting Diarrhea Jaundice (yellowing of the skin)
This is a case update. I’ll also give an update on new Omicron variants and briefly discuss a new anti-Coronavirus drug, Paxlovid.
In the US, cases continue to increase modestly, and may have peaked. This increase in cases are likely due to Omicron sub-variants BA.2 and BA.2.12.1 (more on these later). However, new deaths are still decreasing. I will caution that a rise in new deaths often trails new cases by 2-5 weeks. For the first Omicron wave, deaths followed cases by 2 weeks, and we are currently 4 weeks in to the BA.2 wave.
In California and San Diego County, cases are up modestly. Again, new deaths have not yet begun to rise.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a logarithmic format to emphasize small numbers. Starting on May 2nd, 2022, San Diego County only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from San Diego County Public Health. Graph is presented in a linear format. Starting on May 2nd, 2022, San Diego County only releases information Monday and Thursday each week. Data points shown are extrapolated using this information.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
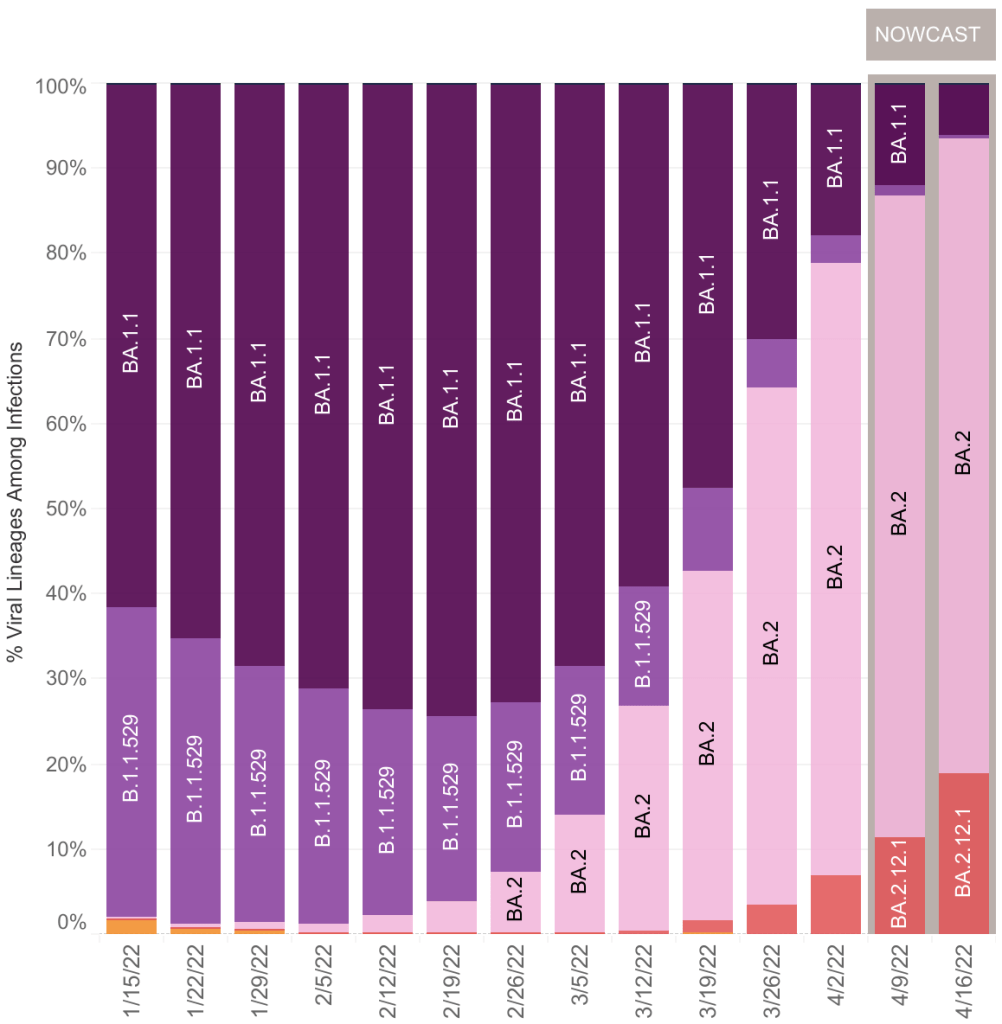
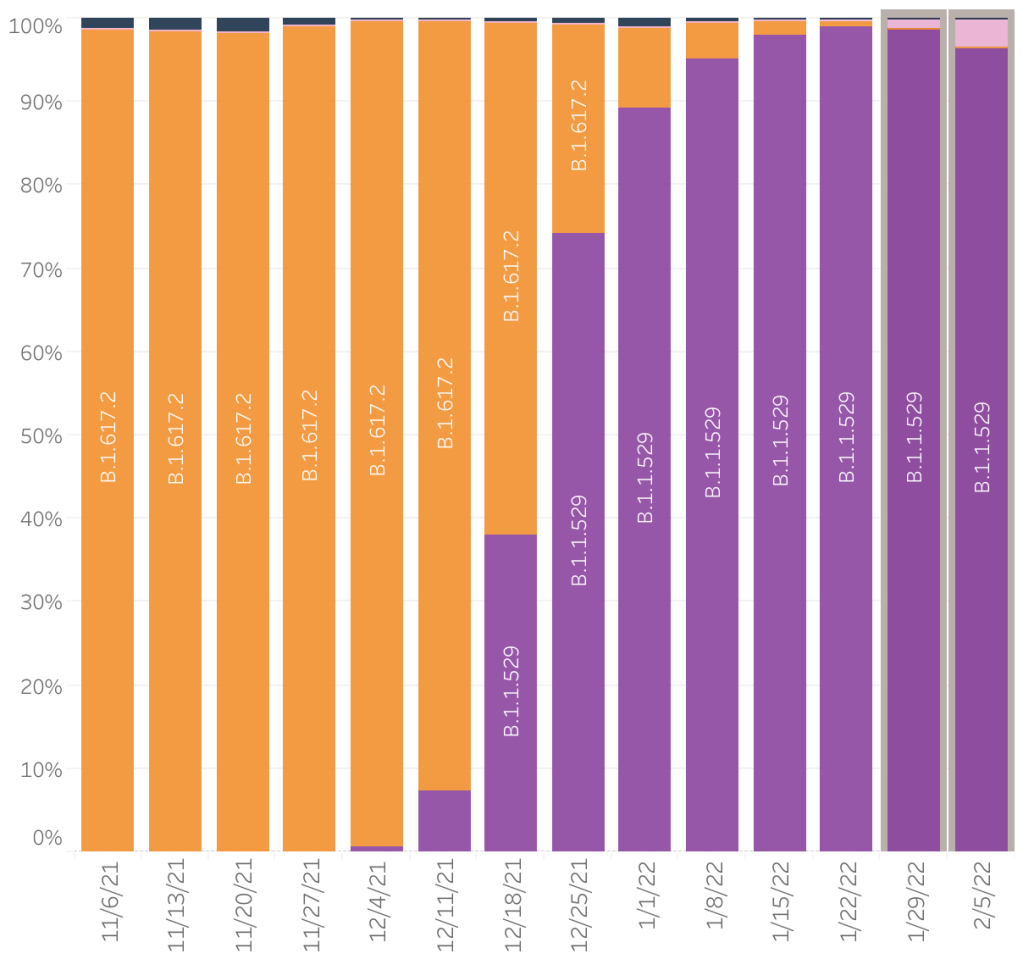
New Omicron sub-variants, BA.2 and BA.2.12.1: BA.2 has been well known for a few weeks. I’ve stated before that BA.2 is very similar to the first Omicron variants, and predicted that it will not have a large impact. A new variant BA.2.12.1 likely falls into the same category. These variants now dominate the current cases with 98% of new cases being due to one of these variants.
These variants are more infectious than the first Omicron sub-variants, but it is still unknown if they are more or less pathogenic. Viruses tend to become more infectious and less pathogenic over time.
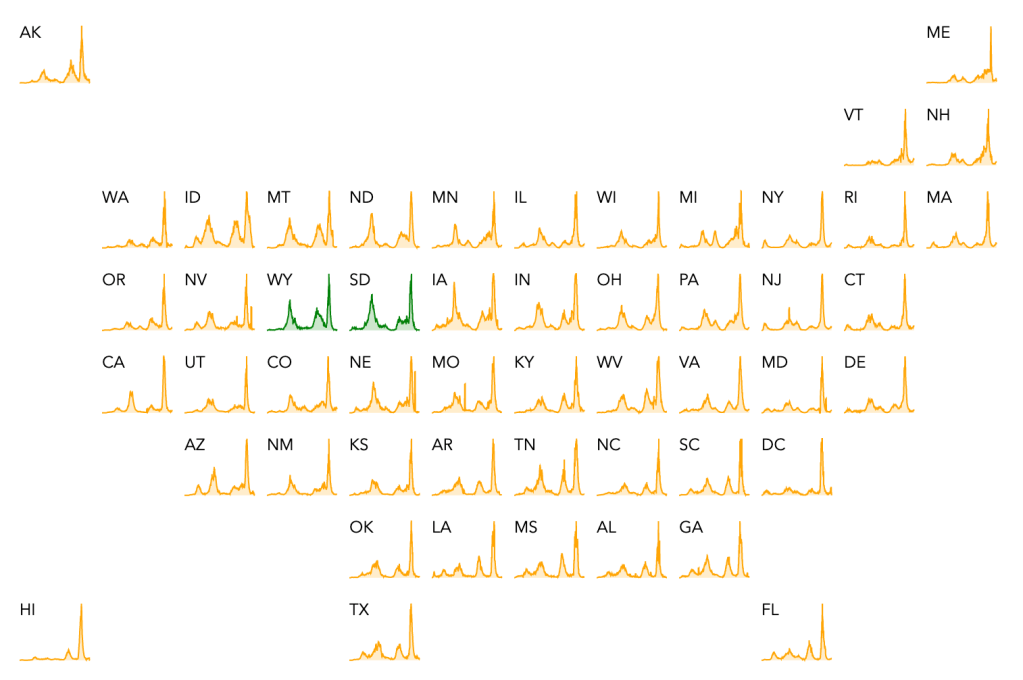
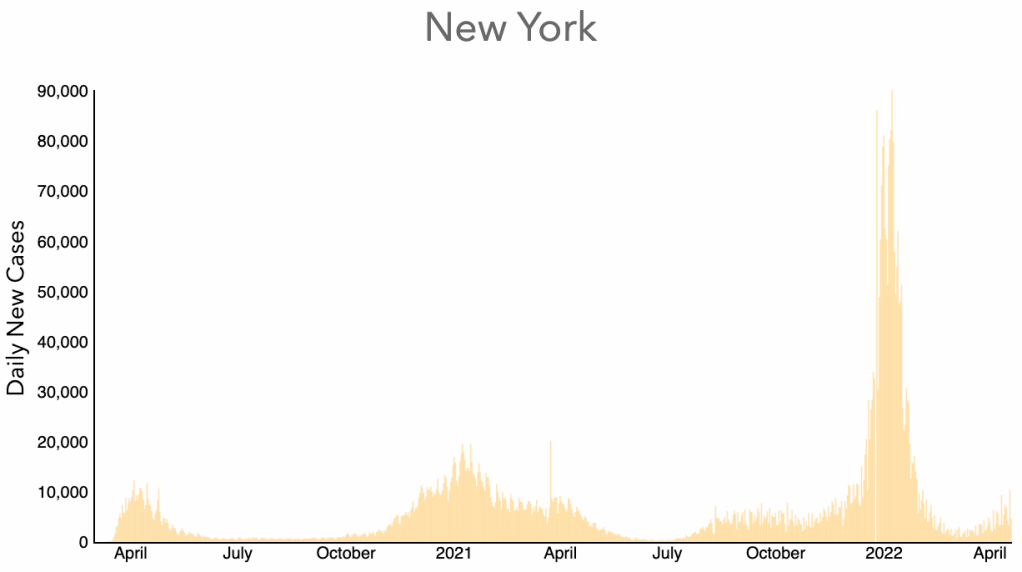
Some Eastern states like New York were the first to see modest new waves due to BA.2. New York has yet to see a significant increase in deaths.
