This is a case update. I’ll also talk about the newly release v@¢¢¡ne mandate from OSHA, whether you should get a booster, and the question of whether v@¢¢¡nes lead to new SARS variants.
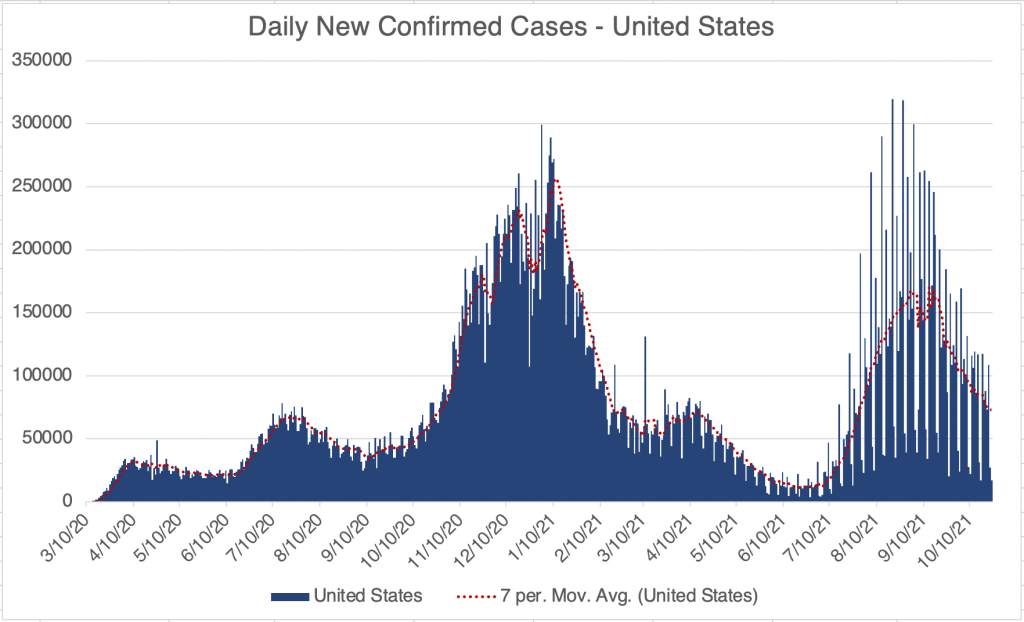
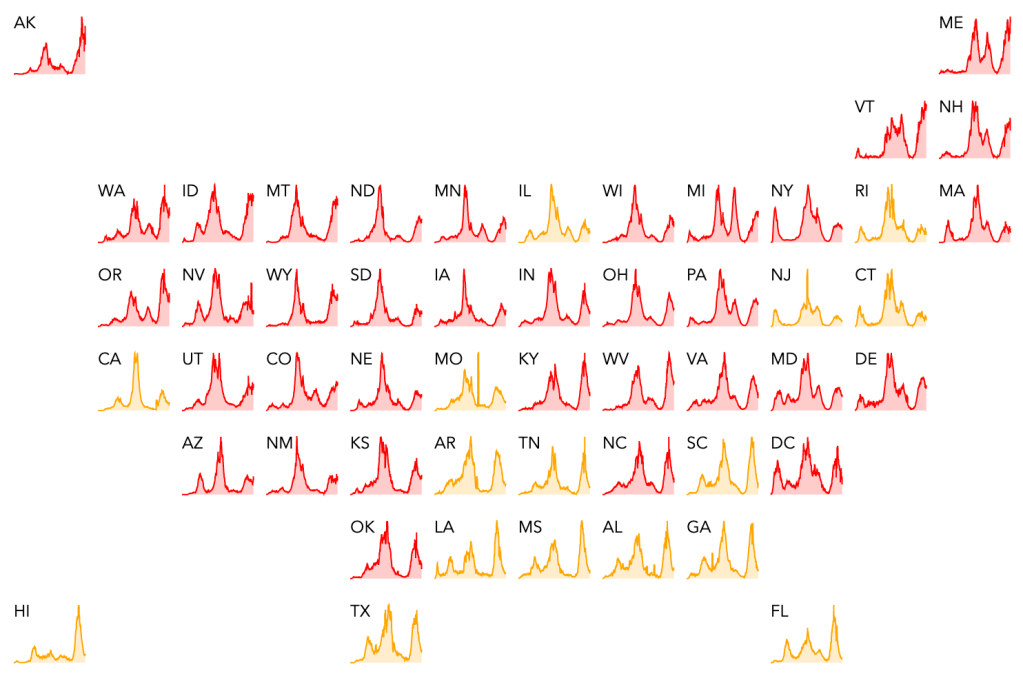
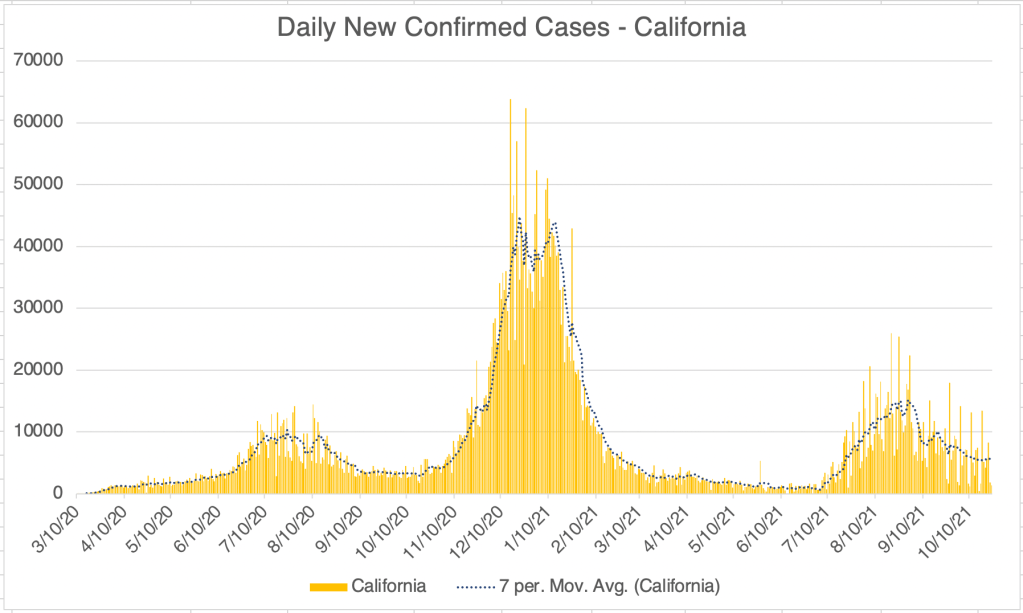
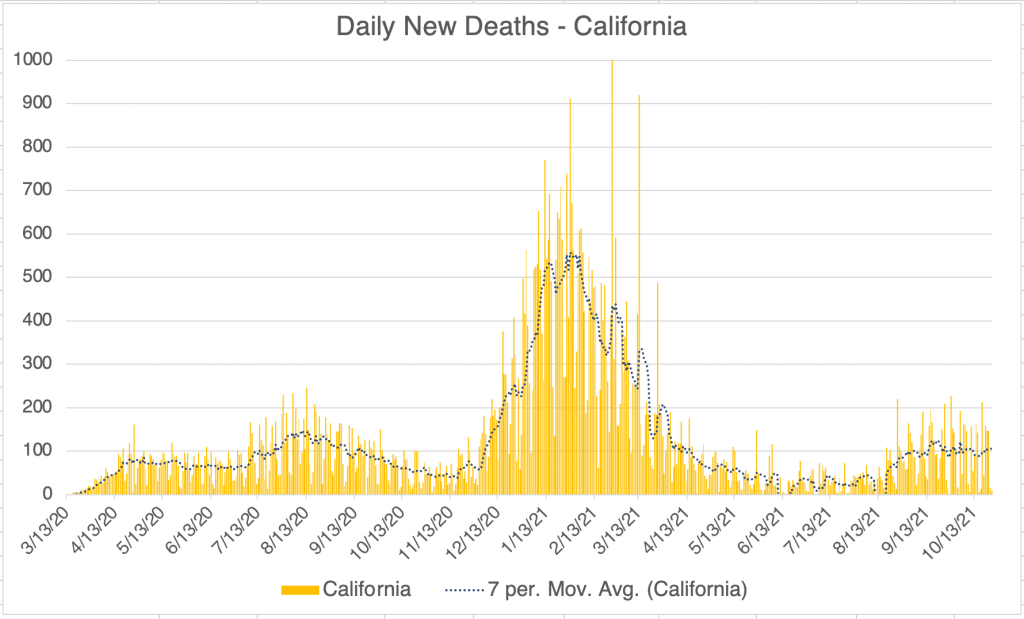