From Worldometer, Daily New Cases, New York State.From Worldometer, Daily New Deaths, New York State.
All this to say, for now, the BA.2 and BA.2.12.1 wave still appears to be somewhat insignificant.
If you had COVID from mid-December to now, you probably had Omicron. Because BA.2 and BA.2.12.1 are very similar to Omicron, you should not be concerned about reinfection until a significantly new variant arises. Some people who had Delta have also been infected with Omicron.
Omicron sub-variants get a lot of press, much more than previous sub-variants. I’ll let you guess why that is. For now, don’t be alarmed about a new Omicron sub-variant. They will probably all fall into the “don’t stress about it” category.
The pandemic isn’t quite over. If you don’t have immunity, you may want to continue to take precautions by wearing an N95, KN95, or KF94 when indoors in public. Cloth masks or blue surgical masks will not protect you from Omicron variant SARS-2 viruses.
Paxlovid: 2 friends of mine got COVID just this week. They were both prescribed Paxlovid, a new anti-SARS medication. The drug is a protease inhibitor, which prevents viruses from maturing as they are formed inside a human cell. Protease inhibitors do not prevent infection, but they can significantly reduce viral load and improve symptoms. Both of my friends are doing well now, one feeling significantly better within just 24 hours. 2 people is a very small sample size so this should not be taken as an endorsement. I’m just pointing out that there is a new therapeutic available.
I will point out that Paxlovid is a Pfizer product. For some, this will cause concern because Pfizer has lost significant trust due to the vaccine mandates and the attending creepiness.
Don’t fear, but be smart, Erik
______________________________________________ Important Update on Paxlovid, from July 2nd, 2022:
This is a post about Tony Fauci’s time with COVID and the drug Paxlovid, which I have discussed in the past.
However, something else very interesting happened. Dr. Fauci took Paxlovid, which I’ve discussed briefly before, and became COVID negative. But after his 5 day course, he became positive again with worse symptoms. This means that a standard 5 day course of Paxlovid will not necessarily reduce your viral load to zero, and patients may experience “Paxlovid rebound”. Fauci even claims that this kind of rebound with Paxlovid is starting to be seen as “typical” as more patients use it.
With so many rebound cases, it’s likely that 5 days is not adequate to eliminate all viruses from the system, allowing rebound. However, Paxlovid does have side-effects, so don’t take it for more than 5 days without consulting your doctor! Hospitals are now only prescribing Paxlovid to high risk patients.
Whenever taking anti-viral or anti-bacterial medications, always take the full course of treatment. If any virus or bacteria survive treatment, they may give rise to a more resistant strain. Don’t just stop your treatment when you feel better. I take anti-biotics as a last report, but when I do, I take the full course. I even made a doctor give me the full 10 day course when she just wanted to give me a half course!
Just to repeat the point on the vaccines, I still hear ads on the radio encouraging vaccination. At this point, the vaccines are really not doing anything against the current COVID variants. There is really no benefit to getting a vaccine or a booster. If you haven’t had COVID yet, I would simply recommend preventative measures. Wear an N95, KN95, or KF94 mask when indoors in public. Cloth and surgical masks will not prevent infection.
This is a case update. I’ll also have a comment about the recent end of the mask mandate on airplanes.
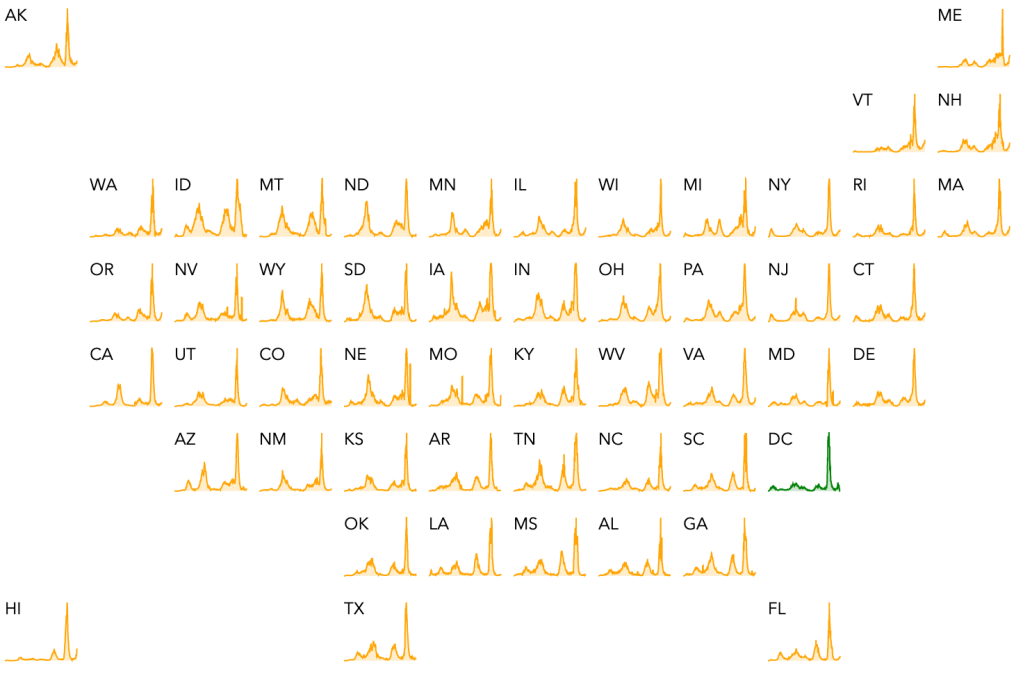
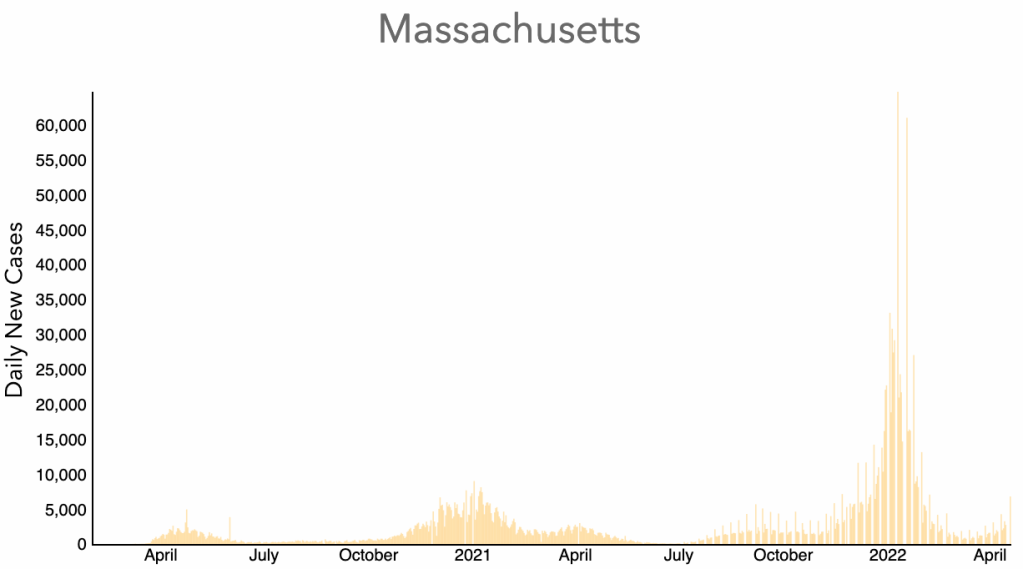
The BA.2 variant is now causing a very modest uptick in cases in the US. 93.4% of cases in the US are now caused by BA.2, some caused by a new subvariant called BA.12.1. Most of the uptick in cases in the US is driven by a rise in cases in Northeast states like New York, New Jersey, Massachusetts and Vermont. Cases remain flat in the rest of the country.
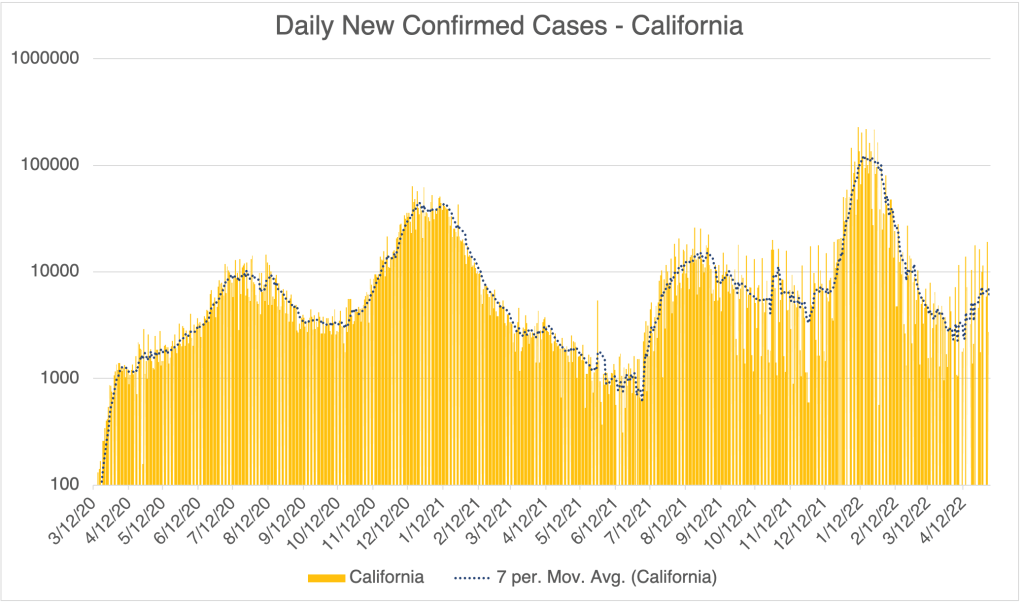
In California, we may be seeing a rise in cases, but reporting has become sporadic, so it’s hard to say for sure. Some days show zero new cases.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.