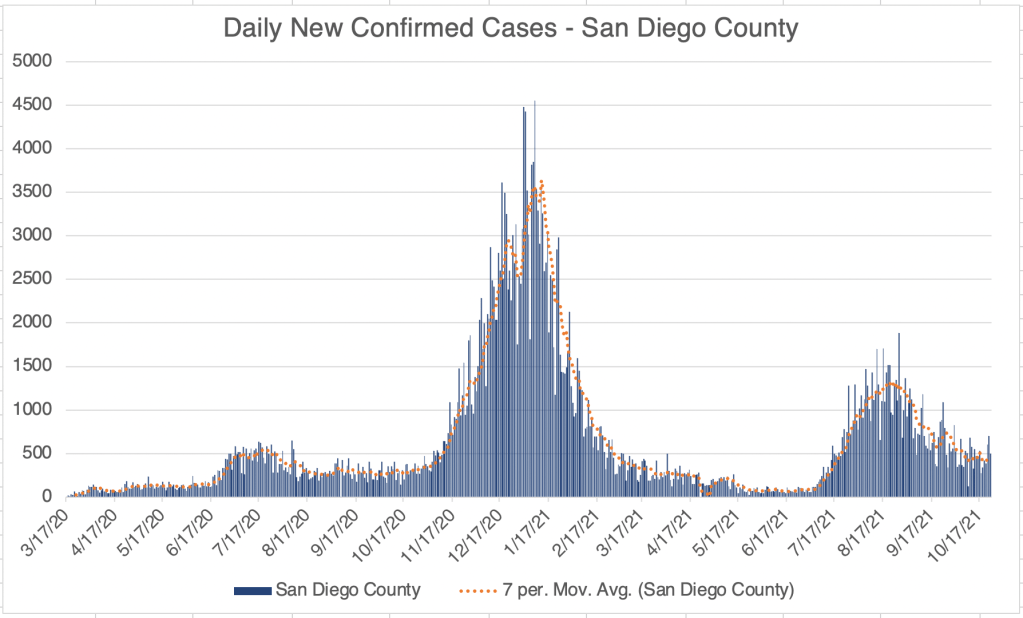
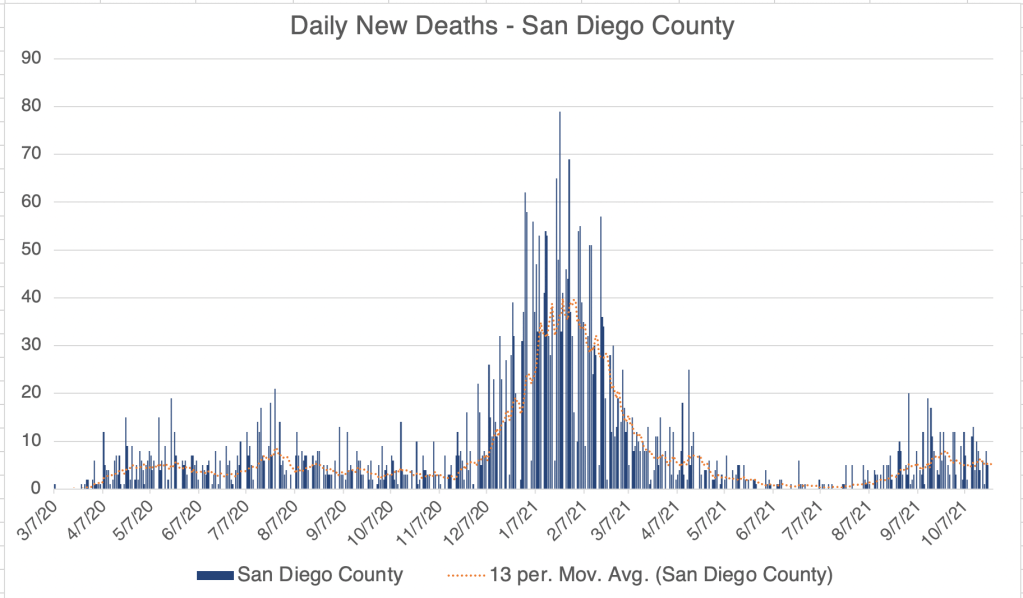
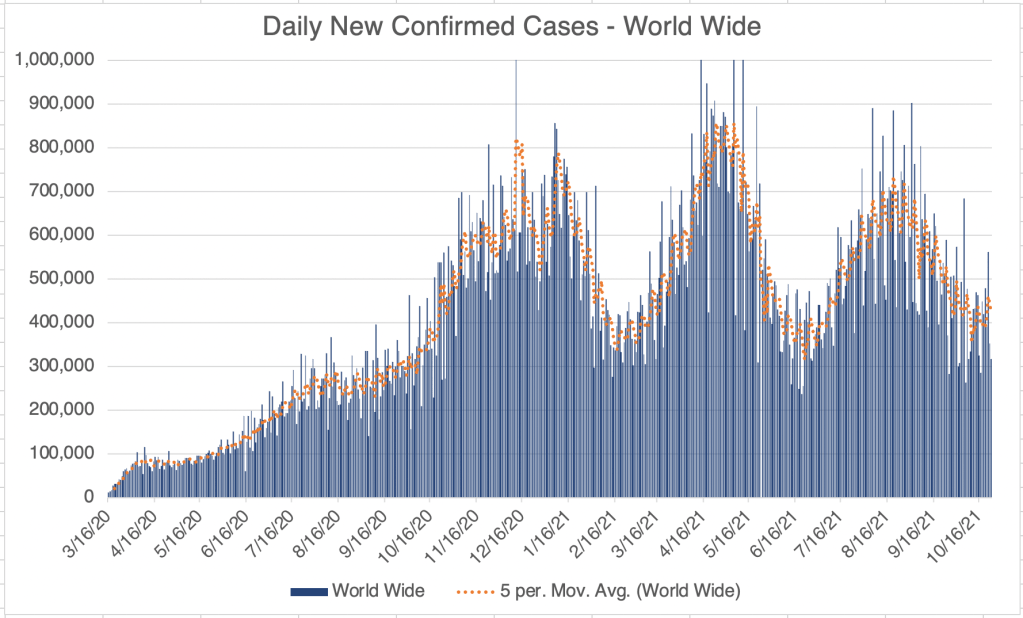
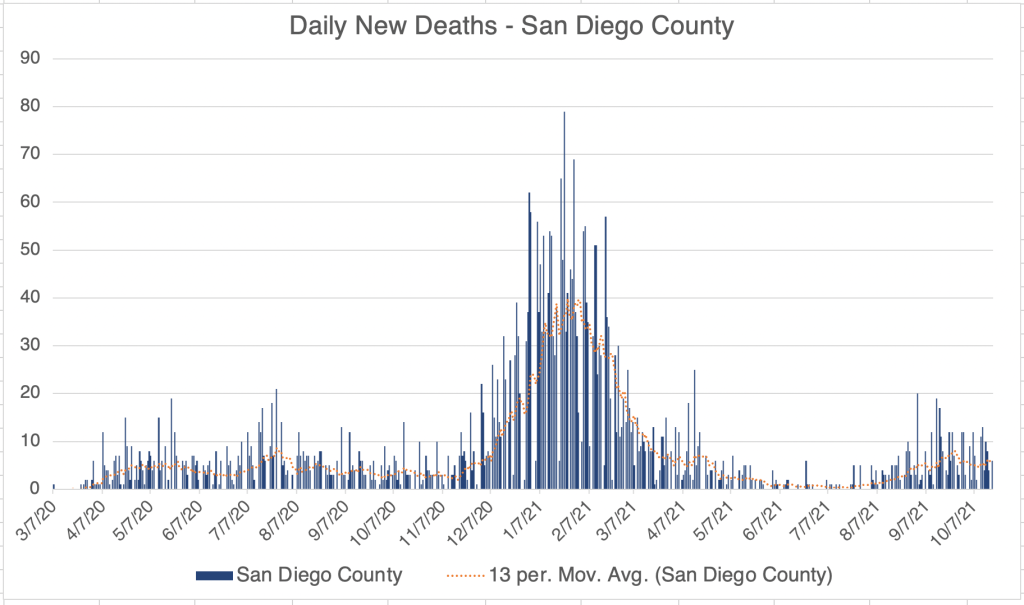
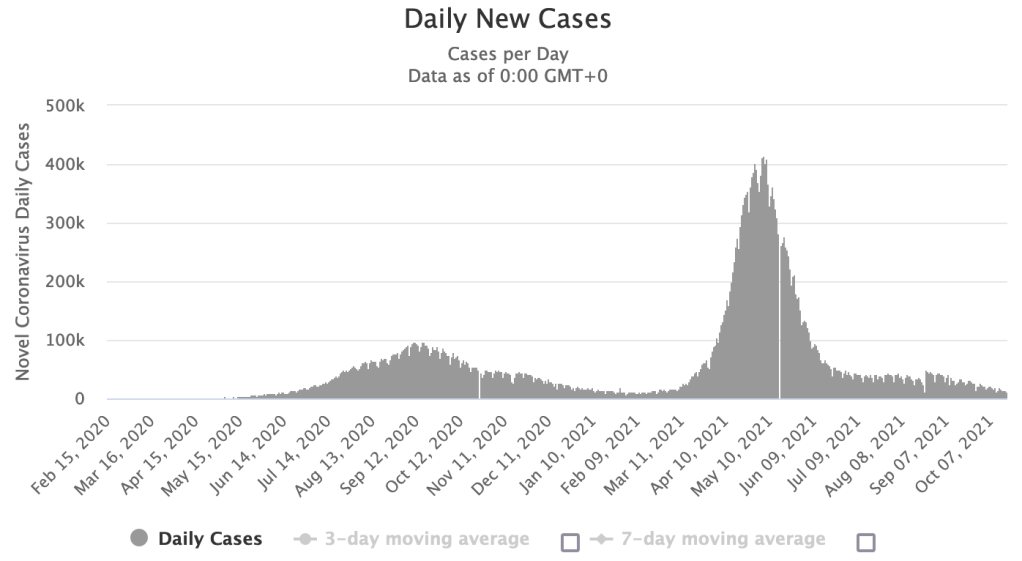
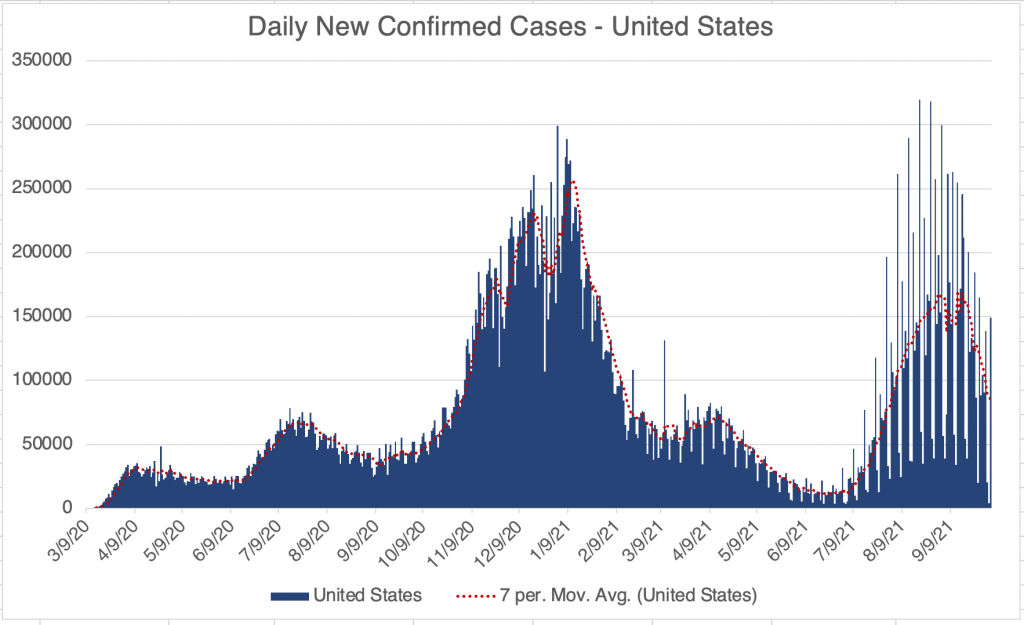
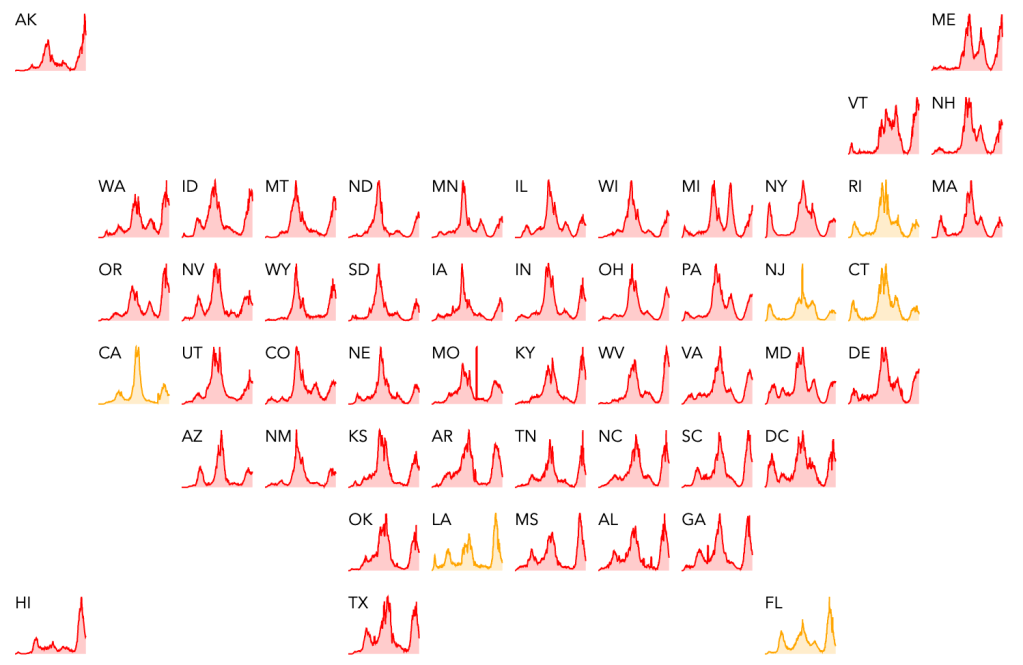
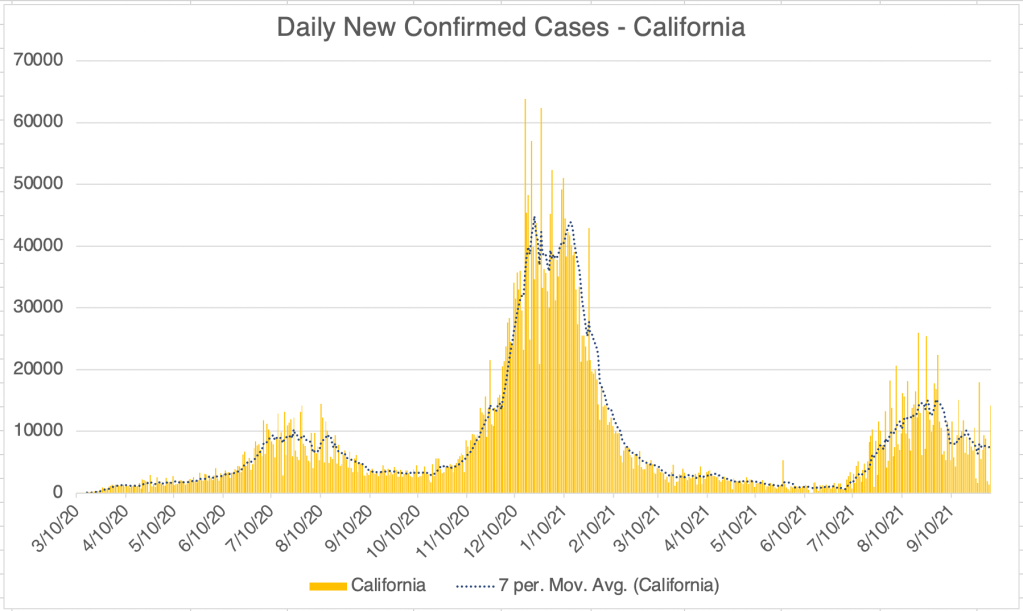
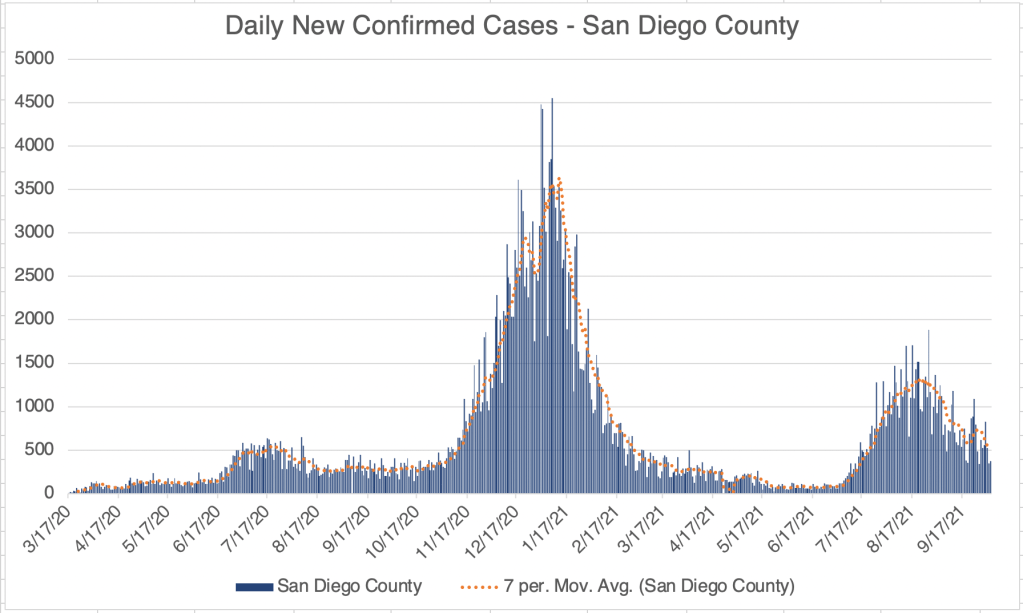