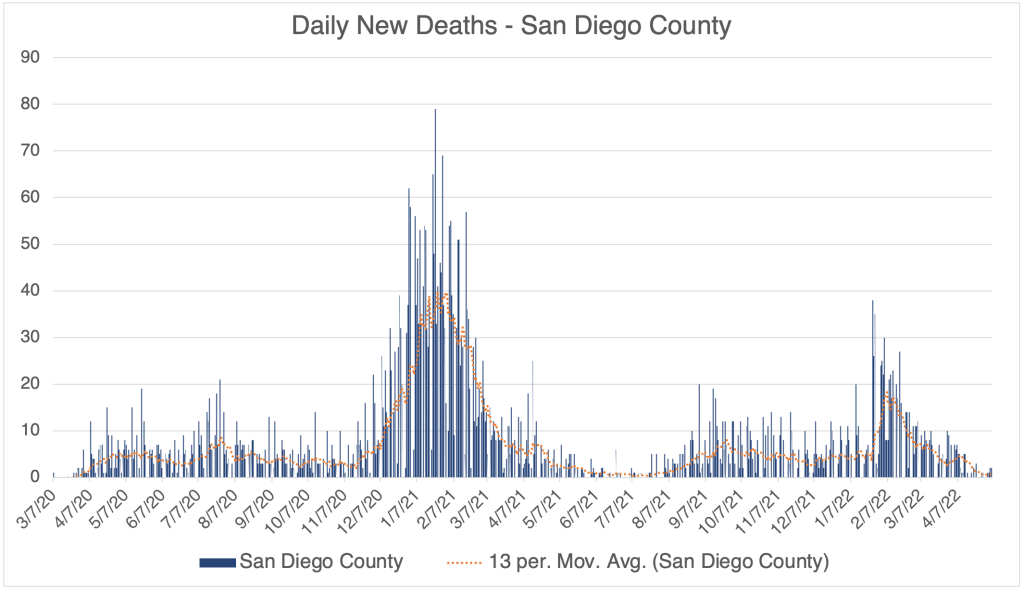
Cases are dropping in San Diego County, and are lower than they were between the Delta and Omicron waves.
Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.
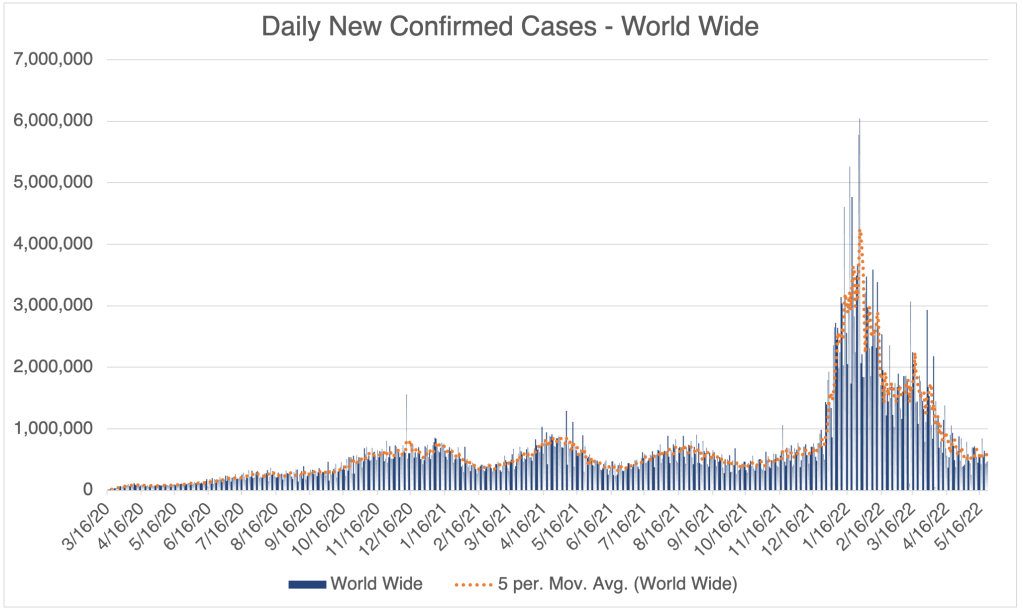
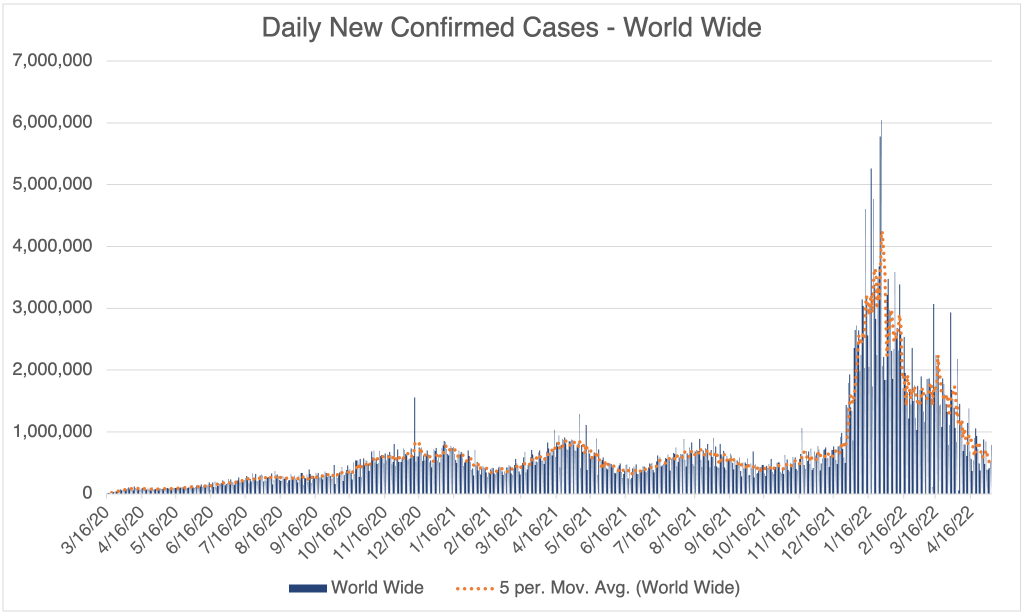
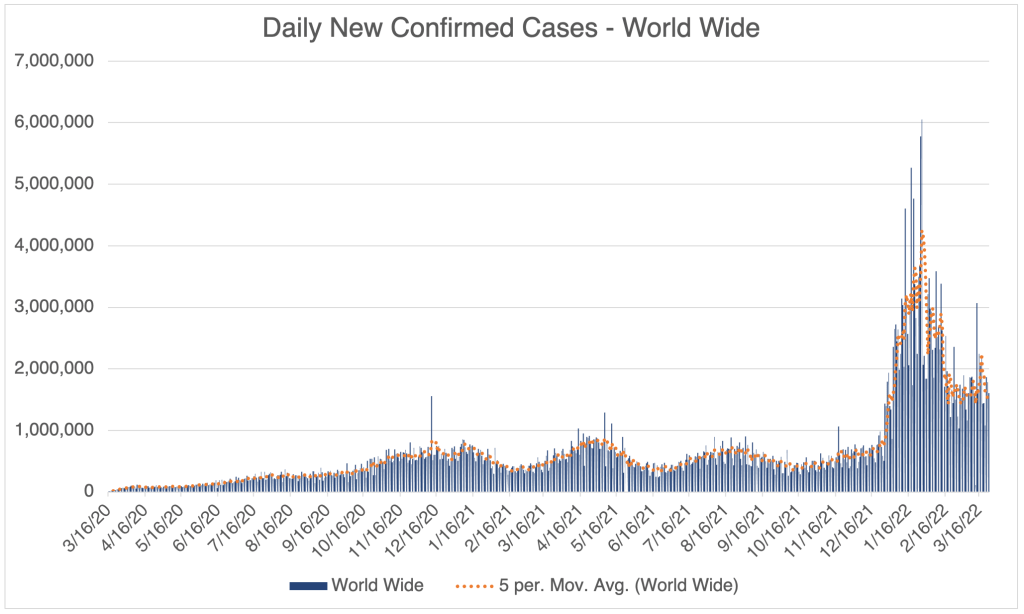
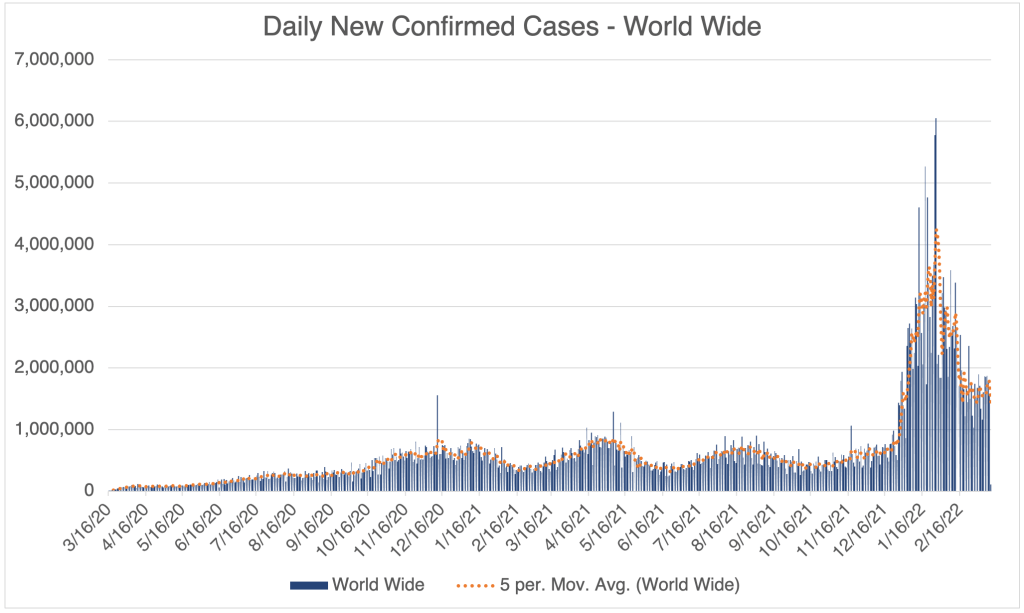
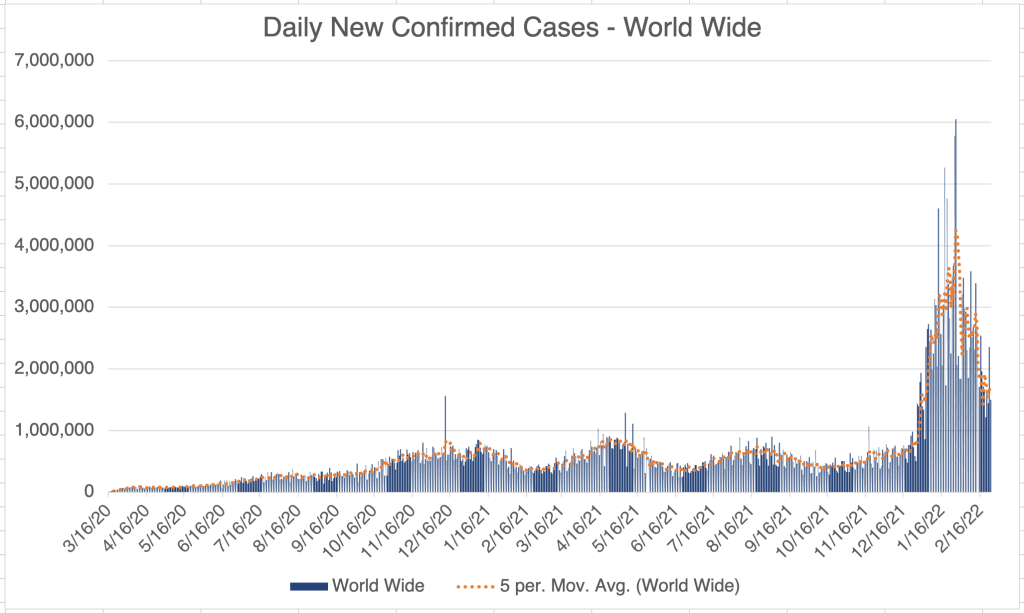
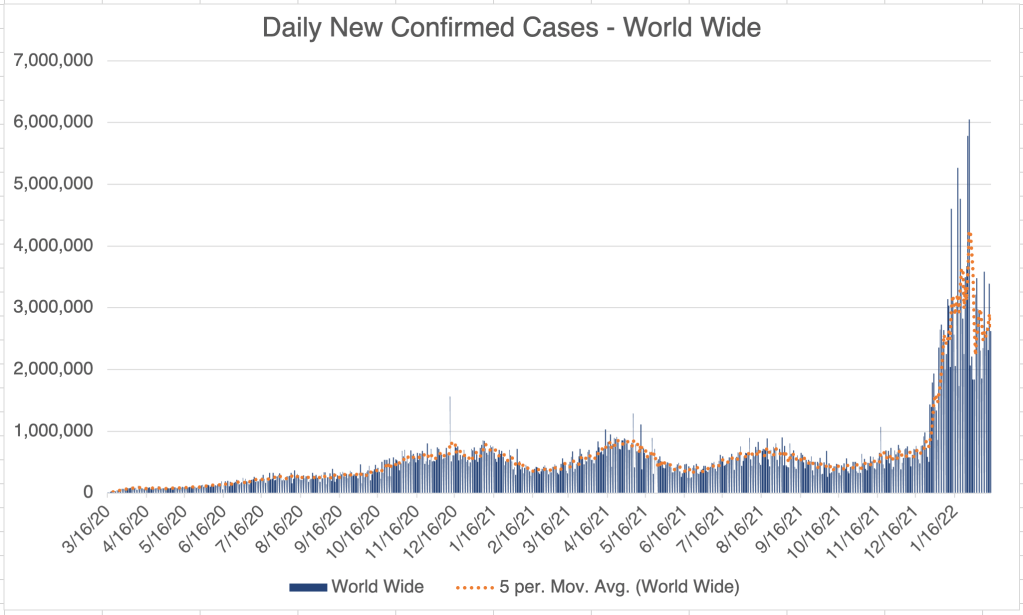
World wide, cases are dropping quickly, reflecting the drop in Omicron cases in many countries.
A friend of mine pointed out to me today that more COVID is being detected in waste water, suggesting another upcoming wave. The only authoritative looking story I’ve seen on this is out of date, from mid-March, so I don’t know how much of an impact this will have.
Mask mandate ends on planes: On Monday, a federal judge struck down the mask mandate for airplanes and other transportation. The judge ruled that the mandate exceeded the CDC’s authority under the Public Health Services Act. Within hours, the news was announced to cheers on aircraft across the country. I’m sure flight attendants are happy to have fewer arguments with passengers!
I was actually all for the mask mandate for most of the pandemic because I traveled a lot and it was kind of alarming to be on a full plane during COVID. I did find it troubling, however, that the mandates allowed nearly useless masks like the blue surgical masks, and did not require the much more effective N95s, KN95s, and KF94s. Why require masks if you aren’t going to require useful masks?
In my last several trips, just in the last few weeks, I went into restaurants, hotel lobbies, stores, gas stations, and everywhere else. The only places still requiring masks were airports, airplanes, and some laboratories. This is especially ironic since the air on an airplane is HEPA filtered and is some of the safest air you will encounter in your life.
Omicron is the last gasp of the pandemic, and cases are now very low. Some estimate that 90% of the American population now has vaccine mediated or natural immunity. I am now in favor of ending the mask mandate on airplanes. If you need to travel by air, haven’t had COVID yet, and are concerned about getting COVID on the plane, I strongly encourage you to wear an N95, KN95, or KF94 while you travel. Don’t bother with a cloth mask or blue surgical mask.
Also, as I’ve stated before, studies now show that vaccine effectiveness drops after 3 months. Also, those with multiple vaccinations, more than a few months old, are now 3x more likely to get an Omicron infection than those who haven’t been vaccinated. For details, see my March 25th post. This is because of Antibody Dependent Enhancement. So if you’re in a high risk category and were vaccinated more than 3 months ago, consider getting a booster. Consult your doctor when making medical decisions.
This is a case update. I’ll also talk about a report from Kim Iverson from The Hill regarding finding in the trove of documents release by Pfizer in March and April.
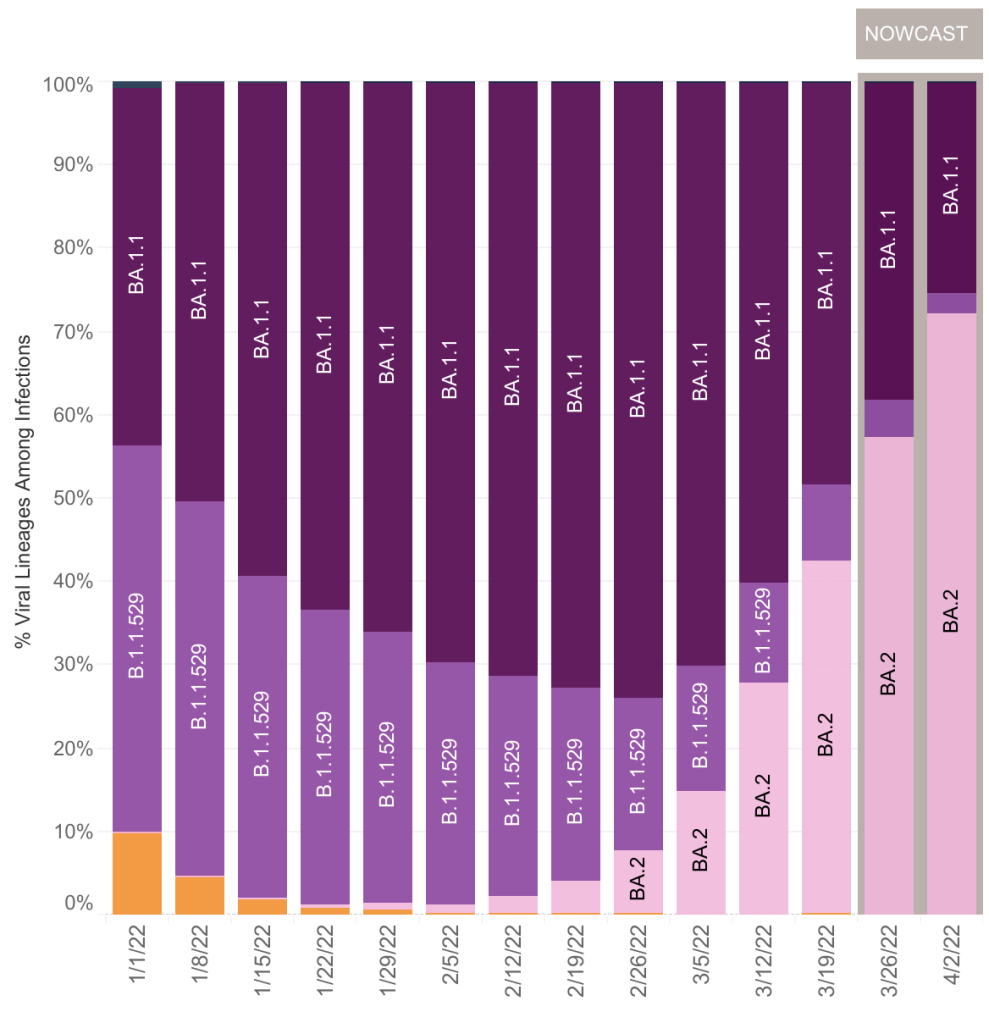
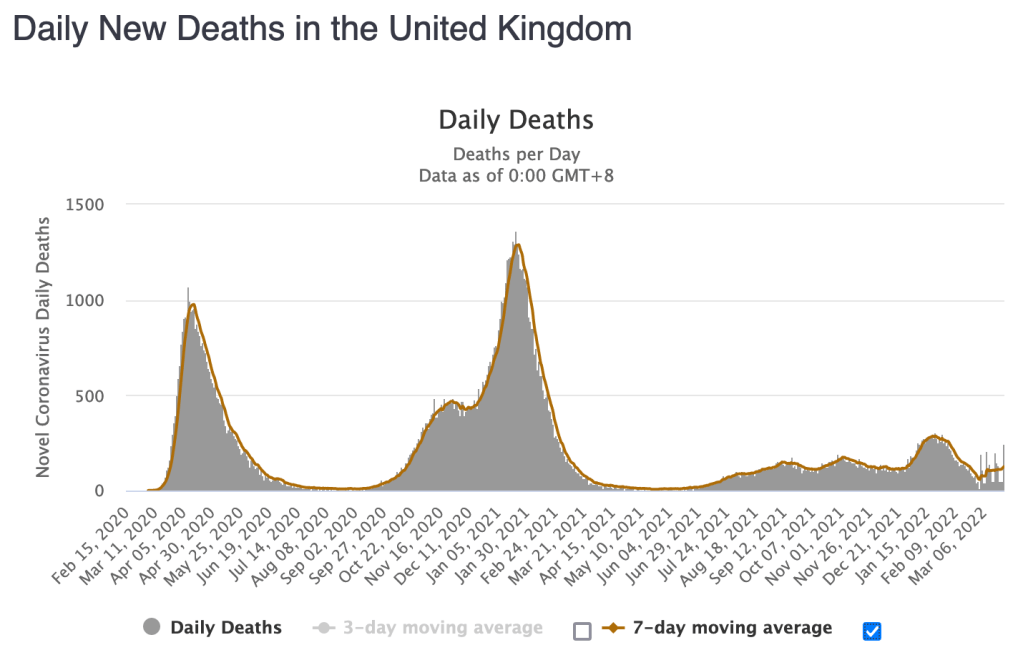
Cases are currently flat in the US. During the Omicron wave in December and January, the US lagged behind cases in the UK by 2 weeks. While the Omicron subvariant BA.2 produced a wave in the UK, it has not yet produced a wave in the US, despite it being 5 weeks since the BA.2 wave started in the UK. I’m going to go out on a limb and say that the slowing of the decrease of cases in the US is all we are going to see of the BA.2 wave in the US. I’ll let you know if this changes. BA.2 cases now constitute 72% of cases in the US.