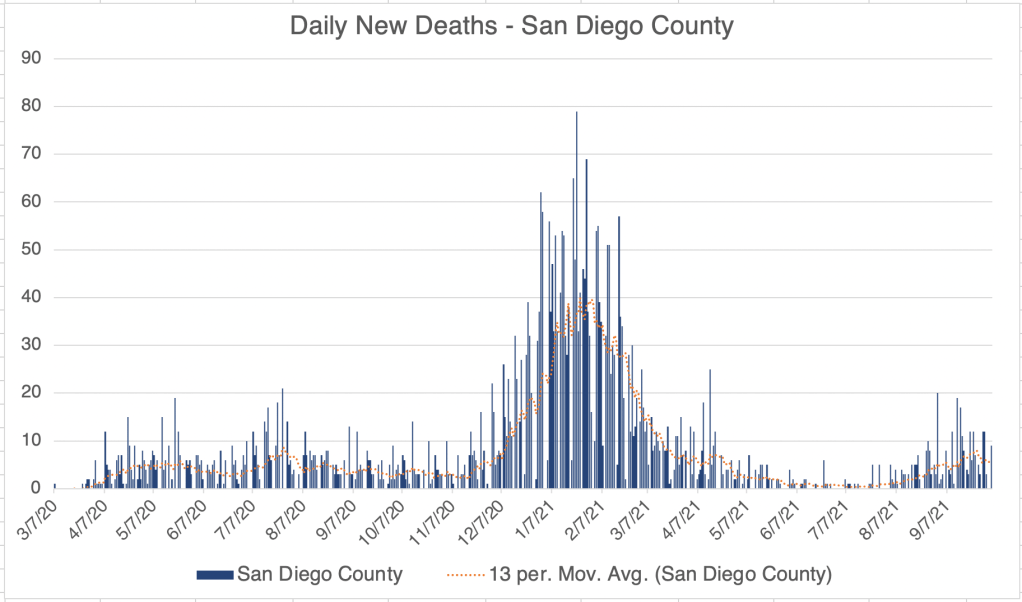
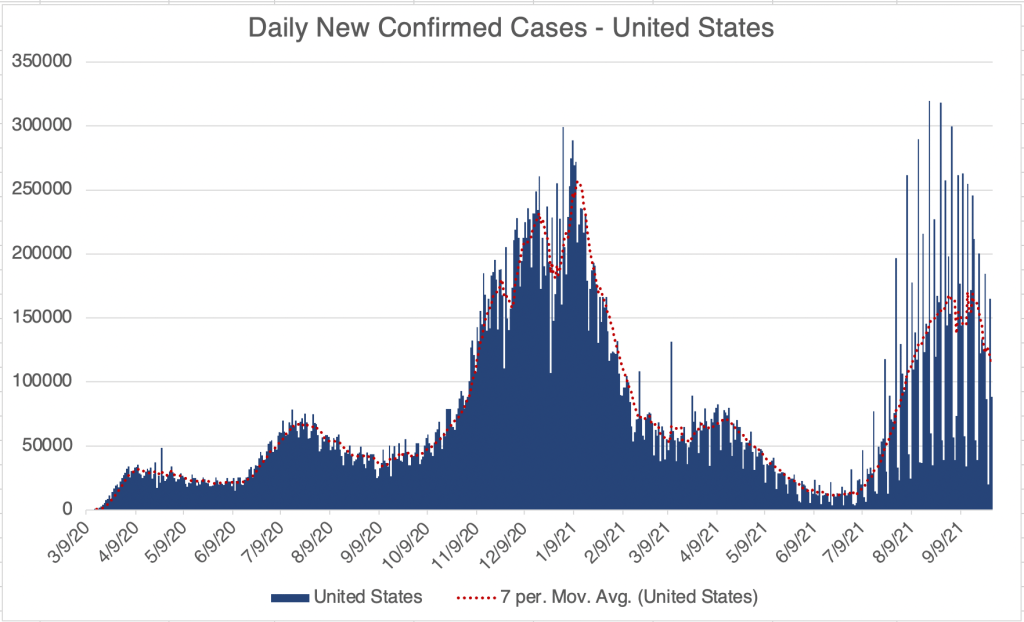
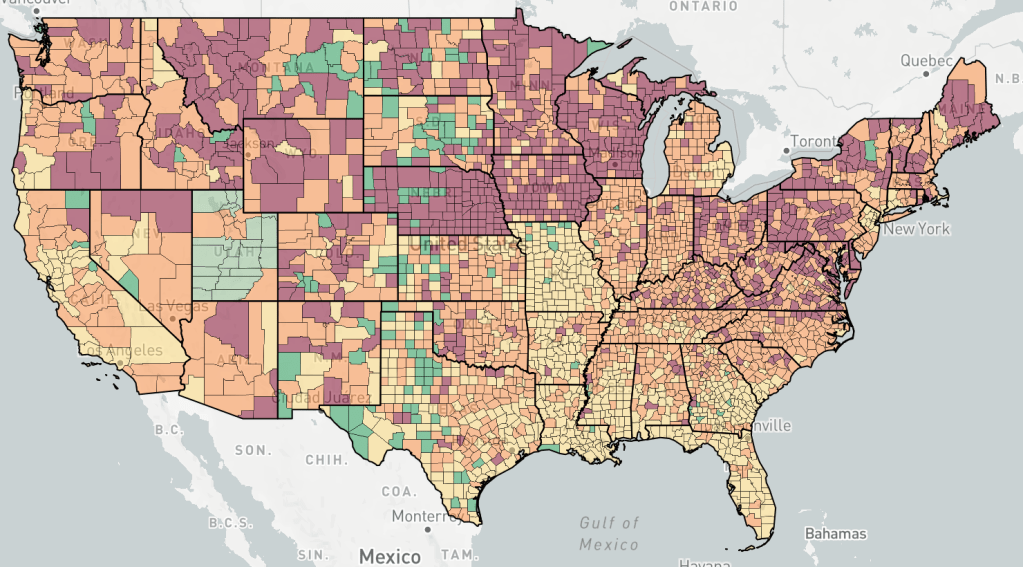
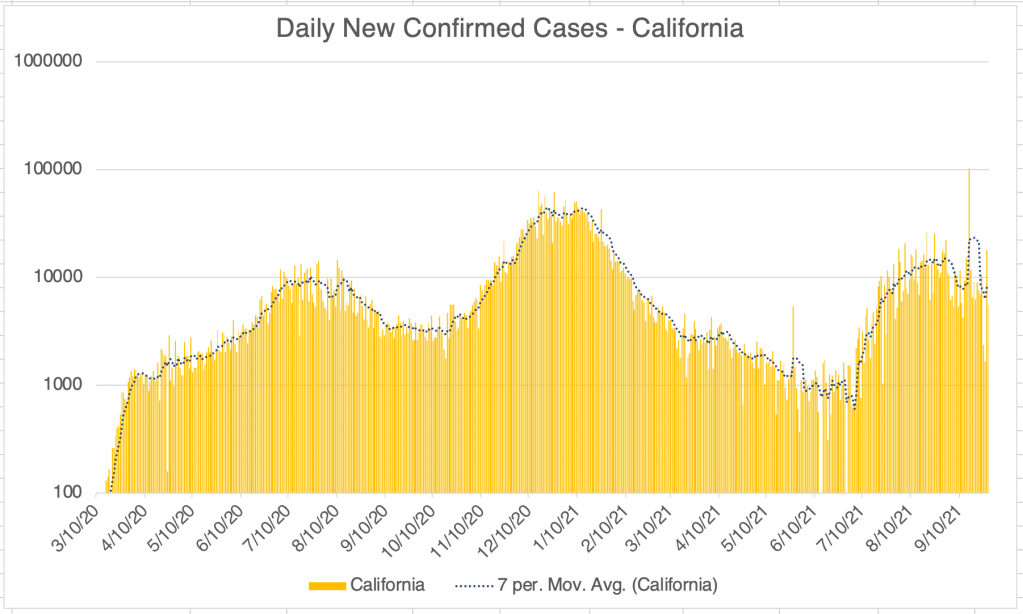
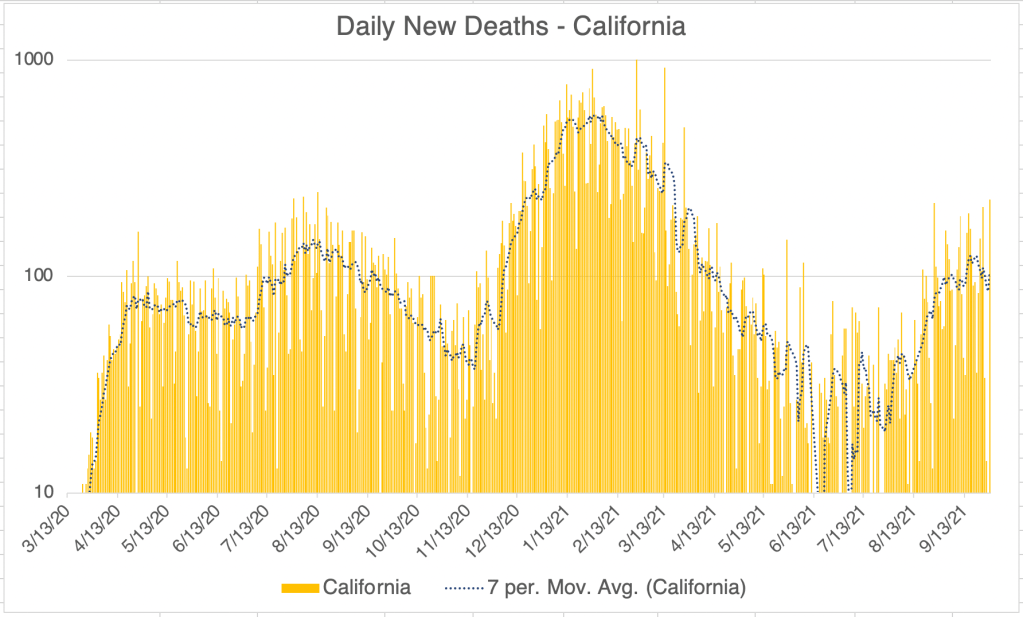
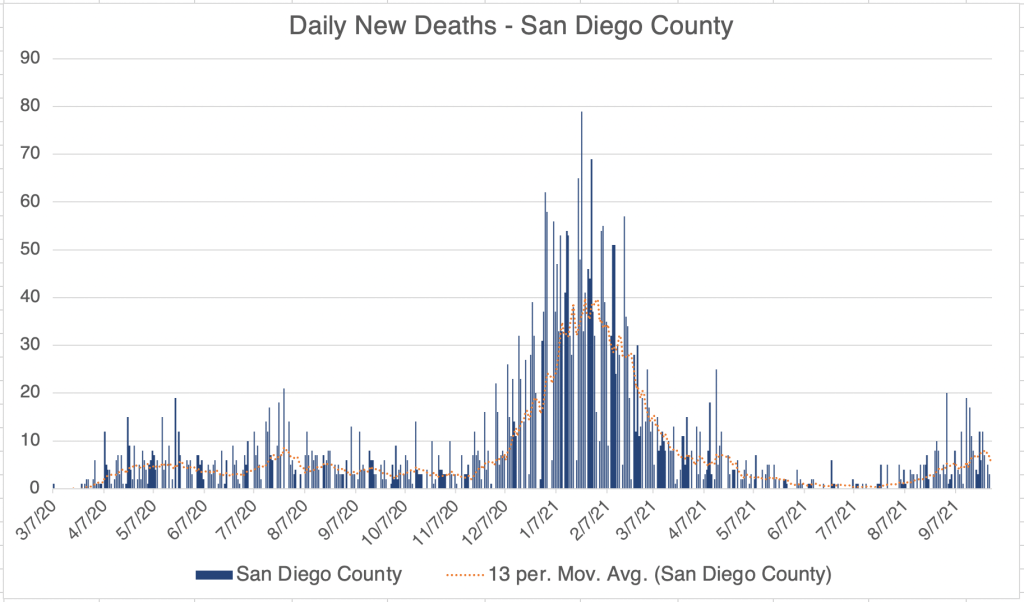
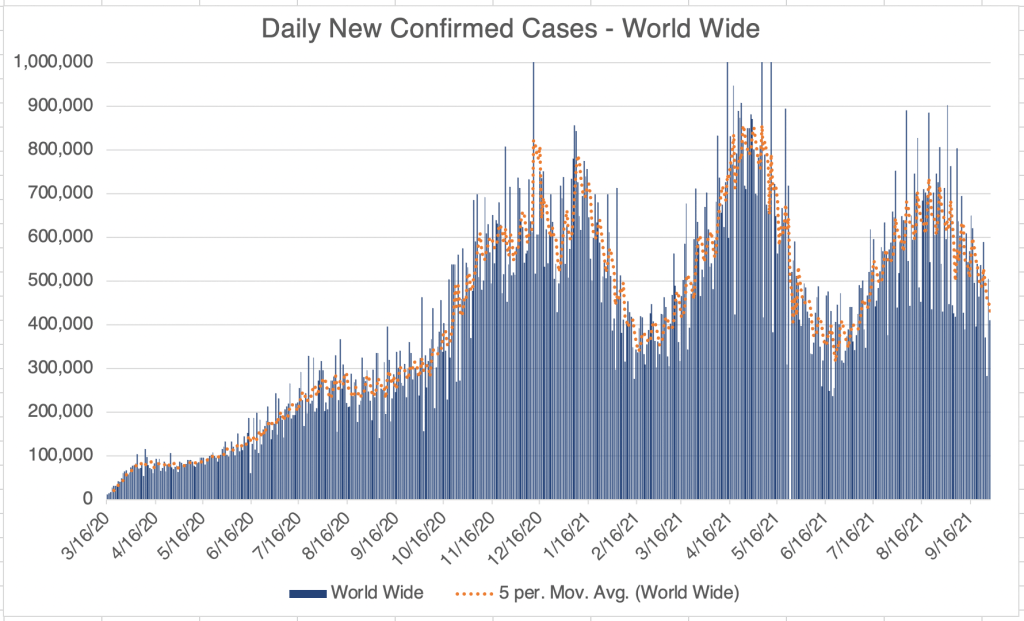
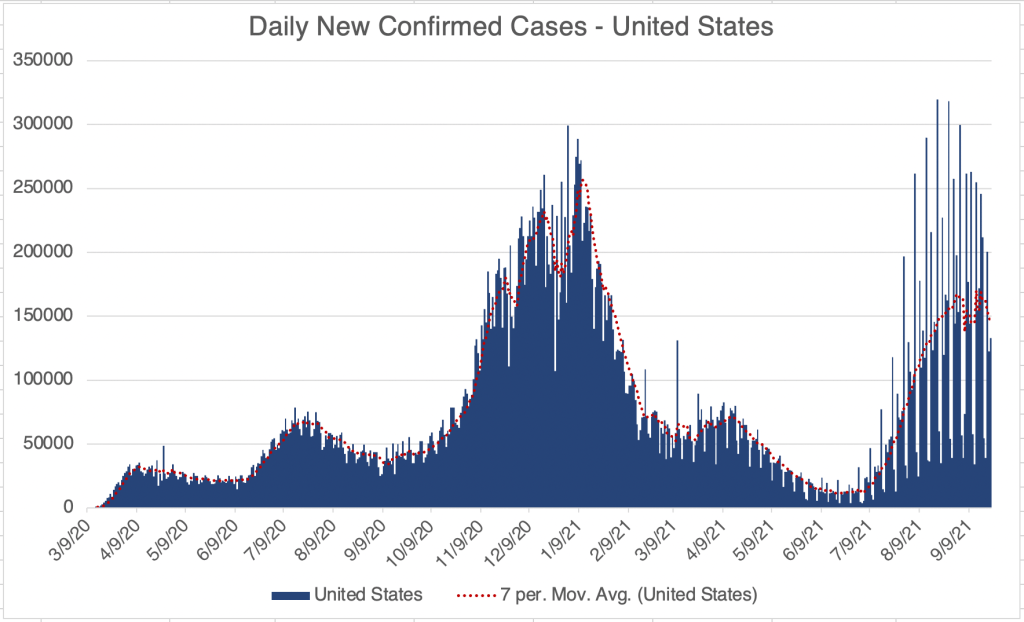