Cases continue to go down in California and San Diego County.
Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from Johns Hopkins University COVID site. Graph is presented in a linear format.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a logarithmic format to emphasize small numbers. Note that each number on the left is 10x higher than the one below it.Graph is by me, from data collected from San Diego County Public Health. See also regularly updated slides from SD County. Graph is presented in a linear format.
XE variant: Just a few days ago, news emerged of a new COVID variant called XE in the UK. The variant is a hybrid of Omicron variants BA.1 and BA.2 and is more transmissible than BA.1. Since XE is very similar to other Omicron variants, I don’t expect it to cause a large wave of cases in the US.
Pfizer Document Analysis from Kim Iverson:Kim Iverson of The Hill released a video claiming that newly released documents from Pfizer confirm what many knew already. The shocking claim is that Pfizer has known the following for a long time:
Natural immunity is as effective as vaccine mediated immunity.
The rate of adverse events is at least 10/100,000 (33,000 for the US population). It’s unclear from Iverson if this is just for Myocarditis or for all adverse events.
It is unknown if the reproductive systems of women are impacted by vaccination. This contradicts public claims that vaccination does not affect reproduction.
A more severe case of COVID triggered by Antibody Dependent Enhancement could not be ruled out. The Lewnard et al paper a surveillance report from the UK have confirmed that higher Omicron infection rates in vaccinated people are likely due to ADE. As far as I’ve seen so far, ADE has not lead to more severe cases.
The documents were obtained because of a Freedom of Information Act (FOIA) lawsuit which required the FDA to produce the documents. Yes, this means that the FDA has had this information and did not disclose these conclusions to the public, instead often releasing information which contradicted these conclusions.
There will continue to be more document releases every month until the end of the year. There will likely be more bombshells, but most of the releases will simply confirm what people have suspected for months but couldn’t prove. I will discuss the most interesting, but not all of these releases.
If you have risk factors like obesity, age, or respiratory problems, you should consider getting a booster. Also, as I said last week, since vaccine effectiveness is substantially reduced after 3 months, those who have been vaccinated with risk factors will need to get a booster every 3-6 months. Try and find a provider who will aspirate before injection! There is no medical reason for someone who has had Omicron or Delta variants to get vaccinated or a booster. Talk to your doctor when making medical decisions.
I am posting about every 2 weeks now instead of every week. I’ll likely post even less unless interesting news comes out.
This is a brief case update. I’ll also make some more comments on BA.2 related waves in Europe, a new paper suggesting that vaccine mRNA persists in the lymph nodes. Also, new evidence from the UK suggests that vaccines lose potency after 6 months and certain vaccinated individuals are more likely to be infected than unvaccinated people.
Cases continue to go down in the US, although the rate of decrease is slowing. As you’ll read below, some suspect that an Omicron variant, BA.2, may cause cases to rise in the US.
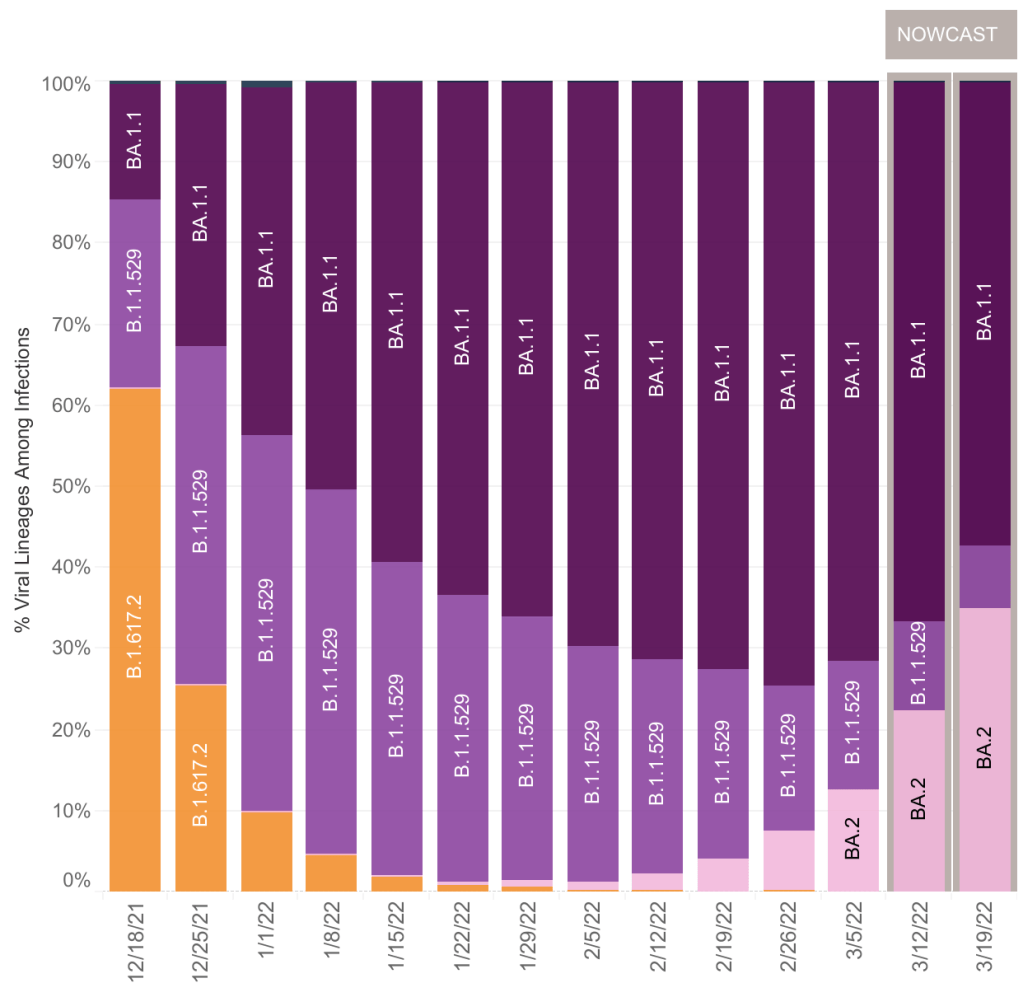
More on BA.2: I have commented on BA.2 before. This variant is a version of the Omicron variant, which is slightly more infectious than Omicron itself. It continues to follow the general trend of new variants being more infectious than older ones. Like the original Omicron, equal portions of B.1.1.529 and BA.1.1, BA.2 has a low fatality rate as compared to previous versions, including Delta.
I originally held that BA.2 is not particularly interesting because of its similarity to the first Omicron strains. This still may be true, but some countries like the UK and the Netherlands have seen significant new peaks after BA.2 became prominent. BA.2 is likely contributing to rising cases globally.
Right now in the US, BA.2 is increasing in prevalence, and is currently 1/3 of SARS-2 found in the US. It’s similarity to previous Omicron versions means that it is displacing B.1.1.529 and BA.1.1, just like Omicron displaced Delta before it. We now have 0% Delta in the US.
Does BA.2 significantly change the picture? I still say no, since the fatality rate with BA.2 is still very low, perhaps even lower than with other Omicrons. We may or may not see a significant BA.2 wave, depending on how many Americans already have resistance to BA.2. If you had Delta or Omicron, you almost certainly won’t get BA.2. Vaccination is only partially effective against Omicron variants.
Most people in my area, northern San Diego County, are basically going back to normal. This is warranted for most. If you have risk factors like age, obesity, or respiratory issues, you will want to remain vigilant and consider a booster. I do not recommend a booster for those without risk factors, and certainly not for those with natural immunity. Talk to your doctor when making medical decisions.
mRNA and Spike Protein Persist in Lymph System for up to 8 weeks: The Journal Cell just published a paper (Röltgen et al) which argues that mRNA and spike protein are present in vaccinated individuals for up to 8 weeks after vaccination. Cell is the third most highly respected journal in cell and molecular biology.
The cells in your body are surrounded by a fluid called “interstitial fluid”. This fluid carries nutrients from nearby blood vessels to your cells, and also carries waste back to the blood vessels. The lymph system is a one-way circulatory system that carries excess interstitial fluid from the extremities of your body back to veins near your arm pits. On the way, they pass through the lymph nodes, a biological filter and part of your immune system that checks for invading particles.
The Röltgen et al paper suggests that vaccine mRNAs from the interstitial fluid collect in the lymph nodes and can persist there for many weeks. They continue to produce spike protein during this time. Remember that vaccines are intended to be given in an intra-muscular manner, meaning that they are intended to be injected to a muscle and stay there. This paper shows that they are able to migrate to the lymph nodes.