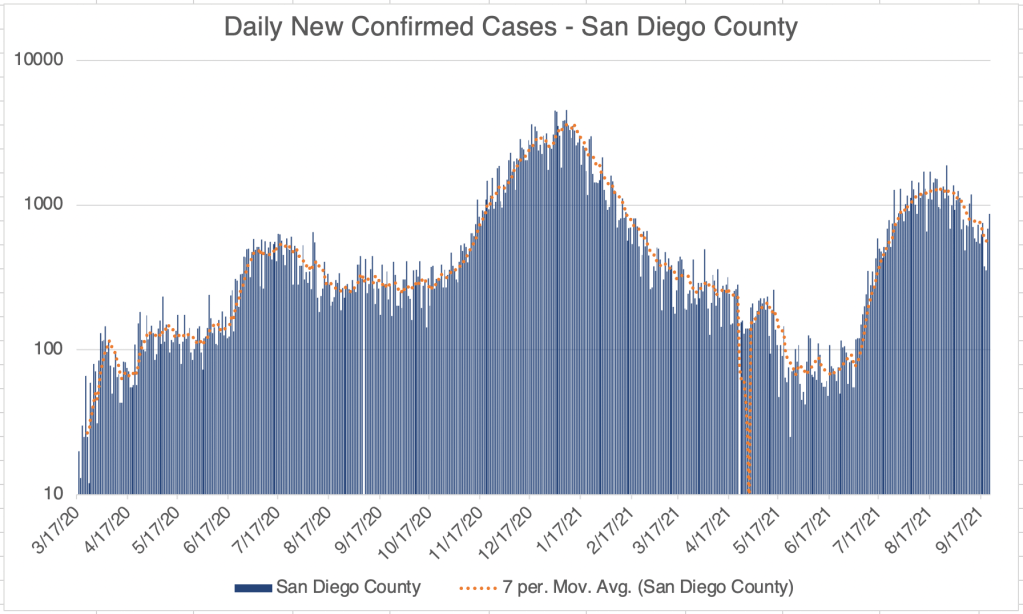
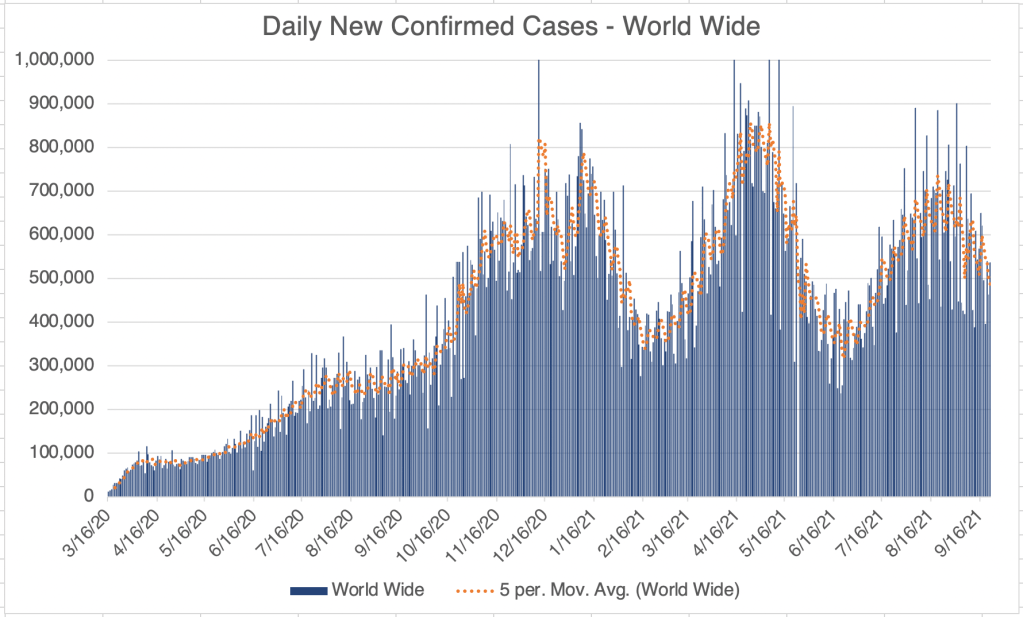
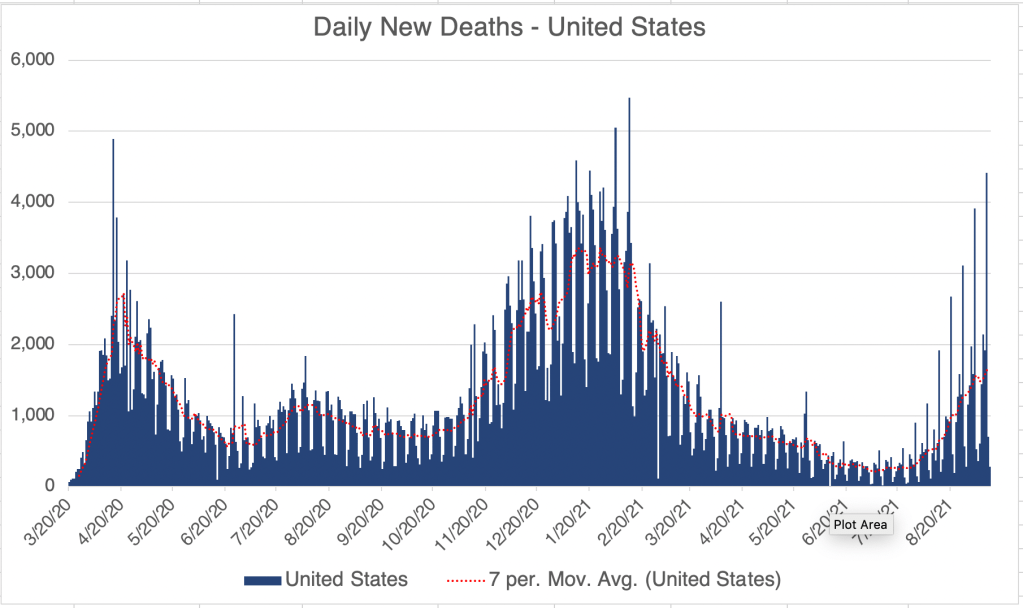
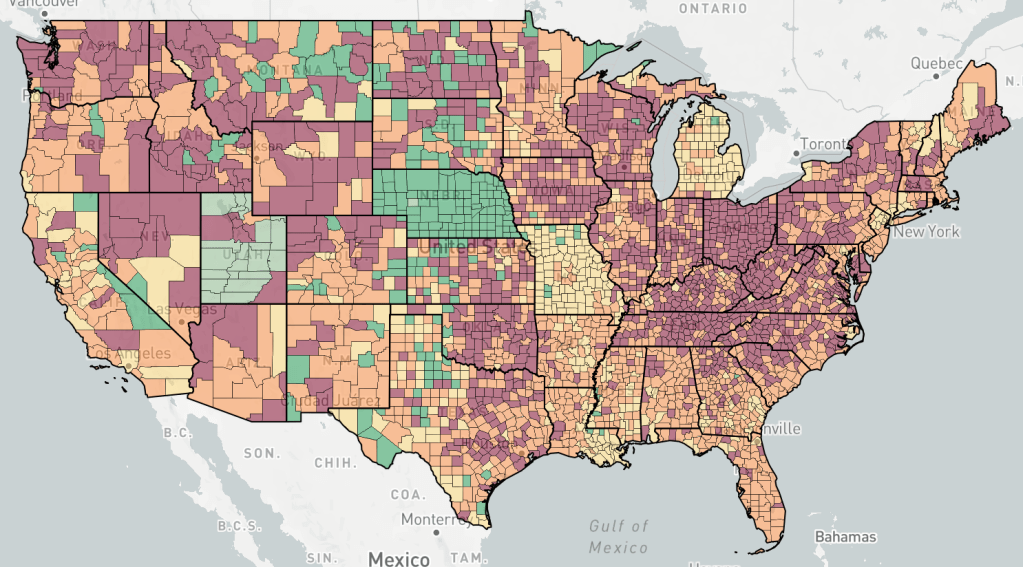
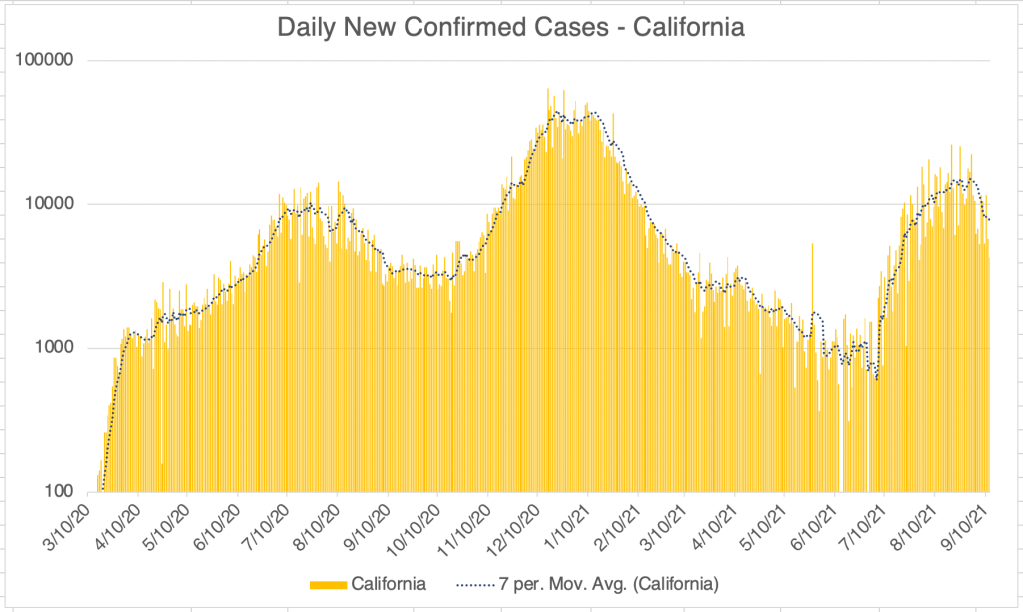
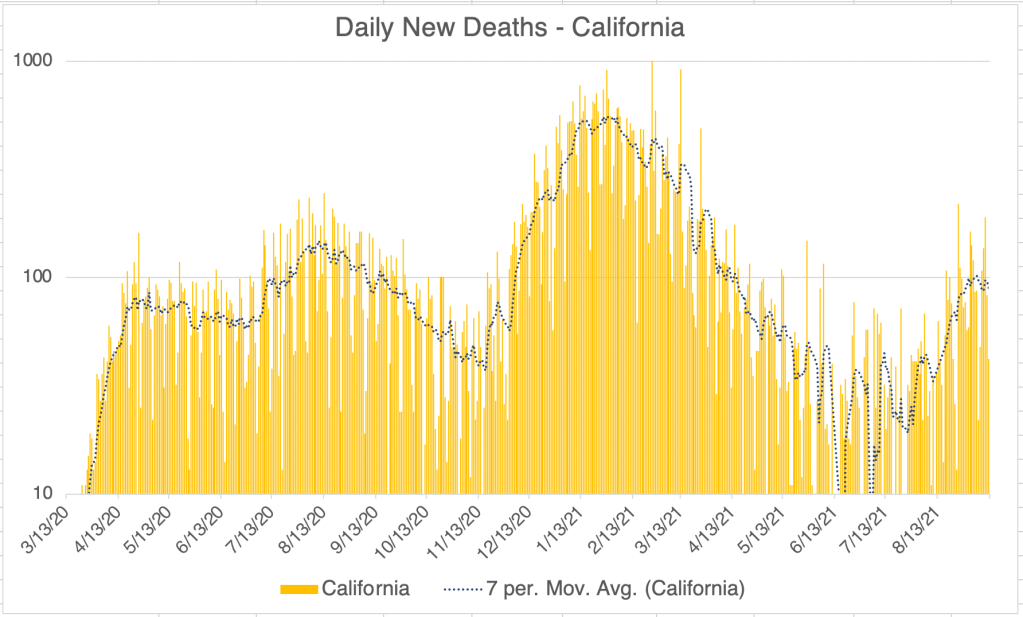
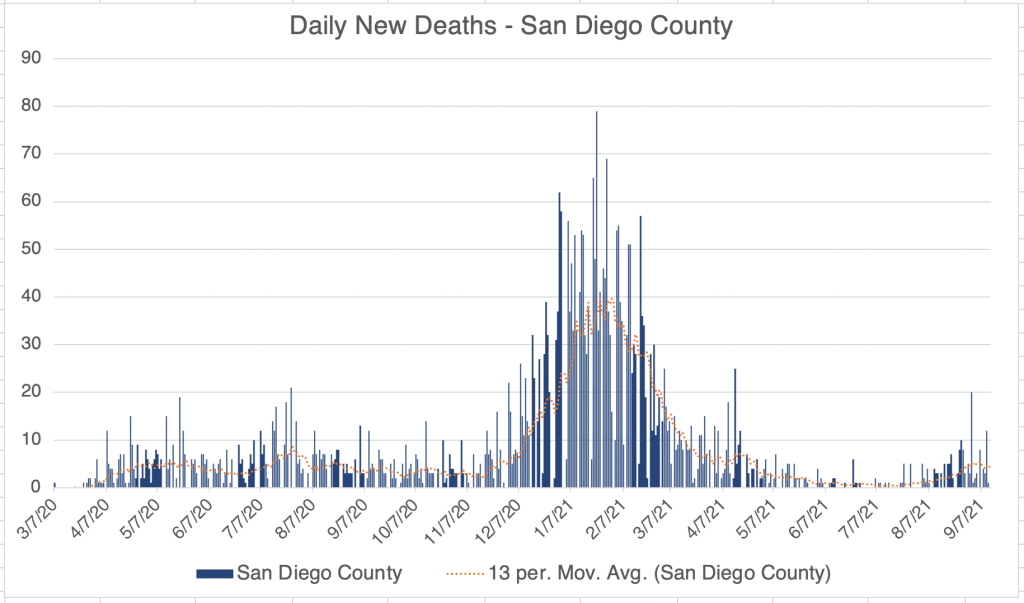
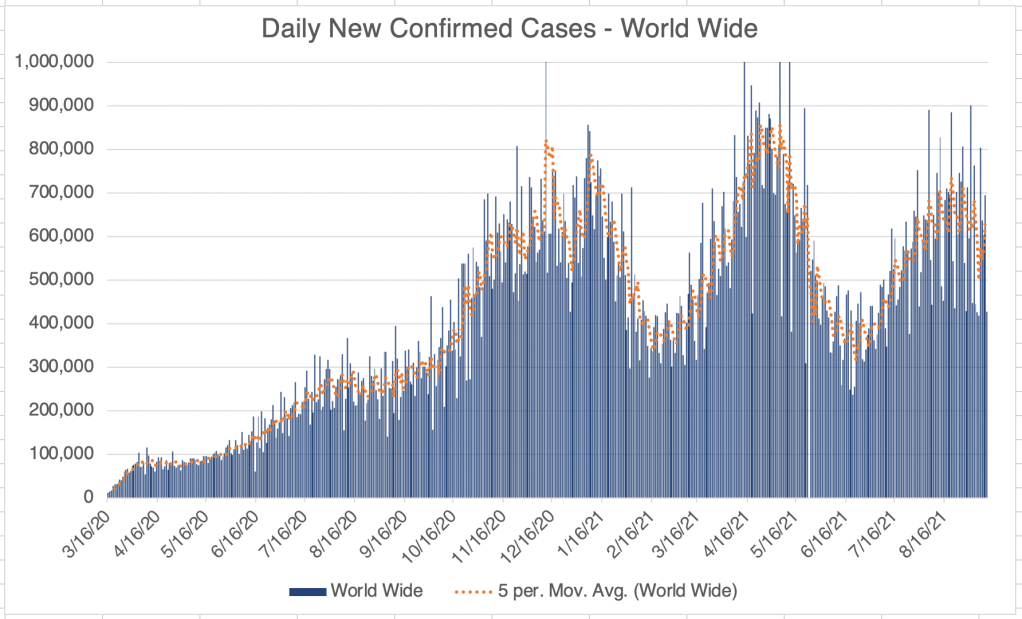
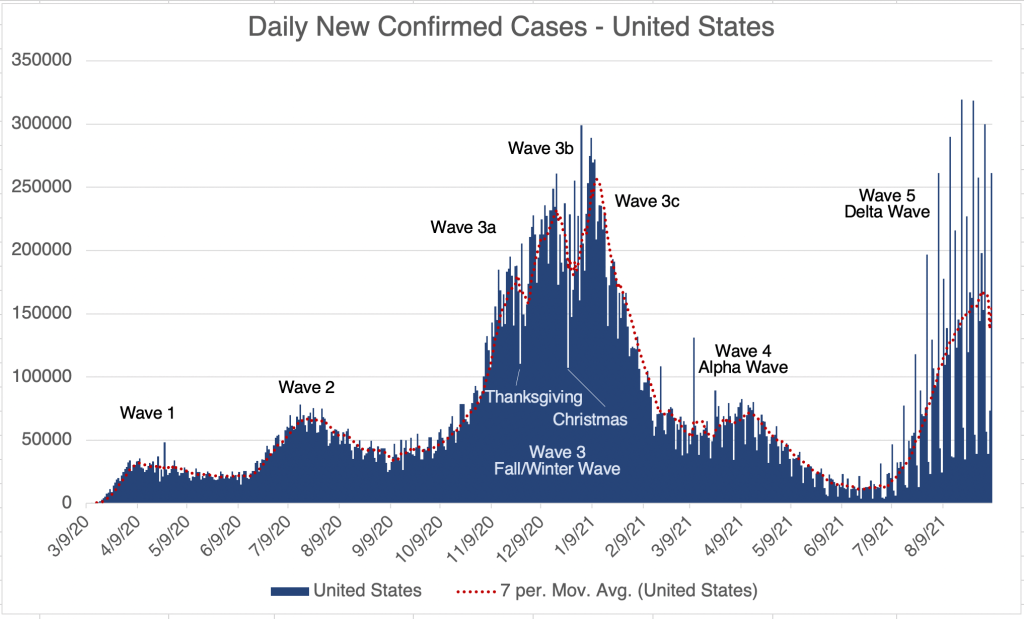
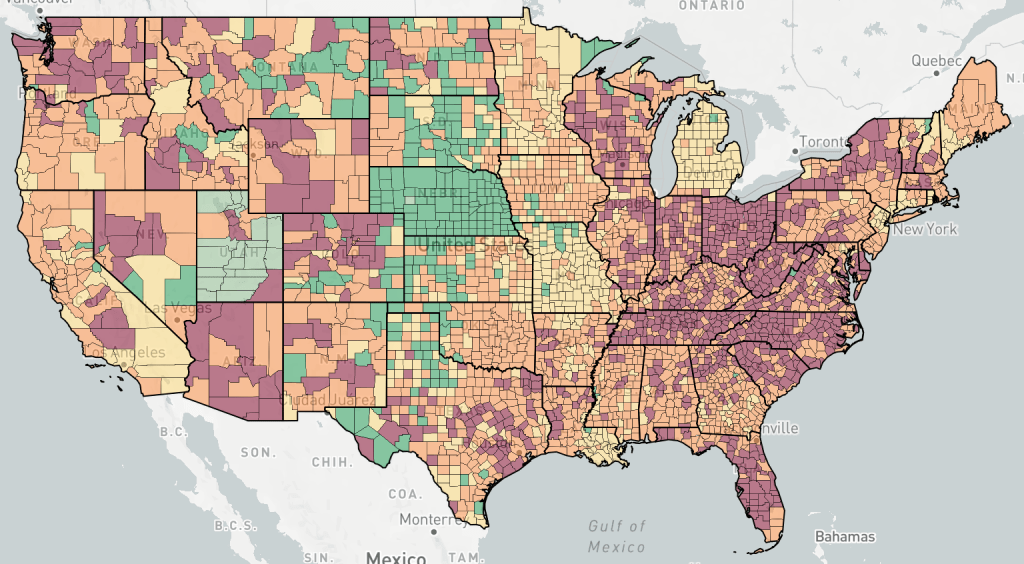
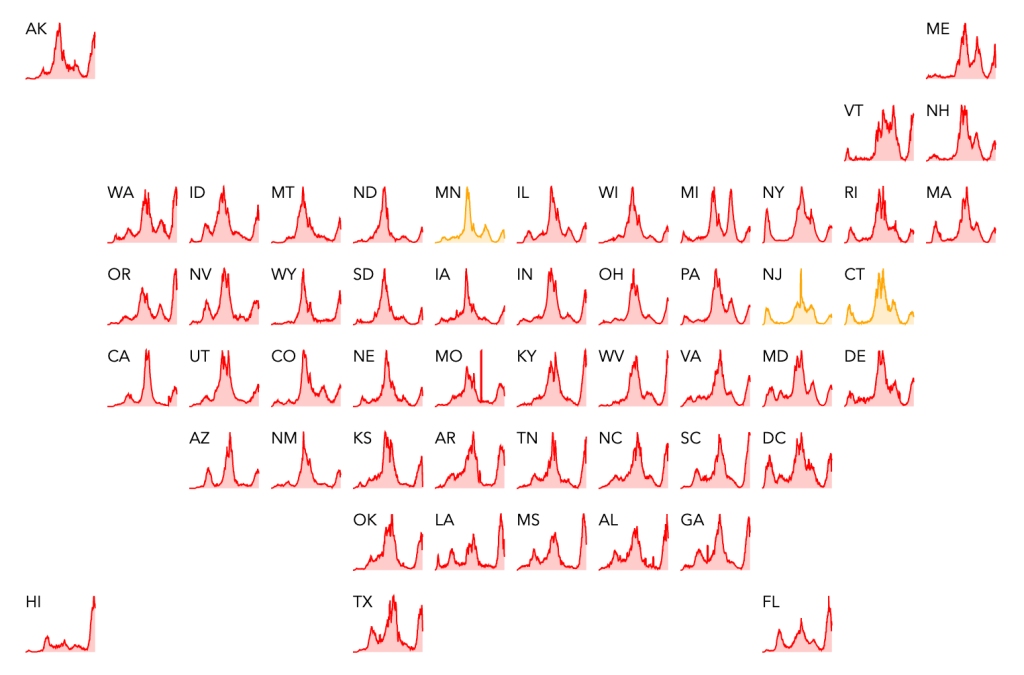
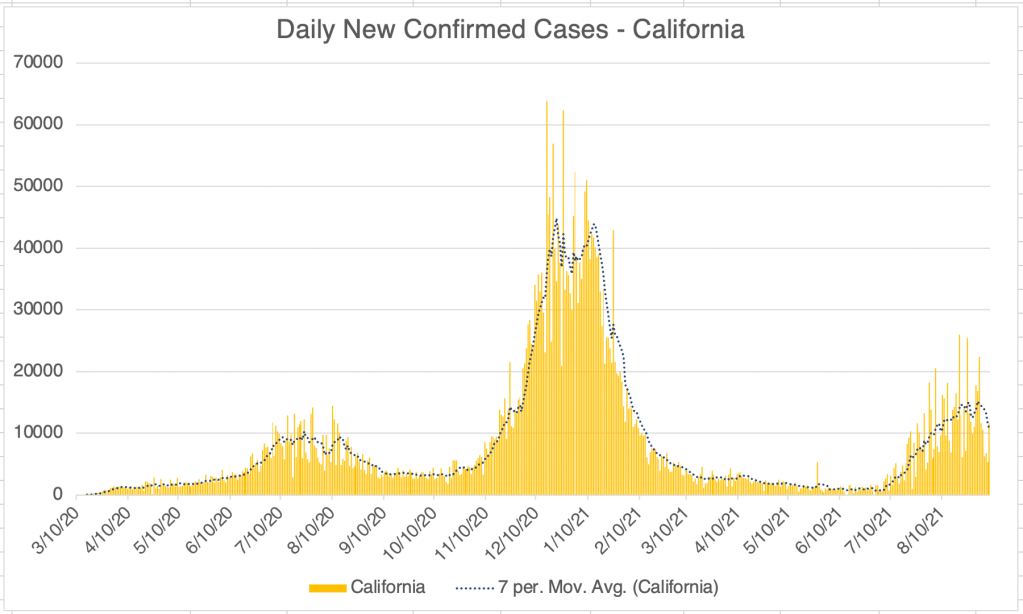
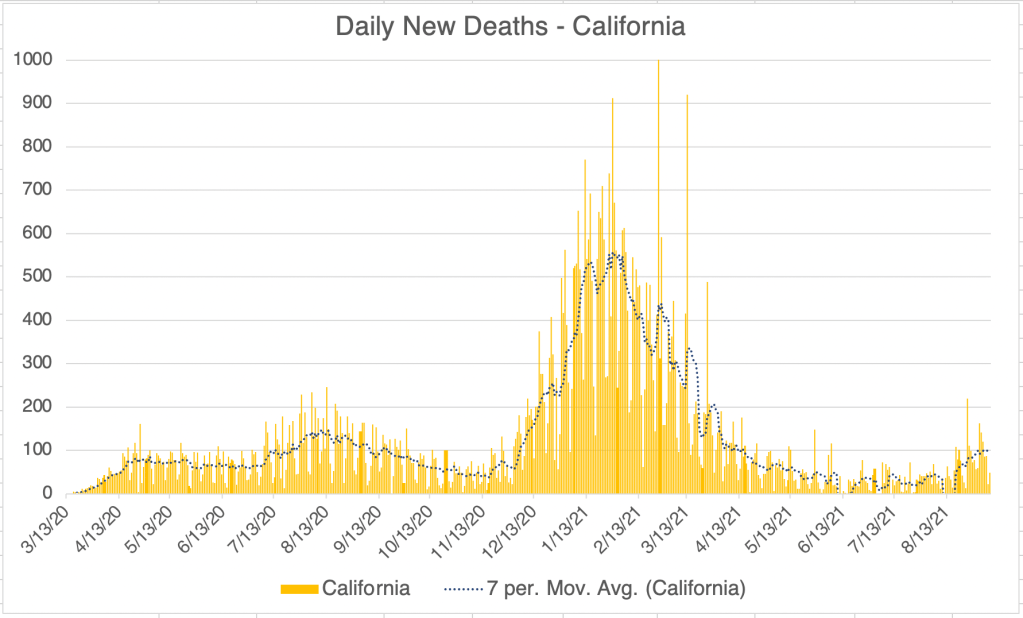
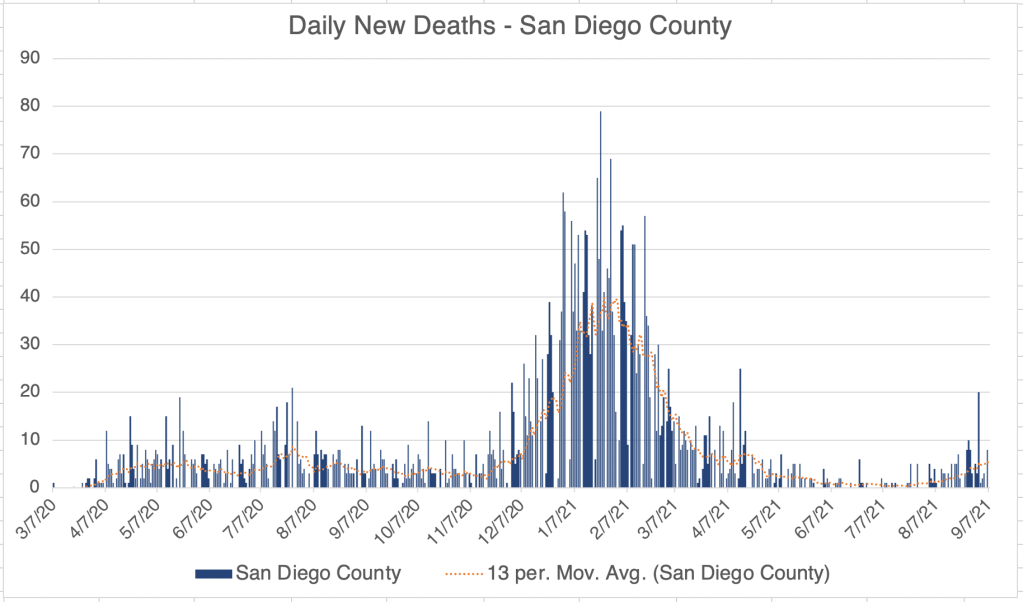
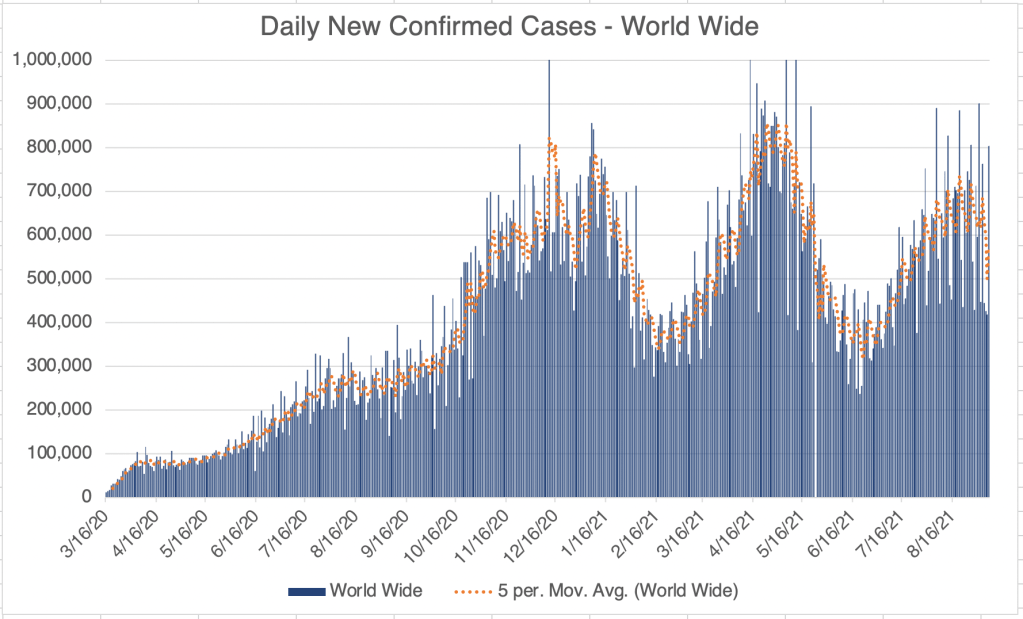
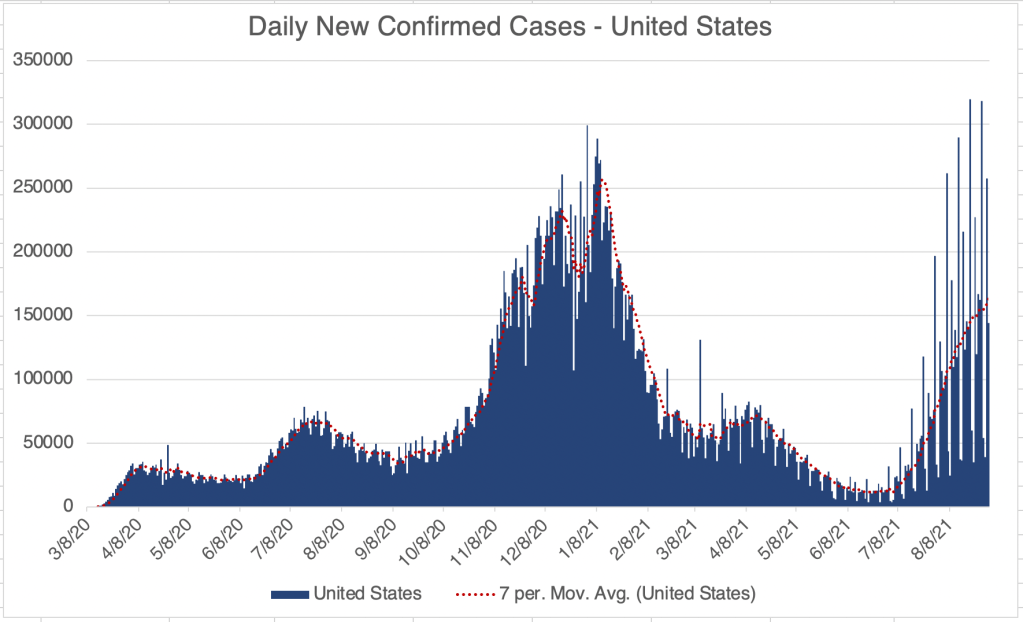
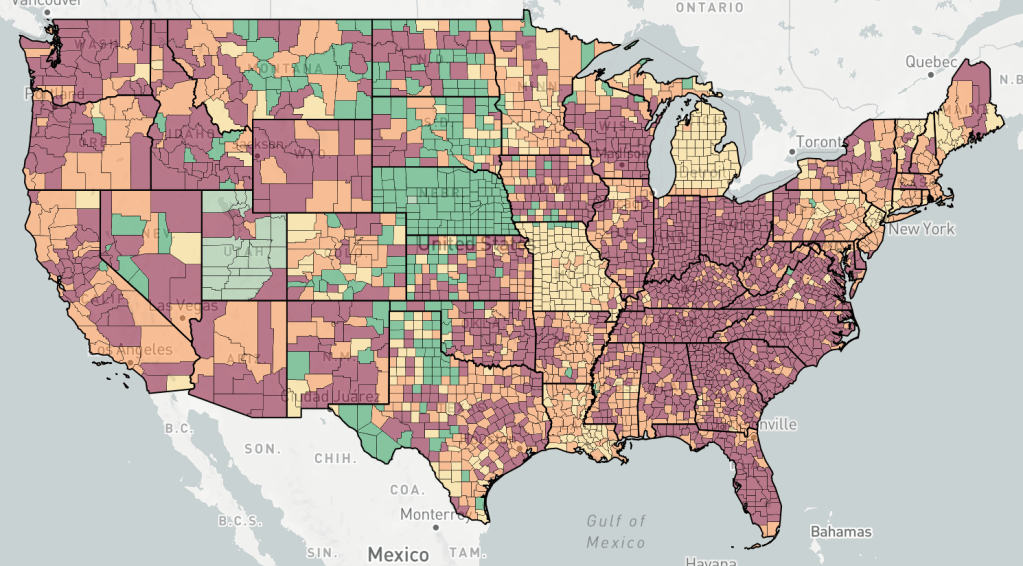
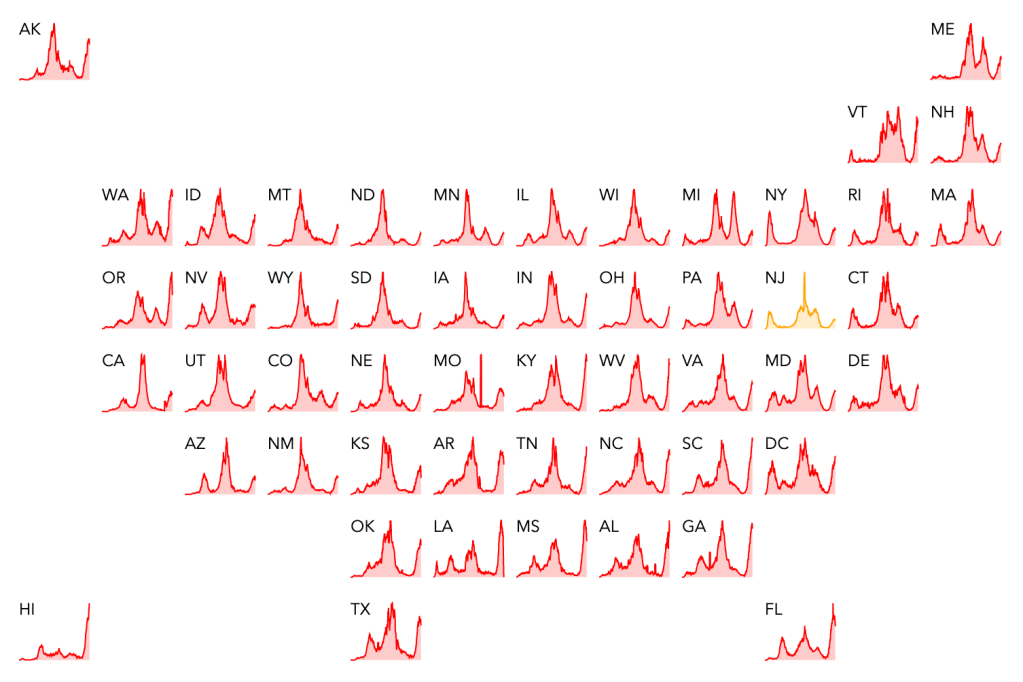