The paper does not discuss the medical importance for this in terms of adverse events. Given the relative rarity of adverse events, I would guess that the presence of vaccine mRNA does not produce adverse events, and that these events are caused by vaccine injection into a vein. Again, the data is not conclusive on this, so this is just my guess at this point.
mRNA technology note: At this point, I have no evidence to suggest that the problem with the new vaccines is the mRNA technology. In my estimation, the likely reason the new vaccines lead to adverse events is that they produce the SARS-2 Spike protein which likely causes inflammation throughout the body. This may only be in vaccine recipients who receive a vaccination in a vein rather than an intra-muscular injection. If you choose to get a vaccination or booster, ask the health care provider to aspirate before injection.
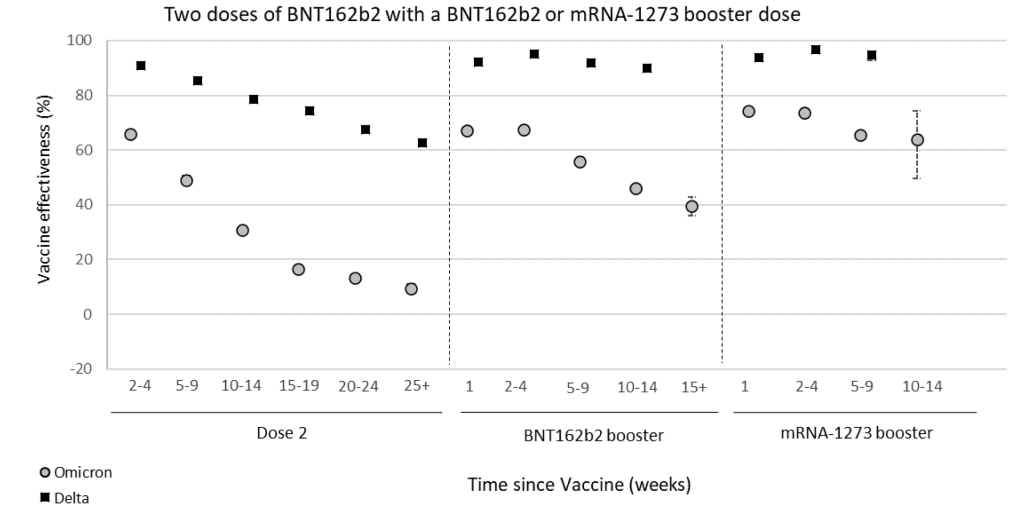
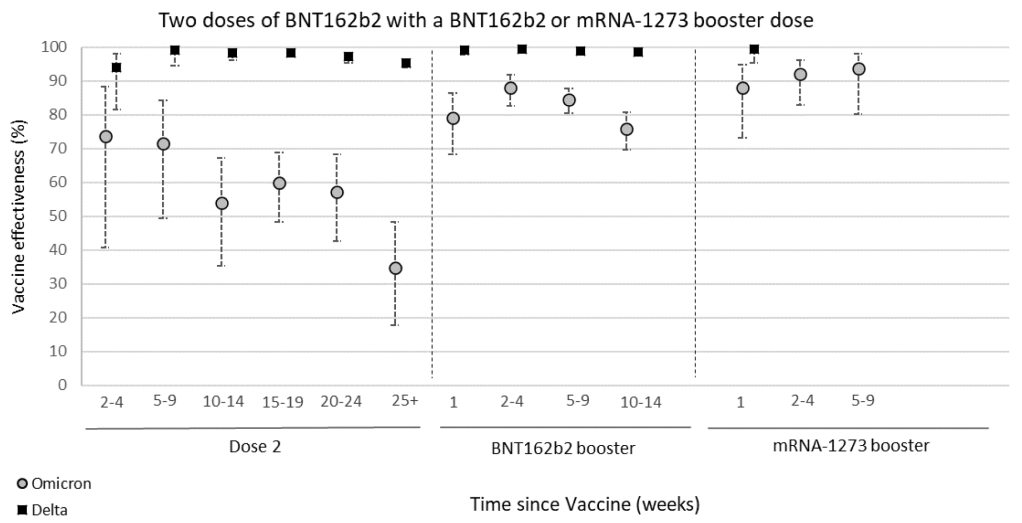
Certain vaccinated individuals are more likely to be infected by Omicron than the unvaccinated: A UK surveillance report shows that vaccine effectiveness against symptomatic Omicron infection goes from around 65% effective soon after 2 doses of vaccine, to around 5% 6 months later. Protection from hospitalization goes down to just 35% after 6 months. These findings suggest that to maintain full protection against Omicron, a vaccinated person will need to get a booster every 3 to 6 months.
From UK Surveillance Report, March 17, 2022, Table 1b. Effectiveness of Pfizer vaccine at preventing symptomatic COVID infection after 2 doses, and after a Pfizer or Moderna booster.From UK Surveillance Report, March 17, 2022, Table 2b. Effectiveness of Pfizer vaccine at preventing hospitalization after 2 doses, and after a Pfizer or Moderna booster.
In another finding from the report, people with 3 doses of vaccine are 3x more likely to be infected with Omicron than unvaccinated individuals. This is the clearest evidence yet that Omicron may be using Antibody Dependent Enhancement (ADE) to infect people. The Lewnard et al paper from a few months ago has a similar finding. For both studies, a certain number of vaccine doses are more likely to increase the chance of infection. If viruses are using the ADE pathway, this effect would be explained more by the timing than by the number of doses per se. For ADE to work, a person needs to have a mediocre immune response to an agent, not a strong or weak one. Since we know vaccine mediated immunity goes down over time, then a person becomes more likely to be reinfected as their immune response goes from strong to mediocre.
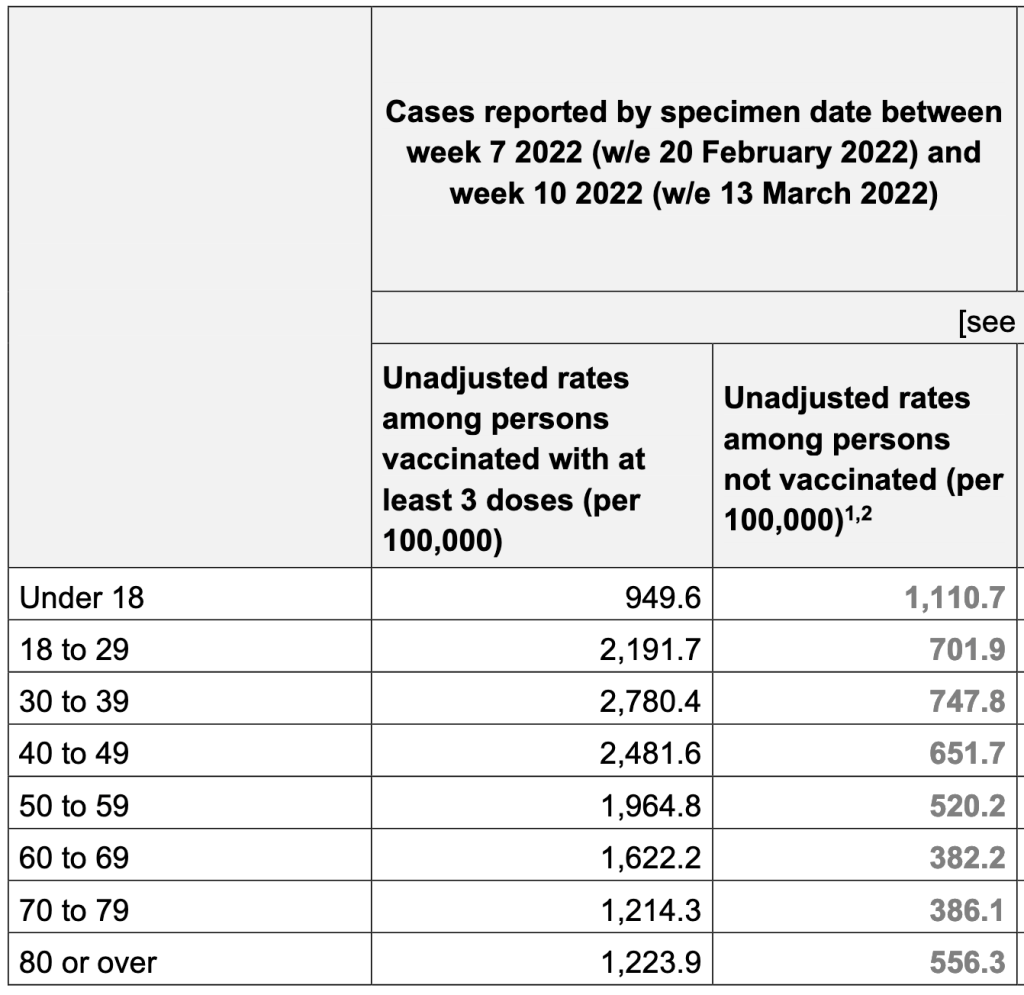
From UK Surveillance Report, March 17, 2022, Table 13. New case rates among UK residents with at least 3 doses of vaccine, and with no vaccination. Numbers are normalized for the percentage of people in each group.
So should you get a booster? Again, if you have risk factors like age, obesity or respiratory problems, you might want to get a booster every 3 – 6 months. Otherwise, you may choose instead to just take extra precautions as Omicron cases continue to fall in the US. If you choose to get a booster, ask them to aspirate before injection. Talk to your doctor when making medical decisions.
I know this is all very complicated. Your questions will help me make this more clear.
Here’s a brief case update. I’ll also have a brief comment about vaccine mandates.
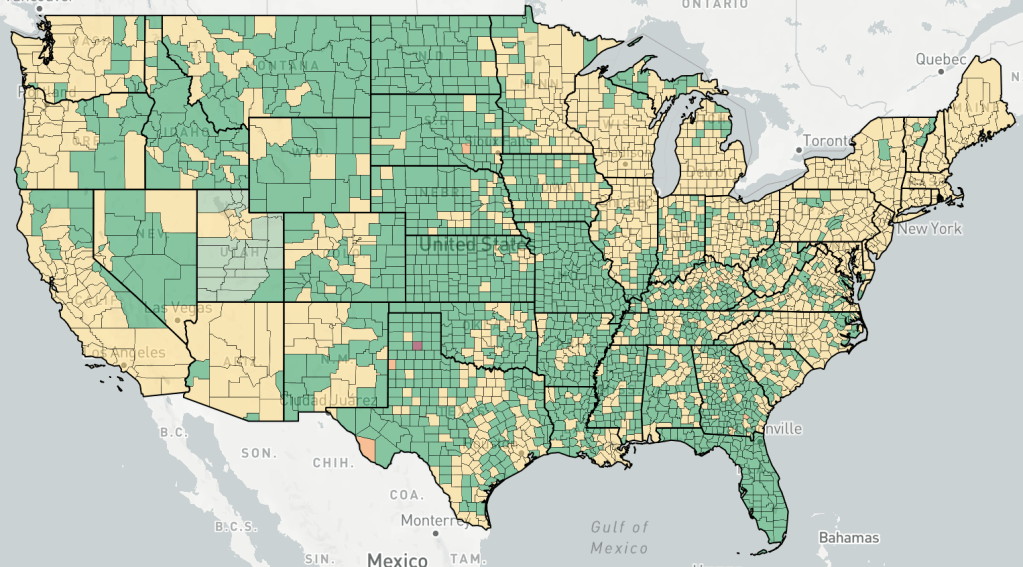
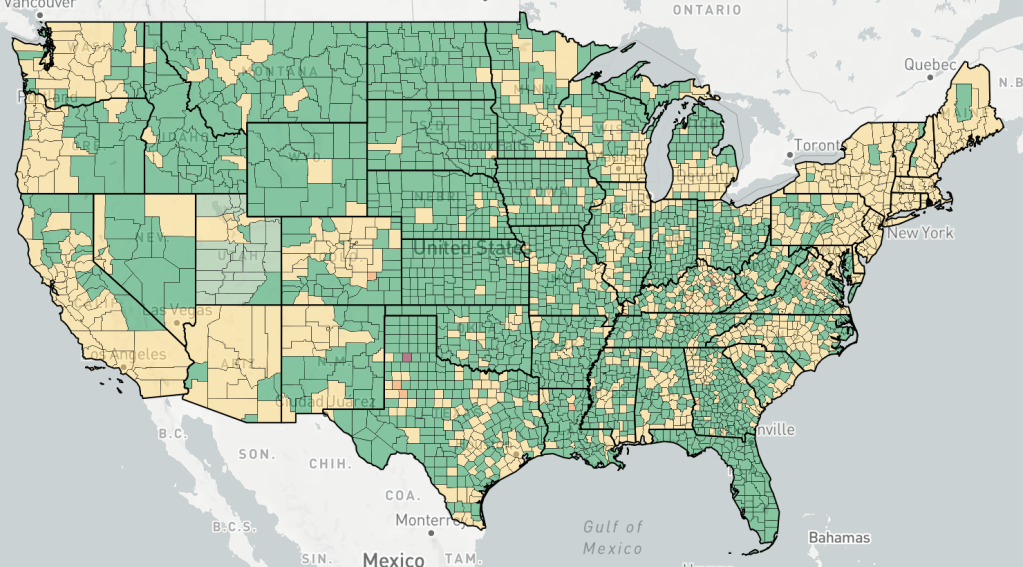
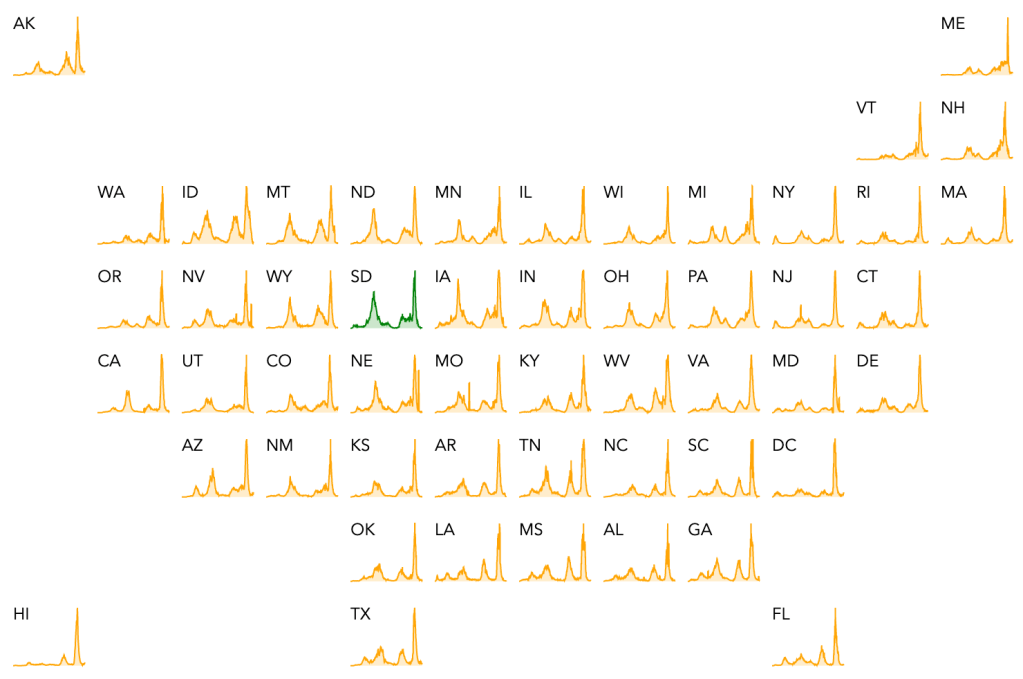
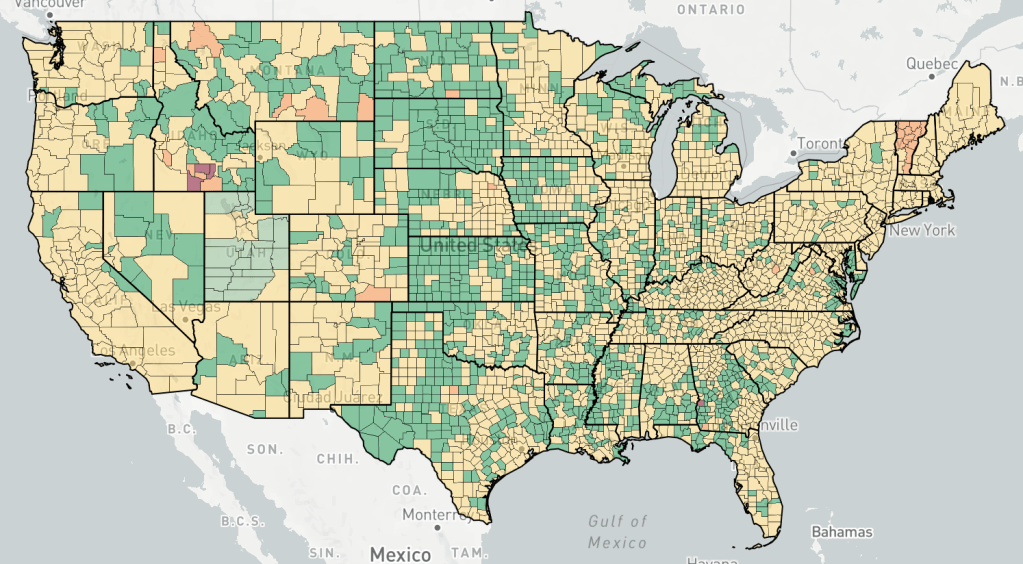
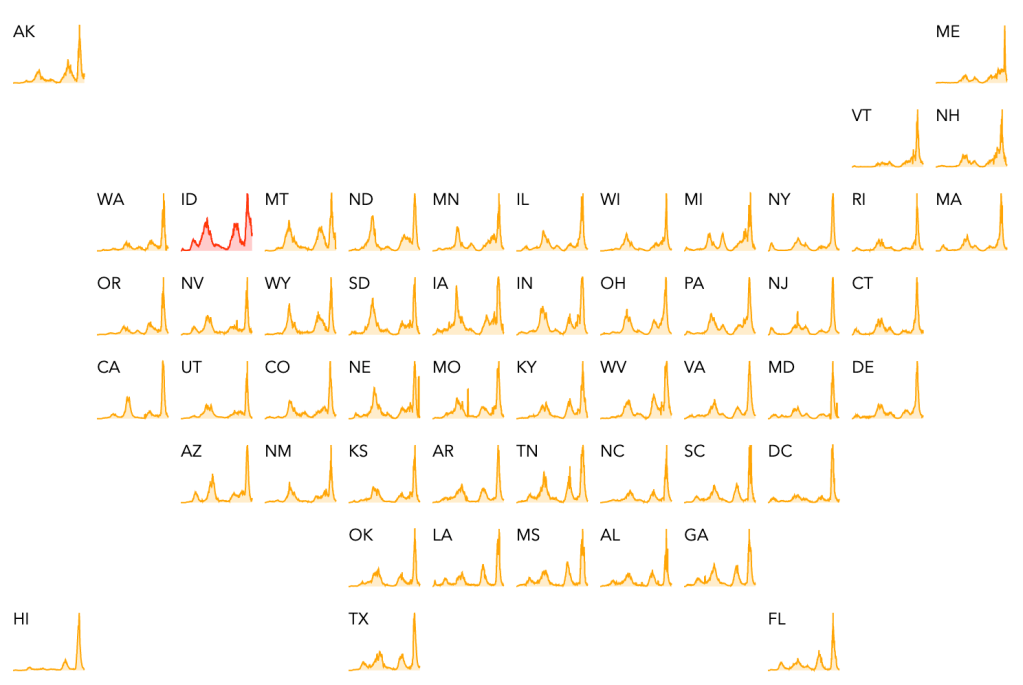
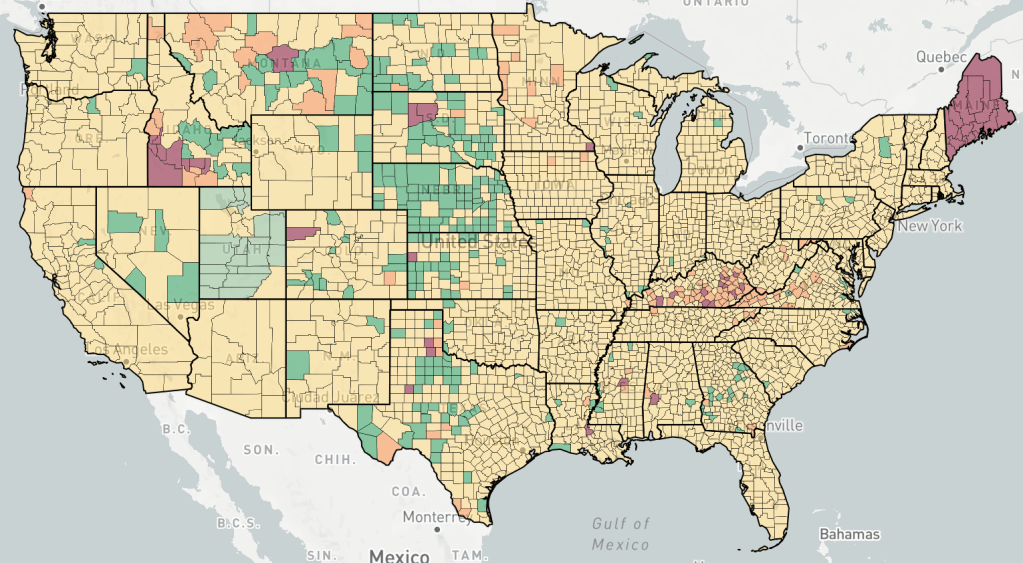
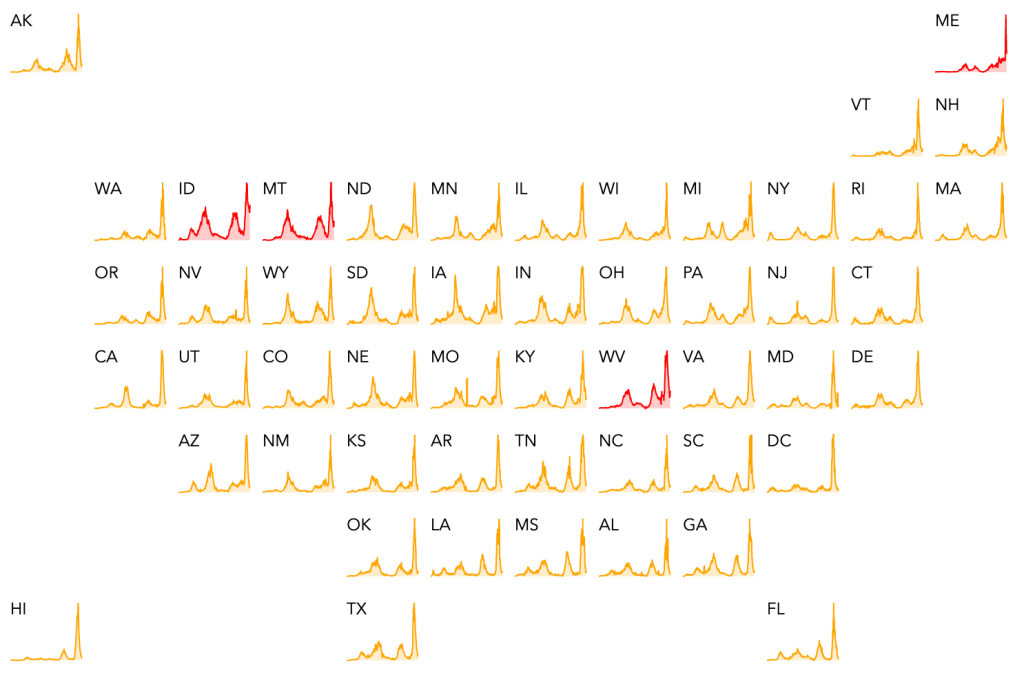
Cases continue to come down in the US, California and San Diego County. Cases in the US are now approaching being as low as they were in the Spring before Delta started. The only current outbreaks, according to endcoronavirus, is in the Twin Falls area in Idaho. Cases are dropping in San Diego County too, but unfortunately, not as fast as other places. LA and San Diego Counties are now #1 and #2 for new case numbers in the US.