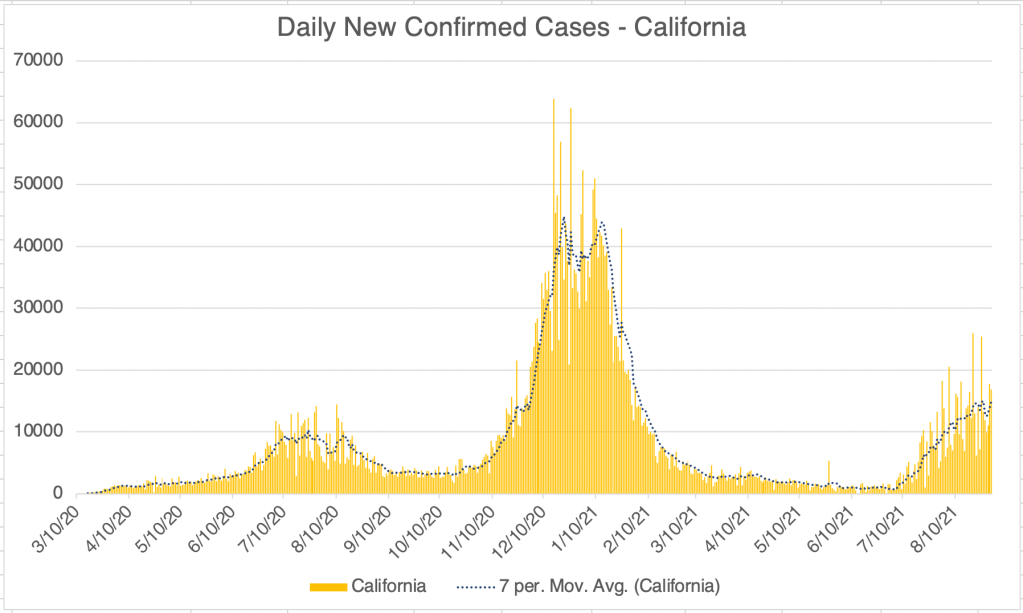
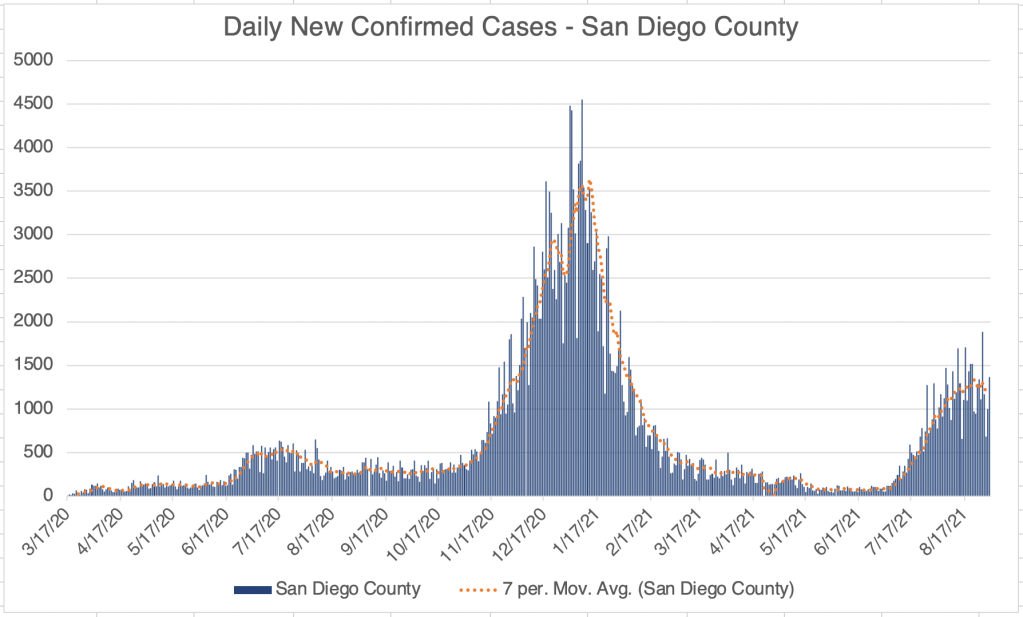
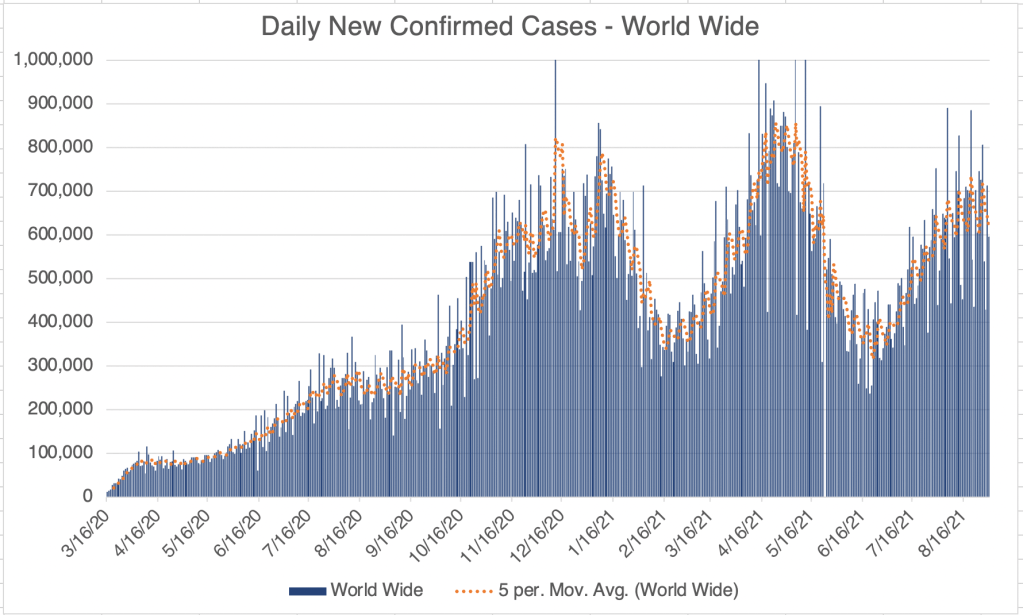
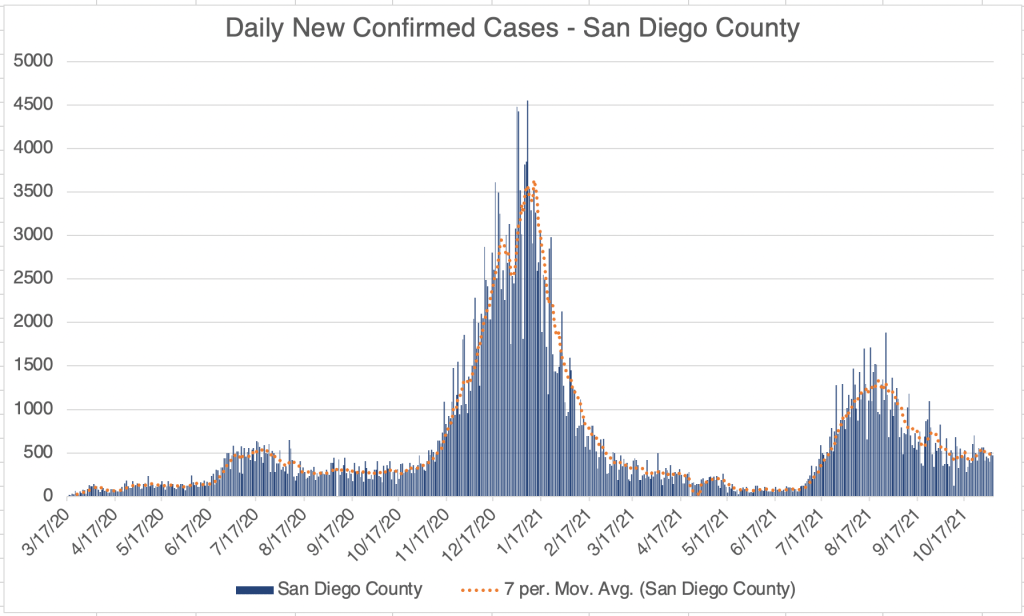
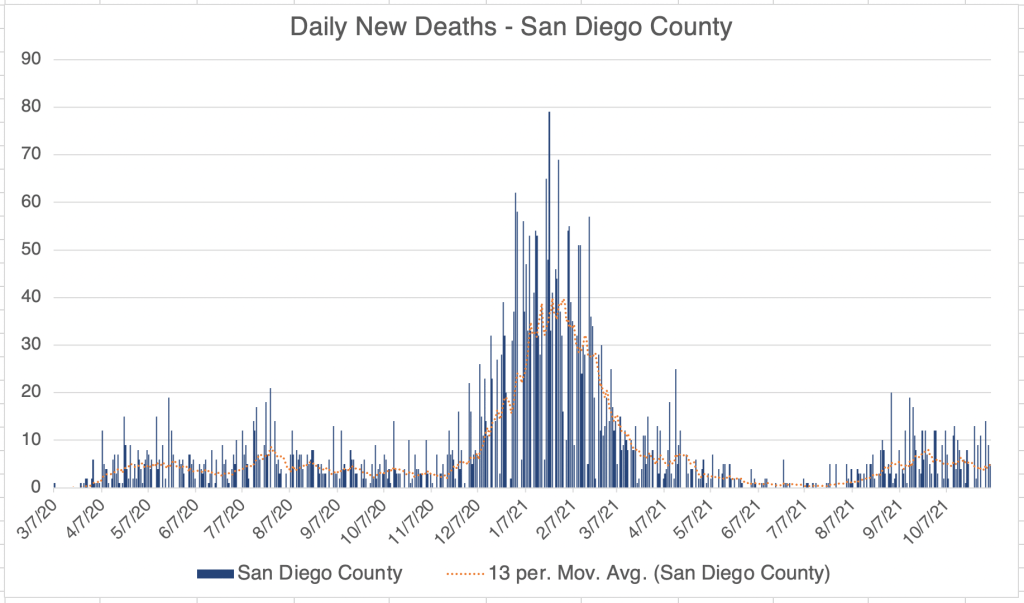
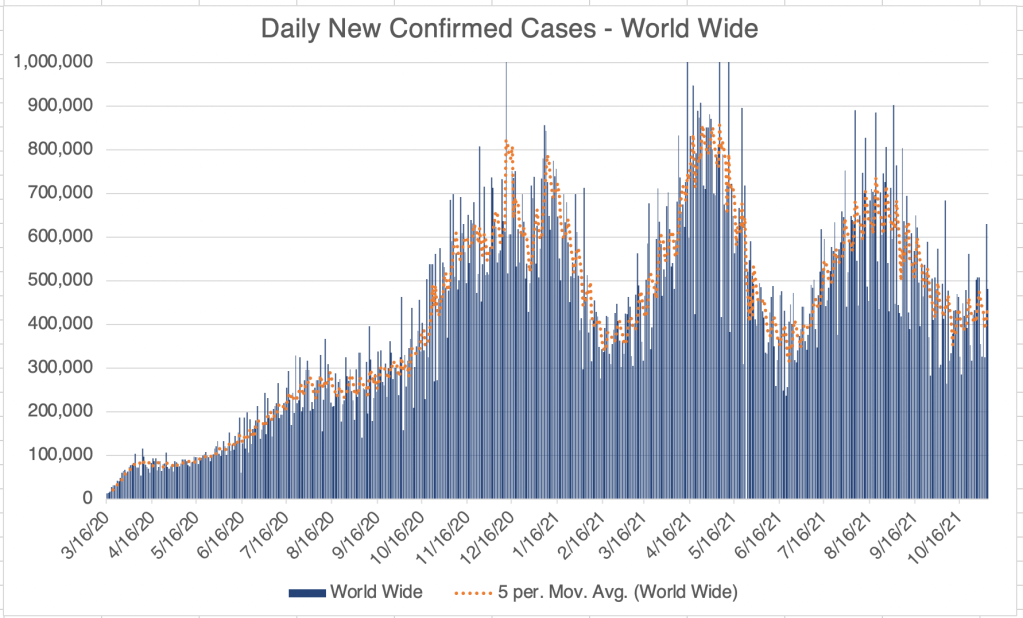
New cases in the US, California, and San Diego County are all fluctuating right now. It’s hard to say if this represents the beginning of a new wave. Most of us are feeling like the pandemic is basically over, but I will point out that in the post-Delta trough, we still have as many new cases per day as we did at the peak of last Summer’s wave. Minnesota, Colorado, New Mexico, and Arizona are all experiencing increases in cases right now.






V@¢¢!ne mandate finally drops: In September, the President said he wanted government agencies to produce a mandate for v@¢¢¡nation. Just this week, OSHA issued an Emergency Temporary Standard. This is official form of the v@¢¢¡ne mandate we’ve been waiting for. The mandate conforms to the news you’ve heard, all employers with more than 100 employees must get v@¢¢¡nation status from all employees, and those who are not v@¢¢¡nated must be tested weekly. The testing option means that the standard does NOT require that everyone be v@¢¢¡nated. Enforcement will begin January 4th, 2022.
Full length OSHA Emergency Temporary Standard.
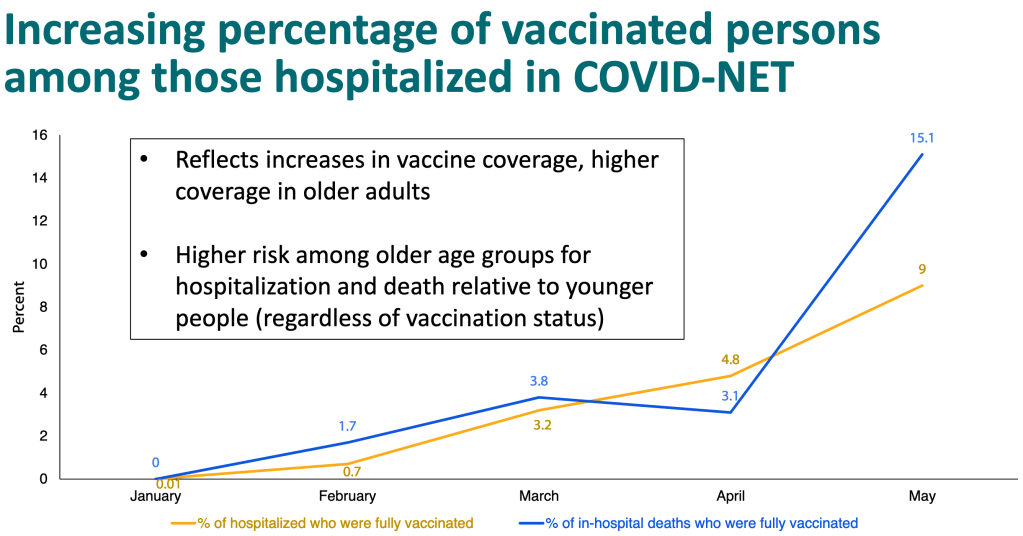
As we saw last week, the CDC has known since July that a significant number of hospitalizations and deaths have occurred in fully v@¢¢¡nated individuals. In addition to this, a recent Lancet paper from Singanayagam et al suggests that the transmission of Delta is less from v@¢¢inated individuals, but is still very significant. In light of this, I think all employees, regardless of v@¢¢¡nation status, should be tested regularly, although it would be impossible to test everyone every week. Ignoring the transmission threat from v@¢¢inated individuals is likely to lead to trouble. Everyone exposed to someone who tested positive for COVID should also be tested.
I saw a truly amazing thing on an OSHA FAQ page regarding v@¢¢ination. I checked it again just now to make sure it was still there. Under the item “Are adverse reactions to the COVID-19 v@¢¢¡ne recordable on the OSHA recordkeeping log?” The answer reads:
DOL and OSHA, as well as other federal agencies, are working diligently to encourage COVID-19 vaccinations. OSHA does not wish to have any appearance of discouraging workers from receiving COVID-19 vaccination, and also does not wish to disincentivize employers’ vaccination efforts. As a result, OSHA will not enforce 29 CFR 1904’s recording requirements to require any employers to record worker side effects from COVID-19 vaccination at least through May 2022. We will reevaluate the agency’s position at that time to determine the best course of action moving forward.
In effect, an official government page is saying, we are asking you to ignore health information in order to get people to do what we want. Some of you may be wondering why so many people are willing to ignore official calls to get v@¢¢¡nated, or are suspicious of government in general. This is why. This also answers the question as to why it is so difficult to get clear information on adverse events. The government appears to have an official policy of ignoring these events.

I’ll say again what I’ve said many times, I am not anti-v@¢¢¡ne. I think many people with risk factors including age, obesity, respiratory or cardiac issues, those who work closely with the public, etc. should get v@¢¢¡nated. However, I am against a v@¢¢¡ne mandate. I am not v@¢¢¡nated, mostly because of the ADE issue, and because I think I can avoid being infected.
I will also state what is obvious to many, but not to some that are making policy. Lying or hiding information from the public will make people mistrust you. You can sometimes force people to comply, but you cannot, even in principle, force people to trust you. Trust must be earned. Once you lose it, it is very difficult to get back.
This rule can be applied to any area of life. Remember this if you’re a husband, wife, parent, child, pastor, politician, consultant, leader of a company, employee, or anything else where trust is required. Trust is earned, and once broken, is very hard to get back.
Should you get a booster?: Several people in the past few weeks have asked me if they should get a booster. Right now, unfortunately, my best answer is “I don’t know”. A booster may improve your immune response to the originally Wuhan strain of the SARS-2 virus, but the Spike protein from the v@¢¢¡ne is likely toxic on it’s own. In addition, the paper from Japan I wrote about some time ago suggests that another booster of the current variety is unlikely to provide complete protection against Delta. Instead they recommend a Delta derived booster.
Anyone who has had COVID or has been v@¢¢¡nated should get a Delta v@¢¢¡ne as soon as it is available to protect from any ADE related effects. Several companies are currently working on v@¢¢¡nes against Delta.
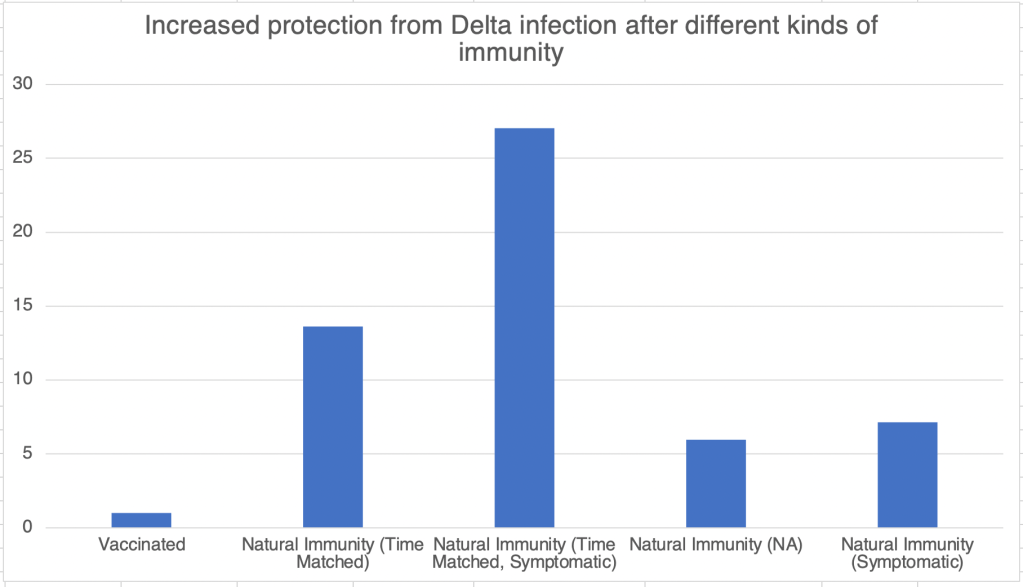
Does the v@¢¢¡ne create variants?: A nobel prize winning scientist is claiming that v@¢¢¡nation creates SARS variants. I absolutely agree that v@¢¢¡nation creates selection pressures that can force viruses to gain new forms to avoid neutralization. However, the very same can be said for natural immunity. Both natural immunity and v@¢¢¡nation create selection pressures that can lead to new viral variants. This is true of all viruses and other invading agents. In spite of this, our bodies are designed to use the immune system to fight off infection, and immunity has had a tremendous benefit, despite the selection pressure it poses. ADE is a rare exception to this rule. Our immune systems work much more quickly than viruses can adapt to them, which is why they are so effective at preventing infectious disease.
____________________________________
Updated November 23rd, 2021:
No COVID case update this week. Like last week, new cases are persistent in the US, California, and San Diego County.
However, just wanted to note that the 5th circuit has placed a second stay on the OSHA vaccine mandate until further notice. OSHA has suspended efforts to enforce the mandate. Text on the OSHA website reads:
“On November 12, 2021, the U.S. Court of Appeals for the Fifth Circuit granted a motion to stay OSHA’s COVID-19 Vaccination and Testing Emergency Temporary Standard, published on November 5, 2021 (86 Fed. Reg. 61402) (“ETS”). The court ordered that OSHA “take no steps to implement or enforce” the ETS “until further court order.” While OSHA remains confident in its authority to protect workers in emergencies, OSHA has suspended activities related to the implementation and enforcement of the ETS pending future developments in the litigation.”
_______________________________________
Don’t fear, but be smart!
Erik