World wide, the US is now in 8th place for countries with the most new COVID cases in the last month. This is a welcome change, since the US has spent large majority of the pandemic in 1st place. Ironically, the country in first place right now is South Korea, which has been doing well for the majority of the pandemic, serving as an example for other countries to follow. The majority of cases country wide have happened in the last month, due to the super infectious but less virulent Omicron variant.
Vaccine mandates still enforced: In January 2022, the Supreme Court struck down the vaccine and testing mandate for all but a few health care workers. Mandates for federal workers are still working their way through the courts. In spite of this, some companies and municipalities are still enforcing the mandates. They often cite vaccine mandates, but the vaccine mandates still do not officially exist, having been struck down. So these entities are enforcing mandates entirely on a voluntary basis, and of their own volition. These entities do not acknowledge the now well known data that natural immunity is better than vaccine mediated immunity at preventing infection and the spread of SARS-2.
As you may have noticed, I’ve been tapering off the frequency of my updates as the pandemic recedes. As things continue to improve, I will post more infrequently.
I have a brief case update today. I’ll also do some more complaining about the CDC, with some vindication from other sources. I’ve complained about them a lot before, so if you’re not interested in more complaints, you can skip the last part of the post.
Cases are still coming down in the US, California, and San Diego County. Cases are about as high in the US now as they were in November, before the Omicron variant appeared. They are still not as low as they were in late June and early July, when the vaccines had been released to everyone, but Delta had not yet ruined the party. Things are improving greatly, and I’m enjoying going out with my new hard won immunity, but the pandemic isn’t over quite yet.
A brief look at endcoronavirus state and county level maps shows that Maine is having an outbreak right now. Looking at a higher resolution graph, the outbreak is actually already over, and cases are dropping again. This may be a real outbreak, but it may also reflect reporting practices in Maine.
Trouble at the CDC: If you’ve been reading my posts, you know that I regard the CDC as one of the main villains of the US response to the pandemic. I don’t have enough data to say that they intentionally under performed, and most pundits I’ve heard chalk this up to simple incompetence. Early on, they basically agreed with whatever the WHO said, even though is was clear that the WHO was repeating Chinese government talking points. Later, I assumed that their slow release of information was because they were just very careful, waiting until there was certainty before releasing information that was already nearly obvious to everyone.
Later, however, things took a dark twist. As useful papers began to come in from other countries like Japan, South Korea, the UK, Israel, South Africa, Sweden and Denmark; Morbidity and Mortality Weekly (MMWR) and Emerging Infectious Diseases (EID), the CDC’s own journals, produced very few useful papers on the pandemic. This despite the fact that the CDCs mission, it’s only job, and supported by 11,000 employees, is to produce information and guidance on the prevention of infectious disease. They don’t even have to implement or enforce their recommendations. The federal and state governments do that.
Then OSHA produced it’s official vaccine mandate. On the FAQ page, OSHA waived the requirement that employers must report adverse events from the COVID vaccination of it’s employees. They explicitly state that “OSHA does not wish to have any appearance of discouraging workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers’ vaccination efforts.” Yes, as of today, February 25, 2022, this ridiculous and damning statement is still on their website. Many have been suspicious that the CDC has not been diligent in collecting data for the Vaccine Adverse Event Reporting System (VAERS), but it was hard to prove it. The statement from OSHA confirmed that the CDC was intentionally blinding itself to data that would help answer questions about the vaccines.
While the vaccines have certainly been helpful in reducing COVID severity and deaths for many, it is suspected that thousands have died directly from the toxic effects of the Spike protein in the vaccine, and many thousands have suffered long term negative health effects. Only recently did a CDC paper admit that natural immunity was better than vaccine mediated immunity, even though that has been known for months, thanks to an Israeli paper.
The New York Times has been supportive of the CDC for much of the pandemic. However, on February 20th, 2022, the Times published an article claiming that the CDC has been withholding information from the public. Better late than never, I suppose. Data withheld includes hospitalization rates for various categories including vaccinated individuals, and the effectiveness of boosters for those younger than 50. Unfortunately, the author says that this is likely only a fraction of the information the CDC has been sitting on like an egg. When asked why so much information had been withheld, a spokesperson said it was because they feared the data would be misinterpreted. This from 11,000 people we pay to communicate to the public.
The United States is the third most populace country in the world, and we have 53 separate approaches to pandemic. The CDC has or could have had a wealth of data that could provide science based guidance to the world. Unfortunately, it appears to me that they have mostly been motivated to sell vaccines, rather than to serve their central function.
FDA corruption: In the meantime, Project Veritas released 2 videos featuring an FDA official revealing corrupt relationships between the FDA and the pharmaceutical companies. These relationships influenced regulation of COVID treatments.
What should be done about the CDC: In general, I’m not for abolishing things willy nilly. I will say, however, that the CDC needs top to bottom review and serious reform. The Director as well as much of senior leadership should be fired. Will any of this happen? Not for the foreseeable future. The CDC is empowered by Congress and overseen by the Executive Branch. Members of Congress are typically motivated by political considerations more than by producing sensible policy. I know I’m stating the obvious. Only when Congress changes will reforms happen. I will also point out that members of all political parties are prone to being absorbed into the Washington Hive. So vote carefully in primary elections! Do your best to select honest people to Congress, and don’t forget to vote local too.
This week I’ll have a case update, then discuss variant BA.2, and Dr. Fauci’s announcement about the end of the Pandemic.
Cases in the US, California, and San Diego County are all still going down sharply. Cases are now at the same level as in mid-December. According to Endcoronavirus, most states have decreasing cases.
Variant BA.2: This new variant is now increasing slightly over the original Omicron. This is no reason to be concerned, however, since BA.2 is just a slightly more infectious version of Omicron. Antibodies against Omicron are expected to be effective against BA.2, so this does not represent a new variant that will cause case numbers to rise.
Dr. Fauci announces the end of the Pandemic: In an article in Financial Times, Dr. Fauci stated that he expects that the pandemic phase of COVID will be over in the next few months. I agree, with the exception that I think a reasonable time frame is more like weeks than months.
He also stated that he thinks boosters will continue to be necessary to keep the virus at bay. On this I have to disagree. The vaccines had a minimal impact on new infections due to Omicron, although they probably had a positive impact on disease severity. Given that the new cases are now very low, and the unknown but real danger from adverse reactions, I think there is now almost no reason to get a vaccine booster. For vaccines to continue to be useful, we need a more current version, against something like Delta or Omicron. I don’t expect we’ll be getting that.
Many scientists, including those I respect, think the virus will become endemic, meaning it will continue to circulate at a low level in different forms basically forever. With some trepidation and perhaps over-optimism, I think Omicron will eventually peter out and SARS-2 will be over. We’ll see if that happens.
Just a brief case update today. New cases are still dropping fast in the US, California, and San Diego County. Cases are now about as many as their were just before Christmas when the Omicron wave was just starting in the US.
The great news is, deaths appear to have peaked in the US 2 weeks ago, and were indeed very low, about as many as last Winter when the cases were far fewer than in the Omicron wave. A little math says that Omicron is roughly a quarter as deadly as the Alpha variant from last Winter.
Another plug for data: Last week I asked for folks to answer the following questions:
1) Have you ever had COVID? If so, when?
2) Have you been vaccinated? When?
3) Have you had COVID multiple times? If so when? What were your symptoms like each time? Were you hospitalized? If so for how long?
4) Is there anything else you’d like to share?
Obviously, a lot of people don’t want to go public with this information. You can post below or direct message me. I want to get an idea of how vaccination and previous infection produced protection for future infection. When you were infected will tell me what SARS-2 variant you had, and whether that variant protected you from future versions.
So far, I’ve only gotten about 30 responses, too few to be useful. If you want chime in, please do so! Thanks!